Back to Journals » Journal of Pain Research » Volume 13
Effect of Additional Pain Neuroscience Education in Interdisciplinary Multimodal Pain Therapy on Current Pain. A Non-Randomized, Controlled Intervention Study
Authors Richter M ![]() , Rauscher C, Kluttig A
, Rauscher C, Kluttig A ![]() , Mallwitz J, Delank KS
, Mallwitz J, Delank KS
Received 14 August 2020
Accepted for publication 21 October 2020
Published 16 November 2020 Volume 2020:13 Pages 2947—2957
DOI https://doi.org/10.2147/JPR.S272943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Michael Richter,1 Christian Rauscher,2 Alexander Kluttig,3 Joachim Mallwitz,4 Karl-Stefan Delank5
1Physiotherapie Am Michel, Hamburg, Germany; 2Rückenzentrum St. Georg, Asklepios Klinik St. Georg, Hamburg, Germany; 3Institute for Medical Epidemiology, Biometrics and Informatics, Interdisciplinary Center for Health Sciences, Martin-Luther-University, Halle-Wittenberg, Halle, Germany; 4Rückenzentrum Am Michel, Praxis Für Orthopädie, Hamburg, Germany; 5Universitätsklinikum (Halle), Department Für Orthopädie, Unfall- Und Wiederherstellungschirurgie, Martin-Luther-Universität, Halle-Wittenberg, Halle, Germany
Correspondence: Alexander Kluttig
Martin-Luther-University, Halle-Wittenberg, Institute for Medical Epidemiology, Biometrics and Informatics, Halle (Saale) 06097, Germany
Tel +49 (0)345 557-3570
Fax +49 (0)345 557-3580
Email [email protected]
Purpose: Interdisciplinary multimodal pain therapy (IMPT) programs for chronic back pain are effective and recommended. The patient-centered and biopsychosocial nature of IMPT is grounded in contemporary understanding that chronic pain states reflect heightened sensitization of the nervous system rather than an issue in the tissue. Teaching patients about pain is part of IMPT programs, though a clinical guideline is lacking. This study aims to answer the following question: Does the addition of an evidence-based pain neuroscience education (PNE) lecture for patients, into an IMPT program, produce superior results than the IMPT program itself?
Patients and Methods: A non-randomized, controlled intervention study was performed with 179 back pain patients indicated for IMPT. Intervention group (N=102) received a four-week IMPT program, which contained 4 one-hour sessions PNE. Control group (N=77) received the same IMPT without the additional PNE. Primary outcome was current pain after intervention. Pain knowledge, physical function, depression, anxiety, stress, quality of life and fear-avoidance were analyzed as secondary outcomes. Outcomes were defined as change of the parameter measured before and immediately after the four-week IMPT. For each outcome, linear regression models were used to estimate the raw and adjusted (sex, age and BMI) effect of additional PNE.
Results: Despite improvement in all outcomes for both groups during the treatment phase, the implemented PNE did not result in additional pain reduction (regression coefficient for PNE effect on pain level 0.34; 95% CI − 6.23– 6.97). Between-group differences could only be shown for pain-related knowledge in favor for the intervention group (0.78; 95% CI 0.35– 1.20).
Conclusion: The additional PNE lecture did not lead to pain reduction beyond the usual IMPT. However, the PNE did increase pain-related knowledge and, therefore, might be helpful in coping with pain after the IMPT program.
Keywords: interdisciplinary multimodal pain therapy, pain neuroscience education, chronic back pain, neurophysiology of pain, pain management
Introduction
Interdisciplinary multimodal pain therapy (IMPT) is a recommended and complex intervention for people with persisting pain.1 Despite the lack of a clear international consensus on the definition for IMPT content, for the German health care system the structure and process parameters are defined and proposed by a task force of the German IASP (International Association for the Study of Pain) chapter.1,2 Their published IMPT contents are recommended as best practice in the national guideline for the treatment of non-specific low back pain.3 Even though IMPT is recommended and first-line treatment for chronic pain patients it is underutilized4,5 and actual content lacks transparency.2
While an interdisciplinary team delivers a variety of interventions, educating the patients is a strong common denominator through all professions and a consistent recommendation from clinical practice guidelines.1,3,6 Patients should receive education about their prognosis, diagnosis and treatment options. Education about pain and its underlying mechanisms also needs to be addressed1 and patients' pain knowledge should be challenged during IMPT in concordance with contemporary pain neuroscience. As there are no detailed descriptions of how to apply pain education content during IMPT it is left at the discretion of the treatment center or institution. Kaiser et al2 call for standardization of therapeutic procedures within IMPT to allow for reproducibility and research, thus it seems meaningful to develop a structured pain education content and explore its therapeutic efficacy.
Over the last two decades, a therapeutic approach named pain neuroscience education (PNE) has evolved.7,8 PNE is an educational intervention aiming to change patients' understanding of what pain is, what function it serves and what biological processes are proven to underpin it.8 The fundamental message is that pain is a marker of the perceived need to protect bodily tissue and not a marker of damage or disease.8,9 If patients adapt a contemporary pain understanding and integrate this new understanding in their life and rehabilitation process, they are more likely to allow adaptive coping strategies and behaviors, are less fearful and have better function in daily life.7 If delivered in a combination with further interventions embracing a biopsychosocial framework PNE shows potential to reduce pain and disability.8
In a recent meta-analysis looking at the effects of PNE for chronic musculoskeletal pain thirteen randomized controlled trials were considered. The results established low clinical relevance of PNE for pain and disability in short and medium term. For kinesiophobia (short term) and catastrophizing (medium term) clinically relevant results could be shown.10 Another meta-analysis looking at PNE for chronic low back pain (CLBP) found moderate evidence that PNE shows small to moderate effects on pain and low-level evidence of a small to moderate effect on disability in the short term and also that PNE shows small to moderate effects on pain and disability at three month follow up.11 The systematic review and meta-analysis by Wood and Hendrick derived that additional PNE to usual physiotherapy interventions in patients with CLBP does improve disability and pain in the short but not long term.12 They concluded that their results provide support for the addition of PNE to routine physiotherapy practice in CLBP.12 The divergent results of the mentioned publications might result from looking at PNE effects for CLBP compared to heterogeneous chronic musculoskeletal pain.7,10–12 Also, Watson et al mention to have made their conclusions on sufficient statistical power compared to the other published works.10
Additionally, it can be hypothesized that dosage, context and style of content delivery are all pitfalls relevant to therapeutic efficacy of PNE. As recommended by Watson et al10 the influence of different PNE dosages needs to be further investigated and to our knowledge, only one study13 looked at dosage response in patients. Amer-Cuenca et al concluded that in patients with fibromyalgia, a higher dosage of PNE does lead to better results for pain intensity at three month follow up compared to less intensive PNE or biomedical education. They suggest to explore those dosage effects in different patient populations.13 As guideline-based IMPT does already imply pain education content and the inclusion of PNE in a wider multidisciplinary pain management has long been supported14 the combination of both might result in better outcomes.
