")
Back to Journals » International Journal of Women's Health » Volume 14
Effect of Grand Multiparity on the Adverse Birth Outcome: A Hospital-Based Prospective Cohort Study in Sidama Region, Ethiopia
Authors Dasa TT , Okunlola MA, Dessie Y
Received 24 November 2021
Accepted for publication 3 March 2022
Published 10 March 2022 Volume 2022:14 Pages 363—372
DOI https://doi.org/10.2147/IJWH.S350991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Tamirat Tesfaye Dasa,1,2 Michael A Okunlola,3 Yadeta Dessie4
1Department of Reproductive Health Sciences, Life and Earth Sciences Institute (Including Agriculture and Health), Pan African University, Ibadan, Nigeria; 2Department of Midwifery, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 3Department of Obstetrics and Gynaecology, College of Medicine, University College Hospital, University of Ibadan, Ibadan, Nigeria; 4School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Tamirat Tesfaye Dasa, Department of Midwifery, College of Medicine and Health Sciences, Hawassa University, P.O. Box 235, Hawassa, Ethiopia, Tel +251 938611577, Email [email protected]
Background: Adverse birth outcome is associated with grand multiparity and is still a major public health problem in developing countries. There is limited information that investigates the effect of grand multiparity on perinatal outcomes in a prospective follow-up design in Ethiopia. Therefore, this study was aimed to investigate the effect of grand multiparity on the occurrence of adverse perinatal outcomes in the Sidama Region of Ethiopia.
Methods: We conducted a prospective follow-up study among 837 women who gave birth in selected public hospitals of the Sidama Region from January 1 to August 31, 2021. Data were collected using a structured questionnaire and medical record review. A modified Poisson regression model with robust standard errors was applied to estimate the adjusted risk ratio and its 95% CI of the risk factors for adverse perinatal outcomes to examine the association of the multi-parities with the adverse birth outcome. STATA Version 14 was used for analysis.
Results: The overall cumulative incidence of adverse perinatal outcomes was 33% (95% CI: 29.9%, 36.4%). After adjusted for confounders, women with grand multiparity gave birth to babies with a higher risk of stillbirth (ARR = 1.6; 95% CI: 1.01– 2.51), macrosomia (ARR = 1.6; 95% CI: 1.23– 2.07), and preterm birth (ARR = 1.3; 95% CI: 1.1– 1.66) compared to their counterparts.
Conclusion: High incidences of adverse perinatal outcomes occurred among women with grand multiparity. We recommend that the region and districts health bureau should give close monitoring for pregnant women with high parity throughout their prenatal, intrapartum, and postpartum periods.
Keywords: birth complication, parity, fetal abnormality, cohort, Sidama, Ethiopia
Background
Grand multiparity is a condition when a woman has at least five deliveries at gestational age greater than or equal to 20 weeks.1–3 In many developed countries, grand multiparity is becoming less of a concern with a low prevalence of 2–4% whereas it is still a public health issue of great concern in developing countries and is a high prevalence of 19%.4–6
Low-and-middle-income countries including Ethiopia’s grand multiparity have still relatively high perinatal outcomes complications compared to high-income countries.7–9 Evidence has shown that grand multiparity increases the incidence of medical and obstetric complications such as anemia, birth asphyxia, preterm birth, low birth weight, macrosomia, low APGAR scores, stillbirth, and a high perinatal mortality rate.10–13 With this connection, grand multipara is associated with higher risks factors of medical and obstetric complications for mothers and fetuses.4,7,14–16
In different studies conducted in developing countries, adverse perinatal outcomes are significantly associated with grand multiparity compared with multiparity.1,4,7,10,15,17–26 The majority of the studies carried out in developing countries, including Ethiopia, implemented incomplete registration of perinatal data with limited variables. There were also limited studies conducted to assess the adverse perinatal outcomes of grand multiparity in Ethiopia. Moreover, there is limited data about the impact of grand multiparity on perinatal outcomes in the study area. Therefore, this study aimed to investigate adverse perinatal outcomes of grand multiparity in selected public hospitals in the Sidama Regional State of Ethiopia.
Methods and Materials
Study Settings, Design, and Period
The study was conducted in Sidama Regional State, Ethiopia. It is situated in the southern part of the country, which is 273 kilometers away from Addis Ababa, the capital city of Ethiopia. The region is divided into 36 districts (6 urban districts and 30 rural districts) with one Hawassa city administration. Hawassa remains the capital city of the region. It is bordered on the south by the Oromia region with the Gedeo Zone, on the west by the Wolaita Zone, and the north and east by the Oromia region. The Sidama people number 8.8 million (4.01% of the national population). The region has 123 health centers and 17 hospitals (one comprehensive referral hospital, four general hospitals, and 12 primary hospitals).
A prospective cohort study was conducted in five public hospitals which are designated as general and referral hospitals providing specialized care for both the mother and newborn and having an obstetric and neonatal intensive care unit (NICU). The study was conducted from January 1 to August 31, 2021.
Cohort Selection, Recruitment, and Exclusions
All multiparity and grand multiparity for childbirth in the region was a source population. Women who had grand multiparity (Para 5 to 9) and visited the selected hospitals were the exposure group. Hence, all women were admitted for delivery to the participating hospitals during the study period. Women who had multiparity (Para 2 to 4) were enrolled as a non-exposed group. The controls were selected based on the five age-interval categories and delivered on the same day of the exposure. In addition, those women with grand multiparity who delivered at another facility (outside the included hospitals) were also excluded as it was difficult to know the perinatal outcomes. We have also excluded women with multiple pregnancies, Primigravida, chronic illness related to pregnancy, great grand multiparity (women who give birth more than ten), women who are mentally or critically ill and unable to communicate were excluded from the study because of the adverse perinatal outcome more occurred. Also, women who would give birth at home were not captured by this study.
