")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Effect of depressive symptoms on the length of hospital stay among patients hospitalized for acute stroke in Japan
Authors Sugawara N , Metoki N, Hagii J, Saito S, Shiroto H, Tomita T, Yasujima M, Okumura K, Yasui-Furukori N, Sawada K
Received 28 June 2015
Accepted for publication 7 September 2015
Published 5 October 2015 Volume 2015:11 Pages 2551—2556
DOI https://doi.org/10.2147/NDT.S91303
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wai Kwong Tang
Norio Sugawara,1 Norifumi Metoki,2 Joji Hagii,2 Shin Saito,2 Hiroshi Shiroto,2 Tetsu Tomita,1 Minoru Yasujima,2 Ken Okumura,3 Norio Yasui-Furukori1
1Department of Neuropsychiatry, Hirosaki University School of Medicine, Hirosaki, Japan; 2Hirosaki Stroke and Rehabilitation Center, Hirosaki, Japan; 3Department of Cardiology, Hirosaki University School of Medicine, Hirosaki, Japan
Background: Depression after stroke is one of the most serious complications of stroke. Although many studies have shown that the length of hospital stay (LOHS) is a measurable and important stroke outcome, research has found limited evidence concerning the effect of depression on LOHS among patients who have experienced acute stroke. The objective of this study was to assess the effect of depression on LOHS among patients hospitalized for acute ischemic stroke in Japan.
Methods: We retrospectively examined 421 patients who had experienced acute ischemic stroke. Stroke severity was measured by the National Institutes of Health Stroke Scale (NIHSS) on the 7th day of hospitalization. On the 10th day of hospitalization, depressive symptoms and functional assessment were assessed by the Japan Stroke Scale (Depression Scale) and the Functional Independence Measure, respectively. A general linear model was employed to assess the effect of probable depression on LOHS.
Results: The prevalence of probable depression in the current sample was 16.3% in males and 17.8% in females. The mean LOHS of participants with probable depression (76.4±49.2 days) was significantly longer than that of participants without probable depression (44.9±39.2 days). An analysis using the general linear model to assess the effect on LOHS revealed a significant interaction between the presence of probable depression and NIHSS scores.
Conclusion: Depression after stroke was associated with significant increases in LOHS. Early detection and treatment for depression are necessary for patients with ischemic stroke.
Keywords: poststroke depression, length of hospital stay, ischemic stroke, Japanese
Introduction
Depression after stroke is a serious neuropsychiatric complication with a high rate of prevalence following a stroke.1,2 The symptoms of depression after stroke are similar to those of endogenous depression; depression after stroke is characterized by the rapid development and onset of symptoms, an absence of reaction to external factors, and inhibition that can affect several areas (cognitive, motor, and motivational).3 With the rapid increase in the population of elderly individuals in Japan, depression after stroke is a growing concern because depression has been regarded as a major risk factor for more functional disability4 and poor rehabilitation outcomes.5 Furthermore, a recent meta-analysis revealed the increased risk (odds ratio; 1.22) for mortality at follow-up among patients with depression after stroke.6
Researchers have increasingly recognized that the length of hospital stay (LOHS) is a measurable and important stroke outcome. In studies investigating the determinants of the direct costs of stroke care, LOHS has been used as an outcome in acute stroke trials.7,8 LOHS must be minimized for economic reasons and to ensure the quality of life of all patients and their families. Although several studies have shown the effect of depression on LOHS among patients hospitalized for acute stroke, all of those studies have come from Western countries.9–12 Furthermore, no studies have made solid corrections for confounders such as the severity of stroke, functional independence, and living status.
The objective of this investigation was to evaluate the effect of depression on LOHS among patients hospitalized for acute stroke in Japan. To the best of our knowledge, this study is the first to assess the relationship between depression and LOHS among patients with acute ischemic stroke in Japan.
