Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Effect of Direct Antiviral Therapy Against HCV on CD4+ T Cell Count in Patients with HIV-HCV Coinfection
Authors Pinchera B ![]() , Zappulo E, Buonomo AR, Cotugno MR, Di Filippo G, Borrelli F, Mercinelli S, Villari R, Gentile I
, Zappulo E, Buonomo AR, Cotugno MR, Di Filippo G, Borrelli F, Mercinelli S, Villari R, Gentile I
Received 12 November 2022
Accepted for publication 28 January 2023
Published 4 February 2023 Volume 2023:15 Pages 23—28
DOI https://doi.org/10.2147/HIV.S395969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Biagio Pinchera, Emanuela Zappulo, Antonio Riccardo Buonomo, Maria Rosaria Cotugno, Giovanni Di Filippo, Francesco Borrelli, Simona Mercinelli, Riccardo Villari, Ivan Gentile
Department of Clinical Medicine and Surgery, Section of Infectious Diseases, University of Naples “Federico II”, Naples, Italy
Correspondence: Biagio Pinchera, Email [email protected]
Background: HCV-related liver disease is an important cause of morbidity and mortality in patients with HIV infection. It is well known that the response rates to HCV therapy are similar between HCV-monoinfected patients and HIV-HV coinfected ones. The aim of this study was to evaluate the impact of HCV eradication on CD4 + T cell count in a population of HIV-HCV coinfected patients.
Materials and Methods: We enrolled patients with HIV-HCV coinfection attending the Infectious Diseases Unit of the A.O.U. Federico II of Naples, from January 2016 to February 2019, treated with ART (AntiRetroviral Therapy) and DAAs (Direct Antiviral Agents). For each patient, we evaluated HIV and HCV viral load and CD4+ T cell count before starting therapy with DAAs, by SVR12 time and by SVR48 time. Fibrosis was evaluated by the mean of Fibroscan®.
Results: Fifty-two patients were enrolled, 40 males. Fibrosis score was F0-F3 in 15 patients and cirrhosis in the remaining 11 (all in Child-Pugh class A). All had been receiving ART, and all were treated with DAAs. Only patient who had not achieved HIV viral suppression for non-compliance also experienced a relapse of HCV infection after the end of DAAs. In all patients, we observed that the CD4+ T cell count at baseline did not show significant variations compared to SVR12 and SVR48 time. We also assessed CD4 count in relation to HIV categories and stage of liver disease, see Table 1. Also, based on the assessments of the subclasses considered, there were no significant changes in the CD4 + T cell count.
Conclusion: Our study shows that HCV viral eradication obtained with DAAs in patients with HIV-HCV coinfection is not associated with significant changes in the CD4 + T cell count, regardless of CDC category and stage of liver disease.
Keywords: HCV, HIV, fibrosis, cirrhosis, DAAs, CD4+ T cell, coinfection
Introduction
About 2.3 million people worldwide are affected by HCV/HIV coinfection, and liver disease is the leading cause of death in coinfected patients.1 Co-infection constitutes a higher risk of morbidity and mortality than HCV monoinfection, in particular, it has been seen that in co-infected patients there is a more rapid progression and evolution towards fibrosis, with a higher risk of developing liver cirrhosis and hepatocarcinoma.2,3
The advent of DAAs has been a real revolution in the history of HCV infection.4,5 While in the past there was a lower sustained virological response (SVR) among co-infected patients receiving Interferon therapy compared to monoinfected patients (18.4% −50% vs 36% −76%), current therapies with DAAs (Direct Acting Antivirals) in co-infected patients demonstrated sustained virological response (SVR) rates similar to those in patients with HCV infection alone, in particular, an SVR of 95–98% was observed among co-infected patients after treatment with DAAs, an SVR similar to 96–100% of monoinfected patients.6–8
Theoretically, since HCV has a tropism for the cells of the immune system, its elimination could lead to a functional recovery of the immune system itself. In this regard, few studies have evaluated the impact of HCV eradication with DAAs on CD4 T cell counts, in particular, J. Giròn Ortega et al observed an improvement in CD4 T cell counts only in co-infected patients without liver cirrhosis.9 The study by Bono et al highlighted a decreased activation of γδ T- and B-cells as well as increases in the Vδ2/Th17 ratio and reduced γ-globulin concentrations in coinfected patients treated with DAAs; these changes were associated with an improvement in liver function.10 In another study conducted by the ICONA Foundation Cohort, it was observed that the eradication of HCV infection after treatment with DAAs showed no impact on CD4 T cell counts.11
The aim of this study was to evaluate the impact of HCV eradication on CD4 + T cell count in a population of HIV-HCV coinfected patients.
