Back to Journals » Patient Preference and Adherence » Volume 20
Effect of Laparoscopic Sleeve Gastrectomy on Female Sexual Function Index (FSFI) and Menstrual Function
Authors Mutlu V ![]() , Barutcu B
, Barutcu B ![]() , Şahin S, Yıldız Ç, Tutcu RE
, Şahin S, Yıldız Ç, Tutcu RE ![]() , Dikmen C, Özdemir AZ
, Dikmen C, Özdemir AZ ![]() , Özbalcı GS, Yılmaz K
, Özbalcı GS, Yılmaz K
Received 11 September 2025
Accepted for publication 22 January 2026
Published 11 February 2026 Volume 2026:20 566811
DOI https://doi.org/10.2147/PPA.S566811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Vahit Mutlu,1 Burak Barutcu,2 Samet Şahin,2 Çağlanur Yıldız,3 Rabia Ebrar Tutcu,2 Ceyhan Dikmen,2 Ayşe Zehra Özdemir,2 Gökhan Selçuk Özbalcı,4 Kadir Yılmaz5
1Department of General Surgery, Uskudar University, İstanbul, Türkiye; 2Department of Obstetrics and Gynecology, Samsun Ondokuz Mayıs University, Samsun, Türkiye; 3Department of Obstetrics and Gynecology, Adıyaman Gölbaşı Government Hospital, Adıyaman, Türkiye; 4Department of General Surgery, Samsun Ondokuz Mayıs University, Samsun, Türkiye; 5Department of Statistics, Istanbul Commerce University, İstanbul, Türkiye
Correspondence: Vahit Mutlu, Uskudar University Department of General Surgery, Yamanevler, Site Yolu Cd No: 27, İstanbul, 34768, Türkiye, Tel +90 530 211 44 32, Email [email protected]
Objective: This study aimed to investigate the effects of Laparoscopic Sleeve Gastrectomy (LSG) surgery on Female Sexual Function Index (FSFI) and menstrual functions.
Methods: A total of 494 sexually active women attempting OMU Faculty of Medicine and diagnosed with obesity and underwent with laparoscopic sleeve gastrectomy before and after the surgery between 17.02.2015 and 10.03.2025 were included in the study.
Results: FSFI before operation was significantly and negatively correlated with age (r=− 0.443; p< 0.01) and Visual Analog Scale (VAS) (r=− 0.675; p< 0.01). FSFI after operation was significantly and negatively correlated with age (r=− 0.383; p< 0.01), menstrual cycle (r=− 0.202; p< 0.05) and VAS (r=− 0.661; p< 0.01). FSFI before and after operation were not significantly correlated with BMI and comorbidity (p> 0.05). Age (OR=− 0.083; p< 0.01) and VAS (OR=− 0.410; p< 0.01) had significant and negative effect on FSFI before operation. Similarly, age (OR=− 0.092; p< 0.01) and VAS (OR=− 0.439; p< 0.01) had significant and negative effect on FSFI after operation.
Conclusion: Menstrual cycle change after LSG also had a decreasing effect on FSFI level after obesity. Therefore, treatment support can be given to women in terms of menstrual cycle in order to increase their sexual quality of life after LSG. Multidisciplinary studies of bariatric surgeon and gynecologist are needed in this regard.
Keywords: laparoscopic sleeve gastrectomy, sexual function, obesity, female sexual function
Introduction
With its increasing prevalence and incidence,1,2 obesity negatively affects the quality of life3 and the motor and cognitive functions4 of individuals in their daily lives. Sexuality, which is an important part of individuals’ daily lives and quality of life, is also one of the functions negatively affected by obesity.5,6 Especially in women, obesity negatively affects sexuality cognitively through body image7,8 and physically due to excess weight.9,10 There are many treatment options in obesity treatment, from lifestyle and nutrition changes to medical treatment, from surgical methods to laparoscopic methods.11 Among surgical methods, Laparoscopic Gastric Sleeve (LSG) is one of the most common bariatric surgery methods in the fight against obesity.12
While the number of studies on sexuality after bariatric surgery has increased in recent years, it is generally reported in these studies that individuals have higher sexual satisfaction after optimal clinical response.13–15 In their study, Steffen et al13 reported that nearly half of the women and men who were dissatisfied with their sexual lives before bariatric surgery had significantly increased sexual life satisfaction after a five-year follow-up. In another study, Paul et al14 reported that patients experienced a significant increase in their sexual lives after laparoscopic Roux-en-Y bypass. Luyssen et al15 reported that the quality of sexual life of individuals increased after bariatric surgery, but there were no significant differences in menstrual characteristics and sexual behaviors. In their study, Loh et al16 reported that bariatric surgery, especially in women under the age of 40, both increased the quality of sexual life and reduced female sexual dysfunction. Wingfield et al17 reported in their comprehensive meta-analysis of 32 articles that there was an improvement in sexual function in both genders after bariatric surgery. Although there are many scales that measure sexual function, the FSFI is one of the most studied scales in this area, with proven validity and reliability, and a high level of validation. The effects of bariatric surgery on sexual quality have been examined for both genders; there were no sufficient studies on the change in FSFI in women after LSG compared to before. Therefore, the aim of this study was to examine the effect of Laparoscopic Sleeve Gastrectomy (LSG) surgery on women’s Sexual Function Index (FSFI) and menstrual functions.
