")
Back to Journals » International Journal of General Medicine » Volume 15
Effect of Altitude on Hemoglobin and Red Blood Cell Indices in Adults in Different Regions of Saudi Arabia
Authors Alkhaldy HY , Awan ZA , Abouzaid AA, Elbahaey HM, Al Amoudi SM, Shehata SF, Saboor M
Received 12 January 2022
Accepted for publication 15 March 2022
Published 31 March 2022 Volume 2022:15 Pages 3559—3565
DOI https://doi.org/10.2147/IJGM.S358139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Husain Y Alkhaldy,1,2 Zuhier A Awan,3,4 Ahmed A Abouzaid,4,5 Hossameldin M Elbahaey,4,6 Saeed M Al Amoudi,5 Shehata F Shehata,7,8 Muhammad Saboor9,10
1Department of Internal Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2Research Center for Advanced Materials Science, King Khalid University, Abha, Saudi Arabia; 3Department of Clinical Biochemistry, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Clinical Pathology, Al-Borg Medical Laboratories, Jeddah, Saudi Arabia; 5Department of Medical Biochemistry, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 6Clinical Pathology Department, Suez Canal University, Ismailia Governorate, Egypt; 7Department of Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia; 8High Institute of Public Health, Alexandria University, Alexandria, Egypt; 9Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 10Medical Research Center, Jazan University, Jazan, Saudi Arabia
Correspondence: Husain Y Alkhaldy, Department of internal medicine, College of Medicine, King Khalid University, P.O.BOX 641, Abha, 61421, Saudi Arabia, Tel +966 72417578 ; +966 5999-15-567, Fax +966 72418111, Email [email protected] Muhammad Saboor, Department of Medical Laboratory Technology, Faculty of Applied Medical Science, Jazan University, Jazan, Saudi Arabia, Tel +966 54 495 9029, Email [email protected]
Purpose: Complete blood count (CBC) is a commonly used blood test for health checks. This study was conducted to compare CBC from two different altitudes and from sea-level populations in order to suggest correction factor for altitude-related increment on the hemoglobin and red blood cell indices.
Patients and Methods: In this retrospective lab records study, large datasets of CBCs over 5-year period were screened from three different regions of Saudi Arabia, Jeddah (a coastal city), Taif City located at 1879 m above sea level, and Abha City at located 2270 m above sea level. Descriptive analysis and significance testing of the CBC variables at different altitude were compared.
Results: A total of 57,059 participants were included for final analysis. Mean hemoglobin (Hb) concentration (g/dL) was 14.81 for men and 13.77 for women at sea level, whereas Hb concentrations were 15.35 and 14.19 for men and women residing at Taif City, respectively, and 15.40 and 14.71 for men and women at Abha City, respectively. Hemoglobin and other red cell indices were significantly different among men and women across different altitude, except for mean corpuscular volume (MCV). The MCV 95th percentile range was lower at sea level and both altitudes as compared to current reference range (76– 91 fL vs 81– 98 fL).
Conclusion: Although altitude-associated increment in Hb concentration was evident in both men and women, it was lower than as suggested by World Health Organization and Centers for Disease and Control. Results of this study can also be used to derive new CBC reference intervals for Saudi residents living at high altitude. A correction factor (ΔHb) of 0.30 g/dL per 1000 m altitude is suggested to be used in adult population living at high altitudes in Saudi Arabia which should help better define anemia and polycythemia at altitude.