Materials and Methods
We conducted an observational retrospective cohort study. We enrolled patients with HIV/HCV co-infection attending the Infectious Diseases Unit of the A.O.U. Federico II of Naples, from January 2016 to February 2019, treated with DAAs and antiretroviral therapy (ART). Diagnosis of HCV and HIV infection was based on the criteria established by the current International Guidelines.1,12 Fibrosis was evaluated by the mean of Fibroscan®. The severity of liver disease was graduated according to the degree of liver fibrosis by Metavir stage or clinical signs. The Metavir score was estimated with a FibroScan© exam performed within 6 months before the beginning of the antiviral treatment. Moreover, clinical cirrhosis was identified according to the presence of clinical, biochemical and ultrasound signs including a blood platelet count lower than 100,000/mm3, hypertrophy of the caudate lobe, nodularity of the liver surfaces, altered straightness of hepatic veins, ascites, porto-systemic encephalopathy, esophageal varices and ultrasound evidence characterizing liver cirrhosis. Decompensated cirrhosis was defined as a cirrhosis in Child-Pugh stage of at least B7, while advanced liver fibrosis was defined as the presence of Metavir score ≥F4 or clinical cirrhosis.13
We evaluated for each patient the epidemiological characteristics, the laboratory data and the clinical characteristics. For each patient, we evaluated HIV and HCV viral load and CD4+ T cell count on the nadir, before starting therapy with DAAs, by SVR12 time and by SVR48 time.
Data were reported as median and interquartile range (IQR) given their non-parametric distribution. For comparisons between continuous variables, the U Mann–Whitney Test was performed. Co-variates significantly associated with death at the univariate analysis were also analyzed in a multivariate model. The p-value for statistical significance was set at <0.05 for all the tests.