Methods
Research Model
The study was designed as longitudinal and retrospective. The differences between the FSFI scores of women who volunteered to participate in the study before and after LSG and the relationships between them and their demographic characteristics were examined. The study was designed as a mixed model, with descriptive screening and relational screening.
Patients
A total of 494 sexually active women attempting OMU Faculty of Medicine and diagnosed with obesity and underwent with laparoscopic sleeve gastrectomy before and after the surgery between 17.02.2015 and 10.03.2025 were included in the study.
Sexually active women who were diagnosed with obesity at OMU Faculty of Medicine and underwent laparoscopic sleeve gastrectomy before and after the surgery between 17.02.2015 and 10.03.2025 were included in the study. The inclusion criteria for the study were as follows:
- Being 18 years of age or older,
- Having had LSG,
- Having FSFI data before and after LSG in the patient file,
- Not having a health condition that would prevent FSFI.
The exclusion criteria for the study were:
- Being under 18 years of age,
- Having incomplete data on FSFI in the file,
- Having a chronic disease that may interfere with sexual functions.
It is known that T2DM negatively affects sexual function. Changes in sexual function may be less noticeable in patients with T2DM, and this may reduce the power of the findings. For thi reason, T2DM and other comorbidity which may effect FSFI were used in analysis as cofounders. After one month, FSFI levels were measured. Time intervals between patients were consistent in order to reduce time effect on research results, because variation in follow-up time could significantly influence FSFI and menstrual cycle outcomes.
Research Data
The Female Sexual Function Index (FSFI) was used to determine the preoperative and postoperative sexual functions of the patients. FSFI is a scale that examines sexual function in women in 19 items and six dimensions. These dimensions are Sexual desire, Sexual arousal, Sexual lubrication, Sexual orgasm, Sexual satisfaction and Sexual pain. Rosen et al18 developed the scale and its Turkish validity was made by Aygin and Aslan.19 The Cronbach Alpha reliability coefficient, which shows the internal consistency coefficient of the scale, was reported as 0.95. In addition to the FSFI scores of the patients, age, Body Mass Index (BMI), Hypertension (HT), Diabetes Mellitus (DM), Visual Analog Scale (VAS), menstrual cycle change and day parameters were obtained.
Ethical Approval
An ethical approval was taken from Ondokuz Mayis University Clinical Research Ethics Committee with B.30.2.ODM.0.0.08/273 grand number. Written patient consent was taken from all participants. Participants were fully informed about the purpose of the study. The research was conducted in accordance with Helsinki Declaration.
Statistical Methods
Frequency analysis was used for description of nominal and ordinal parameters, whereas mean, standard deviation, median and ranges were used for description of scale parameters. Kolmogorov Smirnov test was used for normality of scale parameters. Wilcoxon Signed Rank test was used for differences before and after FSFI scores and dimensions. Spearman’s rho correlation analysis was used for correlations between parameters. Generalized Linear Model (Logit) was used for regression, due to linearization deviations.20,21 SPSS 25.0 for windows was used for analysis at 0.05 significance level and 95% Confidence interval.
Results
In total, 494 sexually active patients included in the final analysis after the inclusion and exclusion criteria. Age mean of patients were 33.13±6.78 with 19–45 age range. BMI of patients were ranged from 31.90 to 68.10 with 42.40±5.46 mean. 5.7% of patients had HT, 11.3% had DM, 4.0% had asthma, and 2.4% had anxiety. Menstrual cycle changes of 66.8% of patients were not known, whereas 17.8% were stated change in menstrual cycle after operation (Table 1).