Methods
Participants
We reviewed the charts of 532 patients who were admitted to the Hirosaki Stroke and Rehabilitation Center for an acute stroke between April 2012 and March 2013. The Hirosaki Stroke and Rehabilitation Center is a hospital that has both an Acute Stroke Unit and a Stroke Rehabilitation Unit and, hence, the ability to treat acute and chronic stroke. A diagnosis of stroke is based on both the presence of acute neurological symptoms and a compatible lesion found using magnetic resonance imaging (Signa EXCITE HD 1.5T; GE Medical Systems, Waukesha, WI, USA). We excluded patients with 1) serious comprehension difficulties (eg, severe aphasia), 2) hemorrhage, or 3) dementia or a history of psychiatric disease (including depression). After a detailed evaluation using the inclusion and exclusion criteria, 421 patients with acute ischemic stroke were enrolled in this study. The following information was collected for each patient: LOHS, demographics (age, sex, level of education, and living status), and stroke severity measured by the National Institutes of Health Stroke Scale (NIHSS) on the 7th day of hospitalization.13
The data collection for this study was approved by the Ethics Committee of the Hirosaki University School of Medicine and the Hirosaki Stroke and Rehabilitation Center. Informed consent was obtained from all patients before the study. The scale assessments were performed by a qualified psychiatric specialist, and the testing was confirmed by a psychiatrist and a neurologist.
Assessment of depressive symptoms and functional independence
The Japan Stroke Scale (Depression Scale) (JSS-D), which was developed by the Japan Stroke Society, was administered to all participants to measure their depressive status.14 JSS-D is a seven-item (mood, feelings of guilt, interest, apathy, anxiety, sleeplessness, and expression) objective measure in which three choices are given for each item. The total score denoting the degree of depression was calculated according to the proper weight of each choice. Probable depression was defined as a score of 2.4 or higher. The scores of JSS-D were significantly correlated with those of the Hamilton Depression Scale (HAM-D17). In addition, the scores of JSS-D were significantly correlated with those of HAM-D17 even in patients having depression without depressed mood, feeling of guilt, and suicide. Furthermore, on the basis of receiver operating characteristic curve analysis of JSS-D, the sensitivity based on this cut-off value was 0.950 and specificity was 0.988 for depression evaluated by the Mini International Neuropsychiatric Interview. In this study, JSS-D data were collected on the 10th day of hospitalization.
The capacity to function independently in the practical task of daily living was assessed by the 18-item Functional Independence Measure (FIM), which scores levels of dependence from 18 (total assistance in all areas) to 126 (complete independence in all areas). A total FIM score is generated by summing the subscale scores of six domains assessing self-care, sphincter management, mobility, locomotion, communication, and social cognition.15 The FIM was administered on the 10th day of hospitalization.
Statistical analysis
Descriptive analyses of the demographic and clinical variables were performed. To compare the main demographic and clinical characteristics between groups, the unpaired Student’s t-test or Mann–Whitney U-test was performed to analyze the continuous variables, and chi-square tests or Fisher’s exact tests were performed to analyze the categorical variables. The data are presented as means ± SD. The relationship between NIHSS scores and LOHS was tested using simple linear regression analysis. To determine the effect of probable depression on LOHS, a general linear model analysis (model 1) that included age, sex, education level, living status, NIHSS scores, FIM scores, and the presence of probable depression was employed. Interactions between the NIHSS scores and the presence of probable depression were also tested in the same model. All variables with P<0.10 in model 1 were subsequently analyzed in model 2. A value of P<0.05 was considered significant. The data were analyzed using PASW Statistics PC software for Windows, Version 18.0.0 (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of participants
Using a score of 2.4, which was identified by a validation study,14 as the optimal cut-off point for identifying probable depression among patients after acute stroke, the frequency of probable clinical depression in the current sample was 16.3% in males (n=43) and 17.8% in females (n=28) (P>0.05). Overall, the mean JSS-D score was 1.53±1.64 for males and 1.77±2.24 for females (P>0.05). The mean LOHS of participants with probable depression (n=71; 76.4±49.2 days) was significantly longer than that of participants without probable depression (n=350; 44.9±39.2 days).
Effect of poststroke depression on LOHS
Trends in LOHS are depicted in Figure 1. A significant relationship between LOHS and NIHSS scores was observed in subjects with and without probable depression (with probable depression, P<0.001; without probable depression, P<0.001). Table 1 lists the results of general linear models for LOHS among patients with ischemic stroke. In model 1, probable depression was significantly associated with LOHS (P<0.01). Living alone, NIHSS scores, and FIM scores significantly affected LOHS. Furthermore, a significant interaction between probable depression and NIHSS scores was observed. In model 2, probable depression was significantly associated with LOHS (P<0.01). Additionally, living alone, NIHSS scores, and FIM scores significantly affected LOHS. Furthermore, a significant interaction between probable depression and NIHSS scores was observed.