With respect to the ethical issues, the study was conducted in compliance with the Declaration of Helsinki and the principles of good clinical practice. For this study, informed consent was obtained from all subjects and/or their legal guardian(s). The study was approved by the “Federico II” Ethics Committee with the code number 242/19.
Results
We enrolled 52 patients. The main demographics and clinical characteristics of the patients enrolled are shown in Table 1.
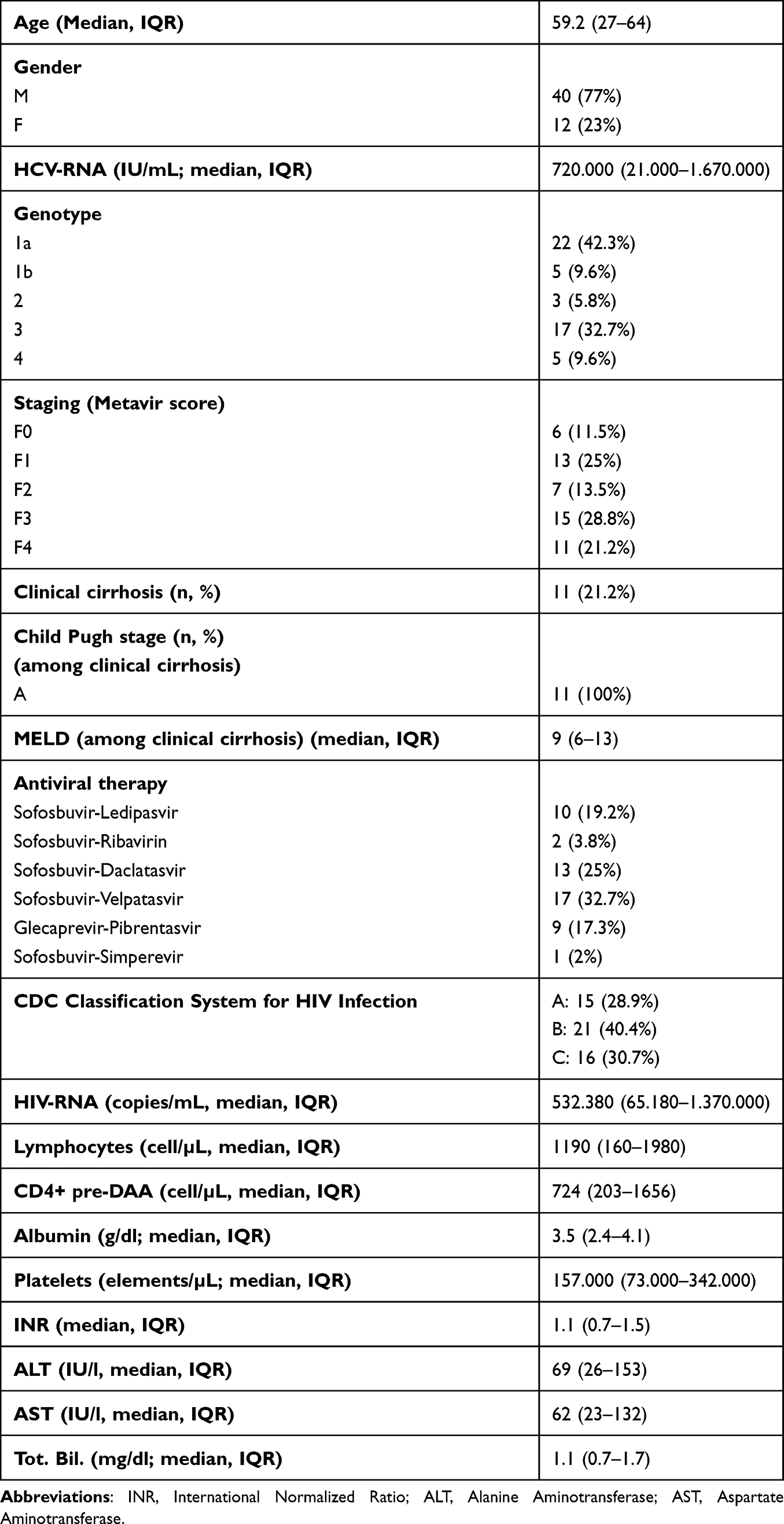 |
Table 1 Anagraphic Clinical Features of Enrolled Patients |
Of the 52 patients enrolled, 40 were male and 27 had HCV genotype 1 (22 subtype 1a), 3 HCV genotype 2, 17 HCV genotype 3, 5 HCV genotype 4). Fibrosis score was F0 in 6 patients, F1 in 13 patients, F2 in 7 patients, F3 in 15 patients and cirrhosis in the remaining 11 (all in Child-Pugh class A) (Table 1). All had been receiving ART, and all but one were virosuppressed (due to non-compliance). All were treated with DAAs (10 with Sofosbuvir-Ledipasvir, 2 with Sofosbuvir-Ribavirin, 13 with Sofosbuvir-Daclatasvir, 17 with Sofosbuvir-Velpatasvir, 9 with Glecaprevir/Pibrentasvir, 1 with Sofosbuvir-Simeprevir) and all but one achieved SVR12 and SVR48. The same patient who had not achieved HIV viral suppression for non-compliance also experimented a relapse of HCV infection after the end of DAAs.
Enrolled patients had a median with IQR of CD4 + nadir equal to 190 (16–670), while they had a CD4 + value before starting DAAs of 724 (203–1656). At the sustained virologic response (SVR12 and SVR 48) they had a CD4 + count, respectively, equal to 684 (201–1815) and 713 (117–1720) (OR for CD4+ count: 1.2, 95 CI (0.6–1.3) pre-treatment vs post-treatment at SVR12; p: 0.310 and OR for CD4+ count: 1.1, 95 CI (0.8–1.2) pre-treatment vs post-treatment at SVR48; p: 0.340) (Table 2). We evaluated the CD4 + count at the nadir, pre-DAA, at the SVR12 and at the SVR48, also in relation to the class to which the CDCs (Center for Diseases Control) belong (Table 2).