For the delivery of a contemporary PNE to patients, it is important to assure that the deliverers have a common depth of understanding of the topic.9,10 Research has shown that health care professionals (HCP) do have deficits in pain knowledge which implies a barrier for sufficient patient education about pain.15 If this is also true for HCP working in the context of IMPT is unknown. To ensure a homogenous, reproducible and an evidence-based pain education during an IMPT program, standardization of the content might be helpful. If the content is based on best available evidence it can avoid a mixed message (biomedical vs biopsychosocial) and assist the team in being consistent which, for physiotherapists, is known to be challenging in chronic pain patients.16
The goal of this study was to evaluate the effects of an additional, structured PNE lecture within an IMPT program. As some PNE topics are part of such programs this is the first study looking at the effects of a higher dosage of PNE applied to patients with chronic back pain. It is hypothesized that the additional PNE will produce superior results, especially less pain, compared to the same program without extra PNE. As secondary outcomes, knowledge about pain, disability, fear-avoidance, health-related quality of life (HrQoL), stress, depression and anxiety were analyzed.
Materials and Methods
Study Design
We used a unicenter, prospective, non-randomized controlled intervention study design. The study was conducted in accordance with the Declaration of Helsinki and registered with the German Clinical Trials Register (DRKS00012945). Ethical approval was obtained by the ethical commission of the medical faculty of the Martin-Luther-University Halle-Wittenberg (ID 2018–38)
Participants
All patients referred to the pain management clinic by their medical doctor were eligible for the study. Every patient was diagnosed with persistent back pain with the imperative for interdisciplinary screening (IS) to triage if IMPT is indicated. The IS consisted of three consultations: 45min medical doctor, 45min physiotherapist and 60min psychologist. During the subsequent team meeting, all professional opinions were of equal value and led to the best possible patient-centered decision.17 IMPT inclusion criteria resulted from the listed operation and procedure code (OPS-2018 1–910). OPS is the German modification of the “International Classification of Procedures in Medicine” and three out of five points ((1) persisting or potential limitation of health-related quality of life or the ability to work (2) failed previous monomodal treatments, pain-related operation or drug withdrawal (3) existing drug addiction or abuse (4) pain-perpetuating psychological comorbidity (5) severe somatic comorbidity) are required for the patients´ inclusion into the IMPT program. The inclusion criteria for the study were an age of 20–60 years, back pain duration for longer than 6 months, no serious spinal pathology and indication for IMPT. If study inclusion criteria were fulfilled, the only reason for exclusion was the unwillingness to participate in the study.
Procedure
Patient recruitment was conducted from April 2018 until August 2019 in a center for IMPT in Hamburg, Germany. On the day of IS (t0) patients filled in an electronically administered questionnaire consisting of the primary and secondary outcomes and a study information leaflet was handed out. If patients were willing to participate, they gave informed consent. Patients were then scheduled for the IMPT program which could result in waiting times due to organizational matters or patient preferences. All participants went through the four-week IMPT. On the last day of the program the questionnaires were filled in again (t1). In December 2018, the therapeutic team was updated on latest pain neuroscience and a weekly one-hour PNE lecture for patients was implemented into the IMPT program. This resulted in two groups: One without (Control group) additional PNE, treated between April and November 2018, and one with the PNE lecture (Intervention group) treated between January and August 2019 (Figure 1).