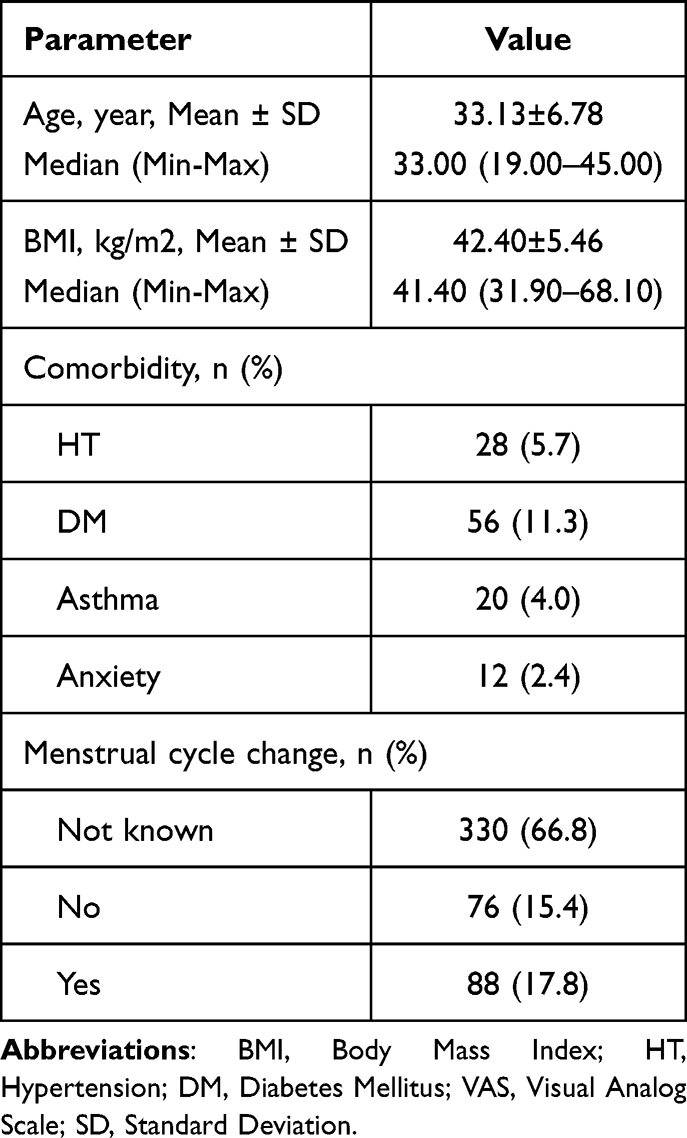 |
Table 1 Baseline Characteristics of Patients |
Sexual desire, arousal, lubrication, orgasm, satisfaction, pain and total FSFI scores were significantly higher in patients after operation (p<0.05). Menstrual cycle and VAS scores of patients were significantly higher before operation (p<0.05) (Table 2).
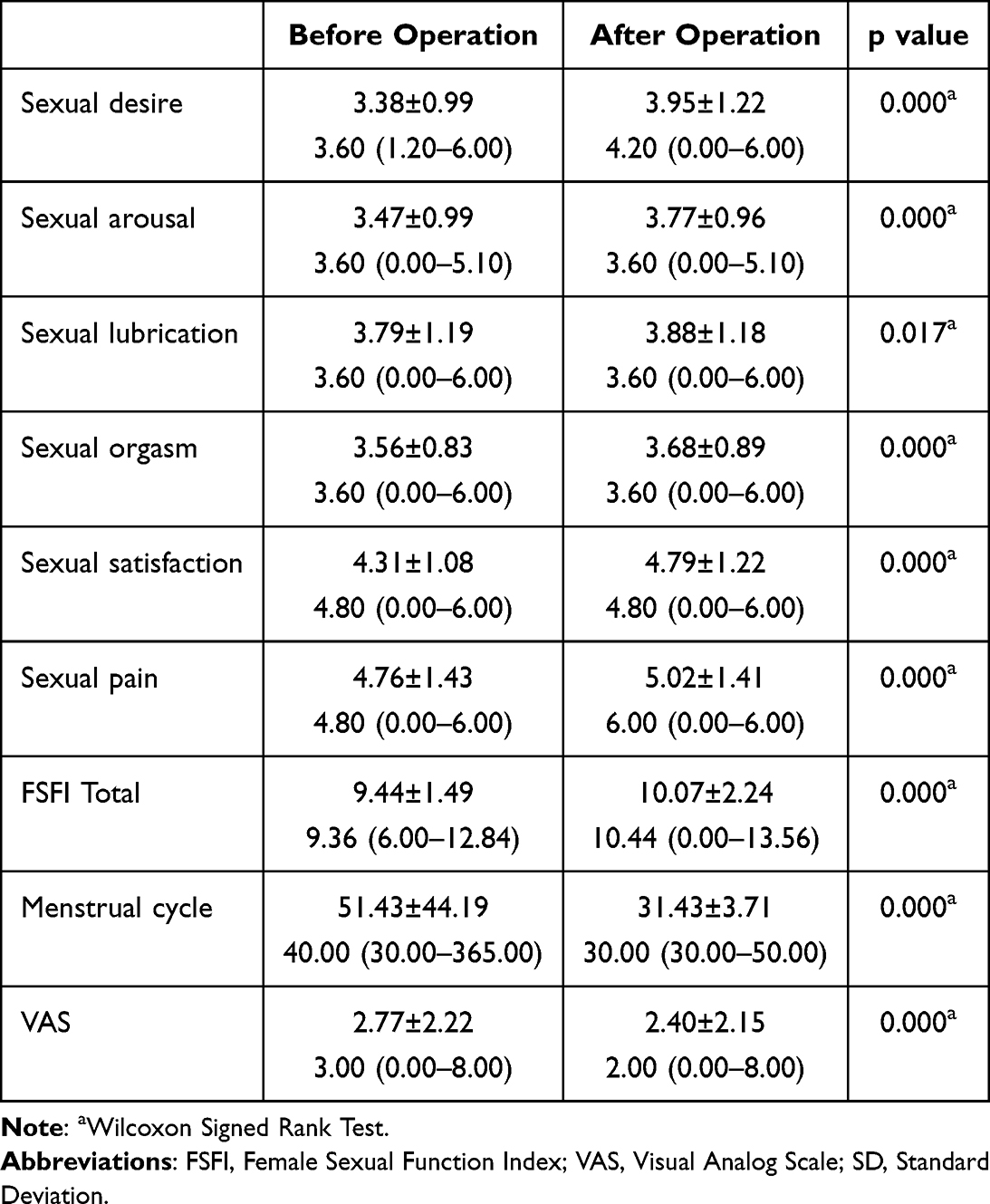 |
Table 2 FSFI Dimension Scores and Differences Before and After Operation |
Spearman’s rho correlation analysis results showed that FSFI before operation was significantly and negatively correlated with age (r=−0.443; p<0.01) and VAS (r=−0.675; p<0.01). FSFI after operation was significantly and negatively correlated with age (r=−0.383; p<0.01), menstrual cycle (r=−0.202; p<0.05) and VAS (r=−0.661; p<0.01). FSFI before and after operation were not significantly correlated with BMI and comorbidity (p>0.05) (Table 3).
 |
