Back to Journals » Drug Design, Development and Therapy » Volume 20
Effect of Intraoperative Low-Dose Lidocaine Administration on the Consumption of Mivacurium During Gynecological Laparoscopic Surgery: A Prospective Clinical Study
Authors Fu JP, Zhou YH, Li SX ![]() , Yang YJ, Wang Q, Lei W, Shen JJ, Chen YL, Xu LL
, Yang YJ, Wang Q, Lei W, Shen JJ, Chen YL, Xu LL
Received 1 February 2026
Accepted for publication 25 May 2026
Published 3 June 2026 Volume 2026:20 600261
DOI https://doi.org/10.2147/DDDT.S600261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Jin-Peng Fu,1,2 Yan-Hong Zhou,2 Shu-Xi Li,2 Ying-Jie Yang,2 Qian Wang,2,3 Wan Lei,2,4 Jian-Jun Shen,5 Yuan-Liang Chen,1 Li-Li Xu2
1Department of Anesthesia, Jinhua Municipal Central Hospital, Jinhua, Zhejiang, People’s Republic of China; 2Department of Anesthesia, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Anesthesia, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Anesthesia, Hangzhou Linping District Maternal & Child Health Care Hospital, Hangzhou, Zhejiang, People’s Republic of China; 5Department of Anesthesia, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Li-Li Xu, Department of Anesthesia, Women’s Hospital, Zhejiang University School of Medicine, No. 1 Xueshi Road, Hangzhou, Zhejiang, 310006, People’s Republic of China, Tel +86 571 87061007, Email [email protected] Yuan-Liang Chen, Department of Anesthesia, Jinhua municipal central hospital, 365 Renming Dong Road, Jinhua, Zhejiang, 321000, People’s Republic of China, Tel +86 13819998824, Email [email protected]
Background: Recent literatures have shown that lidocaine obviously shortened the onset time and reduced the maintenance dose of vecuronium. However, there have been no reports on the use of mivacurium. This study aimed to investigate the effects of lidocaine on the requirement and onset time of mivacurium administration during gynecological laparoscopic surgery.
Methods: 66 patients scheduled for elective gynecological laparoscopic surgery were randomly assigned to receive an intravenous bolus of 1.5 mg·kg− 1 lidocaine followed by a continuous infusion of 2 mg·kg− 1·h− 1 or an equivalent volume of placebo. Neuromuscular block was induced with 0.2 mg·kg− 1 followed by an infusion of 0.2 mg·kg− 1·h− 1 mivacurium. The primary outcome was the onset time of mivacurium. Consumption of mivacurium, extubation time, and postoperative numeric rating scale (NRS) score for pain were recorded.
Results: The onset time of mivacurium was significantly shorter in the lidocaine group than in the control group (mean difference − 25.0 s, 95% CI − 47.8 to − 2.3, P=0.032). Hourly consumption of mivacurium was lower in the lidocaine group than in the control group (median difference, − 0.04 mg·kg− 1·h− 1; 95% CI, − 0.08 to − 0.01; P=0.017). The extubation time was also significantly shorter in the lidocaine group than in the control group (P=0.006). The NRS pain score at 6 h and 12 h after surgery was lower in the lidocaine group than in the control group.
Conclusion: Intravenously administered lidocaine significantly decreased the requirement of mivacurium, shortened the onset time, accelerated the extubation time, and alleviated pain intensity at 6 h and 12 h after surgery, without increasing adverse events in patients with a low risk of airway difficulty undergoing gynecological laparoscopic surgery. Given the small sample size from a single centre, our result requires further verification.
Keywords: lidocaine, mivacurium, muscle relaxation, neuromuscular block, neuromuscular monitoring, tracheal intubating conditions, gynecological laparoscopic surgery
A Letter to the Editor has been published for this article.
Introduction
With the development of minimally invasive technology, laparoscopic gynecological surgery has become one of the most universal procedures for the common benign gynecological diseases such as ovarian cysts and uterine fibroids in women globally.1 Neuromuscular blocking agents (NMBAs) are essential anesthetic agents during the perioperative period of laparoscopic surgery, which can not only meet the needs of tracheal intubation, but also create good surgical space conditions and shorten the patient’s operation time.2 Several previous studies have stated that deep neuromuscular blockade enhanced surgical space conditions during laparoscopy and reduced the pain scores in the post-anesthesia care unit.2–5 However, if NMBAs (such as vecuronium and mivacurium) are overused, it may result in residual neuromuscular blockade (total muscle relaxation index (TOF)) less than 0.9), which has been proven to be a risk factor for severe postoperative respiratory complications and an increase in patient morbidity, even after clinical use of sugammadex and tracheal extubation reversal, with a risk as high as 9.4%.6–8 Although mivacurium is a commonly used short-acting non-depolarizing muscle relaxant, rapid injection, repeated dosing, or prolonged continuous infusion during surgery, especially for patients with low plasma cholinesterase activity, may still lead to excessive muscle relaxation, prolong the postoperative respiratory depression period, increase the risk of pulmonary complications, and also trigger histamine release, thereby causing skin or cardiovascular symptoms.9,10 A recent systematic review and meta-analysis reported that several pharmacological adjuncts, such as magnesium, dexmedetomidine, and clonidine, but not nicardipine, diltiazem, or dexamethasone, may reduce the intraoperative consumption of NMBAs.11 Nonetheless, whether the putative effects are conducive or harmful remains unclear. Therefore, it is necessary to find more effective strategies to reduce NMBA dosage and minimize the occurrence of residual muscle relaxation blockage and related respiratory complications.
Lidocaine, an amide local anesthetic with a molecular structure of C14H22N2O, is metabolized mainly by oxidative N-dealkylation. When administered intravenously, it binds to the reactant alpha-1-glycoprotein to produce analgesic, antihyperalgesic, and antinociceptive effects, primarily by blocking voltage-gated sodium channels.12 Previous studies illuminated that perioperative intravenous administration of lidocaine not only alleviated the stress response and postoperative pain, and reduced the total consumption of opioids and propofol, but also promoted the recovery of gastrointestinal function, and shortened the recovery time and the length of hospital stay.13–15 Interestingly, Munakata et al16 expounded that vecuronium-induced neuromuscular blockade in patients with continuous lower thoracic epidural lidocaine infusion at a rate of 2–3 mg·kg−1·h−1 following a bolus of 1.5–2 mg·kg−1 significantly prolonged the mean clinical duration from administration of the first dose to T1 recovery to 5% of baseline and decreased the maintenance dose of vecuronium, but did not influence the maximum depression of T1 response and onset time obtained by 0.1 mg·kg−1 vecuronium. Importantly, they also claimed that 2% lidocaine 1.5 mg·kg−1 administered 3 min before tracheal intubation shortened the onset time of vecuronium-induced neuromuscular block, but did not alleviate the hemodynamic changes resulted from the tracheal intubation.17
In addition, when anesthesia was induced with 30 mg lidocaine in laparoscopic pelvic surgery (LPS), muscle relaxants were not required during total intravenous anesthesia using propofol and remifentanil.18 However, the potential impact of lidocaine on the onset time, the mean clinical duration, and the maintenance requirements of mivacurium has not yet been elucidated. Therefore, we hypothesized that intraoperative intravenous administration of lidocaine could enhance neuromuscular blockade induced by mivacurium and reduce its total dosage during gynecological laparoscopic surgery. This study was designed to explore the effect of intravenously administered lidocaine on the requirement and onset time of mivacurium administration in patients scheduled for elective gynecological laparoscopic surgery.
Methods
Study Design and Subjects
The Research Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province approved our prospective study protocol on May 5, 2024 (No. IRB-20240144-R), which was then registered in the Chinese Clinical Trial Registry (https://www.chictr.org.cn; Identifier: ChiCTR2400084256) on May 13, 2024. Our research group launched the trial in Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang province, and the patients were enrolled from May 14, 2024, to June 30, 2024. Written informed consent was obtained from all participants. Our study adhered to the Consolidated Standards of Reporting Trials (CONSORT) 2025 statement,19 and was compliant with the TITAN Guidelines 2025-governing declaration and the administration of AI (https://doi.org/10.70389/PJS.100082).20 This study was also conducted in strict accordance with the principles of the Declaration of Helsinki.21
Female patients aged between 18 and 65 years old, with American Society of Anesthesiologists (ASA) classification levels of I–II, and who planned to undergo gynecological laparoscopic surgery under general anesthesia were recruited. We excluded the following patients: those with a body mass index (BMI) greater than 25; those with a history of central nervous system, mental disorders or neuromuscular diseases; those who had used sedatives; those who were expected to have difficulty with mask ventilation; those who are expected to have difficulty with intubation (Mallampati classification as III and IV grades, with a thyromental distance less than 6.5 centimeters and an oral opening less than 3.5 centimeters); those with a history of hypertension, diabetes, heart disease, chronic lung disease, asthma or obstructive sleep apnea syndrome (OSAS); those with abnormal lung or liver function; those allergic to mivacurium chloride or lidocaine; those with acute upper respiratory tract infection; or those who refused to participate in this study.22
Randomization and Blinding
The trial coordinator (FPJ) generated random numbers using IBM SPSS 25.0 (IBM SPSS, Armonk, NY, USA) and then stored the results in the sequentially numbered opaque envelopes. Prior to induction of anesthesia, the professional pharmacist (NJW) opened the randomized envelopes, prepared the research drugs based on the patient groups, and ensured that all the drugs had the same appearance (either lidocaine or placebo). Neither the trial coordinator (FPJ) nor the pharmacist (NJW) participated in the perioperative anesthesia management and care, as well as the postoperative follow-up work. The patients, responsible anesthesiologists (ZHY and LXS), other members of the medical team, and investigators involved in the recruitment of patients, the collection of data, as well as the subsequent follow-up and evaluation work were blinded to the patient groups.
