Back to Journals » Journal of Pain Research » Volume 15
Effect of Acupuncture on Pain, Fatigue, Sleep, Physical Function, Stiffness, Well-Being, and Safety in Fibromyalgia: A Systematic Review and Meta-Analysis
Received 2 December 2021
Accepted for publication 15 January 2022
Published 3 February 2022 Volume 2022:15 Pages 315—329
DOI https://doi.org/10.2147/JPR.S351320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Chengqiang Zheng,1 Tianxiu Zhou2
1School of Sport, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Campus Hospital, Chengdu University of Technology, Chengdu, People’s Republic of China
Correspondence: Tianxiu Zhou
Campus Hospital, Chengdu University of Technology, Chengdu, People’s Republic of China
, Tel +86-13678030472
, Email [email protected]
Purpose: Fibromyalgia (FM) is a syndrome characterized by widespread pain, which caused huge economic and social burden. Acupuncture is often used to manage chronic pain. However, the efficacy of acupuncture in FM is still controversial. This study aimed to systematically review the effects of acupuncture on pain, fatigue, sleep quality, physical function, stiffness, well-being, and safety in FM.
Methods: We searched databases including PubMed, Embase, the Cochrane Library, Wanfang Database, Chongqing Weipu, and the China National Knowledge Infrastructure from inception to September 2021. Eligible studies included randomized or quasi-randomized controlled studies of acupuncture in patients with FM. Quantitative analysis was conducted using RevMan 5.3 software, and risk assessment was performed according to the Cochrane collaboration tool. Safety was quantitatively analyzed.
Results: A total of 13 articles were searched, of which 12 were analyzed quantitatively. Our meta-analysis found that acupuncture could alleviate pain (SMD: − 0.42, 95% CI, − 0.66, − 0.17, P< 0.001, I2=58%) and improve well-being (SMD: − 0.86, 95% CI, − 1.49, 0.24, P=0.007, I2=85%) at post-treatment. In addition, acupuncture showed long-term effects on reducing pain (P=0.03) and improving well-being (P< 0.001). No evidence that acupuncture works on fatigue, sleep quality, physical function, or stiffness was found. No serious adverse events were detected in acupuncture treatment.
Conclusion: Moderate quality of evidence supports acupuncture in reducing pain in patients with FM. Therefore, acupuncture is recommended as a treatment for FM.
Keywords: fibromyalgia, acupuncture, pain, meta-analysis, systematic review
Introduction
Fibromyalgia (FM) is a diffuse pain syndrome with widespread pain, fatigue, and sleep disturbance as the main symptoms caused by the dysfunction of central nervous system sensory afferent processing.1 FM is the third most common chronic musculoskeletal pain after low back pain and osteoarthritis, with an incidence of 2–3% in the general population worldwide.2 FM can affect people of any age and is more common in women, obese people, and those with poor mental health.3 Patients with FM are reported to have considerably higher rates of comorbidities and medical cost burdens than age - and sex-matched healthy individuals,4,5 with average medical costs that are 30% higher than the control group.5
At present, no gold standard treatment for FM is available in the guidelines. The management of FM focuses on improving symptoms, that is, reducing pain and fatigue, improving sleep quality and physical function, and improving quality of life.6,7 Given that pharmacological treatments are often associated with adverse reactions, guidelines recommend that non-pharmacological treatments be considered for the initial management of FM.6,7 Acupuncture is an important component of complementary alternative medicine treatment. Studies indicate that analgesia can be achieved by releasing endogenous opioid or non-opioid substances to activate peripheral and central pain regulation systems8–10 and increase the local blood flow of muscles.11 Recent studies have demonstrated the potential benefits of acupuncture in improving neuropathic pain features and pain catastrophizing in FM patients, as well as the possibility of personalization of treatment.12,13 Therefore, acupuncture is a potential approach for FM.
Studies on the efficacy of acupuncture on FM have shown mixed results. The earliest systematic review concluded that acupuncture is effective only for short-term pain and not for other symptoms, including fatigue and sleep quality.14 Cochrane’s review concluded that acupuncture is not superior to sham acupuncture for FM.15 More recent meta-analyses have shown that acupuncture is effective for pain,16,17 sleep quality, and quality of life but not fatigue.17 This inconsistent evidence creates confusion in clinical practice, so we conducted this meta-analysis to update the results with new clinical studies. Furthermore, given that FM is a multisymptomatic syndrome,7 we performed a comprehensive meta-analysis of various clinical outcomes to gain insight into the potential benefits of acupuncture. Therefore, our research aims to (1) assess the effects of acupuncture on pain, fatigue, sleep quality, physical function, stiffness, and well-being in FM systematically; (2) determine the influence of different parameters of acupuncture on the therapeutic effect; and (3) explore the safety of acupuncture therapy.
Methods
This protocol has been registered in PROSPERO with code CRD42021267743 (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021267743). This meta-analysis was performed based on the PRISMA statement.
Literature Search
We conducted literature searches in six electronic databases, namely, Embase, PubMed, the Cochrane Library, Chongqing Weipu, Wanfang Database, and the China National Knowledge Infrastructure from the date of availability to September 2021, regardless of language type. Detailed retrieval methods are presented in Supplementary Table 1.
Type of Participants
Patients were diagnosed with FM based on recognized diagnostic criteria18 and were not restricted by age, sex, pain intensity, or duration of disease.
Types of Studies
Randomized and quasi-randomized controlled studies of acupuncture for FM were considered. Quasi-randomized study refers to the studies that are not strictly conducted according to the true randomization method, such as date of birth. We excluded animal studies, observational studies, case reports, conference abstracts, commentaries, and letters.
