Back to Journals » Journal of Inflammation Research » Volume 14
Effect of Biologics on Cardiovascular Inflammation: Mechanistic Insights and Risk Reduction
Authors Fragoulis GE, Soulaidopoulos S, Sfikakis PP, Dimitroulas T, Kitas GD
Received 3 March 2021
Accepted for publication 14 April 2021
Published 14 May 2021 Volume 2021:14 Pages 1915—1931
DOI https://doi.org/10.2147/JIR.S282691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
George E Fragoulis,1,* Stergios Soulaidopoulos,2,* Petros P Sfikakis,1 Theodoros Dimitroulas,3 George D Kitas4,5
1Rheumatology Unit, Joint Rheumatology Program, Medical School, First Department of Propaedeutic Internal Medicine, National and Kapodistrian University of Athens, “Laiko” General Hospital, Athens, 115 27, Greece; 2First Department of Cardiology, National and Kapodistrian University of Athens, Hippokration General Hospital, Athens, 115 27, Greece; 3Fourth Department of Internal Medicine, Hippokration Hospital, School of Medicine, Aristotle University of Thessaloniki, Thessaloniki, 546 41, Greece; 4Department of Rheumatology, Russells Hall Hospital, Dudley Group NHS FT, Dudley, DY1 2HQ, UK; 5Arthritis Research UK Epidemiology Unit, University of Manchester, Manchester, M13 9PT, UK
*These authors contributed equally to this work
Correspondence: Stergios Soulaidopoulos
First Department of Cardiology, National and Kapodistrian University of Athens, 114 Vasilissis Sofias av., Athens, 11527, Greece
Tel +306932528561
Fax +302132088676
Email [email protected]
Abstract: It is increasingly recognized that atherosclerosis and consequently cardiovascular disease (CVD) are closely linked with inflammatory processes. The latter is in the center of the pathogenic mechanism underlying autoimmune rheumatic diseases (ARD). It follows then, that optimal control of inflammation in ARDs may lead to a decrease of the accompanied CVD risk. Major trials (eg, CANTOS, CIRT), aimed at examining the possible benefits of immunomodulatory treatments in CVD, demonstrated conflicting results. On the other hand, substantial evidence is accumulating about the possible beneficial effects of biologic disease modifying antirheumatic drugs (bDMARDs) in patients with ARDs, particularly those with rheumatoid arthritis (RA). It seems that bDMARDs (some more than others) alter the lipid profile in RA patients but do not adversely affect, in most cases, the TC/HDL ratio. Favorable effects are noted for arterial stiffness and endothelial function. This is reflected in the lower risk for CVD events, seen in observational studies of RA patients treated with bDMARDs. It should be stressed that more data exist for the TNF-inhibitors than for other bDMARDs, such as tocilizumab, abatacept and rituximab. As regards the spondyloarthropathies (SpA), data are less robust. For TNF-inhibitors, effects appear to be on par with those seen in RA but no conclusions can be drawn for newer biologic drugs used in SpA (eg, IL-17 blockers). Finally, there is accumulating evidence for a beneficial effect of immunosuppressive treatment in cardiac inflammation and function in several ARDs. Introduction of newer therapeutic options in clinical practice seem to have a positive impact on CVD in the setting of ARD. This is probably due to better control of inflammation, but direct improvement in vascular pathology is also a valid hypothesis. Most data are derived from observational studies and, therefore, randomized controlled trials are needed to assess the possible favorable effect of bDMARDs on CVD outcomes.
Keywords: atherosclerosis, cardiovascular disease, biologic agents, interleukins, inflammatory disorders
Introduction
There is now sufficient experimental and clinical evidence to support that atherosclerosis represents a chronic inflammatory process evolving within the wall of large and medium-sized arteries rather than just the result of passive lipid accumulation in the arterial wall.1 In fact, inflammation dominates all steps of the atherogenic process, starting with the recruitment of leukocytes and the expression of pro-inflammatory cytokines at sites of endothelial dysfunction that ultimately result in the formation of and progression to a vulnerable atherosclerotic plaque.2
A complex interplay between the high-grade inflammatory process and classic cardiovascular risk factors has been recognized as the pathogenetic substrate for excessive cardiovascular morbidity and mortality characterizing the whole spectrum of autoimmune rheumatic disorders (ARD), mainly rheumatoid arthritis (RA),3 systemic lupus erythematosus (SLE) and the spondyloarthropathies (SpA).4,5 In particular, the overexpression of several proinflammatory cytokines with an established role in atherogenesis, such as tumor necrosis factor alpha (TNF-α) and interleukin 6 (IL-6), leads to endothelial dysfunction and contributes to the development of premature atherosclerosis.6 Given the shared pathogenic features between the inflammatory response and atherosclerosis, sufficient control of disease activity is one of the two main targets of cardiovascular disease (CVD) management in ARDs (the other one being adequate control of classical CVD risk factors).7 Indeed, a remarkable improvement in surrogate markers of atherosclerosis, such as arterial stiffness and carotid intima-media thickness (cIMT) after sufficient control of the disease in patients with RA has been documented.8,9 Beyond subclinical atherosclerosis, cardiovascular inflammation encompasses ischemic cardiovascular events, such as myocardial infarction and strokes, myocardial inflammation, pericardial inflammation and heart failure, all of which are present in patients with ARD as a consequence of chronic high-grade inflammatory state. To that end, interest is now diverting towards novel therapeutic approaches that expand beyond the management of traditional cardiovascular risk factors, targeting specific agents in the inflammatory cascade with promising results.10
Over the last 3 decades, biologic disease modifying drugs (bDMARDs) have proved to be very effective at controlling the inflammatory burden and altering to the better the natural history of ARDs. Designed to block key mediators of the immune response, namely TNF-α, IL-1 and IL-6, bDMARDs have radically improved the prognosis and quality of life of patients with ARDs. Beyond their striking efficacy in achieving stable and low disease activity, bDMARDs also appear to associate with overall improved cardiovascular outcomes in these populations.11 Based on the inflammatory hypothesis of atherosclerosis, the addition of biologics as a complementary therapeutic option for CVD beyond the context of systemic inflammatory diseases is steadily gaining attention, although large-scale clinical trials with hard cardiovascular endpoints are still scarce.12,13
The aim of this review is to provide an insight into the inflammatory aspects of atherosclerosis and subsequently critically summarize and discuss current data about the effects of biologic treatments on cardiovascular inflammation, focusing on studies assessing their impact on surrogate markers of CVD and cardiovascular outcomes.
Search Strategy
A review of the English literature published in the online databases Medline, Cochrane and Embase was performed to December 2020, searching for randomized controlled trials, observational studies and review articles concerning the association between biologic agents and the risk of cardiovascular events.
The search consisted of three components, each of them represented by specific Medical Subject Headings (MeSH) terms: (a) the autoimmune rheumatic disorder utilizing the terms “rheumatoid arthritis”, “ankylosing spondylitis” and “psoriatic arthritis” and “spondyloarthropathies”; (b) the biologic agent, utilizing the terms “biologics”, “biologic DMARDs”, “TNF-α antagonists”, “TNF inhibitors”, “anti-TNFs”, “anti-IL6”, “anti-IL1”, “canakinumab”, “tocilizumab”, “rituximab”, “abatacept”, “anakinra”, “etanercept”, “infliximab”, “adalimumab”, “golimumab”; “certolizumab pegol” (c) the cardiovascular outcome, identified by the terms “atherosclerosis”, “arteriosclerosis”, “cardiovascular disease”, “cardiovascular risk” and “myocardial infarction”, “cardiovascular death”, “sudden cardiac death”, “heart failure”, “stroke”, “lipids”, “lipid profile”, “cholesterol”, “hypertension”, “arterial stiffness”, “augmentation index”, “endothelial function”, “flow mediated dilatation”, “carotid”, “intima media thickness”. Our search strategy was initially developed for PubMed and modified accordingly for other research engines. In order to look for publications referring to the use of biologics in non-rheumatic conditions, an additional search combining the MeSH terms used for the biologic agent and the cardiovascular outcome in the initial search was also conducted.
The identification of eligible articles was initially carried out by screening titles and abstracts, and finally by reading the full text of the publication. The references of the eligible articles were screened to ensure that no important research data relevant to the subject were missed. Full journal articles, reviews and published abstracts in English from international rheumatology and cardiovascular congresses were included in the search. Not accessible abstracts, data from ongoing pharmaceutical research or reports not translated in English were excluded.14
Pathophysiology – Systemic and Cardiovascular Inflammation
The concept that high-grade inflammation has a central position in the etiopathogenesis of atherosclerosis in ARDs has been primarily based on the observation that various chronic, systemic inflammatory disorders are associated with an excessive risk for cardiovascular events, which cannot be solely explained by the prevalence of traditional cardiovascular risk factors.15,16 For instance, individuals with RA have a 2-fold higher risk for developing CVD than the general population.17 On the other hand, it has been demonstrated that conventional and bDMARDs not only improve markers of systemic inflammation and disease activity parameters,18 but also convey beneficial impact on vascular injury associated with these conditions.18 Figure 1 provides a schematic overview of the complex interrelation between vascular injury and systemic inflammation in ARDs.