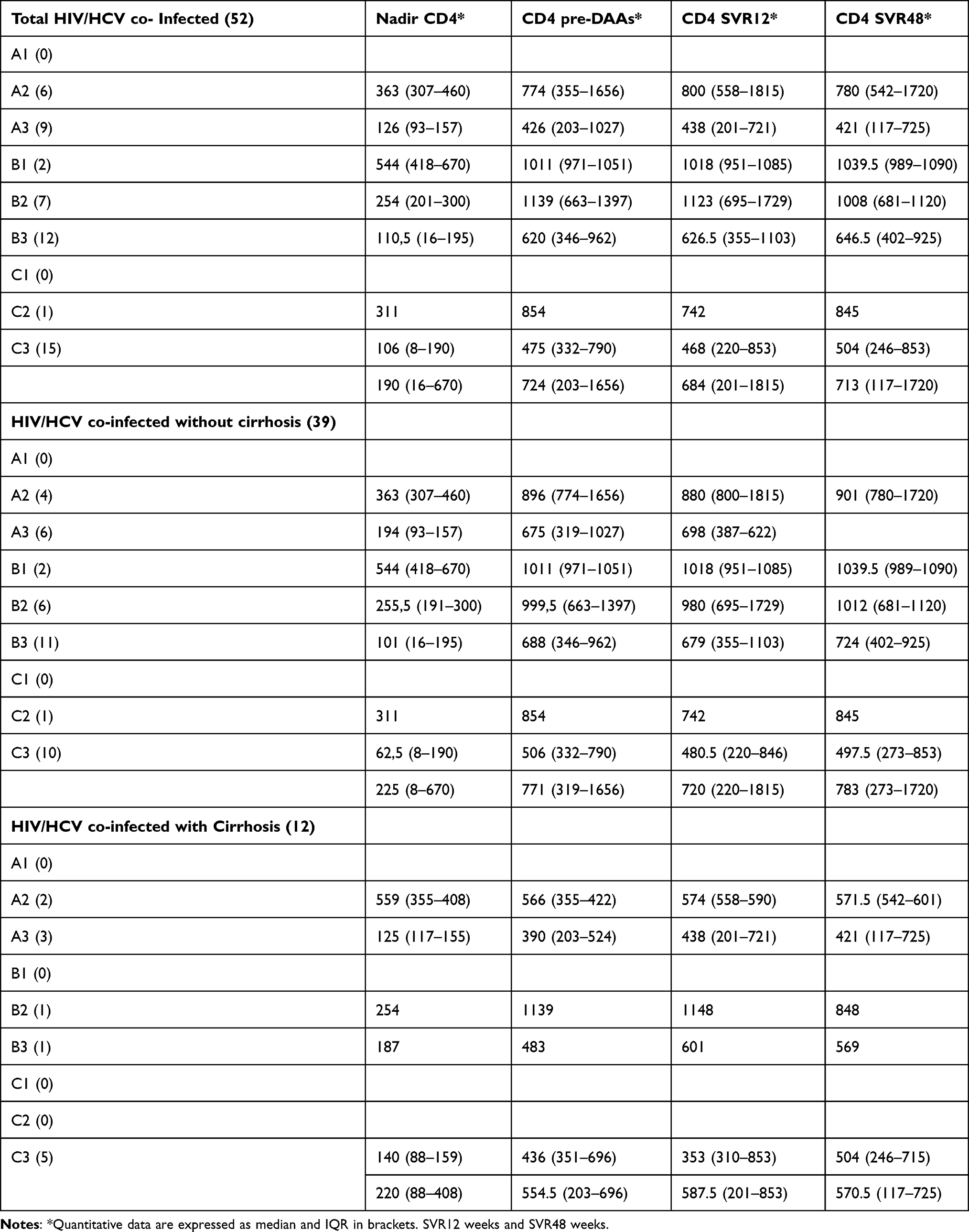 |
Table 2 CD4+ T Cell Count in Patients with HIV-HCV Coinfection by Pre-DAA, by SVR12 and by SVR48 |
The evaluation of the CD4 + count at the nadir, before the start of therapy with DAAs, at the SVR12 and at the SVR48 was also performed by distinguishing the stage of chronic liver disease, in particular, distinguishing the co-infected patients from those without cirrhosis and those with liver cirrhosis. In particular, co-infected patients without liver cirrhosis had pre-DAAs CD4 + counts equal to 771 (319–1656), while at SVR12 and SVR48 CD4 + counts, respectively, equal to 720 (220–1815) and 783 (273–1720) (OR for CD4+ count in patients without cirrhosis: 1.1, 95 CI (0.7–1.4) pre-treatment vs post-treatment at SVR12; p: 0.420 and OR for CD4+ count: 1.2, 95 CI (0.9–1.3) pre-treatment vs post-treatment at SVR48; p: 0.470) (Table 2). Instead, co-infected patients with liver cirrhosis had pre-DAAs CD4 + counts equal to 554.5 (203–696), while at SVR12 and SVR48 CD4 + counts, respectively, equal to 587.5 (201–853) and 570.5 (117–725) (OR for CD4+ count in patients with cirrhosis: 1.2, 95 CI (0.8–1.3) pre-treatment vs post-treatment at SVR12; p: 0.360 and OR for CD4+ count: 1.1, 95 CI (0.7–1.4) pre-treatment vs post-treatment at SVR48; p: 0.380) (Table 2).