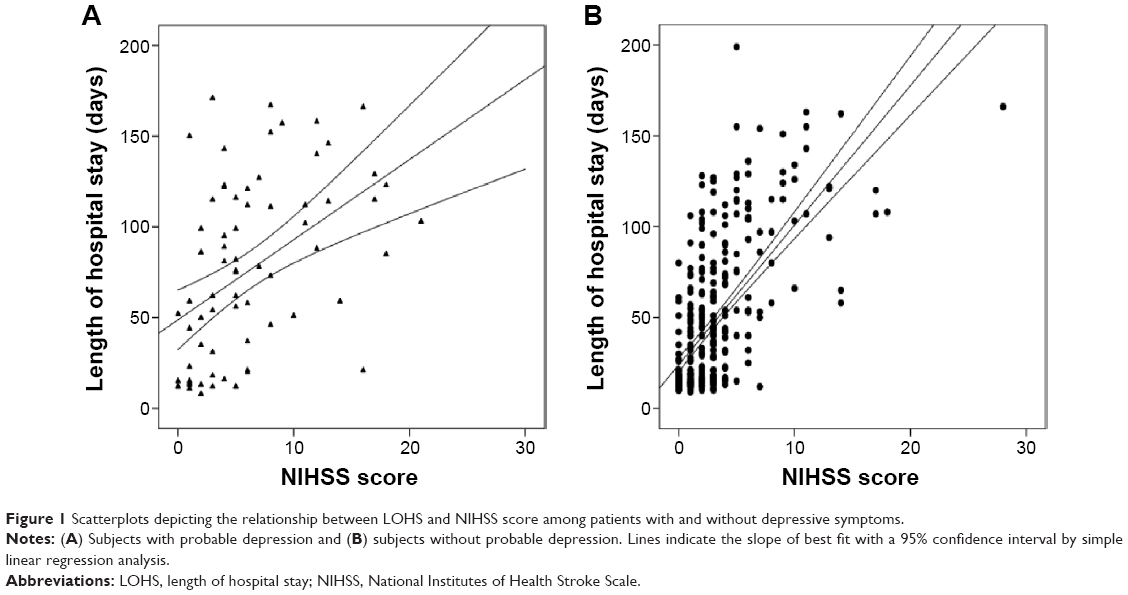 | Figure 1 Scatterplots depicting the relationship between LOHS and NIHSS score among patients with and without depressive symptoms. |
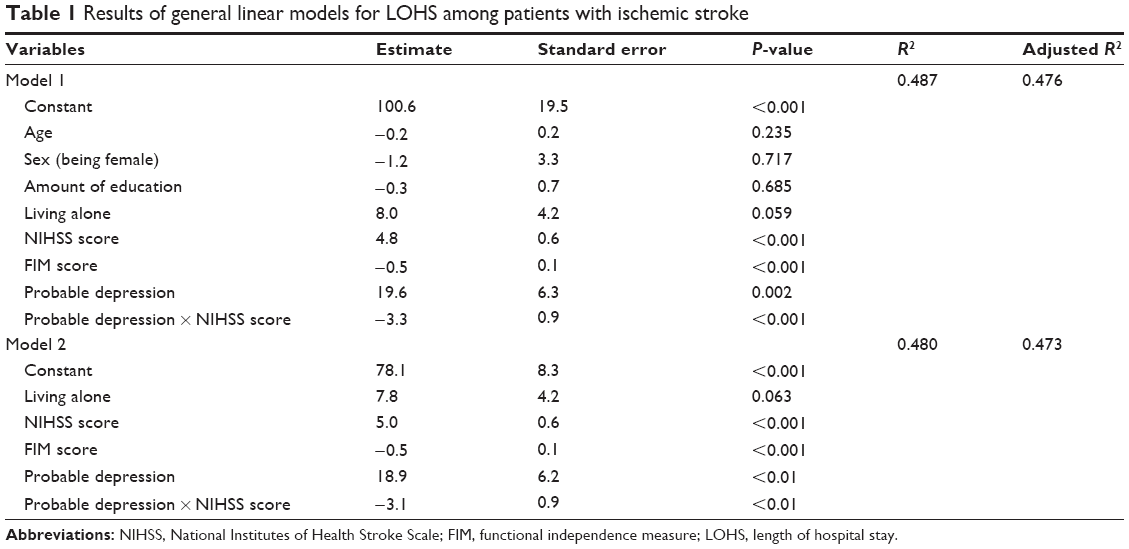 | Table 1 Results of general linear models for LOHS among patients with ischemic stroke |
Discussion
This study was conducted to evaluate the effect of early depressive symptoms on LOHS among patients hospitalized for acute ischemic stroke in Japan. Participants with probable depression had greater LOHS (more than 30 days longer) than those without probable depression. In addition, a significant interaction between the presence of probable depression and the NIHSS scores in a general linear model showed that the ascending trend of LOHS with respect to the NIHSS scores was decelerated in patients with probable depression.
