Back to Journals » International Journal of General Medicine » Volume 14
Effect of APOEϵ4 on Functional Brain Network in Patients with Subjective Cognitive Decline: A Resting State Functional MRI Study
Authors Deng S, Sun L, Chen W, Liu X ![]() , Chen S
, Chen S
Received 4 October 2021
Accepted for publication 6 December 2021
Published 14 December 2021 Volume 2021:14 Pages 9761—9771
DOI https://doi.org/10.2147/IJGM.S342673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Simin Deng,1,* Lingyu Sun,2,* Weijie Chen,1,* Xiaorong Liu,2 Shangjie Chen3
1The Second School of Clinical Medicine, Southern Medical University, Dongguan Tung Wah Hospital, Guangdong, People’s Republic of China; 2Department of Rehabilitation Medicine, Dongguan Tung Wah Hospital, Guangdong, People’s Republic of China; 3Department of Rehabilitation Medicine, Affiliated Baoan Hospital of Shenzhen, Southern Medical University, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shangjie Chen
Department of Rehabilitation Medicine, Affiliated Baoan Hospital of Shenzhen, Southern Medical University, No. 118 Longjing Second Road, Baoan District, Shenzhen, Guangdong, People’s Republic of China
Tel +86-755-27788311
Fax +86-755-29791989
Email [email protected]
Purpose: Subjective cognitive decline (SCD) is the earliest symptom stage of Alzheimer’s disease (AD), and the APOEϵ4 allele is the strongest genetic risk factor for sporadic AD. Based on graph theory, the resting state functional connectivity (rsFC) in SCD patients with APOEϵ4 was studied to explore the effect of APOEϵ4 on the rsFC network properties of SCD patients.
Patients and Methods: This cross-sectional study included MRI image data from 19 SCD patients with APOEϵ4 (SCD+), 29 SCD patients without APOEϵ4 (SCD−), and 30 normal control (NC−) individuals without APOEϵ4. We generated a binary matrix based on anatomical automatic labeling (AAL) 90 atlas to construct the functional network. We then calculated the whole brain network characteristics and intracerebral node characteristics by graph theory.
Results: For the whole brain network characteristics, all three groups showed small-worldness. The SCD+ group had increased compensatory information transfer speed and enhanced integration capability. This group also had high heterogeneity for intracerebral node characteristics, mainly in the default mode network, left superior occipital gyrus, and bilateral putamen.
Conclusion: APOEϵ4 effects the functional brain network in patients with SCD and may be a potential indicator for the identification of SCD.
Keywords: SCD, APOEϵ4 allele, graph theory, whole brain network characteristics, intracerebral node characteristics
Introduction
The incidence of dementia has markedly increased with the aging of the population.1 Alzheimer’s disease (AD) is the most common cause for senile dementia, and nearly 50 million patients worldwide were reported to have AD dementia in 2018 (a statistic that is expected to triple in the next 25 years).1 As a progressive and irreversible neurodegenerative disease,2 AD presents vast societal and familial burdens that would be somewhat alleviated with additional knowledge about the pathophysiology of the disease. To understand the mechanism of AD and its treatment, research at the preclinical level is crucial.1,3 Subjective cognitive decline (SCD) is the preclinical period of AD and the earliest symptom stage. In this state, patients may subjectively experience a cognitive decline, although neuropsychiatric assessment often appears normal.4 The progression of SCD to mild cognitive impairment (MCI; 27%) and AD (14%) is relatively rare,5 and most SCD patients will not experience progressive cognitive decline.4 Because self-perception and neuropsychological methods of diagnosis are often unreliable, we explored whether risk factors appear in early SCD that promote disease progression. Indeed, AD risk factors impact disease progression, but whether AD risk factors can be used as potential indicators to predict SCD progression remains unclear. Here, we explored the influence of AD risk factors on SCD patients.
The Apolipoprotein E4 (APOEε4) allele is the strongest known genetic risk factor for sporadic AD.6 Risk of developing AD in carriers of the APOEε4 (individuals with at least one APOEε4 allele, genotypes ε4/ε4, ε4/ε3) monoallele is 3- to 4-fold higher than general population; the possibility of carriers of the diallele developing AD is 9- to 15-fold higher.7–10 Furthermore, the possibility of carriers developing MCI is 2.2- to 6.2-fold higher than that of non-carriers of APOEε4.11 Finally, the risk for progression to AD in APOEε4 carriers with previously existing cognitive disorders or MCI is 4.1- to 25-fold higher than in non-carriers.12 To confirm whether carrying APOEε4 is a risk factor for SCD progression, we used graph theory analysis of resting-state functional magnetic resonance imaging (rs-fMRI) to observe the characteristics of brain network organization, clarify the internal activities of the brain, and describe and predict dysfunction from the perspective of the network.13
In elderly carriers of the APOEε4 allele, resting state functional connectivity (rsFC) changes before Aβ deposition.14 Default mode network (DMN) functional connectivity (FC) changes in rsFC connectivity also occur in the frontal and posterior lobes, as well as in the right hippocampus in the DMN of SCD patients, although frontal lobe FC in carriers of the APOEε4 allele increases relatively slowly.15 Importantly, FC can be used as one of the earliest potential neuroimaging markers for neurodegenerative disease.16
Here, we hypothesized that (1) APOEε4 effects the functional brain network in patients with SCD, and (2) APOEε4 may be used as an indicator to identify the progress of SCD. To test these hypotheses, we obtained rs-fMRI data from 34 normal control individuals without APOEε4 (NC−), 20 SCD patients with at least one APOEε4 allele (SCD+), and 34 SCD patients without APOEε4 (SCD−) from the Alzheimer’s Disease Neuroimaging Initiative (ADNI). We then constructed a functional brain network based on graph theory and analyzed relevant rsFC data.
