")
Back to Journals » Journal of Pain Research » Volume 13
Effect of Neuraxial Analgesic Procedures on Intraoperative Hemodynamics During Routine Clinical Care of Gynecological and General Surgeries: A Case–Control Query of Electronic Data
Authors Gallegos G, Morgan CJ , Scott G, Benz D, Ness TJ
Received 6 March 2020
Accepted for publication 9 May 2020
Published 22 May 2020 Volume 2020:13 Pages 1163—1172
DOI https://doi.org/10.2147/JPR.S252760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Robert B. Raffa
Gabriel Gallegos,1 Charity J Morgan,2 Garrett Scott,1 David Benz,1 Timothy J Ness1
1Department of Anesthesiology and Perioperative Medicine, University of Alabama at Birmingham, Birmingham, AL 35205, USA; 2Department of Biostatistics, University of Alabama at Birmingham, Birmingham, AL 35205, USA
Correspondence: Timothy J Ness
Department of Anesthesiology and Perioperative Medicine, University of Alabama at Birmingham, BMR2-208, 901 19 th St. S, Birmingham, AL 35205 Tel +1 205-975-9643
Fax +1 205-934-7437
Email [email protected]
Background: The purpose of this study was to determine whether neuraxial analgesic procedures affect intraoperative hemodynamics and/or postoperative outcomes. Previous studies have examined effects in small samples of patients in highly controlled research environments. This study examined “real-world” data from a large sample of subjects receiving routine clinical cares.
Methods: A matched case–control analysis of electronic medical records from a large, academic hospital was performed. Patients who underwent neuraxial procedures preoperatively for postoperative analgesia for abdominal surgery (n=1570) were compared with control patients matched according to age, sex, ASA class and type of surgical procedure. Intraoperative hemodynamic measures, fluids and pressor utilization were quantified. Postoperative outcomes were determined based on the changes in laboratory values, the ordering of imaging studies and admission to an intensive care unit during the seven days following surgery as well as 30-day mortality.
Results: Medical records of 1082 patients who received an epidural catheter placement and 488 patients who received a lumbar intrathecal morphine injection were compared with an equal number of matched control patients. Preoperative placement of an epidural catheter for the management of postoperative pain was demonstrated to be associated with significant reductions in mean arterial pressure intraoperatively and poorer postoperative outcomes (more intensive care unit [ICU] admissions, more myocardial injuries) when compared with controls. A similar analysis of preoperatively administered intrathecal morphine injections was not associated with intraoperative alterations in blood pressure and had improved outcomes (less ICU admissions) in comparison with controls.
Conclusion: In a “real-world” sample, intrathecal morphine administration proved to be highly beneficial as a neuraxial analgesic procedure as it was not associated with intraoperative hypotension and was associated with improved clinical outcomes, in contrast to opposite findings associated with epidural catheter placement. There should be a careful consideration of elective neuraxial method utilized for postoperative pain control, with the present study raising significant concerns related to the use of epidural analgesia and its potential effect on clinical outcomes.
Keywords: neuraxial analgesia, hypotension, perioperative outcomes
Background
Preoperative neuraxial interventions for postoperative pain control are effective and widely used practices.1 Epidural analgesia has been shown to provide better post-operative pain relief when compared to use of intravenous opioid patient-controlled analgesia in patients undergoing intra-abdominal surgery.2 Epidural analgesia has also been shown to reduce the duration of postoperative tracheal intubation and reduces renal and gastric complications3,4 and provides modulation of the autonomic nervous system.5–7 Single-injection intrathecal opioids for postoperative analgesia have also been utilized,8 which has been demonstrated to provide adequate pain control when compared to epidural analgesia,9,10 benefits in reduction of systemic opioids postoperatively,11 and may reduce intensive care unit length of stay while maintaining cardiac stability.12
There is a concern that epidural administration of medication with local anesthetic can produce hypotension due to conduction blockade of sympathetic nervous system fibers causing arterial and venous vasodilation13 which may be potentiated under general anesthesia when high doses and concentrations of local anesthetic are administered prior to induction.14,15 Even postoperative dosing of epidurals in patients undergoing large abdominal procedures such as pancreaticoduodenectomies can lead to sufficient hypotension that limit their use.16 Additionally, intrathecal narcotic analgesia may also cause hemodynamic depression in patients undergoing general anesthesia when coupled with restrictive fluid management.17 The practice at our institution is to perform neuraxial procedures preoperatively with either single-dose use of intrathecal morphine or placement of catheters into the epidural space with eventual infusion of dilute local anesthetic and opioid solutions. It is unknown whether neuraxial procedures used in this fashion have any significant effects on intraoperative hemodynamics.
Intraoperative hypotension, defined by a decrease in mean arterial pressure (MAP) has been shown to have a detrimental impact on postoperative morbidity and mortality.18 Recently, in a systematic review of multiple studies, Wesselink and colleagues reported that intraoperative hypotension increases the risk of adverse outcomes such as stroke, myocardial injury, acute kidney injury, and mortality.19 Specifically, moderate risk of end-organ injury was present when hypotension was prolonged or severe; and even mildly elevated risk was seen when MAP < 80 mmHg >10 minutes.19 Conversely, intraoperative tachycardia and hypertension have also been shown to be independently associated with adverse outcome in non-cardiac surgery of long duration.20
Given the mix of benefits and risks associated with neuraxial procedures for postoperative pain and the potential for intraoperative hypotension and its sequelae, we felt it was appropriate to assess the experience of our own institution. Therefore, the objective of this study was to determine if there are any observable intraoperative hemodynamic changes while under general anesthesia in patients who received a preoperative epidural catheter placement or preoperative intrathecal morphine injection as treatments intended for postoperative pain control.