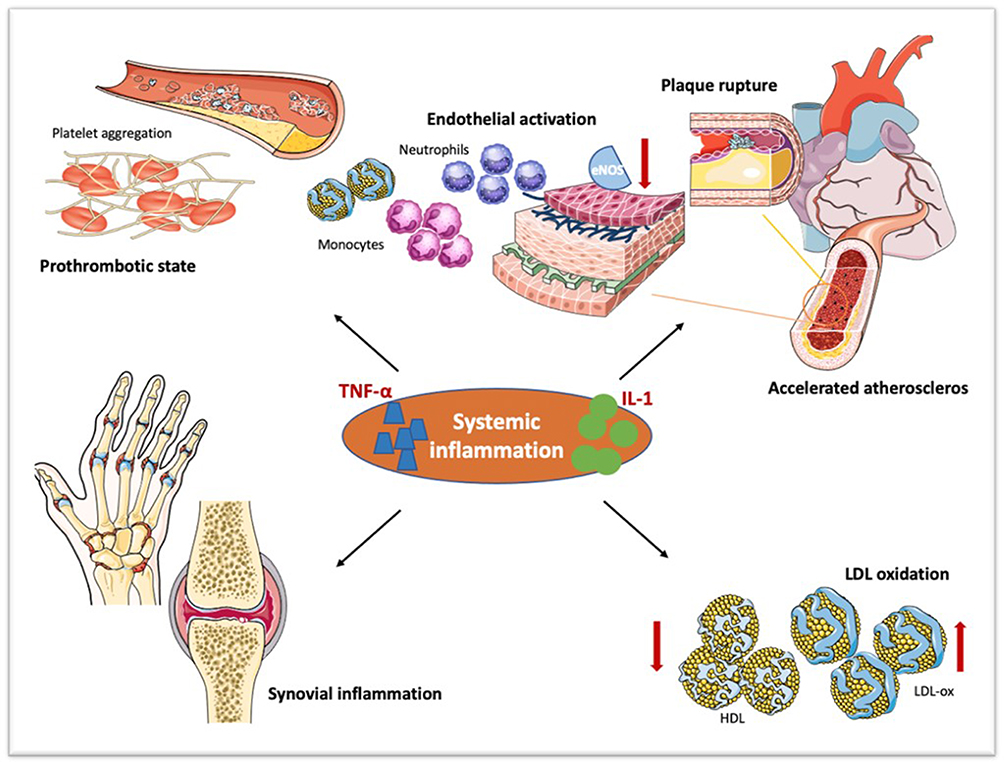 |
Figure 1 Pathogenetic links between systemic and cardiovascular inflammation. Proinflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin-1 (IL-1), upregulated in the setting of systemic inflammation, trigger endothelial activation. The ensuing overexpression of endothelial leukocyte adhesion molecules leads to increased recruitment and activation of inflammatory cells within the arterial wall, resulting in destabilization of endothelial hemostasis, endothelial dysfunction and vascular inflammation. The heightened synthesis of potent procoagulant molecule tissue factors by activated endothelial cells induces platelet adhesion and aggregation, creating a prothrombotic state. Moreover, systemic inflammation associates with an increase in oxidized low-density lipoprotein (LDL-ox) particles along with a reduction in high-density lipoprotein (HDL). These inflammation-driven mechanisms are responsible for the derangement of vascular architecture which represents the earliest step of atherosclerosis, ultimately resulting in vulnerable plaque formation and rupture. |
Endothelial dysfunction is well recognized as one of the earliest steps and major contributors in the development of atherosclerosis.19 It is characterized by the dysregulation of the balance between endothelial-dependent vasoconstriction and vasodilatation, mainly attributed to diminished nitric oxide bioavailability, and the enhanced expression of proinflammatory adhesion molecules, cytokines, chemotactic and prothrombotic factors, all of which participate in the development of atherosclerosis.20 A number of factors may impair endothelial function and act as triggers of endothelial activation. For example, TNF-α, stimulates the expression of endothelial leukocyte adhesion molecules and promotes endothelial cell-leukocyte interaction resulting in increased recruitment and activation of inflammatory cells, within the arterial wall21,22 The ensuing disorganization of the vascular architecture and dysregulation of vascular tone lead to reduced endothelial nitric oxide synthase expression and further derangement of nitric oxide metabolism through various inflammation-driven mechanisms.23,24
The interaction between cytokines and endothelial cells activates the coagulation cascade and promotes intravascular fibrin deposition.25 Systemic inflammation induces the expression of the potent procoagulant molecule, tissue factor, by endothelial cells and platelet adhesion and aggregation,26,27 whereas endogenous fibrinolytic mechanisms are downregulated.28 This thrombotic propensity deteriorates the pro-atherogenic state and accelerates plaque formation. The intrinsic coagulation pathway, which also participates in hemostasis, is mainly mediated by the kallikrein-kinin system, a group of plasma proteins with an integral role in many biological processes, including coagulation and inflammation. Activation of the kallikrein-kinin system has been implicated in cardiovascular disease as a result of bradykinin release, an established proinflammatory mediator as well as the induced changes in the hemostatic system, leading to a hypercoagulable state. Moreover, recent data demonstrate that blockade of the kallikrein-kinin system can reduce complement activation and thereby the inflammatory response on the endothelium, providing additional mechanistic links between inflammation and atherosclerosis.29
Beyond their direct impact on endothelial function, systemic inflammation promotes an atherogenic lipoprotein profile. This is mostly characterized by increased levels of both small, highly atherogenic very low-density lipoprotein (VLDL) and oxidized low-density lipoprotein (LDL) particles, in combination with alterations in high-density lipoprotein (HDL) composition and function.30 A paradoxical suppression of total cholesterol, LDL and HDL levels is observed during the active phases of some chronic inflammatory disorders, such as RA and SLE, presenting an inverse association with the subsequent cardiovascular risk.31,32 This is explained by the disproportionate reduction in levels of HDL compared to LDL cholesterol, giving a more atherogenic total-cholesterol:HDL index.33 On top of lipid abnormalities, systemic inflammation exerts adverse effects on other metabolic pathways such as insulin resistance and body composition and is now considered one of the main pathogenetic mechanisms of the metabolic syndrome.34,35 Thus, it is not surprising that the magnitude of atherosclerosis in RA is comparable to that of diabetes mellitus.36
The CANTOS, CIRT and COLCOT Trials
The understanding of the inflammatory background of atherosclerosis has reasonably given rise to the hypothesis that targeting mediators of the inflammatory process may attenuate the progression of the atherosclerotic plaque and, hence, lead to the reduction of cardiovascular events. Τhe Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) trial was a randomized, double-blind, placebo-controlled trial designed to test the hypothesis that interleukin-1β inhibition with the administration of the human monoclonal antibody canakinumab could prevent recurrent cardiovascular events in patients with a history of myocardial infarction and a persistent pro-inflammatory response, as defined by elevated high-sensitivity C-reactive protein (hsCRP) levels (≥2 mg/L). The trial enrolled over 10,000 patients who were randomly assigned to receive placebo or canakinumab at doses of 50 mg, 150 mg and 300 mg. After a median follow-up period of 3.7 years, it was shown that canakinumab doses of 150 mg and 300 mg significantly reduced the risk for nonfatal myocardial infarction, nonfatal stroke or cardiovascular death by 15% (p = 0.021) and 14% (p = 0.031), respectively, compared to placebo, without any effect on cholesterol levels.37 This favorable effect on cardiovascular events was accompanied by a reduction of about 35–40% in interleukin-6 and hsCRP levels as a consequence of direct interleukin-1β inhibition.
On the other hand, the Cardiovascular Inflammation Reduction Trial (CIRT) found that low-dose methotrexate treatment had no effect on major cardiovascular endpoints in patients with stable coronary artery disease and either type 2 diabetes or metabolic syndrome. The study enrolled 4786 patients who were randomized to receive low-dose methotrexate or placebo, followed for a median period of 2.3 years. The concept was to assess the benefits of a broader spectrum anti-inflammatory approach on cardiovascular outcomes, utilizing the ability of methotrexate to reduce the production of several inflammatory biomarkers, including CRP, interleukin-1, interleukin-6 and TNF-α.38 Nevertheless, no reduction in the levels of the theoretically targeted inflammatory markers was observed in the active medication arm compared to placebo during the study period.
Higher median hsCRP levels in CANTOS at baseline compared to the corresponding values in CIRT which ranged within normal limits (4.2 vs 1.6 mg/L), may account for the contrasting outcomes of these trials, indicating that targeting inflammation may prevent recurrence of cardiovascular events only in those patients with signs of a persistent inflammatory response.39 It may also be assumed that blockade of the central interleukin-1β to interleukin-6 signaling pathway may be more effective than alternative anti-inflammatory approaches, but there is still a long distance to be covered before this theory can be confirmed.
Aiming to further test the inflammatory hypothesis of atherosclerosis, the Colchicine Cardiovascular Outcomes Trial (COLCOT) evaluated the impact of colchicine on cardiovascular outcomes, recruiting approximately 4500 patients with recent myocardial infarction, assigned to receive either colchicine at a daily dose of 0.5 mg or placebo.40 The anti-inflammatory properties of colchicine are attributed to the ability of the drug to inhibit microtubule polymerization, thereby preventing cytokine release and leukocyte migration. More specifically, the suppression of Nod-Like Receptor Protein 3 inflammasome by colchicine seems to be responsible for a down-regulation of interleukin-1β and interleukin-18 production leading to subsequent reductions in interleukin-6 and CRP.41 In COLCOT, treatment with colchicine over a 2-year period led to a 23% reduction in the recurrence of major cardiovascular events, including death from cardiovascular causes, myocardial infarction, stroke and unstable angina resulting in coronary interventions, compared to placebo.40
The Anakinra Trials
Severe reduction in coronary artery blood supply results in acute myocardial ischemia and myocardial necrosis. In the current era, reperfusion strategies aiming to timely restore blood flow within the ischemic region, have revolutionized the treatment of acute myocardial infarction by reducing the loss of vital myocardium, thus resulting in significantly improved outcomes. Despite prompt reperfusion treatments, cardiac injury and myocardial cell death following the ischemic event trigger local and systemic inflammatory responses promoted by intracellular cytokines, such as interleukin-1a. The activation of the inflammatory cascade, despite complete restoration of coronary flow, leads to further loss of cardiomyocytes, impairs myocardial healing and affects myocardial remodeling.42 The intensity of this inflammatory response seems to be associated with worse clinical outcomes, including mechanical complications of myocardial infarction and heart failure.43 Inhibition of the IL-1 pathway for 2 weeks with Anakinra, a recombinant human IL-1 receptor antagonist, in 40 patients with stable STEMI, was found to reduce CRP levels and prevent new-onset heart failure long-term after STEMI but had a neutral effect on recurrent ischemic events compared to placebo in the VCU-ART pilot studies.44,45
The MRC-ILA Heart Study recruited 182 patients with NSTEMI presenting in the first 48 hours after onset of chest pain, randomized to either anakinra treatment or placebo for 2 weeks. Despite a significant suppression in CRP levels in the anakinra arm, the incidence of hard cardiovascular endpoints was similar between the two groups at 30 days and 3 months of follow-up.46
On the other hand, chronic heart failure is considered as a condition of systemic inflammation, characterized by high circulating levels of inflammatory cytokines in response to hypoxia, hemodynamic overload and low-grade cell death.47 IL-1 has been identified as one of the “soluble cardiodepressant factors”, demonstrating negative inotropic effects on the myocardial cells by impairing β-adrenergic receptor signaling downstream in multiple ways.48 The blockade of IL-1 pathways with anakinra has been shown to improve peak oxygen consumption and reduce inflammatory markers in patients with chronic heart failure.49,50 In 60 patients with acute decompensation of heart failure and elevated CRP levels randomized to receive anakinra for 2 weeks, 12 weeks or placebo within 14 days after hospital discharge, an improvement was observed regarding peak oxygen consumption, heart failure biomarkers and quality of life in patients in whom anakinra was continued for 12 weeks.51 In the DHART2 trial, however, among 31 patients with heart failure and preserved ejection fraction randomized to receive either anakinra or placebo, treatment with anakinra for 12 weeks reduced high sensitivity CRP and NT-pro-BNP levels but showed no impact on peak oxygen consumption.52
Recurrent pericarditis is a condition that poses therapeutic challenges because it is corticosteroid dependent and is resistant to treatment with colchicine. The AIRTRIP trial has proposed IL-1 inhibition with anakinra as a promising therapy for recurrent pericarditis, while its efficacy remains to be confirmed in large scale clinical trials.53
Treatment with Biologics and CVD Risk in Inflammatory Arthritides
Although the management of traditional CVD risk factors has constituted for decades the cornerstone of CVD risk prevention strategies, targeting low and/or high grade chronic systemic inflammation emerges as a novel, challenging therapeutic approach for ameliorating the burden of atherosclerotic disease. The rationale for such interventions has been provided by observational and population-based studies in systemic rheumatic diseases, exploring whether antirheumatic treatment has a beneficial impact on vascular injury and CVD outcomes. Particularly for bDMARDs, a number of studies have tried to address this question by examining the effect of treatment on lipid profile, surrogate markers of atherosclerosis and CVD-related outcomes, as summarized in Table 1.
