")
Back to Journals » International Journal of Women's Health » Volume 13
Effect of Happiness Counseling on Depression, Anxiety, and Stress in Women with Recurrent Miscarriage
Authors Elsharkawy NB, Mohamed SM, Awad MH, Ouda MMM
Received 23 October 2020
Accepted for publication 4 February 2021
Published 2 March 2021 Volume 2021:13 Pages 287—295
DOI https://doi.org/10.2147/IJWH.S283946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Nadia Bassuoni Elsharkawy,1,2 Sayeda Mohamed Mohamed,3 Mohamed Hammam Awad,4 Marwa Mohamed Ahmed Ouda1,5
1Nursing Department, College of Applied Medical Sciences, Jouf University, Sakaka, Saudi Arabia; 2Maternal and Newborn Health Nursing Department, Faculty of Nursing, Cairo University, Cairo, Egypt; 3Psychiatric Mental Health Nursing Department, Faculty of Nursing, Cairo University, Cairo, Egypt; 4Obstetrics and Gynecology Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 5Pediatric Nursing Department, Faculty of Nursing, Damanhur University, Egypt
Correspondence: Nadia Bassuoni Elsharkawy
Nursing Department, College of Applied Medical Sciences, Jouf University, Sakaka, Jouf, Kingdom of Saudi Arabia
Tel +966-554180474
Email [email protected]
Purpose: This study investigated the effectiveness of a happiness counseling program on depression, anxiety, and stress in pregnant women with a history of recurrent miscarriage.
Patients and Methods: A parallel randomized controlled trial research design was used in this study, which was conducted at the high-risk inpatient unit of the Obstetrics and Gynecology Hospital of Cairo University Hospitals in Cairo, Egypt. A total of 60 pregnant women who had previously experienced multiple miscarriages were randomly assigned to intervention and control groups (n=30 each). The tools used for data collection were demographic and obstetric data questionnaires and the 21-item Depression, Anxiety, and Stress Scale (DASS-21). Happiness counseling sessions were conducted for the intervention group. Data for qualitative variables were analyzed with the chi-squared test, and the Student’s t test for paired samples was used to compare mean DASS-21 scores of the intervention and control groups. The Pearson correlation coefficient was used to analyze the association between variables.
Results: The happiness counseling sessions reduced depression, anxiety, and stress in women with recurrent miscarriage, resulting in lower mean DASS-21 scores for the intervention group compared to the control group.
Conclusion: The happiness counseling program had a positive effect on reducing depression, anxiety, and stress in women with recurrent miscarriage. We recommend that this program be used as an effective, low-cost, and noninvasive intervention to improve the mental health and overall wellbeing of women with recurrent miscarriage.
Keywords: happiness counseling program, depression, anxiety, stress, recurrent miscarriage
Introduction
Spontaneous abortion or miscarriage is one of the most common complications during pregnancy. It is estimated that miscarriage occurs in 20% of all clinically recognized pregnancies and up to half of all pregnancies.1 Recurrent miscarriage, which affects 2–5% of couples, is defined as the loss of ≥3 or more consecutive pregnancies before the 20th week of gestation.2 Causes of recurrent miscarriage include chromosomal abnormalities in either partner, uterine abnormalities, and the presence of anti-phospholipid antibodies; additionally, an abnormal karyotype in the embryo is observed in 25–50% of cases. However, >50% of recurrent miscarriages are unexplained.3