Keywords: high altitude, reference interval, CBC
Introduction
Complete blood count (CBC) is one of the most important blood tests used to evaluate health status and diseases. Determining a reference interval for CBC is an essential prerequisite to correctly interpret the test’s result. Statistically speaking, two standard deviations (SD) of the mean value of a representative sample population, ie, the central 95% range of results, can be used to define the ideal reference range.1 In principle, reference range values are typically derived from large cohorts of a healthy population. Hemoglobin concentration (Hb), red cell count, and red blood cell (RBC)-derived indices are affected by both physiological and pathological conditions. Well-known physiological determinants of blood elements include age, gender, ethnicity, and altitude. At high altitude, hypoxia-induced erythropoietic drive results in erythrocytosis and an increase in hemoglobin concentration and hematocrit,2 whereas plasma volume decreases at high altitude.3 The World Health Organization (WHO) and Centers for diseases and Control (CDC) have suggested reference intervals derived mainly from studies conducted in the Caucasian population.4,5 It has also suggested a correction factor for hemoglobin when defining anemia at different altitude, which is mainly derived from studies conducted in the highland of South America. However, it is problematic to use unified correction factor because various studies have shown that the relationship between Hb and altitude is not linear, and varies among geographical locations and races; this, in turn, leads to overestimating pathological conditions like anemia.6–8 Moreover, there is no sufficient information about correction factors of RBCs and other derived indices, ie, mean cell volume (MCV), mean cell hemoglobin (MCH), and mean cell hemoglobin concentration (MCHC). Hence, defining a reference range should be based on large epidemiological local studies.
Saudi Arabia is a large country that occupies most of the Arabian Peninsula. Its land includes a desert terrain of central and northern provinces, Coastal Arabian Gulf and Western Red Sea, and Sarawat highlands that stretch across the western border. A moderately high altitude Sarawat highland is heavily inhabited by both rural and urban communities like Taif (1890 m), Aseer highlands (2000–3000 m), Albaha (2270 m) and Faifa (1428 m). Due to high altitude associated-erythrocytosis, dwellers at high altitude are expected to show higher Hb concentration, RBC count, and different values of red cell-derived indices necessitating a local based reference range. The change in such reference intervals is expected to be coupled with a change of the cutoff values that define two commonly evaluated pathological states anemia and polycythemia. To the best of our knowledge, there have been no epidemiological studies conducted to estimate the reference intervals of blood counts in high-altitude Saudi Arabia. Hence, this study was conducted to determine precise reference intervals of CBC parameters for high altitude Saudi Arabia.
Materials and Methods
This was a comparative retrospective lab records review study. The study protocol was approved by the ethical and research committee of King Khalid University, Abha, Saudi Arabia [(ECM#2020-0905)–(HAPO–06–B–001)]. For this study, being retrospective in nature, informed consent was waived off by the Institutional Review Board. The study was conducted according to the Declaration of Helsinki.
CBC results over 5-years (2014–2019) for people, aged 18–60 years, of both sexes who came to a commercial lab (Al-Borg laboratory) for blood testing were selected from three geographical areas; Jeddah, a large coastal city with more than 4 million population, Taif City (1879 m altitude) and from Abha City (2270 m altitude).
Participants who had available full panel of tests at the time of CBC testing were screened. Tests include CBC, kidney profile (urea, creatinine), liver profile (alanine aminotransferase, aspartate aminotransferase, total bilirubin, direct bilirubin), lipid profile (cholesterol, high-density lipoprotein, low density lipoprotein, triglyceride), thyroid function tests (thyroid stimulating hormone, T4), and a fasting blood glucose level or Hb A1c.
Exclusion Criteria
Participants with abnormalities in their blood glucose level, lipid, kidney or liver profiles per the established cutoff values were excluded from the analysis. Participants were also excluded if they had abnormal white blood cell (WBC), Hb, and platelet count according to the used cutoff.
Hemoglobin inclusion was set at Hb more than 12 and 13 g/dL for women and men respectively. To account for altitude effect, participants from the two altitudes were also analyzed using a higher cutoff values for women (12.5 g/dL) and men (13.5 g/dL) and the difference between the two inclusion methods was analyzed. MCV below 75 fL were also excluded in order to minimize the effect of undiagnosed latent iron deficiency or thalassemia trait in the obtained results. Red cell distribution width (RDW) more than 16 were also excluded to minimize the effect of any undiagnosed occult micronutrient deficiencies.
Blood Collection and Laboratory Analysis
The lab protocols are unified throughout different branches of the laboratory using Sysmex XS-1000i/ XS-500i automated analyzers (Sysmex Corporation, Kobe, Japan). The analyzers are calibrated and maintained following the manufacturer guidelines and accreditation standards. Controls are tested daily before running the patients samples.