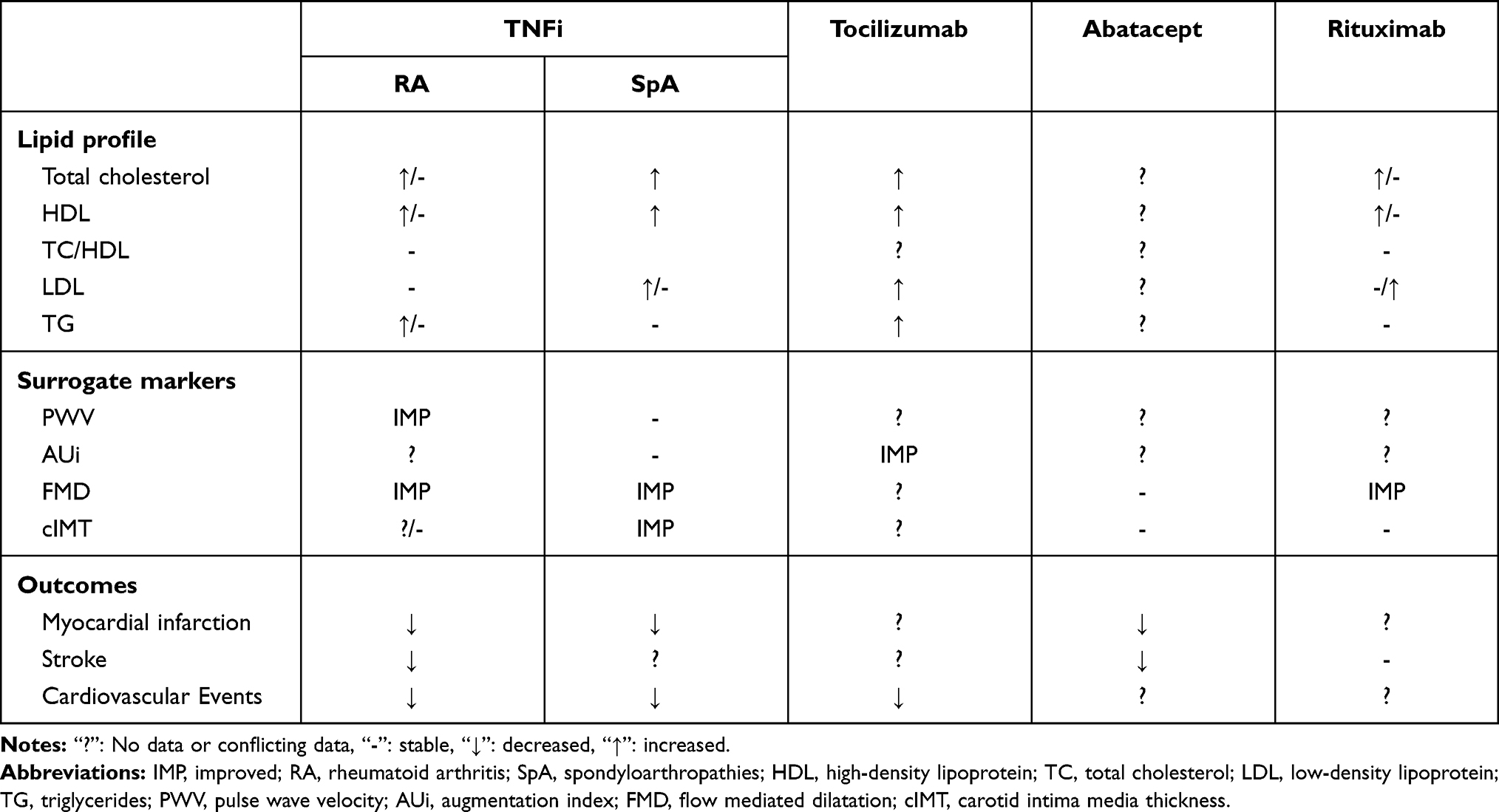 |
Table 1 Summary of the Effects of Biologic DMARDs on Cardiovascular Outcomes and Surrogate Markers |
Findings should generally be interpreted with caution for several reasons: (a) early studies included mixed populations consisting of patients with various types of inflammatory arthritis;54,55 (b) the overwhelming majority of studies with hard end-points are observational, thus causation cannot be ascertained; (c) there are enormous variations in the type, number and disease state of patients included, the main methods used to assess biomarkers and surrogates and even the ascertainment of cardiovascular events. In this review, we focus on studies recruiting individuals with a specific type of arthritis; however it should be acknowledged that studies examining the cardiovascular effect of bDMARDs in patients with SpA are less robust. For studies examining surrogate markers, it is important to bear in mind, at which time points assessments were made. For example, just after administration of a tumor necrosis factor inhibitor (TNFi) or after a specific time interval like 3-, 6-, or 12-months.56,57 Thirdly, disease duration might also play some role in the influence that bDMARDs have on CVD-surrogate markers.58
Rheumatoid Arthritis
Metabolic Factors
Results for TNFi are somehow conflicting for total cholesterol (TC), HDL and triglycerides (TG) which appear to be stabilized or increased upon treatment with these drugs. A meta-analysis has shown that even if TC and HDL are increased, the TC/HDL ratio remains stable.59 In contrast, more consistent results exist for LDL which seems to be unaffected.60 On the other hand, there is a general agreement that IL-6 blockade with tocilizumab results in an increase in most components of the lipid profile.60 Data from systematic reviews and meta-analysis support that such treatment led to increased levels of TC, HDL and LDL.61 However, as shown in a Phase III study evaluating the effect of tocilizumab after 24 weeks of treatment, on CVD risk in RA, despite the increase in TC, LDL and TG, IL-6 inhibition led to an alteration of HDL composition towards an anti-inflammatory phenotype with less serum amyloid-A content.62,63 Data for B-cells depletion treatment, with rituximab are few and sometimes contradictory especially for TC and HDL which appear to be increased or stable,5,64 in contrast to LDL and TG which remain stable.5 Finally, in a study assessing the effect of bDMARDs in various CVD-related biomarkers, it was found that leptin/adipokine ratio was more improved for other biologics (including rituximab, tocilizumab and CTLA-4 inhibitor abatacept) compared to TNFi. In the same study, after 24 weeks, Lipoprotein-a was also more improved when tocilizumab was compared with TNFi.65
A number of observations and systematic reviews suggest that treatment with TNFi improves insulin resistance in RA patients.66,67 However, it remains unknown whether the TNFi exert their beneficial effects directly by normalizing beta cell function and insulin signaling or through other mechanisms independent of TNF-α or systemic inflammation.68 In this respect a longitudinal study indicated that IL-1 inhibition with anakinra resulted in more effective control of patients with type-2 diabetes mellitus compared to TNF-α after six months of treatment.69 The better outcomes were linked with a favorable shift of the adipokine profile in the anakinra group suggesting a crucial role of IL-1β in metabolic dysregulation in diabetic RA patients. More importantly such observations provide evidence for a tailored approach in RA subjects with specific metabolic characteristics.
Surrogate Markers
Although there are some disagreements, it seems that treatment with TNFi in RA leads to favorable outcomes in arterial stiffness as assessed by pulse-wave velocity (PWV) but not with the augmentation index (AUi), which remained unchanged in most of the studies for RA patients treated with TNFi.70–74 Increased CVD risk and a window for improving aortic stiffness, seems to be present also in early RA. In a study enrolling patients with early RA, treatment with TNFi etanercept or with etanercept plus methotrexate, led to improvement in aortic distensibility after one year. Of note, no difference was noticed between treatment arms.75 Endothelial function seems also to be improved76–78 as a recent meta-analysis has shown.79 It has to be stressed however that the different methods used for its measurement might limit the generalizability of these results.79 On the other hand, things are less clear for cIMT76,78 An RCT comparing methotrexate alone versus combination treatment with TNFi infliximab plus methotrexate, showed that there was no difference in cIMT between the two groups.80 Data from other studies, however, support that cIMT regressed or at least remained stable upon treatment with TNFi.74
Not many data are available for the other bDMARDs. In an open-label RCT, after 24 weeks, tocilizumab had the same effect with etanercept or adalimumab in arterial stiffness, as assessed by cardio-ankle vascular index and aortic augmentation index.81 As for rituximab, in a small study, 6 patients resistant to TNFi treatment, received rituximab and displayed significant improvement of flow-mediated dilation (FMD), as early as week 2, being also maintained up to week 6.82 Finally, another study evaluating 38 RA patients showed that FMD was improved at week 24 after rituximab infusion.83 On the other hand, no major effects were seen for cIMT, although longer follow-up period might be needed to assess the atheroprotective effect, if any.64,83 For Abatacept, data are too few to draw a definite conclusion.84 In a study with 45 RA patients, it has been shown that after 12 months of treatment cIMT and FMD remained stable.85
Outcomes
Several lines of evidence support the hypothesis that TNFi are indeed associated with lower risk for CVD events. Data from the British Society of Rheumatology Biologics Registry for RA patients treated with TNFi or bDMARDs-naïve patients receiving conventional DMARDs were recorded for the 2001–2009 time period and linked with the national registry for myocardial infarctions (MI). It was shown that the former (median follow-up per person: 5.3 years) compared to the latter (median follow-up per person: 3.5 years) had less risk for MI.86 In a similar setting, no association was found between exposure to TNFi in RA patients and ischemic stroke.87 Data from about 4000 patients included in the QUEST-RA study – an international multicentre cross‐sectional study selecting data from RA persons in three or more rheumatology clinics in several countries – showed that prolonged exposure to TNFi was combined with lower risk for all CVD events including MI and stroke.88 Finally, in a large prospective study examining data from about 20,000 patients-years, derived from the database of the Australian rheumatology association, it was found that treatment with TNFi or other biologics in patients with inflammatory arthritis (including those with psoriatic arthritis or ankylosing spondylitis) was associated with less CVD events.89 In concert with these studies, a meta-analysis, published in 2011 showed that RA patients treated with TNFi compared to those receiving conventional DMARDs, had lower risk for MI and strokes in data derived from observational cohorts but not from RCTs.78,90 Finally, in the largest meta-analysis so far, Roubille et al found that TNFi treatment lead to reduction in the risk for MI and strokes but not heart failure in RA patients.91
Despite the unfavorable alterations observed in the lipid profile, tocilizumab does not exhibit higher risk for CVD compared to other biologics.92,93 Besides, a study examining single nucleotide polymorphisms (SNP) in the IL-6 receptor gene, found that a specific SNP was associated with altered odds of coronary heart disease in RA patients.94 In a recent RCT enrolling about 3000 patients and comparing tocilizumab vs etanercept, major adverse cardiovascular events were comparable between the two groups, after a mean follow-up of 3.2 years.95 In fact, the most recent meta-analysis has shown IL-6 inhibition with tocilizumab had a lower risk for major adverse cardiovascular events compared to TNFi but not with abatacept.96 With regards to rituximab, data are less robust. The results from the global clinical trial programme (n = 3595 patients, followed up for about 11 years), showed that rates for MI and CVD events were comparable to the general population.97 Of note, a handful of reports raise the possibility of acute MI after rituximab infusion in RA and lymphoma patients98,99 Finally, for abatacept, in a study using data from Marketscan and Medicare, having as a composite primary endpoint the occurrence of MI, transient ischemic attack and coronary revascularization, it was found that during the 31,733 years of follow-up, this regime was better than TNFi in RA patients with diabetes mellitus.100 In a study of a similar setting, RA patients treated with abatacept had 20% lower risk for CVD compared to those who received TNFi, regardless of their baseline CVD status.101 Of note, similar results were reported for older (>65 years-old) patients treated with abatacept. These, analyzing data from 47,193 patients, displayed lower risk for MI, than individuals with RA who received TNFi.102
Conclusion
Overall, one could say that the lipid alterations observed are of limited significance and do not seem to affect cardiovascular outcomes. Surrogate markers, like FMD are found to be improved or at least remain stable, upon treatment with bDMARDs, while hard outcomes like myocardial infarction and stroke are reduced. Results seems to be comparable across different bDMARDs classes, but data are more robust for TNFi.