Types of Interventions
The intervention is acupuncture therapy based on the theory of Chinese medicine, including manual acupuncture (MA) and electro-acupuncture (EA). Studies comparing different acupuncture styles were excluded. Furthermore, studies that combined acupuncture with other treatments, such as cupping and herbal medicine, were excluded.
Types of Control Interventions
Control interventions included sham and simulated or placebo acupuncture. Sham acupuncture refers to the stimulation of penetrating the skin at non acupoint points. Simulated or placebo acupuncture involves applying stimulation without inserting into the skin at acupoints.
Types of Outcome Indicators
Studies have reported at least one significant symptom of FM, including pain, sleep, fatigue, physical function, stiffness, and well-being. The secondary outcome was adverse events, reflecting the safety of acupuncture therapy.
Study Selection
The authors independently reviewed the titles and abstracts on the basis of the inclusion criteria to determine eligible studies. Subsequently, we carefully reviewed the full text for the final selection. Any differences will be resolved through discussion. If no agreement can be obtained, an expert will be consulted to decide whether the article is eligible.
Data Extraction
The following information was extracted by the authors independently using a pre-designed table: study characteristics (author, setting, year, and sample size), interventions, type of stimulation (MA and EA), type of acupuncture (individually adapted and standardized), follow-up period, treatment duration (less than 10 sessions and more than 10 sessions), outcome measures (pain, fatigue, sleep, physical function, stiffness, and well-being), and adverse events.
Measures of Intervention Effect
Mean and standard deviation (SD) of continuous datas were extracted at post-intervention and follow-up, including pain, fatigue, sleep, physical function, stiffness, and well-being. The number of adverse events was extracted to quantitatively evaluate the safety of acupuncture.
Dealing with Missing Data
If data were presented graphically, the software GetData Graph Digitizer version 2.26 was employed to extract the data. When the mean or SD data were missing, we collected data from published meta-analysis articles.14,15
Assessment of Risk of Bias
The Cochrane Collaboration tool was employed to evaluate the risk of bias for listed studies. The Cochrane tool divides bias risk into three categories: low risk, unclear, and high risk. The evaluation was completed by two authors independently.
Quality of Evidence
We applied the Grading of Recommendations Assessment, Development, and Evaluation Guideline Development Tool to evaluate the quality of evidence and determine the level of evidence recommendation. The quality of evidence was rated into very low, low, moderate, and high. Factors that may downgrade the quality of evidence included publication bias, inconsistency of results, indirectness of evidence, imprecision, and risk of bias.
Statistical Analysis
The meta-analysis was completed with Review Manager software (RevMan 5.3). Standardized MD (SMD) was employed to calculate the results of continuous variables with different scales. We used risk ratios (RRs) to evaluate categorical variables. Heterogeneity results were evaluated using the I2 statistic. When I2>50% and heterogeneity was substantial, we used a random effect model for point estimation. When I2<50%, the fixed effect model was used. P<0.05 was considered statistically significant.
Three subgroup analyses were performed to explore factors influencing the short-term effect of acupuncture therapy for FM: type of stimulation (MA vs EA), type of acupuncture (individually adapted vs standardized), and number of sessions (less than 10 sessions vs more than 10 sessions).
We evaluated potential publication bias with funnel plot asymmetry. Egger test was applied to quantitatively evaluate the significance of asymmetry. Sensitivity analysis was carried out to detect the stability of the results by deleting each study individually.
Results
Search Results
A total of 1391 articles were retrieved, of which 332 duplicate articles were removed. The remaining 1059 articles were screened for titles and abstracts, and 987 records did not achieve the inclusion criteria. Finally, the remaining 72 articles were evaluated for their full text, and 13 of the studies were eligible for the systematic review. The original data were not available for one study, so only 12 studies were quantitatively analyzed. The flow chart of study retrieval and screening is presented in Figure 1.