Discussion
Our clinical experience confirmed the prevalence of genotype 1 among the enrolled patients, but at the same time the high prevalence of genotype 3 among co-infected patients was highlighted, probably due to the risk factors of this category of patients, in particular, intravenous drug abuse. Indeed, it is known in the literature that genotype 3 is often associated with patients with a history of intravenous drug abuse.14–17
From our data, it emerged that most of the patients with HIV/HCV co-infection had an advanced stage of liver disease, in particular, 50% of the enrolled patients had an advanced stage of liver disease (15 with F3 and 11 with liver cirrhosis).
In all patients, we observed that the CD4+ T cell count at baseline did not show significant variations compared to SVR12 and SVR48 time figures (724 vs 684, vs 713, respectively; see Table 2). We also assessed CD4 count in relation to HIV categories and stage of liver disease, see Table 2. Also, based on the assessments of the subclasses considered, there were no significant changes in the CD4 + T cell count. These data agreed with the study conducted by ICONA Foundation Studio, in which it was highlighted that the eradication of HCV infection after treatment with DAAs showed no impact on CD4 T cell counts.11 Also, in evaluating the impact of the eradication of HCV infection on the CD4 + count, distinguishing the co-infected patients without liver cirrhosis from those with no change in the CD4 + count was evident. These data contrasted with what was observed by Giròn Ortega et al that observed an improvement in CD4 T cell counts only in co-infected patients without liver cirrhosis.9
Moreover, our study has some important limitations, in particular, the small sample size and the limited observation in time. In light of what has been reported, we believe that it is essential to deepen this topic with further studies that involve a larger sample and that consider an observation longer in time.
Conclusions
Our study shows that viral eradication obtained with DAAs in patients with HIV-HCV coinfection is not associated with significant changes in the CD4 + T cell count, regardless of CDC category and stage of liver disease. Further studies with larger sample size are necessary to confirm these data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rockstroh JK, Bhagani S, Benhamou Y, et al. EACS Executive Committee. European AIDS Clinical Society (EACS) guidelines for the clinical management and treatment of chronic hepatitis B and C coinfection in HIV-infected adults. HIV Med. 2008;9(2):82–88. doi:10.1111/j.1468-1293.2007.00535.x
2. Laiwatthanapaisan R, Sirinawasatien A. Current treatment for hepatitis C virus/human immunodeficiency virus coinfection in adults. World J Clin Cases. 2021;9(18):4491–4499. doi:10.12998/wjcc.v9.i18.4491
3. Buonomo AR, Scotto R, Zappulo E, et al. Severe Vitamin D deficiency increases mortality among patients with liver cirrhosis regardless of the presence of HCC. In Vivo. 2019;33(1):177–182. doi:10.21873/invivo.11456
4. Ghany M, Morgan TR, MG; TR AASLD-IDSA hepatitis c guidance panel. Hepatitis C Guidance 2019 update: American Association for the Study of Liver Diseases-infectious Diseases Society of America recommendations for testing, managing, and treating hepatitis C virus infection. Hepatology. 2020;71::686–721. doi:10.1002/hep.31060
5. Di Minno MN, Ambrosino P, Buonomo AR, et al. Direct-acting antivirals improve endothelial function in patients with chronic hepatitis: a prospective cohort study. Intern Emerg Med. 2020;15(2):263–271. doi:10.1007/s11739-019-02163-8
6. Osinusi A, Townsend K, Kohli A, et al. Virologic response following combined ledipasvir and sofosbuvir administration in patients with HCV genotype 1 and HIV co-infection. JAMA. 2015;313:1232–1239. doi:10.1001/jama.2015.1373