Spondyloarthropathies
Evidence about the association between treatment with biologic drugs and cardiovascular effect, is much less for SpA than for RA. It seems, however, that changes in the lipid profile are similar in both groups of patients.5 Complexity in the interpretation of the results derives also from the different diseases, like ankylosing spondylitis (AS) and psoriatic arthritis (PsA) classified under the umbrella of SpA. In fact, although they have many similarities, especially in terms of clinical manifestations and treatment options, it seems that regarding the underlying pathogenic mechanisms and comorbidities, there are some important differences between these conditions such as distribution of joint involvement – predominantly spinal in AS and peripheral in PsA- unfavorable metabolic profile in PsA, skin disease in PsA and others. Additionally, data are missing for drugs that recently have been added in the rheumatologists’ armamentarium, like anti-IL-17 and anti-IL-23 regimes.
Metabolic Factors
In AS patients, treatment with etanercept led to increase in HDL and TC over the first 3 months. Noteworthy, TC/HDL ratio was better, as were the qualitative changes in HDL. In fact, serum-amyloid A (SAA) disappeared, leading thus to a more atheroprotective HDL.103 In another study examining the effect of anti-TNF treatment in the lipid profile of AS patients, it was found that after 14 weeks of treatment, TC and HDL were increased while TC/HDL ratio, TG and LDL remained unchanged.104 Interestingly, a large study with more than 200 patients with axial SpA (axSpA – the major representative of which is AS) showed that compared to non-TNFi users, patients who were treated with TNFi had no changes in their lipid profile. When comparisons were made in the latter group between baseline and 2-years follow-up, only a statistically significant increase was seen in TC.105 For PsA, Agca et al in 2017 showed that 5-years treatment with etanercept led to increased TC, HDL and LDL, leaving TC/HDL unchanged, however.106
Surrogate Markers
In general and partially in contrast to what is observed for RA, arterial stiffness appears to remain unchanged for most of the studies regarding AS patients.74,107 A small study examining 28 AS patients did not find changes in arterial stiffness as assessed by PWV after 6 months of treatment with TNFi.108 In concert, similar results were presented by other investigators who reported no significant changes in AuI and PWV in AS patients treated with TNFi for 6–12 months.109,110
Treatment with TNFi seems to also have a beneficial effect to endothelial dysfunction in SpA. Syngle et al showed that in 12 AS patients treated with infliximab, FMD was improved after 12 weeks.111 Interestingly, it has also been shown that just after infliximab infusion, adhesion molecules used as surrogate markers for endothelial activation like sE-selectin, are significantly reduced in AS non-diabetic patients.112 Treatment with TNFi has also beneficial effects in microvascular function, since endothelium-dependent vasodilation and capillary recruitment was found to be improved in a small cohort of AS patients treated with etanercept for 1 month.113
Atherosclerotic lesions seem to be significantly improved in SpA patients treated with TNFi. In a study enrolling 81 AS patients, 67 of which were treated with TNFi, it was shown that after a mean follow-up of approximately 5 years, cIMT was stable for patients who continued treatment with TNFi but progressed in those who did not.114 Along the same lines, AS patients treated with TNFi for 2 years exhibited lower values of cIMT and number of atherosclerotic plaques compared to healthy individuals.115 Finally, in a randomized placebo controlled study, although treatment with TNFi golimumab left IMT unchanged, patients being in the placebo arm showed significant progression of IMT at 6 months.109
For PsA, in a small study, enrolling 20 PsA patients treated with TNFi, cIMT was significantly decreased at 3 months. After a mean follow-up of 2 years, the significant improvement of cIMT continued only for patients who had continued treatment with TNFi.80 Similarly, Di Minno et al, in a larger study, found that PsA patients treated with TNFi (mean±SD treatment duration: 52.33±24.11 months) had lower number of plaques and lower cIMT compared to those treated with conventional DMARDs (mean±SD treatment duration: 58.22±29.21 months).116 Noteworthy, treatment duration with TNFi was inversely correlated with cIMT, implying that effect of treatment on atherosclerotic lesions, at least in these patients is cumulative. It is possible that these effects are more pronounced in specific subgroups of patients. In a recent study, including about 300 patients (mean ± SD follow up: 2.9 ± 0.7 years) with psoriasis and PsA, it was found that treatment with TNFi reduced the atherosclerotic progression in males but not in females.117 Importantly, measuring vascular inflammation with positron emission tomography (PET), in a subgroup of this cohort, patients treated with TNFi but not those not receiving biologics, had significantly lower target-to-blood pool ratio (TBR) after 1 year.117
Outcomes
Despite psoriasis and PsA having been recognized to be closely linked with CVD risk, not many studies have assessed the effect of immunosuppressives on that. In a relatively recent meta-analysis about the effect of TNFi on CVD risk in patients with inflammatory arthritis, only 6 studies for psoriasis/PsA were included.91 The investigators were able to show that treatment with these regimes was associated with a reduced risk for all CVD, compared to topical therapy. Similarly, in another meta-analysis, it was shown that, compared to Pso/PsA patients receiving topical treatment or methotrexate, those treated with TNFi, had lower risk for CVD or MI.118 Comparing different biologics, a large study (78,162 patients) using data from US commercial databases for patients with psoriasis or PsA, found that the risk for atrial fibrillation or major adverse CVD events did not differ between patients treated with the IL-23 inhibitor ustekinumab or TNFi.119 Data for newer treatment modalities for PsA and AS, like drugs targeting IL-17, are lacking.
Conclusion
Data are less solid for SpA compared to RA. This is more pronounced for newer therapeutic regimes like anti-IL-17 and anti-IL-23 regimes. In general, despite increase in TC and HDL, TC/HDL ratio remains unchanged. Additionally, treatment with TNF inhibitors seems to improve endothelial dysfunction and atherosclerosis, while limited data support the favorable effect of these drugs in hard CVD outcomes.
The Effect of Anti-Inflammatory Drugs on Myocardial Inflammation and Function
Inflammatory myocardial disease characterized by immune cell infiltration, degeneration and necrosis of cardiomyocytes is common in systemic autoimmune disorders. From a pathophysiological standpoint, such changes culminate in myocardial oedema – the main feature of acute cardiac tissue injury due to autoimmune activation and/or microvascular ischemia – which, if untreated, leads to cardiac tissue fibrosis and subsequently to myocardial dysfunction. Cardiac magnetic resonance (CMR) allows the non-invasive visualization and detailed characterization of the various types of myocardial injury, namely oedema, fibrosis, perfusion defects, coronary vessels inflammatory and structural abnormalities,120 all of which occur in patients with systemic diseases and are tightly linked with heightened risk of CV events in this population.121
CMR based studies have demonstrated a substantial degree of myocardial inflammation in systemic autoimmune diseases such as systemic lupus erythematosus, inflammatory myopathies, scleroderma and systemic vasculitis even in individuals without clinical symptoms and normal evaluation of heart function with echocardiography, electrocardiogram and cardiac biomarkers such as troponin.122–125 For example a retrospective study including 78 newly diagnosed, treatment naïve persons with various systemic autoimmune disorders revealed clinically silent myocardial oedema and fibrosis in the majority of patients.126 Interestingly enough, these abnormalities resolved in follow-up scans after 1 year of treatment for the underlying disease as per physicians’ choice.
Despite the lack of large prospective studies, there are a few reports indicating that anti-inflammatory regimens have a direct beneficial effect on myocardial oedema assessed by CMR before and after therapeutic intervention. Aggressive treatment with intravenous methylprednisolone followed by immunosuppressives such as cyclophosphamide, azathioprine reduced myocardial contrast enhancement on CMR in patients with autoimmune myositis and such findings were in accordance with clinical improvement.110 Similarly, the prompt initiation of steroids and disease modifying drugs improved cardiovascular outcomes in patients with ANCA-positive vasculitis-related cardiomyopathy, suggesting that antirheumatic drugs of various classes hold a crucial role in ameliorating myocardial inflammation across the whole spectrum of systemic inflammatory diseases.127,128 With regards to bDMARDs a small case-series reported considerable improvement in SLE patients with myocarditis treated with rituximab.129
A number of recent CMR-based studies have provided further insights in the relationship between systemic and myocardial inflammation by indicating significant improvement of heart function after treatment with bDMARDs.130 Ntusi et al showed that treatment with TNFi resulted in considerable attenuation of subclinical myocardial oedema in 32 patients with inflammatory arthritides after 3–6 months of treatment.131 Reduction of myocardial inflammation was accompanied by improvement in myocardial function and overall disease activity. In line with these observations, IL-6 inhibition with tocilizumab not only improved left ventricular injection fraction but also normalized structural abnormalities such as left ventricular hypertrophy assessed by mass index, confirming the findings of previous echocardiography studies.132–134 Taken all together these findings suggest a mechanistic role of TNF-α and IL-6 inhibition in modulating myocardial impairment and improving indices of cardiac function in inflammatory diseases. It has been suggested that chronic exposure of the myocardium to pro-inflammatory cytokines mediates – amongst others – adverse ventricular remodeling leading to diastolic dysfunction and heart failure with preserved ejection fraction, one of the leading causes of death in systemic diseases.135–137 Biologic DMARDs may have pleiotropic effects and express their action through suppression of systemic inflammation but also by specific antibody mediated cellular effect on the myocardium. Although some reports suggested an increased frequency of developing heart failure following treatment with bDMARDs,138,139 a systematic review concluded that bDMARDs probably do not increase this risk but in contrast, may have a beneficial effect on morphological and functional parameters of the myocardium highlighting the need for better quality studies.140 To lend more support to the former, treatment with TNFi seems to reduce the levels of N-Terminal probrain natriuretic peptide – a well-established biomarker of cardiac performance – in patients with RA.141 However, and until future large controlled studies address this question, bDMARDs are generally not recommended in patients with functional class III–IV heart-failure.
