")
Back to Journals » Infection and Drug Resistance » Volume 16
Effect of Follow-Up Cerebrospinal Fluid Cultures in Post-Neurosurgical Patients’ Outcome with Gram-Negative Bacterial Meningitis/Encephalitis
Authors Sun J, Shi Y, Ding Y, Wang S, Qian L, Luan X, Li G, Chen Y, Li X, Lv H, Zheng G, Zhang G
Received 4 July 2023
Accepted for publication 7 September 2023
Published 22 September 2023 Volume 2023:16 Pages 6285—6295
DOI https://doi.org/10.2147/IDR.S425799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jialu Sun,1 Yijun Shi,1 Yaowei Ding,1 Siqi Wang,1 Lingye Qian,2 Xin Luan,1 Guoge Li,1 Yuxin Chen,1 Xiaotong Li,1 Hong Lv,1,3,4 Guanghui Zheng,1,3,4,* Guojun Zhang1,3,4,*
1Laboratory, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Laboratory, Beijing An Zhen Hospital, Capital Medical University, Beijing, People’s Republic of China; 3NMPA Key Laboratory for Quality Control of in vitro Diagnostics, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Beijing Engineering Research Center of Immunological Reagents Clinical Research, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanghui Zheng; Guojun Zhang, Beijing Tiantan Hospital, NO. 119 Nansihuan West Road, Fengtai District, Beijing, People’s Republic of China, Tel +86 18600148997 ; +86 13811792425, Email [email protected]; [email protected]
Background: To investigate the factors associated with follow-up CSF cultures (FUCCs) in post-neurosurgical patients with gram-negative bacterial meningitis/encephalitis and the effect of FUCCs on treatment management and patient outcomes.
Methods: This single-centered retrospective cohort study enrolled post-neurosurgical patients with gram-negative bacterial meningitis/encephalitis at a tertiary-care university hospital between 2012 and 2022. The risk factors for 28-day mortality were evaluated using multivariate Cox analysis. FUCC-related risk factors were also analyzed.
Results: Among the 844 enrolled patients, 504 (59.7%) underwent FUCC, and FUCC was found to be associated with lower rates of both all-cause (hazard ratio (HR) 0.391; 95% confidence interval (CI), 0.235– 0.651; p< 0.001) and attributable mortality (HR 0.463; 95% CI, 0.239– 0.897; p=0.023) in Post-neurosurgical patients diagnosed with Gram-negative bacterial meningitis/encephalitis. Moreover, the results of the study underscored that patients with persistent gram-negative bacterial meningitis/encephalitis had a lower all-cause/attributable short-term survival rate according to 28-day mortality Kaplan–Meier analysis (P=0.001/0.006).
Conclusion: Performing FUCC has been demonstrated to lower mortality rates in Post-neurosurgical patients suffering from Gram-negative bacterial meningitis/encephalitis. The higher mortality rate observed in patients with persistent gram-negative bacterial meningitis/encephalitis suggests that performing FUCC is a crucial component of proper patient care and management, and is therefore recommended for use by clinicians as a standard practice. This finding underscores the significance of consistent implementation of FUCC in the management and prognosis of patients with Post-neurosurgical infections.
Keywords: gram-negative bacterial meningitis/encephalitis, follow-up cerebrospinal fluid cultures, all-cause 28-day mortality, persistent meningitis/encephalitis, risk factors
Introduction
In patients who undergo invasive operations such as drainage tube insertion, disruptions in the cranial closure state can predispose them to Gram-negative bacterial meningitis/encephalitis. Consequently, these patients can have a negative effect on their recovery, increase medical costs, consume medical resources, and increase postoperative mortality rates1–3 (Emerson et al, 2012; Hu et al, 2019; van et al, 2022). Intracranial infections occur in 3% to 20% of patients admitted to neurosurgical intensive care units (NICUs), with bacterial infections being the main type of central nervous system infections (CNSIs)4 (Shaban et al, 2016). Reports have shown that most Gram-negative bacteria isolated from neurosurgical intracranial infections were Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa, accounting for 42.1% of the pathogens5 (Wang et al, 2014). Furthermore, the escalation and long-term use of antimicrobials, as well as prolonged hospitalizations, has led to an increase in intracranial infections caused by Gram-negative bacteria, which pose a greater challenge to treat than Gram-positive bacteria because of their resistance to antibiotics and production of highly virulent toxins. To illustrate, Tuon et al reported a mortality rate of 72.7% for nosocomial A. baumannii meningitis/encephalitis6 (Tuon et al, 2010). Therefore, the identification of high-risk Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis, combined with early and effective anti-infection treatment, is crucial to reducing mortality rates and improving patient prognosis7 (Vetter et al, 2020).
Moreover, it has been strongly suggested that follow-up blood cultures (FUBC) for particular pathogens, such as Staphylococcus aureus for ruling out multiple bloodstream infections (BSI) is related to positive prognosis8 (Van Goethem et al, 2022). Conversely, performing FUBCs in patients with gram-negative (GN) BSIs is contentious9–12 (Maskarinec et al, 2020; Kang et al, 2011; Canzoneri et al, 2017; Mitaka et al, 2022). Similar to BSI, gram-negative bacterial meningitis/encephalitis is associated with body fluid infection, wherein follow-up CSF cultures (FUCCs) may be clinically important. However, the role of FUCC in the management of Gram-negative bacterial meningitis/encephalitis is not yet known. The specific definition of follow-up CSF cultures (FUCC) in our study population was a repeated CSF cultures obtained between 24 h and 72 h after the index CSF culture.
Therefore, this study aimed to establish a cohort to evaluate the relationship between FUCC and patient prognosis, and its associated factors. To the best of our knowledge, this is the first global cohort study to evaluate the clinical significance of FUCC.
Methods
Study Design and Setting
We conducted a retrospective cohort of Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis between January 2012 and January 2022. We conducted the study at the Beijing Tiantan Hospital, affiliated with Capital Medical University, which is a tertiary care institution and houses the largest neurology and neurosurgery centers in Asian.