Sample Size Determination and Sampling Procedure
The sample size was calculated by using a double population proportion formula using EPI Info version 7 STAT CALC software cohort study as described by Fleiss with continuity correction to estimate the sample size.27 The parameters that were used to estimate the sample size were: confidence level of 95%, power of 80%, exposed to the non-exposed ratio of 1:2, expected incidence of the outcome in the non-exposed group (24%),16 and incidence of preterm among the exposed group (35%).16 It was estimated based on one study in Pakistan taking incidence of preterm among exposed and non-exposed women to grand multiparity. Adding a 10% loss rate, the final sample size required for the study was 279 exposed and 558 non-exposed women: a total of 837 women were included in this study.
The Sidama region has 17 hospitals (12 primaries, 4 general, and 1 comprehensive referral hospital). Out of the 17 hospitals, 5 (30%) hospitals were selected purposively which provided full packages of maternal and newborn services in the region. That is why it was selected these hospitals as the study area. For each hospital, the sample was allocated an appropriate sample size by using the probability proportional to sample size considering hospital clients’ follow-up from last year’s delivery admission reports. The study participants were included in consecutive sampling techniques until the anticipated sample size was obtained.
Data Collection Tools and Procedures
The data collection tools were developed in the English language, then translated into the local language (Amharic) by language experts. The questionnaires were prepared following a thorough review of different kinds of published literature.7,12,13,17,18,28–40 The interview questionnaires of participants contain the client’s information, socio-demographic factors, obstetrics, and reproductive health history characteristics, maternal health services use during a current and previous pregnancy, nutritional status of women, and adverse perinatal outcome parts. The data were collected from the admission to labour and delivery up to maternal wards. Qualified and trained health professionals were recruited as data collectors and supervisors. Five days of training were given before starting the actual data collection. After the training, a pre-test was conducted to ensure the consistency of tools on 5% of the sample size out of the actual data collection site.
Outcome Variables and Measures
The primary outcome of interest was adverse perinatal outcomes and was categorized as the absence or presence of adverse perinatal outcomes. Adverse perinatal outcomes or complications were defined as the presence of either or more of the following: stillbirth, low birth weight, macrosomia, preterm, admission to neonatal intensive care unit (ICU), and first-minute birth asphyxia in women giving birth more than five or more and less than five births. Stillbirth was defined as a newborn baby with no signs of life at or after 28 completed weeks of pregnancy.41,42 Low birth weight was defined by the world health organization as a newborn birth weight of fewer than 2500 grams regardless of gestational age.43 Preterm birth is a baby born alive before 37 completed weeks of gestation but after 28 weeks of gestation.44 Gestational age was determined based on the last menstrual period and ultrasound measures were taken when prediction by last menstrual period was not possible. Birth asphyxia is defined as failure to initiate and sustain spontaneous breathing at birth.45,46 To grade, the severity of perinatal asphyxia in newborns, the Apgar score was used. A score below 7 at the first minute of life was considered as having first-and fifth-minute birth asphyxia.47
Potential Confounding Variables
Data were collected at baseline and postnatal on several risk factors through labour and delivery, including maternal characteristics and potential confounding variables. Also, detailed pregnancy history was gathered, including pre-existing medical conditions. Some of the included potential confounding variables were socio-demographic characteristics: maternal age, religion, ethnicity, household wealth status, education of respondents, education of husband and occupation; obstetrics and some medical factors: history of preterm birth, history of stillbirth, and unplanned pregnancy. Mid-Upper Arm Circumference (MUAC), body mass index, and sex of the newborn.
Data Analysis
Double data was entered using EpiData version 3.02 software. Entered data was exported to STATA 14 version software for analysis. Data were cleaned for missing values and inconsistencies. Descriptive statistics like frequencies table and summary indices were used to describe the study population. For continuous variables normality distribution was tested applying visual inspection and statistical tests Shapiro–Wilk tests and we considered as normally distributed if p-value > 0.05. Categorical data were compared using the Chi-square test, and an independent sample t-test was applied for the comparison of the mean difference of continuous variables between both groups. As the occurrence of adverse perinatal outcomes was rare, it was compulsory to estimate risk using an appropriate model for rare outcomes. Therefore, we estimated relative risk using a Generalized Linear Model (GLM) with an identity log and binomial link function (log-binomial). We encountered a convergence problem by using the log-binomial approach and therefore changed this model to modified Poisson regression. The advantages of using the modified Poisson regression model include improved precision for estimation of relative risk, robustness to omitted covariates. All variables risk factors with outcomes of interest in bivariable analysis at p-value ≤0.2 were considered as candidates for the multivariable Poisson regression model. In the final model, multivariable Poisson regression analysis was performed to investigate the risk factors between grand multiparity and concerned adverse perinatal outcomes. The risk factors of grand multiparity the regression model was reported using an adjusted risk ratio (ARR) with a 95% confidence interval (CI). Statistical significance was declared when the P-value was less than 0.05. The occurrence of multicollinearity among explanatory variables was ensured using the Variance Inflation Factor at a cut-off point of 1048 and there was no multi-collinearity.