Such observations provide the rationale for large longitudinal studies investigating the results of immunosuppressive treatment on myocardial inflammation and function determined by CMR in systemic rheumatologic diseases in earlier or later stages of the disease.142
Insights of Biologics on CVD Risk and Future Perspectives
Although robust evidence is currently lacking, it appears that treatment with bDMARDs has a positive impact on CVD risk by favorably modifying several aspects of CVD in patients with systemic inflammatory disorders. However, differences in CVD targets should be taken into account when evaluating such data as it is not evident which particular effect and which class of antirheumatic drugs may be responsible for the overall beneficial effect on CVD risk. Apparently, the suppression of systemic inflammation represents the basic mechanism as elevated C-reactive protein has been linked with increased CVD mortality and morbidity in RA patients.143 The increase of lipid levels in these patients – following treatment mainly with TNFi and IL-6 inhibitors – reflects rather the restoration of lipid metabolism to the level prior the onset of inflammatory disease rather than an atherogenetic process. Furthermore, bDMARDs render atheroprotective effects by improving endothelial function, normalizing coagulation status and alleviating insulin resistance. RA individuals with a higher degree of response to TNFi inhibitors, appear to have a lower incidence of CVD events compared to those with suboptimal control of disease activity supporting the link between inflammation and atherosclerosis.144,145 To lend more support, the results of a secondary analysis of the CANTOS trial suggest that patients achieving the largest reduction in high sensitivity C-reactive protein with canakinumab treatment, had better CVD outcomes.146 On the other hand, the influence of concomitant methotrexate administration with bDMARDs on CVD reduction in patients with inflammatory arthritides has not been investigated complicating the interpretation of the data. Given that patients with longstanding, active disease are more likely to be treated with bDMARDs, only a few studies are adjusted for confounding by indication which is a crucial concern for drawing any definite conclusions regarding the precise impact of these regimens on CVD risk.147
Besides inflammatory burden reduction, drug-specific mechanisms may be responsible for the improved outcome. The CANTOS trial provides evidence that IL-1 inhibition may reduce CVD events suggesting a mechanistic relationship between targeting of the IL-1, IL-6 pathway of innate immunity and treatment of atherosclerosis.148 In this regard, IL-6 blockade may also represent a novel target of vascular therapy as the beneficial effects of canakinumab in CANTOS trial are directly linked with the magnitude of IL-6 inhibition.149 The role of other alternative inflammatory pathways has not been investigated yet. For example NLRP3 inflammasome inhibition reduces atherosclerotic lesions and improves myocardial ischemia in experimental models,150,151 whereas the potential athLRP3-inhibiting properties of colchicine may also be associated with atheroprotective action.152
Taken all together future research agenda in this field may include a shift from traditional atherosclerotic macrovascular disease to other mechanisms which may contribute to increased CVD risk such as silent microvascular myocardial injury in parallel with a personalized medicine based on individual characteristics as well as CVD and disease-related risk profile of the patients. In that respect, the identification of biomarkers and clinical predictors in patients with inflammatory conditions might lead to strategies that support individual patients for specific therapies which in turn may target CVD inflammation more effectively.
Conclusions
The introduction of bDMARDs in the treatment armamentarium has revolutionized the overall management of systemic inflammatory diseases culminating in better long term outcomes and improvement in survival of patients suffering from these conditions.153,154 Modern treatment strategies targeting effective control of inflammation seem to have a positive impact on CVD mortality but it still remains unknown whether such observations reflect a direct effect on vascular pathology or are the results of the suppression of systemic inflammation. Lessons taken from inflammatory arthropathies might have implications in the management of atherosclerosis in the general population as indicated by CANTOS trial. The research in this field is in its infancy and future large studies could determine whether bDMARDs could provide further benefit in the prevention and treatment of atherosclerosis beyond established measures such as management of classical CVD factors and lifestyle changes.
Author Contributions
George Fragoulis and Stergios Soulaidopoulos share first authorship. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. All the contributing authors have read and approved the final edition of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Geovanini GR, Libby P. Atherosclerosis and inflammation: overview and updates. Clin Sci. 2018;132(12):1243–1252. doi:10.1042/CS20180306
2. Tedgui A, Mallat Z. Cytokines in atherosclerosis: pathogenic and regulatory pathways. Physiol Rev. 2006;86(2):515–581. doi:10.1152/physrev.00024.2005
3. Arida A, Protogerou AD, Kitas GD, Sfikakis PP. Systemic inflammatory response and atherosclerosis: the paradigm of chronic inflammatory rheumatic diseases. Int J Mol Sci. 2018;19(7):1–27. doi:10.3390/ijms19071890
4. Gasparyan AY. Cardiovascular risk and inflammation in rheumatic diseases. Rheumatol Int. 2017;37(1):1–2. doi:10.1007/s00296-016-3619-8
5. Nurmohamed M, Choy E, Lula S, Kola B, DeMasi R, Accossato P. The impact of biologics and tofacitinib on cardiovascular risk factors and outcomes in patients with rheumatic disease: a systematic literature review. Drug Saf. 2018;41(5):473–488. doi:10.1007/s40264-017-0628-9
6. Zegkos T, Kitas G, Dimitroulas T. Cardiovascular risk in rheumatoid arthritis: assessment, management and next steps. Ther Adv Musculoskelet Dis. 2016;8(3):86–101. doi:10.1177/1759720X16643340
7. Agca R, Heslinga SC, Rollefstad S, et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis. 2017;76(1):17–28. doi:10.1136/annrheumdis-2016-209775
8. Arida A, Protogerou AD, Konstantonis G, Fragiadaki K, Kitas GD, Sfikakis PP. Atherosclerosis is not accelerated in rheumatoid arthritis of low activity or remission, regardless of antirheumatic treatment modalities. Rheumatology. 2017;56:934–939. doi:10.1093/rheumatology/kew506
9. Jamthikar AD, Gupta D, Puvvula A, et al. Cardiovascular risk assessment in patients with rheumatoid arthritis using carotid ultrasound B-mode imaging. Rheumatol Int. 2020;40(12):1921–1939. doi:10.1007/s00296-020-04691-5
10. Tousoulis D, Oikonomou E, Economou EK, Crea F, Kaski JC. Inflammatory cytokines in atherosclerosis: current therapeutic approaches. Eur Heart J. 2016;37(22):1723–1732. doi:10.1093/eurheartj/ehv759
11. Drakopoulou M, Soulaidopoulos S, Oikonomou G, Tousoulis D, Toutouzas K. Cardiovascular effects of biologic disease-modifying anti-rheumatic drugs (DMARDs). Curr Vasc Pharmacol. 2020;18(5):488–506. doi:10.2174/1570161118666200214115532
12. Ridker PM, MacFadyen JG, Thuren T, Libby P. Residual inflammatory risk associated with interleukin-18 and interleukin-6 after successful interleukin-1beta inhibition with canakinumab: further rationale for the development of targeted anti-cytokine therapies for the treatment of atherothrombosis. Eur Heart J. 2020;41(23):2153–2163. doi:10.1093/eurheartj/ehz542
13. Protogerou AD, Zampeli E, Fragiadaki K, Stamatelopoulos K, Papamichael C, Sfikakis PP. A pilot study of endothelial dysfunction and aortic stiffness after interleukin-6 receptor inhibition in rheumatoid arthritis. Atherosclerosis. 2011;219(2):734–736. doi:10.1016/j.atherosclerosis.2011.09.015
14. Gasparyan AY, Ayvazyan L, Blackmore H, Kitas GD. Writing a narrative biomedical review: considerations for authors, peer reviewers, and editors. Rheumatol Int. 2011;31(11):1409–1417. doi:10.1007/s00296-011-1999-3
15. Nurmohamed MT, Heslinga M, Kitas GD. Cardiovascular comorbidity in rheumatic diseases. Nat Rev Rheumatol. 2015;11(12):693–704. doi:10.1038/nrrheum.2015.112
16. Kitas GD, Gabriel SE. Cardiovascular disease in rheumatoid arthritis: state of the art and future perspectives. Ann Rheum Dis. 2011;70(1):8–14. doi:10.1136/ard.2010.142133
17. Hansildaar R, Vedder D, Baniaamam M, Tausche AK, Gerritsen M, Nurmohamed MT. Cardiovascular risk in inflammatory arthritis: rheumatoid arthritis and gout. Lancet Rheumatol. 2020;3(1):e58–e70. doi:10.1016/S2665-9913(20)30221-6
18. Kisiel B, Kruszewski R, Juszkiewicz A, et al. Methotrexate, cyclosporine A, and biologics protect against atherosclerosis in rheumatoid arthritis. J Immunol Res. 2015;2015:1–8. doi:10.1155/2015/759610
19. Steyers CM, Miller FJ. Endothelial dysfunction in chronic inflammatory diseases. Int J Mol Sci. 2014;15(7):11324–11349. doi:10.3390/ijms150711324
20. Sitia S, Tomasoni L, Atzeni F, et al. From endothelial dysfunction to atherosclerosis. Autoimmun Rev. 2010;9(12):830–834. doi:10.1016/j.autrev.2010.07.016
21. Page MJ, Bester J, Pretorius E. The inflammatory effects of TNF-α and complement component 3 on coagulation. Sci Rep. 2018;8(1):1–9. doi:10.1038/s41598-018-20220-8
22. Bamias G, Stamatelopoulos K, Zampeli E, et al. Circulating levels of TNF-like cytokine 1A correlate with the progression of atheromatous lesions in patients with rheumatoid arthritis. Clin Immunol. 2013;147(2):144–150. doi:10.1016/j.clim.2013.03.002
23. Dimitroulas T, Hodson J, Sandoo A, Smith J, Kitas GD. Endothelial injury in rheumatoid arthritis: a crosstalk between dimethylarginines and systemic inflammation. Arthritis Res Ther. 2017;19(1):32. doi:10.1186/s13075-017-1232-1
24. Dimitroulas T, Sandoo A, Douglas K, Kitas G. Symmetric and asymmetric dimethylarginines as biochemical markers of endothelial dysfunction and atherosclerosis in Rheumatoid Arthritis. Mediterr J Rheumatol. 2015;26(2):62–75.
25. Dimitroulas T, Douglas KM, Panoulas VF, et al. Derangement of hemostasis in rheumatoid arthritis: association with demographic, inflammatory and metabolic factors. Clin Rheumatol. 2013;32(9):1357–1364. doi:10.1007/s10067-013-2283-6
26. Gasparyan AY, Stavropoulos-Kalinoglou A, Mikhailidis DP, Douglas KM, Kitas GD. Platelet function in rheumatoid arthritis: arthritic and cardiovascular implications. Rheumatol Int. 2011;31(2):153–164. doi:10.1007/s00296-010-1446-x
27. Al-Rawi ZS, Gorial FI, Al-Bayati AA. Red cell distribution width in rheumatoid arthritis. Mediterr J Rheumatol. 2018;29(1):38–42. doi:10.31138/mjr.29.1.38
28. Bisoendial RJ, Levi M, Tak PP, Stroes ES. The prothrombotic state in rheumatoid arthritis: an additive risk factor for adverse cardiovascular events. Semin Thromb Hemost. 2010;36(4):452–457. doi:10.1055/s-0030-1254054
29. Lopatko I, Ståhl A, Mossberg M, et al. Blockade of the kallikrein-kinin system reduces endothelial complement activation in vascular inflammation. EBioMedicine. 2019;47:319–328.