The attending physicians requested an index and FUCCs based on clinical judgment without being indicated by the study protocol. A microbiological database was used to identify pathogens. Clinical charts and hospital records were reviewed to collect the study variables. FUCC is defined as obtaining one and more CSF cultures repeatedly 24–72h after the index CSF cultures. An investigator systematically checked the accuracy of the data before uploading onto the database.
The local institutional ethics committee approved this study. Informed consent was not required because the data were collected anonymously.
Study Population
All adult Post-neurosurgical patients (≥18 years of age) with gram-negative bacterial meningitis/encephalitis, and one or more positive CSF cultures obtained to rule out infection, were eligible for inclusion. They were evaluated only once during their first episode (index CSF culture).
The inclusion criteria were as follows:
Positive CSF culture results in Gram-negative bacteria and a CSF leukocyte count of > 250 cells/L to confirm CNSI13,14 (Tunkel et al, 2017; Hernández Ortiz et al, 2018).
The exclusion criteria were as follows: (1) patients <18 years, (2) those with polymicrobial CNSI, (3) those with insufficient data, and (4) those experiencing death within 24 h after drawing index CSF for cultures (Figure 1).
 |
Figure 1 Flow diagram of the study cohort. Abbreviation: FUCC, follow-up cerebrospinal fluid culture. |
Variables and Definitions
We used the Beijing Tiantan Hospital clinical database to collect demographic data and medical history, including age, sex, index CSF culture result, FUCC result, infectious pathogens identified, presence of tumor, malignancy, diabetes, and hypertension, traumatic brain injury, duration of surgery, requirement of reoperation, specifics of craniotomy, ICU admission, CSF leakage, extra-ventricular drainage (EVD), and lumbar drainage (LD), mechanical ventilation. Peripheral venous blood and CSF were used to measure leukocytes (C-Leu), neutrophils (C-Neu), protein (C-Pro), and glucose (C-Glu, B-Glu). The primary outcome was 28-day mortality, defined as all-cause mortality within 28 days of the index CSF cultures.
De-escalation therapy: De-escalation was defined as changing an initially covering antibiotic regimen to a narrower spectrum regimen based on index/follow-up antibiotic susceptibility testing (AST) results within 96 hours.15
Peripheral blood samples were collected in the morning after the patients fasted for 12-hours. A lumbar puncture was used to collect the CSF samples. CNSI was classified according to the Infectious Diseases Society of America (IDSA) standards.
Microbiology
All pathogens were classified using standard microbial identification procedures, using the identification systems, VITEK-2 Compact system (bioMerieux, Marcy l ‘etoile, France; based on biochemical reactions) and VITEK MS (bioMerieux, Marcy l ‘etoile, France; based on matrix-assisted laser desorption/ionization time-of-flight mass spectrometry).
Statistical Analysis
For the primary endpoint, univariate and multivariate Cox analyses were used to investigate risk factors for death within 28 days. After validating the proportional hazards and multicollinearity, all variables in the univariate analysis with P < 0.05, were incorporated into a multivariable Cox regression model. Analysis was conducted with the data from the day of CSF culture indexing until death or 28 days later. SPSS 26.0 (IBM, Armonk, NY, USA) and R Studio (version 3.6.1) were used for the analyses. The number of days from the first CSF bacteria positive culture to death in the hospital within 28 days was displayed on Kaplan–Meier curves, and the rates of survival were compared using Log rank testing.
Patients with and without FUCC were compared using the Mann–Whitney and Kruskal–Wallis tests for continuous variables, and the Pearson chi-square or Fisher exact test for categorical variables. Next, we compared the three groups: “positive FUCC”, “negative FUCC”, and “without FUCC”. Patients with positive FUCC results for a pathogen other than the pathogen discovered in the index CSF cultures were excluded from this analysis. In this descriptive analysis, categorical variables are expressed as absolute numbers and relative frequencies. When continuous variables were normally distributed, they are presented as means and standard deviations. When they were not normally distributed, they are presented as median and interquartile range (IQR).
Result
Factors Affecting Survival Among All Patients
The included 844 patients were categorized into the survival and non-survival groups, the potential mortality risk and protective factors screened out were FUCC (p=0.002), C-Leu (p=0.033), C-Pro (p<0.001), CSF to blood glucose ratios (p<0.001), AST (p<0.001), Traumatic Brain injury (p=0.031), Hypertension (p=0.003), Reoperation (p<0.001), Craniotomy (p=0.010), ICU admission (p<0.001), EVD (p=0.009), LD (p=0.008) and Mechanical ventilation (p<0.001)(Table 1). It is worth noting that after the 28-day mortality Kaplan–Meier analysis of patients, we discovered FUCC has a significant difference in both all-cause and attributable mortality between the two groups (p=0.001/0.006) (Figure 2A and B). Furthermore, a risk factor analysis of death in Post-neurosurgical patients with gram-negative bacterial meningitis/encephalitis was performed using propensity score-weighted multifactorial Cox proportional hazards. Obtaining FUCCs was found to be associated with lower rates of both all-cause (hazard ratio (HR) 0.391; 95% confidence interval (CI), 0.235–0.651; p<0.001) and attributable mortality (HR 0.463; 95% CI, 0.239–0.897; p=0.023). Hypertension (HR 1.778; 95% CI, 1.025–3.083; p=0.040), Reoperation (HR 1.719; 95% CI, 1.008–2.930; p=0.047), ICU admission (HR 3.703; 95% CI, 1.812–7.566; p<0.001) and Mechanical ventilation (HR 3.649; 95% CI, 1.890–7.046; p<0.001) are the mortality risk factors. In addition, antibiotic resistance other than ESBLs and Carbapenem-resistance (HR 0.276; 95% CI, 0.105–0.730; p=0.009), as well as the all sensitive group (HR 0.081; 95% CI, 0.034–0.191; p<0.001), were protective factors for mortality in post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis. More details from survival analysis were shown in Figure 2C and D.
