")
Back to Journals » International Journal of General Medicine » Volume 15
Effect of Conbercept Treatment on Macular Edema and Microvascular Structure in Eyes with Retinal Vein Occlusions
Authors Ding X , Wang Y, Zou B, Zang D, Hao Y
Received 11 May 2022
Accepted for publication 24 August 2022
Published 15 September 2022 Volume 2022:15 Pages 7311—7318
DOI https://doi.org/10.2147/IJGM.S373015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoxia Ding, Yu Wang, Bo Zou, Dongxiao Zang, Yi Hao
Department of Ophthalmology, Fushun Eye Hospital, Fushun, Liaoning, People’s Republic of China
Correspondence: Xiaoxia Ding, Fushun Eye Hospital, No. 1 Hupo Street, Xinfu District, Fushun, 113008, People’s Republic of China, Email [email protected]
Objective: To evaluate the efficacy on best corrected visual acuity (BCVA) and microvascular structure changes of conbercept intravitreal injection for the treatment of macular edema (ME) secondary to different types of retinal vein occlusion (RVO) and to explore the baseline OCTA parameters which were related to the change of BCVA and CRT after the intravitreal conbercept injection to RVO.
Methods: A retrospective observational study was conducted involving 67 eyes from 67 patients who were diagnosed with ME secondary to RVO between April 2019 to December 2020. The subjects were divided into branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO) according to the involved vessel, subsequently the subjects received intravitreal conbercept treatment. The BCVA and fundus microstructure were measured to identify predictors of effective outcomes.
Results: BCVA, central retinal thickness (CRT), fovea avascular zone (FAZ), and foveal vascular density (FVD) in superficial capillary plexus (SCP) were significantly changed from baseline to 6-month follow-up in both CRVO and BRVO. In the BRVO group, age and baseline BCVA were correlated with changes of BCVA, while the baseline CRT, FVD in the DCP, and parafovea vascular density (PFVD) in DCP were associated with changes of CRT (P< 0.05). In the CRVO group, the baseline BCVA was correlated with changes of BCVA, while age, gender, baseline CRT, FVD in DCP, and PFVD in DCP were associated with changes of CRT (P< 0.05). There were no serious adverse events (SAEs) related to the drug or the injection procedure.
Conclusion: Intravitreal injections of conbercept can improve BCVA and CRT and change the FVD in SCP effectively both in BRVO and CRVO groups. In addition, the baseline FVD and PFVD in the DCP were related to the change of CRT after intravitreal conbercept treatment.
Keywords: conbercept, retinal vein occlusion, macular edema, microvascular structure, best-corrected visual acuity
Introduction
Retinal vein occlusion (RVO) is an obstruction of the retinal venous system by thrombus formation.1 Many demographic environmental, systemic, and ocular factors increase the risk on incidence of RVO, such as age, cardiovascular comorbidities, hypertension, and glaucoma.2,3 Patients often suffer from sudden, monocular vision loss. Depending on the extent of the affected retinal tissue, distinction is made between central retinal vein occlusion (CRVO) and branch retinal vein occlusion (BRVO). RVO often leads to vision-threatening retinal vascular disorders, such as secondary cystoid macular edema (ME), retinal neovascularization, neovascular glaucoma, and other complications.4 Among those complications, ME is a frequent and main cause of sight-threatening disorders.5 Thus, the prevention and treatment of ME secondary to RVO is still an important clinical issue in practice.
Vascular endothelial growth factor (VEGF) plays a key role in the pathogenesis of ME secondary to RVO.6 It is a cytokine produced by hypoxic cells that stimulates vascular permeability and proliferation by binding to endothelial cell receptors. Based on numbers of prospective clinical trials, anti-VEGF therapy has become the preferred first-line therapy for ME to RVO. Conbercept (Chengdu Kanghong Biotech Co., Ltd., Sichuan, China) is a new recombinant fusion protein consisting of the extracellular domain 2 of VEGF receptor (VEGFR) 1 and extracellular domains 3 and 4 of VEGFR 2 combined with the Fc portion of the human immunoglobulin G1, which can inhibit the activity of VEGF and effectively penetrate the whole retinal layer.7 Importantly, intravitreal injection with conbercept represents an excellent option for treating ME to improve visual acuity in RVO with a satisfactory safety profile and efficacy.8 However, the retinal blood circulation of blocking VEGF remain a concern; one of which is whether anti-VEGF therapy impairs microvascular structure changes in eyes with both BRVO and CRVO. Recently, noninvasive optical coherence tomography angiography (OCTA) provided mapping of several retinal and choroidal vascular layers. The OCTA factors such as FAZ area, vascular density of the SCP, DCP in the fovea and parafovea can evaluate the ocular pathologies with their associated vessels, but few studies explored the predictor effect of OCTA factors on change of BCVA and CRT of RVO. And few reports have been published regarding patients with both BRVO and CRVO complicated by ME who were treated with the conbercept and evaluated using OCTA within a long-term follow-up. The aim of this study is, therefore, to evaluate the efficacy on BVCA and microvascular structure changes of conbercept intravitreal injection for the treatment of macular edema (ME) secondary to different types of retinal vein occlusion (RVO). Another aim of this study was to evaluate the baseline OCTA parameters which were related to the change of BCVA and CRT after the intravitreal conbercept injection to RVO.