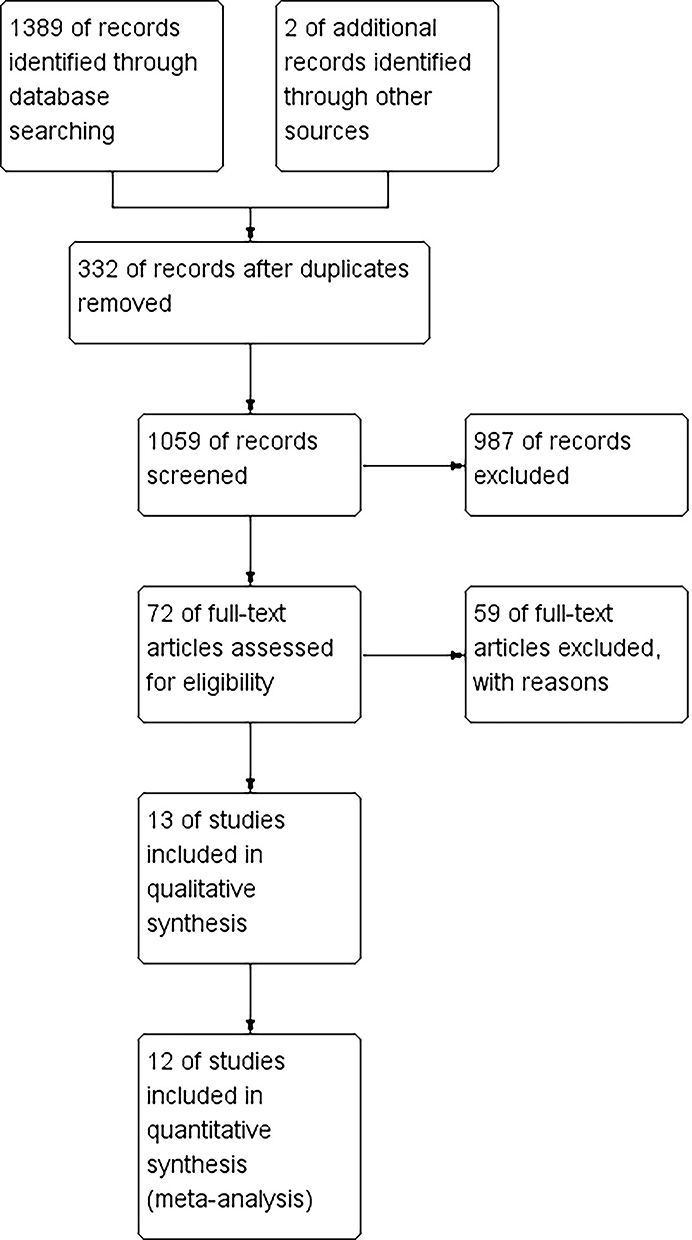 |
Figure 1 Flow chart for research selection strategy based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. Notes: PRISMA figure adapted from Moher D, Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.43 |
Study Characteristics
All participants met the criteria of 1990 ACR18 for the diagnosis of FM. Twelve studies were published in English19–30 and one in Portuguese.31 All experimental groups selected traditional Chinese acupoints for MA or EA, five studies adopted individually adapted acupoint selection scheme,19,20,22,24,26 and the eight other studies used standardized acupoints.21,23,25,27–31 The control group was sham acupuncture or simulated acupuncture. Study characteristics are shown in Table 1.
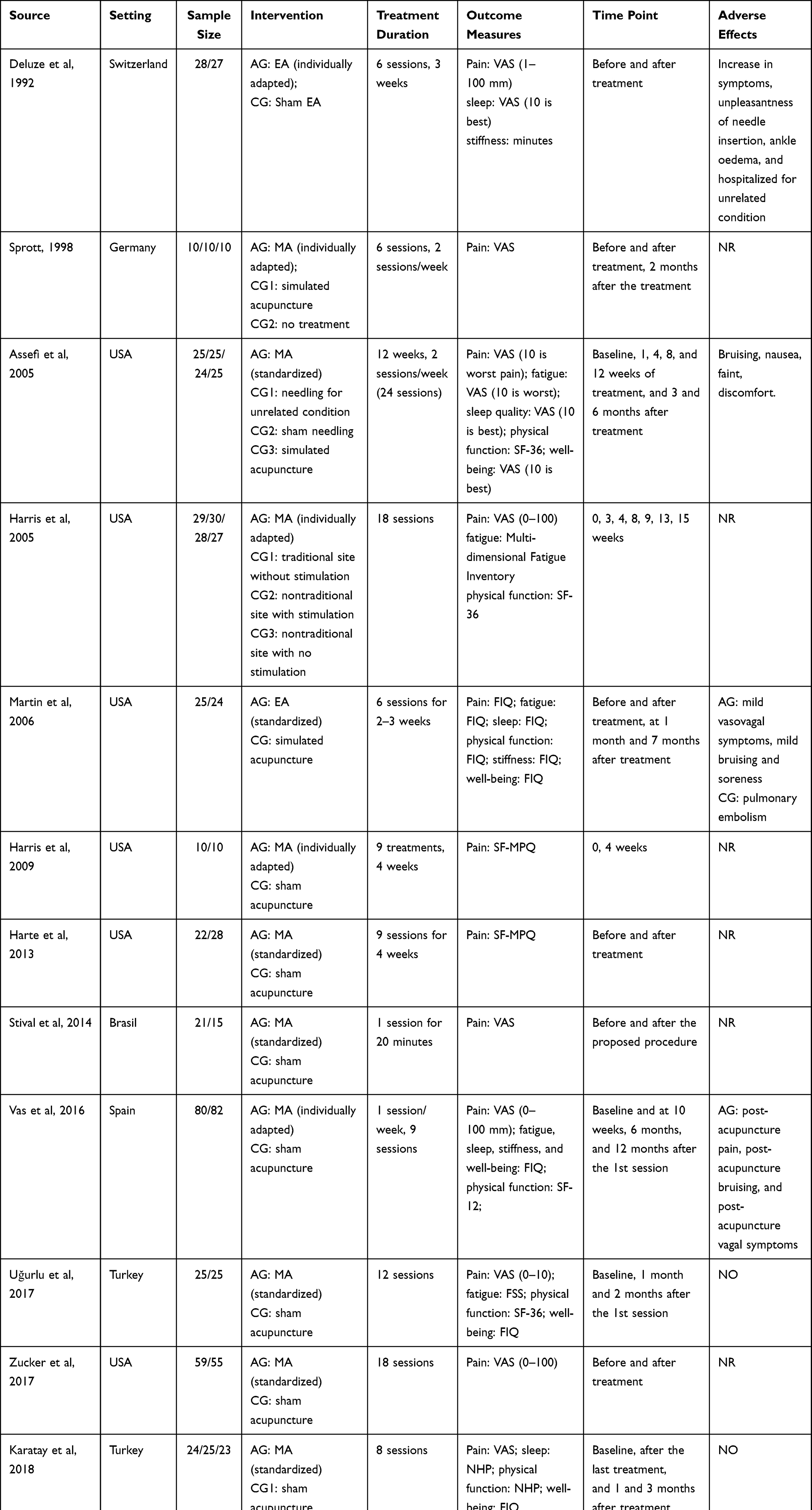 |
Table 1 Characteristics of Included Studies |
Risk of Bias in Reviewed Studies
The risk assessment of bias for the listed studies is presented in Figure 2. All the studies were randomized or quasi-randomized trials, among which the randomization method of four studies was not presented in the article.20,23,24,28 Except for one high-risk study,20 most of the studies on allocation concealment were low risk. Blinding of acupuncturists was at high risk in all studies. In one study,27 neither the patients nor the outcome evaluators were blinded. Nine