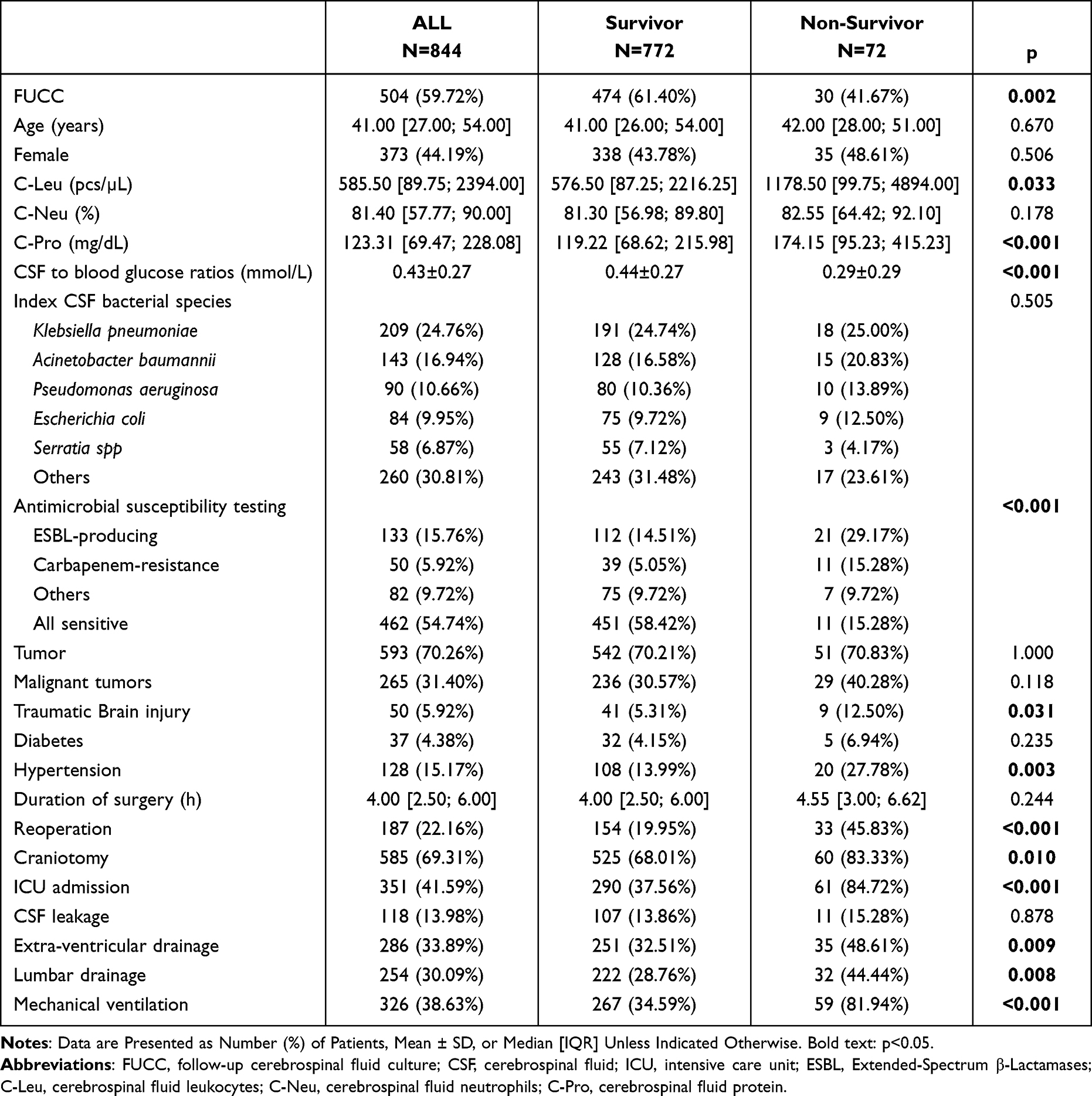 |
Table 1 Comparison of the Factors of the Non-Survivor Group versus the Survivor Group |
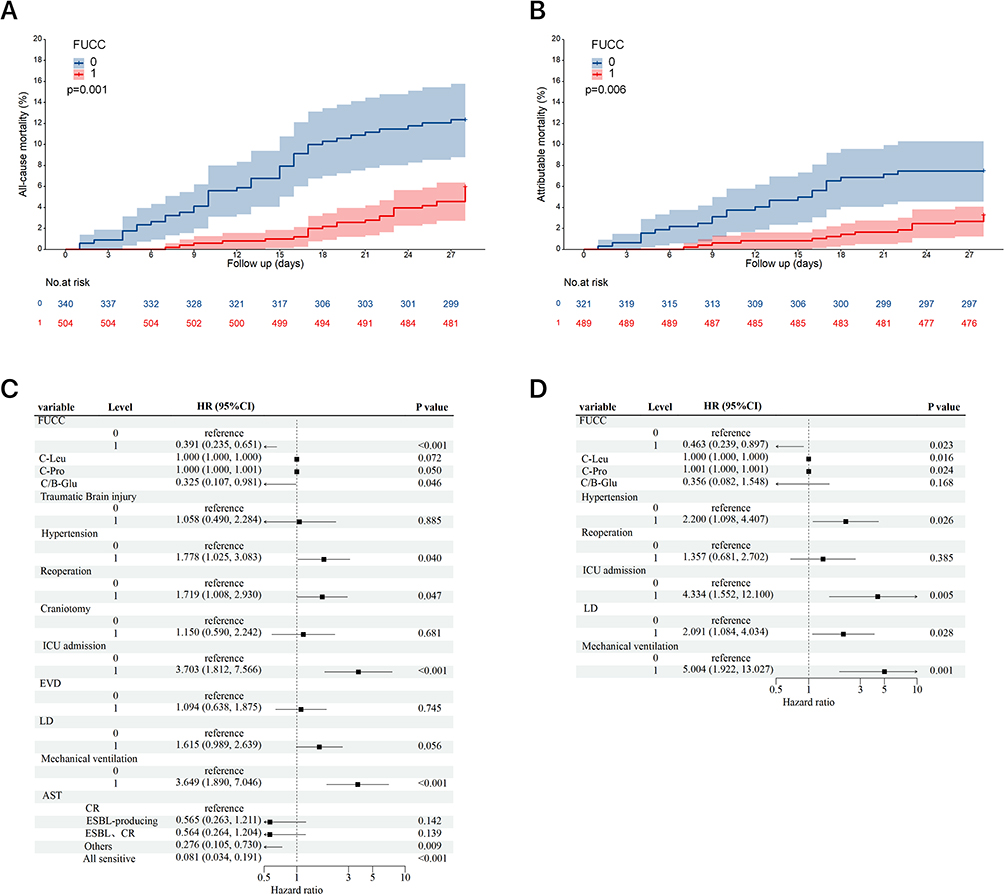 |
Figure 2 Differences in unadjusted Overall 28-day (A) all-cause and (B) attributable in-hospital mortality in post-neurosurgical patients with gram-negative bacterial meningitis/encephalitis. Differences in hazard ratios of (C) all-cause and (D) attributable in-hospital mortality in patients with GNB, as determined by propensity score weighted Cox proportional hazards analyses. Abbreviations: FUCC, follow-up cerebrospinal fluid culture; CI, confidence interval; C/B-Glu, CSF to blood glucose ratios; EVD, Extra-ventricular drainage; LD, Lumbar drainage; AST, Antimicrobial susceptibility testing; CR, Carbapenem-resistance. |
Patient Characteristics and Factors Linked to FUCC Acquisition
Of the 1069 Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis, 225 were excluded (42 patients had co-infections, 83 with incomplete case information or laboratory data, 23 died within 24 h of the initial CSF culture, and 77 were aged < 18 years).
