Back to Journals » Journal of Pain Research » Volume 18
Effect of Contralateral Acupuncture (Geoja Technique) in Musculoskeletal Disorders Stratified by Pulse Strength Differences: A Retrospective Study
Authors Park S ![]() , Lee D, Kim GW, Cho FY, Kim Y
, Lee D, Kim GW, Cho FY, Kim Y ![]() , Kim Y
, Kim Y ![]() , Kim G
, Kim G ![]() , Baek Y
, Baek Y ![]() , Park YC
, Park YC ![]()
Received 2 September 2025
Accepted for publication 12 November 2025
Published 17 November 2025 Volume 2025:18 Pages 6149—6163
DOI https://doi.org/10.2147/JPR.S559379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Sinwoo Park,1,2,* Dongmin Lee,1,3,4,* Go-Woon Kim,1 Foo Young Cho,1 Yeonhak Kim,4 Yuna Kim,2 Gongbin Kim,2 Yonghyeon Baek,3,4 Yeon-Cheol Park3,4
1Department of Clinical Korean Medicine, Graduate School, Kyung Hee University, Seoul, Republic of Korea; 2Hyundong Korean Medical Clinic, Seoul, Republic of Korea; 3Department of Acupuncture & Moxibustion, Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea; 4East-West Bone & Joint Disease Research Institute, Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Yeon-Cheol Park, Department of Acupuncture & Moxibustion, Kyung Hee University Hospital at Gangdong, 892, Dongnam-ro, Gangdong-gu, Seoul, 05278, Republic of Korea, Email [email protected]
Purpose: This retrospective case study explored the effect of contralateral acupuncture (Geoja technique) on patients with one-sided musculoskeletal pain disorders.
Patients and Methods: This retrospective observational study reviewed 109 patients treated for unilateral musculoskeletal pain. Their demographics and clinical characteristics were recorded. Patients were categorized into two groups based on pulse strength differences, diagnosed using a classic Korean medicine method rooted in Donguibogam. Disability and pain intensity were measured using the Numeric Rating Scale (NRS) and Range of Motion (ROM). The treatment effect was assessed by comparing the improvement rates between these groups.
Results: All 109 patients received contralateral acupuncture treatment. Significant improvements in disability and pain intensity were observed in the 65 patients with pulse strength differences. The mean differences and improvement rate of NRS showed clinically relevant changes in both groups; however, the improvement rate in the group with pulse strength differences was statistically significantly higher than in the 44 patients without pulse strength differences.
Conclusion: This study suggests the 2, potential of contralateral acupuncture for pain relief, ROM improvement, and maintaining normal function in patients with musculoskeletal diseases. It also highlights the importance of pulse strength difference for effective treatment. Further studies are required to ensure appropriate patient selection, integrate treatment guidelines, and ascertain optimal outcome measurement criteria to draw robust conclusions regarding the effectiveness of treating musculoskeletal disorders.
Keywords: contralateral acupuncture, Geoja technique, pulse strength, musculoskeletal disorders, retrospective study
A Letter to the Editor has been published for this article.
A Response to Letter by Ms Qiu has been published for this article.
Introduction
Acupuncture is used to treat a number of conditions worldwide, including musculoskeletal diseases. Several studies have reported the effects of acupuncture on pain-related diseases. The effectiveness and safety of acupuncture treatment have been reported in basic experimental studies, clinical trials, randomized control studies, and systematic review.1 Recent studies on acupuncture have expanded to include meridian-specific effects. Specifically, meta-analyses have affirmed acupuncture’s effectiveness in reducing musculoskeletal pain, demonstrating its superiority over sham acupuncture,2 and have explored its neuroimage biomarkers.3 Beyond general pain relief, acupuncture has also shown promise in specific musculoskeletal conditions, such as chronic low back pain and neck pain.4–6
In 2001, the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) were created and have been subsequently used in clinical research to report the findings of clinical trials on acupuncture treatment.7 Acupuncture-related clinical trials have focused on pain points and near acupuncture-point needling, and randomized controlled clinical trials have been conducted on the effects of acupuncture treatment on various diseases.8,9 However, in actual clinical practice, contralateral acupuncture treatment or remote acupoint needling is often performed, which has been reported to be more clinically effective.10 Most previous studies have been at the case series level11 and are generally limited to comparing contralateral acupuncture points and remote acupuncture point needling.12 Few studies have been conducted to ascertain when contralateral acupuncture should be used and the criteria for choosing remote acupuncture points.
Contralateral acupuncture elicits potential analgesic effects through complex neural pathways. Research suggests that acupuncture can induce both ipsilateral and contralateral analgesia through mechanisms that may include the nociceptive system and modulation of the default mode network in the brain.13 Contralateral acupuncture has been observed to stimulate the contralateral sensorimotor network and activate specific brain regions, suggesting different analgesic regulatory mechanisms compared to ipsilateral acupuncture. For instance, studies have shown that contralateral acupuncture at specific acupoints can lead to distinct changes in brain connectivity and activity, indicating a neurophysiological basis for its therapeutic effects.14–17 Furthermore, the transmission of nerve impulses from stimulated acupoints to the central nervous system, crossing the spinal cord, contributes to the generation of acupuncture sensation and its analgesic effects.18,19
According to the historical context of acupuncture, a representative treatment on the healthy side is called Geoja, which is the acupuncture method suggested in Yellow Emperor’s Inner Canon (黃帝內經) and is performed on the opposite side of the body as to where the symptoms have presented.20 This method is used by many modern Korean medicine doctors. In one study, 33% of the respondents used only remote acupoints, and 71% used near and remote acupoints together.21 Many Korean medicine doctors utilize the Geoja technique, but research on its underlying principles and effect is insufficient, necessitating more studies.