Monitoring, Anesthesia Management, and Intervention
All the patients underwent conventional fasting and did not receive any premedication. An intravenous route was constructed after entering the operating room, and electrocardiography (ECG), noninvasive blood pressure (NIBP), and pulse oxygen saturation (SpO2) were used for continuous monitoring. All the recruited patients were randomly allocated to have either an intravenous bolus of 1.5 mg·kg−1 lidocaine23 before anesthesia induction, following a continuous infusion of 2 mg·kg−1·h−124 for 30 min, or an equivalent volume of placebo.
Anesthesia was induced by intravenous injection of midazolam 0.1 mg⋅kg−1, sufentanil 0.5 μg·kg−1, and etomidate 0.4 mg⋅kg−1. The muscle relaxation monitoring module (E-NMT-01, GE Healthcare, Helsinki,) started when patient was unconscious and the anesthesia depth Ai value of the electroencephalogram spectrum monitor achieved 40. The neuromuscular function (NMF) was continuously monitored in the arm (contralateral to intravenous access) by acceleromyographic TOF (frequency 2 Hz, wave width 200μs, current intensity 60 mA, interval 15s) responses of the adductor pollicis muscle to the ulnar nerve stimulation.25,26 When the supramaximal stimulation was achieved and was stable for 5 min, 0.2 mg⋅kg−1 mivacurium was given to the patient. Tracheal intubation was completed at maximal depression at T1 by an experienced anesthesiologist, and the stimulating pattern of muscle relaxation monitoring was converted to TOF stimulation.
The patients underwent mechanical ventilation (Aestiva, GE/Datex-Ohmeda) with volume-controlled ventilation (VCV), respiratory rate 8–10 bpm, inspiration-expiratory (I:E) ratio 1:2, tidal volume 8 mL⋅kg−1 ideal body weight [45.5+0.91x(height cm-152.4)]. PETCO2 was kept at the level of 35–45 mmHg through adjusting the above respiratory settings. Anesthesia was maintained with the continuous infusion of propofol (50–100 μg·kg−1·min−1) and remifentanil (0.05–0.2 μg·kg−1·min−1). The depth of anesthesia (Ai value) was continuously monitored with an electroencephalogram spectrum monitor (Conview YY-105, Zhejiang Puke Medical Technology Co., LTD.) and was maintained 40–60 mmHg, and the mean arterial pressure (MAP) was maintained 60–80 mmHg. During the surgical procedure, the TOF count was kept at 0–1 twitches and the muscle response abolishment was higher than 95%. In case the TOF ratio recovered to 0.25, an additional continuous infusion of 0.2 mg·kg−1·h−1 mivacurium was administered and then an increase of 0.05 mg·kg−1·h−1 mivacurium was given each time every 5 min interval to make TOF ratio reached 0. After full recovery of NMF (TOF ratio≥ 0.9), the patient’s endotracheal tube was removed and was then transported from the operating room to the post-anesthesia care unit (PACU).
After staying in the PACU for at least 30 minutes and achieving a modified Aldrete score of 9, patients were returned to the general wards.27 If the numerical rating scale for pain (NRS, on an 11-point scale, 0=no pain, 10=most severe pain) was higher than 3, intravenous or complementary oral analgesics, including non-steroidal anti-inflammatory drugs, acetaminophen, and opioids, were offered if necessary.
Data Collection and Outcome Assessment
The baseline data including age, body mass index, years of education, family income, stable occupation, surgical diagnosis, preoperative condition, preoperative hemoglobin level, and the ENRICH Marital Satisfaction Scale were all assessed. Intraoperative data included the duration of anesthesia, fluid infusion, type of surgery, medication during anesthesia, surgical space conditions during the entire procedure assessed by the surgeon,28 and the surgical space conditions during dissection of the tumor of the uterus or ovary.2,29 Postoperative data included use of non-steroidal anti-inflammatory drugs (NSAIDs) or opioids, admission to the intensive care unit (ICU), postoperative delirium (assessed using the confusion assessment method),30 and length of hospital stay after surgery.
The primary outcome was the onset time of mivacurium, defined as the time from the administration of a bolus of mivacurium to 100% muscle response abolishment (T1=0). The secondary outcomes included the consumption of mivacurium, the non-response period (defined as the time from 100% muscle response abolishment (T1=0) to firstly partial recovery of first TOF response for the first time (T1>0)), the clinical duration during the maintenance period (defined as the time from the administration of continuous infusion of mivacurium to 25% recovery of first TOF response during recovery from anesthesia), the recovery index (defined as the time between 25% and 75% recovery of first TOF response during recovery from anesthesia), the extubation time (defined as the time from stopping the infusion of mivacurium to extubation), the tracheal intubation conditions,31 the pain NRS score on postoperative 1h, 6h, 12h, and days 1, 2, 3, and Ramsay sedative scale score (ranges from 1 to 6, where 1 indicates restlessness, 6 indicates deeply asleep and does not respond and 2 indicates completely awake, quiet and cooperative) on postoperative 1h, and 6h. The other outcomes included the consumption of remifentanil, clinical duration during the induction period (defined as the time from 100% muscle response abolishment (T1=0) to 25% recovery of the first TOF response for the first time), and postoperative complications.32
The occurrence of adverse events such as hypertension, hypotension, tachycardia, bradycardia, arrhythmia, desaturation, bronchospasm, laryngeal edema, hyperemia, nausea and vomiting, skin flushing, rash, dizziness, tinnitus, paresthesia, myalgia, muscle stiffness or tremor, and convulsions was recorded and treated according to medical protocols when necessary. Hypotension was defined as a systolic blood pressure lower than 20% of the baseline value; while hypertension was defined as a systolic blood pressure higher than 20% of the baseline value; bradycardia was defined as heart rate (HR) lower than 60 beats per minute; and tachycardia was defined as HR higher than 100 beats per minute; desaturation was defined as SpO2 lower than 90%.
Statistical Analysis
Sample Size Estimation
The sample size for our study was estimated by using PASS 15.0 software. It has been reported that the onset time of 0.2 mg·kg−1 mivacurium was 104s-203s.33,34 Based on the results of our pilot study, we estimate that the average onset time of mivacurium was 168.8s, while the average onset time of mivacurium chloride after lidocaine administration was 154.3s, with a standard deviation of 15.7. Based on a statistical power (1-β) of 90% and α of 5%, approximately 52 patients were required. Taking into account a dropout rate of 20%, the sample size was 66 patients (33 in each group).
Outcome Analysis
The outcome analysis was carried out on the intention-to-treat population of the two groups. For the baseline data and perioperative data, the chi-squared test, continuity-corrected chi-squared test, or Fisher’s exact test were employed for the analysis of categorical variables; the Shapiro–Wilk test was performed to evaluate the distribution of continuous variables, then, an independent samples t-test was performed with a normal distribution, while Mann–Whitney U-test were performed with a non-normal distribution.
The primary outcome was the onset time of mivacurium, which was compared using the independent samples t-test, and mean differences and 95% confidence intervals (CIs) were calculated. Among secondary and other outcomes, categorical variables (postoperative complications) were analyzed using the chi-square test, continuity-corrected chi-square test, or Fisher’s exact test. For continuous variables that followed normal distribution, the independent samples t-test was used for analysis; for those that did not follow normal distribution (consumption of mivacurium, non-response period, clinical duration during the maintenance period, recovery index, extubation time, tracheal intubation conditions, pain NRS, Ramsay sedative scale at 1h, 6h, 12h, 1d, 2d, and 3d; consumption of remifentanil; and clinical duration during the induction period), the Mann–Whitney U-test was used for analysis and the Hodges-Lehmann estimator was employed to calculate median differences and 95% CIs. The slope of the consumption of mivacurium or remifentanil was defined as the average increase in the demand for mivacurium or remifentanil per minute of surgery duration, calculated using a linear regression model and compared between groups through analysis of covariance. We also used the generalized estimating equations to analyze and evaluate the interaction of “group × time” for the NRS score of pain, the Ramsay sedation score, MAP, HR, and SpO2.35
For the exploratory analyses, the most severe pain score within 72 h and the area under the curve (AUC) of pain intensity within 72 h we determined.36,37 The between-group difference in the most severe pain score within 72 h was compared using the Mann–Whitney U-test, with median differences and 95% CIs calculated using Hodges-Lehmann estimator. The between-group difference in the AUC of pain intensity within 72 h was compared using the independent-sample t-test, with mean differences and 95% CIs calculated using the independent-sample t-tests.