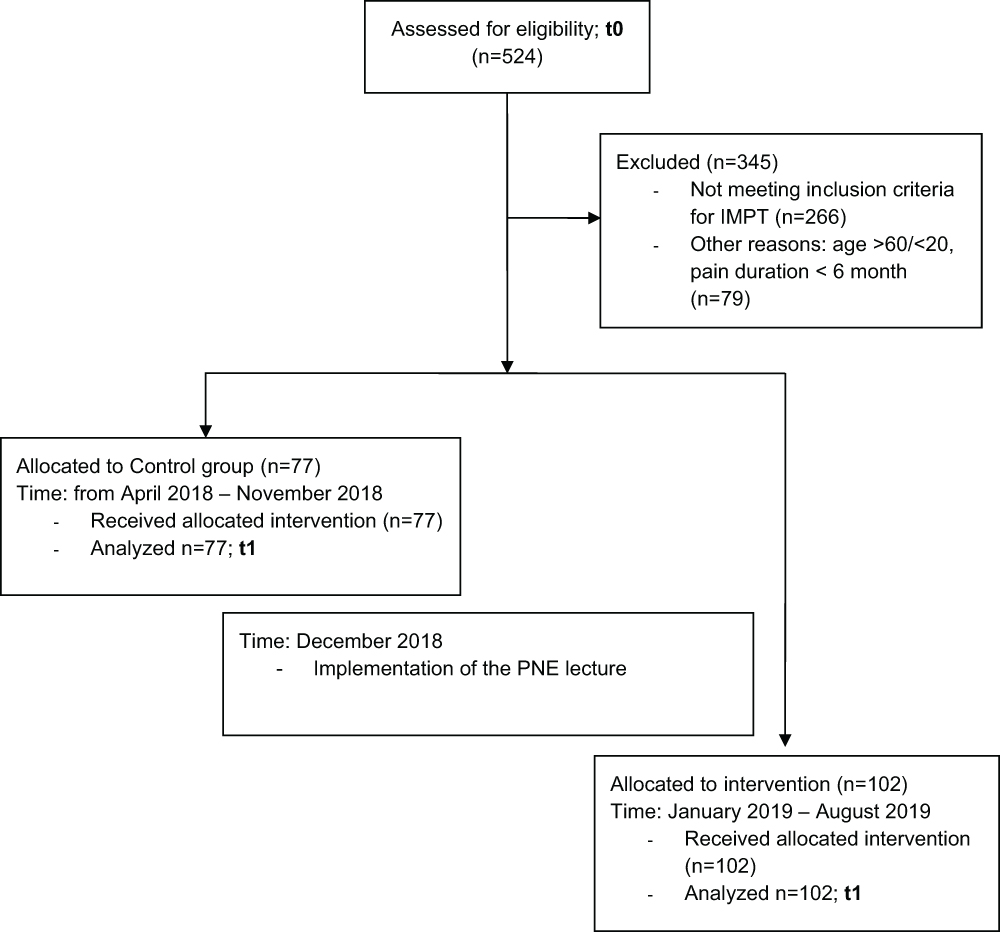 |
Figure 1 Flow of patients through the study. |
Intervention
IMPT Program
All participants received a four-week IMPT fulfilling recommendations for content and team approach.1,2,17,18 The program does accomplish the requirements of the OPS catalogue (OPS-2018 8–91c.11). As summarized in Kaiser et al the complex intervention is best described as
simultaneous, contextual, temporal and coordinated, comprehensive strategy to treat patients with chronic pain by integrating various somatic, physical, as well as psychological treatment approaches according to a predetermined therapeutic plan with consensual therapeutic aims among the therapists
with the primary aim of functional restoration and patients' control over pain.2 The interdisciplinary team is challenged to fundamentally change the patients´ attitude, coping style and beliefs about pain. Patients spend a minimum of four hours daily for four weeks in groups of eight working through a profound therapeutic timetable (Supplementary materials 1), provided by pain specialists, psychologists, physiotherapists and sport scientists, which has been published before.17,18 Table 1 displays the pain relevant information delivered during the IMPT program utilized in this study which adds up to 960 minutes (4 hours per week) of pain-related content. Importantly, all IMPT content remained unchanged for both groups in our study.
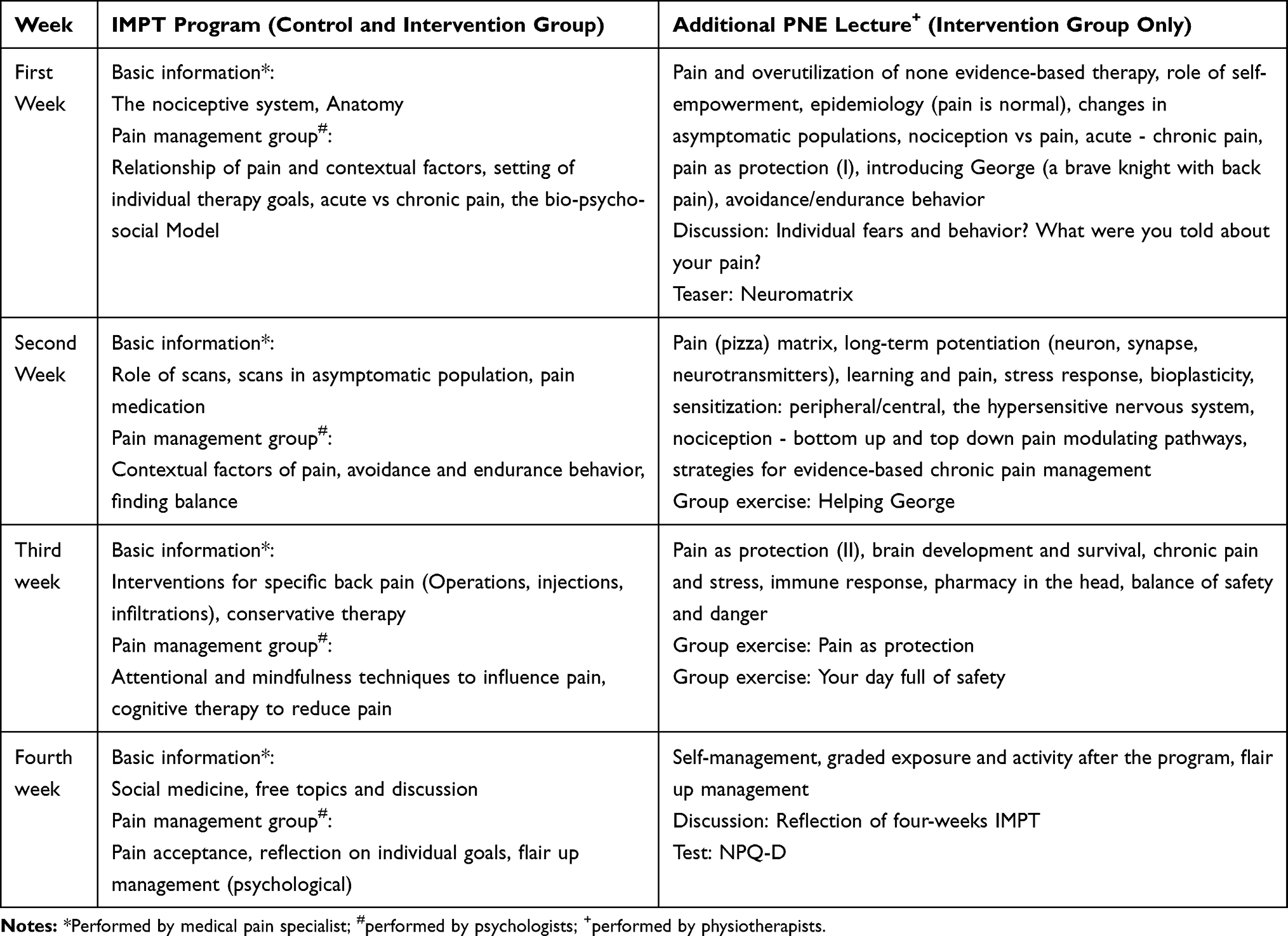 |
Table 1 Pain-Related Content of the Four-Week IMPT Program and the Additional PNE Lectures |
PNE
The intervention group received additional four hours of PNE. The lectures were delivered by members of the physiotherapeutic team. The content was based on published recommendations and learning objectives integrating a modern contemporary understanding of pain science.9,19–23 The PNE was delivered weekly via a PowerPoint™ presentation and was structured using prepared pictures, stories, examples and metaphors to simplify the understanding and promote a positive and deep learning experience. For individualization of the delivered information, group exercises and discussions were applied. Compared to the IMPT pain-related content the added PNE complemented a strong focus on the concept that pain is a marker of the perceived need to protect body tissue, that pain is fundamentally dependent on meaning and a sufficient understanding of the nociceptive system.8,20 The style of content delivery was patient-centered with a positive and confident pain message for the participants. The presentations were developed for a forty-five-minute lecture leaving extra time (15min) for personal questions or comments. Due to the nature of the IMPT program, some of the PNE content was automatically reinforced during subsequent interventions (medical training therapy, work hardening, relaxation therapy), eg (1) pain does not equal damage, therefore some pain during exercises is tolerable or (2) relaxation techniques calm down a hypersensitive nervous system. The reinforcement was not planned or structured. For a detailed description of the PNE intervention see Table 1 and the Template for Intervention Description and Replication (TIDieR) checklist (Supplementary materials 2). The presentation used will be made available for anyone who wishes to access it on reasonable request for up to six month after the date of publication.