studies did not have missing data,19,21–24,26,27,30,31 and three reported missing data due to withdrawal from the trial.25,28,29 Finally, six articles were deemed free of selection bias and other potential biases.19,21,23,24,29,30
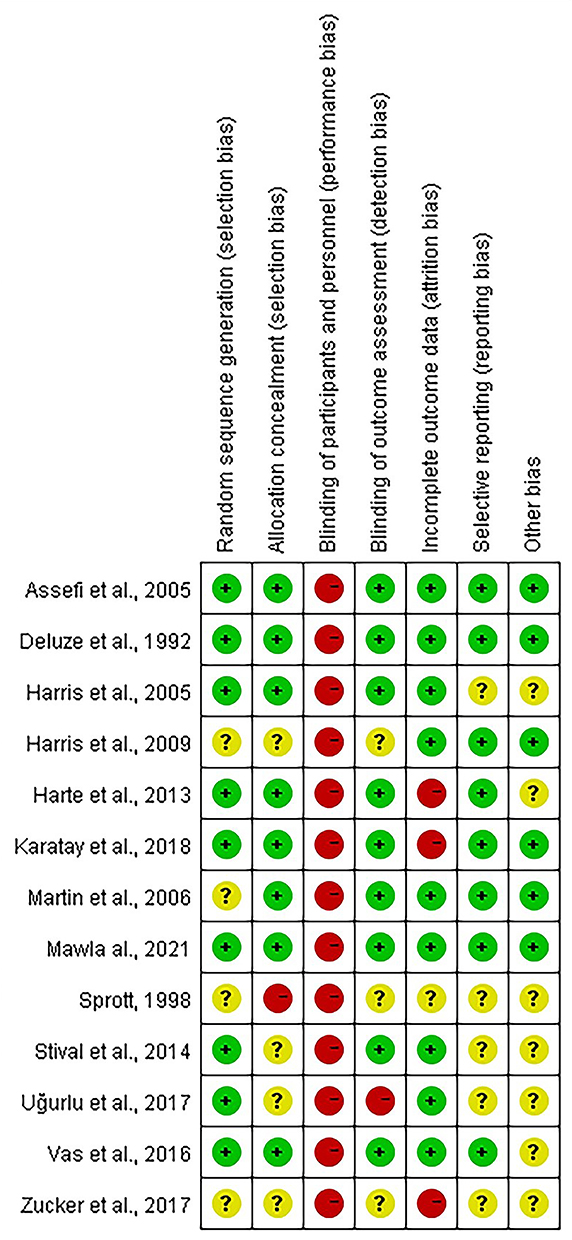 |
Figure 2 Bias risk assessment for included studies. |
Meta-Analysis
Pain
Results related to pain were reported in all studies, and a quantitative analysis was performed on 715 participants in 12 studies. Pain intensity was evaluated by visual analogue scale (VAS), Brief Pain Inventory, and Short Form of McGill Pain Questionnaire. Overall meta-analysis showed that acupuncture had a short-term analgesic effect on FM (SMD: −0.42, 95% CI, −0.66, −0.17, P<0.001, I2=58%) (Table 2). The quality of evidence was rated as moderate due to the large heterogeneity (see Supplementary Table 2). We removed studies individually for sensitivity analysis, and heterogeneity changed significantly after removing one study.27 As there were multiple follow-up visits, we used the results of the last follow-up to analyze the long-term effects of acupuncture treatment (Supplementary Figure 1). In four studies included in the analysis, our results suggested that acupuncture for FM had a long-term analgesic effect. However, sensitivity analysis indicated that the follow-up results were not robust.