Of the 844 patients enrolled, 504 (59.7%) had FUCC (Figure 1). The clinical features of the patients with FUCC differed considerably from those without (Table 2). Overall, patients with FUCC were significantly more likely to have higher C-Leu (248.00 [39.75; 1629.50] / 818.00 [180.25; 3148.00]; p<0.001), C-Neu (75.10 [43.40; 87.50] / 84.00 [68.88; 90.93]; p<0.001, C-Pro (109.65 [59.15; 196.96] / 136.00 [77.52; 240.05]; p=0.001). Patients with FUCC had more CSF leakage (37/81; p=0.042), EVD (92/194; p=0.001), LD (87/167; p=0.023), Mechanical ventilation (147/179; p=0.029) than those without performing FUCC (Table 2).
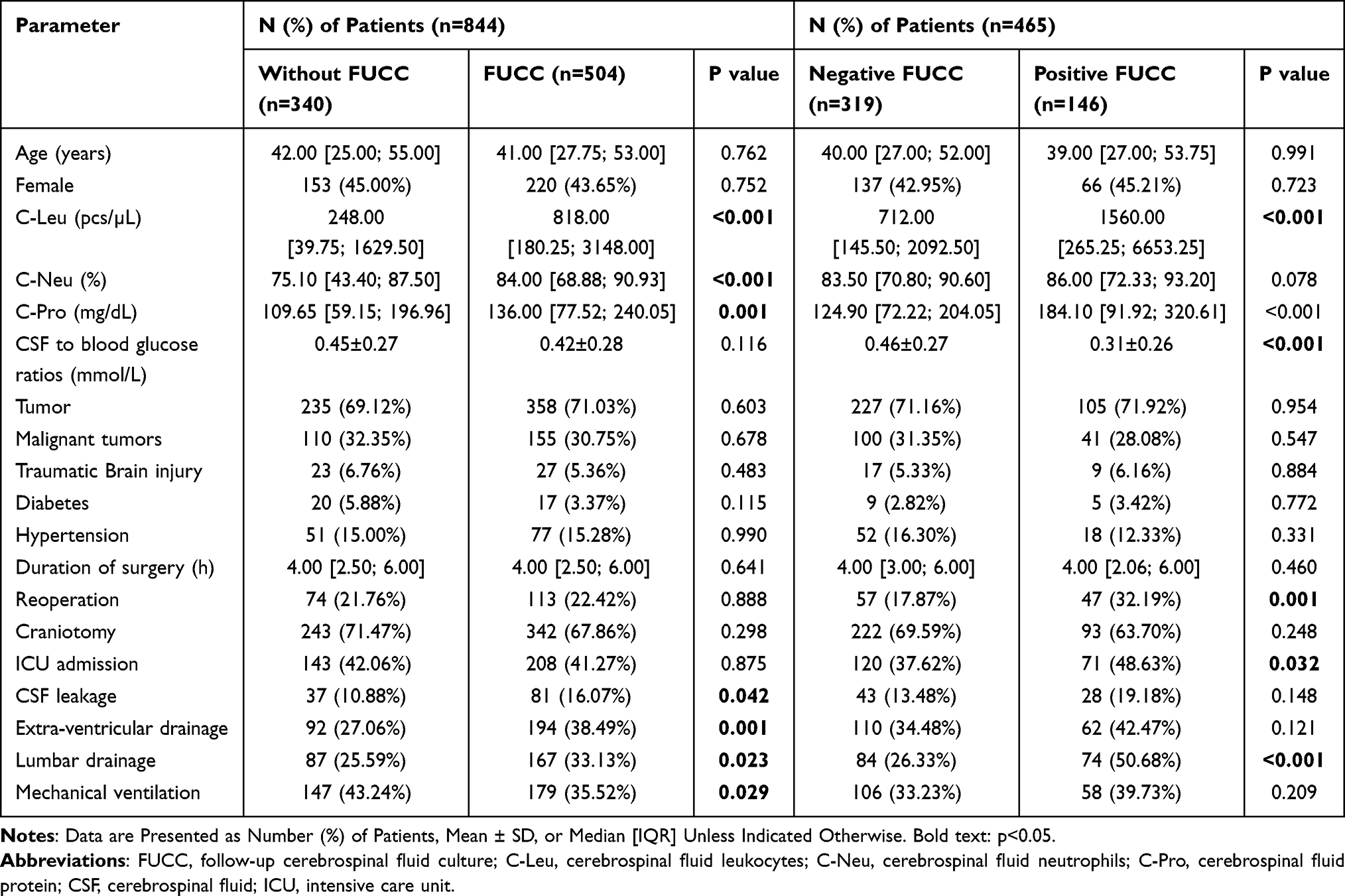 |
Table 2 Post-Neurosurgical Patients with Gram-Negative bacterial Meningitis/Encephalitis with and without Follow-Up Cerebrospinal Fluid Cultures (FUCC) |
We compared the antibiotic applications performed within 96 hours of obtaining the antibiotic susceptibility testing (AST) between patients who underwent FUCC and those who did not and found a significant difference between the two groups. Among them, clinicians performed de-escalation antibiotic therapy in 159 (31.5%) of patients who underwent FUCC, which was significantly higher than in patients who did not undergo FUCC (p=0.031). Besides, patients with FUCC cost less during hospitalization (65,178.20 [39,514.00; 92,327.80]/67,392.07 [33,982.48; 73,720.54]; p=0.09)(Table 3).