Preparing the Team
December 2018 the interdisciplinary team was introduced to the PNE lecture and the team of physiotherapists (n = 8, male/female = 4/4, age: 34.86 ± 6.83, work experience in years: 9.94 ± 5.47) was trained for a consistent delivery of the PNE. The first author (MR) did two sets of the four lectures for supervision purposes and CR supervised his staff regularly during the study period. MR and CR have more than ten years of experience in IMPT work and fulfilled several postgraduate courses related to pain management. The team was supplied with animated PowerPoint™ presentations and a manuscript formulating the spoken word to support their preparation. Through an informal written inquiry, the team members agreed (1) that the preparation time was sufficient and (2) that they felt ready and prepared for the lecture presentation.
Outcome Measures
Primary Outcome
Current Pain Level: Pain was measured on a visual analog scale (VAS) ranging from no pain at all (0) to worst imaginable pain (100). Minimal clinical important difference (MCID) is published with 20mm or 30% decrease.24 We a priori calculated a sample size of 17 in each group, which would have 80% power to detect a difference in means of 20 (the difference between the intervention Group mean of 30 and the control Group mean of 10) assuming that the common standard deviation is 20 using a two group t-test with a 0.05 two-sided significance level. For organizational reasons, all patients fulfilling the inclusion criteria, who were treated within the study period, were also included in the study (N=179). This resulted in a power of >99% to detect an effect of ≥20mm change.
Secondary Outcomes
Hannover functional capacity questionnaire (FFbH-R): The FFbH-R is a valid tool to evaluate functional capacity in back pain patients.25 It consists of twelve items regarding function in activities of daily life (ADL). Results are in percent ranging from 0–100%. 80–100% does imply normal and <60% an impaired function. MCID for all functional outcomes is an increase of 30%.26
Neurophysiology of Pain Questionnaire (NPQ-D): The valid German NPQ-D can be used to measure pain-related knowledge.27 The NPQ-D consists of twelve items measuring the patients’ knowledge. Each correct item is evaluated with one point; thus, the maximum score is twelve points.
Fear avoidance beliefs questionnaire (FABQ): Patient-reported outcome including two domains, over sixteen items, measuring fear avoidance beliefs about work (FABQ: work) and about physical activity (FABQ: physical). Maximum subscale-scores are 42 (work) and 24 (physical activity).28 Higher scores indicate higher fear-avoidance. MCID have been established in different populations resulting in 25% decrease in points for FABQ: physical in women with pelvic girdle pain29 and thirteen-point change in back pain patients.30
12-Item Short-Form Health-Survey (SF12): The SF12 is a self-administered questionnaire measuring health-related quality of life (HrQoL) in two domains (physical and mental) over twelve items. The SF12 is a short version of the SF36 Health-Survey.31 Higher Scores indicating better HrQoL. MCID is established in a population of chronic low back pain patients for the subscales physical (>3.29) and mental (>3.77).32
Depression, Anxiety and Stress Scale (DASS-21): A valid measure for depression, anxiety and stress in adults.33 Each of the three subscales includes seven items; each to be answered from zero (did not apply to me) to three (applied to me much, or most of the time). Measurements are summed up; higher scores implying more relevance of the subscale.
Group Allocation
As can be seen in Figure 1 the group allocation was dependent on the time of participant IS within the study center. Once the PNE implementation was finalized all future participants were then in the intervention group.
Statistical Analysis
For sample description the mean, standard deviation and minimum and maximum values were calculated for continuous covariates, for categorial covariates, percentages are reported. Group differences at baseline were tested by conducting a t-test (continuous variables) or a chi-square test (categorial variables). For group related pre-post-sample statistics mean, standard error and 95% confidence interval (CI) for change of each outcome variable were calculated. The effect of PNE on outcomes was estimated via linear regression models. For each outcome, two models were calculated: a raw model with post intervention values as dependent variable and pre intervention values as well as group variable as independent variables, and an adjusted model, with additional sex, age and BMI as independent covariables. As result, we reported the beta-estimator for the PNE effect, its 95% CI and the p-value for each effect. The significance level was set a-prior at α ≤ 0.05. Missing values were excluded from analysis by listwise deletion. SAS 9.4 was used for data analysis (SAS Institute Inc., NC).
Results
Participants
A total of 524 patients were screened for eligibility. For 266 patients the interdisciplinary team regarded IMPT as not indicated. Another 79 could not be included due to exclusion criteria age (<20, >60) or pain duration of <6 months. Finally, 179 patients were included. No relevant difference between groups could be established. Both groups are homogenous with respect to the distribution of the covariates and directly comparable. See Table 2 for the sample characteristics.
