Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Effect of Glucose Metabolic State Transition on Progression from Stage A to Stage C Heart Failure
Authors Yin M ![]() , Xu X, Li J, Sun Y, Zhen Y, Wu S
, Xu X, Li J, Sun Y, Zhen Y, Wu S ![]() , Fang H
, Fang H
Received 3 March 2025
Accepted for publication 15 May 2025
Published 22 May 2025 Volume 2025:18 Pages 1683—1693
DOI https://doi.org/10.2147/DMSO.S525408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hillary Keenan
Mingjie Yin,1 Xiaoyu Xu,2 Jie Li,1 Yanan Sun,3 Yanfeng Zhen,3 Shouling Wu,4 Hui Fang1,3
1Department of Internal Medicine, Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Training Base, Tangshan Gongren Hospital, Tangshan, Hebei, People’s Republic of China; 3Second Department of Endocrinology and Metabolism, Tangshan Gongren Hospital, Tangshan, Hebei, People’s Republic of China; 4Department of Cardiology, Kailuan General Hospital, Tangshan, Hebei, People’s Republic of China
Correspondence: Hui Fang, Department of Internal Medicine, Hebei Medical University, 361 Zhongshan East Road, Shijiazhuang, Hebei, 050000, People’s Republic of China, Tel +8613831581838, Email [email protected]
Background: Heart failure (HF) constitutes a significant global health challenge. The interplay between the dynamics of glucose metabolic status transitions and the progression of HF has been minimally explored.
Objective: We assessed the impact of shifts in glucose metabolic states on the progression from stage A to stage C HF.
Methods: The Kailuan Study is a large-scale prospective cohort study. Based on data from the Kailuan Study, 41,110 stage A HF patients were included and stratified into 6 groups based on alterations in glucose metabolic status: stable normoglycemic, stable pre-diabetes, diabetes, normoglycemic progressing to pre-diabetes, pre-diabetes back to normoglycemic, and normoglycemic/pre-diabetes progressing to diabetes. Utilizing the Cox proportional hazards regression model, we calculated the hazard ratios (HR) and 95% confidence intervals (CI) associated with the transition to stage C HF among patients with stage A HF with different glucose metabolic state transitions.
Results: Our findings indicated a notably elevated risk for the progression to stage C HF within the diabetic group relative to the stable normoglycemic group (HR, 1.87; 95% CI, 1.66 to 2.10). Additionally, an augmented risk for the progression to stage C HF was observed in the normoglycemic/pre-diabetic to diabetic group (HR, 1.38; 95% CI, 1.15 to 1.65).
Conclusion: Both diabetes and normoglycemic/pre-diabetes progressing to diabetes are associated with heightened risks of progressing from stage A to stage C HF. Conversely, the re-establishment of normoglycemic in pre-diabetes is associated with preventing HF progression.
Keywords: glucose metabolic state, diabetes, pre-diabetes, stage A heart failure, stage C heart failure
Introduction
Heart failure (HF) represents a substantial global health challenge, as evidenced by data from the 2012–2015 China Hypertension Survey, which reports an increasing prevalence of HF among Chinese adults aged 35 years or older, currently at 1.3%.1 Traditional risk factors, such as hypertension, diabetes, and obesity, are well-established contributors to HF.2 Epidemiological cohort studies have consistently demonstrated that diabetes significantly elevates the risk of HF by a factor of 2 to 53,4 and also augments the risk of all-cause mortality post-HF diagnosis by 28% to 60%.5,6 Concurrently, research has indicated that pre-diabetes is associated with a 46% heightened risk of HF.7 Furthermore, it is recognized that elevated blood glucose levels, irrespective of whether they are indicative of pre-diabetes or diabetes, confer an increased susceptibility to HF.4 The potential mechanisms linking glucose metabolism transitions and HF are multifaceted, including the altered energy metabolism of cardiomyocytes due to long-term hyperglycemia caused by insulin resistance,8,9 as well as the damage to the structure and function of cardiomyocytes, and the subsequent myocardial remodeling triggered by oxidative stress.10,11
The 2001 ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult initially categorized HF into 4 stages (A, B, C, and D), delineating the trajectory of the condition’s evolution.12 This classification was reaffirmed in the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.13 Stage A HF is characterized by the presence of high-risk factors without structural cardiac abnormalities or overt signs and symptoms of HF. If patients in stage A HF do not receive early intervention, leading to structural heart abnormalities (stage B HF), their risk of developing symptomatic heart failure (stages C/D HF) will significantly increase.14–16 In addition, although stage C HF has signs and symptoms of HF and structural cardiac abnormalities, standardized treatment can significantly reduce the rate of re-hospitalization, mortality, and the risk of progressing to Stage D HF, which has the poorest prognosis.17,18 Therefore, stage A and stage C HF are critical stages in the progression of HF.
However, previous studies have centered on the influence of baseline glucose metabolic status on HF risk,4,7 with minimal attention given to the interplay between glucose metabolic transitions and HF progression. This study aims to bridge this research gap by leveraging data from the Kailuan Study to further investigate the effect of glucose metabolic state transition on HF progression from stage A to stage C in a large sample size.
Methods
Study Design and Patients
The Kailuan Study is a large-scale prospective cohort study based on a functional community population. We recruited patients diagnosed with stage A HF from the health screenings conducted in 2006 and 2008. The inclusion criteria were as follows: (1) participants who underwent health screenings in 2006 and 2008; (2) subjects who met the criteria for stage A HF, which includes the presence of hypertension, cardiovascular disease, diabetes, or obesity. The exclusion criteria were: (1) any participant with a prior history of HF, valvular heart disease, or cardiomyopathy before the 2008 examination; (2) subjects with incomplete fasting blood glucose (FBG) records, as illustrated in Figure 1. The study protocol was sanctioned by the Medical Ethics Committee of Kailuan General Hospital (Approval No. 2018ZX10715005) and adhered rigorously to the ethical standards of the Declaration of Helsinki. Informed consent was obtained from all participants involved in the study.