7. Berenguer J, Alvarez-Pellicer J, Martín PM, et al.; González-García J GESIDA3603/5607 Study Group. Sustained virological response to interferon plus ribavirin reduces liver-related complications and mortality in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2009;50:407–413. doi:10.1002/hep.23020
8. Coppola N, Portunato F, Buonomo AR, et al. Interferon-free regimens improve kidney function in patients with chronic hepatitis C infection. J Nephrol. 2019;32(5):763–773. doi:10.1007/s40620-019-00608-z
9. Girón-Ortega J-A, Márquez-Coello M, Gutiérrez-Saborido D, Arizcorreta A, Cuesta-Sancho S, José-Antonio G-G. Modifications of CD4 T cells, CD4/CD8 ratio and serum levels of soluble CD14 in HIV-HCV-coinfected patients after sustained HCV response induced by direct-acting antiviral agents: influence of liver cirrhosis. Eur J Clin Microbiol Infect Dis. 2021;40:1863–1871. doi:10.1007/s10096-021-04237-y
10. Valeria B, Tincati C, Van Den Bogaart L, et al. Gamma-Delta T-cell phenotype and function in DAA-Treated HIV-HCV Co-Infected and HCV-mono-infected subjects. Viruses. 2022;14. doi:10.3390/v14081594
11. Bandera A, Lorenzini P, Taramasso L, et al. d’Arminio Monforte, Andrea Gori, for the icona foundation cohort. The impact of DAA-mediated HCV eradication on CD4+ and CD8+ T lymphocyte trajectories in HIV/HCV coinfected patients: data from the ICONA Foundation Cohort. J Viral Hepat. 2021;28(5):779–786. doi:10.1111/jvh.13488
12. European Association for the Study of the Liver. Electronic address: [email protected]; Clinical Practice Guidelines Panel: chair:; EASL Governing Board representative:; Panel members. EASL recommendations on treatment of hepatitis C: final update of the series. J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018
13. Dietrich CF, Bamber J, Berzigotti A, et al. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017. Ultraschall Med. 2017;38(4):e48. doi:10.1055/a-0641-0076
14. Buonomo AR, Scotto R, Pinchera B, et al. Epidemiology and risk factors for hepatitis C virus genotypes in a high prevalence region in Italy. New Microbiol. 2018;41(1):26–29.
15. Gentile I, Pinchera B, Viceconte G, et al. Hepatitis C screening in the Emergency Department of a large hospital in southern Italy: results of a pilot study. Infez Med. 2019;27(1):32–39.
16. Scotto R, Buonomo AR, Moriello NS, et al. Real-world efficacy and safety of pangenotypic direct-acting antivirals against hepatitis C virus infection. Rev Recent Clin Trials. 2019;14(3):173–182. doi:10.2174/1574887114666190306154650
17. Zappulo E, Scotto R, Buonomo AR, Maraolo AE, Pinchera B, Gentile I. Efficacy and safety of a fixed dose combination tablet of asunaprevir + beclabuvir + daclatasvir for the treatment of Hepatitis C. Expert Opin Pharmacother. 2020;21(3):261–273. doi:10.1080/14656566.2019.1697674
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Literature Review of Mathematical Models for Coinfections: Tuberculosis, Malaria, and HIV/AIDS
Inayaturohmat F, Anggriani N, Supriatna AK, Biswas MHA
Journal of Multidisciplinary Healthcare 2024, 17:1091-1109
Published Date: 13 March 2024
Prevalence of HIV, Treponema pallidum and Their Coinfection in Men Who Have Sex with Men, Medellín-Colombia
Cardona-Arias JA, Vidales-Silva M, Ocampo-Ramírez A, Higuita-Gutiérrez LF, Cataño-Correa JC
HIV/AIDS - Research and Palliative Care 2024, 16:141-151
Published Date: 18 April 2024
Hepatic Viral Reservoirs in Concurrent HIV and HBV: From Mechanistic Insight to Integrated Cure Strategies
Bobadilla R, MacLean F, Dave S, Blackard JT, Gianella S
Infection and Drug Resistance 2026, 19:576715
Published Date: 7 March 2026