Ethical Considerations
The research was submitted to Pan Africa University Life and Earth Sciences Institute, University of Ibadan, and the University of the Ibadan/University College Hospital, Ibadan Ethics Committee for approval (Ethics committee assigned number_/EC/20/0439). Following the approval, an official letter of cooperation was written to concerned bodies in the data collection areas. Permission was obtained from the Sidama Regional Health Bureau. Written informed consent was obtained from each study participant, before data collection procedures. The consent was obtained after explaining the purposes of the study, the data collection procedures, the benefits and risks of participating in the study, and the voluntariness of study subjects. The study conforms to the provisions of the Declaration of Helsinki.49
Results
Cohort Recruitment and Follow-Up
In this study, 837 women were recruited of whom 18 were not included due to loss to follow-up, and perinatal outcomes were not registered properly. Finally, a total of 820 participants were followed up to admission to the labour ward, delivery, and the postnatal period. During the follow up four women refused to participate in the study due to certain reasons after being involved in the study cohort leaving 816 study subjects giving a response rate of 97.5%.
Socio-Demographic and Obstetrics Characteristics of Study Participants
The mean (± standard deviation (SD) age was 32.8 ± 3.8 among the grand multipara vs 27.2 ± 3.8 years among multiparity, p < 0.001). The majority of grand multiparous women (72.2%) and multiparous women (58.5%) were aged between 25–34 years. Slightly more than two-thirds (67.5%) of the multiparous women and (49.6%) of the grand multiparous women were urban dwellers. Nearly one-fourth (22.1%) of the multiparous women and (50%) of the grand multiparous women were illiterate. Close to two-thirds (63.1%) of the multiparous women and more than three-fourths (75.7%) of the grand multiparous women were housewives. The number of antenatal care visits had more than four times (42.5% vs 31.7%, χ2=8.1, P=0.005) among multiparous and grand multiparous women, respectively. There was no statistically significant difference between the grand multiparous and multiparous women in the body mass index (Table 1).
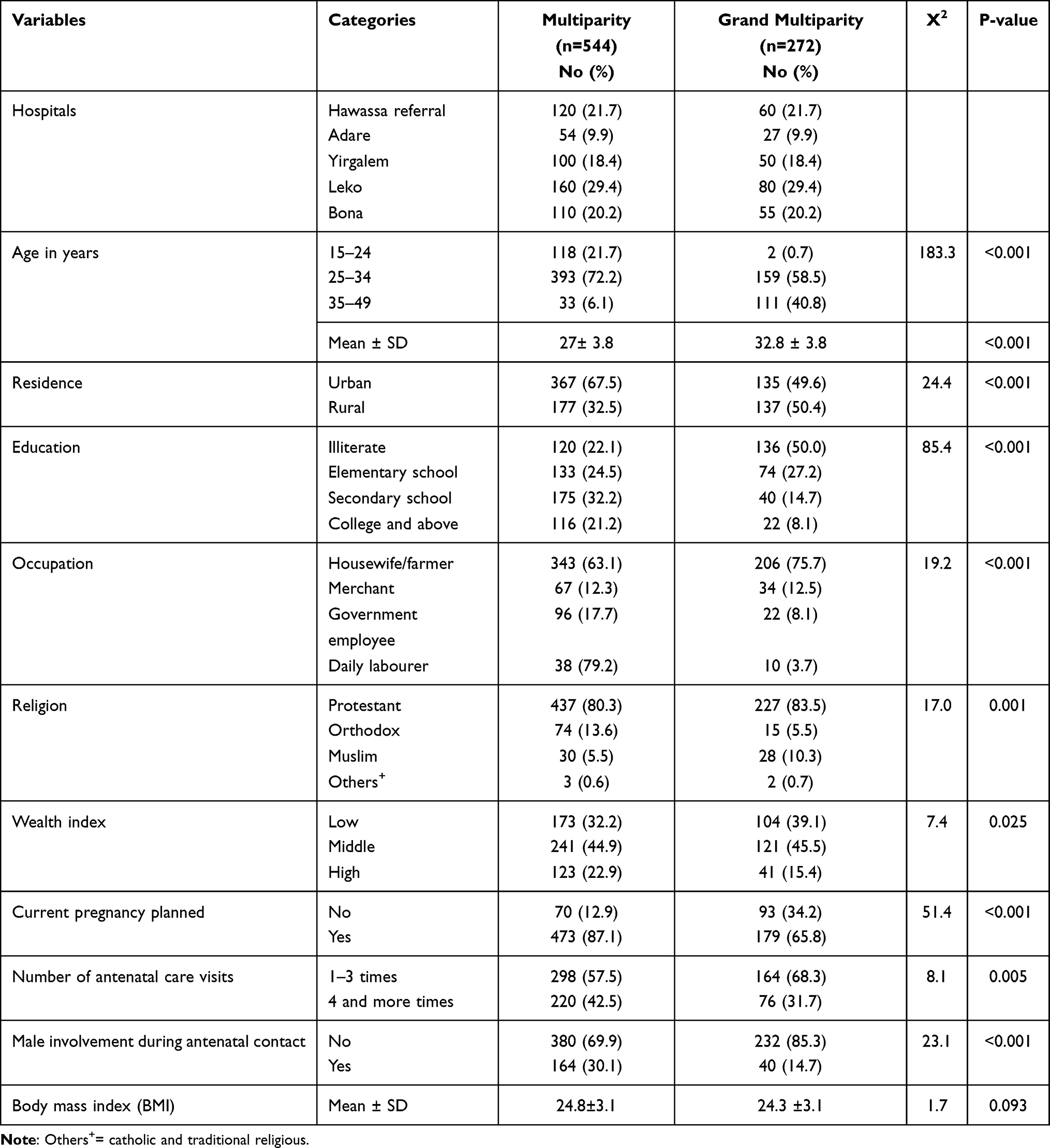 |
Table 1 Selected Socio-Demographic and Obstetrics Characteristics with Grand Multiparity in Sidama Regional State of Ethiopia, 2021 |
Incidence of Adverse Perinatal Outcomes of Study Participants
The overall cumulative incidence of adverse perinatal outcomes was 33% (95% CI: 29.9%, 36.4%). The incidence of adverse perinatal outcomes was 40.8% (95% CI: 35–47) among the grand multiparity and 30.3% (95% CI: 27–34) among the multiparity. As general, 50 resulted in stillbirth (6.1%; 95% CI: 4.6–8.0), 134 in low birth weight (16.4%; 95% CI: 14.0–19.1), 88 in admission to NICU (10.8%; 95% CI: 8.7–13.1), 72 in Apgar score < 7 at 5 minutes (8.8%; 95% CI: 7–11) and 154 resulted in preterm births (18.9%; 95% CI:16.2–21.7) in cohort. Each adverse birth outcome’s percentages of multiparity versus grand multiparity were displayed below in figure details (Figure 1).