For each hypothesis, a two-sided P value less than 0.05 was determined as statistically significant. Bonferroni correction was performed for repeated comparisons. The software we used for statistical analysis and chart drawing were IBM SPSS for Windows version 25.0 (IBM SPSS, Armonk, NY, USA) and GraphPad Prism (version 5.0; GraphPad Software Inc., San Diego, CA, USA).
Results
Patient Characteristics
Between May 14, 2024, and June 30, 2024, 88 patients were recruited for eligibility. Then, nine patients did not meet the inclusion criteria, including BMI higher than 25, and a history of asthma or OSAS, severe sinus bradycardia, and allergy to mivacurium. Thirteen patients declined to participate in the study. Finally, a total of 66 patients were randomly assigned to two groups (n=33 in each group) and enrolled in the final analysis (Figure 1). The baseline demographic data and surgical characteristics were comparable between the two groups (Table 1).
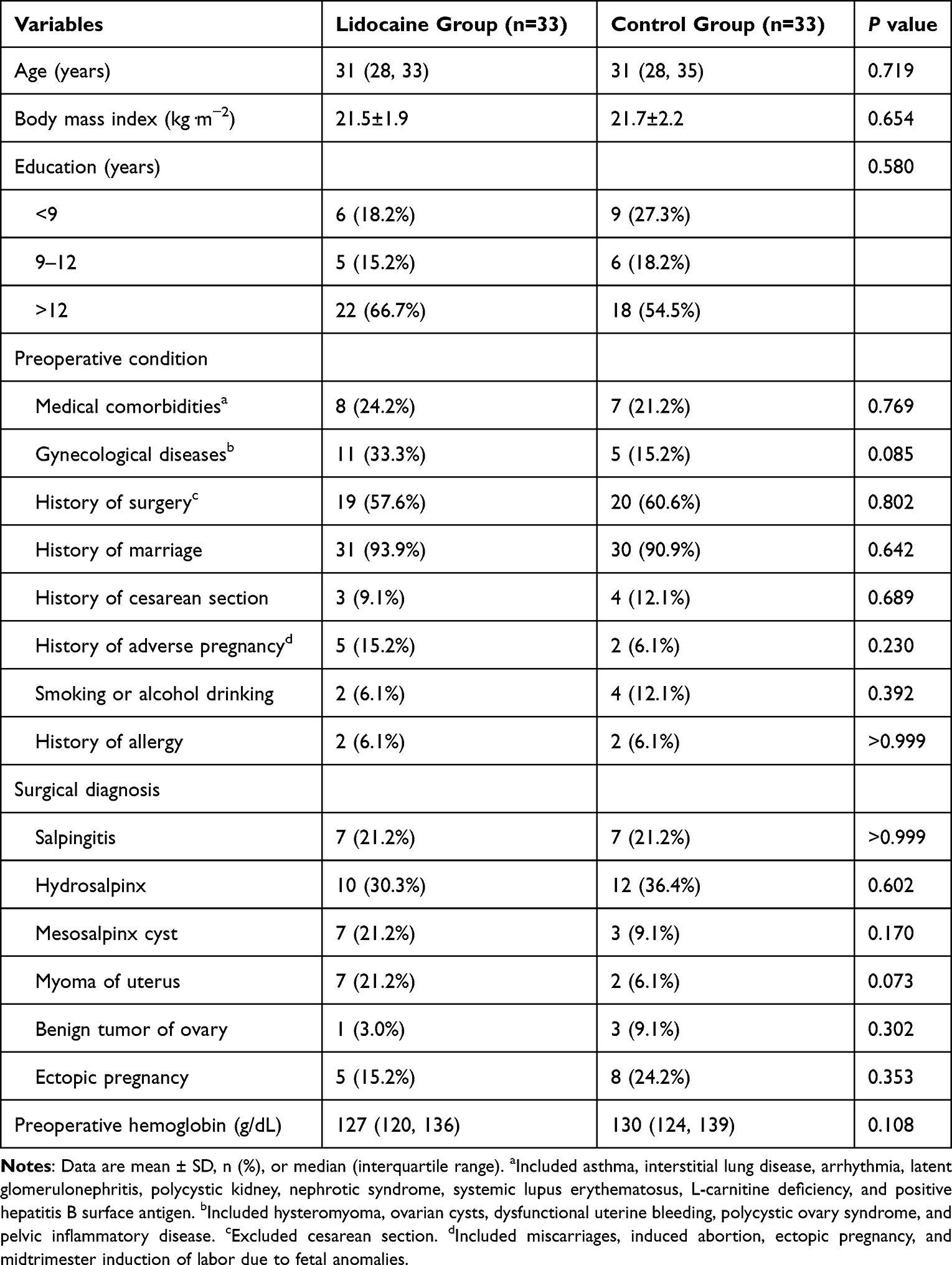 |
Table 1 Baseline Data |
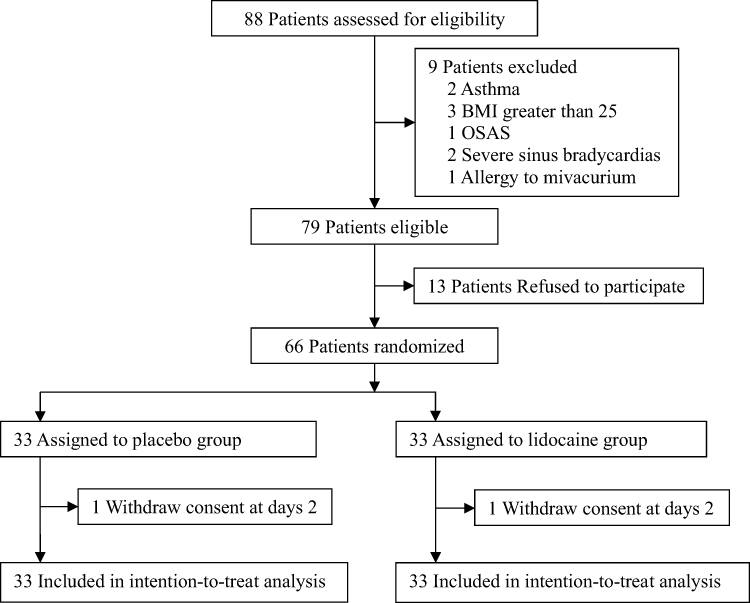 |
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram defining patient assessment and enrollment numbers in the study. |
Perioperative Data
The intraoperative data, including duration of anesthesia, fluid infusion, type of surgery, medication during anesthesia, surgical space conditions during the entire procedure assessed by the surgeon, and surgical space conditions during dissection of the tumor of the uterus or ovary, did not differ between the two groups (Table 2). Postoperative data, including admission to the ICU, use of NSAIDs or opioids, postoperative delirium, and length of hospital stay after surgery, did not differ between the two groups (Table 2).