Data Analysis
The participants’ data were de-identified for any personal information before importing to excel datasheet. After data were extracted, it was revised, coded, and fed to statistical software IBM SPSS version 22 (SPSS, Inc. Chicago, IL). Descriptive analysis, based on frequency and percent distribution, was performed using participants’ residence area, age, and gender. Normal distribution assessment was applied for all scale parameters. For all CBC parameters, descriptive analyses using mean with its 95% confidence interval, median, range, and percentiles (2.5th and 97.5th) were used to assess the normal population range. Any extreme value was minorized using a larger value winsorization method. Student’s t-test was used for comparison of the studied continuous variables among different groups. All statistical analysis was done using two-tailed tests and significance was set at p value <0.05.
Results
More than 120,000 participants were screened. After applying the age and lab exclusion criteria, 46,012 individuals (F: 27,559 and M:18,453) from Jeddah City, 5831 (F: 3656 and M: 2175) from Abha City, and 5216 (F: 3193 and M: 2023) from Taif City were included in the final analysis. The 5% trimmed mean Hb (g/dL) concentration was 14.81 ± 1.13 and 13.77 ± 1.32 for men and women at Jeddah City (sea level), 15.35 ± 1.28 and 14.19 ± 1.37 for men and women at Taif City (1879 m), and 15.40±1.25 and 14.71 ± 1.50 for men and women at Abha City (2270 m), respectively (Table 1). The effect of using the same cutoff values on the mean Hb concentration was modest and restricted to the male population (Table 2).
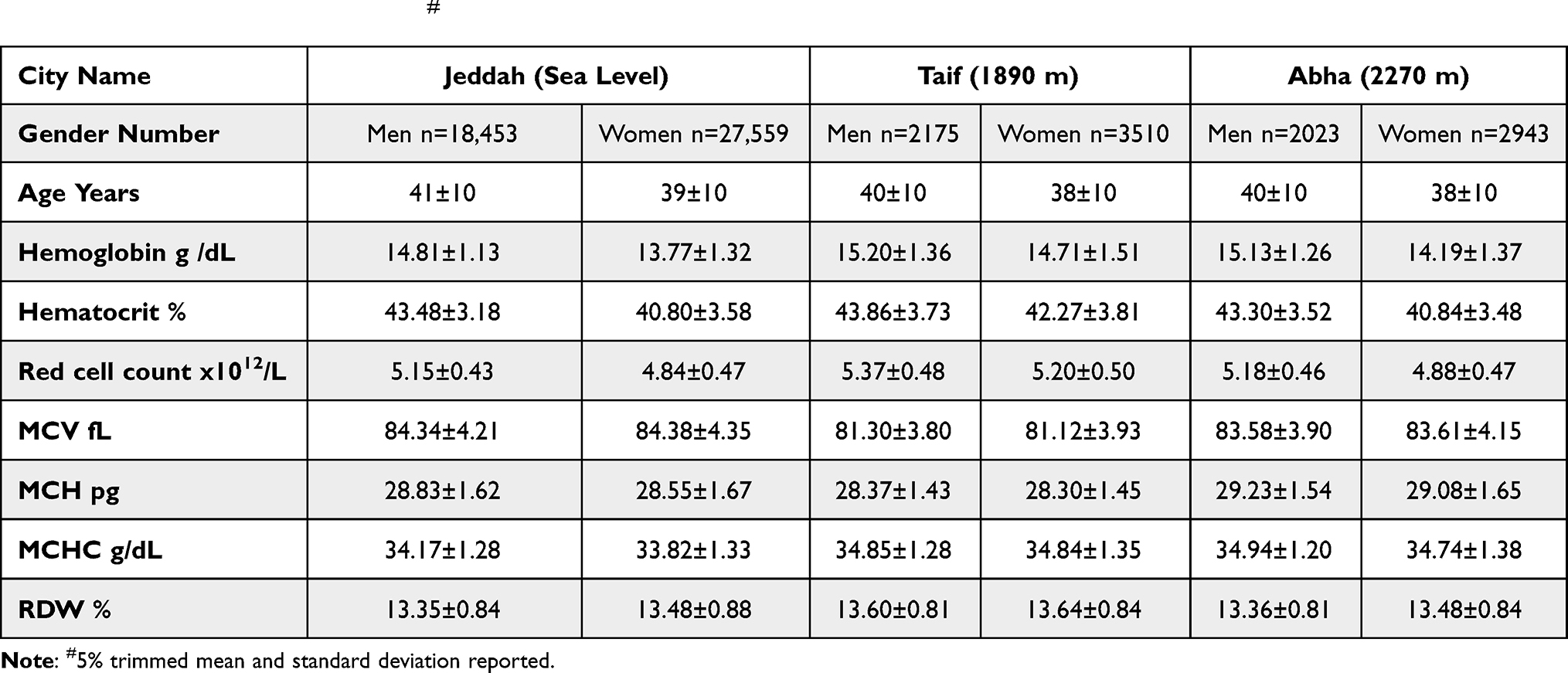 |
Table 1 Descriptive Analysis of CBC Parameters at the Studied Three Geographical Areas Using 12.5 g/dL for Women and 13.5 g/dL for Men as Normal Reference Level# |
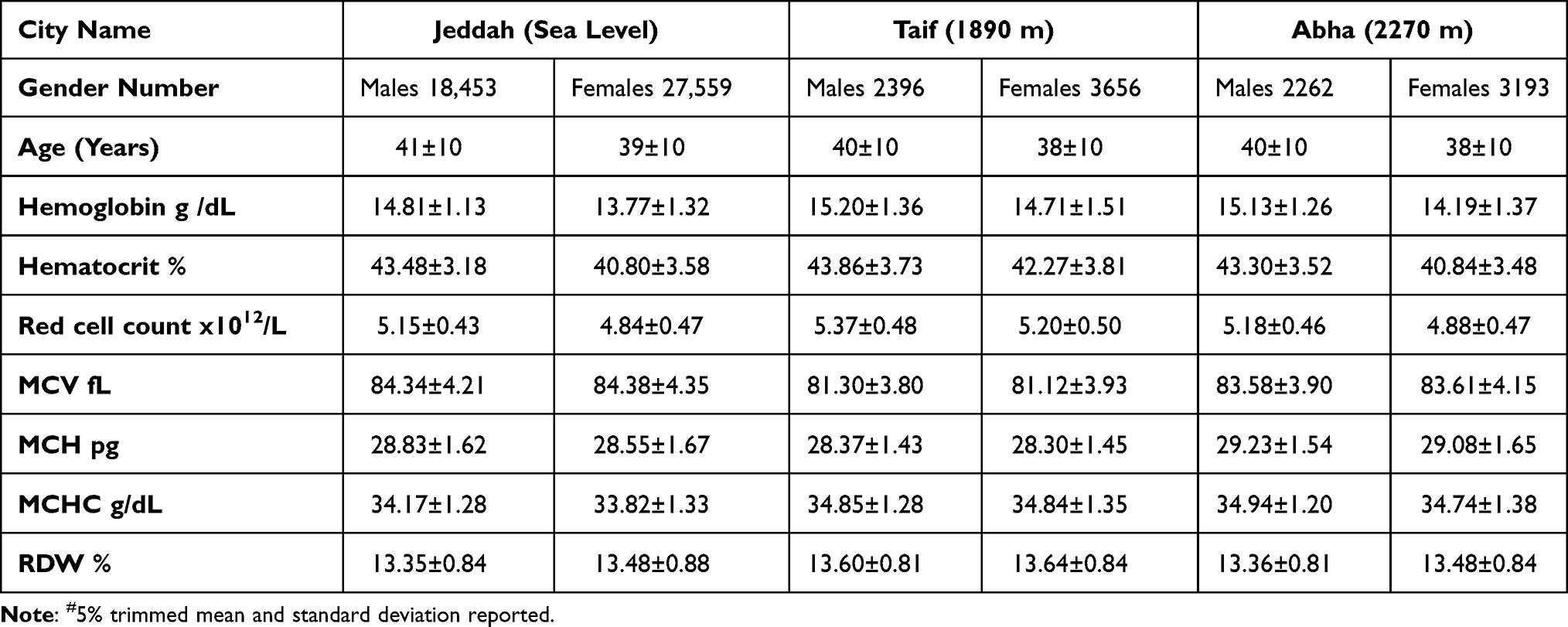 |
Table 2 CBC Parameters at Sea Level and Both Altitudes Using 12 g/dL for Women and 13 g/dL for Men as Lower Normal Reference Level# |
While the 2.5th percentile values of Hb concentration were affected by the cutoff value used for inclusion, the 97.5th percentile values of Hb concentration showed higher values at both altitudes as compared to sea level and to the current reference range, suggesting the need for updating the current reference range at high altitudes (Table 3). At the highest altitude (Abha City), the Hb increment (Δ Hb) was more prominent in women (0.94) g /dL than in men (0.59 g/dL). The 2.5th and 95th percentile range (95th percentile range) of Hb concentration using two different cutoff values for inclusion are shown in Supplementary Table 1.