The experience of miscarriage—especially repeated episodes—can alter a woman’s mental health state and general wellbeing,2 which may manifest as increased rates of anxiety, distress, and depression persisting up to 1 year later. Moreover, the adverse effects of a miscarriage on mental health can continue through subsequent pregnancies.3 It was found that 48–51% of women who had a spontaneous abortion experienced psychological complications. Increased rates of depression, posttraumatic stress disorder, anxiety, obsessive-compulsive disorder, misuse of drugs, anger, sadness, acute stress disorder, sorrow, sleep disorders, feelings of guilt, self-blame, low self-esteem, and marital conflict have been reported in women who have a miscarriage.4–6
A commonly held belief among women is that stress at the time of conception or during pregnancy can harm the fetus and cause problems such as miscarriage. One study reported that 76% of women attending antenatal clinics in the United States thought that stress could have a detrimental effect on pregnancy outcome, with 35% believing that pregnant women should avoid disturbing experiences such as watching violent television programs or attending funerals. In that study, women defined the word “stress” as any threat to their physical or psychological wellbeing or experiences associated with negative emotions. Some physicians and midwives also hold the view that stress can adversely affect the pregnancy, despite the knowledge that fetal chromosomal abnormalities are present in about two-thirds of cases of early pregnancy failure.7
Women with recurrent miscarriages suffer from suboptimal health-related quality of life and experience higher rates of anxiety and depression relative to those without a history of miscarriage.8 Assessment of stress and anxiety is critical for maintaining women’s overall health,9 as it can guide the early implementation of supportive interventions.10
One example of a non-pharmacologic intervention is a happiness training program that improves the cognitive and affective status of patients, allowing them to adopt a more positive attitude toward life events and respond optimistically to challenges by adapting to changing circumstances.11 Many researchers believe that happiness is the starting point for a healthy life, as happy people experience greater life satisfaction and safety, have more choices, and feel a greater connection to society. Conversely, a lack of happiness can cause stress and lead to illness.11
Awareness of the impact of psychosocial stress on women who have experienced repeated miscarriages could lead to improvements in psychological support screening. The present study was carried out in order to determine the effect of a happiness counseling program on depression, anxiety, and stress in pregnant women with a history of recurrent miscarriage. We hypothesized that happiness counseling would lower the levels of depression, anxiety, and stress in these women compared to those who did not receive the intervention. Our findings provide new insights that can guide maternal healthcare practices to ensure optimal pregnancy outcomes for women with a high-risk pregnancy.
Patiets and Methods
A parallel randomized controlled trial was conducted at the high-risk inpatient unit of the Obstetrics and Gynecology Hospital of Cairo University Hospitals from January to June 2019. A total of 60 pregnant women with a history of recurrent miscarriage were randomly assigned to intervention and control groups (n=30 each). The inclusion criteria were as follows: age between 18 and 45 years; and ≥3 previous consecutive miscarriages. Exclusion criteria were women with a medical history of depression or infertility, who had previous experience with psychotherapy, or missed >2 intervention sessions. Optimal sample size was calculated by comparing the means of the 2 groups (intervention and control). The power was set at 0.8; the alpha level at 0.05; and the confidence interval at 95% (Figure 1).
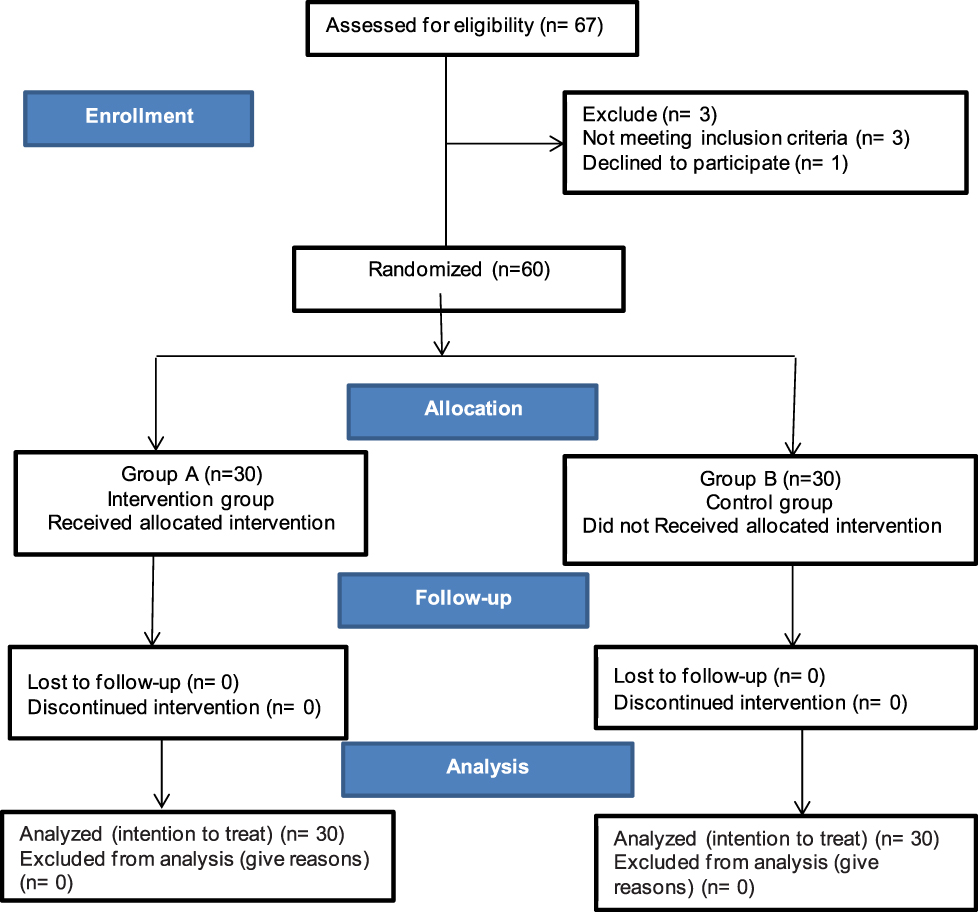 |
Figure 1 Flow chart. |
Data Collection
The following 2 data collection tools were used in this study.