Patients and Methods
Study Subjects
All raw data used in this study, including neuropsychological assessment scale, MRI images, and biomarker data of cerebrospinal fluid (CSF), were obtained from the ADNI (adni.loni.usc.edu) project. As a longitudinal, multicenter study designed to develop clinical, imaging, genetic, and biochemical biomarkers, the ADNI project strives to develop methods for the early detection and subsequent tracking of AD. According to ADNI standard operating procedures, the current study was approved by the Institutional Review Board (IRB) of all participating centers in ADNI. We obtained the approval of our local ethics review committee (Dongguan Tung Wah Hospital medical ethics committee 2019DHLL052) before analysis began. The study included 54 patients with SCD (baseline SCD patients with neuropsychological assessment, CSF biomarkers, APOE genotyping information and 3.0 rs-fMRI data in the ADNI2 database), and 54 normal controls (NC) in a 1:1 random ratio. NC and SCD patients were further divided into the APOEε4+ group and APOEε4- group based on whether they carried the APOEε4 gene. The 54 NC participants included 20 normal control individuals with APOEε4 (NC+) and 34 cases of NC-; the 54 patients with SCD included 20 cases of SCD+ and 34 SCD-. To avoid unwanted effects of APOEε4 on the results of the current study, the number of NC- patients was relatively small. The diagnostic criteria of SCD included: 1) self-reported patient memory loss (combined with a contradictory statement by a caregiver); 2) normal cognitive range on a delayed recall test of the Wechsler Memory Scale-Logical Memory (WMS-LM) task; 3) Mini-Mental State Examination (MMSE) evaluation; and 4) Clinical Dementia Rating Scale (CDR) evaluation. Inclusion criteria of the NC group: no memory impairment or decline as reported by both the patient and caregiver; and comparable scores to SCD patients on test of delayed recall of WMS-LM, MMSE, and CDR. Demographic data included age, sex, and educational level; neuropsychological tests included 1) MMSE; 2) delayed recall of WMS-LM; 3) Alzheimer’s Disease Assessment Scale 13 (ADAS13); 4) Rey Auditory Verbal Learning Test (RAVLT) immediate; and 5) Trail Making Test Part B (TMT-B). Importantly, these tests have been previously associated with SCD progression.17 Finally, CSF biomarkers included β-amyloid protein 1–42 (Aβ1-42), total tau (t-tau), and phosphorylated tau181 (p-tau181); all analyzed subjects had CSF data.
Collection and Preprocessing of MRI Data
All subjects were selected from ADNI2, and structural MRI and rs-fMRI data were obtained for each participant via a 3.0 MRI scanner. Structural MRI images were obtained according to the following scanning parameters: Acquisition Plane=SAGITTAL; Acquisition Type=3D; Coil=PA; Field Strength=3.0 tesla; Flip Angle=9.0 degree; Manufacturer=SIEMENS; Matrix X=240.0 pixels; Matrix Y=256.0 pixels; Matrix Z=176.0; Mfg Model=Prisma_fit; Pixel Spacing X=1.1 mm; Pixel Spacing Y=1.1 mm; Pulse Sequence=GR/IR; Slice Thickness=1.2 mm; TE=3.0 ms; TI=900.0 ms; TR=2300.0 ms; and Weighting=T1. rs-fMRI images were obtained at the following scanning parameters: Field Strength=3.0 tesla; Flip Angle=90.0 degree; Manufacturer=SIEMENS; Matrix X=448.0 pixels; Matrix Y=448.0 pixels; Mfg Model=Prisma; Pixel Spacing X=3.4 mm; Pixel Spacing Y=3.4 mm; Pulse Sequence=EP; Slices=197.0; Slice Thickness=3.4 mm; TE=30.0 ms; and TR=3000.0 ms.
All rs-fMRI data were pre-processed13 using the resting-state functional magnetic resonance imaging data processing toolkit Restplus 1.7 (http://www.restfmri.net/forum/RESTplusV1.7),18 which is based on Statistical Parametric Mapping (SPM12, https://www.fil.ion.ucl.ac.uk/spm/software/spm12) on the MATLAB R2013b platform (The MathWorks Inc., Natick, MA, US) per manufacturer’s recommendation. Briefly, we first converted the data format using dcm2nii to convert the functional image and structural image of the original data into nifti format files. We then removed the first 10 time points due to initial patient and machine instability. Finally, we corrected the time layer (one process for each scan: the interpolation method was used to assure accuracy in the results). The scanning order included the interlayer scan at the beginning of each odd layer; 4. Head motion correction by displacement and rotation threshold values of 3 mm and 3 degrees, respectively. If displacement of head motion exceeded 3 mm or the rotation angle exceeded 3 degrees, the subject was excluded; 5. Spatial standardization, using the echo planar imaging (EPI) registration method, spatial standardization, and data registration to the standard space; 6. De-linear trending due to potential linear drift; 7. Filtration using the effective frequency band of 0.01–0.08 Hz; and 8. Regression covariate analysis (white matter, CSF, and cephalic noise).
Construction and Analysis of Brain Network
The anatomical automatic labeling (AAL) 90 atlas19 was used as the brain region template. Whole brain images were divided into 90 distinct regions, and each was considered a node in the brain network. Pearson’s correlation coefficient between the time series of each pair of regions of interest was calculated using MATLAB-based GRETNA software (The Graph-theoretical Network Analysis Toolkit, www.nitrc.org)20 to generate a binary matrix and construct the functional network.21
Network Properties
To characterize the topological organization of the rsFC network, the following whole brain network characteristics were assessed: small-worldness, global efficiency, local efficiency, characteristic path length, clustering coefficient, and assortativity. For intracerebral node characteristics, we considered nodal efficiency, nodal local efficiency, degree centrality, and betweenness centrality. For the definitions of these network properties and their computations, refer to Rubinov et al,22 as shown in Supplementary File 1.