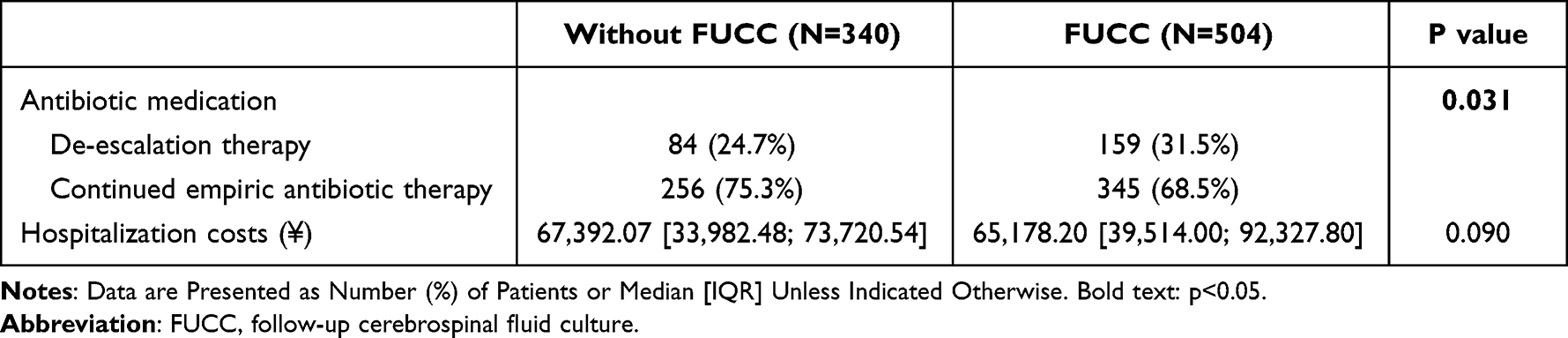 |
Table 3 Antibiotic Therapy and Hospitalization Costs with and without Follow-Up Cerebrospinal Fluid Culture (FUCC) |
The bacteria isolated from FUCC of Post-neurosurgical patients with gram-negative bacterial meningitis/encephalitis were mainly Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Escherichia coli, and Serratia spp. (Figure 3).
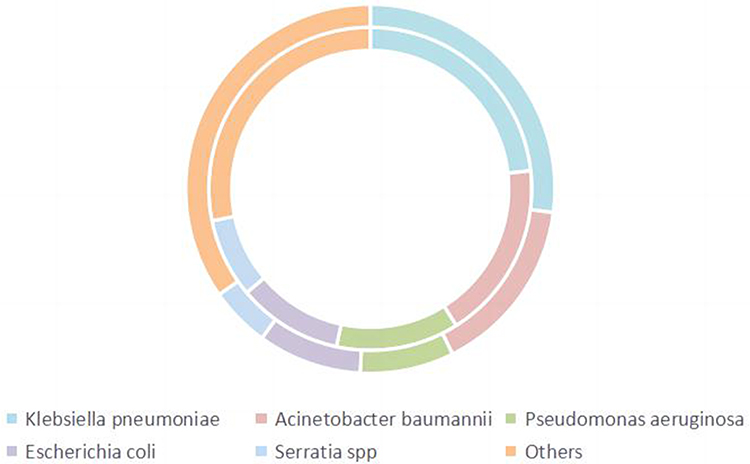 |
Figure 3 Bacterial species in patients with FUCC (Out ring: FUCC, inner ring: Without FUCC). Abbreviation: FUCC, follow-up cerebrospinal fluid culture. |
Among the patients who underwent FUCC, 39 patients had different bacteria grow from the repeat culture. The ratio of patients with different culture results underwent EVD are higher than those possess the same culture bacteria significantly (22, 56.41%; 172, 36.99%, p=0.017). (Supplemental Table 1)
Factors Affecting Survival Among Patients with FUCC
The included 504 patients were categorized into the survival and non-survival groups, the potential mortality risk and protective factors screened out were FUCC positive (p=0.001), C-Glu (p=0.001), B-Glu (p<0.001), Hypertension (p=0.016), ICU admission (p<0.001), LD (p<0.001) and Mechanical ventilation (p<0.001) (Supplemental Table 2). We further compared 28-day mortality rate between the positive and negative FUCC groups, and the findings indicated a significant difference in both all-cause and attributable mortality between the two groups (p<0.001/=0.06), whereas FUCC positive was linked to a lower short-term survival rate (Supplemental Figure 1). However, when we perform a risk factor analysis of death in FUCC using propensity score-weighted Cox proportional hazards, the results indicated FUCC positive is not a predictor of mortality (hazard ratio (HR) 2.159; 95% confidence interval (CI), 0.669–7.196; p =0.194, 0.557–3.695; p=0.455), other details were presented in Supplemental Figure 2.