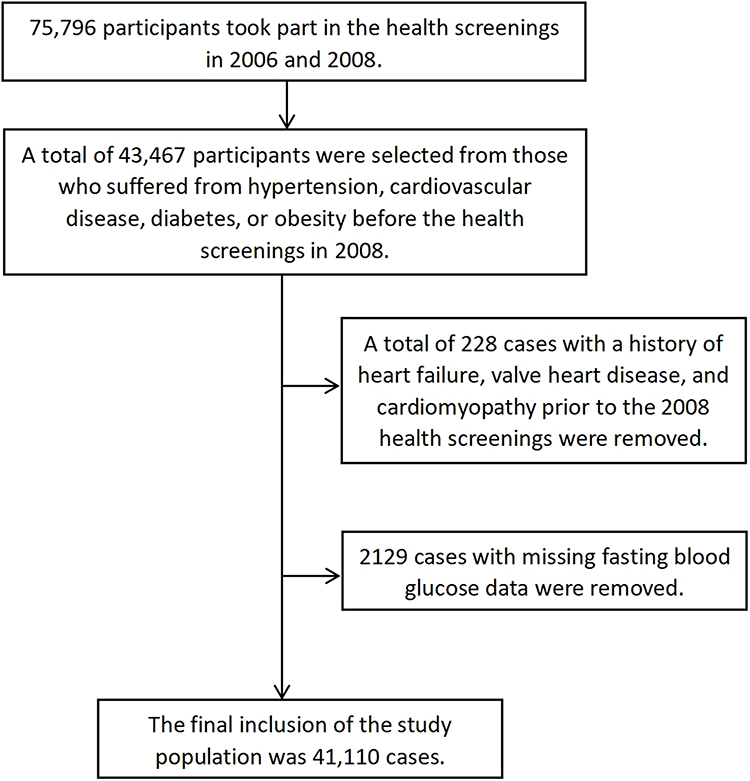 |
Figure 1 Inclusion exclusion flowchart. |
Data Collection
We gathered demographic details, including gender and age, along with information on health behaviors such as smoking status, alcohol consumption, frequency of physical exercise, and salt habits. Additionally, we documented the medical history of hypertension, cardiovascular disease, and diabetes, as well as the medications history, specifically, the utilization of lipid-lowering, antihypertensive, and hypoglycemic agents. This information was systematically collected from the study cohort through a comprehensive questionnaire. Concurrently, we also recorded anthropometric measurements, including height, weight, waist circumferences, hip circumferences, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate. Furthermore, we assessed various biochemical parameters: FBG, triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and highly sensitive C-reactive protein (hs-CRP), following the methodologies delineated in the referenced scholarly publications.19
Relevant Definitions
Glucose metabolic state transitions are categorized into 6 groups: stable normoglycemic (twice FBG < 6.1 mmol/L with no history of diabetes and no use of hypoglycemic medications), stable pre-diabetes (6.1 mmol/L ≤ twice FBG < 7.0 mmol/L with no history of diabetes and no use of hypoglycemic medications), diabetes (the first FBG ≥ 7.0 mmol/L or the first FBG < 7.0 mmol/L but with a clear diagnosis of diabetes or use of hypoglycemic drugs), normoglycemic progressing to pre-diabetes, pre-diabetes back to normoglycemic, and normoglycemic/pre-diabetes progressing to diabetes. Hypertension is diagnosed based on SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg; if there is a history of clearly diagnosed hypertension or use of antihypertensive medications, hypertension can also be rendered, even if SBP < 140 mmHg and DBP < 90 mmHg. Cardiovascular diseases encompass a spectrum of conditions, including coronary heart disease (myocardial infarction, coronary stenting/bypass) and stroke (hemorrhagic stroke, ischemic stroke). The Body Mass Index (BMI) is calculated using the formula: weight (kg)/height (m)2, BMI ≥ 28 kg/m2 is considered obese. The waist-to-hip ratio is calculated using the formula: waist circumference (cm)/hip circumference (cm). Smoking status is defined by the consumption of at least 1 cigarette per day on average over the past year. Alcohol consumption is categorized based on gender-specific thresholds: men consumed ≥2 standard drinks/day and women consumed ≥1 standard drink/day on average over the past year. Regular physical exercise is defined as performing exercises at least 3 times per week, with each session enduring a minimum of 30 minutes, while occasional exercise is defined as having 1 to 2 sessions of exercise lasting over 30 minutes per week. Salt habits are stratified into three categories based on daily intake of sodium chloride: low (<6 g), medium (6–12 g), and high (>12 g).
Outcomes
The follow-up study commenced after patients with stage A HF complete the 2008 health screenings, and the primary endpoint was defined as the progression to stage C HF during the follow-up. The final follow-up date was set for December 31, 2020 for participants without event occurrence. Should a participant not experience the endpoint event but expire during the study, the expiration date was considered the endpoint of the follow-up. Trained medical staff reviewed participants’ hospitalization data at hospitals affiliated with Kailuan Group and city-designated insurance hospitals to confirm the occurrence of stage C HF events. Data on the first progression to stage C HF were collected, including left ventricular ejection fraction (LVEF) and N-terminal pro B-type natriuretic peptide (NT-proBNP) (Supplementary Table 1).
Determination of Stage A HF: Participants exhibited no prior history of HF and were classified as stage A HF before the health screenings in 2008. Definition of Stage A HF: (1) There are risk factors for HF, including hypertension, cardiovascular disease, diabetes, or obesity. (2) The absence of symptoms or structural heart disease (including valvular heart disease or cardiomyopathy).