Methods
Ethics Statement
This study protocol conforms to the ethical guidelines of the tenets of the Declaration of Helsinki (2008) and was approved by the Institutional Review Board of Fushun Eye Hospital. There was a waiver of consent in the present retrospective study as this project meets the criteria according to Health & Human Services regulations.
Study Population
This retrospective study is of patients with an established diagnosis of ME secondary to RVO who received intravitreal conbercept injections from April 2019 to December 2020. Patients who developed an RVO within 6 months of the enrollment date with ME secondary to either a BRVO or CRVO [as confirmed on fundus angiography or optical coherence tomography (OCT)] were consecutively recruited into the study.
All patients were identified at ophthalmologic clinic of Fushun Eye Hospital. Inclusion criteria were as follows: age ≥18 years old; intraocular pressure (IOP) <21 mmHg, best-corrected visual acuity (BCVA) ≥0.3 (logarithm of the minimum angle of resolution, logMAR),9 and central retinal thickness (CRT) ≥250 µm; and accepted OCTA examinations. Exclusion criteria were as follows: presence of chronic dacryocystitis, glaucoma, cataract, severe proliferative vitreoretinopathy or vitreous hemorrhage, macular epiretinal membrane or macular ischemia, diabetic retinopathy, age-related macular degeneration, ocular trauma history, or other retinal/ocular diseases; prior systemic anti-VEGF therapy, and undergone intraocular steroid therapy in the study eye within 3 months.
Study Examinations
At baseline, all patients underwent a comprehensive ophthalmologic examination, which included measurement of BCVA, slit-lamp biomicroscopy, indirect ophthalmoscopy, IOP (Canon TX-20, Canon Corporation, Tokyo, Japan), CRT [spectral-domain OCT (Spectralis, Heidelberg Engineering, Heidelberg, Germany)], fovea avascular zone (FAZ), fovea vascular density (FVD), and parafovea vascular density (PFVD) in superficial capillary plexus (SCP) and in deep capillary plexus (DCP) using OCTA (software ReVue version 2017.1.0.155, Optovue Inc., Fremont, CA), fluorescein fundus angiography (FFA, Spectralis, Heidelberg, Germany). Systemic and ophthalmic medical history, as reported by patients, was also carefully reviewed. BCVA, IOP, CRT, and OCTA measurements were re-examined 1-, 2-, 3-, and 6-months after treatment.
Study Treatments
All eyes were treated by intravitreal injection of conbercept (0.05 mL/0.5 mg; Chengdu Kang Hong Biotechnology Co., Ltd.) on a 3 + pro re nata (3+PRN) basis. Eyes were re-injected if either of the following conditions occurred during follow-up: 1) increase of 100 μm in CRT compared with the previous measurement; 2) >2 lines of vision decrease in Snellen acuity; 3) presence of new retinal neovascularization.
The Evaluation of Fundus Microstructure
For each eye, a 6×6-mm scan centered on the fovea was acquired using OCTA. The SCP en face image was segmented with an inner boundary at 3 μm beneath the internal limiting membrane and an outer boundary set at 15 μm beneath the inner plexiform layer, whereas the DCP en face image was segmented with an inner boundary 15 μm beneath the inner plexiform layer and an outer boundary at 70 μm beneath the inner plexiform layer. The FAZ, vascular density of the SCP, DCP in the fovea and parafovea automatically generated by the instrument was recorded (Figure 1).
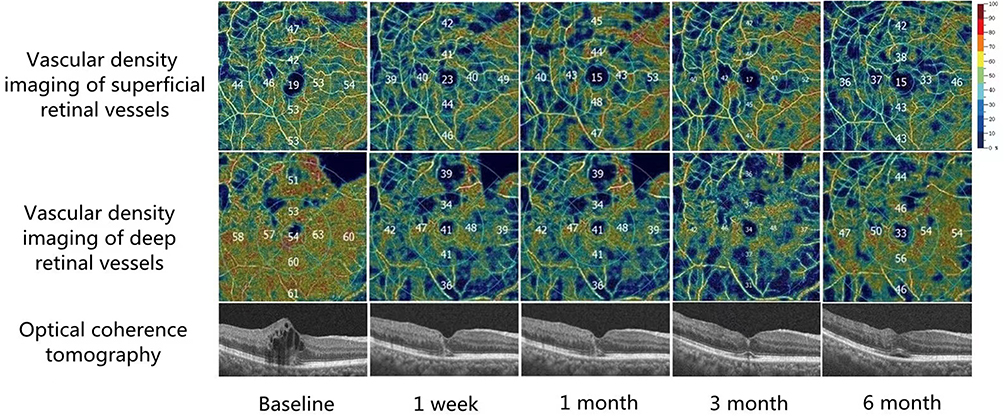 |
Figure 1 The changes of vascular density of SCP and DCP after intravitreous Conbercept injections. A 65-year-old female presented with marked severe cystoid macular edema secondary to branch retinal vein occlusion in the left eye. This patient received four intravitreous conbercept injections at baseline, 1, 2, and 5 months. After 6 months, his best corrected visual acuity (logMAR) significantly improved from 1.0 at baseline to 0.3 associated with an obvious reduction in central retinal thickness. |
Definition
BRVO was defined by the presence of retinal hemorrhages or other biomicroscopic evidence of RVO and a dilated venous system in one or two quadrants of the retina drained by the same vein; CRVO was defined as a RVO that involved four retinal quadrants.10 Vessel density was calculated as the proportion of the measured area occupied by blood vessels with flow, defined as pixels having decorrelation values above the threshold level. The fovea was defined as the area within the central 1-mm ring of the Early treatment Diabetic retinopathy Study (ETDRS) grid. Parafovea was defined as the area between the central 1- and the 3-mm ring of the ETDRS grid. The duration of BRVO or CRVO at baseline was determined using the onset of symptoms (the date when the patient first became aware of a decrease in visual acuity) as the start date of the RVO.