Factors Influencing Positive vs Negative FUCC
Patients with positive FUCC had higher C-Leu (712.00 [145.50; 2092.50] / 1560.00 [265.25; 6653.25]; p<0.001), C-Pro (124.90 [72.22; 204.05] / 184.10 [91.92; 320.61]; p<0.001), CSF to blood glucose ratios (0.46±0.27 / 0.31±0.26; p<0.001). Patients with positive FUCC had more reoperation (57/319, 17.87% vs 47/146, 32.19%; p=0.001), ICU admission (120/319, 37.62% vs 71/146; 48.63%; p=0.032) and LD (84/319, 26.33% vs 74/146, 50.68%; p<0.001) (Table 2).
Discussion
Patients who undergo neurosurgery are at an increased risk of developing hospital-acquired central nervous system infections (CNSI), particularly intracranial infections resulting from traumatic brain injury and neurosurgical procedures. Based on a national study, the incidence of intracranial infection after neurosurgery was 14.81%. These infections are associated with high rates of disability and mortality. Recent data indicate that CNSI caused by Gram-negative bacteria are on the rise, and patients who develop these infections have a high risk of death. For instance, Erdem et al16 reported a mortality rate of 45% among patients with A. baumannii meningitis/encephalitis. To diagnose CNSI in these patients, positive bacterial culture of specimens like cerebrospinal fluid, implants, and drain tips are considered the gold standard. Despite this, meeting clinical needs is challenging due to the low positivity rate and time-consuming nature of the test. Başpınar et al17 observed this problem in their recent study.
FUCC was found to be an independent protective factor in the results of survival analysis adjusted for important covariates. In addition, a 28-day mortality Kaplan-Meier analysis demonstrated that FUCC was associated with lower short-term mortality. These findings are consistent with previous studies on FUBC in gram-negative bacteremia (GNB). For instance, Maskarinec et al9 used propensity score-weighted Cox proportional risk models in 1702 GNB patients, revealing that access to FUBC was linked to reduced all-cause and attributable mortality. Giannella et al18 further confirmed this link in 274 GNB patients matched for severity. Similarly, our study showed that patients lacking FUCC had a higher mortality rate, suggesting a missed opportunity for source control, complication identification, and optimization of antimicrobial agent management. In specific cases, such as with postoperative extraventricular drainage, shunt devices, and Ommaya capsules. We conducted an analysis on antibiotic use in patients within 96 hours after FUCCs were performed and antibiotic susceptibility testing (AST) results were obtained. Our findings revealed a higher proportion of patients undergoing antibiotic de-escalation after FUCCs. De-escalation refers to adjusting empirical antibiotic therapy to the narrowest spectrum based on AST results. Furthermore, we observed that the mean hospitalization cost for patients who underwent FUCC was lower compared to those who did not, although this difference was not statistically significant. Nonetheless, it demonstrates a certain tendency. It is plausible that with more precise treatment, the overall duration of the patient’s illness would be shortened. Similar conclusions were obtained in a previous review15,19 on antibiotic de-escalation in bloodstream infections and pneumonia, observational studies show lower mortality following antibiotic de-escalation guided by culture results among patients with bacteraemia. Apart from this, FUCC can facilitate the prompt removal of persistent CNSI to prevent further complications. For instance, in cases where the infection involves bone flaps, cranial osteomyelitis, and post-cranioplasty infection, bone flaps and artificial implants can be removed to minimize the likelihood of more serious complications. CNSI are highly susceptible to seizures and have a high mortality rate. As such, the typical duration of treatment for these infections is four to eight weeks, and antimicrobial therapy should continue for one to two weeks after criteria for clinical cure have been met. Patients who have higher levels of C-Leu, C-Neu, and C-Pro, and are more susceptible to experiencing CSF leakage, EVD, LD, and mechanical ventilation. Consequently, these patients are more likely to undergo FUCC. The findings suggest that timely implementation of FUCC is associated with adjustments in antibiotic therapy to achieve precision treatment and improved short-term survival outcomes. This indicates that patients with more severe clinical conditions are more likely to benefit from FUCC, as it allows for close monitoring of their condition, shorter illness duration, and more targeted therapy.
At the same time, we identified 39 patients with FUCC results that differed from the index culture. Upon reviewing the treatment course of these patients, we observed that clinicians did not modify the anti-infective treatment regimen after receiving the FUCC results. However, it is noteworthy that the majority of these patients demonstrated improvement in their condition. Furthermore, the FUCCs from these 39 patients exhibited diverse pathogen types, including coagulase-negative staphylococci, which have a 60% probability of contamination. So the possibility of operational contamination cannot be disregarded. To investigate the impact of cerebrospinal fluid (CSF) retention sites on the culture results, we compared the types of central nervous system infections (CNSIs) in these 39 patients with those who had concordant repeat culture results. Interestingly, patients who underwent external ventricular drainage (EVD) were more likely to exhibit different repeat culture results, with a significant difference observed between the two groups. EVD-associated CNSIs are prone to more complicated infections as well as other complications, which may have contributed to this result.20
FUCC positivity is defined as Persistent Gram-negative bacterial meningitis/encephalitis in this study. The Cox proportional hazard analysis using propensity score weighting revealed that FUCC positivity was not a predictor of mortality, which may be due to the insufficient sample size. However, the Kaplan-Meier analysis demonstrated that patients with persistent Gram-negative bacterial meningitis/encephalitis had a higher mortality rate than FUCC-negative patients, both in terms of infection-related death and all-cause mortality, consistent with previous research21 on carbapenem-resistant Gram-negative bloodstream infections. The review22 (Gatti et al, 2023) that collected data from a total of 11 observational studies reiterated similar conclusions. Therefore, we believe that FUCC is useful in identifying those at high risk of poor prognosis and that, upon a positive FUCC result, these patients should receive more aggressive and precise treatment. Furthermore, LD, ICU admission, and mechanical ventilation were found to be independent predictors of death according to multivariate analysis.