Within the traditional framework, acupuncture point selection often involves specific points such as the Five important acupoints (五腧穴). These points are located on the twelve main meridians and are frequently used to activate or balance the flow of Qi (氣).22,23 For instance, in clinical practice, the sedation of Fire point (火穴) and the supplementation of Water point (水穴) are widely employed for effective pain relief.24 The selection and combination of these specific acupoints are crucial because the patterns of meridian imbalance vary with different diseases, and addressing these imbalances is key to treating ailments.25,26
In Yellow Emperor’s Inner Canon (黃帝內經), if the pain is on the left side and the pulse on the right side is diseased, the patient is treated with Geoja.27 Similarly, Donguibogam (東醫寶鑑) stated that if the left pulse is strong, the right side is diseased, and if the right pulse is strong, the left side is diseased. Therefore, in the case of a patient who mainly complains of pain, such as musculoskeletal disorders, it is considered necessary to compare the strength of the left and right pulses and perform the Geoja technique. While indications and procedural methods for the Geoja technique used in clinical practice are reported through classical literature reviews, establishing a scientific basis remains challenging due to the lack of robust clinical research on Geoja.
Therefore, this retrospective study aims to compare the therapeutic effect of Geoja in patients with different left and right pulse strengths and to examine the basis for its use in acupuncture treatment. Our findings are intended to be used as basic data for prospective research and ultimately for increasing the use of Geoja technique in the clinical field. This study hypothesizes that patients exhibiting a discernible difference in pulse strength between the left and right sides will experience a more significant therapeutic response to Geoja technique for musculoskeletal pain.
Materials and Methods
Patients and Eligibility
This study conducted a retrospective study on 109 patients who received treatment for musculoskeletal pain disease limited to one side at the Hyundong Korean Medical Clinic, Seoul, Republic of Korea, between January and August 2022. The inclusion criteria were as follows: (1) pain in one side only and (2) acupuncture in the other side only. Participants who have the following characteristics were excluded: (1) pain in both sides or pain in the center, (2) structural deformation of the joint, and (3) near acupuncture-point needling.
Difference in Pulse Strength
According to the classic context of Korean medicine, pulse diagnosis is a palpation test performed through direct contact between the physician’s finger and patient’s wrist.28 In Donguibogam (東醫寶鑑), the physician uses his/her middle finger to first press the Gwan (關) area (styloid process of radius), and the fingers on both sides of the middle finger are lowered side by side, so that the front finger is Chon (寸), and the back finger is Cheok (尺) (Figure 1). If the patient’s arm is long, the finger gap is spread and pressed; if the patient’s arm is short, the finger gap is narrowed and pressed.
 |
Figure 1 Pulse diagnosis regions. The Gwan area corresponds to the styloid process of the radius. |
After entering the clinic, the patient sits on a chair and places his/her left arm on a table. The physician examines the patient’s Chon, Gwan, and Cheok (寸關尺) using the index, middle, and ring finger and then examines the patient’s Chon, Gwan, and Cheok (寸關尺) through his/her index finger in order. When the left side is completed, we should proceed to the right side. The physician presses slightly to examine the pulse area and then deeply to examine it. While pressing down so hard that the pulse is not felt in the physician’s finger, slowly lift the finger to measure the power at the point where the pulse strength is felt the most powerful. Subsequently, the left and right strength pulses are compared; if there is a difference in force, one side is recorded as strong, and if there is no difference in force, it is recorded similarly. This is based on Donguibogam (東醫寶鑑) and follows the pulse diagnosis method described in acupuncture textbooks.
Acupuncture Treatment