Statistical Analysis
SPSS 20.0 statistical analysis software was used for the analysis of demographic data, neuropsychological assessment, and CSF biomarkers. For continuous variables, one-way analysis of variance (ANOVA) was used. Two sample t-test was then performed for significant results. For binary variables (such as sex), the χ2 test was used. P<0.05 was considered statistically significant. The network properties were analyzed by one-way ANOVA F-test and two-sample t-test in the Global and Nodal Metric Comparison module of GRETNA for each of the three groups. An AAL90 template was used where the sparsity was 0.05–0.26, the interval was 0.01 (sparsity ≤ 0.26, 90% of the subjects have small-world attributes), and the number of iterations was 500. For significant results, a two-sample t-test was used for post hoc analysis and the threshold was set to p<0.05. Multiple comparison correction (few and fdr) was then performed. None passed the correction, and the uncorrected results were selected.
Results
Demographic Data
This study included 30 NC−, 29 SCD− and 19 SCD+ subjects (nine participants were excluded due to poor image quality). Table 1 summarizes demographics, neuropsychological evaluation, and CSF biomarkers of each group. No significant differences were observed in sex, educational level, or neuropsychological performance between the three groups (p>0.05). The SCD+ group (69.82±5.18 years) was significantly younger than the SCD− group (72.17±4.91 years) (p=0.014) and NC− group (74.50±5.86 years) (p=0.014); had significantly higher TAU levels (281.87±100.14 pg/mL) than the SCD− group (207.53±74.37 pg/mL) (p=0.004) and NC− group (225.49±64.00 pg/mL) (p=0.004); and had significantly higher PTAU levels (26.41±11.19 pg/mL) than the SCD− group (18.31±6.92 pg/mL) (p=0.002) and NC− group (19.12±5.87 pg/mL) (p=0.002). Hence, these three indicators were used as regression covariates for statistical analysis in subsequent image processing; the significance threshold was set to p<0.05.
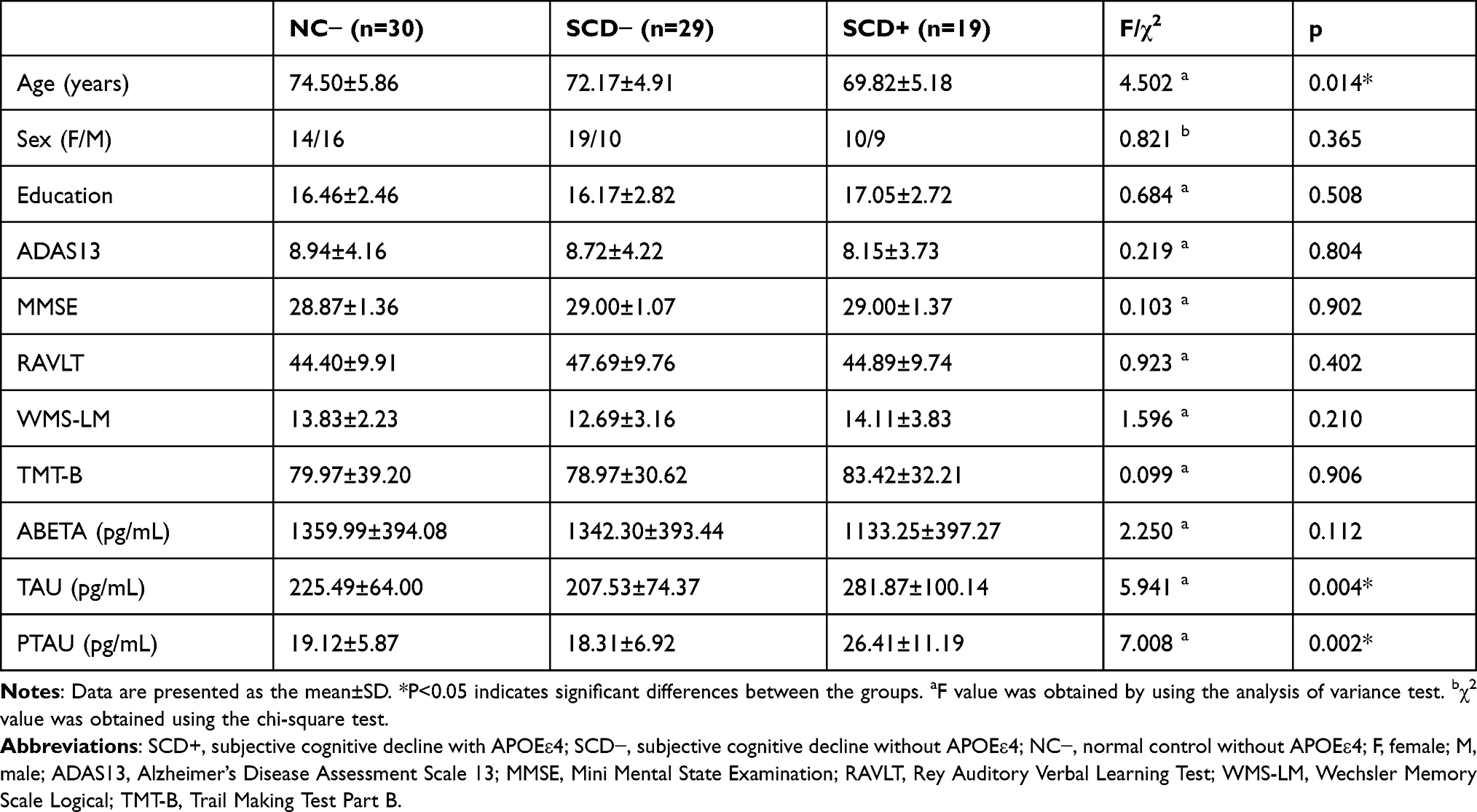 |
Table 1 Differences in Demographic Characteristics, Neuropsychological Assessment, and Cerebrospinal Fluid Biomarkers Among Three Groups of Subjects |
Whole Brain Network Characteristics
When the sparsity value is 0.05–0.26 and the interval is 0.01, the area under the curve (AUC) acts as an independent variable for statistical comparison between groups. Whole brain network characteristic results among SCD+, SCD−, and NC− patients are shown in Figures 1 and 2 and Table 2. SCD+, SCD−, and NC− groups all showed small-world property in the functional network, characterized by normalized clustering coefficients (γ) (γ>1) and normalized characteristic path length (λ) (λ≈1). SCD+, SCD−, and NC− groups were within the wider sparse threshold range (0.05~0.26). The AUC of shortest path length (LP) (0.5104±0.6413) (Figure 1A, p=0.035) and λ (0.2387±0.0056) (Figures 1C and 2A, p=0.000) was significantly lower in the SCD+ group compared to the SCD− group (0.5431±0.6287, 0.2525±0.0142) and NC− group (0.5588±0.6113, 0.2531±0.0133); there was no significant change in clustering coefficient (CP). The small-world property (σ) was defined by CP and LP, σ= γ/λ, and the σ value of SCD+ group increased. The AUC of global efficiency was higher in the SCD+ group (0.936±0.0752) compared to the NC− group (0.872±0.0749) (Figure 2B, p=0.023), although the SCD+ group had lower assortativity (0.490±0.1551) than the SCD− (0.638±0.1980) and NC− (0.601±0.1591) groups (Figure 2C, p=0.017). Statistical analyses were performed with and without regression covariates, although no differences were observed.