- Demographic and obstetric data questionnaires were developed by our group to collect information about the patient’s age, level of education, occupation, gravidity, number of previous miscarriages and full-term pregnancies, duration of marriage, and gestational age in weeks of the current pregnancy.
- The 21-item Depression, Anxiety, and Stress Scale (DASS-21) is a short form of the 42-item DASS.12 The scale is divided into 3 subscales of 7 items each. The depression subscale assesses hopelessness, dysphoria, and engagement in life, self-deprecation, anhedonia, and inertia. The anxiety subscale assesses autonomic arousal, situational anxiety, subjective experience of anxious affect, and skeletal muscle effects. The stress subscale is sensitive to chronic nonspecific arousal levels and assesses nervous arousal; difficulty relaxing; and being irritable/over reactive, easily upset/agitated, and impatient. The scores for depression, anxiety, and stress are determined by summing the scores for the relevant items. The scoring system is based on a 4-point Likert scale ranging from 0 to 3 (0=does not apply to me at all, 1=applies some of the time, 2=applies to a considerable degree or for a good part of the time, and 3=applies very much or most of the time). The reliability of the DASS-21 in this study population was α=0.95. The subscales had good internal reliability (Cronbach’s α values of 0.82–0.84 for the depression subscale, 0.74–0.81 for the anxiety subscale; and 0.74–0.88 for the stress subscale)13 and strong convergent, discriminant validity.14
Intervention
After obtaining official approval to conduct the study, we interviewed all participants and explained the nature and purpose of the study before obtaining their written consent. For the pretest, DASS-21 and demographic and obstetric data questionnaires were administered, after which the participants were randomly assigned to intervention and control groups as follows. For 1 week, pregnant women who joined the study during the first 3 days of the week were assigned to the control group, and those who joined the study in the second 4 days of the week were assigned to the intervention group. This was reversed for the following week. The intervention group received happiness counseling program notifications regarding the time and place of the 1-h sessions (09:00–10:00), which were held in the conference hall of the hospital and consisted of 2 phases (assessment and program implementation).
- Assessment phase (2 sessions). The participants were introduced to each other and informed about the method and structure of the sessions. Participants described their expectations for the training program and completed the questionnaires.
- Implementation phase (8 sessions). The happiness counseling program was structured as follows.
- Session 1. Scientific information regarding the definition, prevalence, causes, diagnostic methods, and treatments for miscarriage was provided to the participants.
- Session 2. Participants were acquainted with techniques to increase their physical activity, productivity, and engagement in useful and meaningful activities.
- Session 3. Participants were taught the principles of better planning and organization and techniques for managing concerns, demands, and wishes.
- Session 4. Participants were taught techniques for increasing creativity and living in the present.
- Session 5. Participants were taught techniques for social enhancement and being real.
- Session 6. Participants were taught techniques for increasing intimacy with others as the primary source of happiness and prioritizing and valuing happiness.
- Session 7. Participants were taught techniques for expressing their thoughts/emotions and increasing optimism.
- Session 8. The techniques taught in the previous sessions were reviewed and the questionnaires were re-administered to collect data from both groups for post-program assessment.