30. van Diepen JA, Berbée JFP, Havekes LM, Rensen PCN. Interactions between inflammation and lipid metabolism: relevance for efficacy of anti-inflammatory drugs in the treatment of atherosclerosis. Atherosclerosis. 2013;228(2):306–315. doi:10.1016/j.atherosclerosis.2013.02.028
31. E. Toms T, P. Symmons D, D. Kitas G. Dyslipidaemia in rheumatoid arthritis: the role of inflammation, drugs, lifestyle and genetic factors. Curr Vasc Pharmacol. 2010;8(3):301–326. doi:10.2174/157016110791112269
32. Myasoedova E, Crowson CS, Kremers HM, et al. Lipid paradox in rheumatoid arthritis: the impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann Rheum Dis. 2011;70(3):482–487. doi:10.1136/ard.2010.135871
33. Georgiadis AN, Papavasiliou EC, Lourida ES, et al. Atherogenic lipid profile is a feature characteristic of patients with early rheumatoid arthritis: effect of early treatment–a prospective, controlled study. Arthritis Res Ther. 2006;8(3):R82. doi:10.1186/ar1952
34. Sattar N, Kitas GD. Rheumatoid arthritis: testing the inflammation-insulin resistance link in clinical trials. Nat Rev Rheumatol. 2013;9(12):702–703. doi:10.1038/nrrheum.2013.178
35. Stavropoulos-Kalinoglou A, Metsios GS, Koutedakis Y, Kitas GD. Body-size phenotypes and cardiometabolic risk in Rheumatoid Arthritis (Short Title: subgroups of obesity in RA). Mediterr J Rheumatol. 2016;27(2):48–54. doi:10.31138/mjr.27.2.48
36. Stamatelopoulos KS, Kitas GD, Papamichael CM, et al. Atherosclerosis in rheumatoid arthritis versus diabetes: a comparative study. Arter Thromb Vasc Biol. 2009;29(10):1702–1708. doi:10.1161/ATVBAHA.109.190108
37. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
38. Halilova KI, Brown EE, Morgan SL, et al. Markers of treatment response to methotrexate in rheumatoid arthritis: where do we stand? Int J Rheumatol. 2012;2012:1–7. doi:10.1155/2012/978396
39. Ridker PM. Anti-inflammatory therapy for atherosclerosis: interpreting divergent results from the CANTOS and CIRT clinical trials. J Intern Med. 2019;285(5):503–509. doi:10.1111/joim.12862
40. Tardif J-C, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
41. Slobodnick A, Shah B, Krasnokutsky S, Pillinger MH. Update on colchicine, 2017. Rheumatology. 2018;57(1):i4–i11. doi:10.1093/rheumatology/kex453
42. Abbate A, Toldo S, Marchetti C, Kron J, Van Tassell BW, Dinarello CA. Interleukin-1 and the inflammasome as therapeutic targets in cardiovascular disease. Circ Res. 2020;126:1260–1280. doi:10.1161/CIRCRESAHA.120.315937
43. Seropian IM, Toldo S, Van Tassell BW, Abbate A. Anti-inflammatory strategies for ventricular remodeling following St-segment elevation acute myocardial infarction. J Am Coll Cardiol. 2014;63(16):1593–1603. doi:10.1016/j.jacc.2014.01.014
44. Abbate A, Van Tassell BW, Biondi-Zoccai G, et al. Effects of interleukin-1 blockade with anakinra on adverse cardiac remodeling and heart failure after acute myocardial infarction [from the virginia commonwealth university-anakinra remodeling trial (2) (vcu-art2) pilot study]. Am J Cardiol. 2013;111(10):1394–1400. doi:10.1016/j.amjcard.2013.01.287
45. Abbate A, Kontos MC, Abouzaki NA, et al. Comparative safety of interleukin-1 blockade with anakinra in patients with ST-segment elevation acute myocardial infarction (from the VCU-ART and VCU-ART2 pilot studies). Am J Cardiol. 2015;115(3):288–292. doi:10.1016/j.amjcard.2014.11.003
46. Morton AC, Rothman AMK, Greenwood JP, et al. The effect of interleukin-1 receptor antagonist therapy on markers of inflammation in non-ST elevation acute coronary syndromes: the MRC-ILA Heart Study. Eur Heart J. 2015;36(6):377–384. doi:10.1093/eurheartj/ehu272
47. Yndestad A, Damås JK, Øie E, Ueland T, Gullestad L, Aukrust P. Systemic inflammation in heart failure - The whys and wherefores. Heart Fail Rev. 2006;11(1):83–92. doi:10.1007/s10741-006-9196-2
48. Van Tassell BW, Toldo S, Mezzaroma E, Abbate A. Targeting interleukin-1 in heart disease. Circulation. 2013;128(17):1910–1923. doi:10.1161/CIRCULATIONAHA.113.003199
49. van Tassell BW, Arena RA, Toldo S, et al. Enhanced interleukin-1 activity contributes to exercise intolerance in patients with systolic heart failure. PLoS One. 2012;7(3):e33438. doi:10.1371/journal.pone.0033438
50. Van Tassell BW, Abouzaki NA, Erdle CO, et al. Interleukin-1 blockade in acute decompensated heart failure: a randomized, double-blinded, placebo-controlled pilot study. J Cardiovasc Pharmacol. 2016;67(6):544–551. doi:10.1097/FJC.0000000000000378
51. Van Tassell BW, Canada J, Carbone S, et al. Interleukin-1 blockade in recently decompensated systolic heart failure: results from REDHART (Recently Decompensated Heart Failure Anakinra Response Trial). Circ Heart Fail. 2017;10(11).
52. Van Tassell BW, Trankle CR, Canada JM, et al. IL-1 blockade in patients with heart failure with preserved ejection fraction. Circ Heart Fail. 2018;11(8):e005036. doi:10.1161/CIRCHEARTFAILURE.118.005036
53. Brucato A, Imazio M, Gattorno M, et al. Effect of anakinra on recurrent pericarditis among patients with colchicine resistance and corticosteroid dependence: the AIRTRIP randomized clinical trial. JAMA. 2016;316(18):1906–1912. doi:10.1001/jama.2016.15826
54. Spanakis E, Sidiropoulos P, Papadakis J, et al. Modest but sustained increase of serum high density lipoprotein cholesterol levels in patients with inflammatory arthritides treated with infliximab. J Rheumatol. 2006;33(12):2440–2446.
55. Kiortsis DN, Mavridis AK, Filippatos TD, Vasakos S, Nikas SN, Drosos AA. Effects of infliximab treatment on lipoprotein profile in patients with rheumatoid arthritis and ankylosing spondylitis. J Rheumatol. 2006;33(5):921–923.
56. Mazzoccoli G, Notarsanto I, de Pinto GD, et al. Anti-tumor necrosis factor-alpha therapy and changes of flow-mediated vasodilatation in psoriatic and rheumatoid arthritis patients. Intern Emerg Med. 2010;5(6):495–500. doi:10.1007/s11739-010-0458-6
57. Angel K, Provan SA, Fagerhol MK, Mowinckel P, Kvien TK, Atar D. Effect of 1-year anti-TNF-alpha therapy on aortic stiffness, carotid atherosclerosis, and calprotectin in inflammatory arthropathies: a controlled study. Am J Hypertens. 2012;25(6):644–650. doi:10.1038/ajh.2012.12
58. Angel K, Provan SA, Hammer HB, Mowinckel P, Kvien TK, Atar D. Changes in arterial stiffness during continued infliximab treatment in patients with inflammatory arthropathies. Fundam Clin Pharmacol. 2011;25(4):511–517. doi:10.1111/j.1472-8206.2010.00872.x
59. van Sijl AM, Peters MJ, Knol DL, et al. The effect of TNF-alpha blocking therapy on lipid levels in rheumatoid arthritis: a meta-analysis. Semin Arthritis Rheum. 2011;41(3):393–400. doi:10.1016/j.semarthrit.2011.04.003
60. Fragoulis GE, Panayotidis I, Nikiphorou E. Cardiovascular risk in rheumatoid arthritis and mechanistic links: from pathophysiology to treatment. Curr Vasc Pharmacol. 2020;18(5):431–446.
61. Souto A, Salgado E, Maneiro JR, Mera A, Carmona L, Gomez-Reino JJ. Lipid profile changes in patients with chronic inflammatory arthritis treated with biologic agents and tofacitinib in randomized clinical trials: a systematic review and meta-analysis. Arthritis Rheumatol. 2015;67(1):117–127. doi:10.1002/art.38894
62. Makrilakis K, Fragiadaki K, Sfikakis PP, Kitas GD. Chemerin and cardiovascular risk in rheumatoid arthritis after interleukin 6 receptor blockade. J Rheumatol. 2015;42(2):349. doi:10.3899/jrheum.141115
63. McInnes IB, Thompson L, Giles JT, et al. Effect of interleukin-6 receptor blockade on surrogates of vascular risk in rheumatoid arthritis: MEASURE, a randomised, placebo-controlled study. Ann Rheum Dis. 2015;74(4):694–702. doi:10.1136/annrheumdis-2013-204345
64. Kerekes G, Soltesz P, Der H, et al. Effects of rituximab treatment on endothelial dysfunction, carotid atherosclerosis, and lipid profile in rheumatoid arthritis. Clin Rheumatol. 2009;28(6):705–710. doi:10.1007/s10067-009-1095-1
65. Virone A, Bastard JP, Fellahi S, et al. Comparative effect of tumour necrosis factor inhibitors versus other biological agents on cardiovascular risk-associated biomarkers in patients with rheumatoid arthritis. RMD Open. 2019;5(2):e000897. doi:10.1136/rmdopen-2019-000897
66. Leporini C, Russo E, D’Angelo S, et al. Insulin-sensiting effects of tumor necrosis factor alpha inhibitors in rheumatoid arthritis: a systematic review and meta-analysis. Rev Recent Clin Trials. 2018;13(3):184–191. doi:10.2174/1574887113666180314100340
67. Stavropoulos-Kalinoglou A, Metsios GS, Panoulas VF, Nightingale P, Koutedakis Y, Kitas GD. Anti-tumour necrosis factor alpha therapy improves insulin sensitivity in normal-weight but not in obese patients with rheumatoid arthritis. Arthritis Res Ther. 2012;14(4):R160. doi:10.1186/ar3900
68. Stagakis I, Bertsias G, Karvounaris S, et al. Anti-tumor necrosis factor therapy improves insulin resistance, beta cell function and insulin signaling in active rheumatoid arthritis patients with high insulin resistance. Arthritis Res Ther. 2012;14(3):R141. doi:10.1186/ar3874
69. Ruscitti P, Ursini F, Cipriani P, et al. IL-1 inhibition improves insulin resistance and adipokines in rheumatoid arthritis patients with comorbid type 2 diabetes: an observational study. Med. 2019;98(7):e14587. doi:10.1097/MD.0000000000014587
70. Vassilopoulos D, Gravos A, Vlachopoulos C, et al. Adalimumab decreases aortic stiffness independently of its effect in disease activity in patients with rheumatoid arthritis. Clin Rheumatol. 2015;34(2):359–364. doi:10.1007/s10067-014-2718-8
71. Sandoo A, Veldhuijzen van Zanten JJCS, Metsios GS, et al. Vascular function and morphology in rheumatoid arthritis: a systematic review. Rheumatol. 2011;50(11):2125–2139. doi:10.1093/rheumatology/ker275
72. Dulai R, Perry M, Twycross-Lewis R, Morrissey D, Atzeni F, Greenwald S. The effect of tumor necrosis factor-alpha antagonists on arterial stiffness in rheumatoid arthritis: a literature review. Semin Arthritis Rheum. 2012;42(1):1–8. doi:10.1016/j.semarthrit.2012.02.002
73. Zhu TY, Griffith JF, Qin L. Alterations of bone density, microstructure, and strength of the distal radius in male patients with rheumatoid arthritis: a case-control study with HR-pQCT. J Bone Miner Res. 2014;29(9):2118–2129. doi:10.1002/jbmr.2221
74. Tam LS, Kitas GD, Gonzalez-Gay MA. Can suppression of inflammation by anti-TNF prevent progression of subclinical atherosclerosis in inflammatory arthritis? Rheumatol. 2014;53(6):1108–1119. doi:10.1093/rheumatology/ket454
75. Plein S, Erhayiem B, Fent G, et al. Cardiovascular effects of biological versus conventional synthetic disease-modifying antirheumatic drug therapy in treatment-naive, early rheumatoid arthritis. Ann Rheum Dis. 2020;79(11):1414–1422. doi:10.1136/annrheumdis-2020-217653
76. Sidiropoulos PI, Siakka P, Pagonidis K, et al. Sustained improvement of vascular endothelial function during anti‐TNFα treatment in rheumatoid arthritis patients. Scand J Rheumatol. 2009;38(1):6–10. doi:10.1080/03009740802363768
77. Tam LS, Shang Q, Li EK, et al. Infliximab is associated with improvement in arterial stiffness in patients with early rheumatoid arthritis – a randomized trial. J Rheumatol. 2012;39(12):2267–2275. doi:10.3899/jrheum.120541
78. Peters MJ, van Sijl AM, Voskuyl AE, Sattar N, Smulders YM, Nurmohamed MT. The effects of tumor necrosis factor inhibitors on cardiovascular risk in rheumatoid arthritis. Curr Pharm Des. 2012;18(11):1502–1511. doi:10.2174/138161212799504786
79. Ursini F, Leporini C, Bene F, et al. Anti-TNF-alpha agents and endothelial function in rheumatoid arthritis: a systematic review and meta-analysis. Sci Rep. 2017;7(1):5346. doi:10.1038/s41598-017-05759-2
80. Tam LS, Li EK, Shang Q, et al. Tumour necrosis factor alpha blockade is associated with sustained regression of carotid intima-media thickness for patients with active psoriatic arthritis: a 2-year pilot study. Ann Rheum Dis. 2011;70(4):705–706. doi:10.1136/ard.2010.131359
81. Kume K, Amano K, Yamada S, Hatta K, Ohta H, Kuwaba N. Tocilizumab monotherapy reduces arterial stiffness as effectively as etanercept or adalimumab monotherapy in rheumatoid arthritis: an open-label randomized controlled trial. J Rheumatol. 2011;38(10):2169–2171. doi:10.3899/jrheum.110340
82. Gonzalez-Juanatey C, Llorca J, Vazquez-Rodriguez TR, Diaz-Varela N, Garcia-Quiroga H, Gonzalez-Gay MA. Short-term improvement of endothelial function in rituximab-treated rheumatoid arthritis patients refractory to tumor necrosis factor alpha blocker therapy. Arthritis Rheum. 2008;59(12):1821–1824. doi:10.1002/art.24308
83. Benucci M, Saviola G, Manfredi M, Sarzi-Puttini P, Atzeni F. Factors correlated with improvement of endothelial dysfunction during rituximab therapy in patients with rheumatoid arthritis. Biologics. 2013;7:69–75. doi:10.2147/BTT.S39182
84. Sandoo A, Kitas GD. The impact of abatacept treatment on the vasculature in patients with rheumatoid arthritis. Clin Exp Rheumatol. 2015;33(4):589.