 |
Table 2 Characteristics of Global Properties Among Three Groups of Subjects |
 |
Figure 1 Small-world parameters of the global cerebral resting-state functional network among three groups of subjects at a sparsity rating of 0.05–0.26. (A) LP, Shortest path length, compared with that of the NC− and SCD−; the LP of the SCD+ was not significantly different (P˃0.05). (B) CP, Clustering coefficient, compared with that of the NC− and SCD−; the CP of the SCD+ was not significantly different (P˃0.05). (C) Lambda (λ), Normalized characteristic path length, compared with that of the NC− and SCD−; the LP of the SCD+ was significantly decreased (P<0.05). (D) Sigma (σ), Small-worldness, compared with that of the NC− and SCD−; the σ of the SCD+ was not significantly different (P˃0.05). Abbreviations: SCD+, subjective cognitive decline with APOEε4; SCD−, subjective cognitive decline without APOEε4; NC−, normal control without APOEε4; LP, shortest path length; CP, clustering coefficient; λ, normalized characteristic path length; σ, small-worldness. |
 |
Figure 2 Characteristics of global properties among three groups of subjects with statistical significance. (A) Lambda (λ), Normalized characteristic path length, compared with that of the NC− and SCD−; the λ of the SCD+ was significantly decreased (P<0.05). (B) Global Efficiency, compared with that of the NC−; the global efficiency of the SCD+ was significantly increased (P<0.05). (C) Assortativity, compared with that of the NC− and SCD−; the assortativity of the SCD+ was significantly increased (P<0.05). *** indicates statistically significant. Abbreviations: SCD+, subjective cognitive decline with APOEε4; SCD−, subjective cognitive decline without APOEε4; NC−, normal control without APOEε4. |
Intracerebral Node Characteristics
We then compared node characteristics in the functional network between the SCD+ group and SCD− and NC− groups. The SCD+ group had high heterogeneity in intracerebral node characteristics, particularly in the DMN, left superior occipital gyrus, and bilateral putamen. The specific manifestations were as follows: lower local efficiency at the superior occipital gyrus node and higher local efficiency in three discrete regions including the right putamen, posterior cingulate cortex, and left putamen (p<0.05; Figure 3, Table 3); In addition, the SCD+ group had higher degree centrality at the posterior cingulate cortex, although lower degree centrality at the dorsolateral superior frontal gyrus (p<0.05; Figure 3, Table 4). Statistical analyses were performed with and without regression covariates separately, which revealed no difference.
 |
Table 3 Brain Regions with Significant Nodal Local Efficiency Differences Between the Groups |
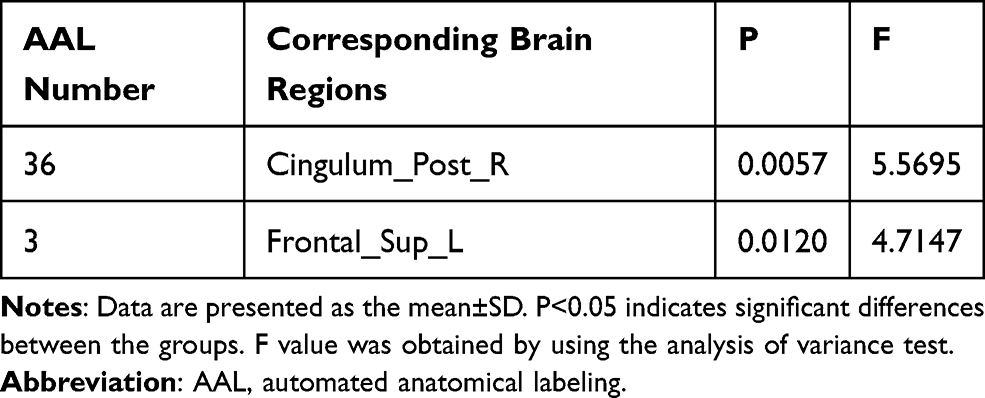 |
Table 4 Brain Regions with Significant Degree Centrality Differences Between Groups |
 |
Figure 3 Differences in nodal local efficiency and degree centrality (DC) among subjective cognitive decline with APOEε4 (SCD+), subjective cognitive decline without APOEε4 (SCD−) and normal control without APOEε4 (NC−). The statistical criterion for groups was set at P<0.05, uncorrected. Abbreviations: SFGdor. L, superior frontal gyrus, dorsolateral, left; SOG.L, superior occipital gyrus, left; PUT.L, lenticular nucleus, putamen, left; PUT.R, lenticular nucleus, putamen, right; PCG.R, posterior cingulate gyrus, right. |
Discussion
In seeking to understand the mechanism and treatment of AD, current research is heavily focused on the early stage of the disease.23 Thus, patients with SCD ability are valuable individuals looking for preclinical AD.24 This study investigated whether there are rsFC changes in SCD patients with the APOEε4 allele in terms of whole brain network characteristics and intracerebral node characteristics. The effect of APOEε4 on the functional brain network of SCD patients was examined. We utilized graph theory-based analysis to determine whether the SCD+ group had similar rsFC changes to MCI and AD relative to the SCD− and NC− groups. In support of our hypotheses, the three groups each presented with small-world properties; however, the SCD+ group had significantly lower LP than the SCD− and NC− groups but higher global efficiency than the NC− group, with compensatory information transfer speed increase and enhanced integration capability. The SCD+ group rsFC was highly heterogeneous at intracerebral nodes but showed similar abnormal DMN region connectivity to MCI or AD (higher at the level of the posterior cingulate cortex and lower in the dorsolateral superior frontal gyrus), together with compensatory effects at the bilateral putamen and left superior occipital gyrus.