Each session ended with a 5- to 10-min review of the content; feedback was also obtained from the patients at this time. At the end of the program, all of the techniques for enhancing happiness were reviewed and the participants were asked about their current levels of happiness and optimism. Any questions from the participants were answered by the investigators. The pretest was administered before the start of intervention and the posttest was administered 1 month after the last session.
Ethical Consideration
Official approval for the study was obtained from the scientific research ethics committee of the Faculty of Nursing at Cairo University and relevant hospital authorities. The study purpose was explained to chairperson of the continuing education department and nurses’ supervisors to obtain their support for conducting the study and facilitate the data collection process. The participants were informed that they had the right to withdraw from the study at any time without any adverse consequences. Code numbers were generated and used to ensure patient data confidentiality. Happiness counseling was provided to the control group after the end of the study, and the investigators made themselves available to answer any questions about the techniques and methods used in the program. This study was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
Data were analyzed using SPSS v21 software (SPSS Inc., Chicago, IL, USA), and are presented in the form of descriptive statistics (eg, frequency, percentages, mean, and standard deviation). The chi-squared test was used to analyze qualitative variables (eg, demographic data). The Student’s t test for paired samples was used to compare mean DASS-21 scores of intervention and control groups and pre- and posttest scores. The Pearson correlation coefficient (r) was used to analyze the association between variables. The level of statistical significance was set at P<0.05.
Results
Demographic Characteristics and Obstetric Profile of the Study Population
The study enrolled 60 pregnant women with a history of recurrent miscarriage. The intervention and control groups were similar in terms of demographic characteristics and obstetric profile including age, educational level, occupation, gravidity, number of miscarriages, and gestational age in weeks (Table 1). The mean ages (±SD) of the control and intervention groups were 32.7±4.46 and 32.00±4.49 years, respectively. About half (53.3%) of the control group and two-thirds (66.7%) of the intervention group had secondary school education (diploma); and 46.7% and 40%, respectively, held jobs but were on sick leave or hospitalized during the pregnancy because of their history of recurrent miscarriage. The duration of marriage ranged from 6–10 years in 40% of study participants; 56.7% of the control group vs 53.3% of the intervention group had previously been pregnant between 4 and 6 times with almost the same number of miscarriages; and 23.3% and 20%, respectively, were at a gestational age of 17–24 weeks during the study period. There were no statistically significant differences in demographic variables between the 2 groups.
 |
Table 1 Demographic Characteristics and Obstetric Profile of the Study Population |
There were statistical significant associations for the intervention group after the program between stress and age (P=0.008), education level (P=0.001), occupation (P=0.022), gravidity (P=0.047), and number of full-term pregnancies (P<0.001), but no relationship between depression or anxiety and demographic characteristics.
Effect of the Happiness Counseling Program on Stress, Anxiety, and Stress
A significant positive correlation was observed between depression and stress in the study population (r=0.457, P=0.000). There were statistically significant differences in the rates of depression, anxiety, and stress between the intervention and control groups before and after the counseling program (Table 2). Prior to the first counseling session, 56.7% and 73.3% of patients in the intervention and control groups, respectively, had severe depression (P=0.575). After the program, there was a significant decrease in the rate of severe depression in the intervention group (6.7%) but no change in the control group (56.7%) (P<0.001 was between groups). The same trends were observed for anxiety and stress levels. Before the program, 66.7% of patients in the intervention group and 63.3% in the control group had severe anxiety, with no significant difference between the 2 groups (P>0.05). However, after the program, the percentage of patients with severe anxiety decreased in the intervention group (30.0%) but not in the control group (66.7%), with a significant difference between the groups (P=0.012). Before the program, 60.0% of patients in the intervention group and 63.3% of those in the control group had severe stress (P=0.264); after the program, the rate of severe stress decreased in the intervention group (13.3%) but there was no change in the control group (60.0%) (P<0.001 between groups).