Statistical Analysis
All statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL). Quantitative data were expressed as mean value±standard deviation (SD), while qualitative data were expressed as frequency (percentage). The Student’s t-test or the Mann–Whitney U-test was used to determine the significance of the differences in quantitative data between BRVO and CRVO groups. Categorical variables were compared using the Chi-square test. Multivariable linear regression model was used for assessing the influence factors on the change of BCVA and CRT from baseline to the last visit. All statistical tests were two-sided and a P-value less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
Sixty-seven eyes of 67 patients (51 eyes with BRVO and 16 eyes with CRVO) were enrolled. The baseline characteristics of two groups are presented in Table 1. Patients in the BRVO group had significantly better BCVA and lower levels of CRT and FAZ, while the duration of the BRVO group was significantly longer and FVD in DCP was significantly larger in the BRVO group compared to the CRVO group.
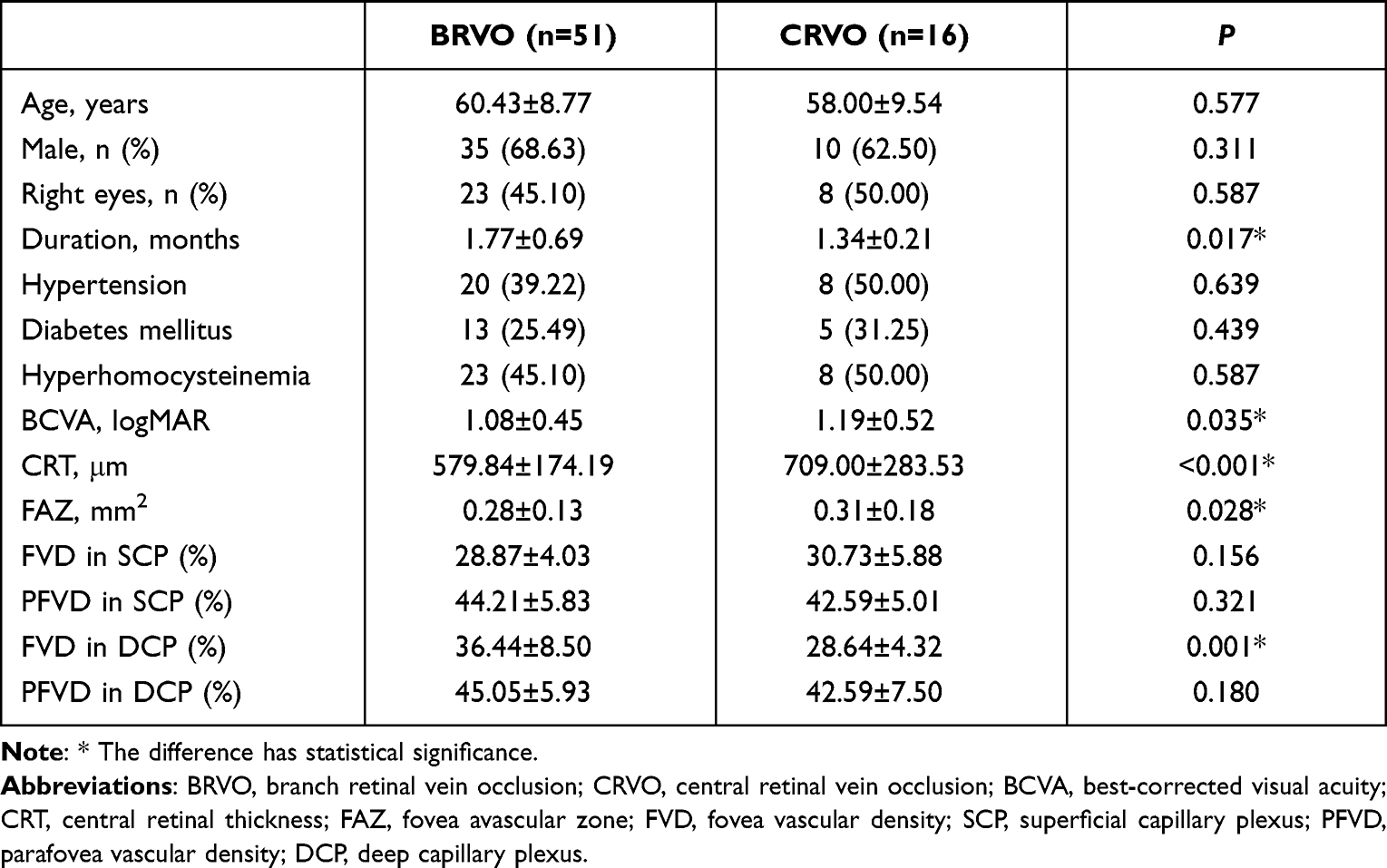 |
Table 1 Baseline Characteristics of the Included Subjects |
Changes of Patients’ Characteristics in Two Groups
The mean changes of BCVA, CRT, FAZ, and FVD in SCP from baseline to month 6 in BRVO and CRVO groups are referred to in Figure 2A–D. The changes of the PFVD in SCP, FVD in DCP, and PFVD in DCP were not significant both in BRVO and CRVO groups (Figure 2E–G).