All treatment interventions were performed by Korean medicine doctors with more than 5 years of clinical experience according to preset treatment guidelines based on the patient’s condition. Infrared treatment (IR3000, Haedong Medical, Korea) was performed during acupuncture (30 min). Manual acupuncture needles (0.2 mm in diameter, 30 mm in length, Dongbang, Gyeonggi-do, Korea) was used according to the meridian where the patient complained of pain and was performed on the opposite arm and leg of the painful lesions. The acupuncture point comprised a place to sedate the fire point (火穴) and supplement the water point (水穴) among five important acupoints (五腧穴) (Table 1). The Young-su-bo-sa (迎隨補瀉) method was implemented, and each acupoint was inserted along the meridians Qi (氣) flow in the case of supplement and against the meridians Qi (氣) flow in the case of sedate. The method used in this study is described in the acupuncture medicine textbook of the Korean Medicine University. All acupuncture treatments were performed until the De-qi (得氣) sensation (soreness, fullness, heaviness, or distension) was achieved. Further details of the treatment interventions, such as the acupoints and insertion method, are described in the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) checklist (Table 2).7
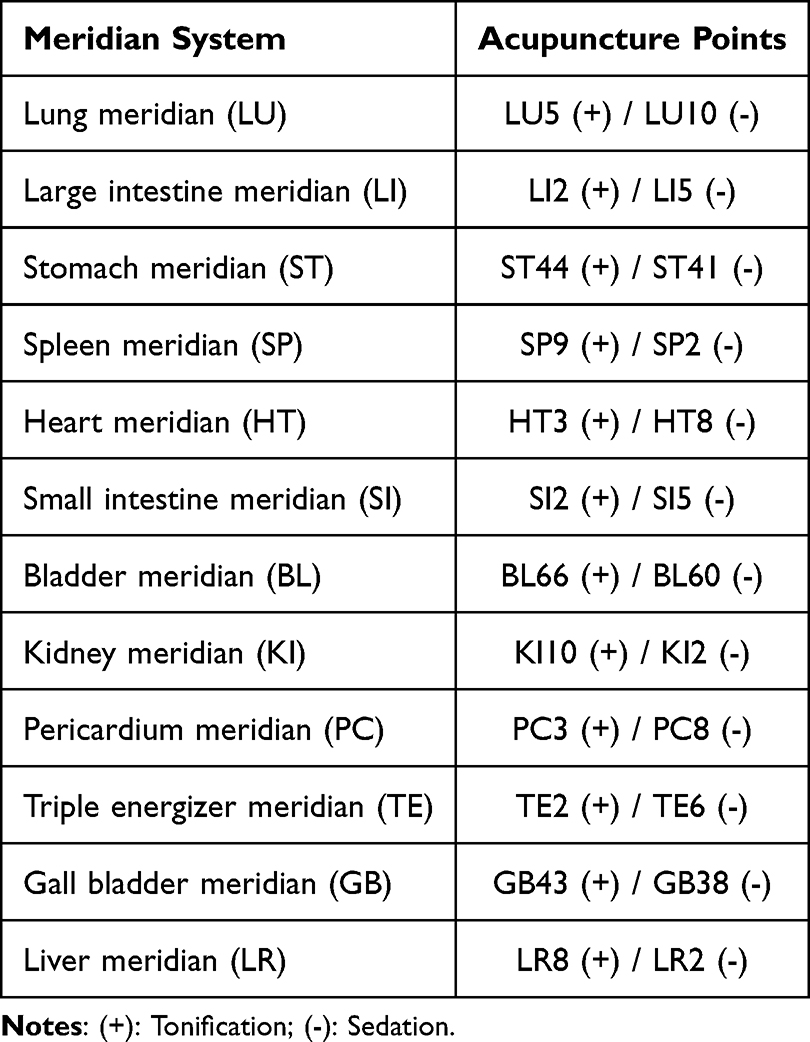 |
Table 1 Acupuncture Treatment According to the Diagnosed Meridians |
 |
Table 2 Details of the Acupuncture Treatments for Lesions of the Meridian System Based on the STRICTA 2010 Checklist. Acupuncture Treatment According to the Diagnosed Meridians |
Study Protocol
This study included 109 patients who met the inclusion criteria. The lesions and meridian system in which patients complained of pain were identified and classified into groups with different pulse strengths and groups with the same pulse strength. All patients who met the inclusion criteria complained of pain in only one side and received acupuncture on the opposite side. The improvement rate of each disease was measured using the numerical rating scale (NRS) at baseline and at the end of treatment. Joint dysfunction was assessed using the range of motion (ROM) test to determine musculoskeletal function. To analyze clinically meaningful changes, we analyzed the improvement rate after treatment by group. The NRS assumed that all initial pain values were similar and analyzed the improvement rate after treatment was analyzed. The ROM was used to classify the grade according to the angle (Table 3) and confirm the grade change before and after treatment.
 |
Table 3 Flexion Tests at Major Joints |
Statistical Analysis
Statistical analyses were performed using the SPSS version 18.0 for Windows (SPSS Inc. Chicago, IL, USA), and statistical significance was set at p-values of <0.05. The homogeneity of the demographical and clinical characteristics was analyzed using the chi-square test and independent t-test. To analyze clinically meaningful changes, we analyzed the improvement rate after treatment by group. The NRS assumed that all initial pain values were similar, and analyzed the improvement rate after treatment was analyzed. The degree of recovery (%) is presented as the mean ± standard deviation to compare the two groups with a difference in pulse strength. Differences between the two groups were analyzed using an independent t-test.
Results
Patient Clinical Characteristics
Among the patients treated during the study period, 109 met the inclusion criteria. If the intensity was remarkably strong between the left and right Chon, Gwan, Cheok (寸關尺) in any region, there was a difference in the strength of the pulse (group A and group C). If it was similar overall, then there was no difference in the strength of the pulse (group B and group D) (Tables 4 and 5). Of the 109 patients, 65 showed difference in pulse strength, and 44 showed no difference in pulse strength (Table 6).
 |
Table 4 Clinical Characteristics of Upper Limbs Patients |
 |
Table 5 Clinical Characteristics of Lower Limbs Patients |
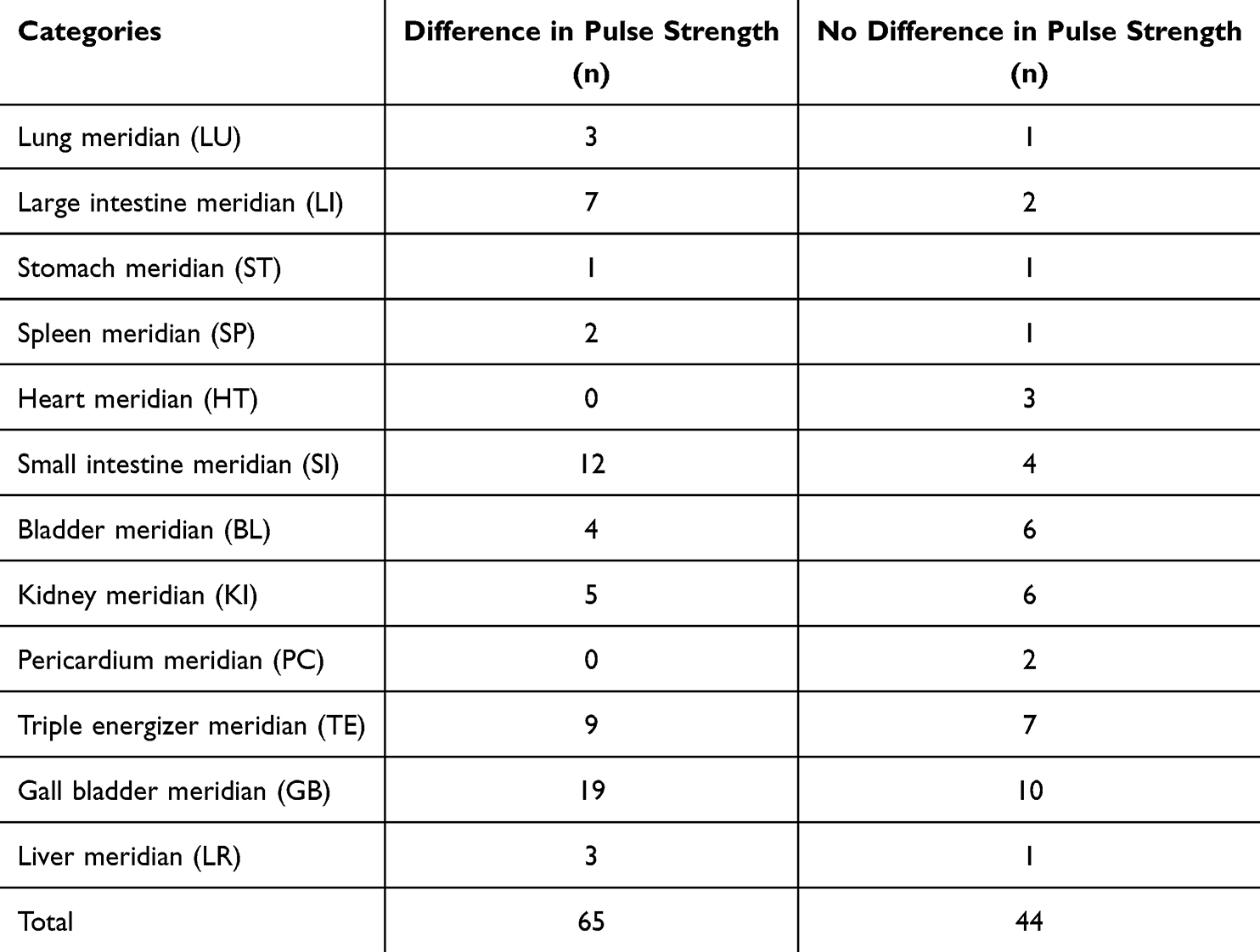 |
Table 6 Lesions in the Meridian System |