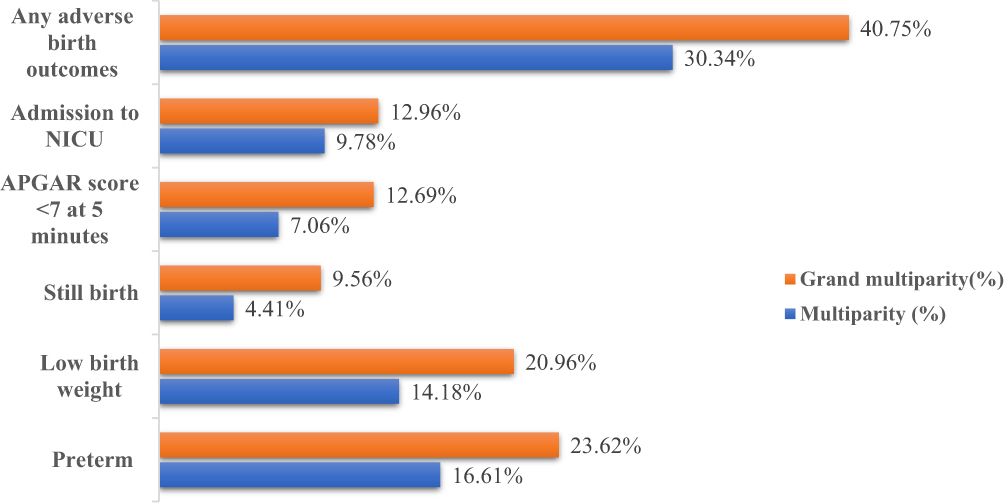 |
Figure 1 Adverse perinatal outcomes among grand multiparity (n = 272) and multiparity (n = 544) in selected public hospitals in the Sidama Regional State, Ethiopia 2021. |
Association Between Parity and Perinatal Outcomes
The Chi-square test for parity and perinatal outcomes is shown in Table 2. The incidence of preterm birth was higher among babies born from women with grand multiparous than multiparous women (23.6% vs 16.4%, P=0.02). Likewise, low birth weight was higher among women with grand multiparous than multiparous women (21.0% vs 14.2%, p=0.014). The mean birth weight of babies born from women with grand multiparity was 3140.3 grams and multiparity was 3165.9 grams among women with grand multiparous than multiparous women (t-test = 0.53, P-value=0.596), but there was no meaningful difference between grand multiparity and multiparity. Furthermore, 9.6% of newborn babies from women with grand multiparity and 4.4% from multiparity were stillbirth (P<0.001). Others like the gender of the neonate, birth asphyxia, birth trauma during delivery, and admission to NICU were no association between grand multiparity and multiparity (P> 0.05) (Table 2).