Table 3 Spearman’s Rho Correlation Analysis Between Total FSFI and Baseline Characteristics of Patients Before and After Operation |
Generalized Linear Model (Logit) results showed that age (OR=−0.083; p<0.01) and VAS (OR=−0.410; p<0.01) had significant and negative effect on FSFI before operation. Similarly, age (OR=−0.092; p<0.01) and VAS (OR=−0.439; p<0.01) had significant and negative effect on FSFI after operation. Effect of VAS was higher than effect of age in both before and after operation. Menstrual cycle effect was the lowest among other parameters after operation (Table 4).
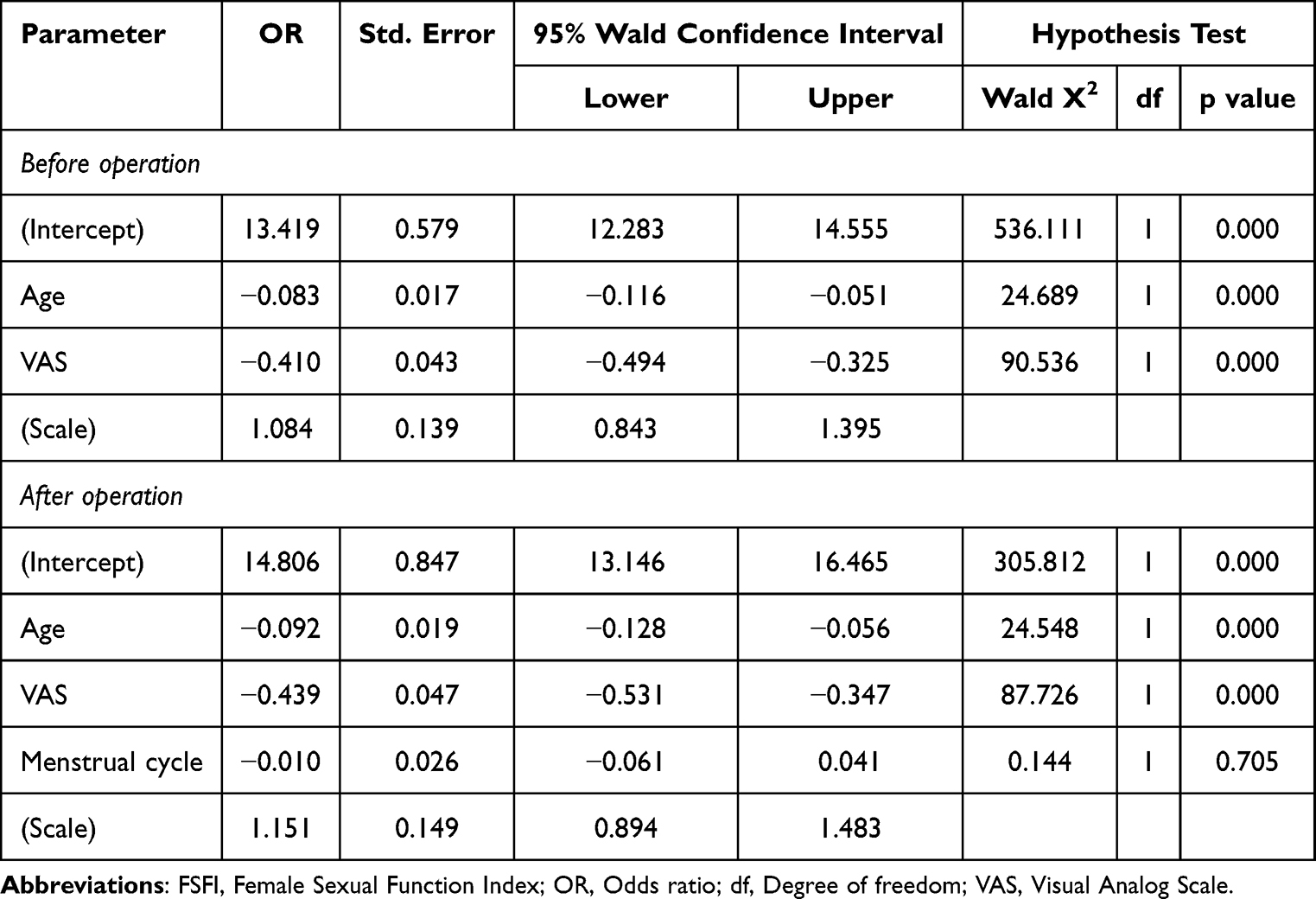 |
Table 4 Generalized Linear Model (Logit) on Effects of Significantly Correlated Factors on FSFI Before and After Operation |
Correlation between VAS and FSFI was significant for both before and after operation and its direction was negative. Before operation, correlation coefficient was higher showing more strong correlation (Figure 1).