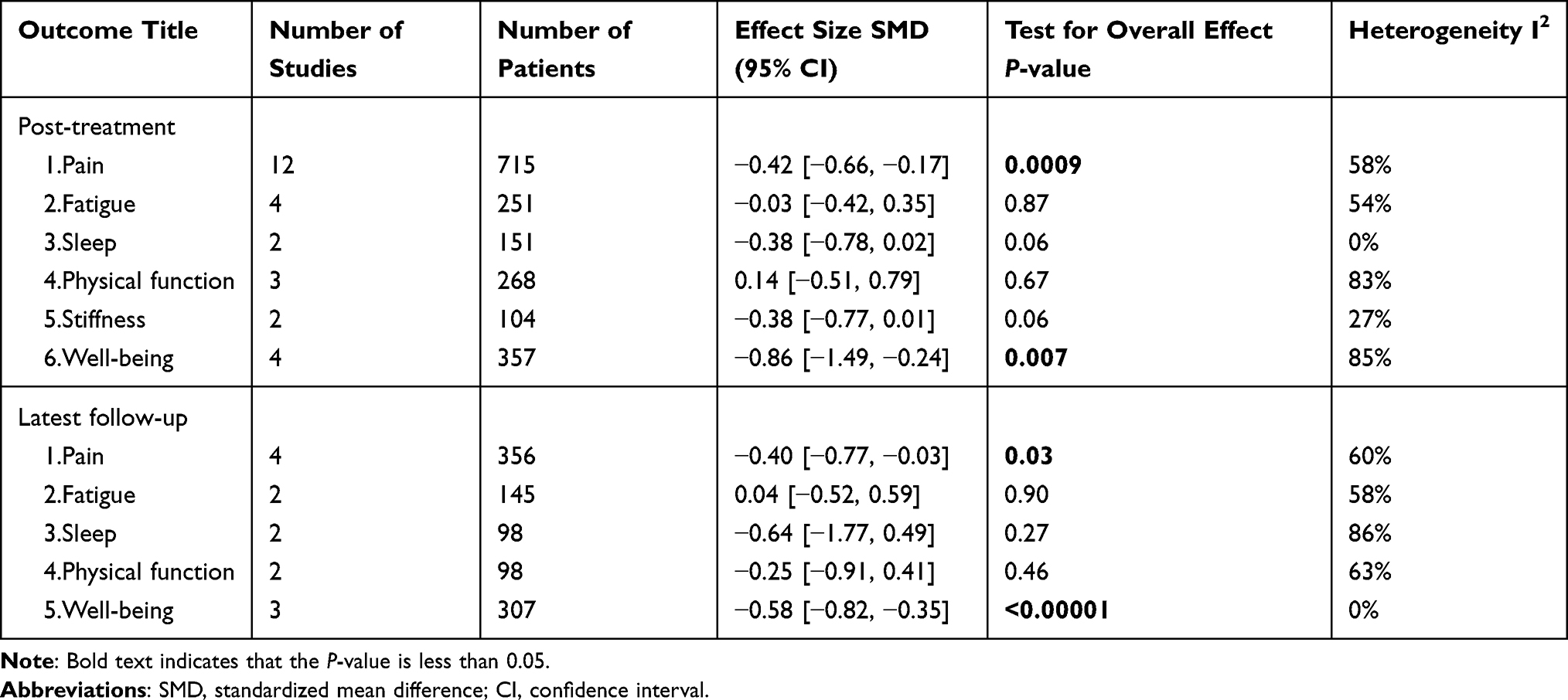 |
Table 2 Effect Sizes of Acupuncture Group Compared with Control Group on Selected Outcome Variables |
Subgroup Analysis
Type of stimulation Our subgroup analysis showed no significant difference in analgesia between MA (SMD: −0.33, 95% CI, −0.63, −0.04, P=0.008, I2=68%) and EA (SMD: −0.46, 95% CI, −0.79, −0.12, P=0.03, I2=0%) (Figure 3) based on a random-effects model. Sensitivity analysis reflected that the significance of the analgesic effect disappeared when we removed one study in the EA subgroup.19
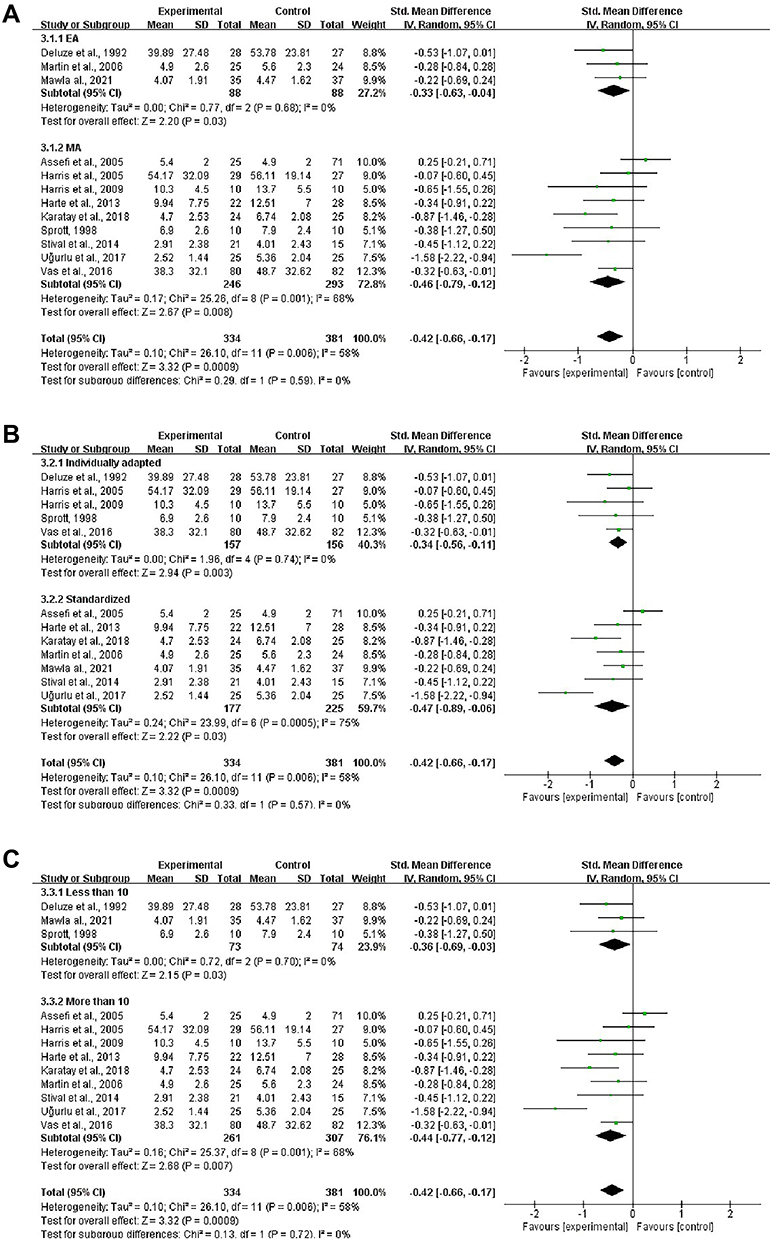 |
Figure 3 Forest plots of the analgesic effect of acupuncture in the post-treatment. (A) Subgroup analysis: manual acupuncture vs electroacupuncture. (B) Subgroup analysis: individual adapted acupuncture vs standardized acupuncture. (C) Subgroup analysis: less than 10 sessions vs more than 10 sessions. |
Type of acupuncture Different types of acupuncture were adopted in the reviewed studies. Acupuncture was effective in both the individualized adapted acupuncture group (SMD: −0.34, 95% CI, −0.56, −0.11, P=0.003, I2=0%) and the standardized acupuncture group (SMD: −0.47, 95% CI, −0.89, −0.06, P=0.03, I2=75%). However, in the standardized treatment subgroup, the effect became ineffective after two studies were removed.27,29
Number of sessions We also performed subgroup analyses based on treatment duration (less than 10 sessions vs more than 10 sessions). Only three studies had fewer than 10 treatment sessions. The results showed short-term analgesic effect for less than 10 sessions (SMD: −0.36, 95% CI, −0.69, −0.03, P=0.03, I2=0%) and for more than 10 sessions (SMD: −0.44, 95% CI, −0.77, −0.12, P=0.007, I2=68%). Sensitivity analysis showed that acupuncture with less than 10 sessions did not produce an effect after removing a study.19 Thus, the result was not robust.
Fatigue
The studies included in the analysis used VAS, Fatigue Severity Scale, and Multi-dimensional Fatigue Inventory to measure the fatigue outcome. Higher scores indicated more fatigue. For short-term efficacy, our meta-analysis demonstrated that acupuncture did not relieve fatigue in patients with FM compared with the control group (SMD: −0.03, 95% CI, −0.42, 0.35, P=0.87, I2=54%) (Supplementary Figure 2). The heterogeneity of fatigue results changed significantly when two studies were removed.21,27 The quality of evidence was rated as low for the comparison of the acupuncture and control groups.
Two studies have reported the long-term effects of acupuncture on fatigue.21,23 Pooled effect showed that acupuncture had no long-term effect on improving fatigue in patients with FM (SMD: 0.04, 95% CI, −0.52, 0.59, P=0.9, I2=58%).
Sleep