Our study found FUCC positive in 31.3% of all patients, which is much higher than the rate of FUBC that has been reported so far. Maskarinec et al9 found that only about 20% of patients with GNB infection underwent FUBC, which laterally indicates that GN-CNSI is not easily cured by antibiotic therapy and that the infection progresses rapidly and is more severe. In addition to this, the changes in inflammatory laboratory indicators were more significant in patients who underwent FUCC, especially the significant decrease in CSF glucose was highly indicative of infection23 (Davis et al, 2018). In terms of some clinical operations, patients who underwent FUCC had more CSF leakage symptoms and performed more EVD and LD operations, which are themselves an invasive adjuvant therapy with exposed incisions, and therefore their infections are less likely to be cured, with high requirements for aseptic maintenance and possible contamination of certain medical origin. In contrast, there is a significant difference in inflammatory indexes in the CSF of FUCC-positive patients compared to negative patients, we reviewed the literature and found that FUBC-positive patients with bacteremic urinary tract infection (UTI), usually showed higher initial inflammatory markers, longer time for fever reduction, more frequent ICU admissions, and a higher chance of cancer24 (Shi et al, 2019). Also, FUCC-positive patients underwent more reoperation and more ICU admissions. This echoes the findings of Jeannie et al25 for Follow-up blood cultures in E. coli and Klebsiella spp. Bacteremia, the study indicated that FUBC-positive patients are more likely to have an intravascular source of infection, cardiac device and hemodialysis dependency, and are associated with an increased risk of death. Although there is no clear evidence from the literature on FUCC and Gram-negative bacterial meningitis/encephalitis, the study of GN-BSI also provide side evidence of the reliability of our findings.
Expert consensus on the diagnosis and management of infections in China indicates positive bacterial cultures of specimen smears, drains tips, implants and cerebrospinal fluid are the gold standard for diagnosis, but contamination and colonization need to be excluded. Despite the rapid development of new technologies such as metagenomics next generation sequencing (mNGS) and multiplex PCR in the diagnosis of CNSI, there is still no substitute for the therapeutic guidance of CSF culture in CNSI. This study emphasizes the importance of using CSF culture appropriately to maximize therapeutic benefits for Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis. Further exploration of this topic is warranted.
Our study had limitations. First, this was a single-centered retrospective study with the possibility of unmeasured confounding factors. Second, we determined the rate of persistent Gram-negative bacterial meningitis/encephalitis using cultural methods such as identifying families and species. Although we reduced survival bias in various ways, it could not be eliminated. Finally, given a large number of tested hypotheses, it is crucial to highlight that the p-value may still imply false-positive results.
Nevertheless, this study is the first to analyze the FUCC role in Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis. Our study found that FUCC is an independent protective factor of death. Patients with persistent Gram-negative bacterial meningitis/encephalitis are linked to higher mortality, which indicate that perform FUCC contributes to the prognosis of patients and is worthy of general promotion by clinicians in managing patients. FUCC is commonly used in patients with more severe infections, possess CSF leakage symptoms and perform EVD, LD operations. In contrast, FUCC positive patients tend to undergo reoperation and ICU admission, and are more susceptible to A. baumannii infection. Further studies are required to confirm whether FUCC can be used as a standard diagnostic measure for Post-neurosurgical patients with Gram-negative bacterial meningitis/encephalitis. Our study underscore the importance of incorporating FUCC into clinical practice as a valuable tool for guiding treatment decisions and improving patient outcomes. Further research is warranted to explore the long-term benefits and cost-effectiveness of FUCC in larger patient populations.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are not publicly available due to individual privacy could be compromised, but they are available from the corresponding author (Guojun Zhang) on reasonable request.
Patient Consent Statement
Our study has been conducted in accordance with the Declaration of Helsinki and been approved by the Beijing Tiantan Hospital of Capital Medical University. We performed a retrospective analysis of patient clinical information and did not conduct experiments on patient specimens. The data of the patients were maintained with confidentiality. In this study, only the medical records obtained from previous clinical treatment were used for retrospective analysis, and there was almost no risk to the patients. Considering of these reasons, after consultation with the Ethics Committee of Beijing Tiantan Hospital of Capital Medical University, written patient consent was not required.