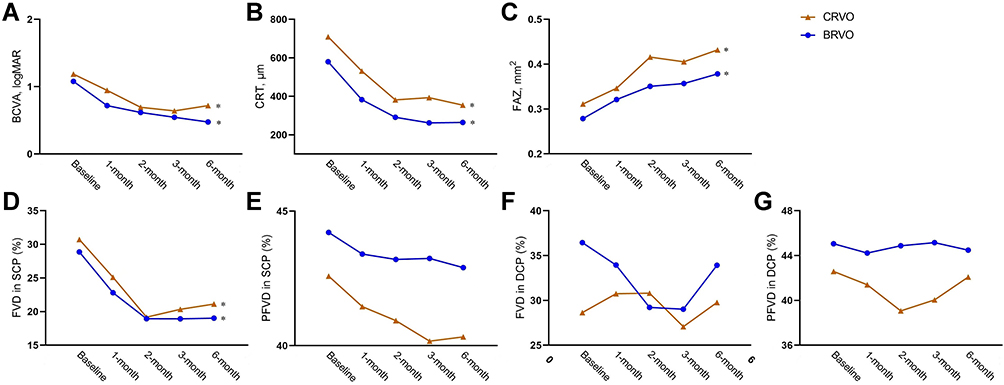 |
Figure 2 Time course of evaluation of the therapeutic effect of intravitreous Conbercept injection at baseline and each follow-up visit evaluation of branch retinal vein occlusion (BRVO) group and central retinal vein occlusion (CRVO) group. (A) Best-corrected visual acuity (BCVA) logarithm of the minimum angle of resolution (logMAR); (B) Central retinal thickness (CRT); (C) Fovea avascular zone (FAZ); (D) Fovea vascular density (FVD) in superficial capillary plexus (SCP); (E) Parafovea vascular density (PFVD) in superficial capillary plexus (SCP); (F) Fovea vascular density (FVD) in deep capillary plexus (DCP); (G) Parafovea vascular density (PFVD) in deep capillary plexus (DCP). *Significance between baseline and month 6. |
Baseline Characteristics with Changes of BCVA and CRT
The results of the linear regression analysis of basic characteristics with changes of BCVA and CRT from baseline to follow-up in two groups are summarized in Tables 2 and 