At the whole brain network level, the SCD+, SCD−, and NC− groups all had small-world property. Among each of the whole brain network characteristics, statistically significant indicators included λ (significantly lower in the SCD+ group compared to the SCD− and NC− groups), global efficiency (higher in the SCD+ group compared to the NC group), and assortativity (lower in the SCD+ group compared to the SCD− and NC− groups). The λ was used to measure global information transmission capability of the network: a lower λ indicated higher information transfer speed between network nodes. In SCD+ patients, an increase in global efficiency value indicates enhanced brain network integration. Furthermore, lower assortativity suggests few similarities in the brain network connection of SCD+ patients. These results demonstrate that SCD occurs in the mild neuron injury stage with sufficient functional compensation,25 which is consistent with previous results.26 However, due to differences in study samples, our results are inconsistent with those of Xu et al.27 Notably, SCD patients were not further stratified into APOEε4 carriers or non-carriers Xu et al,27 which may explain the discrepancy. Indeed, the presence or absence of the APOEε4 allele may affect disease progression. APOEε4 disrupts nerve signals in specific regions by affecting cholesterol metabolism, Aβ phagocytosis, neurotrophic support, and synaptic pruning of astrocytes, and early brain activities adapt to demand and induce recombination of the brain rsFC.
When comparing intracephalic node characteristics in the functional network between the SCD+ group and the SCD− and NC− groups, the SCD+ group had lower local efficiency at the level of the left superior occipital gyrus node, part of the anterior lateral occipital complex (aLOC) that has been implicated in the primary sensory processing and coding of object shape.28 Koolschijn et al29 increased glutamic acid and subsequently reduced γ-aminobutyric acid via transcranial direct current stimulation (tDCS) to quantify the concentration of two key metabolites in this region using magnetic resonance spectroscopy (MRS). By recording the reduction of γ-aminobutyric acid and the increase of glutamic acid in aLOC before and after tDCS, Koolschijn et al29 found that the excitation/inhibition imbalance in the aLOC region damages hippocampal memory discrimination. Interestingly, the SCD+ group had lower local efficiency at the level of the superior occipital gyrus, and SCD patients with the APOEε4 allele showed significantly lower local efficiency than SCD patients and NCs. This reduction in local efficiency resulted in lower information transmission capability between network nodes and broke the original excitement/inhibition balance in the aLOC region, affecting hippocampal memory discrimination and causing memory decline.
The efficiency at the posterior cingulate cortex node was increased in the SCD+ group. As part of posterior medial cortex, the posterior cingulate cortex has high connectivity anatomically and a high basal metabolic rate; it is a central component of the DMN.30 The posterior cingulate cortex has a strong connectivity with DMN and connects with the frontal-parietal region to mediate cognition and the parahippocampal gyrus to aid in memory formation. In a study on directed functional connectivity, Yu et al31 report enhanced directed connectivity from the whole brain to the posterior cingulate cortex in AD and MCI patients. Notably, patients in the SCD+ group presented with higher local node efficiency and stronger information transmission capabilities between network nodes, which may affect local metabolism in the presence of the APOEε4 allele. To overcome the inefficiency of the network, the brain compensatively increases its neural activities to meet demand. The posterior cingulate cortex affects connectivity in the DMN, frontal-parietal region, and parahippocampal gyrus. Indeed, in early neuron injury models, inter-node information requires compensatory enhancement to maintain cognitive function.
The local efficiency at the level of the putamen was higher in the SCD+ group. Sekutowicz et al32 observed that the activation of the right putamen during cognitive task switching was associated with bistable perceptual switching. Furthermore, Durstewitz et al33 reported that basal ganglion activity increased cognitive flexibility through selective and dynamic gating functions and accelerated the renewal of the prefrontal cortex representation. Finally, in a study on amnestic MCI, Cai et al34 found that the FC between the putamen and hippocampus was reduced, and amnestic MCI rapidly progressed into AD. In SCD patients with the APOEε4 allele, prefrontal lobe characteristics show compensatory alterations with enhanced local efficiency of bilateral putamen.