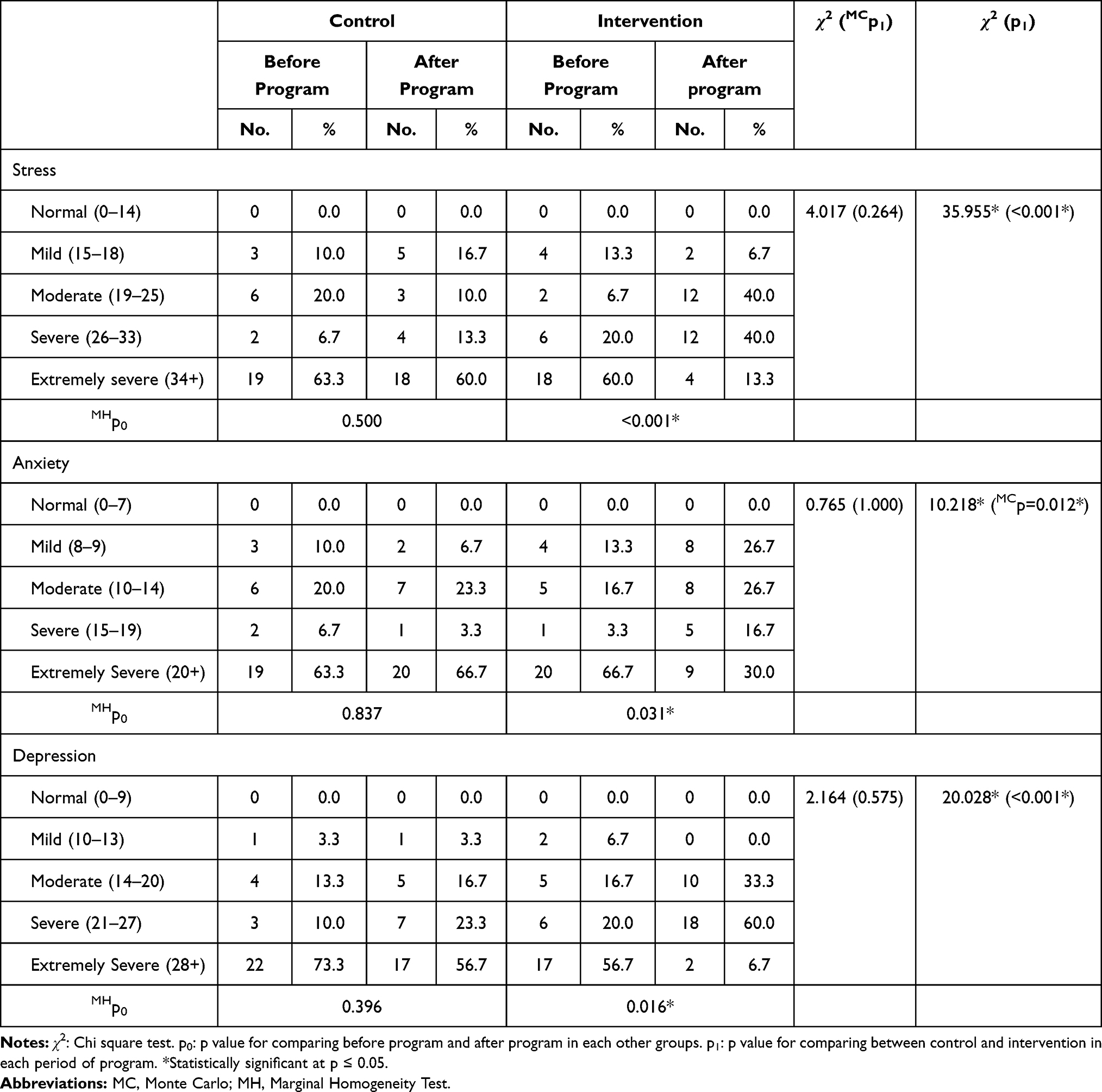 |
Table 2 Mean Scores of Depression, Anxiety, and Stress in the Intervention and Control Groups Before and 1 Month After Psychological Intervention (Happiness Counseling Program) |
Pre and post intervention DASS-21 scores were compared in the intervention and control groups (Table 3). The mean depression score decreased after the program in the intervention group (pre: 29.70±10.48 vs post: 21.37±3.50) whereas no difference was observed in the control group (pre: 34.30±9.85 vs post: 30.80±9.13). Similarly, the mean anxiety score (pre: 30.0±14.11 vs post: 15.30±6.04) and mean stress score (pre: 35.13±9.59 vs post: 24.0±3.32) decreased in the intervention group but not in the control group (pre: 29.13±13.80 vs post: 29.60±13.13 and pre: 33.60±9.78 vs post: 32.97±9.10, respectively). The differences in mean post-intervention depression, anxiety, and stress scores between the intervention and control groups were statistically significant (P<0.001).