Methods
Human Subjects
This informatics-based study was conducted at the University of Alabama at Birmingham University Hospital by querying the electronic medical record database and concluded to be exempt from oversight for human subject research by the University of Alabama at Birmingham Institutional Review Board due to its use of de-identified data. Medical records of patients who underwent general anesthesia for a non-emergent abdominal surgery by either a gynecologic or general surgeon between the dates of 1/1/2013 - 2/22/2017 at the University of Alabama at Birmingham Hospital were selectively queried in a de-identified fashion stratified using billing codes. Extracted data consisted of age, American Society of Anesthesiologists (ASA) physical status classification, sex, surgical specialty, primary surgeon, imaging and laboratory values (obtained preoperatively and for seven days postoperatively), pre- and intraoperative drugs utilized and pre- and intraoperative hemodynamic data. Two experimental groups were created based on whether they had received a preoperative neuraxial procedure for postoperative pain control: those that had an epidural catheter placement (Epidural Treatment group) and those that had a preoperative intrathecal morphine injection (Intrathecal Treatment group). Since there were significant differences in the demographics of the Epidural Treatment group and the Intrathecal Treatment group (see Table 1), two separate control groups were identified for comparison (Epidural and Intrathecal Control groups, respectively). The experimental subjects were then each matched at a 1:1 ratio with control subjects based on age (±5 years), ASA classification, sex, and type of surgery. To limit variability, subjects were restricted to those who were ASA status 2 or 3 in non-emergent, non-obstetric cases.
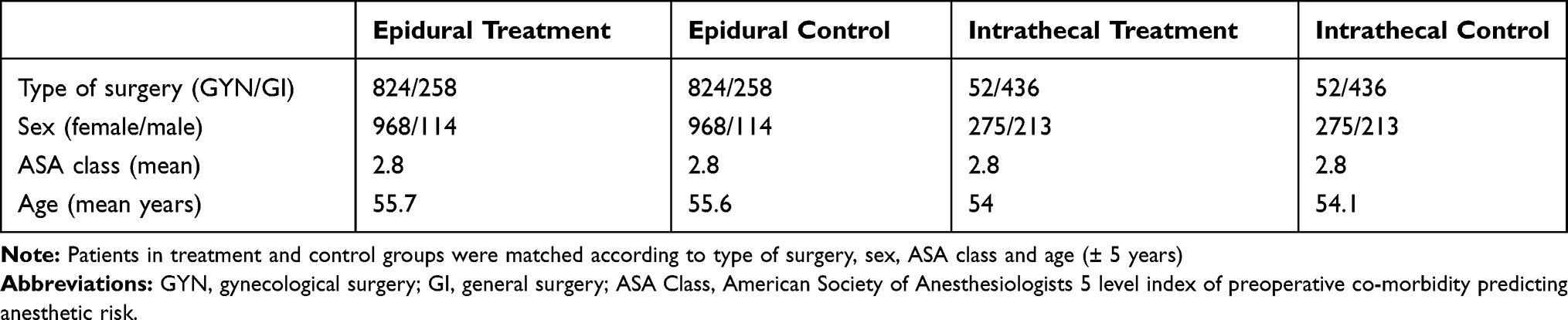 |
Table 1 Demographics of Study Groups |
Epidural Analgesia
Epidural catheters were placed using a loss-of-resistance technique while in the pre-anesthesia preparation area. The precise levels of catheter placement are not known from this analysis but billing codes indicated they were at a thoracic level in 942 subjects and at a lumbar level in 140 subjects. Following epidural catheter placement, a test dose of 3 mL of 1.5% lidocaine with 1:200,000 parts epinephrine added is always injected epidurally as a “test” dose. Catheters are replaced if identified as intravascularly placed. If an intrathecal catheter placement is identified, it is removed and either the procedure abandoned or the catheter replaced. Only subjects with negative test doses were included as part of the Epidural Treatment group. Charting related to the precise timing of the start of epidural infusions was unreliable and not extractable in a de-identified fashion. As a consequence, it is unknown whether individual subjects in the Epidural Treatment group received more than a test dose of local anesthetic preoperatively. There is variable practice among practitioners at our center with some starting epidural infusions of dilute (0.1%) bupivacaine and fentanyl (5–10 micrograms per mL) at the beginning of the case and others waiting until arrival in the post-anesthesia care unit. The only consistent practice pattern of our anesthesiologists is to discontinue intraoperative epidural infusions if there is sustained hypotension.
Intrathecal Morphine Analgesia
All subjects in the Intrathecal Treatment group received their injections in the pre-anesthesia preparation area, typically 30–60 minutes prior to presentation to the operating rooms. These injections were performed at lumbar levels below the level of the conus medullaris and consisted of 100 or 150 micrograms of preservative-free morphine sulfate diluted in 1–2 mL of normal saline.
Control Subject Pretreatments
All subjects in the two Control groups received care in the pre-anesthesia preparation area, typically 30–60 minutes prior to presentation to the operating rooms. There they received sedation and hydration at the discretion of the attending anesthesiologist.
Hemodynamic Measures
In order to selectively assess the intraoperative effects of the neuraxial procedures, hemodynamic measures which were analyzed were limited to those obtained in the pre-anesthesia preparation area, during the pre-induction period and for 60 minutes post-induction of general anesthesia. This limited-time allowed for a consistent period of measure and to avoid variability due to other causes that occur later in cases such as surgical blood loss. In most cases non-invasive blood pressures are obtained approximately every three minutes but in some cases a more frequent measuring of blood pressure occurred. Measures of hypotension duration were based on each individual measure. For purposes of graphical display and analysis, multiple measures obtained over six minute periods were averaged.