DMN is roughly divided into three parts: dorsal and ventral prefrontal cortex, posterior cingulate cortex, and adjacent precuneus plus lateral parietal cortex.35 In SCD patients, DMN rsFC appears heterogeneous.16,36–42 Davis et al43 proposed that functional compensation mechanisms of aging shift and aging actually reduces inactivation of the posterior midline cortex, but increases inactivation of the medial frontal cortex. Our study is consistent with this model, as rsFC was increased in the posterior cingulate cortex but decreased in the dorsolateral superior frontal gyrus. Furthermore, in complex, non-linear dynamic diseases, temporal and spatial changes in the cross-brain network may gradually evolve from the “in-network stage” to the “whole network stage”, and finally to the “multi-network compensation stage”.15
rsFC abnormalities in the SCD+ group were similar to those of MCI and AD patients, as manifested in dysfunctional brain regions; however, local efficiency and connectivity also increased or decreased, respectively, as did the compensatory function between each node and the whole brain network before SCD+ progressed to MCI or AD. rsFC abnormalities in the SCD+ group were also markedly more severe than those in the SCD− and NC groups, which might be correlated to APOEε4 presence. Staffaroni et al44 found no notable differences in rsFC longitudinal trajectory at baseline or DMN in the subjective memory of patients with APOEε4. However, Chiesa et al15 reported that the increase of rsFC was slower at the levels of the frontal and prefrontal lobes in subjective memory complaints with the APOEε4 allele. Here, we report that rsFC was altered slightly in the SCD− group, indicating that SCD patients may have a minor nerve injury. However, the degree of rsFC change in the SCD+ group was even greater and associated with the APOEε4 allele in cholesterol metabolism and Aβ phagocytosis of astrocytes in the brain, and the exacerbation of Aβ deposition- and tau-induced neurodegeneration and atrophy to aggravate nerve injury.
APOEε4 affects the functional brain network in patients with SCD. The SCD+ group demonstrated similar changes in compensatory whole brain network activity and intracerebral node characteristics in patients with MCI and AD dementia. Clinically, Hong et al45 compared baseline characteristics between stable and progressive SCD to predict the relevant factors for SCD progression: presence of the APOEε4 allele was one of the strongest predictors of the transformation from SCD to objective cognitive impairment. Dik et al46 also found that in elderly individuals, the effects of SCD and the presence of the APOEε4 allele were additive, and the cognitive decline of subjects with both factors was twice that of subjects with one or neither. Furthermore, in a neuroimaging study, Striepens et al47 measured the volume of hippocampus, entorhinal cortex, and amygdala by structural MRI and found that the negative impact of APOEε4 on episodic memory and hippocampal volume supported SCD as the preclinical stage of AD. Finally, the longitudinal trajectory of DMN in SCD patients in a voxel study15 observed wide DMN FC changes at the levels of the frontal lobe, posterior lobe, and right hippocampus, but slow FC increases in the frontal lobe in APOEε4 carriers.13
In a cross-sectional study, the current experiment did not evaluate whether APOEε4-related changes in brain functions are directly associated with future occurrence of MCI or AD. Since there is currently no clear definition of SCD, SCD in this study was based on individual memory complaints, and represented the subjective memory complaint group (SMC) well, but not overall SCD.48 Since the ADNI database included fewer SCD patients who had neuropsychological assessment, CSF biomarkers, APOE genotyping information, and rs-fMRI data, our sample size was relatively small, which affected the reliability of the results. In future studies, a larger sample size and stricter quality control standards should be used to improve the reliability of results. AD pathological markers used in this study were obtained from CSF but are still an indirect way to reflect AD pathology. Therefore, in future studies, the addition of live animal models and the confirmation with molecular imaging and molecular biology data will help to further research of the pathophysiological mechanism and changes in MRI indicators. Although there was no difference in neuropsychological assessment among groups in this study, future studies should include more detailed neuropsychological scores, such as anxiety scale.
In this study, graph theory was used to analyze rsFC changes in SCD patients with the APOEε4 allele and determine whether APOEε4 affects the functional brain network of SCD patients. Although the rsFC was highly heterogeneous, we found that SCD patients with the APOEε4 allele demonstrate abnormal DMN connectivity and compensatory effects at the levels of the bilateral putamen and left superior occipital gyrus. Our results indicate that APOEε4 affects the functional brain network of patients with SCD, and the relationship between APOEε4 biomarkers and pathological cognitive decline has been reliably reported.49 The APOEε4 collection method is fast, noninvasive, and relatively low-cost,50 and the presence of the APOEε4 allele may be a tool to identify cognitive decline in SCD patients in clinical practice.
Conclusion
This study utilized graph theory to study the rsFC of SCD patients with APOEε4 in an effort to explore the effect of APOEε4 on functional brain networks of SCD patients. We found that the SCD+ group had increased compensatory information transfer speed and enhanced integration capability, with a lower AUC of LP, λ, and assortativity, but higher global efficiency. The SCD+ group also has high heterogeneity in intracerebral node characteristics, mainly in the DMN, left superior occipital gyrus, and bilateral putamen. Therefore, we believe that APOEε4 effects the functional brain network in patients with SCD and may be used as a potential indicator of SCD progress.
Acknowledgments
This work was partially supported by the National Natural Science Foundation of China (Grant No. 81973922); Dongguan Science and Technology of Social Development Program (Grant No. 202050715046225); Subject of Shenzhen Science and Technology Innovation Commission (Grant No. JCYJ20190809151013581).
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC; Johnson & Johnson Pharmaceutical Research & Development LLC; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
We thank LetPub (www.letpub.com) for linguistic assistance and pre-submission expert review.
Disclosure
The authors report no conflicts of interest in this work, and the data accessed comply with relevant data protection and privacy regulations.