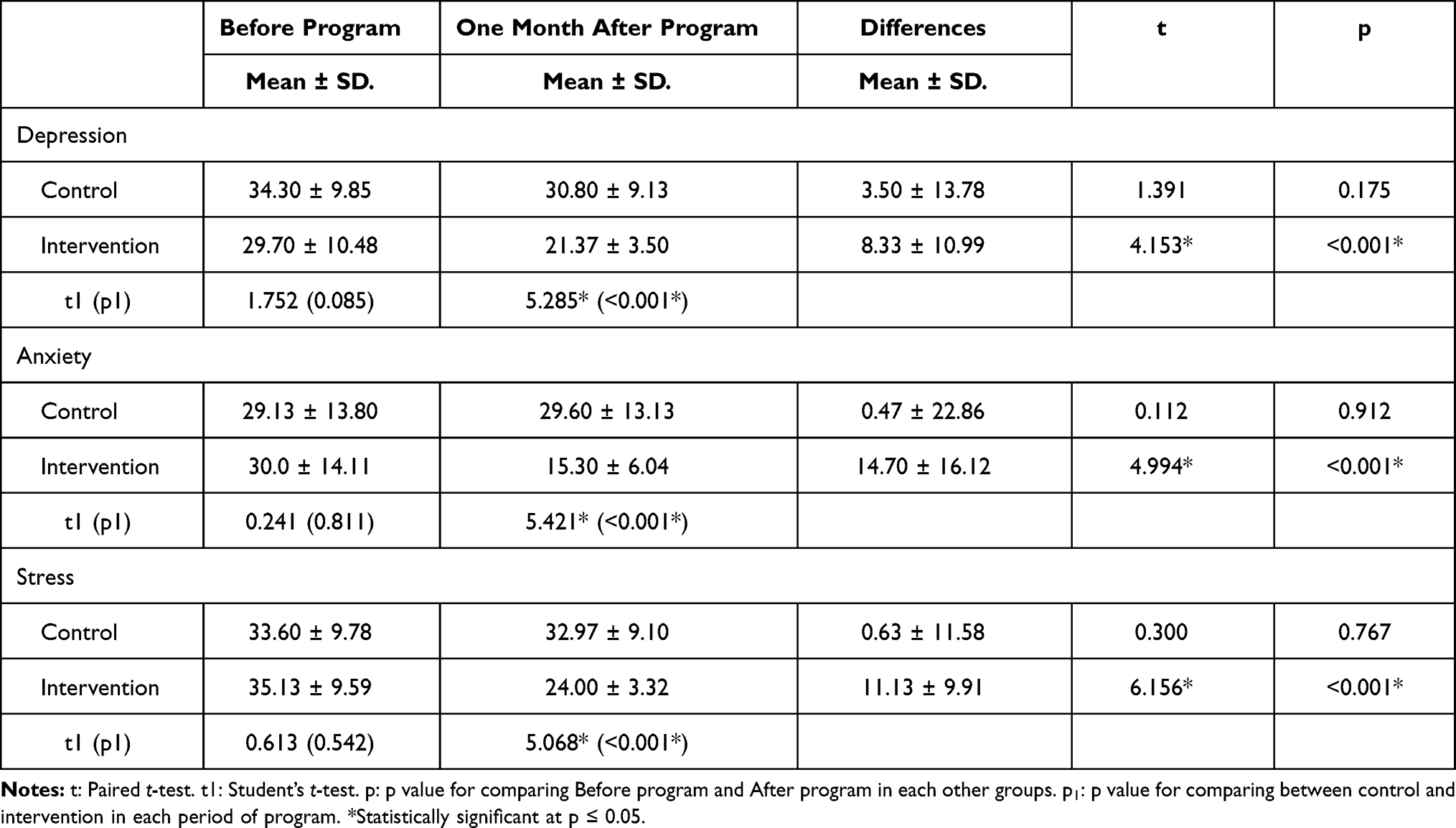 |
Table 3 Mean DASS-21 Scores of the Intervention and Control Groups Before and After Participation in the Happiness Counseling Program |
Discussion
The current study aimed to determine evaluated the effectiveness of happiness counseling on depression, anxiety, and stress in pregnant women with a history of recurrent miscarriage. The findings show that mean depression, anxiety, and stress scores were decreased in the intervention group and differed significantly from those in the control group 1 month after the intervention. These results indicate that psychological interventions during pregnancy can improve the mental health status of women who have previously experienced multiple miscarriages. Our results are in agreement with a previous study of women who had a history of recurrent miscarriage that found statistically significant differences in depression and anxiety levels between the intervention and control groups 1 month after the intervention (P<0.001).4 Another study demonstrated that counseling decreased anxiety within 3 months of a psychological intervention in women who had experienced a miscarriage.15 Women with postpartum depression showed a significant decrease in mean depression scores 2 months after participating in a happiness program.11 Others have demonstrated that happiness training reduced mean depression, anxiety, and stress scores in hemodialysis patients16 and decreased depression in older women.17 Additionally, providing psychological support to women who had undergone abortion improved their quality of life.18
Women with recurrent miscarriages experience higher rates of depression, anxiety, and stress compared to their spouses and women in the general population.19 A stepwise multiple regression analysis of key predictors of depressive symptoms in women of childbearing age showed that 62.9% of the variance could be explained by stress, anxiety, and history of recurrent miscarriage. In the present study, there was a strong correlation between depression and anxiety levels in women with recurrent miscarriage. It is possible that the women had difficulty in recognizing the feelings that they experienced, and the fear that they might never have a child may have led to arguments with their spouse, causing additional stress to already fragile marriages. A significant association between miscarriage and depression has been reported,20 and pregnant women with a history of miscarriage are at higher risk of anxiety and depression. One study investigating the psychological state of women in the first year after a miscarriage found that the rate of depression was 26.8% immediately after the miscarriage, 18.4% at 3 months, 16.4% at 6 months, and 9.3% at 12 months without any psychological intervention and.21