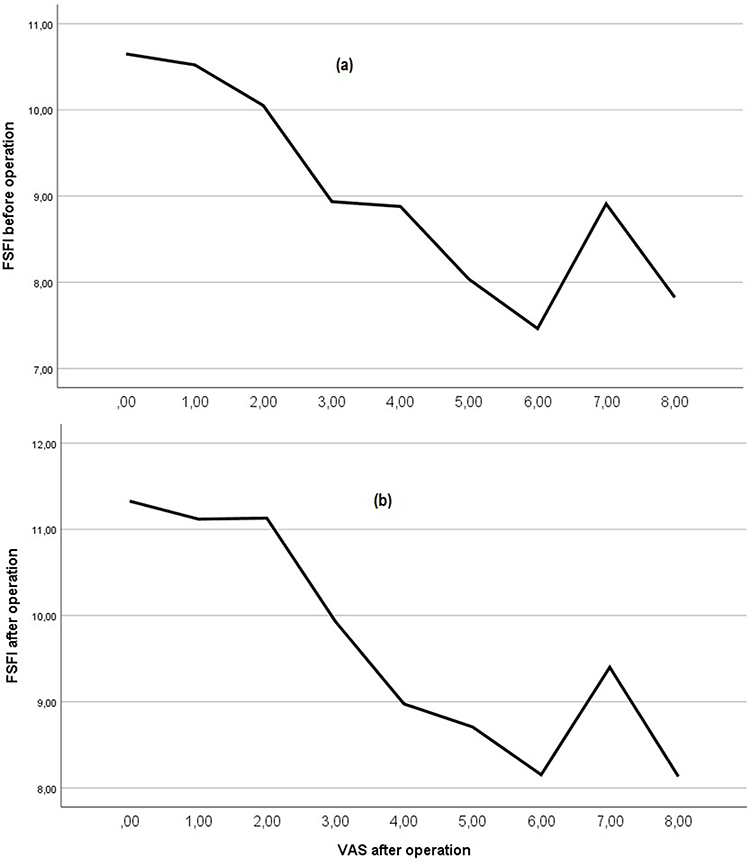 |
Figure 1 Correlation between FSFI and VAS before (a) and after (b) operation. |
Correlation between age and FSFI was significant for both before and after operation and its direction was negative. Before operation, correlation coefficient was higher showing more strong correlation (Figure 2).