The pooled effects of acupuncture on sleep were analyzed in two studies.23,29 Sleep quality was measured on VAS and Nottingham Health Profile (NHP) sleep subscale, with lower scores indicating better sleep quality. Very low quality of evidence showed that acupuncture had no effect on sleep quality in the short term (SMD: 0.08, 95% CI, −0.59, 0.76, P=0.06, I2=0%) or in the long term (SMD: −0.64, 95% CI, −1.77, 0.49, P=0.27, I2=86%) (Supplementary Figure 3).
Physical Function
Three studies were included to quantitatively analyze the short-term effects of acupuncture on physical function, as measured by the Short Form-36 questionnaire.22,26,27 Our results demonstrated that acupuncture did not improve physical function in patients with FM (SMD: 0.14, 95% CI, −0.51, 0.79, P=0.67, I2=83%) (Supplementary Figure 4). Sensitivity analysis indicated that the results were unreliable, and the quality of evidence was low.
Three studies reported follow-up results of acupuncture on physical function, two of which were meta-analyzed.23,29 Physical function in the two studies included in the quantitative analysis was assessed using the subscale of the Fibromyalgia Impact Questionnaire (FIQ) and NHP questionnaires. The pooled effect size of acupuncture was −0.25 (95% CI, −0.91, 0.41, P=0.46, I2=63%), suggesting that acupuncture did not produce a long-term beneficial effect on physical function in FM subjects.
Stiffness
Two studies reported short-term effects of acupuncture on stiffness,19,23 and only one reported long-term effects.23 Our results suggested that acupuncture did not relieve stiffness in patients with FM, regardless of short-term (SMD: −0.38, 95% CI, −0.77, 0.01) (Supplementary Figure 5) or long-term effects (SMD: −0.13, 95% CI, −0.69, 0.43). The quality of evidence for both short- and long-term effects of stiffness was low.
Well-Being
Well-being outcomes were reported in five studies, measured by FIQ in four studies23,26,27,29 and VAS in one article.21 Meta-analysis results showed that acupuncture improved well-being in patients with FM compared with controls (SMD: −0.86, 95% CI, −1.49, −0.24) (Supplementary Figure 6). The quality of evidence was assessed as low. In addition, the pooled effect size of well-being follow-up results indicated the effectiveness of acupuncture (SMD: −0.58, 95% CI, −0.82, −0.35). Sensitivity analysis showed that the follow-up results of acupuncture improving well-being were stable, and the quality of evidence was moderate.
Safety
Among the 13 studies included in the systematic review, two studies had no adverse reactions, and four studies reported unpleasantness of needle insertion, bruising, nausea, fainting, and other adverse events. The seven remaining articles did not report the outcome of adverse events. Our results showed that the incidence of adverse events did not differ significantly between the acupuncture group and the control group (RR: 0.44, 95% CI, 0.12, 1.63, P=0.22, I2=67%) (Figure 4).