Psychological support following spontaneous abortion is important; especially for women who wish to become pregnant within 1 year of the miscarriage.6 Education and counseling were found to be highly effective in reducing post abortion psychological complications.22 Cognitive-behavioral stress management was also shown to increase happiness in women with infertility,23 while a happiness program similar to the one used in the current study minimized stress in the mothers of children with cleft lip and palate.10 Thus, happiness programs can significantly reduce depression, anxiety, and stress symptoms in a variety of patient populations.
Conclusion
A limitation of this study is that the underlying causes of recurrent miscarriage were not considered in the analysis. Nonetheless, our results demonstrate that the happiness counseling program is an effective, low-cost, and noninvasive strategy for reducing depression, anxiety, and stress in women with a history of recurrent miscarriage, thereby improving their mental health and overall wellbeing.
Recommendations
- In-service training and continuing education programs related to happiness counseling should be provided to all nurses working in the maternity and mental health units of hospitals.
- Further studies are needed to evaluate the effect of family responses, attitudes, and behaviors on social adaptation in patients with recurrent miscarriage.
- Additional follow-up is needed to assess the long-term adaptation of patients with recurrent miscarriage who participated in the happiness counseling program.
Data Sharing Statement
Data in this article are available from the corresponding author upon request.
Acknowledgments
The authors thank the study participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. San Lazaro Campillo I, Meaney S, McNamara K, O’Donoghue K. Psychological and support interventions to reduce levels of stress, anxiety or depression on women’s subsequent pregnancy with a history of miscarriage: an empty systematic review. BMJ Open. 2017;7(9):e017802. doi:10.1136/bmjopen-2017-017802
2. Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013;99(1):63. doi:10.1016/j.fertnstert.2012.09.023
3. Nakano Y, Akechi T, Furukawa TA, Sugiura-Ogasawara M. Cognitive behavior therapy for psychological distress in patients with recurrent miscarriage. Psychol Res Behav Manag. 2013;6:37–43. doi:10.2147/PRBM.S44327
4. Khodakarami B, Mafakheri B, Shobeiri F, Soltanian A, Mohagheghi H. The effect of fordyce happiness cognitive- behavioral counseling on the anxiety and depression of women with spontaneous miscarriage. J Pharm Sci Res. 2017;9(12):2335–2341.