Several studies concerning the comorbidity of depression and LOHS have shown that patients with depression are likely to stay longer at hospitals. In a US study, Saravay et al16 clarified the association between LOHS and depression based on the Zung Self-Rating Depression Scale (SDS) among 278 medical and surgical inpatients. In another study conducted in the US, Levenson et al17 showed that patients with high levels of psychopathology had longer stays and higher costs during the index hospitalization but that no differences were observed during subsequent hospitalizations among 1,020 medical patients. In a Japanese study of 51 patients with noncancer diseases, Hosaka et al18 showed that patients with depression stayed longer at the hospital than those without depression. There are some explanations for relationship between increased LOHS and depression after stroke. One possible explanation for this relationship is that patients with depression after stroke had lower functional independence in activities of daily living.19 Lower functional independence might delay patients from achieving the maximal benefit of rehabilitation therapies. Another explanation is that patients with depression might resist hospital discharge. Depressed patients might hope for more support from medical personnel and comprehensive care in an inpatient ward.20
In patients with stroke,9–12 several studies have reported associations between LOHS and psychiatric disorders; however, one study failed to find such an association.21 Concerning the relationship between the severity of psychiatric symptoms and LOHS, Schubert et al22 showed a positive correlation between Geriatric Depression Scale scores and LOHS among 14 patients in a rehabilitation ward. In addition, Galynker et al23 reported that the Negative Symptoms subscale of the Positive and Negative Symptom Scale in stroke patients was associated with a longer LOHS.23 Although the mean LOHS of patients with probable depression was greater than those without probable depression, we found a different trend describing the relationship between LOHS and NIHSS scores among patients with and without probable depression in the general linear model. Patients with depression after stroke may not receive sufficient treatment relative to the severity of their stroke symptoms.
Recently, selective serotonin reuptake inhibitors (SSRIs) have been widely used for depression after stroke. There is growing evidence that SSRIs may enhance stroke recovery.24 Although absolute risk is likely to be very low, SSRIs may increase the risk of intracranial hemorrhage.25 To clarify the effect of SSRIs on cerebrovascular events and mortality following a stroke, further well-designed clinical studies are needed.
Apart from the depression after stroke, many studies report that other factors are associated with LOHS among patients with stroke. Previous studies have identified that functional dependency26,27 and severity of stroke28 are also related to longer LOHS. Furthermore, living alone before stroke was reported to be a risk factor for institutionalization after acute stroke hospitalization.29,30 Consistent with previous results, we included living status, NIHSS scores, and FIM scores in the linear regression model to predict LOHS.
The current findings must be cautiously interpreted for the following reasons. First, this study used only one measure of depressive symptoms, the JSS-D, and patients were not diagnosed as having clinical depression using the Diagnostic and Statistical Manual of Mental Disorders, fourth edition. Although JSS-D screening has been thoroughly validated and widely used to assess depressive symptoms, this tool is not a formal diagnostic tool for depression. In addition, JSS-D was not designed to assess apathy, which has been reported to be associated with recovery from stroke-related physical disabilities.31 Second, the assessment of depressive symptoms was conducted on the 10th day of hospitalization. Although half of median prehospital delays have been reported to last between 3 and 4 hours,32 we cannot completely eliminate the possible influence of delays between the onset of symptoms and hospital admission. Second, this study excluded patients with severe aphasia or altered consciousness. Furthermore, in our study, who died in the hospital were not included as participants. This exclusion might limit the generalizability of our findings. Third, the study population consisted only of patients who were admitted to the Hirosaki Stroke and Rehabilitation Center; therefore, it may not reflect the characteristics of the entire Japanese population with depression after stroke. Further studies that include patients from various public and private hospitals are needed. Finally, several potential confounding factors, such as socioeconomic status, medical complications, and medication, were not assessed by our study. In particular, approximately 20% of patients after stroke suffered anxiety disorders or posttraumatic stress disorder, which might have influenced JSS-D scores.33–35 The absence of the aforementioned factors might have influenced the current findings.36–39
Conclusion
Depression after stroke was found to be associated with significantly increased LOHS even after adjusting for possible confounders. The interaction between probable depression and NIHSS scores in the general linear model may indicate that patients with probable depression might not receive sufficient treatment relative to the severity of their stroke symptoms. Early detection and treatment for depressive symptoms are needed for patients with ischemic stroke.