The mean age, period from the onset of pain to the initial visit, number of treatments, and treatments duration in group A (upper limb pain and differences in pulse strength) were 44.95 ± 13.43 years, 30.39 ± 53.69 days, 2.16 ± 1.57 times, and 4.05 ± 4.31 days, respectively. The mean age, period from the onset of pain to the initial visit, number of treatments, and treatments duration in group B (upper limb pain and no differences in pulse strength) were 48.83 ± 18.39 years, 31.22 ± 53.73 days, 2.70 ± 2.23 times, 5.30 ± 5.00 days, respectively. The mean age and the period from the onset of pain to the initial visit were similar between the two groups. The mean number of treatments and treatment duration were longer in group B than in group A; however, the difference was not statistically significant (Table 4). In group C (lower limb pain and differences in pulse strength), the mean age, period from the onset of pain to the initial visit, number of treatments, and treatments duration were 47.15 ± 18.07 years, 15.11 ± 35.37 days, 2.59 ± 1.74 times, 4.85 ± 4.13 days, respectively. The mean age, period from the onset of pain to the initial visit, number of treatments, and treatments duration in group D (lower limb pain and no differences in pulse strength) were 49.48 ± 18.65 years, 39.29 ± 62.27 days, 2.05 ± 1.72 times, 3.10 ± 4.01 days, respectively. The mean ages of the two groups were similar. The mean period from the onset of pain to the initial visit was shorter in group C than in group D, and the mean number of treatments and treatment duration were shorter in group D than in group C; however, no statistically significant differences were observed (Table 5).
The patients with upper limb pain included 23 with shoulder pain (difference in pulse strength, 14; no difference in pulse strength, 9), 13 with shoulder girdle pain (difference in pulse strength, 10; no difference in pulse strength, 3), 7 with arm pain (difference in pulse strength, 3; no difference in pulse strength, 4), 7 with elbow pain (difference in pulse strength, 6; no difference in pulse strength, 1), 5 with wrist pain (difference in pulse strength, 2; no difference in pulse strength, 3), 4 with finger pain (difference in pulse strength, 3; no difference in pulse strength, 1), and 2 with palm pain (difference in pulse strength, 0; no difference in pulse strength, 2). The patients with lower limb pain included 13 with knee pain (difference in pulse strength, 5; no difference in pulse strength, 8), 6 with thigh pain (difference in pulse strength, 5; no difference in pulse strength, 1), 8 with leg pain (difference in pulse strength, 6; no difference in pulse strength, 2), 16 with ankle pain (difference in pulse strength, 8; no difference in pulse strength, 8), and 5 with sole pain (difference in pulse strength, 3; no difference in pulse strength, 2) (Table 7).
 |
Table 7 Painful Lesions |
Regarding the pain meridians, 4 patients had LU meridian pain (difference in pulse strength, 3; no difference in pulse strength, 1), 9 had LI meridian pain (difference in pulse strength, 7; no difference in pulse strength, 2), 2 had ST meridian pain (difference in pulse strength, 1; no difference in pulse strength, 1), 3 had SP meridian pain (difference in pulse strength, 2; no difference in pulse strength, 1), 3 had HT meridian pain (difference in pulse strength, 0; no difference in pulse strength, 3), 16 had SI meridian pain (difference in pulse strength, 12; no difference in pulse strength, 4), 10 had BL meridian pain (difference in pulse strength, 4; no difference in pulse strength, 6), 11 had KI meridian pain (difference in pulse strength, 5; no difference in pulse strength, 6), 2 had PC meridian pain (difference in pulse strength, 0; no difference in pulse strength, 2), 16 had TE meridian pain (difference in pulse strength, 9; no difference in pulse strength, 7), 29 had GB meridian pain (difference in pulse strength, 19; no difference in pulse strength, 10), 4 had LR meridian pain (difference in pulse strength, 3; no difference in pulse strength, 1) (Table 6).
Analysis of Disability and Pain Improvement
The degree of pain and disability status of all patients were measured using the NRS and ROM, respectively. Researcher notified the patient that the pre-treatment pain NRS was 10, and asked for the post-treatment pain NRS score. Based on the scores spoken by the patients, the pain improvement rates of each patient were recorded and compared. Not all patients had ROM limitations; therefore, the ROM improvement rate was compared between patients with ROM limitations.