Determination of Stage C HF: Participants exhibited no prior history of HF at the 2008 health screenings, with conditions that subsequently progressed to Stage C HF during the follow-up. Definition of Stage C HF: (1) Manifestations of heart failure, characterized by dyspnea, fatigue, and signs of fluid retention, accompanied by a distinct classification of cardiac function according to the New York Heart Association (NYHA) class II to IV or Killip class II to IV upon discharge; (2) LVEF not exceeding 50%, as ascertained by two-dimensional and Doppler echocardiographic evaluation utilizing the modified Simpson method; (3) Increased plasma levels of NT-proBNP. The diagnosis of Stage C HF necessitates the presence of condition (1) in conjunction with at least one of the conditions (2) or (3).
Statistical Analysis
SAS9.4 statistical software was used for statistical analysis. The baseline data of the study subjects were analyzed descriptively, and the continuous variables distributed symmetrically were expressed as mean ± standard deviation, and the comparison between groups was performed by one-way ANOVA; the skewed continuous variables were expressed as median (interquartile range), and the comparison between groups was performed by the Kruskal–Wallis test; and the categorical variables were expressed as percentages, and the comparison between groups was performed by chi-squared or Fisher’ tests. Missing values for covariates were imputed by multiple interpolations.
The cumulative incidence of progression to stage C HF in patients with stage A HF with different glucose metabolic state transitions was calculated using the Kaplan–Meier method. Differences among groups were evaluated with the Log rank test. The hazard ratio (HR) and 95% confidence interval (CI) of progression to stage C HF in patients with stage A HF with different glucose metabolic state transitions were analyzed by the Cox proportional risk regression model. Model I adjusted for gender (male, female) and age. Model II additionally adjusted for smoking (yes, no), alcohol-drinker (yes, no), frequency of physical exercise (never, occasional, regular), salt habits (low, medium, high), waist-to-hip ratio (≤0.9 for men or ≤0.8 for women, >0.9 for men or >0.8 for women), SBP, TG, LDL-C, and HDL-C. Model III further adjusted for the use of lipid-lowering medications at baseline (yes, no) and the use of antihypertensive medications at baseline (yes, no). To assess the robustness of the findings, the following sensitivity analyses were performed: (1) defining glucose metabolic state transitions based on records from the three follow-up visits in 2006, 2008, and 2010; and (2) repeating the multifactorial Cox regression analyses after excluding participants with a history of hypertension, obesity, cardiovascular disease, coronary heart disease, and stroke. Two-sided tests were performed with P < 0.05 as the difference was statistically significant.