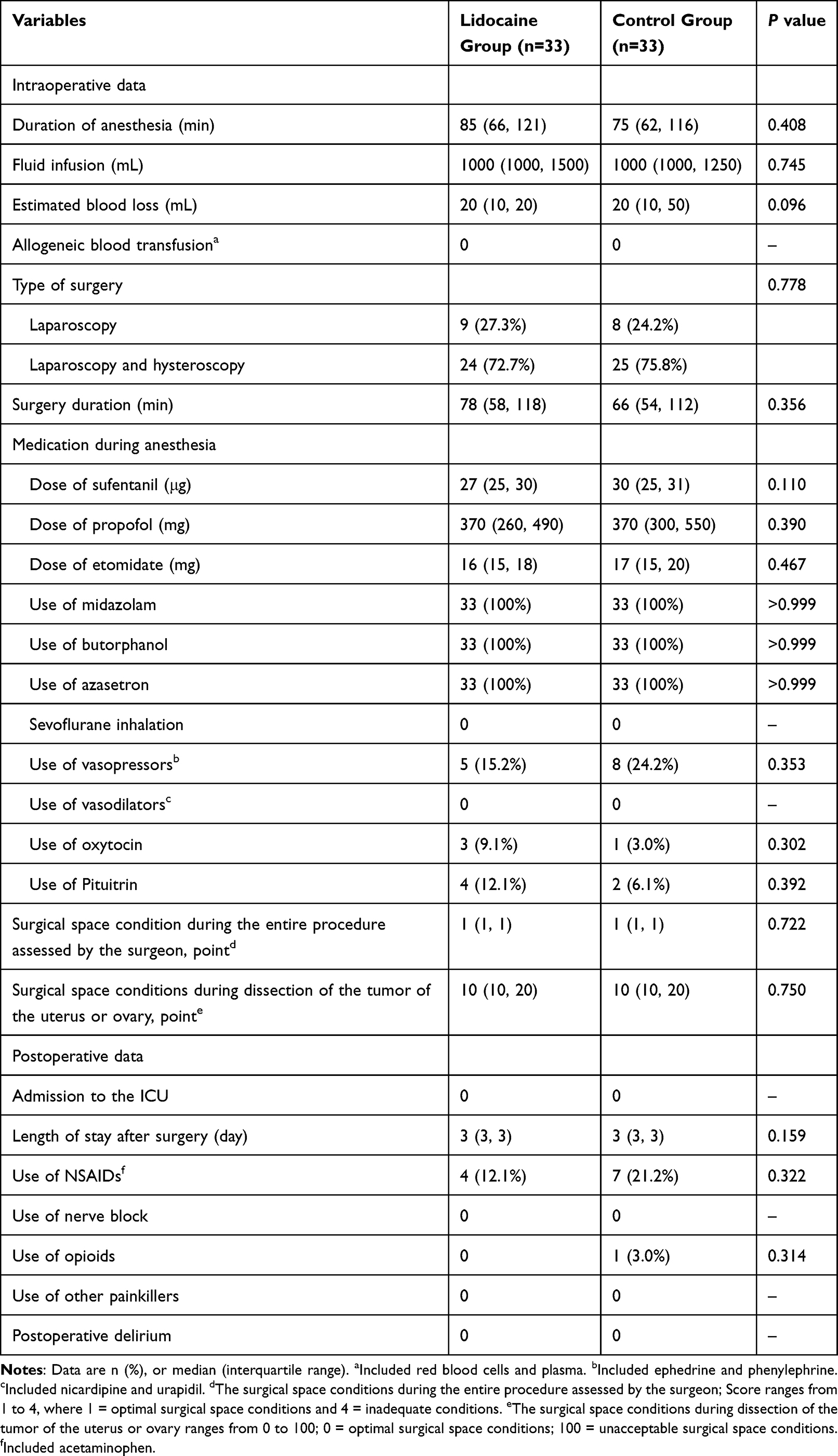 |
Table 2 Intraoperative and Postoperative Data |
Efficacy Outcomes
The onset time of mivacurium was obviously shorter in the lidocaine group than in the control group (mean difference −25.0 s, 95% CI −47.8 to −2.3, P=0.032) (Table 3 and Figure 2). The nonresponse period, clinical duration during the maintenance period, recovery index, and tracheal intubation conditions did not differ between the two groups (Table 3 and Figure 2). The hourly mivacurium consumption was also lower in the lidocaine group (0.21 [0.18 to 0.29] mg·kg−1·h−1) when compared with those in the control group (0.26 [0.23 to 0.32] mg·kg−1·h−1) (P=0.017; Table 3); the total mivacurium consumption did not differ between the two groups (Table 3). Additionally, the slope of the mivacurium consumption-duration curves was lower in the lidocaine group (0.0032 [95% CI, 0.0026–0.0039]) than in the control group (0.0047 [95% CI, 0.0039–0.0055]) (P=0.005, Table 3 and Figure 3). The extubation time was significantly shorter in the lidocaine group than in the control group (median difference, −3 min; 95% CI, −5 to −1; P=0.006) (Table 3 and Figure 4).
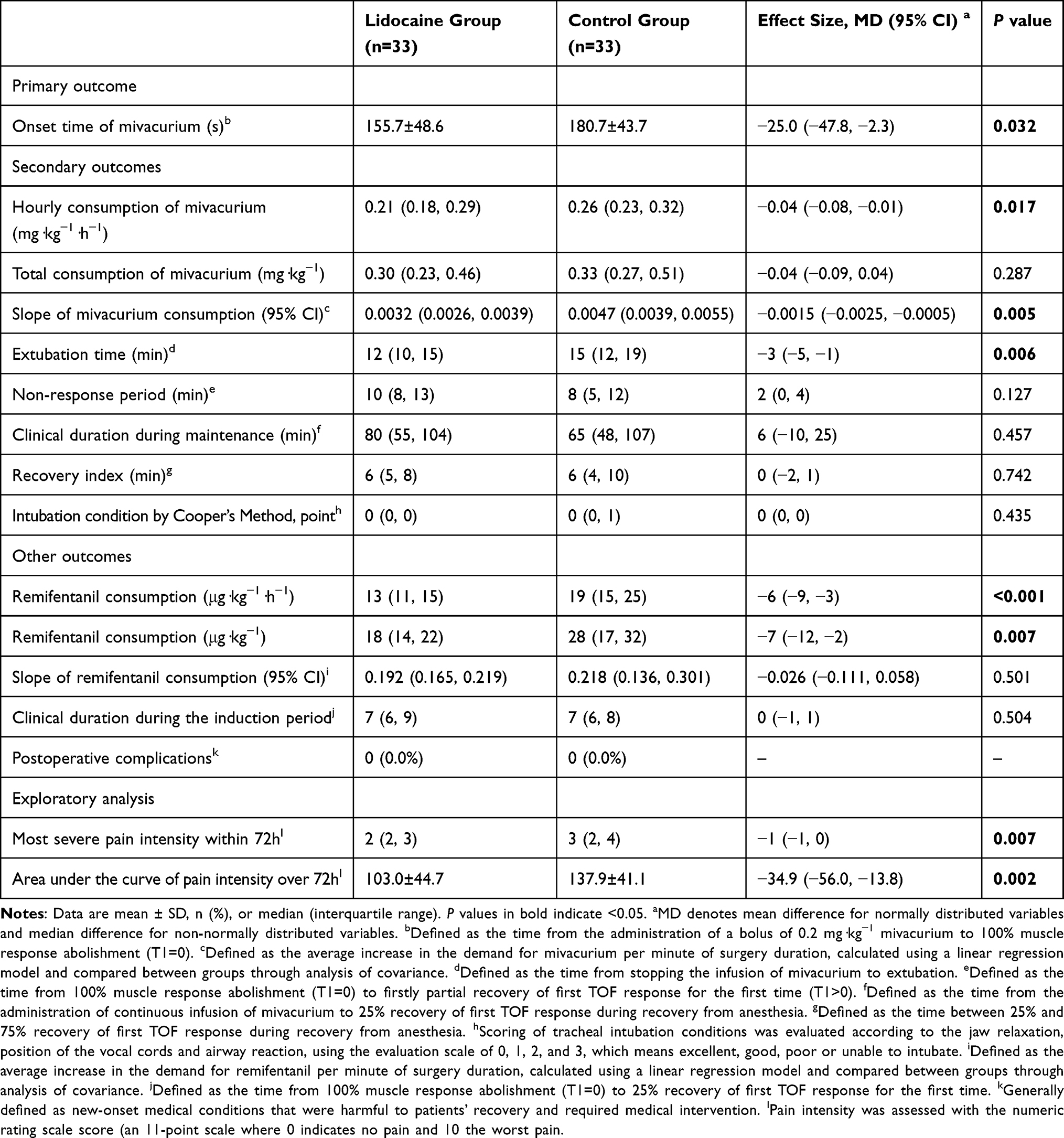 |
Table 3 Efficacy Outcomes |
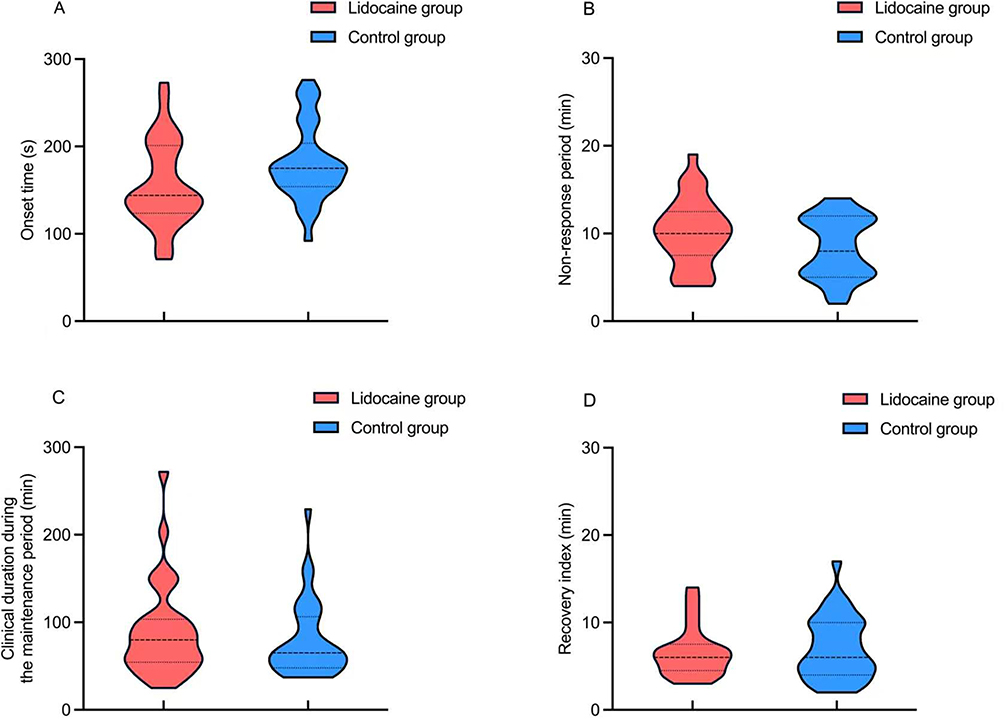 |
Figure 2 Comparison of the onset time (A), nonresponse period (B), clinical duration during the maintenance period of mivacurium (C), and recovery index (D) between the two groups. |
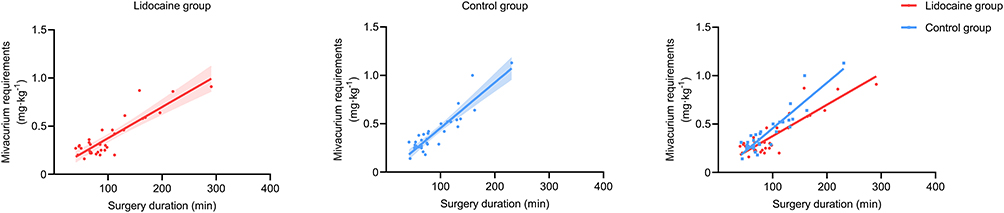 |
Figure 3 Comparison of mivacurium requirements between the two groups. |
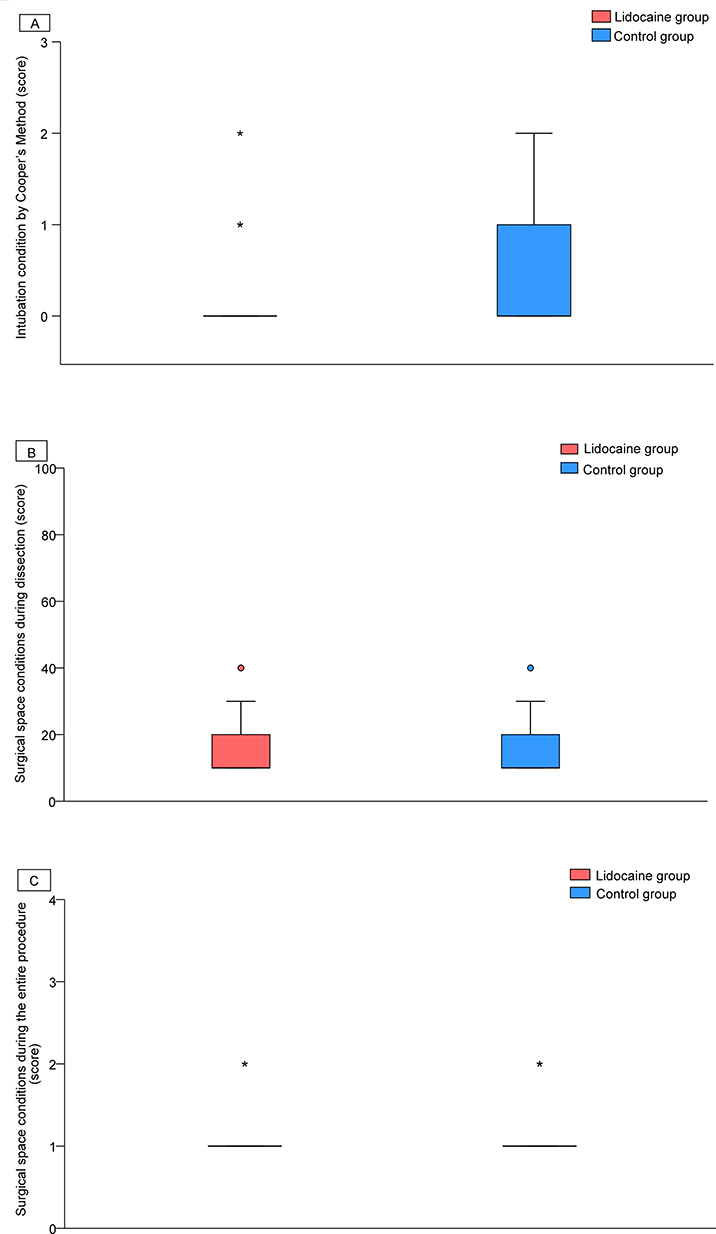 |
Figure 4 Comparison of the scoring of tracheal intubation conditions (A), surgical space conditions during the entire procedure assessed by the surgeon (B), and surgical space conditions during dissection of the uterine or ovarian tumor (C) between the two groups. The box and whisker plots show medians, interquartile ranges, and outer ranges; individual points indicate mild outliers (○, outside 1.5 times the interquartile range) and extreme outliers (*, outside 3 times the interquartile range). |
The clinical duration during the induction period and postoperative complications did not differ between the groups (Table 3). Hourly remifentanil consumption was also lower in the lidocaine group (13 [11–15] mg·kg−1·h−1) than in the control group (19 [15–25] mg·kg−1·h−1) (P<0.001; Table 3), and total remifentanil consumption was also lower in the lidocaine group (18 [14–22] mg·kg−1) than in the control group (28 [17–32] mg·kg−1) (P = 0.007; Table 3). However, the slope of the remifentanil consumption-duration curves did not differ between the two groups (Table 3 and Figure 3).