The pain improvement rates were 54.74 ± 19.55%, 31.30 ± 21.60%, 56.30 ± 17.35%, and 29.52 ± 19.87% in groups A, B (p < 0.001), C, and D (p < 0.001), respectively. The difference in the improvement rate between the groups with and without a pulse strength difference was statistically significant (Table 8). The distribution of NRS improvement rates for both upper and lower limbs is further visualized using box-and-whisker plots, respectively. These figures offer a detailed view of how improvement rates vary depending on the presence or absence of a pulse strength difference. For upper limb pain, patients with a pulse strength difference exhibited a median improvement rate of 50%, with an interquartile range (IQR) spanning 40% to 70%. In contrast, those without a pulse strength difference showed a median improvement rate of 20%, and their IQR ranged from 10% to 40%. Similarly, in cases of lower limb pain, the pulse difference group had a median improvement rate of 60% and an IQR of 40% to 70%, while the no difference group had a median improvement rate of 20% and an IQR of 15% to 30%. Across both upper and lower limbs, patients with a difference in pulse strength consistently demonstrated a higher median improvement rate and a broader range of improvement compared to those without a pulse strength difference (Figures 2 and 3).
 |
Table 8 Pain Improvement Rate |
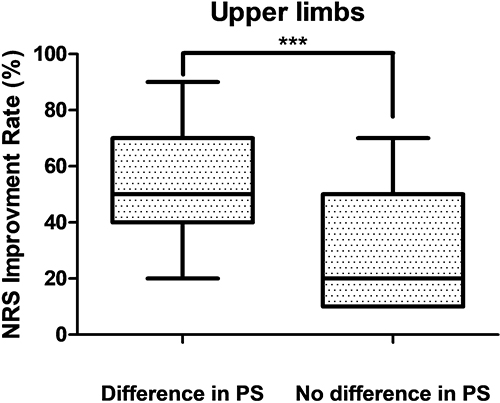 |
Figure 2 Distribution of NRS improvement rates for upper limbs according to pulse strength difference (exclusive-median quartile calculation). The boxes represent the interquartile range (IQR) calculated by excluding the overall median from each half of the dataset, with the line inside each box denoting the median. The whiskers indicate the minimum and maximum values. Abbreviations: NRS, Numerical rating scale; PS, pulse strength. |
 |
Figure 3 Distribution of NRS improvement rates for lower limbs according to pulse strength difference (exclusive-median quartile calculation). The boxes represent the interquartile range (IQR) calculated by excluding the overall median from each half of the dataset, with the line inside each box denoting the median. The whiskers indicate the minimum and maximum values. Abbreviations: NRS, Numerical rating scale; PS, pulse strength. |
Of all patients, 13 had shoulder joints pain (difference in pulse strength, 9; no difference in pulse strength, 4), 3 had elbow joints pain (difference in pulse strength, 3; no difference in pulse strength, 0), 2 had wrist joints pain (difference in pulse strength, 1; no difference in pulse strength, 1), and 4 had knee joints pain (difference in pulse strength, 3; no difference in pulse strength, 1). The degree of ROM limitation was recorded by dividing the steps according to the angle set; if this did not fall under the fifth stage, the patient had a restricted ROM (Table 3). Of the 16 patients with differences in pulse strength, 14 showed an improvement of grade 1 or higher, and 3 patients showed an improvement of grade 2 or higher. In contrast, only one of 6 patients with no difference in pulse strength showed an improvement of grade 1 or higher (Table 9).
 |
Table 9 Degree of ROM Improvement |
Discussion
This retrospective study suggests that the Geoja technique may be more effective in relieving pain and improving ROM in patients with musculoskeletal pain, particularly when a clear difference in left and right pulse strength is observed. During the course of this study, adverse events typically monitored in clinical practice, such as immediate adverse reactions during treatment, were recorded in the medical charts. No significant or unusual adverse findings were noted.
According to a text of musculoskeletal treatment using acupuncture in Western medicine, the goal of treatment for patients with musculoskeletal pain is to relieve pain, improve ROM, and maintain normal function. In general, acupuncture treatment for patients with musculoskeletal pain can be selected for myofascial pain points that are directly related to pain, tenderness, and traditional acupuncture points. Among the above three conditions, an acupoint that satisfied two or more conditions was selected. When selected, acupoint stimulation was performed according to the patient’s temperament or response. The treatment effect is maximized by gradually increasing the amount of treatment, such as adding more acupoints, long-term immersion, or electric acupuncture.29
In Korea, the development of the Clinical Practice Guidelines (CPGs) of Korean Medicine began in 2016 and is scheduled to be further developed by 2029.30 According to a survey on acupuncture treatment for knee pain in the CPGs for Korean Medicine, 50% of patients received near acupuncture and contralateral acupuncture, while 25.6% received only contralateral acupuncture. The CPGs for Korean Medicine recommendations for the Geoja method showed that while it was widely used in the clinical field, more observational and/or control studies are required to confirm its efficacy.31
Geoja has been used as an effective acupuncture treatment for pain relief in Korean medicine clinical practice. The most basic of these approaches is to diagnose pain meridians and use five important acupoints (五腧穴) of the corresponding meridians on the contralateral side. In particular, treatments that sedate the fire point (火穴) and supplement the water point (水穴) are widely used to provide pain relief.24 For example, as in this study, if a patient had pain in the LU meridian, the LU5 point was supplemented, and the LU10 point was sedated. Among the supplementary and sedative methods to increase acupuncture effect, the Yeong-su-bo-sa method of needling according to the direction of the meridians was used. This technique is the most representative complementary and sedative method among Korean medicine acupuncture treatments. In addition, according to the Korean medicine literature, small-scale studies, and surveys of clinicians, it is important to evaluate the pulse strength when treating using Geoja technique in clinical practice. In this study, As described in Korean medicine literature, the standard was to compare the strength of the left and right pulses.
Our study’s results indicate that 44 (67.6%) of 65 patients with pulse strength differences showed greater than 50% improvement, averaging 55% improvement. In contrast, only 8 (18.2%) of 44 patients without pulse strength differences showed greater than 50% improvement, with an average of approximately 30% improvement. Furthermore, 14 (87.5%) of 16 patients with ROM restrictions and pulse strength differences showed an improvement of at least one grade, with 3 patients improving by two or more grades. In comparison, only 1 out of 6 patients (16.7%) with ROM restrictions and no pulse strength difference showed an improvement of at least one grade. In particular, the effect of acupuncture on the patient with the highest difference in pulse strength was interesting. This patient had complained of elbow pain a week prior, and after receiving only one treatment, the NRS score improved by 70%, and the ROM improved from grade 2 to 4. Another patient with a marked difference in pulse strength complained of shoulder pain 1 month before treatment. However, the NRS 100% improved, and the ROM improved from grades 3 to 5 after 6 treatments over 2 weeks. The detailed analysis of NRS improvement rates, further strengthens the findings regarding the Geoja technique’s efficacy. The median NRS improvement rate of approximately 60% in patients with pulse strength differences, compared to 30% in those without, distinctly highlights a more pronounced central tendency for improvement in the former group. Moreover, the IQR of 40~70% for the pulse-difference group versus 10~40% for the no-difference group indicates not only a higher average response but also a broader and more consistently effective treatment outcome across a larger proportion of patients with a difference in pulse strength. This robust difference in distribution reinforces the clinical relevance of pulse strength assessment in predicting and achieving superior therapeutic benefits with the Geoja technique.