Intraoperative Drug/Fluid Administration
Vasoactive agents and fluids administered intraoperatively were extracted from patient records. “More than minimal” intravenous vasopressor use was arbitrarily defined as any total amount greater than 80 μg phenylephrine (including infusions) or 10 mg ephedrine or any use of epinephrine or vasopressin. The rationale for this definition is that it is a common practice at our institution for one or two doses of ephedrine (5 mg) or phenylephrine (40 μg) to be given intravenously during the period of time immediately following induction but repeated doses typically represents a patient-related issue.
Clinical Outcomes
Outcomes data were derived from post-operative measures documented in their medical record. Subjects’ were defined as having a significant elevation in serum troponin levels representative of a myocardial injury if measured as ≥0.03 ng/mL within seven days of the surgery. It is not the practice at our institution to obtain preoperative serum troponin measures, but other “standard” labs are more commonly obtained. As a consequence, renal injury could be defined as a rise of serum creatinine measures of 0.3 mg/dl over preoperative serum creatinine levels within seven days of the surgery. Order of a head CT (computed tomography) within seven days of surgery was used as a surrogate of mental status changes. Admission to an intensive care unit (ICU) within seven days of surgery was used as a surrogate of a deteriorated clinical condition. Administration of naloxone was used as a surrogate of presumed opioid-induced respiratory depression. A death note within 30 days of the surgery was used as a measure of 30-day mortality. Use of de-identified data limited additional definition of precise clinical conditions. Pulmonary function, pain and analgesia were not studied as clinical outcomes in the current analysis.
Statistics
Mean hemodynamic measures for the Epidural and Intrathecal Treatment groups were compared to their matched controls using a repeated measures two-way ANOVA with Bonferroni-corrected post hoc comparisons. Duration of hypotension/tachycardia data was quantified in minutes meeting the defined criterion (eg, number of minutes with MAP ≤ 65 mm Hg) which were then compared using an unpaired t-test. Fisher’s test (χ2) was used to compare categorical data. P<0.05 was considered statistically significant. Data are presented as the mean ± standard deviation unless otherwise stated.
Results
Patient and Procedure Characteristics
The Epidural Treatment group did differ from the Intrathecal Treatment group in that more women and gynecological surgeries were present in that group such that a direct comparison of data from these two groups was not deemed appropriate and hence the two separate control cohorts were identified for comparison. As would be expected based on the selection of a matched cohort, the age, sex, ASA class and surgical types were similar in treatment groups versus their control groups (Table 1). Gynecological surgeries involved non-obstetric, abdominal surgery for both benign and malignant disorders involving the ovaries, uterus, vagina and/or Fallopian tubes. General surgeries involved abdominal surgery for both benign and malignant disorders involving the gallbladder, pancreas, stomach, small intestine, colon and/or rectum. Vascular and urological surgeries were not included in these patient samples. The duration of the cases was statistically longer in both Treatment groups in comparison with their respective Controls (Epidural Treatment group 216±115 min vs 182±82 min for Epidural Control group, p<0.001; Intrathecal Treatment group 247±108 min vs 230±117 min for Intrathecal Control group, p=0.0187).
Repeated Hemodynamic Measures
Preoperatively the mean arterial pressures (MAPs) and heart rates (HRs) of both the Epidural Treatment group and the Intrathecal Treatment group were significantly elevated in the pre-anesthesia preparation area when compared with their respective Control groups (see “Pre” measures in Figure 1). Notably, these patients with elevated MAPs and HRs were all about to undergo a preoperative neuraxial procedure. In the operating rooms immediately prior to the induction of general anesthesia, MAPs were significantly lower in both Treatment groups when compared with their own pre-anesthesia preparation area measures. Similarly, the MAP and HR of the Epidural Treatment group were lower in comparison with its Control group immediately prior to the induction of general anesthesia, whereas the HRs but not the MAPs of the Intrathecal Treatment group were lower than the Intrathecal Controls at the same time point. Following induction of general anesthesia, all four groups demonstrated reductions in their MAP and initial increases in their HRs followed by a return to pre-induction levels. The Epidural Treatment group but not the Intrathecal Group had statistically significant lower MAPs in comparison with their respective Control groups in the first 30 minutes following induction (Figure 1). HRs were statistically lower at most time points in the Epidural Treatment Group in comparison with its Control group; a similar, but statistically less robust effect was present in the HRs of the Intrathecal Treatment group in comparison with its Control group. The overall differences between the groups were small in relation to average MAP values, differing by only a few mm Hg of pressure for the total samples. However, there was significant variability within each of the groups. To capture the magnitude of hypotension in these patients, the number of minutes in which MAPs were at or below 75, 65 and/or 55 mm Hg pressure respectively during the first hour after the induction of general anesthesia were also quantified. As apparent in the upper section of Table 2, the Epidural Treatment group had statistically more minutes of low MAPs that were ≤75 mm Hg and ≤65 mm Hg pressure when compared with the Epidural Control group. In contrast, there were no differences in minutes of low MAPs between the Intrathecal Treatment and the Intrathecal Control groups (Table 3).