Results
Baseline Characteristics Analysis
Among the 41,110 participants with stage A HF, the study comprised 34,151 males (83.07%) with a mean age of 53.10 ± 11.59 years, and 6959 females (16.93%) with a mean age of 53.69 ± 10.00 years. Relative to the stable normoglycemic group, the diabetic group had a higher proportion of females, age, FBG, TG, TC, LDL-C, hs-CRP, heart rate, frequency of physical exercise, the prevalence of cardiovascular disease, the rate of lipid-lowering and antihypertensive medications use at baseline, and the rate of lipid-lowering medications use during follow-up, while HDL-C, SBP, DBP, BMI, waist-to-hip ratio, the proportion of smoking, the proportion of alcohol-drinker, salt intake, the prevalence of hypertension, the prevalence of obesity, and the rate of antihypertensive medications use during follow-up are lower (Table 1).
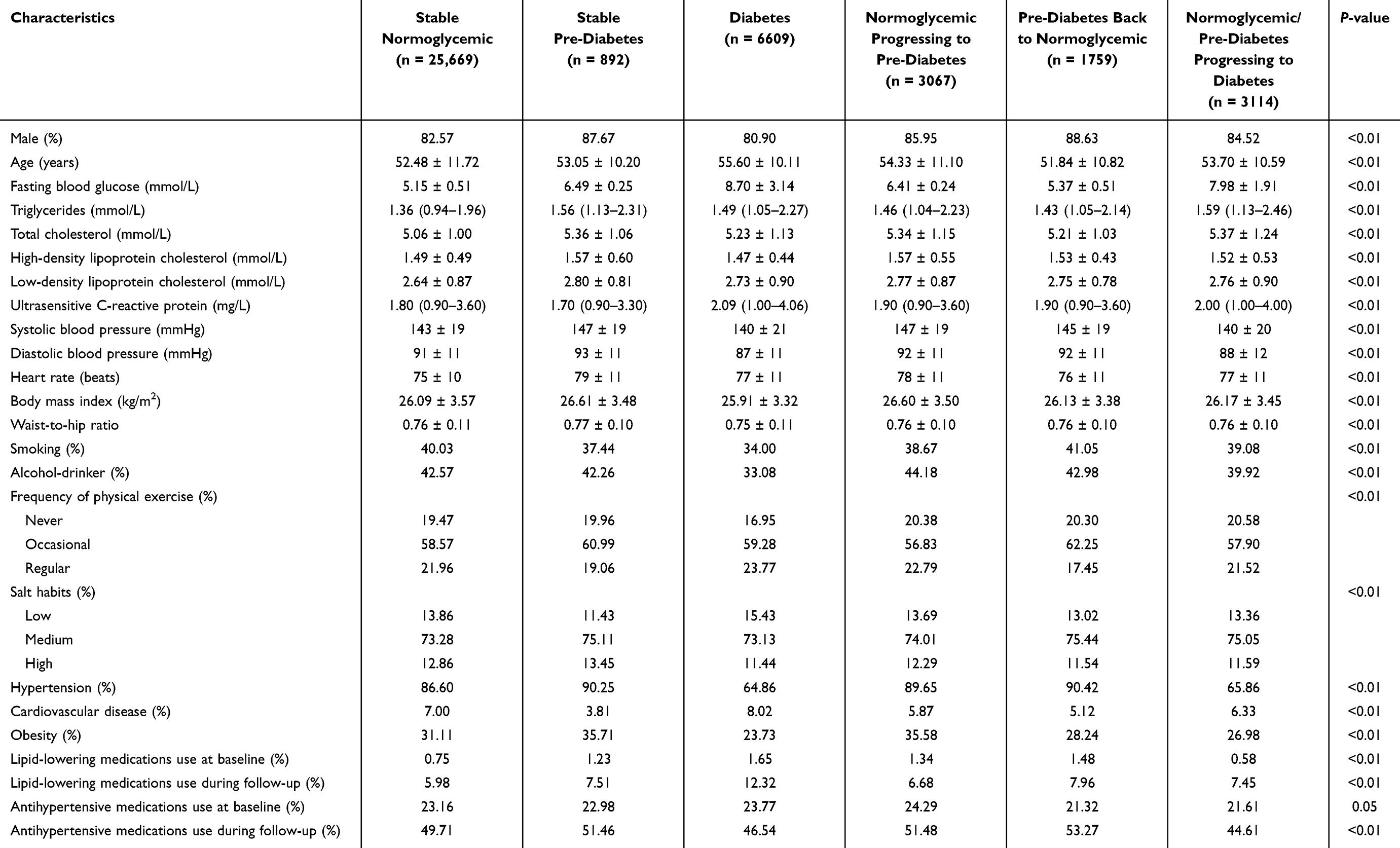 |
Table 1 Characteristics by Different Glucose Metabolic State Transitions |
Analysis of Cumulative Morbidity and Morbidity Density
Over a mean follow-up duration of 11.00 ± 2.42 years, 1604 patients with stage A HF progressed to stage C HF. The cumulative incidence of progression to stage C HF in the stable normoglycemic, stable pre-diabetic, diabetic, normoglycemic progression to pre-diabetic, pre-diabetic back to normoglycemic, and normoglycemic/pre-diabetic progression to diabetic groups was 3.41% (826/25,669), 3.09% (26/892), 7.21% (432/6609), 4. 27% (122/3067), 3.42% (57/1759) and 4.88% (141/3114), with statistically significant differences between the groups (P < 0.01, Figure 2). The incidence densities were, in descending order, 2.89/1000 person-years, 2.63/1000 person-years, 6.20/1000 person-years, 3.61/1000 person-years, 2.93/1000 person-years, 4.13/1000 person-years.
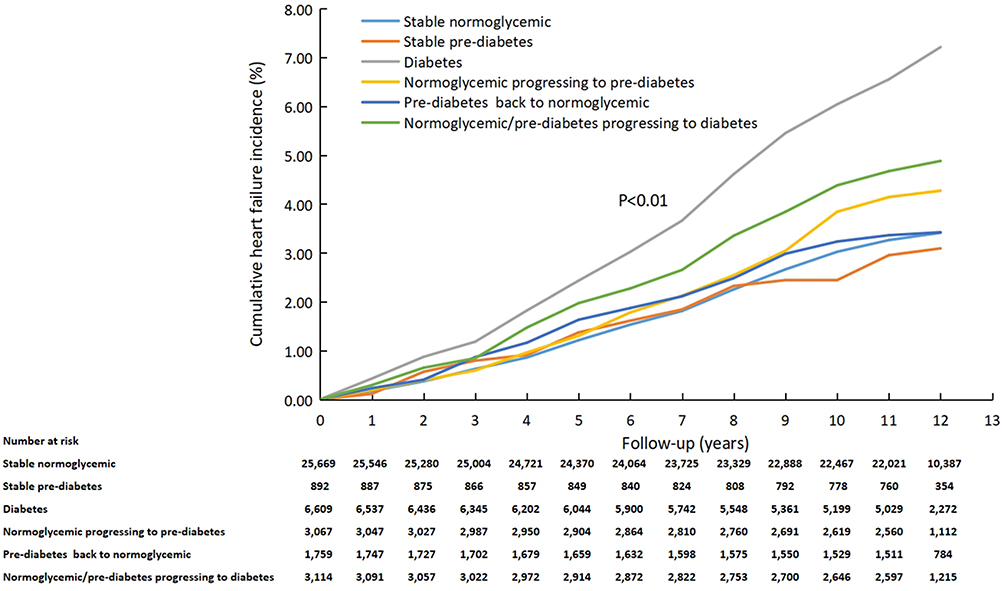 |
Figure 2 The cumulative incidence curve of progression to stage C heart failure in different glucose metabolic state transitions. |
Multifactorial Cox Regression Analysis of the Effect of Different Glucose Metabolic State Transition Scenarios on the Risk of Progression to Stage C HF in Patients with Stage A HF
In patients with stage A HF, there was a significantly increased risk of progression to stage C HF in the diabetic group compared with the stable normoglycemic group (HR, 1.87; 95% CI, 1.66–2.10) and an increased risk of progression to stage C HF in the normoglycemic/pre-diabetic to diabetic group (HR, 1.38; 95% CI, 1.15–1.65) (Table 2).