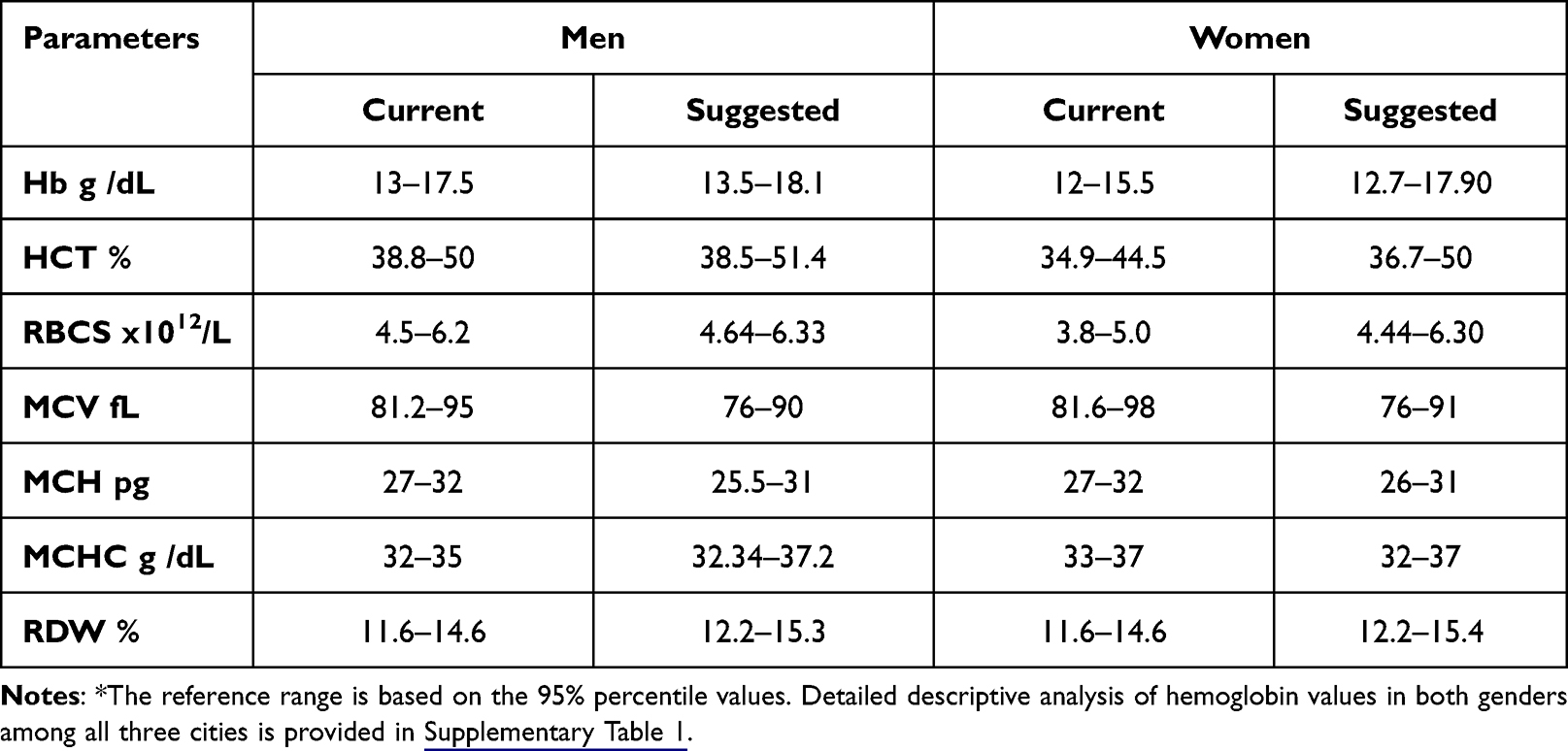 |
Table 3 The Proposed Update to the Currently Utilized Range According to Suggestions from Our Study* |
The difference in the Hb concentration, RBCs, and derived indices, except MCV, were significantly different between genders at the same altitude and between the same gender at different cities (p value <0.001 for all comparisons).