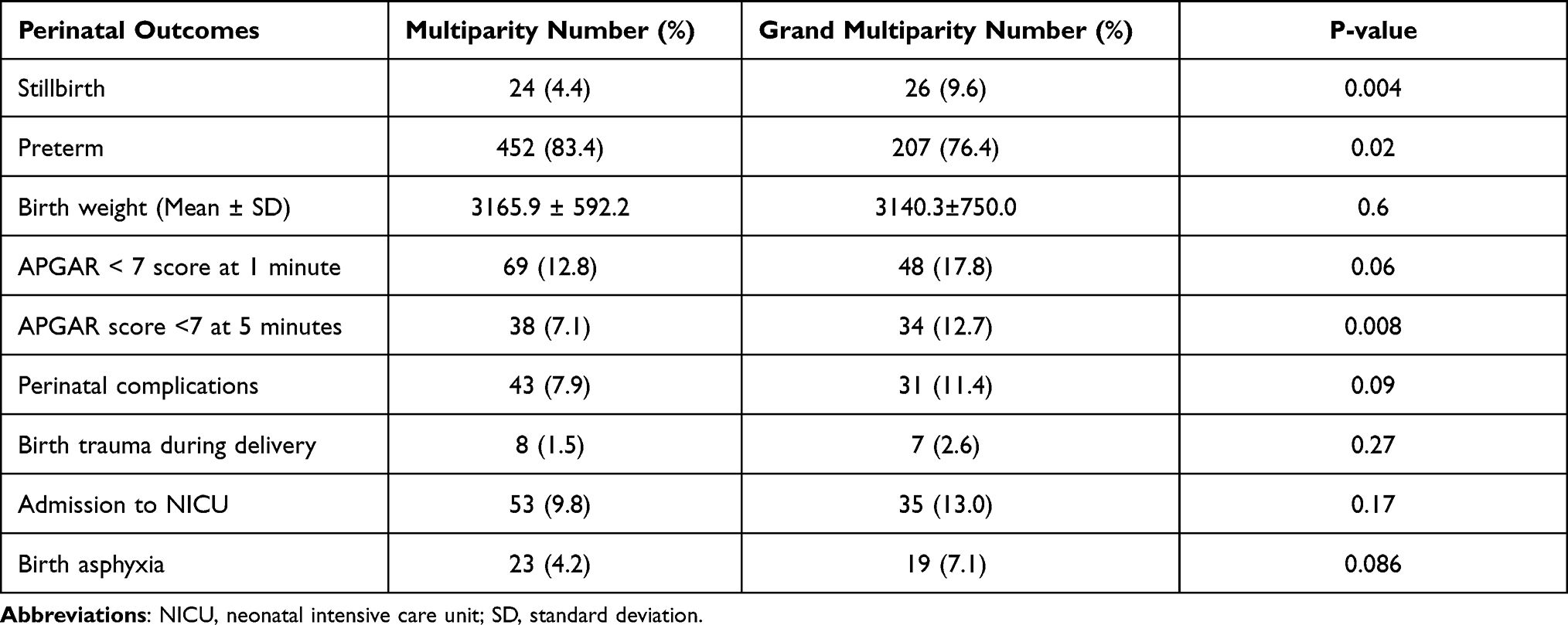 |
Table 2 Association Between Parity and Perinatal Birth Outcomes Among Study Participants in Sidama Region of Ethiopia, 2021 |
Risk of Adverse Perinatal Outcomes Associated with Grand Multiparous Women
In multivariate Poisson regression modelling, the risk of having stillbirth was significantly increased in women with grand multiparity compared to multiparity adjusted relative risk (aRR) = 1.6; 95% CI: 1.01,2.51), macrosomia (aRR = 1.6; 95% CI: 1.23–2.07), preterm delivery (aRR = 1.35% CI: 1.1–1.66) (Table 3).
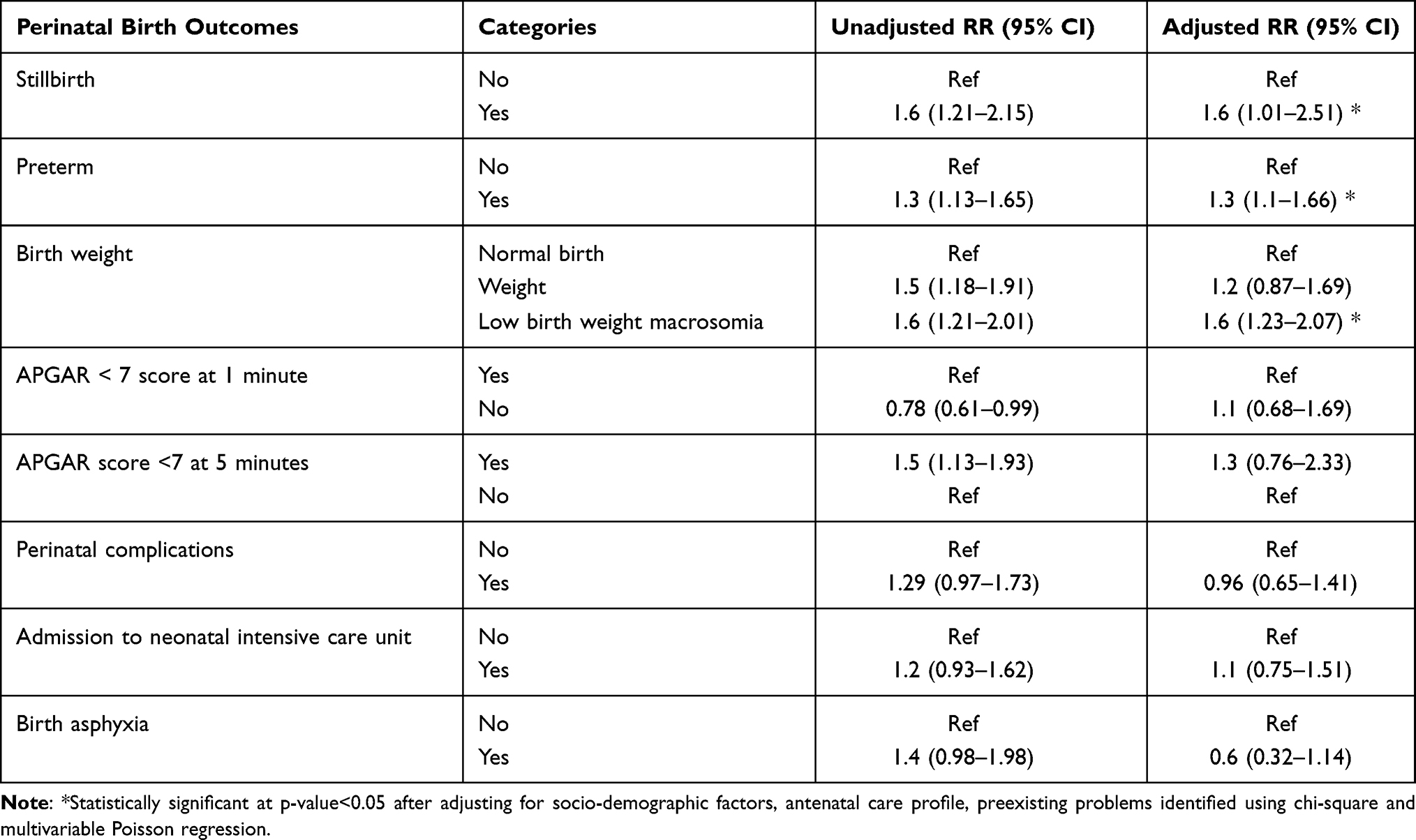 |
Table 3 Risk of Adverse Perinatal Outcomes Associated with Grand Multiparous Women in Public General Hospitals in Sidama Region of Ethiopia, 2021 |
Discussion
This study compared potential adverse perinatal outcomes between the grand multipara women and those not. The overall cumulative incidence of adverse perinatal outcomes was 33% (95% CI: 29.9%, 36.4%). The cumulative incidence of adverse perinatal outcomes was 40.8% (95% CI: 35–47) among grand multiparous compared to their counterparts 30.3% (95% CI: 27–34) which was different (P-value=0.003). In this finding, many perinatal complications were shown to be higher in grand multiparous women than multiparas (stillbirth, preterm, big baby, and Apgar score <7 at 5 minutes, P<0.05). In the present study, we found that the cumulative incidence of adverse perinatal outcomes was significantly higher in grand multiparous women than multiparous women. This finding is consistent with the previous studies which were conducted in Iraq, Jordan, Saudi Arabia, and Ethiopia.14,17,22,30 Conversely, there were no statistically significant differences in adverse perinatal outcomes between grand multiparous and multiparous women as the studies conducted in rural Cameroon and Ethiopia.2,12 The possible explanation might be due to the quality of health care, trained health personnel, and application of different standard protocols for proper management of health care services from pregnancy to delivery.2
The present study revealed that preterm birth was significantly higher among grand multiparous (23.6%). This finding was comparable to the studies conducted in Ethiopia (19%), Nigeria (25%), and Bangladesh (23%).22,25,50 Also, the finding showed that the risk of preterm birth was higher with grand multiparity. This finding is similar to the study conducted in Tanzania.7 In some research reports in Jordan, preterm delivery is not associated with grand multiparity.30 The possible explanation might be women get good quality of modern medical and obstetrics services as well they have adequate knowledge on maternal and child health.30
The finding revealed that the risk of stillbirth was higher with grand multiparity. This finding is similar to the study conducted in Mali33 and Tanzania.7 However, in another study, grand multiparity was not a risk factor for stillbirth the study was done in Nigeria.51 The possible explanation might be differences across studies related to the utilization of antenatal care services across countries.52,53 The other explanation is that most pregnant women arrived late having an already intrauterine death or with hypoxic babies during delivery.15
Regarding birth weight, the risk of macrosomia was significantly higher in grand multiparity than multiparity. This finding is similar to the study conducted in Kano, Nigeria,54 Oman,55 Mali,33 and Saudi Arabia.26