The findings from this study are consistent with previous research on contralateral needling techniques. For instance, a clinical study on mild and moderate carpal tunnel syndrome found that combined therapy using regular acupuncture and contralateral needling at distal acupoints was superior to regular acupuncture alone in terms of therapeutic effects, including median nerve electrophysiology, symptom severity, and function status scores.12 Similarly, research on the contralateral needling method and its applications in treating upper-limb pain11 further supports the efficacy of this approach. Our study extends these observations by specifically linking enhanced outcomes to the presence of a discernible pulse strength difference, which is a novel aspect in this context. These preliminary data suggest that the Geoja technique is a viable treatment option for musculoskeletal pain, with potentially more significant therapeutic effects in patients exhibiting differences in pulse strength.
The enhanced therapeutic effects observed with the Geoja technique, particularly in patients exhibiting pulse strength differences, warrant deeper exploration into the underlying mechanisms. Ipsilateral acupuncture primarily focuses on stimulating points on the same side as the pain for local effects, such as muscle relaxation or immediate pain gating. In contrast, contralateral needling, guided by subtle diagnostic cues like pulse differences, suggests a more holistic, systemic regulatory action. One compelling hypothesis involves the modulation of the autonomic nervous system. Contralateral needling could trigger a balanced regulation of sympathetic and parasympathetic activities,32 thereby influencing pain perception, inflammation, and tissue healing.33–35 This systemic effect, potentially mediated through neuroendocrine pathways, might explain the broader improvements seen beyond the immediate site of needling.36,37 Furthermore, the specific meridian system responses to contralateral stimulation, interpreted through pulse diagnostics, offer another crucial mechanistic avenue. Traditional Korean medicine posits that differences in pulse strength indicate imbalances or dysfunctions within specific meridians,38 and applying the Geoja technique to the contralateral side aims to re-establish the Qi (氣) flow and balance in the affected meridian system.39,40 Future research should explore these distinct mechanistic pathways through studies designed to compare the physiological impacts of ipsilateral versus contralateral acupuncture, especially in cases where systemic imbalances are indicated by pulse differences, to advance our understanding of the Geoja technique.
The strength of the pulse can be sufficiently determined through subjective diagnosis. According to a research on Clinical Application of Muja (繆刺) and Geoja (巨刺) Acupuncture Methods, acupuncture technique related to Geoja are discussed in detail.41 However, the subjective nature of pulse strength assessment by Korean medicine doctors introduces variability, underscoring the need for more objective evaluation methods and tools. Previous studies using cardiovascular simulators have identified pulse parameters such as depth, rate, shape, and strength, reporting that pulse strength varies among individuals and body regions, and is related to pulse amplitude.42 Although our study’s comparison of pulse strength is conceptually similar to evaluating the peak point of pulse amplitude in such simulator studies, the direct connection between subjective strength assessment and objective amplitude measurement remains speculative without empirical evidence. Therefore, to overcome this limitation, future research should explore specific technologies like pulse wave analysis devices capable of objectively measuring parameters such as pulse amplitude. This would help bridge the gap between subjective “strength” assessment and objective “amplitude” measurement. Prospective studies employing such objective tools for pulse strength are needed to scientifically validate the clinical utility of pulse diagnosis in this context.
The CPGs of Korean Medicine consider pulses as an essential diagnosis process before treatment. In particular, pulse diagnosis is crucial in acupuncture treatment. Some research have been conducted on pulses.43,44 Despite this recognized importance and ongoing research efforts, the field of pulse diagnosis still faces limitations in comprehensive studies.
This retrospective study, while offering initial insights into the Geoja technique, highlights several critical considerations that must be acknowledged. As a retrospective chart review, the study’s design inherently limits the ability to draw definitive conclusions regarding treatment effects. The primary objective was to observe the short-term effectiveness of contralateral needling in reducing pain and improving function in musculoskeletal conditions, a goal for which the treatment duration was deemed sufficient. However, a limitation is the absence of long-term follow-up, which restricts the understanding of sustained outcomes for conditions that may have chronic aspects. Another significant methodological challenge lies in the assumption that all patients began with a baseline NRS score of 10 for pain. This was a pragmatic choice in a retrospective study where initial pain scores were not consistently recorded using a standardized scale prior to the intervention. This approach aimed to standardize the measurement of relative improvement from a perceived high pain state, allowing for consistent calculation of improvement rates when only post-treatment NRS scores were reliably available. While this method does not allow for absolute comparisons of severity, it provided a practical way to assess the degree of perceived relief reported by patients relative to a high pain threshold that typically prompts individuals to seek treatment. Furthermore, as an inherent limitation of retrospective studies, concerns regarding potential biases, such as selection bias and recall bias, should also be considered. Finally, the group analyses presented in this study primarily serve descriptive purposes, illustrating observed trends rather than statistically powered subgroup differences. The small sample sizes, particularly within these groups, were not sufficient for robust statistical analysis. Additionally, adjustments for multiple comparisons or confounders, such as age and pain duration, were not applied. These factors, alongside the absence of control groups and the inherent variability introduced by subjective pulse assessment, collectively temper confidence in drawing definitive conclusions and underscore the need for more rigorously designed prospective studies.
Despite these limitations, this study offers several notable strengths. It presents valuable preliminary clinical data on the application of the Geoja technique in a real-world Korean medical clinic setting, a technique whose efficacy is widely recognized clinically but lacks extensive empirical research. The study provides initial evidence supporting the hypothesis that patients with discernible pulse strength differences may experience greater therapeutic benefits from Geoja acupuncture. Furthermore, by categorizing and presenting the clinical characteristics of patients with various types of musculoskeletal pain, the study generates crucial foundational data. This information, encompassing treatment duration, visit frequency, and number of treatments, can be instrumental in designing future, more rigorous studies, including informing sample size calculations and the development of refined selection criteria and treatment indicators. The detailed description of the traditional pulse diagnosis method and acupuncture technique also contributes to the transparency and replicability of this traditional Korean medicine intervention, paving the way for further scientific investigation.