85. Benucci M, Bandinelli F, Damiani A, et al. Factors correlated with the improvement of endothelial dysfunction during Abatacept therapy in patients with rheumatoid arthritis. J Inflamm Res. 2018;11:247–252. doi:10.2147/JIR.S156822
86. Low AS, Symmons DP, Lunt M, et al. Relationship between exposure to tumour necrosis factor inhibitor therapy and incidence and severity of myocardial infarction in patients with rheumatoid arthritis. Ann Rheum Dis. 2017;76(4):654–660. doi:10.1136/annrheumdis-2016-209784
87. Low AS, Lunt M, Mercer LK, et al. Association between ischemic stroke and tumor necrosis factor inhibitor therapy in patients with rheumatoid arthritis. Arthritis Rheumatol. 2016;68(6):1337–1345. doi:10.1002/art.39582
88. Naranjo A, Sokka T, Descalzo MA, et al. Cardiovascular disease in patients with rheumatoid arthritis: results from the QUEST-RA study. Arthritis Res Ther. 2008;10(2):R30. doi:10.1186/ar2383
89. Lee JL, Sinnathurai P, Buchbinder R, Hill C, Lassere M, March L. Biologics and cardiovascular events in inflammatory arthritis: a prospective national cohort study. Arthritis Res Ther. 2018;20(1):171. doi:10.1186/s13075-018-1669-x
90. Barnabe C, Martin BJ, Ghali WA. Systematic review and meta-analysis: anti-tumor necrosis factor alpha therapy and cardiovascular events in rheumatoid arthritis. Arthritis Care Res. 2011;63(4):522–529. doi:10.1002/acr.20371
91. Roubille C, Richer V, Starnino T, et al. The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(3):480–489. doi:10.1136/annrheumdis-2014-206624
92. Kim SC, Solomon DH, Rogers JR, et al. No difference in cardiovascular risk of tocilizumab versus abatacept for rheumatoid arthritis: a multi-database cohort study. Semin Arthritis Rheum. 2018;48(3):399–405. doi:10.1016/j.semarthrit.2018.03.012
93. Xie F, Yun H, Levitan EB, Muntner P, Curtis JR. Tocilizumab and the risk of cardiovascular disease: direct comparison among biologic disease-modifying antirheumatic drugs for rheumatoid arthritis patients. Arthritis Care Res. 2019;71(8):1004–1018. doi:10.1002/acr.23737
94. Swerdlow DI, Holmes MV, Kuchenbaecker KB, et al. The interleukin-6 receptor as a target for prevention of coronary heart disease: a mendelian randomisation analysis. Lancet. 2012;379(9822):1214–1224.
95. Giles JT, Sattar N, Gabriel S, et al. Cardiovascular safety of tocilizumab versus etanercept in rheumatoid arthritis: a randomized controlled trial. Arthritis Rheumatol. 2020;72(1):31–40. doi:10.1002/art.41095
96. Singh S, Fumery M, Singh AG, et al. Comparative risk of cardiovascular events with biologic and synthetic disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res. 2020;72(4):561–576. doi:10.1002/acr.23875
97. van Vollenhoven RF, Fleischmann RM, Furst DE, Lacey S, Lehane PB. Longterm safety of rituximab: final report of the rheumatoid arthritis global clinical trial program over 11 years. J Rheumatol. 2015;42(10):1761–1766. doi:10.3899/jrheum.150051
98. van Sijl AM, van der Weele W, Nurmohamed MT. Myocardial infarction after rituximab treatment for rheumatoid arthritis: is there a link? Curr Pharm Des. 2014;20(4):496–499.
99. Lee L, Kukreti V. Rituximab-induced coronary vasospasm. Case Rep Hematol. 2012;2012:984986. doi:10.1155/2012/984986
100. Kang EH, Jin Y, Brill G, et al. Comparative cardiovascular risk of abatacept and tumor necrosis factor inhibitors in patients with rheumatoid arthritis with and without diabetes mellitus: a multidatabase cohort study. J Am Heart Assoc. 2018;7(3).
101. Jin Y, Kang EH, Brill G, Desai RJ, Kim SC. Cardiovascular (CV) risk after initiation of abatacept versus TNF inhibitors in rheumatoid arthritis patients with and without baseline CV disease. J Rheumatol. 2018;45(9):1240–1248. doi:10.3899/jrheum.170926
102. Zhang J, Xie F, Yun H, et al. Comparative effects of biologics on cardiovascular risk among older patients with rheumatoid arthritis. Ann Rheum Dis. 2016;75(10):1813–1818. doi:10.1136/annrheumdis-2015-207870
103. van Eijk IC, de Vries MK, Levels JH, et al. Improvement of lipid profile is accompanied by atheroprotective alterations in high-density lipoprotein composition upon tumor necrosis factor blockade: a prospective cohort study in ankylosing spondylitis. Arthritis Rheum. 2009;60(5):1324–1330. doi:10.1002/art.24492
104. Mathieu S, Dubost JJ, Tournadre A, Malochet-Guinamand S, Ristori JM, Soubrier M. Effects of 14 weeks of TNF alpha blockade treatment on lipid profile in ankylosing spondylitis. Jt Bone Spine. 2010;77(1):50–52. doi:10.1016/j.jbspin.2009.05.012
105. Min HK, Lee J, Ju JH, Park SH, Kwok SK. Impact of TNF-alpha inhibitor on lipid profile and atherogenic index of plasma in axial spondyloarthritis: 2-year follow-up data from the Catholic Axial Spondyloarthritis COhort (CASCO). Clin Rheumatol. 2020;39(2):471–477. doi:10.1007/s10067-019-04767-z
106. Agca R, Heslinga M, Kneepkens EL, van Dongen C, Nurmohamed MT. The effects of 5-year etanercept therapy on cardiovascular risk factors in patients with psoriatic arthritis. J Rheumatol. 2017;44(9):1362–1368. doi:10.3899/jrheum.161418
107. Arida A, Protogerou AD, Konstantonis G, et al. Subclinical atherosclerosis is not accelerated in patients with ankylosing spondylitis with low disease activity: new data and metaanalysis of published studies. J Rheumatol. 2015;42(11):2098–2105. doi:10.3899/jrheum.150316
108. Capkin E, Karkucak M, Kiris A, et al. Anti-TNF-alpha therapy may not improve arterial stiffness in patients with AS: a 24-week follow-up. Rheumatol. 2012;51(5):910–914. doi:10.1093/rheumatology/ker434
109. Tam LS, Shang Q, Kun EW, et al. The effects of golimumab on subclinical atherosclerosis and arterial stiffness in ankylosing spondylitis-a randomized, placebo-controlled pilot trial. Rheumatol. 2014;53(6):1065–1074. doi:10.1093/rheumatology/ket469
110. Mathieu S, Pereira B, Couderc M, Rabois E, Dubost JJ, Soubrier M. No significant changes in arterial stiffness in patients with ankylosing spondylitis after tumour necrosis factor alpha blockade treatment for 6 and 12 months. Rheumatol. 2013;52(1):204–209. doi:10.1093/rheumatology/kes272
111. Syngle A, Vohra K, Sharma A, Kaur L. Endothelial dysfunction in ankylosing spondylitis improves after tumor necrosis factor-alpha blockade. Clin Rheumatol. 2010;29(7):763–770. doi:10.1007/s10067-010-1402-x
112. Genre F, Lopez-Mejias R, Miranda-Filloy JA, et al. Anti-TNF-alpha therapy reduces endothelial cell activation in non-diabetic ankylosing spondylitis patients. Rheumatol Int. 2015;35(12):2069–2078. doi:10.1007/s00296-015-3314-1
113. Van Eijk IC, Peters MJL, Serné EH, et al. Microvascular function is impaired in ankylosing spondylitis and improves after tumour necrosis factor α blockade. Ann Rheum Dis. 2009;68(3):362–366. doi:10.1136/ard.2007.086777
114. van Sijl AM, van Eijk IC, Peters MJ, et al. Tumour necrosis factor blocking agents and progression of subclinical atherosclerosis in patients with ankylosing spondylitis. Ann Rheum Dis. 2015;74(1):119–123. doi:10.1136/annrheumdis-2013-203934
115. Zardi EM, Pipita ME, Giorgi C, Lichinchi D, Zardi DM, Afeltra A. Differences in carotid atherosclerosis between patients with ankylosing spondylitis treated with tumor necrosis factor-alpha antagonists and healthy matched controls. Med. 2018;97(27):e11250. doi:10.1097/MD.0000000000011250
116. Di Minno MN, Iervolino S, Peluso R, Scarpa R, Di Minno G; Ca Rrd study group. Carotid intima-media thickness in psoriatic arthritis: differences between tumor necrosis factor-alpha blockers and traditional disease-modifying antirheumatic drugs. Arter Thromb Vasc Biol. 2011;31(3):705–712. doi:10.1161/ATVBAHA.110.214585
117. Eder L, Joshi AA, Dey AK, et al. Association of tumor necrosis factor inhibitor treatment with reduced indices of subclinical atherosclerosis in patients with psoriatic disease. Arthritis Rheumatol. 2018;70(3):408–416. doi:10.1002/art.40366
118. Yang ZS, Lin NN, Li L, Li Y. The effect of TNF inhibitors on cardiovascular events in psoriasis and psoriatic arthritis: an updated meta-analysis. Clin Rev Allergy Immunol. 2016;51(2):240–247. doi:10.1007/s12016-016-8560-9
119. Lee MP, Desai RJ, Jin Y, Brill G, Ogdie A, Kim SC. Association of ustekinumab vs TNF inhibitor therapy with risk of atrial fibrillation and cardiovascular events in patients with psoriasis or psoriatic arthritis. JAMA Dermatol. 2019;155(6):700–707. doi:10.1001/jamadermatol.2019.0001
120. Mavrogeni SI, Kitas GD, Dimitroulas T, et al. Cardiovascular magnetic resonance in rheumatology: current status and recommendations for use. Int J Cardiol. 2016;217:135–148. doi:10.1016/j.ijcard.2016.04.158