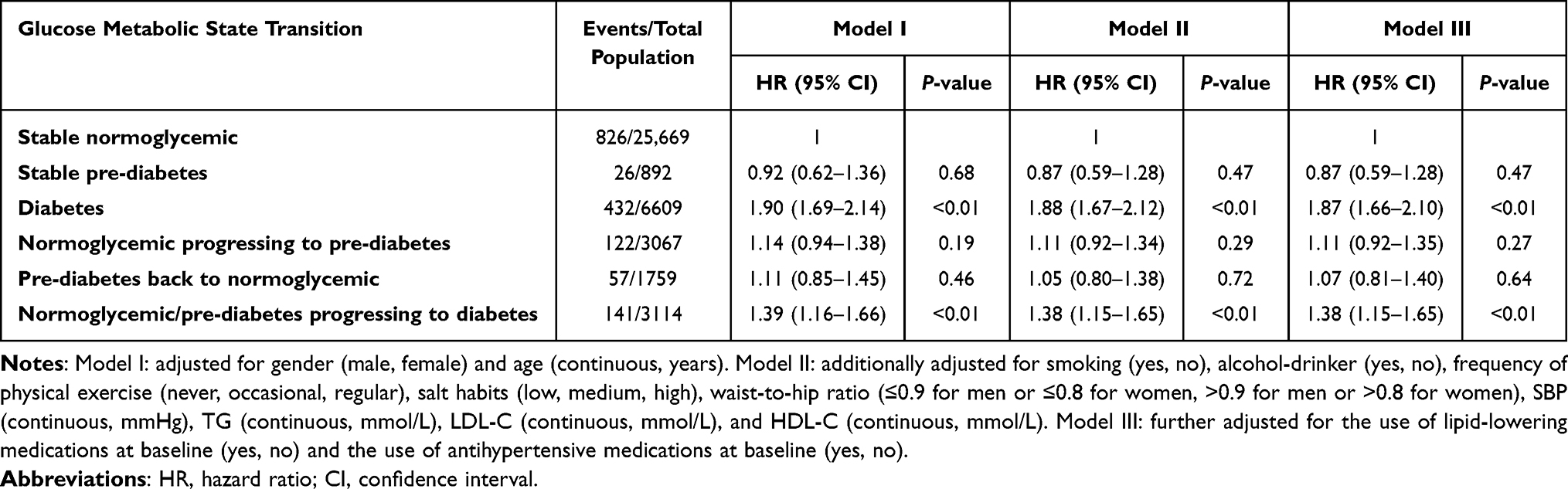 |
Table 2 Associations of Glucose Metabolic State Transition with Risk of Progression to Stage C Heart Failure in Patients with Stage A Heart Failure |
Sensitivity Analysis
Following the classification of glucose metabolic state transitions derived from three follow-up assessments conducted in 2006, 2008, and 2010 (Table 3), and the subsequent exclusion of participants with a history of cardiovascular disease, coronary heart disease, and stroke (Table 4), the findings remained largely consistent with the primary analysis. Nonetheless, upon the exclusion of participants with a history of hypertension, a significant reduction in the risk of progression to stage C HF was observed within the diabetic group, and the normoglycemic/pre-diabetic progression to the diabetic group. In addition, after excluding obese patients, the risk of progression to stage C HF in the diabetes group, and the normoglycemic/pre-diabetic progression to the diabetic group increased from 87% and 38% to 98% and 53%, respectively (Table 4).
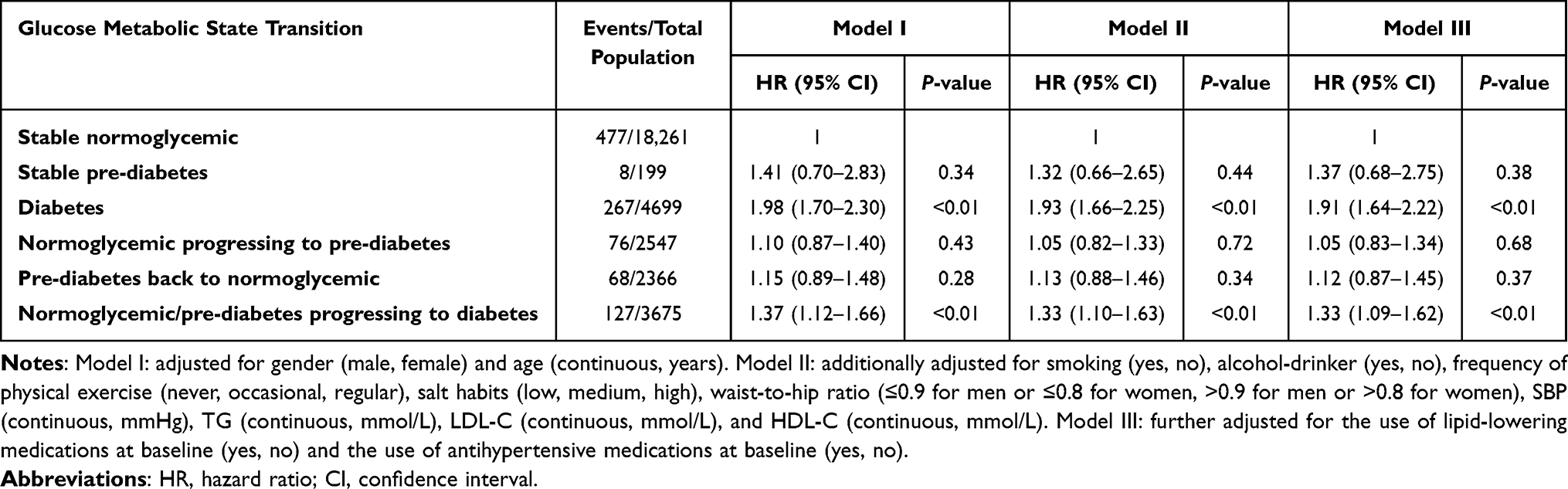 |
Table 3 Associations of Glucose Metabolic State Transition (2006, 2008, and 2010) with Risk of Progression to Stage C Heart Failure in Patients with Stage A Heart Failure |
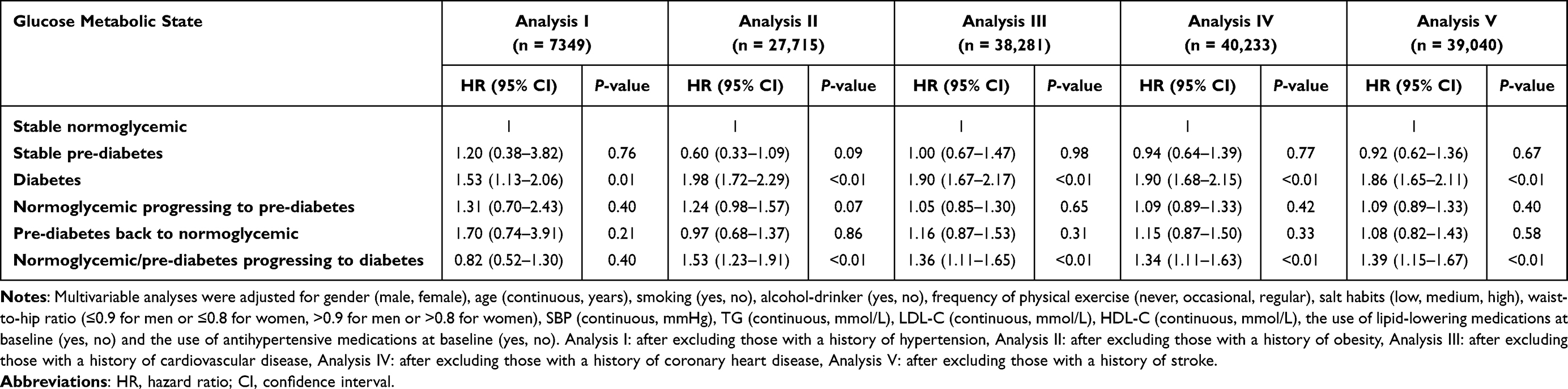 |
Table 4 Associations of Glucose Metabolic State Transition with Risk of Progression to Stage C Heart Failure in Patients with Stage A Heart Failure After Excluding Those with a History of Hypertension, Obesity, Cardiovascular Disease, Coronary Heart Disease, and Stroke |
Discussion
In our study, we observed that alterations in glucose metabolic states significantly influence the risk of HF progression. Specifically, diabetes was found to escalate the risk of progressing from stage A to stage C HF. Moreover, even the transition from normoglycemic/pre-diabetes to diabetes was associated with a notably heightened risk for the progression from stage A to stage C HF.