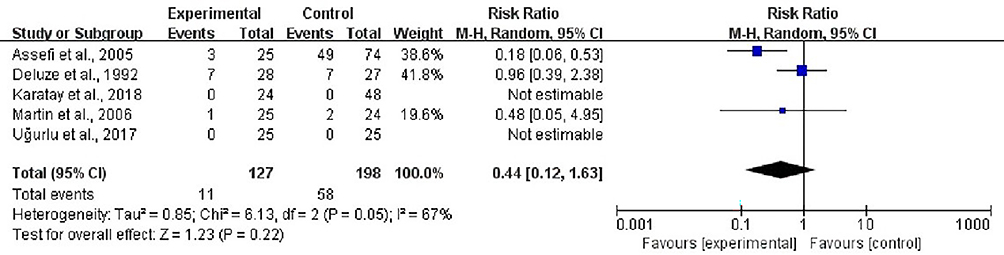 |
Figure 4 The forest plot of adverse events. |
Publication Bias
A funnel plot was qualitatively examined for publication bias (Figure 5). We also conducted egger test to quantitatively detect the symmetry of the funnel plot (P=0.235). Despite the limited number of studies, no potential publication bias was detected.
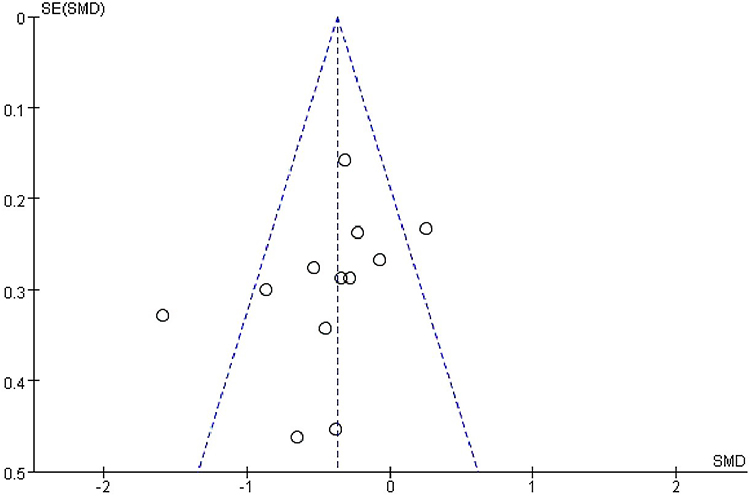 |
Figure 5 Publication bias funnel plots of standard errors and effect sizes of the included studies. |
Discussion
Summary of Main Results
This meta-analysis included 12 studies with 715 participants comparing the effects of real acupuncture with control intervention. The results indicated that acupuncture could effectively relieve pain and improve well-being in patients with FM, with both short - and long-term benefits. However, acupuncture had no effect on fatigue, sleep, physical function, and stiffness compared with control treatment. The subgroup analysis indicated that the real acupuncture group produced more analgesic effects than the control group, with different number of sessions, types of acupuncture, and stimulation. In addition, acupuncture was not associated with serious reactions and had a reliable safety profile.
Interpreting the Findings
SMD used in meta-analysis is an effect size called Hedges g. According to Cohen’s classification of effect size, our results showed that acupuncture had a small analgesic effect on FMS.32 Acupuncture may activate various bioactive chemicals such as opioids and serotonin to relieve pain through peripheral, spinal, and supraspinal mechanisms.24,33,34 A recent neuroimaging study suggested that acupuncture regulates somatosensory functional connectivity and is associated with insula gamma-aminobutyric acid to produce analgesia.30 Simulated acupuncture may also produce physiological responses similar to real acupuncture but with much weaker intensity. Studies have shown that EA may alleviate pain by inhibiting COX-2 and upregulating endocannabinoid.34,35 In addition, thalamocortical network dysfunction is considered as a possible pathophysiological mechanism of fibromyalgia.36 Pulvinar is a very important but less noticed brain region in the thalamus, which is widely connected to cortical and subcortical structures and plays an important role in visual detection, auditory processing, pain modulation, and multisensory integration.37–40 A recent study suggested that fibromyalgia patients exhibit structural abnormalities and functional network dysfunction in the pulvinar nucleus, which is associated with abnormal pain perception and modulation.36 Acupuncture may alleviate pain by regulating the neural circuits of pain, which deserves further exploration by future research. Furthermore, acupuncture can increase the local blood flow of skin and muscles to relieve the pain of patients with FM.11 The degree and duration of increased microcirculation may depend on the depth of acupuncture and the patient’s health condition.11
Our subgroup analysis showed that the real acupuncture was superior to the control intervention for different types of stimulation and acupuncture, as well as for different number of sessions. Our results were in contradiction with those of our predecessor, suggesting that acupuncture showed analgesic effects only in the EA subgroup, the personalized treatment subgroup, or the subgroup less than 10 sessions.14 However, our sensitivity analysis demonstrated that the results were not robust in the EA subgroup, the standardized acupuncture subgroup, and the subgroup with less than 10 sessions. In the standardized acupuncture subgroup, the confidence interval of the results was quite wide, which reduced the reliability of the results. Therefore, we recommend more than 10 sessions of personalized manual acupuncture to relieve pain.