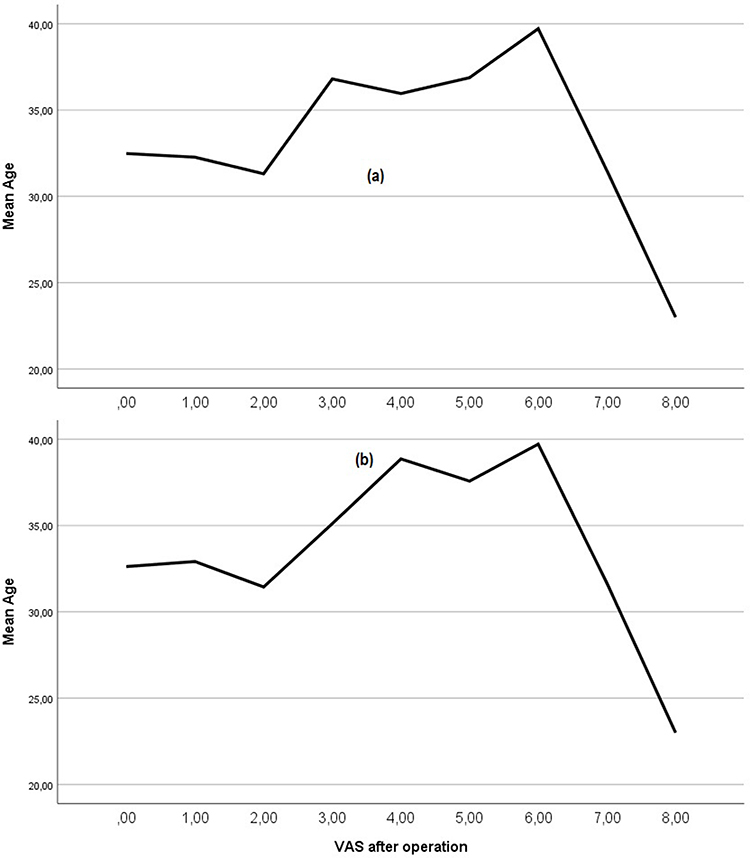 |
Figure 2 Correlation between VAS and age before (a) and after (b) operation. |
Discussion
This study aimed to investigate the effects of Laparoscopic Sleeve Gastrectomy (LSG) surgery on women’s Sexual Function Index (FSFI) and menstrual functions, and within this framework, 494 women who applied to our clinic in the last ten years were included in the study. According to the results obtained, there was a statistically significant increase in the FSFI total score and all dimensions after LSG, while there was a significant decrease in menstrual cycle and VAS levels.
Sexual life is an important part of individuals’ daily lives and is particularly related to body image in women.7,8 Obesity is an important health problem that negatively affects both body image and physical sexual life in women.9,10 The general result of studies on obesity is that obesity reduces the quality of sexual life in both genders. However, a significant increase in the quality of sexual life is observed after bariatric surgery.14–17 In our study, the FSFI total score and all sub-dimension scores, as an indicator of the quality of sexual life in women, increased statistically significantly after LSG. In this respect, our study is in line with the studies in the literature.
Studies on sexual life after LSG have reported similar results to studies on bariatric surgery and obesity and sexual life.22–25 Akan et al22 applied a survey to 53 female patients and reported a significant increase in FSFI levels after LSG. Şimşek et al23 reported in their study on 55 women that LSG can be effective in both increasing FSFI levels and reducing sexual dysfunction in women. Korany24 reported in his study that patients’ self-confidence increased after LSG and that this positively affected sexual life. In another study, Dilimulati et al25 reported that testosterone and hormones that can affect sexuality were more regular after LGS. de Almeida Menezes et al26 evaluated sexual quality of female after gastric bypass, and reported that gastric bypass increases sexuality of women. Abouelgreed et al27 argued that gastric sleeve increases sexual function in long term. Szoka et al28 reported that bariatric surgery demography is closely related with sexual quality and properties of patients. These and similar studies reveal that individuals can have a higher quality sexual life after LSG. Our study obtained results that are compatible with the literature in terms of both menstrual cycle and associating this with LSG.
Although age had an effect both before and after the operation, pain was the most important factor at both measurement times. Pain and the effect of age increased after the operation compared to before. Therefore, we believe that patients are more sensitive after surgery. The significant effect related to sexuality was quantitatively demonstrated in our study. However, whether this effect stems from weight loss or the surgical procedure is a matter that requires further investigation. In this regard, further research could focus on the variables of surgical and weight loss effects. It is known that LSG decreases blood ghrelin levels and increases GLP-1 levels which may affect FSFI and sexual desire of patients. However, their direct and indirect relationships are in a complex structure, and must be examined in future research. The FSFI total score normally ranges from 2 to 36, but the we found totals around 9–12. We believe that before operation, having obesity and after operation, having an operation may cause this difference.
Limitations of the Study
The most important limitation of the study is that the number of patients who were not followed up is high, since it is based on a 10-year follow-up. Since patients can receive health services in both private and public sectors and because of the density in public hospitals, there may be interruptions in patient follow-up. Although we examined every case that applied to our hospital in the last 10 years, the real LSG prevalence and incidence are different from these due to the loss of follow-up.
Another important limitation of the study is the limited number of multidisciplinary studies focusing on the relationship between menstrual cycle, sexual life and obesity. In this respect, studies that will compare the results of the study are limited. This is another important limitation of the study. Since our study focused on the survey, we were unable to plan a research that also considered estrogen and progesterone hormones. However, in clinical trials, these parameters could be added to better reveal clinical and laboratory effects. Many factors such as nutrition, sleep patterns, daily workload, and stress affect sexual function, and these factors may be interpreted as cofounders. Since our study was designed on online survey methods, these are important limitations. Two-thirds of the sample has “menstrual cycle not known”, which severely weakens any conclusion regarding menstrual function.
Contributions of the Research to Literature and Clinical Practice
The most important contribution of the study to the literature is that, unlike similar studies examining the relationship between LSG and sexual life, it examined the FSFI level with a multidimensional advanced analysis and associated it with the menstrual cycle. In this respect, the study can be a basic source for further studies. In addition, the examination of 10-year application records in the study makes the study important in terms of longitudinal sampling.