The mean value of MCV and the 95th percentile range (76–91 fL) were lower as compared to current reference range (Tables 1–3). The mean values of MCV were not significantly different between men and women subjects or between cities. However, there was a trend toward significant lower MCV at Abha as compared to Taif and Jeddah (p value = 0.06). Analysis per age groups, young (18–40) and middle aged (41–60), showed no significant age-related difference (Supplementary Tables 2 and 3).
Discussion
The precise interpretation of CBC of individuals residing at high altitude is a common dilemma for health practitioners, especially for results at the borders of the reference intervals, and how to define anemia and polycythemia.7 This study had two main objectives, first to compare altitude-associated effect on CBC between sea-level inhabitants and altitude population and secondly to compare the CBC results with other regions and population across the world. This study discusses the disparity in Hb, RBC count, and red cell indices at high altitude as compared to sea level and proposes a locally derived altitude-associated Hb correction factor and newly determined reference intervals for the local population.
To overcome the unavailability of the precise reference range, WHO and CDC have suggested applying a correction factor for different altitudes to correctly define anemia.4,9,10 However, many researchers have shown that altitude-associated increase in Hb is not linear and varies geographically and between different races – with the highest increase in the Andes compared to others.6–8 This racial and geographical difference was hypothesized due to the recent human inhabitation of South America as compared with the old world, Asia, and Africa. In general, the South American highlanders show higher Hb concentration as compared with Asian and African highlanders.11
The Sarawat highlands of nowadays Saudi Arabia has been inhabited for many thousands years. The inhabited areas are usually moderately high, 1500–3000 m above sea level. The mean Hb concentration at the studied two altitudes was found to be 15.35–15.40 g/dL in men and 14.19–14.71 g/dL in women, respectively, compared with 14.81 g/dL and 13.77 g/dL for men and women, respectively, at sea level. This change in Hb concentration (Δ Hb) is translated into 0.30–0.47 g/dL per 1000 m altitude. A variable Δ Hb has been reported worldwide up to 1.05 g/dL/1000 m altitude. At high altitude, the Saudi population has less mean Hb compared to European and North and South Americans yet more than the Chinese population.6 At Asmara, capital of Eritrea, which is at an altitude similar to that of Abha City, the mean Hb for men was found to be 15.4 g/dL, which is similar to what we reported for men at Abha; whereas the Eritrean women have slightly higher mean hemoglobin than that of women at Abha (14.9 versus 14.71 g/dL). It is worth mentioning that the study of Asmara population had a smaller sample and used a different hematology analyzer (Beckman Coulter).12 In conclusion, Saudi population seems well adapted to altitude with results more comparable to similarly inhabited altitude areas in nearby African Horn and Asia.
The WHO and CDC suggested correction factors for different altitudes were meant to help correctly define anemia.4,9,10 However, there is no such correction factor for the upper limit, ie, polycythemia, leaving the epidemiological estimation of reference intervals the only applicable method. The 95th percentile values of Hb concentration at Abha City are 18.1 g/dL and 17.9 g/dL for men and women, respectively. Hence, usage of the current reference intervals for Hb will label many individuals, otherwise normal, as polycythemic. The WHO diagnostic criteria for polycythemia vera (PV) state that if the level of Hb exceeds more than 16 g/dL and 16.5 g/dl and hematocrit values more than 48% and 49% for women and men, respectively, a case of polycythemia should be suspected.13 This definition does not account for altitude-related effects on Hb. Thus, it is expected that a significant number of people at high altitude may be evaluated for polycythemia vera unnecessarily. Thus, it is important to consider the altitude effect when interpreting the clinical picture and/ or apply diagnostic criteria that were not validated for high-altitude inhabitants.