In terms of immediate newborn complications, this study showed that there was no statistical difference in the two groups as regards the Apgar< 7 score at 1 minute, birth trauma, birth asphyxia, admission to neonatal intensive care unit, perinatal complication, and sex of newborn.
The strength of our study was its prospective nature, control of confounding factors, and low loss to follow-up. Yet, limitations observed in this study include the follow-up periods were not included after perinatal periods, and for some cases, gestational age was reported subjectively rather than objectively.
Conclusions
In this study, high incidences of adverse perinatal outcomes occurred among women with grand multiparity. Also, compared to women of low parity, grand multiparous women are at higher risk of having stillbirths, preterm delivery, and big babies. We recommend that all the stakeholders should give close monitoring for pregnant women with high parity throughout their prenatal, intrapartum, and postpartum periods. Further, we recommend that the researchers conduct studies about the effect as early as start to follow up grand multigravida on the adverse perinatal outcomes.
Abbreviations
ANC, antenatal care; Apgar score, appearance, pulse, grimace, activity, and respiration score; ARR, adjusted relative risk; LBW, low birth weight; NICU, neonatal intensive care unit; CRR, crude relative risk; SD, standard deviation; WHO, World Health Organization.
Data Sharing Statement
The datasets used during this study are available from the principal investigator on reasonable request.
Acknowledgments
We would like to thank the Pan African University of Life and Earth Sciences Institute, the African Union for financial support, and the University of Ibadan for hosting this Ph.D. program. Our appreciation also goes to data collectors and supervisors for their diligence during data collection to obtain necessary information. Our special thanks also go to participants who generously shared their thoughts and feelings despite other commitments. In addition, our thanks go to the Sidama regional health bureau and administrators of all hospitals included in this study for giving us the necessary background information to conduct this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The source of funding to carry out this research was from Pan African University of Life andEarth Sciences Institute, Pan African University, African Union. The funding organization had no role in the design of the study and collection, analysis, and interpretation of data, or in writing the manuscript; this was the role of the authors.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Njoku CO, Abeshi SE, Emechebe CI. Grand Multiparity: obstetric outcome in comparison with multiparous women in a developing country. Open J Obstet Gynecol. 2017;7(7):707. doi:10.4236/ojog.2017.77071
2. Ajong AB, Agbor VN, Simo LP, Noubiap JJ, Njim T. Grand multiparity in rural Cameroon: prevalence and adverse maternal and fetal delivery outcomes. BMC Pregnancy Childbirth. 2019;19(1):1–7. doi:10.1186/s12884-019-2370-z
3. Aliyu MH, Jolly PE, Ehiri JE, Salihu HM. High parity and adverse birth outcomes: exploring the maze. Birth. 2005;32(1):45–59. doi:10.1111/j.0730-7659.2005.00344.x
4. Mgaya AH, Massawe SN, Kidanto HL, Mgaya HN. Grand multiparity: is it still a risk in pregnancy? BMC Pregnancy Childbirth. 2013;13(1):241. doi:10.1186/1471-2393-13-241
5. World Health Organization. WHO report. Geneva: World Health Organization; 2004. Available from:. http://www.who.int/whr/2004/annex/country/can/en/.