The NRS pain score was lower in the lidocaine group than in the control group at 6 h after surgery (P=0.004), and 12 h after surgery (P=0.001); the NRS pain score at 1 h after surgery, 1 d after surgery, 2 days after surgery, and 3 days after surgery did not differ between the groups (Table 4 and Figure 5). The Ramsay sedation scale score at all time points did not differ between the groups (Table 4 and Figure 5). The analysis results of the generalized estimating equation indicated that there was no interaction between time and group for the NRS score of pain (P=0.593) or the Ramsay sedation score (P=0.591). No significant differences were observed between the two groups in the MAP, HR, or SpO2 at any time point throughout the entire surgical procedure (Supplemental Table S1). The analysis results of the generalized estimating equation indicated that there was no interaction between time and group for the MAP (P=0.583), HR (P=0.516), or SpO2 (P=0.05).
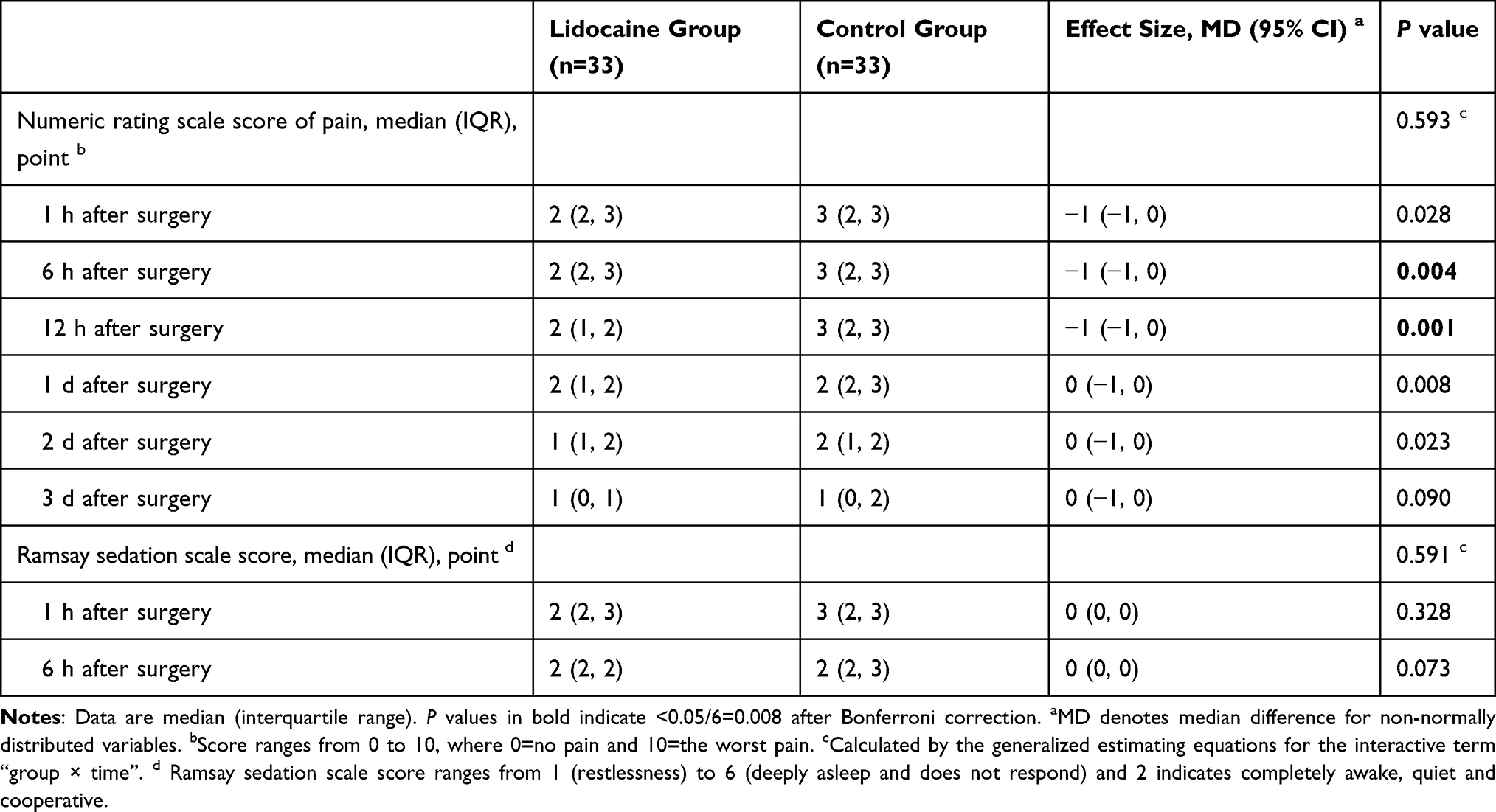 |
Table 4 Numeric Rating Scale Score of Pain and Ramsay Sedation Scale Score During the Perioperative Period (Secondary Outcomes) |
 |
Figure 5 Comparison of the NRS pain score (A) and Ramsay Sedation Scale score (B) between the two groups within postoperative 24h. NRS, a numeric rating scale, is an 11-point scale where 0=no pain and 10= worst pain. The Ramsay Sedation Scale is a 6-point scale where 1=restlessness; 2=completely awake, quiet, and cooperative; 3=drowsiness but responding to verbal commands; 4=light asleep but responding to touch or pain; 5= asleep but slowly responding to touch or pain; and 6= deep asleep and does not respond. The box and whisker plots show medians, interquartile ranges, and outer ranges; individual points indicate mild outliers (○, outside 1.5 times the interquartile range) and extreme outliers (*, outside 3 times the interquartile range).(#, P<0.008 versus the control group). |
In the exploratory analysis, the most severe pain score within 72 h was lower in the lidocaine group than in the control group (median difference −1, 95% CI, −1 to 0; P=0.007) (Table 3), and the AUC of pain intensity within 72 h was also lower in the lidocaine group than in the control group (mean difference −34.9, 95% CI −56.0 to −13.8, P=0.002) (P = 0.002; Table 3).