5. Bicking Kinsey C, Baptiste-Roberts K, Zhu J, Kjerulff KH. Effect of previous miscarriage on depressive symptoms during subsequent pregnancy and postpartum in the first baby study. Matern Child Health J. 2015;19(2):391–400. doi:10.1007/s10995-014-1521-0
6. Haghparast E, Faramarzi M, Hassanzadeh R. Psychiatric symptoms and pregnancy distress in subsequent pregnancy after spontaneous abortion history. Pak J Med Sci. 2016;32(5):1097–1101. doi:10.12669/pjms.325.10909
7. Qu F, Wu Y, Zhu Y, et al. The association between psychological stress and miscarriage: a systematic review and meta-analysis. Sci Rep. 2017;7:1731. doi:10.1038/s41598-017-01792-3
8. Tavoli Z, Mohammadi M, Tavoli A, et al. Quality of life and psychological distress in women with recurrent miscarriage: a comparative study. Health Qual Life Outcomes. 2018;16:150. doi:10.1186/s12955-018-0982-z
9. Kicia M, Skurzak A, Wiktor K, Iwanowicz-Palus G, Wiktor H. Anxiety and stress in miscarriage. Pol J Public Health. 2015;125(3):162–165. doi:10.1515/pjph-2015-0046
10. Hemati Z, Abbasi S, Paki S, Kiani D. The effect of happiness training based on fordyce model on perceived stress in the mothers of children with cleft lip and palate. J Caring Sci. 2017;6(2):173–181. doi:10.15171/jcs.2017.017
11. Rabiei L, Mazaheri MA, Masoudi R, Hasheminia SA. Fordyce happiness program and postpartum depression. J Res Med Sci. 2014;19(3):251–256.
12. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety & Stress Scales.
13. Norton PJ. Depression anxiety and stress scales (DASS-21): psychometric analysis across four racial groups. Anxiety Stress Coping. 2007;20:3, 253–265. doi:10.1080/10615800701309279
14. Henry JD, Crawford JR. The short-form version of the depression anxiety stress scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(Pt 2):227–239. PMID: 16004657. doi:10.1348/014466505X29657.
15. Moradi MM, Jahdi F, Fatemi NS, Montazeri A. The effect of counseling on anxiety levels of women with spontaneous abortion. Payesh. 2016;15(2):174–179.
16. Mehrabi Y, Ghazavi Z, Shahgholian N. Effect of fordyce’s happiness program on stress, anxiety, and depression among the patients undergoing hemodialysis. Iranian J Nurs Midwifery Res. 2017;22:1904.
17. Nassab ZK, Allahvirdiyani K. The effects of fordyce’s happiness training on decreasing depression among elderly women. Procedia Soc Behav Sci. 2013;84:501–503. doi:10.1016/j.sbspro.2013.06.592
18. Rahbar N, Ghorban R, Moazen S, Asl N. Association between spontaneous abortion and general health condition. Iran J Obstet Gynecol Infertil. 2010;13(1):7–12.
19. Chen SL, Chang SM, Kuo PL, Chen CH. Stress, anxiety and depression perceived by couples with recurrent miscarriage. Int J Nurs Pract. 2020;26(2):e12796. PMID: 31713284. doi:10.1111/ijn.12796.
20. Farahat TM, Alkot MM, Emam KA. Risk factors of maternal depression and anxiety in El-Fayum city. Menoufia Med J. 2015;28:65762.
21. Lok IH, Yip AS, Lee DT, Sahota D, Chung TK. A 1-year longitudinal study of psychological morbidity after miscarriage. Fertil Steril. 2010;93(6):1966–1975. PMID: 19185858. doi:10.1016/j.fertnstert.2008.12.048.
22. Gould H, Perrucci A, Barar R, Sinkford D, Foster DG. Patient education and emotional support practices in abortion care facilities in the United States. Women’s Health Issues. 2012;22(4):e359–64. PMID: 22609254. doi:10.1016/j.whi.2012.04.003.
23. Hashemi F, Ali Poor A, Feili A. The effectiveness of cognitive behavioral stress management therapy on happiness among infertile women. Armaghane Danesh. 2013;18(9):678–686.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.