MCV is the most useful and commonly used among the three RBC indices (MCV, MCH, and MCHC).14 Classification of anemia is mainly based on the RBC size, ie, MCV, whereas the MCH is closely related with an almost linear relationship with MCV.15 In this study, the MCV 95th percentile range is skewed toward lower value. This observation was noted across all studied three cities. The 2.5th percentile of MCV in the present study at both sea level and altitudes is 76 fL as compared to 81 fL in the currently used reference range at both sea level and high altitudes. The MCV obtained from central province Saudi Arabia adolescents' is 81fL ± 6.1 in keeping with what we reported here.16 The MCV value of 86 fL (75–94) has been reported in a study on adult Moroccan population.17 Most studies of the Middle East or Africa reported a similar MCV range and lower 2.5th percentile that is usually lower as compared to the western reported reference intervals, which suggests some racial impacts.18–22 Alpha thalassemia has been thought to be a contributing genetic effect to this noticed difference in Hb and MCV between White and African Americans.23 The MCV values at Abha (southern region) showed a trend toward significant lower MCV, as compared to Taif and Jeddah (western region). Southern region of Saudi Arabia has higher prevalence of thalassemia as compared to western region of Saudi Arabia.24 The inclusion criteria of (RDW <16) and (MCV > 75 fL) were meant to minimize the effect of undiagnosed occult deficiencies like iron deficiency anemia. Latent iron deficiency alone is an unlikely cause of this effect that is similarly evident in both studied men and women.
This study has some limitations. Chronic health conditions were indirectly excluded using the available lab tests since no health records of the participants were available. Habits known to affect Hb concentration like smoking were also not assessed. The status of micronutrients like iron, B12 and folate that might affect the CBC results was not assessed as well. Finally, although we think that the vast majority of the participants are Saudi citizens, the ethnicity of the participants was not directly assessed.
Conclusion
Only modest increase in Hb concentration was noted in this study, which could be explained by the moderately high altitude that is inhabited. The increment in Hb concentration (Δ Hb) was estimated at 0.3 g/dL/1000 m altitude. This correction can be used to update the current CBC reference range in order to better define anemia and polycythemia at high-altitude. The suggested update still needs to be validated at the local laboratories per quality standards. More studies are needed to further explore the nature and possible causes of the observed difference in the MCV range as compared to other populations.
Acknowledgments
We acknowledge the Research Center for Advanced Material Science (RCAMS), King Khalid University, Abha for supporting this study through a grant (Reference No. KKU/RCAMS/G0001-21). We want also to thank the administration of Al-Borg laboratories for providing the data and the facilitation of data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bertholf RL. Statistical methods for establishing and validating reference intervals. Lab Med. 2006;37(5):306–310. doi:10.1309/cbmhprfnlu1xa4xv
2. Azad P. Haddad G. Molecular basis of hypoxia-induced excessive erythrocytosis of high altitude. FASEB J. 2018;32:lb405.
3. Myhre LG, Dill DB, Hall FG, Brown DK. Blood volume changes during three-week residence at high altitude. Clin Chem. 1970;16(1):7–14. doi:10.1093/clinchem/16.1.7
4. Chan M; World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva: Switz World Heal Organ; 2011.
5. Hurtado A, Merino C, Delgado E. Influence of anoxemia on the hemopoietic activity. Arch Intern Med. 1945;75(5):284–323. doi:10.1001/archinte.1945.00210290007002
6. Gassmann M, Mairbäurl H, Livshits L, et al. The increase in hemoglobin concentration with altitude varies among human populations. Ann N Y Acad Sci. 2019;1450:204–220. doi:10.1111/nyas.14136
7. Gonzales GF, Fano D, Vasquez-Velasquez C. Diagnosis of anemia in populations at high altitudes. Rev Peru Med Exp Salud Publica. 2017;34(4):699–708. Catalan. doi:10.17843/rpmesp.2017.344.3208
8. Sharma AJ, Addo OY, Mei Z, Suchdev PS. Reexamination of hemoglobin adjustments to define anemia: altitude and smoking. Ann N Y Acad Sci. 2019;1450(1):190–203. doi:10.1111/nyas.14167
9. Centers for Disease Control. CDC criteria for anemia in children and childbearing-aged women. MMWR Morb Mortal Wkly Rep. 1989;38(22):400–404.