3, respectively. In the BRVO group, age and baseline BCVA were correlated with changes of BCVA (P<0.05); the baseline CRT, FVD in the DCP, and PFVD in DCP were associated with changes of CRT (P<0.05). In the CRVO group, the baseline BCVA were correlated with changes of BCVA (P<0.05); age, gender, baseline CRT, FVD in DCP, and PFVD in DCP were associated with changes of CRT (P<0.05).
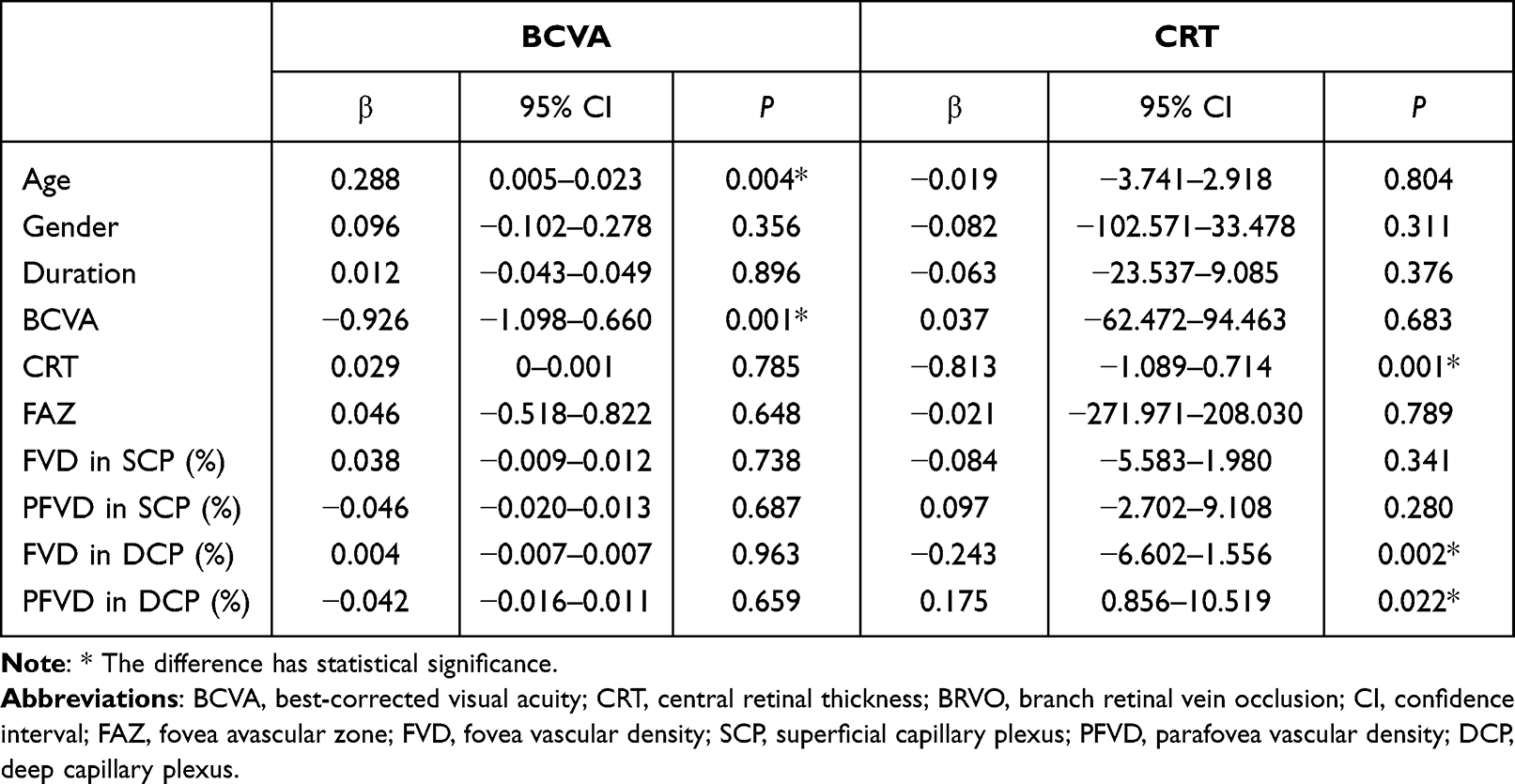 |
Table 2 Linear Regression Analysis of Baseline Characteristics with Changes of BCVA and CRT Over 6 Months in BRVO |
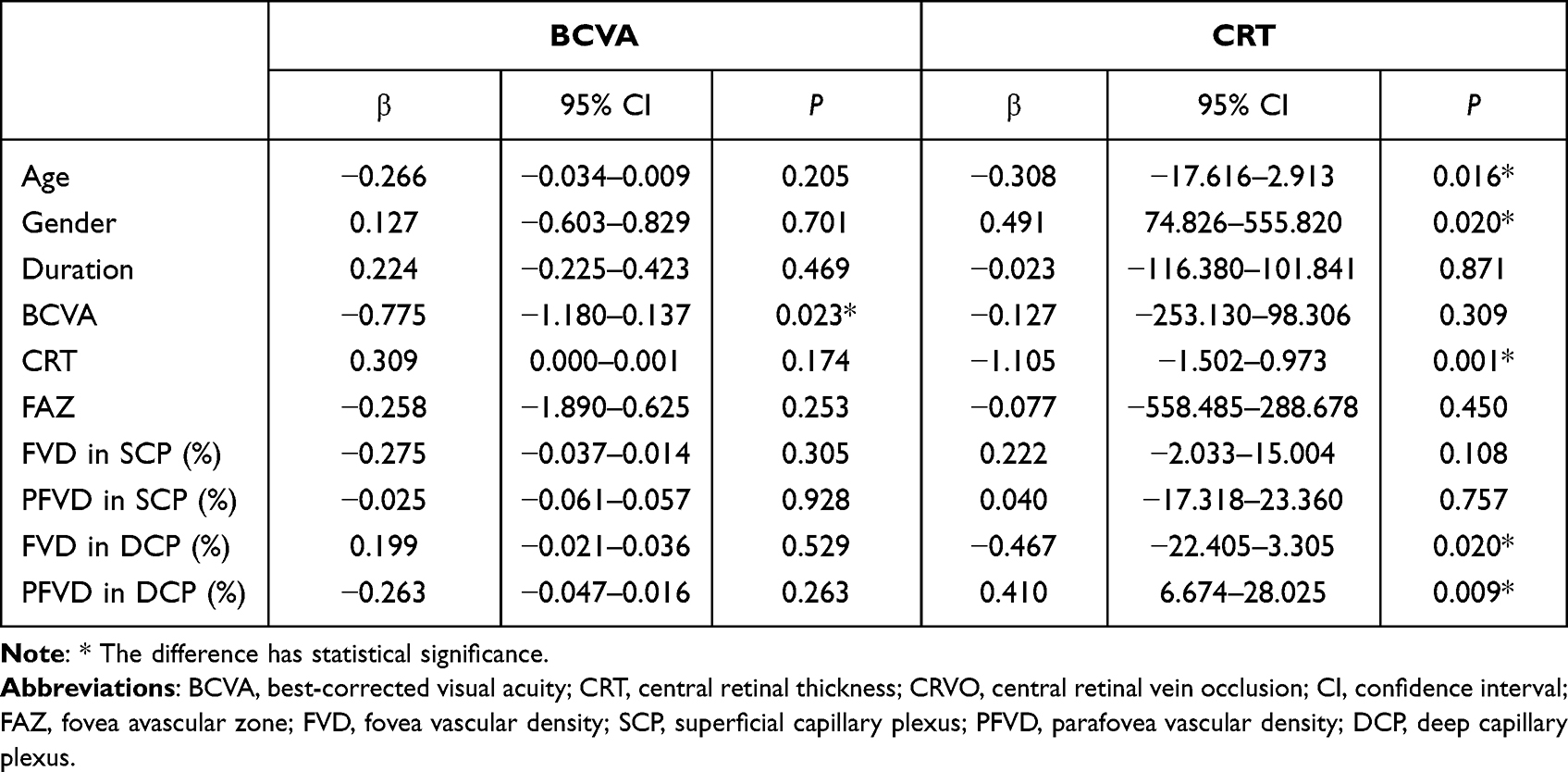 |
Table 3 Linear Regression Analysis of Baseline Characteristics with Changes of BCVA and CRT Over 6 Months in CRVO |
Number of Injections
In the per protocol set, the mean number of injections was 3.59±0.73 (interquartile range=4.00–3.00) in BRVO and 4.00±0.89 (interquartile range=4.75–3.00) in CRVO from baseline to month 6. There was not a significant difference between the groups regarding the mean number of injections (P=0.07).