The contribution of the study to clinical practice is that it reveals the effect of menstrual cycle on FSFI after bariatric surgery in women. In this way, both the surgeon and the gynecologist can focus more on menstrual cycle regulation in patient follow-up to prevent possible sexual function and quality losses after LSG.
Conclusion
Although there were functions that significantly decreased VAS FSFI level with age before and after LSG, menstrual cycle change after LSG also had a decreasing effect on FSFI level after obesity. Therefore, treatment support can be given to women in terms of menstrual cycle in order to increase their sexual quality of life after LSG. Multidisciplinary studies of bariatric surgeon and gynecologist are needed in this regard.
In addition to the research limitations and being single-centered, multicenter and larger sample size studies are needed to reduce the effects experienced in data tracking. In addition, multivariate and advanced analyses of the factors that may affect menstrual cycle changes after LSG may contribute positively to the field. Obesity surgery primarily helps individuals achieve a healthier appearance, which in turn is linked to many psychological processes, particularly sexuality. Therefore, in addition to the direct benefits of obesity surgery, further research into its indirect effects, especially on sexuality and psychological processes, would be beneficial.
Data Sharing Statement
Data are restricted from ethical approval, and may be asked from corresponding author.
Ethics Approval
An ethical approval was taken from Ondokuz Mayis University Clinical Research Ethics Committee with with B.30.2.ODM.0.0.08/273 grand number. Written patient consent was taken from all participants. Participants were fully informed about the purpose of the study. The research was conducted in accordance with Helsinki Declaration.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reilly JJ, El-Hamdouchi A, Diouf A, Monyeki A, Somda SA. Determining the worldwide prevalence of obesity. Lancet. 2018;391(10132):1773–9. doi:10.1016/S0140-6736(18)30794-3
2. Haththotuwa RN, Wijeyaratne CN, Senarath U. Worldwide epidemic of obesity. In: Obesity and Obstetrics. Elsevier; 2020:3–8.
3. Taylor VH, Forhan M, Vigod SN, McIntyre RS, Morrison KM. The impact of obesity on quality of life. Best Pract Res Clin Endocrinol Metab. 2013;27(2):139–146. doi:10.1016/j.beem.2013.04.004
4. Wang C, Chan JS, Ren L, Yan JH. Obesity reduces cognitive and motor functions across the lifespan. Neural Plast. 2016;2016(1):2473081. doi:10.1155/2016/2473081
5. Larsen SH, Wagner G, Heitmann BL. Sexual function and obesity. Int J Obesity. 2007;31(8):1189–1198. doi:10.1038/sj.ijo.0803604
6. Kolotkin RL, Zunker C, Østbye T. Sexual functioning and obesity: a review. Obesity. 2012;20(12):2325–2333. doi:10.1038/oby.2012.104
7. Taskin Yilmaz F, Karakoç Kumsar A, Demirel G. The effect of body image on sexual quality of life in obese married women. Health Care Women Int. 2019;40(4):479–492. doi:10.1080/07399332.2018.1542432
8. McNabney SM. Obesity, body image dissatisfaction, and sexual dysfunction: a narrative review. Sexes. 2022;3(1):20–39. doi:10.3390/sexes3010002
9. Shah MB. Obesity and sexuality in women. Obstet Gynecol Clin. 2009;36(2):347–360. doi:10.1016/j.ogc.2009.04.004
10. Jarząbek-Bielecka G, Wilczak M, Potasińska-Sobkowska A, et al. Overweight, obesity and female sexuality in perimenopause: a preliminary report. Menopause Review/Przeglad Menopauzalny. 2015;14(2):97–104.
11. Bult MJ, van Dalen T, Muller AF. Surgical treatment of obesity. European J Endocrinol. 2008;158(2):135–145. doi:10.1530/EJE-07-0145
12. Shi X, Karmali S, Sharma AM, Birch DW. A review of laparoscopic sleeve gastrectomy for morbid obesity. Obesity Surg. 2010;20(8):1171–1177. doi:10.1007/s11695-010-0145-8
13. Steffen KJ, King WC, White GE, et al. Changes in sexual functioning in women and men in the 5 years after bariatric surgery. JAMA Surg. 2019;154(6):487–498. doi:10.1001/jamasurg.2018.1162
14. Paul R, Andersson E, Wirén M, Frisk J. Health-related quality of life, sexuality and hormone status after laparoscopic Roux-En-Y gastric bypass in women. Obesity Surg. 2020;30(2):493–500. doi:10.1007/s11695-019-04197-5
15. Luyssen J, Jans G, Bogaerts A, et al. Contraception, menstruation, and sexuality after bariatric surgery: a prospective cohort study. Obesity Surg. 2018;28(5):1385–1393. doi:10.1007/s11695-017-3033-7
16. Loh HH, Shahar MA, Loh HS, Yee A. Female sexual dysfunction after bariatric surgery in women with obesity: a systematic review and meta-analysis. Scand J Surg. 2022;111(1):14574969211072395. doi:10.1177/14574969211072395
17. Wingfield LR, Kulendran M, Laws G, Chahal H, Scholtz S, Purkayastha S. Change in sexual dysfunction following bariatric surgery. Obesity Surg. 2016;26(2):387–394. doi:10.1007/s11695-015-1937-7
18. Rosen R, Brown C, Heiman J, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
19. Aygin D, Aslan FE. Kadın Cinsel İşlev Ölçeği’nin Türkçeye Uyarlaması. Turkiye Klinikleri J Med Sci. 2005;25(3):393–399.