A principal outcome of our study indicated a substantial 87% increase in the risk of progression from stage A to stage C HF within the diabetic group relative to the stable normoglycemic group. Intriguingly, the normoglycemic/pre-diabetic progressing to diabetes group also demonstrated a significant 38% increase in the risk of progression to stage C HF. Although there are no previous studies similar to ours, findings show a 106% increased risk of HF in patients with baseline diabetes4 and a 58% increased risk of HF in patients with baseline pre-diabetes20 compared with those with normal baseline glucose metabolism. A limitation of prior studies is that they focused on single blood glucose measurement or baseline metabolic status, overlooking the dynamic changes in glucose metabolism throughout the follow-up. Furthermore, although previous studies have found that diabetes may further increase the risk of HF in patients with stable coronary artery disease,21 myocardial infarction,22 and hypertension,23 they have not investigated the risk of HF progression in these high-risk populations.
Another important finding of ours is that although the risk of progression from stage A to stage C HF was increased by 7% in the pre-diabetic back to normoglycemia group compared with the stable normoglycemic group, it did not reach a statistically significant difference (P = 0.64, 95% CI: 0.81–1.40). This finding holds profound clinical relevance, particularly for the pre-diabetic group, suggesting that proactive lifestyle modifications could potentially mitigate the risk of progression to diabetes and impede the advancement of HF from stage A to stage C. Extensive evidence from randomized controlled trials corroborates that lifestyle interventions can decrease the likelihood of diabetes development in pre-diabetes participants by 36%–58%.24–26 Drawing from our study and corroborative research, aggressive lifestyle interventions or even pharmacological interventions should be given to people with pre-diabetes, especially those with pre-diabetes in combination with other HF risk factors such as coronary heart disease, hypertension, and chronic kidney disease, to stop the progression to diabetes or even return to normoglycemic and thus reduce the progression to HF.27
Given that diabetes is often comorbid with other diseases that are significantly linked to HF risk, we excluded patients with hypertension, obesity, cardiovascular disease, coronary heart disease, and stroke separately to estimate the true strength of the association between glucose metabolic state transitions and the risk of HF progression. We found no significant increase in the risk of progression from stage A to stage C HF in the normoglycemic/pre-diabetic to the diabetic group after excluding the hypertensive group, whereas the risk of progression from stage A to stage C HF in the diabetic group decreased from an increase of 87% to an increase of 53%, suggesting that there may be a synergistic effect between the effects of hypertension and glucose metabolic status and transition on the risk of HF progression. Notably, after excluding patients with cardiovascular disease, coronary heart disease, and stroke, which are macrovascular lesions, the risk of progression from stage A HF to stage C HF in the two groups did not change significantly from the main analysis, suggesting that progression of our glucose metabolic status may contribute to an increased risk of HF progression through myocardial dysfunction due to microvascular pathology, but not through macrovascular vascular lesions.28,29 Moreover, after excluding obese patients, the risk of progression to stage C HF in the diabetes group, and the normoglycemic/pre-diabetic progression to the diabetic group increased from 87% and 38% to 98% and 53%, respectively. A similar finding from previous studies that the risk of hospitalization for HF was increased by 99% in lean diabetic patients compared with obese diabetic patients, which may be related to the higher prevalence of left ventricular diastolic dysfunction in lean diabetic patients.30 This underscores the necessity for early screening of microvascular complications and routine cardiac function assessments in stage A HF patients, irrespective of obesity status.
The pathological mechanisms linking the glucose metabolic state transition and the risk of HF are complex and involve multiple aspects such as impaired glucose metabolism, microvascular lesions, myocardial interstitial fibrosis, and cardiomyocyte hypertrophy.31 Firstly, long-term hyperglycemia caused by insulin resistance induces a phenotypic shift in cardiomyocytes, transitioning their energy metabolism from preferential utilization of fatty acids to preferential utilization of glucose.8 This phenotypic shift consequently results in insufficient energy supply to cardiomyocytes.9 Secondly, biomolecular research indicates that oxidative stress affects the structure and function of cardiomyocytes through multiple mechanisms. It can trigger excessive production of reactive oxygen species in mitochondria, disrupt mitochondrial membrane potential, and lead to mitochondrial swelling and dysfunction, which impacts myocardial energy metabolism and triggers sympathetic excitation and sodium storage. It can also activate proteases within cardiomyocytes (such as caspases), cleaving cytoskeletal proteins (such as desmin). This process not only disrupts the structural integrity of cardiomyocytes, leading to disordered myofibrils and decreased myocardial compliance, but also activates signaling pathways (such as TNF-α), thereby triggering myocardial remodeling (such as hypertrophy and fibrosis).10,11 Finally, diabetic endothelial dysfunction can lead to coronary microvascular dysfunction, which in turn significantly reduces coronary blood flow reserve. This reduction in blood flow reserve can cause myocardial ischemia and hypoxia and ultimately may lead to myocardial cell death and myocardial function decline.32,33 In addition, the presence of high-risk factors for HF, such as hypertension and obesity, during the progression of glucose metabolism can further exacerbate the deterioration of myocardial structure and function, such as ventricular hypertrophy and myocardial fibrosis.34,35 Meanwhile, our results showed that metabolic indicators such as FBG, TG, TC, LDL-C, and hs-CRP were significantly higher in the normoglycemic/pre-diabetic progression to diabetic and diabetic groups compared with the stable normoglycemic group; therefore, we hypothesized that metabolic factors associated with pre-diabetes may also adversely affect myocardial function through microangiopathy.