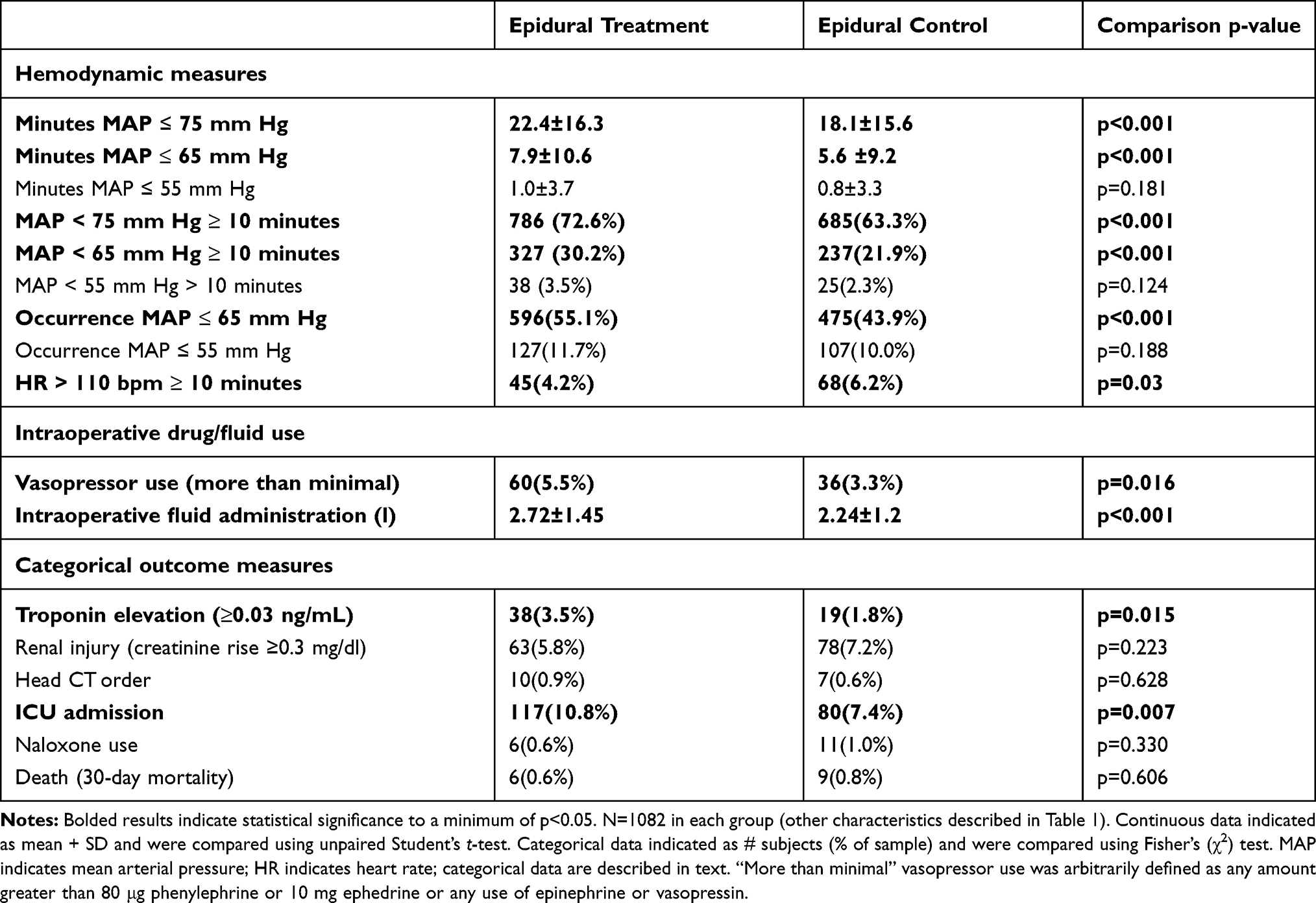 |
Table 2 Effect of Epidural Treatment on Intraoperative Hemodynamics and Postoperative Outcomes |
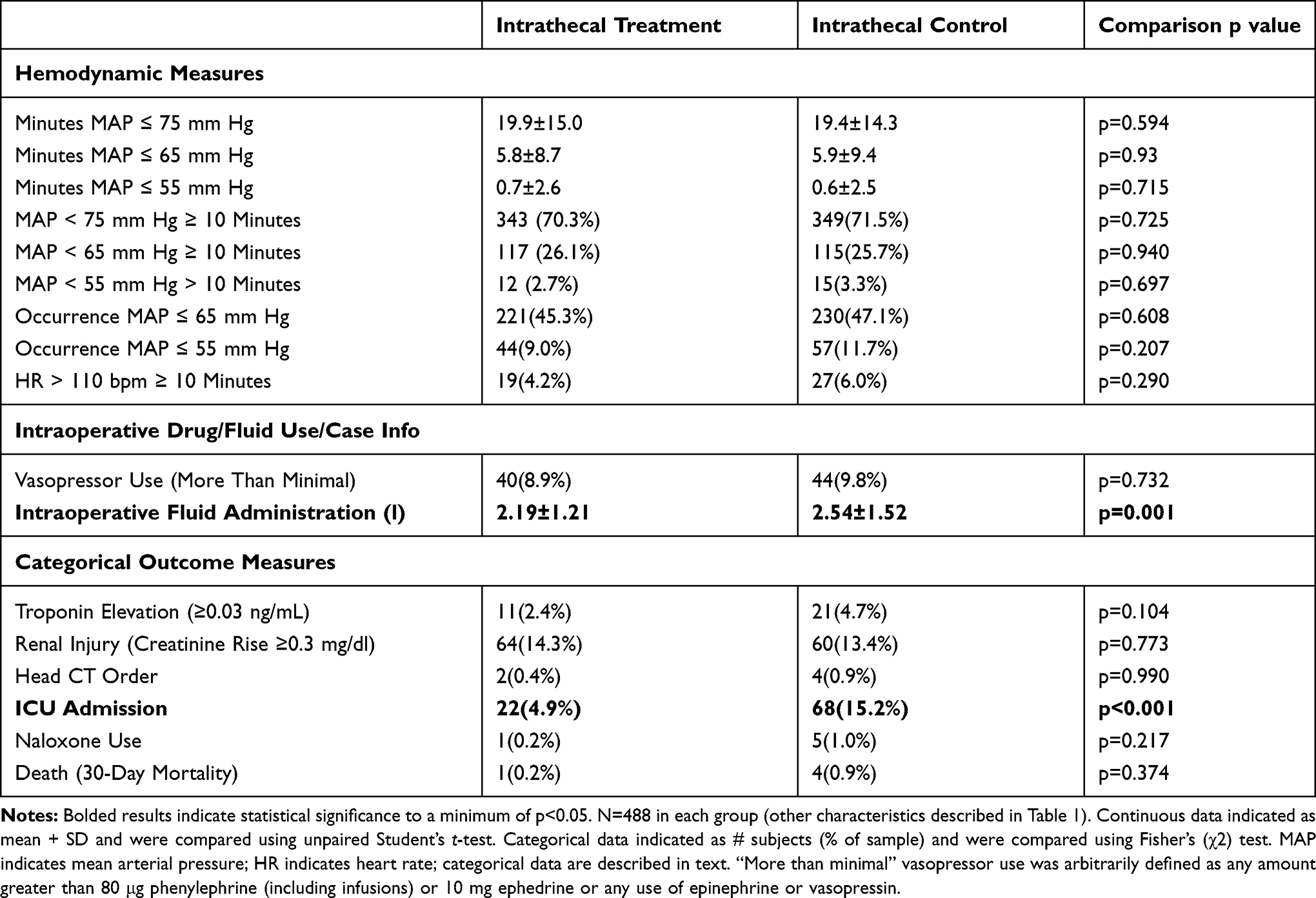 |
Table 3 Effect of Intrathecal Treatment on Intraoperative Hemodynamics and Postoperative Outcomes |
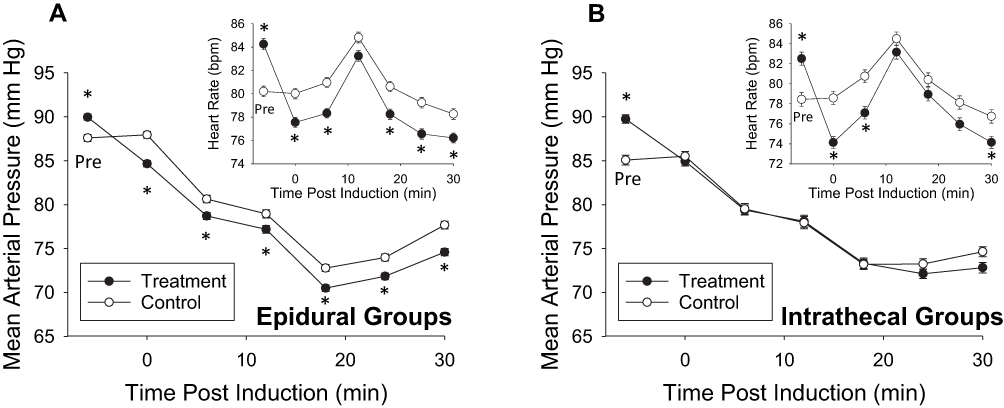 |
Figure 1 Intraoperative hemodynamic measures for subjects who received preoperative neuraxial procedures for postoperative pain management. In panel (A), data for subjects who had epidural catheters placed (Treatment n=1082) and their matched cohort (Control; n=1082). In panel (B) data for subjects who had intrathecal morphine injections (Treatment; n=488) and their matched cohort (Control; n=488). Large graphs present mean arterial pressure measures preoperatively (Pre) and as means of multiple blood pressure measurements for the 6-minute periods preceding the indicated time post-induction of general anesthesia. A 30-minute post-induction period was chosen as most representative of the effect of the neuraxial procedures. Insets present similar representation of heart rate measures. Data represents Means ± SEM. *Indicates statistically significant difference between Treatment and Control measures, p<0.05. |
Categorical Hemodynamic Measures
Using the results of the published literature correlating poor outcomes with hemodynamic alterations as a guide [eg, 19,20], operational definitions of hemodynamic criteria were defined as occurrences of MAP ≤ 65 or ≤55 mm Hg, or periods of MAP measurement ≤75, ≤65 or ≤55 mm Hg for 10 or more minutes or periods of HR ≥ 110 bpm for 10 or more minutes. These categorical measures were all limited to the first hour following the induction of general anesthesia. As indicated in Table 2, the Epidural Treatment group had statistically more occurrences of low MAP ≤ 65 mm Hg, more periods of low MAP ≤ 75 mm Hg and ≤65 mm Hg for 10 or more minutes than was noted in the Epidural Control group. This finding is consistent with a significantly greater use of pressors and a significantly greater amount of fluid administration in the Epidural Treatment group than in the Epidural Control group (Table 2). There were, however, significantly fewer subjects who experienced HRs >110 bpm for 10 minutes or more in the Epidural Treatment group in comparison with its Epidural Control group. Similar to the continuous hemodynamic measures, there were no statistically significant differences in the categorical hemodynamic measures or pressor use when the Intrathecal Treatment group was compared with the Intrathecal Control group (Table 3).