Safety Outcomes
Throughout the entire surgical procedure and within the three days following the operation, the incidence of adverse events such as hypertension, hypotension, arrhythmia, tachycardia, bradycardia, desaturation, and bronchospasm did not differ between the groups. The risks of nausea and vomiting, skin flushing, rash, dizziness, tinnitus, paresthesia, myalgia, muscle stiffness or tremor, and convulsions did not differ between the groups. Table 5 reported only adverse events with at least one occurrence in either group.
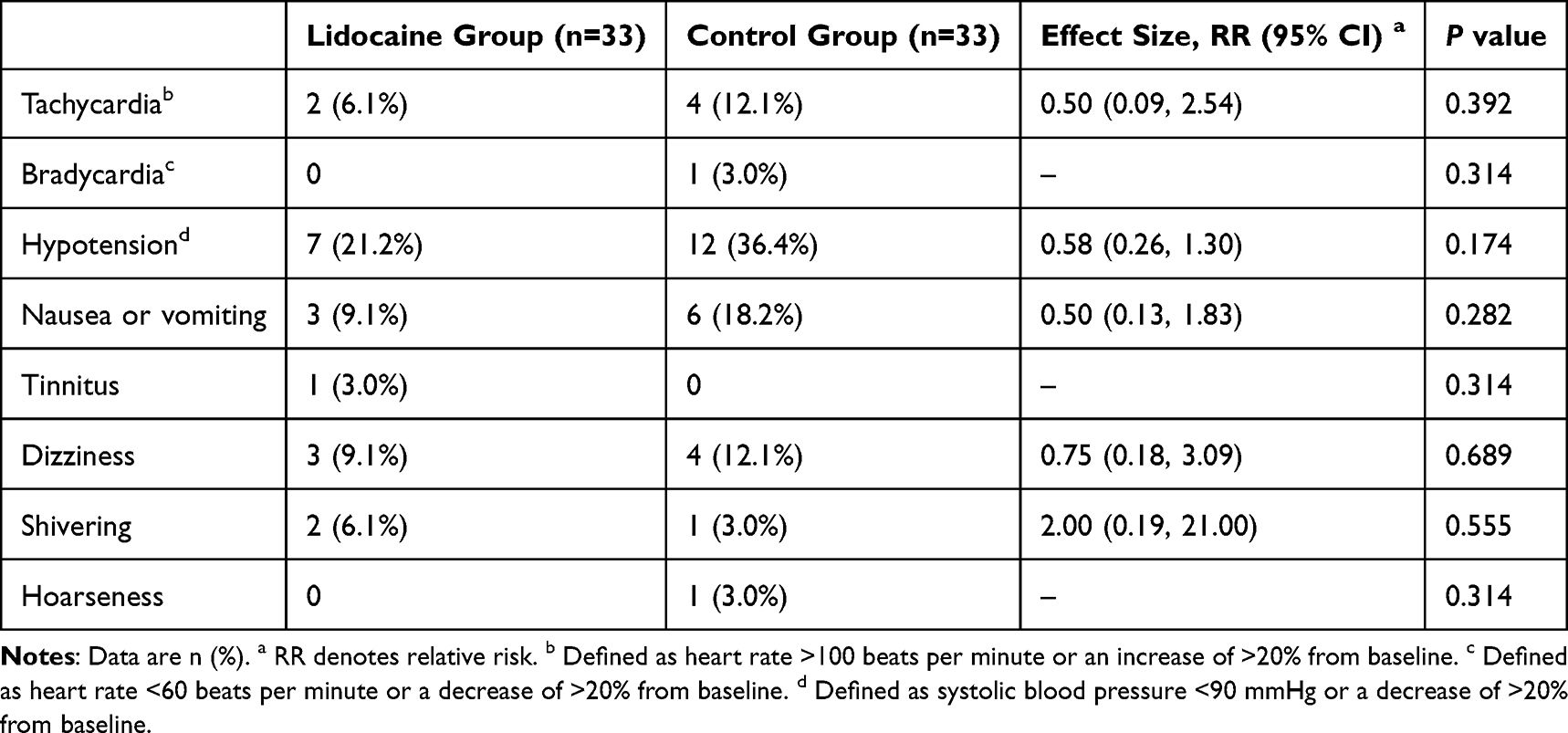 |
Table 5 Adverse Events |
Discussion
In this prospective study, we first evaluated the effects of lidocaine on the dosage requirements and onset time of mivacurium administration during gynecological laparoscopic surgery. Notably, we were delighted to discover that intraoperative intravenous administration of low-dose lidocaine significantly reduced the hourly requirements of mivacurium, accelerated its onset time, shortened extubation time, and improved postoperative pain without causing adverse events during gynecological laparoscopic surgery, suggesting that the medication regimen for lidocaine may reduce the risk of residual muscle relaxation after surgery to some extent.
Mivacurium is one of the shortest acting non-depolarizing neuromuscular blocking agents (NDMRs) available and has the advantages of short infusion time and unchanged recovery characteristics.38 Furthermore, it has been proved to provide the best conditions for tracheal intubation and improve the surgical environment.38 However, some clinical conditions, diseases (such as infections, oculopharyngeal muscular dystrophy, congenital heart defects, renal failure, liver cirrhosis) and drug interactions are considered to potentially lead to resistance to NDMRs, which may result in difficulties in intubation or suboptimal operating conditions during the surgery.39 Lidocaine, as an amide local anesthetic, has been increasingly used in surgical patients because of its neuromuscular blocking properties.40 According to previous reports, pre-treatment with intravenous 2% lidocaine 1.5 mg·kg−1 prior to tracheal intubation remarkably reduced the time to onset of neuromuscular block caused by vecuronium,17 Whereas, several direct evidences still showed that intravenous lidocaine 1.5 mg·kg−1 followed by a continuous infusion of 2 mg·kg−1·h−1 throughout surgery has no impact on the onset time of a 0.6 mg·kg−1 rocuronium-induced neuromuscular block,41,42 and a bolus of 3 mg·kg−1 lidocaine with a continuous infusion of 3 mg·kg−1·h−1 during the operation did not change the speed of onset of cisatracurium and exert any additional impact on the cisatracurium-induced neuromuscular block, even combined with magnesium sulfate.40 Our team firstly investigated the effect of low-dose lidocaine on the neuromuscular block profile of mivacurium during gynecological laparoscopic surgery and found that our dose of lidocaine significantly shortened the onset time of mivacurium, which contributed to establish the airway earlier and reduce the risks of hypoxemia, airway obstruction, and aspiration during anesthesia induction. We speculated that there might be two possible reasons. Firstly, lidocaine may enhance the blocking effect of mivacurium at the neuromuscular junction by inhibiting nerve conduction, thereby increasing the intensity of muscle relaxation. Secondly, lidocaine may also indirectly affect the effect of muscle relaxants through mechanisms such as regulating calcium ion channels or influencing the release of presynaptic neurotransmitters. Nevertheless, the reduction in the onset time of muscle relaxation was relatively small, so its impact on the overall intubation time was rather minor. Moreover, specific mechanisms such as direct neuromuscular regulation, analgesic synergy, or other pharmacological responses remain unclear at present and warrant further exploration through more research.
Low-dose lidocaine may have a relatively brief duration of action, limiting its ability to prolong the enhancement of the neuromuscular blocking effects. Present evidence showed that the lower thoracic epidural continuous injection of lidocaine significantly prolonged the mean clinical duration from administration of the first dose to T1 recovery to 5% of baseline obtained by vecuronium 0.1 mg·kg−1.16 Conversely, a randomized controlled trial conducted in Switzerland reported that intravenous lidocaine at a bolus dose of 1.5 mg·kg−1 followed by a continuous infusion of 2 mg·kg−1·h−1 did not influence the clinical duration (until first twitch has recovered to 25%) of the neuromuscular blockade induced by a standard intubation dose of rocuronium in adults undergoing surgery.41 Likewise, our lidocaine dosage regimen did not alter the non-response period or clinical duration during induction, nor did it improve intubation conditions, which may be attributable to the inclusion of a relatively young female patient population. However, it is still necessary to perform large-scale studies to investigate the actual impact of intraoperative lidocaine supplementation on the clinical duration of action of mivacurium.