Serious Adverse Events
Intravitreal conbercept was generally well tolerated. From baseline to 6 months follow-up, the cases experiencing at least one ocular side adverse events (SAE) in the study eye was similar in BRVO and CRVO groups, and all the SAEs were not related to the drug or the injection procedure (Table 4).
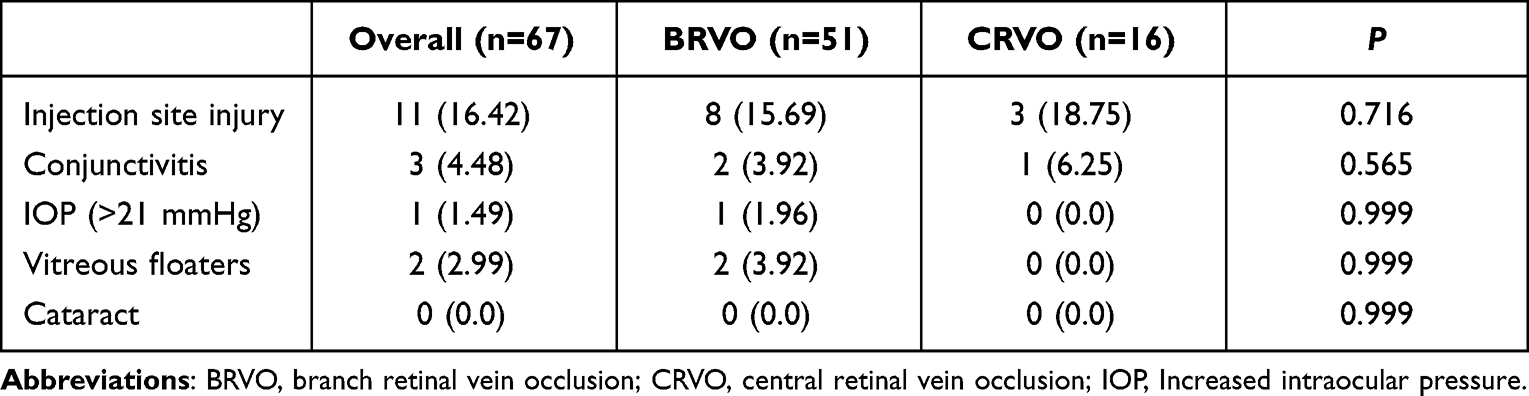 |
Table 4 Ocular Serious Adverse Events After Injection of Conbercept, n (%) |
Discussion
Overexpression of VEGF and its receptors has been closely related to serum protein exudation, retinal thickening, and the presence of ME.11 In addition, ischemia of local retinal tissue after RVO can increase VEGF in the retinal pigment epithelium, pericytes, and microvascular endothelial cells. VEGF causes blood vessels to expand and increases blood flow, as well as increasing permeability through enhanced production of nitric oxide, and this leads to the accumulation of liquid, ME formation.12 CRVO and BRVO are two distinct clinical entities with varying natural course and the response to and length of treatment,13 although CRVO accounts for only approximately 20% of RVOs, it leads to poorer visual acuity prognoses and quality-of-life when compared to patients with BRVO.14,15 Anti-VEGF agents therapy has been promoted for the management of RVO because it can inhibit angiogenesis and decrease vascular permeability in retina,16 several studies have confirmed the effect of different anti-VEGF agents against RVO, such as VIBRANT study (demonstrated the efficacy of monthly intravitreal aflibercept injection on macular edema secondary to BRVO at 24 weeks) and RETAIN study (described good long-term results in BRVO patients treated with ranibizumab).17,18 Conbercept has strong bioactivity with VEGF.16,19 In our study we established the efficacy on logMAR BCVA and CRT of conbercept intravitreal injection for the treatment of macular edema secondary to RVO, which was compatible with the findings of previous studies.8,20 In the study, we established the safety of intravitreal conbercept therapy on RVO, there are no ocular side adverse events (SAE) in the study eye which were related to the drug or the injection procedure in both BRVO and CRVO groups.