Future research on Geoja acupuncture is required to derive a method to objectively compare left and right pulses. In addition, scientific studies such as randomized controlled clinical studies that specify the selection criteria, treatment period, and the number of treatments for pain diseases should be conducted. This study retrospectively verified the treatment effect of the Geoja technique by comparing the left and right pulse strengths. The clinical characteristics derived from this study, including treatment period, visit period, and number of treatments for variria, sample counts, or treatment indicators for future studies.
Conclusion
This study suggests that Geoja treatment can be effective for pain relief and functional improvement, particularly in patients exhibiting prominent differences in pulse strength between their left and right wrists. Geoja appears to be a safe and effective approach for managing musculoskeletal pain. In this study, a treatment technology that is widely used in Korean medicine, known as opposite treatment, was identified, and the clinical data obtained can provide important information for the design of randomized control studies using objective diagnostic tools and clinical characteristic evaluation indicators. However, the generalizability of these findings to all musculoskeletal disorders is limited. This study focused exclusively on unilateral pain and grouped various musculoskeletal disorders together, which may obscure condition-specific outcomes given their distinct natural courses and treatment responses. In addition, safety claims need more systematic monitoring of adverse events in future prospective studies.
The clinical application of Geoja technique can be further enhanced through prospective clinical trials that focus on optimal disease conditions, standardized interventions, and objective evaluations. Given the critical role of pulse strength differences in the Geoja technique, research is needed to objectively assess pulse characteristics, and standardized treatment combinations based on diagnosis and symptoms should be developed. Prospective, controlled studies are essential to confirm the causal relationship and definitively establish the effectiveness of this technique.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Statement
This retrospective chart review study was conducted in accordance with the Declaration of Helsinki 1975. The study analyzed only pre-existing clinical data from the Hyundong Korean Medical Clinic, Seoul, Republic of Korea, which were fully de-identified and contained no personally identifiable information. According to the guidelines of the Ministry of Health and Welfare of the Republic of Korea, the use of pre-existing, de-identified data does not require prior consent. In addition, under the Bioethics and Safety Act of the Republic of Korea (Enforcement Regulation Article 13, Paragraph 1, Subparagraph 3), such research is exempt from institutional review board (IRB) approval. As the Hyundong Korean Medical Clinic does not operate an institutional review board, ethical approval could not be sought, and no IRB approval number is available. Written informed consent was not required because the data were analyzed retrospectively in a de-identified manner. Although IRB approval and written informed consent were not required for this type of research, written informed consent was voluntarily obtained from all patients, and the collected data were used strictly within the scope permitted for research purposes. This manuscript has been prepared in accordance with the Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (ICMJE guidelines).
Acknowledgments
The authors would like to thank Editage (www.editage.co.kr), for editing and reviewing this manuscript for English language.
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: RS-2020-KH087677).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choi S-K, Moon J-H, Jang W-S, et al. The effectiveness of acupuncture for herpes zoster: a systematic review and meta-analysis. J Acupunct Res. 2023;40(1):16–34. doi:10.13045/jar.2022.00416
2. Putri KE, Murti B, Prasetya H. The effectiveness of acupuncture in reducing musculoskeletal pain: a meta-analysis. Inter Conf Public Health Procee. 2020;5(1):420.
3. Yu Z, Wang -R-R, Wei W, et al. A coordinate-based meta-analysis of acupuncture for chronic pain: evidence from fMRI studies. Front Neurosci. 2022;16:1049887. doi:10.3389/fnins.2022.1049887
4. Zhang Y, Wang C. Acupuncture and chronic musculoskeletal pain. Curr Rheumatol Rep. 2020;22(11):80. doi:10.1007/s11926-020-00954-z
5. Kim J, Lee S, Kim A. A meta-analysis of the effect size of acupuncture on the improvement of low back pain. J Korea Acad Indus Cooperat Soc. 2022;4(4):456–466. doi:10.5762/KAIS.2022.23.4.456
6. Jo H-R, Noh E-J, Oh S-H, et al. Comparative effectiveness of different acupuncture therapies for neck pain. Medicine. 2022;101(33):e29656. doi:10.1097/MD.0000000000029656
7. MacPherson H, Jobst KA, et al. Improving the reporting of interventions in clinical trials of acupuncture: the updated and revised STRICTA. J Altern Complementary Med. 2010;16(9):
8. Heon JS, Jang K-J, Moon H-R, et al. Effect of Korean medicine treatment combined with conventional medicine in patients diagnosed with plantar fasciitis. J Acupunct Res. 2022;39(2):145–149. doi:10.13045/jar.2022.00045
9. Lee I-S, Kim D, Kim JS. Acupuncture points for low back pain patients in clinical trial. J Converge Korean Med. 2021;1(1):25–33.
10. Park J-Y, Yun K-J, Choi Y-J, et al. Comparative study of treatment effect between near acupuncture point needling and near acupuncture with remote acupuncture point needling on treatment of posterior neck pain. J Acupunct Res. 2011;28(1):85–92.
11. M-z Y. Contralateral needling method and its applications in treating upper-limb pain. J Acupunct Tuina Sci. 2012;10(1):58–61. doi:10.1007/s11726-012-0571-3
12. Chen L, Xue L, Li S, Kang T, Chen H, Hou C. Clinical research on mild and moderate carpal tunnel syndrome treated with contralateral needling technique at distal acupoints and acupuncture at local acupoints. Zhongguo Zhen. 2017;37(5):479–482.