121. Mavrogeni S. Assessment of cardiovascular involvement in Connective Tissue Disease: let’s open Pandora’s box. Mediterr J Rheumatol. 2016;27(3):91–93. doi:10.31138/mjr.27.3.91
122. Seneviratne MG, Grieve SM, Figtree GA, et al. Prevalence, distribution and clinical correlates of myocardial fibrosis in systemic lupus erythematosus: a cardiac magnetic resonance study. Lupus. 2016;25(6):573–581. doi:10.1177/0961203315622275
123. Opinc AH, Makowski MA, Lukasik ZM, Makowska JS. Cardiovascular complications in patients with idiopathic inflammatory myopathies: does heart matter in idiopathic inflammatory myopathies? Heart Fail Rev. 2021;26(1):111–125. doi:10.1007/s10741-019-09909-8
124. Galea N, Rosato E, Gigante A, et al. Early myocardial damage and microvascular dysfunction in asymptomatic patients with systemic sclerosis: a cardiovascular magnetic resonance study with cold pressor test. PLoS One. 2020;15(12):e0244282. doi:10.1371/journal.pone.0244282
125. Mavrogeni SI, Dimitroulas T, Kitas GD. Cardiovascular magnetic resonance in the diagnosis and management of cardiac and vascular involvement in the systemic vasculitides. Curr Opin Rheumatol. 2019;31(1):16–24. doi:10.1097/BOR.0000000000000560
126. Mavrogeni S, Markousis-Mavrogenis G, Koutsogeorgopoulou L, et al. Cardiovascular magnetic resonance imaging pattern at the time of diagnosis of treatment naive patients with connective tissue diseases. Int J Cardiol. 2017;236:151–156. doi:10.1016/j.ijcard.2017.01.104
127. Fijolek J, Wiatr E, Gawryluk D, et al. The significance of cardiac magnetic resonance imaging in detection and monitoring of the treatment efficacy of heart involvement in eosinophilic granulomatosis with polyangiitis patients. Sarcoidosis Vasc Diffus Lung Dis. 2016;33(1):51–58.
128. Miszalski-Jamka T, Szczeklik W, Sokolowska B, et al. Noncorticosteroid immunosuppression limits myocardial damage and contractile dysfunction in eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome). J Am Coll Cardiol. 2015;65(1):103–105. doi:10.1016/j.jacc.2014.08.055
129. Wang CR, Tsai YS, Li WT. Lupus myocarditis receiving the rituximab therapy-a monocentric retrospective study. Clin Rheumatol. 2018;37(6):1701–1707. doi:10.1007/s10067-017-3971-4
130. Kobayashi Y, Kobayashi H, Giles J, Yokoe I, Nishiwaki A, Takei M. Impact of biological treatment on left ventricular function and morphology in rheumatoid arthritis patients without cardiac symptoms, assessed by cardiac magnetic resonance imaging. Scand J Rheumatol. 2017;46(4):328–329. doi:10.3109/03009742.2016.1173722
131. Ntusi NAB, Francis JM, Sever E, et al. Anti-TNF modulation reduces myocardial inflammation and improves cardiovascular function in systemic rheumatic diseases. Int J Cardiol. 2018;270:253–259. doi:10.1016/j.ijcard.2018.06.099
132. Daien CI, Fesler P, Du Cailar G, et al. Etanercept normalises left ventricular mass in patients with rheumatoid arthritis. Ann Rheum Dis. 2013;72(6):881–887. doi:10.1136/annrheumdis-2012-201489
133. Kotyla PJ, Owczarek A, Rakoczy J, Lewicki M, Kucharz EJ, Emery P. Infliximab treatment increases left ventricular ejection fraction in patients with rheumatoid arthritis: assessment of heart function by echocardiography, endothelin 1, interleukin 6, and NT-pro brain natriuretic peptide. J Rheumatol. 2012;39(4):701–706. doi:10.3899/jrheum.110751
134. Kobayashi H, Kobayashi Y, Giles JT, Yoneyama K, Nakajima Y, Takei M. Tocilizumab treatment increases left ventricular ejection fraction and decreases left ventricular mass index in patients with rheumatoid arthritis without cardiac symptoms: assessed using 3.0 tesla cardiac magnetic resonance imaging. J Rheumatol. 2014;41(10):1916–1921. doi:10.3899/jrheum.131540
135. Ahlers MJ, Lowery BD, Farber-Eger E, et al. Heart failure risk associated with rheumatoid arthritis-related chronic inflammation. J Am Heart Assoc. 2020;9(10):e014661.
136. Caforio ALP, Adler Y, Agostini C, et al. Diagnosis and management of myocardial involvement in systemic immune-mediated diseases: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Disease. Eur Heart J. 2017;38(35):2649–2662. doi:10.1093/eurheartj/ehx321
137. Antoniades L, Sfikakis PP, Mavrikakis M. Glucocorticoid effects on myocardial performance in patients with systemic sclerosis. Clin Exp Rheumatol. 2001;19(4):431–437.
138. Cole J, Busti A, Kazi S. The incidence of new onset congestive heart failure and heart failure exacerbation in Veteran’s Affairs patients receiving tumor necrosis factor alpha antagonists. Rheumatol Int. 2007;27(4):369–373. doi:10.1007/s00296-006-0215-3
139. Curtis JR, Kramer JM, Martin C, et al. Heart failure among younger rheumatoid arthritis and Crohn’s patients exposed to TNF-alpha antagonists. Rheumatology (Oxford). 2007;46(11):1688–1693. doi:10.1093/rheumatology/kem212
140. Baniaamam M, Paulus WJ, Blanken AB, Nurmohamed MT. The effect of biological DMARDs on the risk of congestive heart failure in rheumatoid arthritis: a systematic review. Expert Opin Biol Ther. 2018;18(5):585–594. doi:10.1080/14712598.2018.1462794
141. Tomas L, Lazurova I, Pundova L, et al. Acute and long-term effect of infliximab on humoral and echocardiographic parameters in patients with chronic inflammatory diseases. Clin Rheumatol. 2013;32(1):61–66. doi:10.1007/s10067-012-2091-4
142. Mavrogeni SI, Sfikakis PP, Dimitroulas T, et al. Can cardiovascular magnetic resonance prompt early cardiovascular/rheumatic treatment in autoimmune rheumatic diseases? Current practice and future perspectives. Rheumatol Int. 2018;38(6):949–958. doi:10.1007/s00296-018-4004-6
143. Goodson NJ, Symmons DP, Scott DG, Bunn D, Lunt M, Silman AJ. Baseline levels of C-reactive protein and prediction of death from cardiovascular disease in patients with inflammatory polyarthritis: a ten-year followup study of a primary care-based inception cohort. Arthritis Rheum. 2005;52(8):2293–2299. doi:10.1002/art.21204
144. Dixon WG, Watson KD, Lunt M, et al. Reduction in the incidence of myocardial infarction in patients with rheumatoid arthritis who respond to anti-tumor necrosis factor alpha therapy: results from the British Society for Rheumatology Biologics Register. Arthritis Rheum. 2007;56(9):2905–2912. doi:10.1002/art.22809
145. Gasparyan AY. Cardiovascular risk and inflammation: pathophysiological mechanisms, drug design, and targets. Curr Pharm Des. 2012;18(11):1447–1449. doi:10.2174/138161212799504777
146. Ridker PM, MacFadyen JG, Everett BM, et al. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: a secondary analysis from the CANTOS randomised controlled trial. Lancet. 2018;391(10118):319–328. doi:10.1016/S0140-6736(17)32814-3
147. Semb AG, Ikdahl E, Wibetoe G, Crowson C, Rollefstad S. Atherosclerotic cardiovascular disease prevention in rheumatoid arthritis. Nat Rev Rheumatol. 2020;16(7):361–379. doi:10.1038/s41584-020-0428-y
148. Ridker PM. Clinician’s guide to reducing inflammation to reduce atherothrombotic risk: JACC review topic of the week. J Am Coll Cardiol. 2018;72(25):3320–3331. doi:10.1016/j.jacc.2018.06.082
149. Ridker PM, Libby P, MacFadyen JG, et al. Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Eur Heart J. 2018;39(38):3499–3507. doi:10.1093/eurheartj/ehy310
150. van Hout GP, Bosch L, Ellenbroek GH, et al. The selective NLRP3-inflammasome inhibitor MCC950 reduces infarct size and preserves cardiac function in a pig model of myocardial infarction. Eur Heart J. 2017;38(11):828–836.
151. van der Heijden T, Kritikou E, Venema W, et al. NLRP3 inflammasome inhibition by MCC950 reduces atherosclerotic lesion development in apolipoprotein E-deficient mice-brief report. Arter Thromb Vasc Biol. 2017;37(8):1457–1461. doi:10.1161/ATVBAHA.117.309575
152. Nidorf SM, Eikelboom JW, Budgeon CA, Thompson PL. Low-dose colchicine for secondary prevention of cardiovascular disease. J Am Coll Cardiol. 2013;61(4):404–410. doi:10.1016/j.jacc.2012.10.027
153. Provan SA, Lillegraven S, Sexton J, et al. Trends in all-cause and cardiovascular mortality in patients with incident rheumatoid arthritis: a 20-year follow-up matched case-cohort study. Rheumatol. 2020;59(3):505–512.
154. Lacaille D, Avina-Zubieta JA, Sayre EC, Abrahamowicz M. Improvement in 5-year mortality in incident rheumatoid arthritis compared with the general population-closing the mortality gap. Ann Rheum Dis. 2017;76(6):1057–1063. doi:10.1136/annrheumdis-2016-209562
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.