Categorical Clinical Outcome Measures
The most robust correlation with neuraxial procedures was observed in admissions to intensive care units (ICUs). Whereas subjects in the Epidural Treatment group had significantly more ICU admissions than subjects in the Epidural Control group (Table 2), the opposite was true for the Intrathecal Treatment group which had fewer ICU admissions than the Intrathecal Control group (Table 3). The other measured clinical outcome that found clinical significance was the incidence of perioperative myocardial injury as determined by an elevation in serum troponin levels, which was significantly greater in the Epidural Treatment group than in the Epidural Control group. A similar increase in incidence was not noted in the Intrathecal Treatment group. There were no other statistically significant differences in clinical outcome measures noted. We were not able to extract reliable data related to the incidence of pulmonary dysfunction, however one would expect if the patient had a tenuous respiratory status, they would be transferred to the ICU.
Discussion
The most important finding of the present matched case–control study was that placement of an epidural catheter for postoperative pain control was associated with greater intraoperative hypotension and increases in ICU admission and perioperative myocardial injury. That epidural analgesia might be associated with lower blood pressures intra-operatively was not wholly unexpected, given its known effects at producing sympathectomy. Preoperative oral consumption restrictions and treatment with a bowel preparation prior to abdominal surgery (both of which would be likely in elective gynecologic and general surgery cases) would potentially result in hypovolemia that would make the effects of any sympathectomy more prominent. What was not expected prior to our performing this analysis was the magnitude and duration of the depressor responses in some individuals and the differences noted in clinical outcomes. Our pre-analysis bias was that any depressor responses could and would be appropriately treated with pressor agents such that few intraoperative differences would be noted except perhaps in the use of pressors. We also expected to see improvements in clinical outcomes such as was observed in the Intrathecal Treatment group. What was noted in the Epidural Treatment group was more pressor use, more fluid administration and despite that, more prolonged depressions in MAP in patients undergoing general anesthesia who had an epidural catheter in place. This group also had poorer clinical outcomes when compared with controls. Low intraoperative MAPs have been associated with deleterious clinical outcomes in multiple perioperative investigations19 and so the association seems logical. Given that the Intrathecal Treatment group had benefits without the problems noted in the Epidural Treatment group, it would suggest that this neuraxial method should be the preferred method as a postoperative analgesic technique.
We are not the first to observe potentially deleterious effects of epidural analgesia for postoperative pain control coupled with general anesthesia. The unadjusted analysis of the POISE 2 study21 reported that 69.7% of subjects who received general anesthesia and a thoracic epidural catheter (similar to most of the Epidural Treatment group in the present study) had clinically important hypotension compared with 55.5% of subjects who only received general anesthesia (p<0.001 for difference) and the rate of perioperative myocardial infarctions in the epidural group was 9.6% versus 5.6% in the no epidural group (p<0.001 for difference). Similar, but even more robust deleterious effects were noted in the original POISE study.22 Belavy et al23 noted that subjects having general anesthesia for an abdominal hysterectomy who also received an epidural catheter for postoperative pain (a group that formed the largest sample of the present study) had a greater number of postoperative complications.
This is not to say that there are no reports of significantly improved clinical outcomes in subjects who selectively received epidural analgesia for postoperative pain control. However, of recent reports, those with statistically robust benefits of treatment appear related predominantly to upper abdominal surgeries such as pancreatic or hepatic surgery24–26 but not lower abdominal surgeries such as colorectal surgery or cystectomy.27–30 The most common improvements in outcome that have been noted relate to pulmonary function. DaSilva et al,27 who quantified factors such as ICU days, length of hospitalization and cost of hospitalization found epidural analgesia for laparoscopic colectomy surgeries resulted in longer hospital stays and higher costs in comparison with patients treated with conventional analgesia. This is in contrast to multiple reports demonstrating generally positive effects of single-shot intrathecal opioid injections31–34 with shorter lengths of stay, improved analgesia and improved or unchanged risk of complications. There are few head-to-head comparisons of intrathecal treatment with epidural treatment. We are not able to do such a true comparison in the present data set since our baseline patient characteristics differed between the two groups, but the opposite direction of effects suggest intrathecal treatment may be preferable to epidural treatment. A recent report by Kjolhede and colleagues35 did perform a comparison of the two treatments and found advantages to the intrathecal treatment they utilized over the epidural treatment they utilized. However, since they also administered bupivacaine as part of their intrathecal treatment, we can make only limited comparison with our study results.
The present study is unique in that it represents a “real-world” experience of use of neuraxial procedures for the control of postoperative pain with only standard-of-care clinical criteria used for inclusion/exclusion of neuraxial treatment (eg, presence of anticoagulation) and routine clinical cares given intra- and peri-operatively (as opposed to using tightly controlled research protocols). This allowed us to observe what is more likely to occur in a typical non-research-based practice although one must recognize that unique aspects of our own institutional practices may not reflect those of other institutions. Our study is also unique because it presents an analysis of intraoperative hemodynamics which are normally only briefly mentioned or left unanalyzed in other reports related to clinical outcomes. We were unable to find any literature reference that presented hemodynamic data in association with neuraxial procedures in a similar, categorical fashion.
In our study, we selected a standardized period of time post-induction of general anesthesia for quantitative analysis since this is the time when anesthesia-induced hypotension occurs and when active surgical factors such as blood loss are less unlikely to alter hemodynamic measures. For this reason, we believe it offers a realistic assessment of the intraoperative hemodynamic effects of the neuraxial procedures themselves. There are obvious limitations associated with the present study. It was a retrospective analysis that has all of the limitations that such an analysis entails. With its methodology, we were not able to assess all important outcomes, in particular, we were not able to perform a focal evaluation of pulmonary function and we did not collect data related to other potential confounders (eg, intraoperative body temperature, hypotension outside of the study period) and potential interactions between these unmeasured variables. That said, numerous important outcomes were able to be assessed using de-identified data extraction.