Funding
This study was supported by Beijing Hospital Authority Clinical Medicine Development of Special Funding (grant no. ZYLX202108), Beijing Municipal Administration of Hospitals Incubating Program (grant no. PX2022021), Beijing Municipal Natural Science Foundation (code: NO.7222052), Beijing Hospitals Authority’s Ascent Plan (DFL20220505), Medical Talent Program for High-hroughput Sequencing Technology in Infectious Diseases, China(Grant No. MTP2022A011) and Beijing High-level Public health technical Personnel Training program (2022-2-013).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Emerson CB, Eyzaguirre LM, Albrecht JS, Comer AC, Harris AD, Furuno JP. Healthcare-associated infection and hospital readmission. Infect Control Hosp Epidemiol. 2012;33(6):539–544. doi:10.1086/665725
2. Hu Y, He W, Yao D, Dai H. Intrathecal or intraventricular antimicrobial therapy for post-neurosurgical intracranial infection due to multidrug-resistant and extensively drug-resistant Gram-negative bacteria: a systematic review and meta-analysis. Int J Antimicrob Agents. 2019;54(5):556–561. doi:10.1016/j.ijantimicag.2019.08.002
3. van de Beek D, Brouwer MC, Koedel U, Wall EC. Community-acquired bacterial meningitis/encephalitis. Lancet. 2021;398(10306):1171–1183. doi:10.1016/S0140-6736(21)00883-7
4. Shaban-Nejad A, Mamiya H, Riazanov A, et al. From cues to nudge: a knowledge-based framework for surveillance of healthcare-associated infections. J Med Syst. 2016;40(1):23. doi:10.1007/s10916-015-0364-6
5. Wang JH, Lin PC, Chou CH, et al. Intraventricular antimicrobial therapy in postneurosurgical Gram-negative bacillary meningitis/encephalitis or ventriculitis: a hospital-based retrospective study. J Microbiol Immunol Infect. 2014;47(3):204–210. doi:10.1016/j.jmii.2012.08.028
6. Tuon FF, Penteado-Filho SR, Amarante D, Andrade MA, Borba LA. Mortality rate in patients with nosocomial Acinetobacter meningitis/encephalitis from a Brazilian hospital. Braz J Infect Dis. 2010;14(5):437–440. doi:10.1016/S1413-8670(10)70090-8
7. Vetter P, Schibler M, Herrmann JL, Boutolleau D. Diagnostic challenges of central nervous system infection: extensive multiplex panels versus stepwise guided approach. Clin Microbiol Infect. 2020;26(6):706–712. doi:10.1016/j.cmi.2019.12.013
8. Van Goethem S, Boogaerts H, Cuykx M, et al. Follow-up blood cultures in Staphylococcus aureus bacteremia: a probability-based optimization. Eur J Clin Microbiol Infect Dis. 2022;41(10):1263–1268. doi:10.1007/s10096-022-04487-4
9. Maskarinec SA, Park LP, Ruffin F, et al. Positive follow-up blood cultures identify high mortality risk among patients with Gram-negative bacteraemia. Clin Microbiol Infect. 2020;26(7):904–910. doi:10.1016/j.cmi.2020.01.025
10. Kang CI, Song JH, Chung DR, et al. Risk factors and pathogenic significance of severe sepsis and septic shock in 2286 patients with gram-negative bacteremia. J Infect. 2011;62(1):26–33. doi:10.1016/j.jinf.2010.10.010
11. Canzoneri CN, Akhavan BJ, Tosur Z, Andrade P, Aisenberg GM. Follow-up blood cultures in gram-negative bacteremia: are they needed. Clin Infect Dis. 2017;65(11):1776–1779. doi:10.1093/cid/cix648
12. Mitaka H, Fujitani S, Kuno T, Perlman DC. Association between follow-up blood cultures for gram-negative bacilli bacteremia and length of hospital stay and duration of antibiotic treatment: a propensity score-matched cohort study. Infect Control Hosp Epidemiol. 2023;44(3):474–479. doi:10.1017/ice.2022.110
13. Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for healthcare-associated ventriculitis and meningitis/encephalitis. Clin Infect Dis. 2017;64(6):e34–e65. doi:10.1093/cid/ciw861
14. Hernández Ortiz OH, García García HI, Muñoz Ramírez F, et al. Development of a prediction rule for diagnosing postoperative meningitis/encephalitis: a cross-sectional study. J Neurosurg. 2018;128(1):262–271. doi:10.3171/2016.10.JNS16379
15. Paul M, Dickstein Y, Raz-Pasteur A. Antibiotic de-escalation for bloodstream infections and pneumonia: systematic review and meta-analysis. Clin Microbiol Infect. 2016;22(12):960–967. doi:10.1016/j.cmi.2016.05.023
16. Erdem I, Hakan T, Ceran N, et al. Clinical features, laboratory data, management and the risk factors that affect the mortality in patients with postoperative meningitis/encephalitis. Neurol India. 2008;56(4):433–437. doi:10.4103/0028-3886.44629
17. Başpınar EÖ, Dayan S, Bekçibaşı M, et al. Comparison of culture and PCR methods in the diagnosis of bacterial meningitis/encephalitis. Braz J Microbiol. 2017;48(2):232–236. doi:10.1016/j.bjm.2016.06.014
18. Giannella M, Pascale R, Pancaldi L, et al. Follow-up blood cultures are associated with improved outcome of patients with gram-negative bloodstream infections: retrospective observational cohort study. Clin Microbiol Infect. 2020;26(7):897–903. doi:10.1016/j.cmi.2020.01.023
19. Masterton RG. Antibiotic de-escalation. Crit Care Clin. 2011;27(1):149–162. doi:10.1016/j.ccc.2010.09.009
20. Ulloque-Caamaño L, Mo-Carrascal J, Maraby J, et al. Ventriculitis associated with extraventricular drainage: etiology, diagnosis and treatment focused on neurocritic care units. Cir Cir. 2019;87(2):230–240. doi:10.24875/CIRU.18000052
21. Sathya Kumar AM, George MM, Bhanuprasad K, et al. Persistent bacteremia predicts poor outcomes among neutropenic patients with carbapenem-resistant gram-negative bloodstream infections receiving appropriate therapy. Ann Clin Microbiol Antimicrob. 2023;22(1):12. doi:10.1186/s12941-023-00561-7
22. Gatti M, Bonazzetti C, Tazza B, et al. Impact on clinical outcome of follow-up blood cultures and risk factors for persistent bacteraemia in patients with gram-negative bloodstream infections: a systematic review with meta-analysis. Clin Microbiol Infect. 2023;29(9):1150–1158. doi:10.1016/j.cmi.2023.02.024
23. Davis LE. Acute Bacterial meningitis/encephalitis. Continuum. 2018;24(5):1264–1283. doi:10.1212/CON.0000000000000660
24. Shi H, Kang CI, Cho SY, Huh K, Chung DR, Peck KR. Follow-up blood cultures add little value in the management of bacteremic urinary tract infections. Eur J Clin Microbiol Infect Dis. 2019;38(4):695–702. doi:10.1007/s10096-019-03484-4
25. Chan JD, Ta A, Lynch JB, Bryson-Cahn C. Follow-up blood cultures in E. coli and Klebsiella spp. bacteremia-opportunities for diagnostic and antimicrobial stewardship. Eur J Clin Microbiol Infect Dis. 2021;40(5):1107–1111. doi:10.1007/s10096-020-04141-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.