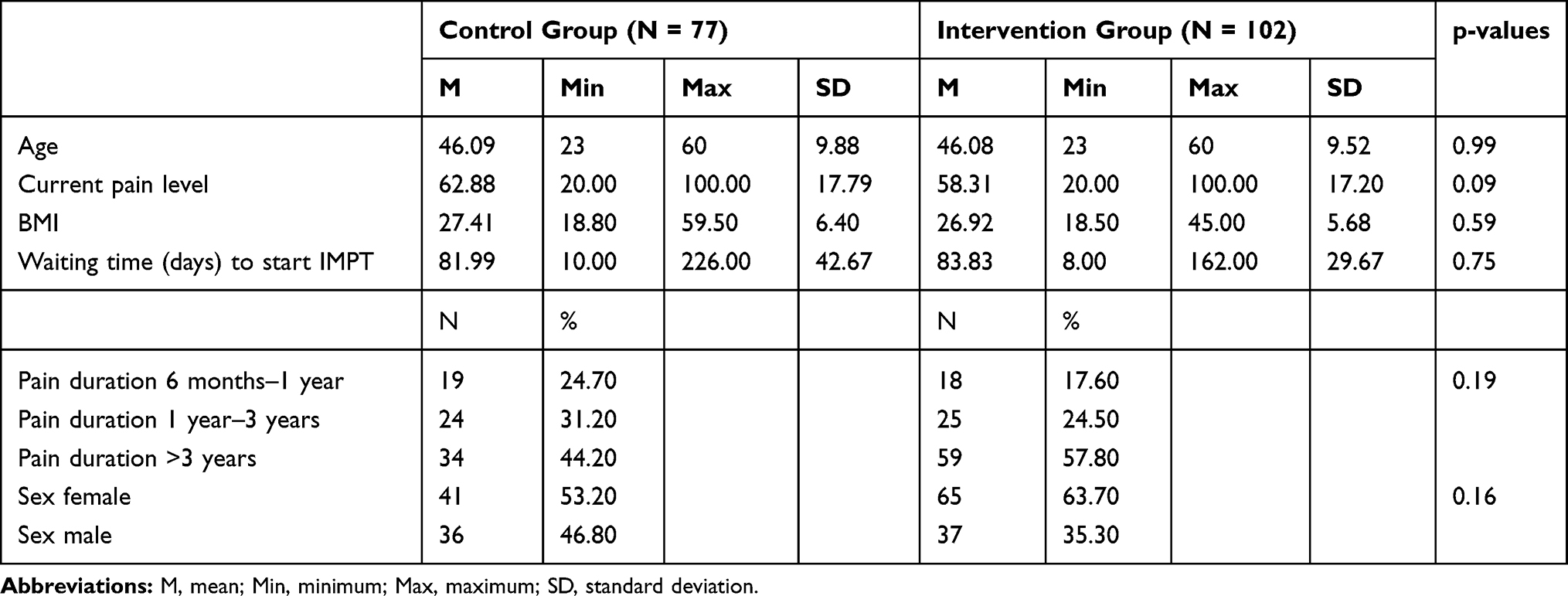 |
Table 2 Sample Description |
Primary Outcome
Current Pain
In our study, current pain level of chronic back pain patients, measured before and directly after the IMPT, decreased −30.03 (95% CI −35.31 to −24.76) in the intervention and −33.09 (95% CI −38.19 to −27.99) in the control group, resulting in a between-group difference of 3mm on a 100mm scale in favor for the control group (Table 3). No effect could be observed of additional PNE on change of current pain level in the raw (regression coefficient for PNE effect 0.11; 95% CI −6.42–6.65; p = 0.97) as well as in the adjusted model (0.34; 95% CI −6.23–6.97; p = 0.92) (Table 4).
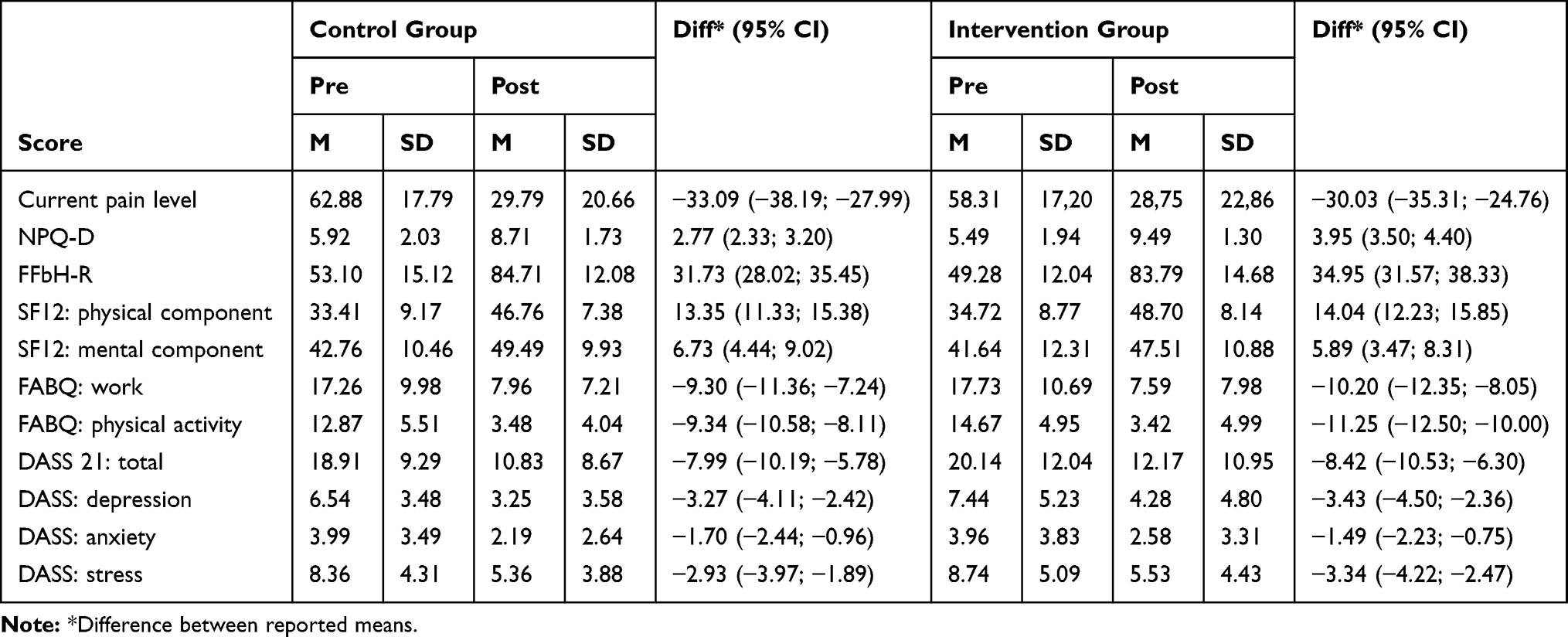 |
Table 3 Changes in Primary and Secondary Outcomes for Both Groups |
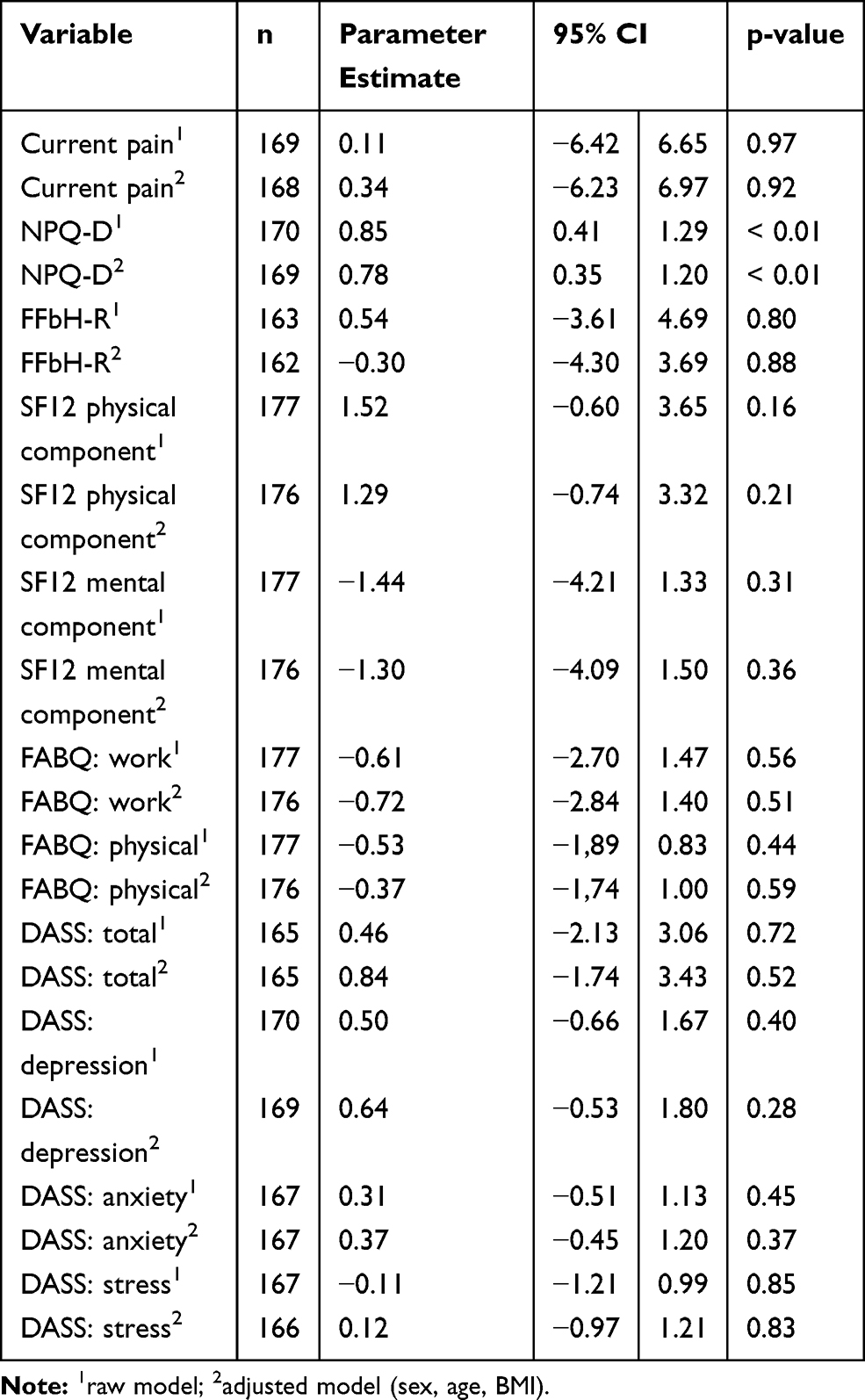 |
Table 4 Effect of Additional Pain Neuroscience Education on Primary and Secondary Outcomes |
Secondary Outcomes
In this study, all secondary outcomes improved in both groups during the intervention time (Table 3). However, additional effect of PNE was observed only for pain knowledge. We found improvement of NPQ-D in the raw (0.85; 95% CI 0.41 to 1.29; p < 0.01), as well as the adjusted (0.78; 0.35 to 1.20; p < 0.01) linear regression model in favor for the intervention group. However, no effect could be observed for additional PNE on any other secondary outcome (Table 4).
Discussion
In this non-randomized, controlled intervention study, we found evidence that in patients with chronic back pain additional 4 one-hour PNE lectures during an IMPT program had no extra benefit on current pain levels directly after the four-week program compared to the same IMPT without these lectures. Despite pain knowledge none of the secondary outcomes proofed to be superior in the intervention group.
We could show that all patients, not depending on group allocation, did improve over the intervention period. MCID thresholds could be attained for current pain, function, fear-avoidance and HrQoL thus implying clinically meaningful improvements for all study participants.
Research points out that the effects of PNE on pain intensity are uncertain, but a higher dosage and intensity does show a tendency towards larger effects and needs to be further investigated to be able to provide guidance on optimizing interventions and outcomes.10–12 In our study, we show a clinically relevant pain reduction over the intervention time in both groups which implies that a further pain reduction constitutes a therapeutic challenge. Our results prove that a higher dosage of pain education (additional four hours) was not sufficient to achieve superior results. Supposedly this might be due to an attained ceiling effect for pain reduction through the IMPT program alone. If an even higher intensity of PNE or another style of delivery (one-on-one vs groups of eight) would have produced better results therefore is questionable.