Our study carries significant clinical implications, particularly for stage A HF patients. Diabetes and normoglycemic/pre-diabetes progression to diabetes are both associated with an increased risk of HF progression. Conversely, the restoration of normoglycemia from pre-diabetes may mitigate this risk. This suggests that it is important to understand the transition of glucose metabolic status in patients with stage A HF, to actively screen for microvascular lesions, to perform cardiac function tests, and to reduce the likelihood of HF progression by implementing targeted therapies (SGLT-2 inhibitors,36 GLP-1 agonists37) to key populations.
There are some limitations to this study: Firstly, the classification of glucose metabolic status based on FBG, diabetes history, and hypoglycemic medications usage may omit participants with impaired glucose tolerance or undiagnosed diabetes, potentially leading to an underestimation of the diseases’ prevalence and their correlation with HF progression risk.38 Secondly, the study population was limited to insured participants of Asian descent. This may restrict the generalizability of our findings and necessitates further validation in broader and more diverse populations.
Conclusion
In summary, diabetes, normoglycemic/pre-diabetes progression to diabetes may both associated with an increased risk of progression from stage A to stage C HF. Conversely, the restoration of normoglycemia from pre-diabetes may mitigate this risk. Consequently, it is essential in clinical practice to continuously monitor blood glucose levels in stage A HF patients and to conduct a thorough assessment of their risk factors. This comprehensive approach is vital for the timely and precise development of intervention strategies aimed at mitigating HF progression.
Acknowledgments
The authors thank all the members of the Kailuan Study Team for their contributions and the participants who contributed their data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Hebei Province (grant number H2024105016).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Hao G, Wang X, Chen Z, et al. Prevalence of heart failure and left ventricular dysfunction in China: the China hypertension survey, 2012-2015. Eur J Heart Fail. 2019;21(11):1329–1337. doi:10.1002/ejhf.1629
2. Dunlay SM, Weston SA, Jacobsen SJ, et al. Risk factors for heart failure: a population-based case-control study. Am J Med. 2009;122(11):1023–1028. doi:10.1016/j.amjmed.2009.04.022
3. Ohkuma T, Komorita Y, Peters SAE, et al. Diabetes as a risk factor for heart failure in women and men: a systematic review and meta-analysis of 47 cohorts including 12 million individuals. Diabetologia. 2019;62(9):1550–1560. doi:10.1007/s00125-019-4926-x
4. Aune D, Schlesinger S, Neuenschwander M, et al. Diabetes mellitus, blood glucose and the risk of heart failure: a systematic review and meta-analysis of prospective studies. Nutr, Metab Cardiovasc Dis. 2018;28(11):1081–1091. doi:10.1016/j.numecd.2018.07.005
5. Johansson I, Edner M, Dahlström U, et al. Is the prognosis in patients with diabetes and heart failure a matter of unsatisfactory management? An observational study from the Swedish heart failure registry. Eur J Heart Fail. 2014;16(4):409–418. doi:10.1002/ejhf.44
6. Dauriz M, Mantovani A, Bonapace S, et al. Prognostic impact of diabetes on long-term survival outcomes in patients with heart failure: a meta-analysis. Diabetes Care. 2017;40(11):1597–1605. doi:10.2337/dc17-0697
7. Wang J, Sarnola K, Ruotsalainen S, et al. The metabolic syndrome predicts incident congestive heart failure: a 20-year follow-up study of elderly Finns. Atherosclerosis. 2010;210(1):237–242. doi:10.1016/j.atherosclerosis.2009.10.042
8. Rodrigues B, McNeill JH. The diabetic heart: metabolic causes for the development of a cardiomyopathy. Cardiovasc Res. 1992;26(10):913–922. doi:10.1093/cvr/26.10.913
9. Lopaschuk GD. Abnormal mechanical function in diabetes: relationship to altered myocardial carbohydrate/lipid metabolism. Coron Artery Dis. 1996;7(2):116–123. doi:10.1097/00019501-199602000-00004
10. Randhawa VK, Dhanvantari S, Connelly KA. How diabetes and heart failure modulate each other and condition management. Can J Cardiol. 2021;37(4):595–608. doi:10.1016/j.cjca.2020.11.014
11. Yancey DM, Guichard JL, Ahmed MI, et al. Cardiomyocyte mitochondrial oxidative stress and cytoskeletal breakdown in the heart with a primary volume overload. Am J Physiol Heart Circ Physiol. 2015;308(6):H651–63. doi:10.1152/ajpheart.00638.2014
12. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: executive summary a report of the American college of cardiology/American heart association task force on practice guidelines (committee to revise the 1995 guidelines for the evaluation and management of heart failure): developed in collaboration with the international society for heart and lung transplantation; endorsed by the heart failure society of America. Circulation. 2001;104(24):2996–3007. doi:10.1161/hc4901.102568
13. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79(17):1757–1780. doi:10.1016/j.jacc.2021.12.011
14. Xanthakis V, Enserro DM, Larson MG, et al. Prevalence, neurohormonal correlates, and prognosis of heart failure stages in the community. JACC Heart Fail. 2016;4(10):808–815. doi:10.1016/j.jchf.2016.05.001