OCTA is a fast, noninvasive test, and allows improved and accurate visualization of microvascular changes. OCTA allows better visualization of the microvascular abnormalities in RVO, including neovascular fronds, FAZ, and other microvascular abnormalities at the level of the SCP and DCP.21–23 In the current study, we found FAZ area and mean foveal vascular density at the level of the SCP as measured by OCTA changed after intravitreal conbercept injection. Mean parafoveal vascular density at the level of the SCP and DCP as measured by OCTA remained stable after following intravitreal conbercept injection. Previous studies illustrated that anti-VEGF therapy did not worsen capillary nonperfusion.24 The enlargement of FAZ area may be due to the ischemia which had caused nonreversible damage of retinal capillary in RVO patients. Another possible cause was the retinal capillary system in eyes with cystoid macular edema (CME) which may be displaced by the physical effect of the cystoid spaces, and the central macula was more apt to be affected by CME. Consequently, the enlargement of FAZ and the decrease of foveal vascular density at the level of SCP simply reflect a resolution of segmentation artifact and not deterioration in the capillary flow. Parafoveal vascular density at the level of the SCP and DCP which was less affected by CME remained stable after intravitreal conbercept injection. Feucht et al25 reported similar changes of FAZ measured in FA images after anti-VEGF therapy in CME secondary to RVO. However, several studies showed that retinal capillary density and FAZ area remained statistically unchanged in the short-term after a single intravitreal injection of an anti-VEGF agent.26,27
In our study, we established baseline BCVA was the predictor of the change of BCVA, patients with low baseline BCVA showed greater improvement than patients with higher baseline BCVA. However, in our study we did not find the baseline CRT and duration were associated with BCVA outcomes, which was not consistent with the former study.28 We found higher baseline CRT was associated with a greater decrease in CRT that was consistent with the findings of Scott et al,29 and we did not find duration was associated with the change of CRT.
None of these OCTA factors such as FAZ area, vascular density of the SCP, DCP in the fovea and parafovea were found to be associated with BCVA outcome after intravitreal injections in our study. Nevertheless, in both BRVO and CRVO groups, we found baseline FVD and PFVD in the DCP were related to the change of CRT, which might suggest the micro-structure of the DCP was more easily affected by ME.30,31
Notably, the present study has some limitations. First, the number of patients was relatively small. Because there is no previous report on the differences between BRVO and CRVO after conbercept treatment, it is difficult to calculate the sample size. Herein, we included 67 patients with RVO, but only 16 patients with CRVO. We knew that the power for determining if any differences between diagnosis types have any hope of reaching significance was limited. A further large sample size study is needed to provide robust evidence. Second, there is a possibility of significant referral bias because of the retrospective and single-center design of the study. Third, data on more long-term events and follow-up were relatively insufficient and are planned to be included in a future study. At last some types of artifacts may affect the OCTA measurements, especially in eyes with ocular diseases.32
Conclusion
Intravitreal injections of conbercept can improve BCVA, CRT, and change the FVD in SCP effectively in both BRVO and CRVO groups. In addition, the baseline FVD and PFVD in the DCP were related to the change of CRT after intravitreal conbercept treatment.
Acknowledgments
We would like to thank Gang Zhai for critically reviewing the study proposal, Jingbin Zhao and Junting Zhang for collecting data, and Qiao Wang, who provided and cared for study patients.
Funding
This study was supported by Liaoning Province Natural Science Foundation of China (No. 20180550094).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Keel S, Xie J, Foreman J, van Wijngaarden P, Taylor HR, Dirani M. Prevalence of retinal vein occlusion in the Australian National Eye Health Survey. Clin Exp Ophthalmol. 2018;46:260–265. doi:10.1111/ceo.13031
2. Trovato Battagliola E, Pacella F, Malvasi M, et al. Risk factors in central retinal vein occlusion: a multi-center case-control study conducted on the Italian population: demographic, environmental, systemic, and ocular factors that increase the risk for major thrombotic events in the retinal venous system. Eur J Ophthalmol. 2021:11206721211064469. doi: 10.1177/11206721211064469
3. Pacella F, Bongiovanni G, Malvasi M, et al. Impact of cardiovascular risk factors on incidence and severity of Retinal Vein Occlusion. La Clinica terapeutica. 2020;171:e534–e538. doi:10.7417/CT.2020.2269
4. Klein R, Klein BE, Moss SE, Meuer SM. The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc. 2000;98:
5. Maggio E, Mete M, Maraone G, Attanasio M, Guerriero M, Pertile G. Intravitreal injections for macular edema secondary to retinal vein occlusion: long-term functional and anatomic outcomes. J Ophthalmol. 2020;2020:7817542. doi:10.1155/2020/7817542
6. Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331:1480–1487. doi:10.1056/NEJM199412013312203
7. Zhang M, Yu D, Yang C, et al. The pharmacology study of a new recombinant human VEGF receptor-fc fusion protein on experimental choroidal neovascularization. Pharmaceut Res. 2009;26:204–210. doi:10.1007/s11095-008-9718-9