6. Hoque M, Hoque E, Kader SB. Pregnancy complications of grandmultiparity at a rural setting of South Africa; 2008.
7. Muniro Z, Tarimo CS, Mahande MJ, Maro E, Mchome B. Grand multiparity as a predictor of adverse pregnancy outcome among women who delivered at a tertiary hospital in Northern Tanzania. BMC Pregnancy Childbirth. 2019;19(1):1–8. doi:10.1186/s12884-019-2377-5
8. UNICEF. Maternal mortality fell by almost half between 1990 and 2015; 2017.
9. Abou Zahr C. Global burden of maternal death and disability. Br Med Bull. 2003;67(1):1–11. doi:10.1093/bmb/ldg015
10. Afzal A, Mahajan N, Firdous N. Pregnancy outcomes in grand multiparous patients: a hospital based study from Jammu and Kashmir, India. Int J Reprod Contracep Obstet Gynecol. 2016;5(3):788–792.
11. Singh S, Chawan J, Mangla D. A descriptive study: maternal and fetal outcome of grand multipara. Int J Reprod Contracept Obstet Gynecol. 2015;4(1):219–224.
12. Yimer NB, Tenaw Z, Gedefaw A. Pregnancy outcomes in grand multiparous women: does parity matter? A comparative study. Ethiopia J Reprod Health. 2020;12(1):11.
13. Roy I, Burande A, Choubey R. Obstetric outcome in grand multipara–a Meghalaya experience. J OBGYN. 2019;5(2):103–106. doi:10.21276/obgyn.2019.5.2.8
14. Al-Shaikh GK, Ibrahim GH, Fayed AA, Al-Mandeel H. Grand multiparity and the possible risk of adverse maternal and neonatal outcomes: a dilemma to be deciphered. BMC Pregnancy Childbirth. 2017;17(1):310. doi:10.1186/s12884-017-1508-0
15. Khatun J. Obstetrical outcome of grand multipara. J Bangladesh Coll Phys Surg. 2016;34(4):184–187. doi:10.3329/jbcps.v34i4.32407
16. Qamar A, Asif U, Qamar S. Maternal and fetal outcome in grand multipara. Pak Armed Forces Med J. 2015;65(1):135–140.
17. Alwan BA, Abdulridha AS. Maternal and fetal outcomes of labor in grand-multipara women. Indian J Public Health Res Dev. 2019;10(8):2001–2006. doi:10.5958/0976-5506.2019.02147.8
18. Alsammani MA, Jafer A, Khieri S, Ali A, Shaaeldin M. Effect of grand multiparity on pregnancy outcomes in women under 35 years of age: a comparative study. Med Arch. 2019;73(2):92–96. doi:10.5455/medarh.2019.73.92-96
19. Alhainiah MH, Abdulljabbar HS, Bukhari YA. The prevalence, the fetal and maternal outcomes in grand multiparas women. Mater Sociomed. 2018;30(2):118. doi:10.5455/msm.2018.30.118-120
20. Addah A, Ikobho E. A comparison of the pregnancy and labour outcomes between nulliparous and grand multiparous pregnancies in the Niger Delta. J Adv Med Medl Res. 2018;27(3):1–9. doi:10.9734/JAMMR/2018/42931
21. Niaz A, Noor S, Javed N. Comparison of placental abruption between multipara and grand multipara. Ann Punjab Med Coll. 2017;11(2):172–174.
22. Aragaw F, Mahtemsilllasie M, Jarso H. Grand multiparity and pregnancy related complications among women who gave birth at Jimma University specialized hospital, Jimma, Southwest Ethiopia. Gynecol Obstet. 2017;7(4):438. doi:10.4172/2161-0932.1000438
23. Sultan S, Ojha J. Grand multi parity still and obstetric challenge-a clinical study of grand multi Para in a tertiary care center. J Evol Med Dent Sci. 2013;12(39):7423–7430. doi:10.14260/jemds/1318
24. Parveen T, Iqbal T, Kausar T. Grand multiparity and its obstetrical complications at Bahawal Victoria Hospital Bahawalpur. Pak J Med Health Sci. 2014;8(3):706–708.
25. Ahmed N, Akhter S, Das T. Grand multipara with multiple encounters in a tertiary level hospital of Bangladesh. Int J Gynecol Obstet. 2015;131:E445.
26. Alsammani MA, Ahmed SR. Grand multiparity: risk factors and outcome in a tertiary hospital: a comparative study. Mater Sociomed. 2015;27(4):244. doi:10.5455/msm.2015.27.244-247
27. Fleiss JL, Levin B, Paik MC. Statistical Methods for Rates and Proportions. john wiley & sons; 2013.
28. Central Statistical Agency (CSA). [Ethiopia] and ICF, Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF., In the DHS Program ICF; 2016.
29. Al-Obaidly S, Khaldi HM, Emad N, Al-Ibrahim A, Bayo A. Review of pregnancy outcomes in grand multiparous Qatari women: a retrospective cohort study. BJOG. 2019;126:132.