References
1. Lane CA, Hardy J, Schott JM. Alzheimer’s disease. Eur J Neurol. 2018;25(1):59–70. doi:10.1111/ene.13439
2. Hao N, Wang Z, Liu P, et al. Acoustofluidic multimodal diagnostic system for Alzheimer’s disease. Biosens Bioelectron. 2021;196:113730. doi:10.1016/j.bios.2021.113730
3. Scheltens P, Blennow K, Breteler MMB, et al. Alzheimer’s disease. Lancet. 2016;388(10043):505–517. doi:10.1016/S0140-6736(15)01124-1
4. Jessen F, Amariglio RE, Buckley RF, et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020;19(3):271–278. doi:10.1016/S1474-4422(19)30368-0
5. Mitchell AJ, Beaumont H, Ferguson D, Yadegarfar M, Stubbs B. Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: meta-analysis. Acta Psychiatr Scand. 2014;130(6):439–451. doi:10.1111/acps.12336
6. Serrano-Pozo A, Das S, Hyman BT. APOE and Alzheimer’s disease: advances in genetics, pathophysiology, and therapeutic approaches. Lancet Neurol. 2021;20(1):68–80. doi:10.1016/S1474-4422(20)30412-9
7. Yamazaki Y, Zhao N, Caulfield TR, Liu CC, Bu G. Apolipoprotein E and Alzheimer disease: pathobiology and targeting strategies. Nat Rev Neurol. 2019;15(9):501–518.
8. Farrer LA, Cupples LA, Haines JL, et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer disease meta analysis consortium. JAMA. 1997;278(16):1349–1356. doi:10.1001/jama.1997.03550160069041
9. Neu SC, Pa J, Kukull W, et al. Apolipoprotein E genotype and sex risk factors for Alzheimer disease: a meta-analysis. JAMA Neurol. 2017;74(10):1178–1189. doi:10.1001/jamaneurol.2017.2188
10. Genin E, Hannequin D, Wallon D, et al. APOE and Alzheimer disease: a major gene with semi-dominant inheritance. Mol Psychiatry. 2011;16(9):903–907. doi:10.1038/mp.2011.52
11. Scarabino D, Broggio E, Gambina G, Maida C, Gaudio MR, Corbo RM. Apolipoprotein E genotypes and plasma levels in mild cognitive impairment conversion to Alzheimer’s disease: a follow-up study. Am J Med Genet B Neuropsychiatr Genet. 2016;171(8):1131–1138. doi:10.1002/ajmg.b.32495
12. Tschanz JT, Welsh-Bohmer KA, Lyketsos CG, et al. Conversion to dementia from mild cognitive disorder: the Cache County study. Neurology. 2006;67(2):229–234. doi:10.1212/01.wnl.0000224748.48011.84
13. Medaglia JD. Graph theoretic analysis of resting state functional MR imaging. Neuroimaging Clin N Am. 2017;27(4):593–607. doi:10.1016/j.nic.2017.06.008
14. Sheline YI, Morris JC, Snyder AZ, et al. APOE4 allele disrupts resting state fMRI connectivity in the absence of amyloid plaques or decreased CSF Aβ42. J Neurosci. 2010;30(50):17035–17040. doi:10.1523/JNEUROSCI.3987-10.2010
15. Chiesa PA, Cavedo E, Vergallo A, et al. Differential default mode network trajectories in asymptomatic individuals at risk for Alzheimer’s disease. Alzheimers Dement. 2019;15(7):940–950. doi:10.1016/j.jalz.2019.03.006
16. Dong C, Liu T, Wen W, et al. Altered functional connectivity strength in informant-reported subjective cognitive decline: a resting-state functional magnetic resonance imaging study. Alzheimers Dement. 2018;10:688–697.
17. Veitch DP, Weiner MW, Aisen PS, et al. Understanding disease progression and improving Alzheimer’s disease clinical trials: recent highlights from the Alzheimer’s disease neuroimaging initiative. Alzheimers Dement. 2019;15(1):106–152. doi:10.1016/j.jalz.2018.08.005
18. Jia X-Z, Wang J, Sun H-Y, et al. RESTplus: an improved toolkit for resting-state functional magnetic resonance imaging data processing. Sci Bull. 2019;64(14):953–954. doi:10.1016/j.scib.2019.05.008
19. Tzourio-Mazoyer N, Landeau B, Papathanassiou D, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. NeuroImage. 2002;15(1):273–289. doi:10.1006/nimg.2001.0978
20. Wang J, Wang X, Xia M, Liao X, Evans A, He Y. GRETNA: a graph theoretical network analysis toolbox for imaging connectomics. Front Hum Neurosci. 2015;9:386. doi:10.3389/fnhum.2015.00386
21. Achard S, Bullmore E. Efficiency and cost of economical brain functional networks. PLoS Comput Biol. 2007;3(2):e17. doi:10.1371/journal.pcbi.0030017
22. Rubinov M, Sporns O. Complex network measures of brain connectivity: uses and interpretations. NeuroImage. 2010;52(3):1059–1069. doi:10.1016/j.neuroimage.2009.10.003
23. Bessi V, Mazzeo S, Padiglioni S, et al. From subjective cognitive decline to Alzheimer’s disease: the predictive role of neuropsychological Assessment, personality traits, and cognitive reserve. A 7-year follow-up study. J Alzheimers Dis. 2018;63(4):1523–1535. doi:10.3233/JAD-171180
24. Pike KE, Cavuoto MG, Li L, Wright BJ, Kinsella GJ. Subjective cognitive decline: level of risk for future dementia and mild cognitive impairment, a meta-analysis of longitudinal studies. Neuropsychol Rev. 2021. doi:10.1007/s11065-021-09522-3
25. Sperling RA, Jack CR
26. Chen H, Sheng X, Luo C, et al. The compensatory phenomenon of the functional connectome related to pathological biomarkers in individuals with subjective cognitive decline. Transl Neurodegener. 2020;9(1):21. doi:10.1186/s40035-020-00201-6
27. Xu X, Li W, Tao M, et al. Effective and accurate diagnosis of subjective cognitive decline based on functional connection and graph theory view. Front Neurosci. 2020;14:577887. doi:10.3389/fnins.2020.577887