We demonstrated that the PNE lecture changed the patients' pain knowledge significantly better than the control group. As the content of the lecture was aiming at knowledge reconceptualization this was expected. Even though pain knowledge gain was superior for the intervention group, both groups improved their pain knowledge during therapy (intervention 9.49 ± 1.30 vs control 8.71 ± 1.73). Recently published results show that a two-day PNE seminar for physiotherapists lead to a NPQ-D score of 9.98 ± 1.73.27 Considering those scores as a reference, then the mean pain knowledge in all our study participants can be regarded as sufficient. Our conclusion concerning the knowledge gain in the control group is that the IMPT content alone already delivers an adequate pain message to patients, which results from the implementation of published recommendations.1 If this is applicable to other institutions offering IMPT is unknown. Comparing the mean pre-post difference of the two groups (intervention 3.95; 95% CI 3.50 to 4.40 vs control 2.77; CI 95% 2.33 to 3.20) it might be statistically significant, as established by the adjusted linear regression model used, but as all other outcomes are comparable between groups, the difference in pain knowledge does not imply any clinical relevance in the short term.
PNE does influence psychosocial factors like kinesiophobia and catastrophizing which are known to lead to pain persistence and chronicity.10 Hypothetically the intervention group patients will show better long-term results than the controls, as similar effects have been shown in a study done by Moseley et al.9 In their study, the superior pain reduction of the PNE-group appeared after three and twelve months. They claim that the PNE-group patients' conceptual changes were durable (compared to controls) which might have led to better self-efficacy and long-lasting better pain management skills. Watson et al postulate that PNE content, like pacing and graded exposure, will take time before their skilled application during daily activities.10 From their perspective, this might cause a delayed effect of PNE on disability.10 Lee et al could show that an improvement in pain knowledge is associated with less pain and disability one year later.34 If these positive long-term effects apply to our study will remain unknown due to the lack of a follow-up.
Strength and Limitations
A strength of our study is to have used a structured PNE intervention thus allowing for reproducibility and the exploration of a dosage response, which was recommended by Watson et al.10 As suggested by current literature, we added the PNE to interventions embracing a bio-psycho-social model of patient care, allowing PNE to unfold its best efficacy.8–11 Our study is the first to look at the effects of different dosages of PNE applied to patients suffering from chronic back pain.
One main limitation of our study was the allocation of participants to the intervention and control group, which was not at random, but depended on the date of the first consultation. This may have led to structural inequality between the groups. However, baseline characteristic in both groups seem comparable regarding the main potential confounders. Nevertheless, we calculated linear regression models to also quantify the confounder-adjusted effect of intervention on primary and secondary outcomes. No relevant change in estimates was found after adjusting for age, sex and BMI and after additional mutual adjustment for further potential confounders (baseline pain duration, DASS score, FABQ, SF12, FFbH-R, NPQ-D) (results not shown).
A control group receiving no intervention would have allowed to determine if the IMPT treatment phase was better than no treatment at all or natural history. From the authors' perspective, this was not considered as it is ethically not justifiable.
Another limitation is that the authors measured the outcomes directly after the IMPT, whereas a follow-up after three to six months would have added more to the scientific knowledge base of PNE.10
Regarding the choice of outcomes, the authors missed assessing psychosocial factors relevant to PNE such as kinesiophobia, catastrophizing or self-efficacy.11 In addition, patient and provider satisfaction with the IMPT service were not considered and program adherence was merely recorded for the intervention group as stated in the TIDieR checklist (Supplementary materials 2).
The pain-related content delivered during the IMPT was not changed for our study and presented as usual. Some elements of the added PNE lectures surely were part of the IMPT program already (Table 1) which might have been perceived as duplicated information by the patients. The authors suggest, that hearing PNE topics more than once is helpful to reinforce the patients’ understanding of the delivered information. This idea does also find support in our results, which show higher pain knowledge in the intervention group.
Finally, educating the team in the study center was limited to the presentation of the PNE lectures designed for the study. PNE teachers need an excellent understanding of pain neurophysiology but also, they should have caring, insightful and pedagogical skills for best content delivery.11 There was no competency assessment evaluating the HCP skills to deliver the PNE content.
Clinical and research implications
As proposed by other researchers higher pain-related knowledge seems to be to the patients' benefit in the long term regarding pain and disability.9,10,34 Therefore, long-term effects need to be further investigated.
We suggest that our PNE lecture might show better effects in a clinical situation, where an interdisciplinary team is not already delivering a structured and up-to-date pain education or even in a monodisciplinary setting, eg outpatient physiotherapy.
Due to the design of our study, some pain-related information was delivered more than once. If this was helpful or not is unclear but diminishing all doubled information could be an option to save human and monetary resources.
Conclusion
The addition of 4 one-hour PNE sessions into a four-week IMPT program for chronic back pain patients does not lead to superior results at discharge for current pain but does increase pain-related knowledge. We conclude that the application of a higher dosage of pain education content within the IMPT has not been successful in achieving better patient-relevant outcomes in the short term. Nevertheless, the higher pain knowledge scores could lead to better pain management in the long term.
Abbreviations
IMPT, interdisciplinary multimodal pain therapy; PNE, pain neuroscience education; HrQoL, health related quality of life; IS, interdisciplinary screening; OPS, operation and procedure code; MCID, minimally clinical important difference; FFbH-R, hannover functional capacity questionnaire; NPQ-D, neurophysiology of pain questionnaire; FABQ, fear avoidance beliefs questionnaire; SF12, 12-item short-form health survey; DASS, depression, anxiety and stress scale; HCP, health care practitioners; CLBP, chronic low back pain.
Data Sharing Statement
The datasets used and analyzed during the study are available from the corresponding author on reasonable request.
Informed Consent
Informed consent was obtained from all participants prior to participation.
Acknowledgments
The work done by the therapeutic team and staff of the study center is acknowledged and appreciated. The manuscript was submitted as a partial fulfilment of the requirements for the Dr. rer. medic. degree of Michael Richter (MR).
Funding
There was no funding for this research project.
Disclosure
The authors declare to have no competing interests.
References
1. Arnold B, Brinkschmidt T, et al. Multimodale Schmerztherapie für die Behandlung chronischer Schmerzsyndrome. Der Schmerz. 2014;28(5):459–472. doi:10.1007/s00482-014-1471-x
2. Kaiser U, Treede RD, Sabatowski R. Multimodal pain therapy in chronic noncancer pain—Gold standard or need for further clarification? Pain. 2017;158(10):1853–1859. doi:10.1097/j.pain.0000000000000902
3. Chenot JF, Greitemann B, Kladny B, Petzke F, Pfingsten M, Schorr SG. Nichtspezifischer Kreuzschmerz. Dtsch Arztebl Int. 2017;114(51–52):883–890.