15. Ammar KA, Jacobsen SJ, Mahoney DW, et al. Prevalence and prognostic significance of heart failure stages: application of the American college of cardiology/American heart association heart failure staging criteria in the community. Circulation. 2007;115(12):1563–1570. doi:10.1161/circulationaha.106.666818
16. Del Gobbo LC, Kalantarian S, Imamura F, et al. Contribution of major lifestyle risk factors for incident heart failure in older adults: the cardiovascular health study. JACC Heart Fail. 2015;3(7):520–528. doi:10.1016/j.jchf.2015.02.009
17. McAlister FA, Stewart S, Ferrua S, et al. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol. 2004;44(4):810–819. doi:10.1016/j.jacc.2004.05.055
18. Parajuli DR, Kourbelis C, Franzon J, et al. Effectiveness of the pharmacist-involved multidisciplinary management of heart failure to improve hospitalizations and mortality rates in 4630 patients: a systematic review and meta-analysis of randomized controlled trials. J Card Fail. 2019;25(9):744–756. doi:10.1016/j.cardfail.2019.07.455
19. Liu Y, Jin C, Xing A, et al. Serum uric acid levels and the risk of impaired fasting glucose: a prospective study in adults of north China. PLoS One. 2013;8(12):e84712. doi:10.1371/journal.pone.0084712
20. Cai X, Liu X, Sun L, et al. Prediabetes and the risk of heart failure: a meta-analysis. Diabetes Obes Metab. 2021;23(8):1746–1753. doi:10.1111/dom.14388
21. van Melle JP, Bot M, de Jonge P, et al. Diabetes, glycemic control, and new-onset heart failure in patients with stable coronary artery disease: data from the heart and soul study. Diabetes Care. 2010;33(9):2084–2089. doi:10.2337/dc10-0286
22. Stone PH, Muller JE, Hartwell T, et al. The effect of diabetes mellitus on prognosis and serial left ventricular function after acute myocardial infarction: contribution of both coronary disease and diastolic left ventricular dysfunction to the adverse prognosis. The MILIS study group. J Am Coll Cardiol. 1989;14(1):49–57. doi:10.1016/0735-1097(89)90053-3
23. Bertoni AG, Hundley WG, Massing MW, et al. Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care. 2004;27(3):699–703. doi:10.2337/diacare.27.3.699
24. Lindström J, Louheranta A, Mannelin M, et al. The Finnish Diabetes Prevention Study (DPS): lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care. 2003;26(12):3230–3236. doi:10.2337/diacare.26.12.3230
25. Lindström J, Ilanne-Parikka P, Peltonen M, et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: follow-up of the Finnish Diabetes Prevention Study. Lancet. 2006;368(9548):1673–1679. doi:10.1016/s0140-6736(06)69701-8
26. Diabetes Prevention Program (DPP) Research Group. The diabetes prevention program (DPP): description of lifestyle intervention. Diabetes Care. 2002;25(12):2165–2171. doi:10.2337/diacare.25.12.2165
27. Zand A, Ibrahim K, Patham B. Prediabetes: why should we care? Methodist DeBakey Cardiovasc J. 2018;14(4):289–297. doi:10.14797/mdcj-14-4-289
28. Sezer M, Kocaaga M, Aslanger E, et al. Bimodal pattern of coronary microvascular involvement in diabetes mellitus. J Am Heart Assoc. 2016;5(11). doi:10.1161/jaha.116.003995
29. Horton WB, Barrett EJ. Microvascular dysfunction in diabetes mellitus and cardiometabolic disease. Endocr Rev. 2021;42(1):29–55. doi:10.1210/endrev/bnaa025
30. Tromp J, Tay WT, Ouwerkerk W, et al. Multimorbidity in patients with heart failure from 11 Asian regions: a prospective cohort study using the ASIAN-HF registry. PLoS Med. 2018;15(3):e1002541. doi:10.1371/journal.pmed.1002541
31. Bauters C, Lamblin N, Mc Fadden EP, et al. Influence of diabetes mellitus on heart failure risk and outcome. Cardiovasc Diabetol. 2003;2(1):1. doi:10.1186/1475-2840-2-1
32. Nitenberg A, Valensi P, Sachs R, et al. Impairment of coronary vascular reserve and ACh-induced coronary vasodilation in diabetic patients with angiographically normal coronary arteries and normal left ventricular systolic function. Diabetes. 1993;42(7):1017–1025. doi:10.2337/diab.42.7.1017
33. Nahser PJ, Brown RE, Oskarsson H, et al. Maximal coronary flow reserve and metabolic coronary vasodilation in patients with diabetes mellitus. Circulation. 1995;91(3):635–640. doi:10.1161/01.cir.91.3.635
34. Sacks D, Baxter B, Campbell BCV, et al. Multisociety consensus quality improvement revised consensus statement for endovascular therapy of acute ischemic stroke. Int J Stroke. 2018;13(6):612–632. doi:10.1177/1747493018778713
35. Madamanchi C, Alhosaini H, Sumida A, et al. Obesity and natriuretic peptides, BNP and NT-proBNP: mechanisms and diagnostic implications for heart failure. Int J Cardiol. 2014;176(3):611–617. doi:10.1016/j.ijcard.2014.08.007
36. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/NEJMoa1812389
37. Waqas SA, Sohail MU, Saad M, et al. Efficacy of GLP-1 receptor agonists in patients with heart failure and mildly reduced or preserved ejection fraction: a systematic review and meta-analysis. J Card Fail. 2025. doi:10.1016/j.cardfail.2025.01.022
38. DECODE Study Group, European Diabetes Epidemiology Group. Is the current definition for diabetes relevant to mortality risk from all causes and cardiovascular and noncardiovascular diseases? Diabetes Care. 2003;26(3):688–696. doi:10.2337/diacare.26.3.688
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.