Despite numerous studies showing the benefits of intraoperative systemic NMBAs in various surgeries, excessive use can lead to postoperative residual neuromuscular block and increased respiratory complications, such as, pulmonary infection and atelectasis.6,8 Currently, few researches paid more attention to the effects of the perioperative adjuncts on the consumption of NMBAs and draw the determined judgements. Strikingly, a previous randomized controlled trial stated that the intraoperative systemic lidocaine infusion (1.5 mg·kg−1 bolus, then 1.5 mg·kg−1·h−1) can result in decreased intraoperative consumption of rocuronium and higher TOF ratios at time of extubation and on arrival to PACU in generally anesthetized patients.43 Local anesthetics act on neuromuscular transmission in a dose-dependent manner and may potentiate the effects of NMBAs. We summarized the dosage of mivacurium and found that our use of lidocaine infusion successfully delayed the hourly consumption of mivacurium and flattened the slope of the mivacurium chloride consumption-duration curves, implying that lidocaine not only accelerated the onset of mivacurium but also enhanced its muscle relaxant effect, thereby helping achieve a clinically acceptable depth of neuromuscular blockade. However, the amount of muscle relaxant saved was relatively small, so the overall clinical benefits of adding lidocaine still need to be further evaluated.
Previous evidence showed that intraoperative intravenous lidocaine did not prolong the time to spontaneous recovery of a TOF ratio ≥ 0.9 after administered cisatracurium.23 Similarly, our findings showed no significant changes in the clinical duration during the maintenance period and the recovery index, which may be due to the shorter infusion time of lidocaine. Importantly, we observed the shortened extubation time, suggesting that lidocaine may reduce the incidence of residual neuromuscular block by influencing the sensitivity of neuromuscular conduction, thereby altering the dose requirement of mivacurium. Despite previous literature indicating that intraoperative intravenous administration of 1 mg·kg−1 lidocaine followed by continuous infusion at 1.5 mg·kg−1·h−1 did not reduce the extubation time in elderly patients undergoing hip fracture.44 This discrepancy could be attributed to differences in patient age, lidocaine dosing, and surgical type. However, our data also reflect the strong synergistic effects of lidocaine. Further high-quality studies are needed to investigate its impact on recovery time, extubation time, and mivacurium requirements in broader populations.
During the entire surgical procedure, continuous intravenous infusion of systemic lidocaine has analgesic, antihyperalgesic, and anti-inflammatory properties. A recent meta-analysis including six randomized controlled trials confirmed that intravenous lidocaine can lower postoperative pain scores, cumulative opioid requirements, and opioid-related adverse effects following laparoscopic cholecystectomy.45 Similarly, a randomized controlled trial declared that in elderly patients received intravenous lidocaine at 1 mg·kg−1 followed by continuous infusion at 1.5 mg·kg−1·h−1, the intraoperative total dosage of sufentanil, remifentanil, and propofol were obviously lower than in patients receiving normal saline during hip fracture surgery.44 Consistent with these findings, our study showed that intraoperative supplemental lidocaine significantly reduced the intraoperative requirements for remifentanil, suggesting that systemic lidocaine has a certain analgesic effect. In addition, our results also exhibited that lidocaine as an adjuvant significantly improved the NRS score for pain at 6 h and 12 h after surgery, suggesting that continuous intraoperative infusion of lidocaine has a short-term reduction in pain scores at 6 h and 12 h. In view of our small sample size, the clinical safety and postoperative outcomes of this patient population require further clarification. Our team has presented new insights regarding the use of lidocaine as an adjunctive medication, and has emphasized its new value and advantages in the perioperative period. This has provided new ideas for the perioperative care, drug selection, and optimal drug combination for patients undergoing laparoscopic surgery. More high-quality clinical trials are warranted to better understand its application and full effect in both generalized and special populations.
Limitations
Certainly, our study still had several limitations. First, participants with abnormal anatomy, a history of neuromuscular diseases, or a high risk of airway difficulties (eg, obesity and OSAS) have been excluded from our study, however, they may be more suitable for and would benefit from our protocol; therefore, they will be a key target population for our next study design. Second, only one of the commonly used intravenous doses (1.5 mg·kg−1 followed by a continuous infusion of 2 mg·kg−1·h−1) was selected. There is insufficient clinical evidence of the synergistic effect of intravenous lidocaine on muscle relaxation, and the optimal dose and infusion duration of lidocaine need to be further clarified. Third, it is significant to consider its potential side effects and safety profiles. Larger studies are warranted to fully evaluate the safety, long-term effects, and optimal administration strategies for intravenous lidocaine in different patient populations. Fourth, although the current study found that lidocaine significantly shortened the onset time of mivacurium and accelerated the extubation time and no apparent complications were observed in our participants, the effects of intravenous ancillary administration of lidocaine at various doses on mivacurium and the occurrence of adverse events remain unclear, and more high-quality follow-up studies are needed for systematic evaluation. Fifth, although the onset time of mivacurium was shortened by 25s and hourly consumption decreased by 0.04 mg·kg−1·h−1, the practical impact of these changes in routine clinical settings may be modest. Given that a 25s reduction is unlikely to influence standard intubation timing and the dosage saving is relatively small, the overall benefit of adding lidocaine infusion warrants further evaluation. Sixth, although the study observed significant effects of lidocaine on mivacurium but lacked a detailed exploration of the underlying mechanisms for example direct neuromuscular modulation, analgesic synergy, or other pharmacologic reactions. Our team’s future research will focus on further in-depth exploration of the potential pharmacological and molecular biological mechanisms of the interaction between lidocaine and mivacurium.
Conclusions
In summary, our initial research suggested that the intraoperative administration of low-dose lidocaine significantly reduced the hourly consumption of mivacurium, expedited the onset time, shortened the extubation time, and decreased the pain score at 6 h and 12 h after surgery, without increasing adverse events in patients with a low risk of airway difficulty. Accordingly, we speculated that whether the intravenous administration of lidocaine could potentially lower the risk of residual neuromuscular blockade after surgery remains uncertain at present and requires confirmation in future studies. However, due to the small single-centre sample, our research results need to be further verified through future large-sample multi-center studies. However, in clinical practice, anesthesiologists still need to fully understand the potential interaction between lidocaine and mivacurium, and rationally adjust the timing and dosage of medication to ensure the safety and controllability of the anesthesia process. Future research should further explore the interaction mechanisms of these two drugs under different physiological and pathological conditions to provide a more solid theoretical basis for individualized anesthesia management.
Data Sharing Statement
All information required is given in the text and supplementary materials, other supplementary information can be obtained upon Email from the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest.
References
1. Shi X, Chen S, Yang Y, Liu L, Huang L. Laparoscopic surgeries for uterine fibroids and ovarian cysts reduce ovarian reserve via age- and surgical type-manner. Gynecol Endocrinol. 2022;38(12):1068–17. doi:10.1080/09513590.2022.2128104
2. Staehr-Rye AK, Rasmussen LS, Rosenberg J, et al. Surgical space conditions during low-pressure laparoscopic cholecystectomy with deep versus moderate neuromuscular blockade: a randomized clinical study. Anesth Analg. 2014;119(5):1084–1092. doi:10.1213/ANE.0000000000000316
3. Barrio J, Errando CL, San Miguel G, et al. Effect of depth of neuromuscular blockade on the abdominal space during pneumoperitoneum establishment in laparoscopic surgery. J Clin Anesth. 2016;34:197–203. doi:10.1016/j.jclinane.2016.04.017
4. Bruintjes MH, van Helden EV, Braat AE, et al. Deep neuromuscular block to optimize surgical space conditions during laparoscopic surgery: a systematic review and meta-analysis. Br J Anaesth. 2017;118(6):834–842. doi:10.1093/bja/aex116
5. Madsen MV, Gätke MR, Springborg HH, Rosenberg J, Lund J, Istre O. Optimising abdominal space with deep neuromuscular blockade in gynaecologic laparoscopy--a randomised, blinded crossover study. Acta Anaesthesiol Scand. 2015;59(4):441–447. doi:10.1111/aas.12493
6. Fortier LP, McKeen D, Turner K, et al. The RECITE study: a Canadian prospective, multicenter study of the incidence and severity of residual neuromuscular blockade. Anesth Analg. 2015;121(2):366–372. doi:10.1213/ANE.0000000000000757
7. Kotake Y, Ochiai R, Suzuki T, et al. Reversal with sugammadex in the absence of monitoring did not preclude residual neuromuscular block. Anesth Analg. 2013;117(2):345–351. doi:10.1213/ANE.0b013e3182999672
8. Saager L, Maiese EM, Bash LD, et al. Incidence, risk factors, and consequences of residual neuromuscular block in the United States: the prospective, observational, multicenter RECITE-US study. J Clin Anesth. 2019;55:33–41. doi:10.1016/j.jclinane.2018.12.042
9. Frampton JE, McTavish D. Mivacurium: a review of its pharmacology and therapeutic potential in general anaesthesia. Drugs. 1993;45(6):1066–1089. doi:10.2165/00003495-199345060-00009