Conclusions
The present study observed a correlation between placement of an epidural catheter preoperatively for postoperative pain control and intraoperative blood pressures, a correlation that was not observed when intrathecal morphine was administered preoperatively for postoperative pain control. An increased incidence of ICU admissions and postoperative myocardial injuries was also noted when an epidural catheter was placed. Although causality can not be determined by an observational study, the most parsimonious interpretation of these results suggests that there may be advantage to the use of intrathecal opioids as a “do-no-harm” analgesic alternative since there appear to be beneficial effects on outcome coupled with the absence of the potential harms noted above for epidural analgesia. What is needed are prospective, controlled trials that compare epidural analgesia directly with intrathecal analgesia for multiple different types of surgery with an emphasis on evaluation of postoperative outcomes.
Abbreviations
ANOVA, analysis of variance; ASA, American Society of Anesthesiologists; CT, computed tomography; dl, deciliter; HR, heart rate; ICU, intensive care unit; IT, intrathecal; MAP, mean arterial pressure; mg, milligram; mL, milliliter; ng, nanogram; SEM, standard error of the mean; μg, microgram.
Data Sharing Statement
All de-identified data are available from the authors upon request.
Ethics Approval
This retrospective study of de-identified data was conducted at the University of Alabama at Birmingham University Hospital electronic medical record database and concluded to be exempt from oversight for human subjects research by the University of Alabama at Birmingham Institutional Review Board due to its use of de-identified data.
Consent for Publication
All authors give their consent for the publication of this manuscript.
Acknowledgments
The study built on previous observations by Andrew Cochran MD who performed an initial pilot trial addressing similar issues as part of a department-sponsored study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: enhanced Recovery After Surgery (ERAS) group recommendations. Arch Surg. 2009;144(10):961–969. doi:10.1001/archsurg.2009.170
2. Werawatganon T, Charuluxanun S. Patient controlled intravenous opioid analgesia versus continuous epidural analgesia for pain after intra-abdominal surgery. Cochrane Database Syst Rev. 2005;CD004088. doi:10.1002/14651858.CD004088.pub2
3. Nishimori M, Low JH, Zheng H, Ballantyne JC. Epidural pain relief versus systemic opioid-based pain relief for abdominal aortic surgery. Cochrane Database Syst Rev. 2012;CD005059. doi:10.1002/14651858.CD005059.pub3
4. Cashman JN, Dolin SJ. Respiratory and haemodynamic effects of acute postoperative pain management: evidence from published data. Br J Anaesth. 2004;93(2):212–223. doi:10.1093/bja/aeh180
5. Mahajan A, Takamiya T, Benharash P, Zhou W. Effect of thoracic epidural anesthesia on heart rate variability in a porcine model. Physiol Rep. 2017;5(7):e13116. doi:10.14814/phy2.13116
6. Shin S, Bai SJ, Rha KH, So Y, Oh YJ. The effects of combined epidural and general anesthesia on the autonomic nervous system and bioavailability of nitric oxide in patients undergoing laparoscopic pelvic surgery. Surg Endosc. 2013;27(3):918–926. doi:10.1007/s00464-012-2536-5
7. Licker M, Spiliopoulos A, Tschopp JM. Influence of thoracic epidural analgesia on cardiovascular autonomic control after thoracic surgery. Br J Anaesth. 2003;91(4):525–531. doi:10.1093/bja/aeg212
8. Levy BF, Tilney HS, Dowson HM, Rockall TA. A systematic review of postoperative analgesia following laparoscopic colorectal surgery. Colorectal Dis. 2010;12(1):5–15. doi:10.1111/j.1463-1318.2009.01799.x
9. Virlos I, Clements D, Beynon J, Ratnalikar V, Khot U. Short-term outcomes with intrathecal versus epidural analgesia in laparoscopic colorectal surgery. Br J Surg. 2010;97(9):1401–1406. doi:10.1002/bjs.7127
10. Hassan WMNW, Nayan AM, Hassan AA, Zaini RHM. Comparison of single-shot intrathecal morphine injection and continuous epidural bupivacaine for post-operative analgaesia after elective abdominal hysterectomy. Malays J Med Sci. 2017;24(6):21–28. doi:10.21315/mjms2017.24.6.3
11. Kong SK, Onsiong SM, Chiu WK, Li MK. Use of intrathecal morphine for postoperative pain relief after elective laparoscopic colorectal surgery. Anaesthesia. 2002;57(12):1168–1173. doi:10.1046/j.1365-2044.2002.02873.x
12. Elgendy H, Helmy HAR. Intrathecal morphine improves hemodynamic parameters and analgesia in patients undergoing aortic valve replacement surgery: a prospective, double-blind, randomized trial. Pain Physician. 2017;20(5):405–412.