8. Sun Z, Zhou H, Lin B, et al. Efficacy and safety of intravitreal conbercept injections in macular edema secondary to retinal vein occlusion. Retina. 2017;37:1723–1730. doi:10.1097/IAE.0000000000001404
9. Holladay JT. Proper method for calculating average visual acuity. J Refract Surg. 1995;13(1997):388–391. doi:10.3928/1081-597X-19970701-16
10. Sperduto RD, Hiller R, Chew E, et al. Risk factors for hemiretinal vein occlusion: comparison with risk factors for central and branch retinal vein occlusion: the eye disease case-control study. Ophthalmology. 1998;105:765–771. doi:10.1016/S0161-6420(98)95012-6
11. Feng J, Zhao T, Zhang Y, Ma Y, Jiang Y. Differences in aqueous concentrations of cytokines in macular edema secondary to branch and central retinal vein occlusion. PLoS One. 2013;8:e68149. doi:10.1371/journal.pone.0068149
12. Tao Y, Huang C, Liu M, et al. Short-term effect of intravitreal conbercept injection on major and macular branch retinal vein occlusion. J Int Med Res. 2019;47:1202–1209. doi:10.1177/0300060518819613
13. Chatziralli I, Nicholson L, Sivaprasad S, Hykin P. Intravitreal steroid and anti-vascular endothelial growth agents for the management of retinal vein occlusion: evidence from randomized trials. Exp Opinion Biol Ther. 2015;15:1685–1697. doi:10.1517/14712598.2015.1086744
14. Sivaprasad S, Amoaku WM, Hykin P, Guideline Group RV. The Royal College of Ophthalmologists Guidelines on retinal vein occlusions: executive summary. Eye. 2016;30:642. doi:10.1038/eye.2016.16
15. Cugati S, Wang JJ, Rochtchina E, Mitchell P. Ten-year incidence of retinal vein occlusion in an older population: the Blue Mountains Eye Study. Arch Ophthalmol. 2006;124:726–732. doi:10.1001/archopht.124.5.726
16. Wang Q, Li T, Wu Z, et al. Novel VEGF decoy receptor fusion protein conbercept targeting multiple VEGF isoforms provide remarkable anti-angiogenesis effect in vivo. PLoS One. 2013;8:e70544. doi:10.1371/journal.pone.0070544
17. Campochiaro PA, Clark WL, Boyer DS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT study. Ophthalmology. 2015;122:538–544. doi:10.1016/j.ophtha.2014.08.031
18. Campochiaro PA, Sophie R, Pearlman J, et al. Long-term outcomes in patients with retinal vein occlusion treated with ranibizumab: the RETAIN study. Ophthalmology. 2014;121:209–219. doi:10.1016/j.ophtha.2013.08.038
19. Zhang X, Wu J, Wu C, Bian AL, Geng S, Dai RP. Comparison of aqueous humor levels of PlGF and VEGF in proliferative diabetic retinopathy before and after intravitreal conbercept injection. Diabetes Res Clin Pract. 2020;162:108083.
20. Chen X, Hu TM, Zuo J, et al. Intravitreal conbercept for branch retinal vein occlusion induced macular edema: one initial injection versus three monthly injections. BMC Ophthalmol. 2020;20:225. doi:10.1186/s12886-020-01494-x
21. Tsai G, Banaee T, Conti FF, Singh RP. Optical coherence tomography angiography in eyes with retinal vein occlusion. J Ophthalmic Vis Res. 2018;13:315–332. doi:10.4103/jovr.jovr_264_17
22. Glacet-Bernard A, Sellam A, Coscas F, Coscas G, Souied EH. Optical coherence tomography angiography in retinal vein occlusion treated with dexamethasone implant: a new test for follow-up evaluation. Eur J Ophthalmol. 2016;26:460–468. doi:10.5301/ejo.5000829
23. Mastropasqua R, Toto L, Di Antonio L, et al. Optical coherence tomography angiography microvascular findings in macular edema due to central and branch retinal vein occlusions. Sci Rep. 2017;7:40763. doi:10.1038/srep40763
24. Campochiaro PA, Bhisitkul RB, Shapiro H, Rubio RG. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology. 2013;120:795–802. doi:10.1016/j.ophtha.2012.09.032
25. Feucht N, Schönbach EM, Lanzl I, Kotliar K, Lohmann CP, Maier M. Changes in the foveal microstructure after intravitreal bevacizumab application in patients with retinal vascular disease. Clin Ophthalmol. 2013;7:173–178. doi:10.2147/OPTH.S37544
26. Ghasemi Falavarjani K, Iafe NA, Hubschman JP, Tsui I, Sadda SR, Sarraf D. Optical coherence tomography angiography analysis of the foveal avascular zone and macular vessel density after Anti-VEGF therapy in eyes with diabetic macular edema and retinal vein occlusion. Invest Ophthalmol Visual Sci. 2017;58:30–34. doi:10.1167/iovs.16-20579
27. Michaelides M, Fraser-Bell S, Hamilton R, et al. Macular perfusion determined by fundus fluorescein angiography at the 4-month time point in a prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (Bolt Study): report 1. Retina. 2010;30:781–786. doi:10.1097/IAE.0b013e3181d2f145
28. Hsueh J, Wai KM, Conti FF, Conti TF, Singh RP. Impact of time to anti-vascular endothelial growth factor intervention on visual outcomes for patients diagnosed with retinal vein occlusion. Ophthal Surg, Lasers Imag Retina. 2018;49:832–837. doi:10.3928/23258160-20181101-03
29. Scott IU, VanVeldhuisen PC, Ip MS, et al. Baseline factors associated with 6-month visual acuity and retinal thickness outcomes in patients with macular edema secondary to central retinal vein occlusion or hemiretinal vein occlusion: SCORE2 Study Report 4. JAMA Ophthalmol. 2017;135:639–649. doi:10.1001/jamaophthalmol.2017.1141
30. Kang JW, Yoo R, Jo YH, Kim HC. Correlation of microvascular structures on optical coherence tomography angiography with visual acuity in retinal vein occlusion. Retina. 2017;37:1700–1709. doi:10.1097/IAE.0000000000001403
31. Coscas F, Glacet-Bernard A, Miere A, et al. Optical coherence tomography angiography in retinal vein occlusion: evaluation of superficial and deep capillary plexa. Am J Ophthalmol. 2016;161:
32. Ghasemi Falavarjani K, Al-Sheikh M, Akil H, Sadda SR. Image artefacts in swept-source optical coherence tomography angiography. Br J Ophthalmol. 2017;101:564–568. doi:10.1136/bjophthalmol-2016-309104
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.