10. Ortiz JR, Carrascosa F. Mivacurium. Rev Esp Anestesiol Reanim. 1997;44(8):315–320.
11. Weber V, Abbott TEF, Ackland GL. Reducing the dose of neuromuscular blocking agents with adjuncts: a systematic review and meta-analysis. Br J Anaesth. 2021;126(3):608–621. doi:10.1016/j.bja.2020.09.048
12. Beaussier M, Delbos A, Maurice-Szamburski A, Ecoffey C, Mercadal L. Perioperative use of intravenous lidocaine. Drugs. 2018;78(12):1229–1246. doi:10.1007/s40265-018-0955-x
13. Xu L, Wang C, Dai S, et al. Intravenous lidocaine attenuates response to cervical dilation for hysteroscopy: a randomised controlled trial. Br J Anaesth. 2021;127(5):e166–e168. doi:10.1016/j.bja.2021.07.020
14. Yao W, Zhang L, Lu G, et al. Use of intravenous lidocaine for dose reduction of propofol in paediatric colonoscopy patients: a randomised placebo-controlled study. BMC Anesthesiol. 2021;21(1):299. doi:10.1186/s12871-021-01525-0
15. Hung KC, Chu CC, Hsing CH, et al. Association between perioperative intravenous lidocaine and subjective quality of recovery: a meta-analysis of randomized controlled trials. J Clin Anesth. 2021;75:110521. doi:10.1016/j.jclinane.2021.110521
16. Munakata K, Suzuki T, Watanabe N, et al. Influence of epidural lidocaine injection on vecuronium-induced neuromuscular blockade. Masui. 2004;53(12):1377–1380.
17. Nonaka A, Sugawara T, Suzuki S, Masamune T, Kumazawa T. Pretreatment with lidocaine accelerates onset of vecuronium-induced neuromuscular blockade. Masui. 2002;51(8):880–883.
18. Paek CM, Yi JW, Lee BJ, Kang JM. No supplemental muscle relaxants are required during propofol and remifentanil total intravenous anesthesia for laparoscopic pelvic surgery. J Laparoendosc Adv Surg Tech A. 2009;19(1):33–37. doi:10.1089/lap.2008.0051
19. Hopewell S, Chan AW, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. BMJ. 2025;389:e081123. doi:10.1136/bmj-2024-081123
20. Agha R, Mathew G, Rashid R, et al. Transparency in the reporting of artificial INtelligence – the TITAN guideline. Premier J Sci. 2025. doi:10.70389/PJS.100082
21. World Medical Association. Declaration of helsinki: ethical principles for medical research involving human participants. JAMA. 2025;333(1):71–74. doi:10.1001/jama.2024.21972
22. Langeron O, Masso E, Huraux C, et al. Prediction of difficult mask ventilation. Anesthesiology. 2000;92(5):1229–1236. doi:10.1097/00000542-200005000-00009
23. Hans GA, Defresne A, Ki B, et al. Effect of an intravenous infusion of lidocaine on cisatracurium-induced neuromuscular block duration: a randomized-controlled trial. Acta Anaesthesiol Scand. 2010;54(10):1192–1196. doi:10.1111/j.1399-6576.2010.02304.x
24. De Oliveira GS, Fitzgerald P, Streicher LF, Marcus RJ, McCarthy RJ. Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery. Anesth Analg. 2012;115(2):262–267. doi:10.1213/ANE.0b013e318257a380
25. Fuchs-Buder T, Brull SJ, Fagerlund MJ, et al. Good clinical research practice (GCRP) in pharmacodynamic studies of neuromuscular blocking agents III: the 2023 Geneva revision. Acta Anaesthesiol Scand. 2023;67(8):994–1017. doi:10.1111/aas.14279
26. Cardoso LS, Martins CR, Tardelli MA. Effects of intravenous lidocaine on the pharmacodynamics of rocuronium. Rev Bras Anestesiol. 2005;55(4):371–380. doi:10.1590/S0034-70942005000400001
27. Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7(1):89–91. doi:10.1016/0952-8180(94)00001-K
28. Williams MT, Rice I, Ewen SP, Elliott SM. A comparison of the effect of two anaesthetic techniques on surgical conditions during gynaecological laparoscopy. Anaesthesia. 2003;58(6):574–578. doi:10.1046/j.1365-2044.2003.03150.x
29. King M, Sujirattanawimol N, Danielson DR, Hall BA, Schroeder DR, Warner DO. Requirements for muscle relaxants during radical retropubic prostatectomy. Anesthesiology. 2000;93(6):1392–1397. doi:10.1097/00000542-200012000-00008
30. Antoine V, Belmin J, Blain H, et al. The confusion assessment method: transcultural adaptation of a French version. Rev Epidemiol Sante Publique. 2018;66(3):187–194. doi:10.1016/j.respe.2018.01.133
31. Cooper R, Mirakhur RK, Clarke RS, Boules Z. Comparison of intubating conditions after administration of Org 9246 (rocuronium) and suxamethonium. Br J Anaesth. 1992;69(3):269–273. doi:10.1093/bja/69.3.269
32. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
33. Hemmerling TM, Donati F, Beaulieu P, Babin D. Phonomyography of the corrugator supercilii muscle: signal characteristics, best recording site and comparison with acceleromyography. Br J Anaesth. 2002;88(3):389–393. doi:10.1093/bja/88.3.389
34. Vested M, Kempff-Andersen S, Creutzburg A, et al. Onset time, duration of action, and intubating conditions after mivacurium in elderly and younger patients. Acta Anaesthesiol Scand. 2024;68(7):898–905. doi:10.1111/aas.14440
35. Pandit JJ. The analysis of variance in anaesthetic research: statistics, biography and history. Anaesthesia. 2010;65(12):1212–1220. doi:10.1111/j.1365-2044.2010.06542.x
36. Matthews JN, Altman DG, Campbell MJ, Royston P. Analysis of serial measurements in medical research. BMJ. 1990;300(6719):230–235. doi:10.1136/bmj.300.6719.230
37. Andersen LPK, Gögenur I, Torup H, Rosenberg J, Werner MU. Assessment of postoperative analgesic drug efficacy: method of data analysis is critical. Anesthesia Analg. 2017;125(3):1008–1013. doi:10.1213/ANE.0000000000002007
38. Zeng R, Liu X, Zhang J, et al. The efficacy and safety of mivacurium in pediatric patients. BMC Anesthesiol. 2017;17(1):58. doi:10.1186/s12871-017-0350-2
39. Mørk EL, Kristensen ML, Stokholm JB, Söderström CM, Madsen MV, Gätke MR. Resistance towards nondepolarising muscle relaxants: prolonged onset time: a systematic review. Eur J Anaesthesiol. 2019;36(7):477–485. doi:10.1097/EJA.0000000000000991
40. Paula-Garcia WN, Oliveira-Paula GH, de Boer HD, Garcia LV. Lidocaine combined with magnesium sulfate preserved hemodynamic stability during general anesthesia without prolonging neuromuscular blockade: a randomized, double-blind, controlled trial. BMC Anesthesiol. 2021;21(1):91. doi:10.1186/s12871-021-01311-y
41. Czarnetzki C, Lysakowski C, Elia N, Tramèr MR. Intravenous lidocaine has no impact on rocuronium-induced neuromuscular block. Randomised study. Acta Anaesthesiol Scand. 2012;56(4):474–481. doi:10.1111/j.1399-6576.2011.02625.x
42. So SY, Kim YH, Ko YK, Park SI, Pak HJ, Jung WS. Effect of lidocaine (40 mg) mixed to prevent injection pain of propofol on the intubating conditions and onset time of rocuronium. Korean J Anesthesiol. 2013;64(1):29–33. doi:10.4097/kjae.2013.64.1.29
43. Omar AM. Effect of systemic lidocaine infusion on train-of-four ratios during recovery from general anesthesia. Egypt J Anaesth. 2019;28(4):281–286. doi:10.1016/j.egja.2012.07.002
44. Li X, Wu J, Lan H, et al. Effect of intraoperative intravenous lidocaine on postoperative delirium in elderly patients with hip fracture: a prospective randomized controlled trial. Drug Des Devel Ther. 2023;17:3749–3756. doi:10.2147/DDDT.S437599
45. Li J, Wang G, Xu W, Ding M, Yu W. Efficacy of intravenous lidocaine on pain relief in patients undergoing laparoscopic cholecystectomy: a meta-analysis from randomized controlled trials. Int J Surg Feb. 2018;50:137–145. doi:10.1016/j.ijsu.2018.01.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of 3 Rates for the Continuous Infusion of Mivacurium During Ambulatory Vitreoretinal Surgery Under General Anesthesia: A Prospective, Randomized, Controlled Clinical Trial
Zhang Y, Xi C, Yue J, Zhao M, Wang G
Drug Design, Development and Therapy 2022, 16:3133-3143
Published Date: 16 September 2022