Acknowledgments
We are grateful to all of the volunteers who participated in this study. The authors express their gratitude to Ms Sachie Narita, Ms Ruriko Ono, and Ms Ayako Osanai for their help with this study.
Disclosure
The authors report no conflicts of interests in this work.
References
Ayerbe L, Ayis S, Wolfe CD, Rudd AG. Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br J Psychiatry. 2013;202:14–21. | ||
Hackett ML, Pickles K. Part I: frequency of depression after stroke: an updated systematic review and meta-analysis of observational studies. Int J Stroke. 2014;9:1017–1025. | ||
Lipsey JR, Spencer WC, Rabins PV, Robinson RG. Phenomenological comparison of poststroke depression and functional depression. Am J Psychiatry. 1986;143:527–529. | ||
Cully JA, Gfeller JD, Heise RA, Ross MJ, Teal CR, Kunik ME. Geriatric depression, medical diagnosis, and functional recovery during acute rehabilitation. Arch Phys Med Rehabil. 2005;86:2256–2260. | ||
Gillen R, Tennen H, McKee TE, Gernert-Dott P, Affleck G. Depressive symptoms and history of depression predict rehabilitation efficiency in stroke patients. Arch Phys Med Rehabil. 2001;82:1645–1649. | ||
Bartoli F, Lillia N, Lax A, et al. Depression after stroke and risk of mortality: a systematic review and meta-analysis. Stroke Res Treat. 2013;2013:862978. | ||
Roberts L, Counsell C. Assessment of clinical outcomes in acute stroke trials. Stroke. 1998;29:986–991. | ||
Saxena SK, Ng TP, Yong D, Fong NP, Gerald K. Total direct cost, length of hospital stay, institutional discharges and their determinants from rehabilitation settings in stroke patients. Acta Neurol Scand. 2006;114:307–314. | ||
Ebrahim S, Barer D, Nouri F. Affective illness after stroke. Br J Psychiatry. 1987;151:52–56. | ||
Cushman LA. Secondary neuropsychiatric complications in stroke: implications for acute care. Arch Phys Med Rehabil. 1988;69:877–879. | ||
Fulop G, Strain JJ, Fahs MC, Hammer JS, Lyons JS. Medical disorders associated with psychiatric comorbidity and prolonged hospital stay. Hosp Community Psychiatry. 1989;40:80–82. | ||
Eastwood MR, Rifat SL, Nobbs H, Ruderman J. Mood disorder following cerebrovascular accident. Br J Psychiatry. 1989;154:195–200. | ||
Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20:864–870. | ||
Kaji Y, Hirata K. Usefulness of the Japan Stroke Scale-Depression Scale-(JSS-D) for the diagnosis of post-stroke depression. Intern Med. 2008;47:225–229. | ||
Keith RA, Granger CV, Hamilton BB, Sherwin FS. The functional independence measure: a new tool for rehabilitation. Adv Clin Rehabil. 1987;1:6–18. | ||
Saravay SM, Steinberg MD, Weinschel B, Pollack S, Alovis N. Psychological comorbidity and length of stay in the general hospital. Am J Psychiatry. 1991;148:324–329. | ||
Levenson JL, Hamer RM, Rossiter LF. Psychopathology and pain in medical in-patients predict resource use during hospitalization but not rehospitalization. J Psychosom Res. 1992;36:585–592. | ||
Hosaka T, Aoki T, Watanabe T, Okuyama T, Kurosawa H. Comorbidity of depression among physically ill patients and its effect on the length of hospital stay. Psychiatry Clin Neurosci. 1999;53:491–495. | ||
Badaru UM, Ogwumike OO, Adeniyi AF, Olowe OO. Variation in functional independence among stroke survivors having fatigue and depression. Neurol Res Int. 2013;2013:842980. | ||
McCusker J, Latimer E, Cole M, Ciampi A, Sewitch M. The nature of informal caregiving for medically ill older people with and without depression. Int J Geriatr Psychiatry. 2009;24:239–246. | ||