13. Holte K, Foss NB, Svensen C, Lund C, Madsen JL, Kehlet H. Epidural anesthesia, hypotension and changes in intravascular volume. Anesthesiology. 2004;100(2):281–286. doi:10.1097/00000542-200402000-00016
14. Borghi B, Casati A, Iuorio S, et al. Frequency of hypotension and bradycardia during general anesthesia, epidural anesthesia, or integrated epidural-general anesthesia for total hip replacement. J Clin Anesth. 2002;14(2):102–106. doi:10.1016/S0952-8180(01)00362-2
15. Kasaba T, Kondou O, Yoshimura Y, Watanabe Y, Takasaki M. Haemodynamic effects of induction of general anaesthesia with propofol during epidural anaesthesia. Can J Anesth. 1998;45(11):1061–1065. doi:10.1007/BF03012392
16. Axelrod TM, Mendez BM, Abood GJ, Sinacore JM, Aranha GV, Shoup M. Peri-operative epidural may not be the preferred form of analgesia in select patients undergoing pancreaticoduodenectomy. J Surg Oncol. 2015;111(3):306–310. doi:10.1002/jso.23815
17. Hübner M, Lovely JK, Huebner M, Slettedahl SW, Jacob AK, Larson DW. Intrathecal analgesia and restrictive perioperative fluid management within enhanced recovery pathway: hemodynamic implications. J Am Coll Surg. 2013;216(6):1124–1134. doi:10.1016/j.jamcollsurg.2013.02.011
18. Charlson ME, MacKenzie CR, Gold JP, et al. The preoperative and intraoperative hemodynamic predictors of postoperative myocardial infarction or ischemia in patients undergoing noncardiac surgery. Ann Surg. 1989;210(5):637–648. doi:10.1097/00000658-198911000-00012
19. Wesselink EM, Kappen TH, Torn HM, Slooter AJC, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018;121(4):706–721. doi:10.1016/j.bja.2018.04.036
20. Reich DL, Bennett-Guerrero E, Bodian CA, Hossain S, Winfree W, Krol M. Intraoperative tachycardia and hypertension are independently associated with adverse outcome in noncardiac surgery of long duration. Anesth Analg. 2002;95(2):273–277. doi:10.1097/00000539-200208000-00003
21. Leslie K, McIlroy D, Kasza J, et al. Neuraxial block and postoperative epidural analgesia: effects on outcomes in the POISE-2 trial. Brit J Anaesth. 2016;116(1):100–112. doi:10.1093/bja/aev255
22. Leslie K, Myles KP, Devereaux P, et al. Neuraxial block, death and serious cardiovascular morbidity in the POISE trial. Brit J Anaesth. 2013;111(3):382–390. doi:10.1093/bja/aet120
23. Belavy D, Janda M, Baker J, Obermair A. Epidural analgesia is associated with an increased incidence of postoperative complications in patients requiring an abdominal hysterectomy for early stage endometrial cancer. Gyn Oncol. 2013;131(2):423–429. doi:10.1016/j.ygyno.2013.08.027
24. Sanford DE, Hawkins HG, Fields RC. Improved peri-operative outcomes with epidural analgesia in patients undergoing a pancreatectomy: a nationwide analysis. Int Hepatol Pancreato Biliary J. 2015;17(6):551–558. doi:10.1111/hpb.12392
25. Amini N, Kim Y, Hyder O, et al. A nationwide analysis of the use and outcomes of perioperative epidural analgesia in patients undergoing hepatic and pancreatic surgery. Am J Surg. 2015;210(3):483–491. doi:10.1016/j.amjsurg.2015.04.009
26. Popping DM, Elia N, Van Aken HK, et al. Impact of epidural analgesia on mortality and morbidity after surgery. AnnSurg. 2014;259:1056–1067. doi:10.1097/SLA.0000000000000237
27. DaSilva M, Lomelin D, Tsui J, Klinginsmith M, Tadaki C, Langenfeld S. Pain control for laparoscopic colectomy: an analysis of the incidence and utility of epidural analgesia compared to conventional analgesia. Tech Coloproctol. 2015;19(9):515–520. doi:10.1007/s10151-015-1336-z
28. Rigg JRA, Jamrozik K, Myles PS, et al. Epidural anaesthesia and analgesia and outcome of major surgery: a randomized trial. Lancet. 2002;359(9314):1276–1282. doi:10.1097/00000539-200302000-00046
29. Halabi WJ, Kang CY, Nguyen VQ, et al. Epidural analgesia in laparoscopic colorectal surgery: a nationwide analysis of use and outcomes. JAMA Surg. 2014;149(2):130–136. doi:10.1001/jamasurg.2013.3186
30. Winer AG, Sfakianos JP, Puttanniah VG, Bochner BH. Comparison of perioperative outcomes for epidural versus intravenous patient-controlled analgesia after radical cystectomy. Reg Anesth Pain Med. 2015;40(3):239–244. doi:10.1097/AAP.0000000000000219
31. Koning MV, Teunissen AJW, van der Harst E, Ruijgrok EJ, Stolker RJ. Intrathecal morphine for laparoscopic segmental colonic resection as part of an enhanced recovery program: a randomized controlled trial. Reg Anesth Pain Med. 2018;43(2):166–173. doi:10.1097/AAP.0000000000000703
32. Meylan N, Elia N, Lysakowski C, Tramer MR. Benefit and risk of intrathecal morphine without local anaesthetic in patients undergoing major surgery: meta-analysis of randomized trials. Br J Anaesth. 2009;102(2):156–167. doi:10.1093/bja/aen368
33. Roy J-D, Massicotte L, Sassine M-P, Seal RF, Roy A. A comparison of intrathecal morphine/fentanyl and patient-controlled analgesia with patient-controlled analgesia alone for analgesia after liver resection. Pain Med. 2006;103:990–994. doi:10.1213/01.ane.0000238040.41872.7e
34. Dichtwald S, Ben-Haim M, Papismedov L, Hazan S, Cattan A, Matot I. Intrathecal morphine versus intravenous opioid administration to impact postoperative analgesia in hepato-pancreatic surgery: a randomized controlled trial. J Anesth. 2017;31(2):237–245. doi:10.1007/s00540-016-2286-y
35. Kjolhede P, Bergdahl O, Borendal Wodlin N, Nilsson L. Effect of intrathecal morphine and epidural analgesia on postoperative recovery after abdominal surgery for gynecologic malignancy: an open-label randomized trial. BMJ Open. 2019;9:e024484. doi:10.1136/bmjopen-2018-024484
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.