20. Yılmaz K, Turanlı M. A multi-disciplinary investigation of linearization deviations in different regression models. Asian J Prob Statistics. 2023;22(3):15–19. doi:10.9734/ajpas/2023/v22i3484
21. Yilmaz K, Turanlı M. A multi-disciplinary investigation on minimizing linearization deviations in different regression models. Change & shaping the future, IV. ASC-2022/Fall Congress ISBN 978-625-8048-99-5.
22. Akan S, Uruc F, Aydin MT, Verit A. The effect of sleeve gastrectomy technique on women’s sexual function: a prospective study. Revista Internacional de Andrologia. 2018;16(4):167–173. doi:10.1016/j.androl.2017.12.003
23. Şimşek HU, Varol EN, Güler SA, Şimşek T, Şahin E, Cantürk NZ. Menstrual and sexual functions in female patients after sleeve gastrectomy due to obesity: obesity and sexual function. Arch Gynecol Obstetrics. 2025;1–7.
24. Korany BM. Lived experience of patients following robotic sleeve surgery. Assiut Scientific Nurs J. 2023;11(38):240–249.
25. Dilimulati D, Cai M, Lin Z, et al. Correlation between sex hormones and non-alcoholic fatty liver disease before and after laparoscopic sleeve gastrectomy. Obesity Surg. 2021;31(11):4901–4910. doi:10.1007/s11695-021-05663-9
26. de Almeida Menezes M, Herbella FAM, de Godoy Dos Santos G, Valezi AC. Influence of gastric bypass on obese women sexual function—a prospective study. Obesity Surg. 2021;31(8):3793–3798. doi:10.1007/s11695-021-05509-4
27. Abouelgreed TA, Elatreisy A, El-Sherbeiny AF, et al. Long-term effect of sleeve gastrectomy surgery on Hormonal Profile, Semen parameters and sexual functions of obese infertile men; a prospective observational study. Basic Clin Androl. 2023;33(1):16. doi:10.1186/s12610-023-00191-1
28. Szoka N, Szoka S, Friedman K, Portenier D. Sexual and gender minority bariatric patients: an unseen population. Bariatric Surg Pract Patient Care. 2021;16(1):30–35. doi:10.1089/bari.2020.0049
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Weight Loss Outcome of Laparoscopic Sleeve Gastrectomy Predicted by the Percentage of Excess Weight Loss at 6 Months in Chinese Patients with Body Mass Index ≥ 32.5 Kg/m2
Wang L, Tian C, Xu G, Sang Q, Chen G, Yu C, Wuyun Q, Wang Z, Chen W, Amin B, Wang D, Lian D, Zhang N
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2235-2247
Published Date: 29 July 2022
Serum Fibrinogen-Like Protein 1 Levels in Obese Patients Before and After Laparoscopic Sleeve Gastrectomy: A Six-Month Longitudinal Study
Dilimulati D, Du L, Huang X, Jayachandran M, Cai M, Zhang Y, Zhou D, Zhu J, Su L, Zhang M, Qu S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2511-2520
Published Date: 17 August 2022
Predictive Factors of Menstrual Recovery After Laparoscopic Sleeve Gastrectomy in Polycystic Ovary Syndrome Women with Obesity
Cai M, Zhang Y, Gao J, Dilimulati D, Bu L, Cheng X, Du L, Zhou D, Zhu J, Qu S, Zhang M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1755-1766
Published Date: 13 June 2023
Establishing a Prediction Model for Weight Loss Outcomes After LSG in Chinese Obese Patients with BMI ≥ 32.5 Kg/m2 Using Body Composition Data
Wang L, Sun Y, Sang Q, Wang Z, Yu C, Li Z, Shang M, Zhang N, Du D
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1467-1487
Published Date: 7 May 2025
Hyperuricemia Remission After Sleeve Gastrectomy in Chinese Patients and Establishment of a Preoperative Predictive Model: A Retrospective Cohort Study with a Mean Follow-Up of 20 Months
Chen X, Li Z, Wang Z, Sun Y, Shang M, Tian C, Liao Z, Lian D, Amin B, Du D, Xu G, Zhang N, Wang L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2825-2836
Published Date: 12 August 2025