13. Dimitrova A, Harrington A, Memmott T, Sisley J, Oken B. Acupuncture-induced changes in nociception, measured by pain-related evoked potentials: a pilot mechanistic study. J Integrat Complemen Med. 2022;28(11):862–869. doi:10.1089/jicm.2021.0369
14. Yan C-Q, Huo J-W, Wang X, et al. Different degree centrality changes in the brain after acupuncture on contralateral or ipsilateral acupoint in patients with chronic shoulder pain: a resting‐state fMRI study. Neural Plast. 2020;2020(1):5701042. doi:10.1155/2020/5701042
15. Zhao C, Xu H, X A, et al. Cerebral mechanism of opposing needling for managing acute pain after unilateral total knee arthroplasty: study protocol for a randomized, sham-controlled clinical trial. Trials. 2022;23(1):133. doi:10.1186/s13063-022-06066-6
16. Lee I-S, Chae Y. Cognitive components of acupuncture treatment. Integrat Med Res. 2021;10(4):100754. doi:10.1016/j.imr.2021.100754
17. Dorsher PT, da Silva MAH. Acupuncture’s neuroanatomic and neurophysiologic basis. Longhua Chin Med. 2022;5:8. doi:10.21037/lcm-21-48
18. Liu J, Gong C. Study on neural pathways of acupuncture analgesia. Interl J Clin Acupunct. 2023;32(4).
19. Xiao Y, Chen Y, Feng Y, Lee K. Advances in neural mechanisms related to acupuncture sensation. Trad Med Modern Med. 2022;5(01n04):1–12. doi:10.1142/S2575900023300011
20. Gong C. On contralateral needling method by Ma Shi originated from the yellow emperor’s classic of medicine. Interl J Clin Acupunct. 2018;27(1).
21. Han C-H, Shin S-W, Ahn S-W, Choi S-M. A survey of actual state of treatment with acupuncture and moxibustion in Korea. J Acupunct Res. 2005;22(6):141–153.
22. Amori P, Aldo L. Acupuncture. Adv Integrat Dermatol. 2019;467–475.
23. Deadman P. The five shu-points. J Chin Med. 1993;31.
24. Kim H-J, Kang J-S. Study on the seventy-fifth question of. J Korean Med Classics. 2009;22(4):189–198.
25. Y-r C, Zhu J, Song J-S, She Y. Discussion on point selection and compatibility of acupuncture formula. Zhongguo Zhen Jiu. 2012;32(1):65–68.
26. Zhou W, Benharash P. Effects and mechanisms of acupuncture based on the principle of meridians. Innov Acupunct Med. 2014;7(4):190–193.
27. Kim S-H. SUNHO YOUNGCHOO. JUMIN; 2003.
28. Experiences KT. Expressions, and boundary-crossings: East Asian tactile diagnostics in South Korea. Med Anthropolog. 2023;42(1):76–89. doi:10.1080/01459740.2022.2139181
29. White A, Cummings M, Filshie J. An introduction to western medical acupuncture. Elsevier Health Sci. 2018.
30. Medicine NCf K. Development status of CPGs in Korean medicine. Secondary development status of CPGs in Korean medicine. Available from: https://nikom.or.kr/engnckm/html.do?menu_idx=81.
31. Medicine NCf K. Clinical practice guidelines DB. Secondary clinical practice guidelines DB. Available from: https://nikom.or.kr/engnckm/module/practiceGuide/index.do?menu_idx=4&gubun=INT&code_gubun=mds?menu_idx=4.
32. Chou L-W, Kao M-J, Lin J-G. Probable mechanisms of needling therapies for myofascial pain control. Evid Based Complemen Alternat Med. 2012;2012(1):705327. doi:10.1155/2012/705327
33. Li RW, Guo J, Dou J, et al. Effect of the contralateral needling therapy on post-stroke shoulder-hand syndrome. Zhen ci yan jiu. 2020;45(2):152–156. doi:10.13702/j.1000-0607.1904786
34. Lu K-W, Hsu C-K, Hsieh C-L, Yang J, Lin Y-W. Probing the effects and mechanisms of electroacupuncture at ipsilateral or contralateral ST36–ST37 acupoints on CFA-induced inflammatory pain. Sci Rep. 2016;6(1):22123. doi:10.1038/srep22123
35. Dunning J, Butts R, Mourad F, Young I, Flannagan S, Perreault T. Dry needling: a literature review with implications for clinical practice guidelines. Phys Ther Rev. 2014;19(4):252–265. doi:10.1179/108331913X13844245102034
36. McDonald JL, Cripps AW, Smith PK. Mediators, receptors, and signalling pathways in the anti‐inflammatory and antihyperalgesic effects of acupuncture. Evid Based Complemen Alternat Med. 2015;2015(1):975632. doi:10.1155/2015/975632
37. Li -Q-Q, Shi G-X, Xu Q, Wang J, Liu C-Z, Wang L-P. Acupuncture effect and central autonomic regulation. Evid Based Complemen Alternat Med. 2013;2013(1):267959.
38. Yin C, Park H-J, Chae Y, et al. Korean acupuncture: the individualized and practical acupuncture. Neurologic Res. 2007;29(sup1):10–15. doi:10.1179/016164107X172301
39. Lin J-A, Wong C-S, Lee M-S, et al. Successful treatment of primary dysmenorrhea by collateral Meridian acupressure therapy. J Manipulat Physiolog Therape. 2010;33(1):70–75. doi:10.1016/j.jmpt.2009.11.003
40. Wong C-S, Yeh -C-C, Ko S-C. Overview of collateral Meridian therapy in pain management: a modified formulated Chinese acupuncture. In:Pain Management-Current Issues and Opinions. IntechOpen;2012.
41. Ban S-W. Clinical Application of Muja(繆刺) and Geoja(巨刺) Acupuncture Methods. Kyunghee university graduate school; 2012.
42. Lee J-Y, Jang M, Shin S-H. Study on the depth, rate, shape, and strength of pulse with cardiovascular simulator. Evid Based Complemen Alternat Med. 2017;2017(1):2867191. doi:10.1155/2017/2867191
43. Kwak B, Yoon J. A study on left-renying and right-Qikou pulse diagnosis (左人迎· 右氣口 脈診法). J Korean Med Classics. 2020;33(1):89–101.
44. Jeong C-H, Jang W-C. The fundamental principles of pulse feeling (脈診) of. J Korean Med Classics. 2007;20(1):137–149.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.