28. Barron HC, Vogels TP, Emir UE, et al. Unmasking latent inhibitory connections in human cortex to reveal dormant cortical memories. Neuron. 2016;90(1):191–203. doi:10.1016/j.neuron.2016.02.031
29. Koolschijn RS, Emir UE, Pantelides AC, Nili H, Behrens TEJ, Barron HC. The hippocampus and neocortical inhibitory engrams protect against memory interference. Neuron. 2019;101(3):528–541.e526. doi:10.1016/j.neuron.2018.11.042
30. Leech R, Sharp DJ. The role of the posterior cingulate cortex in cognition and disease. Brain. 2014;137(Pt 1):12–32. doi:10.1093/brain/awt162
31. Yu E, Liao Z, Mao D, et al. Directed functional connectivity of posterior cingulate cortex and whole brain in alzheimer’s disease and mild cognitive impairment. Curr Alzheimer Res. 2017;14(6):628–635. doi:10.2174/1567205013666161201201000
32. Sekutowicz M, Schmack K, Steimke R, et al. Striatal activation as a neural link between cognitive and perceptual flexibility. NeuroImage. 2016;141:393–398. doi:10.1016/j.neuroimage.2016.07.046
33. Durstewitz D, Seamans JK. The dual-state theory of prefrontal cortex dopamine function with relevance to catechol-o-methyltransferase genotypes and schizophrenia. Biol Psychiatry. 2008;64(9):739–749. doi:10.1016/j.biopsych.2008.05.015
34. Cai S, Chong T, Peng Y, et al. Altered functional brain networks in amnestic mild cognitive impairment: a resting-state fMRI study. Brain Imaging Behav. 2017;11(3):619–631. doi:10.1007/s11682-016-9539-0
35. Raichle ME. The brain’s default mode network. Annu Rev Neurosci. 2015;38(1):433–447. doi:10.1146/annurev-neuro-071013-014030
36. Dillen KNH, Jacobs HIL, Kukolja J, et al. Functional disintegration of the default mode network in prodromal Alzheimer’s disease. J Alzheimers Dis. 2017;59(1):169–187. doi:10.3233/JAD-161120
37. Wang Y, Risacher SL, West JD, et al. Altered default mode network connectivity in older adults with cognitive complaints and amnestic mild cognitive impairment. J Alzheimers Dis. 2013;35(4):751–760. doi:10.3233/JAD-130080
38. Yasuno F, Kazui H, Yamamoto A, et al. Resting-state synchrony between the retrosplenial cortex and anterior medial cortical structures relates to memory complaints in subjective cognitive impairment. Neurobiol Aging. 2015;36(6):2145–2152. doi:10.1016/j.neurobiolaging.2015.03.006
39. Viviano RP, Hayes JM, Pruitt PJ, et al. Aberrant memory system connectivity and working memory performance in subjective cognitive decline. NeuroImage. 2019;185:556–564. doi:10.1016/j.neuroimage.2018.10.015
40. Hafkemeijer A, Altmann-Schneider I, Oleksik AM, et al. Increased functional connectivity and brain atrophy in elderly with subjective memory complaints. Brain Connect. 2013;3(4):353–362. doi:10.1089/brain.2013.0144
41. Verfaillie SCJ, Pichet Binette A, Vachon-Presseau E, et al. Subjective cognitive decline is associated with altered default mode network connectivity in individuals with a family history of Alzheimer’s disease. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3(5):463–472. doi:10.1016/j.bpsc.2017.11.012
42. Dillen KNH, Jacobs HIL, Kukolja J, et al. Aberrant functional connectivity differentiates retrosplenial cortex from posterior cingulate cortex in prodromal Alzheimer’s disease. Neurobiol Aging. 2016;44:114–126. doi:10.1016/j.neurobiolaging.2016.04.010
43. Davis SW, Dennis NA, Daselaar SM, Fleck MS, Cabeza R. Que PASA? The posterior-anterior shift in aging. Cereb Cortex. 2008;18(5):1201–1209.
44. Staffaroni AM, Brown JA, Casaletto KB, et al. The longitudinal trajectory of default mode network connectivity in healthy older adults varies as a function of age and is associated with changes in episodic memory and processing speed. J Neurosci. 2018;38(11):2809–2817. doi:10.1523/JNEUROSCI.3067-17.2018
45. Hong YJ, Yoon B, Shim YS, et al. Predictors of clinical progression of subjective memory impairment in elderly subjects: data from the Clinical Research Centers for Dementia of South Korea (CREDOS). Dement Geriatr Cogn Disord. 2015;40(3–4):158–165. doi:10.1159/000430807
46. Dik MG, Jonker C, Comijs HC, et al. Memory complaints and APOE-epsilon4 accelerate cognitive decline in cognitively normal elderly. Neurology. 2001;57(12):2217–2222. doi:10.1212/WNL.57.12.2217
47. Striepens N, Scheef L, Wind A, et al. Interaction effects of subjective memory impairment and ApoE4 genotype on episodic memory and hippocampal volume. Psychol Med. 2011;41(9):1997–2006. doi:10.1017/S0033291711000067
48. Jessen F, Amariglio RE, van Boxtel M, et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014;10(6):844–852. doi:10.1016/j.jalz.2014.01.001
49. Allan CL, Ebmeier KP. The influence of ApoE4 on clinical progression of dementia: a meta-analysis. Int J Geriatr Psychiatry. 2011;26(5):520–526. doi:10.1002/gps.2559
50. Ali JI, Smart CM, Gawryluk JR. Subjective cognitive decline and APOE varepsilon4: a systematic review. J Alzheimers Dis. 2018;65(1):303–320. doi:10.3233/JAD-180248
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.