30. Alnadi A, Alnadi A, Almajalii A, Muhaidat N, Al-Qatawneh A, Badran EF. Obstetrics and perinatal outcome of grand multiparity in Jordan: a case-control study. Clin Exp Obstet Gynecol. 2019;46(2):250–257.
31. Alshebly MM. Pregnancy outcome in advanced maternal age in Saudi women. Int J Gynecol Obstet. 2018;143:602–603.
32. Roy R, Vernekar M. Feto-maternal outcome in grand multipara. Int J Reprod Contracept Obstet Gynecol. 2017;6(2):2846–2851. doi:10.18203/2320-1770.ijrcog20172562
33. Teguete I, Maiga AW, Leppert PC. Maternal and neonatal outcomes of grand multiparas over two decades in Mali. Acta Obstet Gynecol Scand. 2012;91(5):580–586. doi:10.1111/j.1600-0412.2012.01372.x
34. Woday A, Muluneh MD, Sherif S. Determinants of preterm birth among mothers who gave birth at public hospitals in the Amhara region, Ethiopia: a case-control study. PLoS One. 2019;14(11):e0225060. doi:10.1371/journal.pone.0225060
35. Gebremeskel F, Gultie T, Kejela G, Hailu D, Workneh Y. Determinants of adverse birth outcome among mothers who gave birth at hospitals in Gamo Gofa Zone, Southern Ethiopia: a facility based case control study. Qual Prim Care. 2017;25(5):259–266.
36. Kassa GM, Arowojolu AO, Odukogbe AA, Yalew AW. Adverse neonatal outcomes of adolescent pregnancy in Northwest Ethiopia. PLoS One. 2019;14(6):e0218259. doi:10.1371/journal.pone.0218259
37. Tsegaye B, Kassa A. Prevalence of adverse birth outcome and associated factors among women who delivered in Hawassa town governmental health institutions, south Ethiopia, in 2017. Reprod Health. 2018;15(1):193. doi:10.1186/s12978-018-0631-3
38. Adane AA, Ayele TA, Ararsa LG, Bitew BD, Zeleke BM. Adverse birth outcomes among deliveries at Gondar University hospital, Northwest Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):90. doi:10.1186/1471-2393-14-90
39. Hailemichael HT, Debelew GT, Alema HB, Weldu MG, Misgina KH. Determinants of adverse birth outcome in Tigrai region, North Ethiopia: hospital-based case-control study. BMC Pediatr. 2020;20(1):1–9. doi:10.1186/s12887-019-1835-6
40. Cherie N, Mebratu A. Adverse birth out comes and associated factors among delivered mothers in Dessie referral hospital North East Ethiopia; 2018:1–6.
41. World Health Organization. The International Statistical Classification of Diseases and Health Related Problems ICD-10: Tenth Revision. Tabular List. Vol. 1. World Health Organization; 2004.
42. Da Silva FT, Gonik B, McMillan M, et al. Stillbirth: case definition and guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine. 2016;34(49):6057. doi:10.1016/j.vaccine.2016.03.044
43. World Health Organization. Organization WH. International Statistical Classification of Diseases and Related Health Problems, Tenth Revision.
44. World Health Organization. WHO recommendations on interventions to improve preterm birth outcomes; 2015.
45. World Health Organization. Guidelines on Basic Newborn Resuscitation. Geneva: World Health Organization; 2012.
46. Federal Ministry of Healthof Ethiopia. Neonatal Intensive Care Unit (NICU) training management protocol; 2014.
47. Watterberg KL, Aucott S, Benitz WE. The apgar score. Pediatrics. 2015;136(4):819–822. doi:10.1542/peds.2015-2651
48. Craney TA, Surles JG. Model-dependent variance inflation factor cutoff values. Qual Eng. 2002;14(3):391–403. doi:10.1081/QEN-120001878
49. Association WM. Declaration of Helsinki. Ethical principles for medical research involving human subjects. Jahrbuch Für Wissenschaft Und Ethik. 2009;14(1):233–238. doi:10.1515/9783110208856.233
50. Adeniran A, Fawole A, Fakeye O, et al. Grandmultiparity: evaluating obstetric and neonatal outcomes after eliminating confounders; 2014.
51. Eugene MI, Abedinego OA. Grandmultiparity: is it really an independent predictor of adverse pregnancy outcomes? Saudi J Health Sci. 2017;6(2):77. doi:10.4103/sjhs.sjhs_98_16
52. Moazzem Hossain S, El NS, Ibrahim S, et al. Maternal and neonatal health in select districts of Iraq: findings from a recent household survey. J Pregnancy Child Health. 2018;5(5):10–4172.
53. Ftwi M, Gebretsadik GG-E, Berhe H, et al. Coverage of completion of four ANC visits based on recommended time schedule in Northern Ethiopia: a community-based cross-sectional study design. PLoS One. 2020;15(8):e0236965. doi:10.1371/journal.pone.0236965
54. Omole-Ohonsi A, Ashimi A. Grand multiparity: obstetric performance in Aminu Kano teaching hospital, Kano, Nigeria. Niger J Clin Pract. 2011;14(1):6. doi:10.4103/1119-3077.79231
55. Al-Farsi YM, Brooks DR, Werler MM, Cabral HJ, Al-Shafaee MA, Wallenburg HC. Effect of high parity on occurrence of some fetal growth indices: a cohort study. Int J Womens Health. 2012;4:289. doi:10.2147/IJWH.S32190
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.