Sinyor D, Amato P, Kaloupek DG, Becker R, Goldenberg M, Coopersmith H. Post-stroke depression: relationships to functional impairment, coping strategies, and rehabilitation outcome. Stroke. 1986;17:1102–1107. | ||
Schubert DS, Burns R, Paras W, Sioson E. Increase of medical hospital length of stay by depression in stroke and amputation patients: a pilot study. Psychother Psychosom. 1992;57:61–66. | ||
Galynker I, Prikhojan A, Phillips E, Focseneanu M, Ieronimo C, Rosenthal R. Negative symptoms in stroke patients and length of hospital stay. J Nerv Ment Dis. 1997;185:616–621. | ||
Mead GE, Hsieh CF, Lee R, et al. Selective serotonin reuptake inhibitors (SSRIs) for stroke recovery. Cochrane Database Syst Rev. 2012;11:CD009286. | ||
Mortensen JK, Andersen G. Safety of selective serotonin reuptake inhibitor treatment in recovering stroke patients. Expert Opin Drug Saf. 2015;14:911–919. | ||
Ohwaki K, Hashimoto H, Sato M, Tokuda H, Yano E. Gender and family composition related to discharge destination and length of hospital stay after acute stroke. Tohoku J Exp Med. 2005;207:325–332. | ||
Ekstrand E, Ringsberg KA, Pessah-Rasmussen H. The physiotherapy clinical outcome variables scale predicts length of hospital stay, discharge destination and future home facility in the acute comprehensive stroke unit. J Rehabil Med. 2008;40:524–528. | ||
Somerford PJ, Lee AH, Yau KK. Ischemic stroke hospital stay and discharge destination. Ann Epidemiol. 2004;14:773–777. | ||
Glader EL, Stegmayr B, Norrving B, et al. Sex differences in management and outcome after stroke: a Swedish national perspective. Stroke. 2003;34:1970–1975. | ||
Reeves MJ, Prager M, Fang J, Stamplecoski M, Kapral MK. Impact of living alone on the care and outcomes of patients with acute stroke. Stroke. 2014;45:3083–3085. | ||
Hama S, Yamashita H, Yamawaki S, Kurosi K. Post-stroke depression and apathy: Interactions between functional recover, lesion detection, and emotional response. Psychogeriatrics. 2011;11:68–76. | ||
Evenson KR, Foraker RE, Morris DL, Rosamond WD. A comprehensive review of prehospital and in-hospital delay times in acute stroke care. Int J Stroke. 2009;4:187–199. | ||
Campbell Burton CA, Murray J, Holmes J, et al. Frequency of anxiety after stroke: a systematic review and meta-analysis of observational studies. Int J Stroke. 2013;8:545–559. | ||
Edmondson D, Richardson S, Fausett JK, Falzon L, Howard VJ, Kronish IM. Prevalence of PTSD in survivors of stroke and transient ischemic attack: a meta-analytic review. PLoS One. 2013;8:e66435. | ||
Javidi H, Yadollahie M. Post-traumatic stress disorder. Int J Occup Environ Med. 2012;3:2–9. | ||
Kulik JA, Mahler HI. Marital quality predicts hospital stay following coronary artery bypass surgery for women but not men. Soc Sci Med. 2006;63:2031–2040. | ||
Epstein AM, Stern RS, Tognetti J, et al. The association of patients’ socioeconomic characteristics with the length of hospital stay and hospital charges within diagnosis-related groups. N Engl J Med. 1988;318:1579–1585. | ||
Di Iorio A, Longo A, Mitidieri Costanza A, et al. Factors related to the length of in-hospital stay of geriatric patients. Aging. 1999;11:150–154. | ||
Tirschwell DL, Kukull WA, Longstreth WT Jr. Medical complications of ischemic stroke and length of hospital stay: experience in Seattle, Washington. J Stroke Cerebrovasc Dis. 1999;8:336–343. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.