4. Behrendt S, Kulas H, Marschall U, Steffens M, Schiffhorst G, Bleß HH. Welche Rückenschmerzpatienten profitieren von einer multimodalen Schmerztherapie? Eine komparative Kostenanalyse auf Basis von GKV-Routinedaten. Das Gesundheitswesen. 2016;78(S 01):e120–e127. doi:10.1055/s-0042-110401
5. Deutsche Schmerzgesellschaft e.V. Forschungsagenda – perspektive Schmerzforschung Deutschland. Schmerz. 2017. 33:245. doi:10.21962/ForA_2017.001.1
6. Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79–86. doi:10.1136/bjsports-2018-099878
7. Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiotherapy Theory Pract. 2016;32(5):332–355. doi:10.1080/09593985.2016.1194646
8. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
9. Moseley GL, Butler DS. Explain Pain Supercharged. Adelaide, Australia: Noigroup publications; 2017.
10. Watson JA, Ryan CG, Cooper L, et al. Pain neuroscience education for adults with chronic musculoskeletal pain: a mixed-methods systematic review and meta-analysis. J Pain. 2019;20(10):1140e1–1140e22. doi:10.1016/j.jpain.2019.02.011
11. Tegner H, Frederiksen P, Esbensen BA, Juhl C. Neurophysiological pain-education for patients with chronic low back pain – a systematic review and meta-analysis. Clin J Pain. 2018;34:778–786. doi:10.1097/AJP.0000000000000594
12. Wood L, Hendrick PA. A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: short- and long-term outcomes of pain and disability. Eur J of Pain. 2019;23(2):234–249. doi:10.1002/ejp.1314
13. Amer-Cuenca JJ, Pecos-Martín D, Martínez-Merinero P, et al. How much is needed? Comparison of the effectiveness of different pain education dosages in patients with fibromyalgia. Pain Med. 2020;21(4):782–793. doi:10.1093/pm/pnz069
14. Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J of Pain. 2004;20(5):324–330. doi:10.1097/00002508-200409000-00007
15. Thompson K, Johnson MI, Milligan J, Briggs M. Twenty-five years of pain education research—what have we learned? Findings from a comprehensive scoping review of research into pre-registration pain education for health professionals. Pain. 2018;159(11):2146–2158. doi:10.1097/j.pain.0000000000001352
16. Synnott A, O’Keeffe M, Bunzli S, Dankaerts W, O’Sullivan P, O’Sullivan K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: a systematic review. J of Physiotherapy. 2015;61(2):68–76. doi:10.1016/j.jphys.2015.02.016
17. Hamel M, Heinrich M, Niemier K, Marnitz U. Rückenschmerzen therapieren: Von der multimodalen Idee zur interdisziplinären Lösung (1. Aufl.). De Gruyter, Berlin: Boston; 2018.
18. Mallwitz J, Dörner T, Richter M. Multimodale interdisziplinäre Therapie beim chronischen Rückenschmerz. Orthopädie und Unfallchirurgie up2date. 2014;9(06):463–480. doi:10.1055/s-0033-1358047
19. Hush JM, Nicholas M, Dean CM. Embedding the IASP pain curriculum into a 3-year pre-licensure physical therapy program: redesigning pain education for future clinicians. Pain Reports. 2018;3(2):e645. doi:10.1097/PR9.0000000000000645
20. Moseley G, Butler DS. The Explain Pain Handbook. Protectometer. Adelaide, Australia: Noigroup Publications; 2015.
21. Nijs J, van Wilgen CP, van Oosterwijck J, van Ittersum M, Meeus M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: practice guidelines. Man Ther. 2011;16(5):413–418. doi:10.1016/j.math.2011.04.005
22. Richter M. „Schmerzen verstehen“ in der Praxis. Man Med. 2017;55(5):265–273. doi:10.1007/s00337-017-0300-6
23. Louw A, Puentedura E. Therapeutic Neuroscience Education. Teaching Patients About Pain: A Guide for Clinicians. Story City: International Spine and Pain Institute; 2013.
24. Schomacher J. Gütekriterien der visuellen Analogskala zur Schmerzbewertung. Physioscience. 2008;4(03):125–133. doi:10.1055/s-2008-1027685
25. Kohlmann T, Raspe H. Hannover Functional Questionnaire in ambulatory diagnosis of functional disability caused by backache. Rehabilitation (Stuttg). 1996;35(1):I–VIII.
26. Ostelo R, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi:10.1097/BRS.0b013e31815e3a10
27. Richter M, Maurus B, Egan Moog M, Rauscher C, Regenspurger K, Delank KS. German version of the Neurophysiology of Pain Questionnaire: translation, cross-cultural adaptation, reliability and validity. Der Schmerz. 2019;33(3):244–252. doi:10.1007/s00482-019-0366-2
28. Pfingsten M, Kröner-Herwig B, Leibing E, Kronshage U, Hildebrandt J. Validation of the German version of the fear-avoidance beliefs questionnaire. Eur J Pain. 2000;4(3):259–266. doi:10.1053/eujp.2000.0178
29. Grotle M, Garratt AM, Krogstad Jenssen H, Stuge B. Reliability and construct validity of self-report questionnaires for patients with pelvic girdle pain. Phys Ther. 2012;92(1):111–123. doi:10.2522/ptj.20110076
30. George SZ, Fritz JM, McNeil DW. Fear-avoidance beliefs as measured by the fear-avoidance beliefs questionnaire: change in fear-avoidance beliefs questionnaire is predictive of change in self-report of disability and pain intensity for patients with acute low back pain. Clin J Pain. 2006;22(2):197–203. doi:10.1097/01.ajp.0000148627.92498.54
31. Jr JE W, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
32. Díaz-Arribas MJ, Fernández-Serrano M, Royuela A, et al. Minimal clinically important difference in quality of life for patients with low back pain. Spine. 2017;42(24):1908–1916. doi:10.1097/BRS.0000000000002298
33. Nilges P, Essau C. Die depressions-angst-stress-skalen. Der Schmerz. 2015;29(6):649–657. doi:10.1007/s00482-015-0019-z
34. Lee H, McAuley JH, Hübscher M, et al. Does changing pain-related knowledge reduce pain and improve function through changes in catastrophizing? Pain. 2016;157(4):922–930. doi:10.1097/j.pain.0000000000000472
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.