10. Sullivan KM, Mei Z, Grummer-Strawn L, Parvanta I. Haemoglobin adjustments to define anemia. Trop Med Int Heal. 2008;13(10):1267–1271. doi:10.1111/j.1365-3156.2008.02143.x
11. Ocas-Cordova S, Tapia V, Gonzales GF. Hemoglobin concentration in children at different altitudes in Peru: proposal for [Hb] correction for altitude to diagnose anemia and polycythemia. High Alt Med Biol. 2018;19(4):398–403. doi:10.1089/ham.2018.0032
12. Takubo T, Tatsumi N, Satoh N, et al. Evaluation of hematological values obtained with reference automated hematology analyzers of six manufacturers. Southeast Asian J Trop Med Public Health. 2002;33(Suppl 2):62–67.
13. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
14. Buttarello M. Laboratory diagnosis of anemia: are the old and new red cell parameters useful in classification and treatment, how? Int J Lab Hematol. 2016;38:123–132. doi:10.1111/ijlh.12500
15. Fischer SL, Fischer SP. Mean corpuscular volume. Arch Intern Med. 1983;143(2):282–283. doi:10.1001/archinte.1983.00350020108020
16. El-Hazmi MAF, Warsy AS. Normal reference values for hematological parameters, red cell indices, Hb A2 and Hb F from early childhood through adolescence in Saudis. Ann Saudi Med. 2001;21(3–4):165–169. doi:10.5144/0256-4947.2001.165
17. Bakrim S, Motiaa Y, Benajiba M, Ouarour A, Masrar A. Establishment of the hematology reference intervals in a healthy population of adults in the Northwest of Morocco (Tangier-Tetouan region). Pan Afr Med J. 2018;29:169. doi:10.11604/pamj.2018.29.169.13042
18. Nordin G, Mårtensson A, Swolin B, et al. A multicentre study of reference intervals for haemoglobin, basic blood cell counts and erythrocyte indices in the adult population of the Nordic countries. Scand J Clin Lab Invest. 2004;64(4):385–398. doi:10.1080/00365510410002797
19. Al MLA, Denic S, Al JON, Narchi H, Souid A-K, Al-Hammadi S. Red cell parameters in infant and children from the Arabian Peninsula. Am J Blood Res. 2015;5(2):101–107.
20. Serena V, Alessandro M, Maurizio TN, et al. Baseline haematological and biochemical reference values for healthy male adults from Mali. Pan Afr Med J. 2019;32. doi:10.11604/pamj.2019.32.5.12797
21. Karita E, Ketter N, Price MA, et al. CLSI-derived hematology and biochemistry reference intervals for healthy adults in eastern and Southern Africa. PLoS One. 2009;4(2):e4401. doi:10.1371/journal.pone.0004401
22. Odhiambo C, Oyaro B, Odipo R, et al. Evaluation of locally established reference intervals for hematology and biochemistry parameters in Western Kenya. PLoS One. 2015;10(4):e0123140. doi:10.1371/journal.pone.0123140
23. Beutler E, West C. Hematologic differences between African-Americans and whites: the roles of iron deficiency and α-thalassemia on hemoglobin levels and mean corpuscular volume. Blood. 2005;106(2):740–745. doi:10.1182/blood-2005-02-0713
24. Alsaeed ES, Farhat GN, Assiri AM, et al. Distribution of hemoglobinopathy disorders in Saudi Arabia based on data from the premarital screening and genetic counseling program, 2011–2015. J Epidemiol Glob Health. 2018;7:S41–S47. doi:10.1016/j.jegh.2017.12.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.