Complete blinding is usually difficult to achieve in acupuncture research, and the bias caused by incomplete blinding may lead to low reliability of the research results.33 In all experiments, the acupuncturist knew the grouping of each subject. Although studies have blinded the subjects, they may not be completely successful. In addition, during acupuncture treatment, the acupuncturist will communicate closely with the patient, usually involving some suggestive sentences. For example, the acupuncturist will ask the subject whether he feels angry after acupuncture, which may partly explain the small effect observed.41
In addition to short- and long-term effects on well-being, acupuncture had no significant effect on other important outcome measures of FM, including fatigue, sleep quality, physical function, and stiffness. A systematic review of eight RCTs concluded that acupuncture can improve the sleep quality and overall well-being in patients with FM.17 An earlier review concluded that acupuncture is not effective in improving fatigue, sleep quality, or physical function.14 These results should be treated with caution, as the small number of included studies and sample sizes may result in inaccurate results. In addition, the quality of evidence was evaluated as very low to moderate. Therefore, more clinical studies may be needed to explore the effects of acupuncture in the future.
Comparisons with Other Reviews
Several previous reviews have also examined the effect of acupuncture on FM syndrome, with mixed results. A high-quality systematic review of seven RCTs published in 2010 showed a small analgesic effect after acupuncture (SMD: 0.25, 95% CI, 0.49, 0.02, P = 0.04).14 However, this review does not recommend acupuncture for the treatment of FM due to the risk of bias. A Cochrane systematic review published in 2013 indicated that acupuncture did not relieve pain or fatigue, nor did it improve sleep quality or global well-being compared with sham acupuncture.15 Another meta-analysis showed moderate quality of evidence supporting acupuncture for the management of pain in FM compared with medication or sham acupuncture, but unclear therapeutic effects for other key symptoms of FM were noted.16 Another review of eight articles demonstrated that real acupuncture is more effective than sham acupuncture in alleviating pain and improving sleep quality and general health but not fatigue.17 Overall, the available evidence on the effectiveness of acupuncture for FM is controversial, especially for other important symptoms besides pain such as fatigue, stiffness, and sleep quality.
Compared with previous studies, we added three RCT studies and systematically assessed the effects of acupuncture on pain, fatigue, sleep, physical function, stiffness, well-being, and safety in patients with FM. We used SMD to calculated the pooled effect size of different scale data to aggregate more evidence. Our results were consistent with recent reviews that acupuncture can produce analgesic effects in patients with FM.16,17 However, our review concluded that acupuncture lacks effectiveness in treating other symptoms of FM, including fatigue, sleep, stiffness, and physical function. Notably, the publication bias was quantitatively analyzed, and the results showed no potential publication bias. We believe that our updated and more comprehensive evidence of acupuncture for FM may provide a better reference for medical practitioners.
Limitations and Clinical Implications
This review had some limitations. The main disadvantage is the limited number of articles and research subjects included in this systematic review, which may lead to inaccurate results. Considering the difficulty of including all grey literature and extracting their data, we did not include grey literature in this meta-analysis. Given the absence of publication bias, we consider our results based on current retrieval strategies to be reliable. Finally, systematic reviews may overstate the effectiveness of acupuncture, because some of the RCTs did not minimize the risk of bias.42,35
In view of the above limitations, future studies with large sample sizes and rigorous design should be conducted to improve the quality of evidence. The Standards for Reporting Interventions in Controlled Studies of Acupuncture guidelines should be used to accurately report acupuncture interventions.13 Considering that FM is a syndrome of widespread pain with multiple symptoms, future research should conduct a more comprehensive evaluation to determine the efficacy of acupuncture on FM. In addition, the incidence of adverse events and loss of follow-up should be reported.
Conclusion
In conclusion, low to moderate quality of evidence suggests that real acupuncture is more effective than control treatment in alleviating pain and improving well-being in both the short- and long-term. Furthermore, we believe that manual acupuncture with at least 10 sessions can achieve better analgesic effect. However, acupuncture has no effect on improving other symptoms of FM, including fatigue, sleep quality, physical function, and stiffness. We consider acupuncture to be a potentially effective and safe way to manage FM, but the impact on practice is limited. In addition, large-scale trials are needed to explore the long-term clinical efficacy of acupuncture on FM and to explore the underlying mechanisms of acupuncture.
Acknowledgment
We are very grateful to Xue Jiang for her help in using the software for data analysis.
Disclosure
The authors declare that they have no known conflicts of interest.
References
1. Sarzi-Puttini P, Giorgi V, Marotto D, et al. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020;16(11):645–660. doi:10.1038/s41584-020-00506-w
2. Spaeth M. Epidemiology, costs, and the economic burden of fibromyalgia. Arthritis Res Ther. 2009;11(3):117. doi:10.1186/ar2715
3. Häuser W, Ablin J, Fitzcharles MA, et al. Fibromyalgia. Nat Rev Dis Primers. 2015;1:15022. doi:10.1038/nrdp.2015.22
4. Lachaine J, Beauchemin C, Landry PA. Clinical and economic characteristics of patients with fibromyalgia syndrome. Clin J Pain. 2010;26(4):284–290. doi:10.1097/AJP.0b013e3181cf599f
5. Berger A, Dukes E, Martin S, et al. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract. 2007;61(9):1498–1508. doi:10.1111/j.1742-1241.2007.01480.x
6. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76(2):318–328. doi:10.1136/annrheumdis-2016-209724
7. Bair MJ, Krebs EE. Fibromyalgia. Ann Intern Med. 2020;172(5):Itc33–itc48. doi:10.7326/AITC202003030
8. Coutaux A. Non-pharmacological treatments for pain relief: TENS and acupuncture. Joint Bone Spine. 2017;84(6):657–661. doi:10.1016/j.jbspin.2017.02.005
9. Tang Y, Yin HY, Rubini P, et al. Acupuncture-induced analgesia: a neurobiological basis in purinergic signaling. Neuroscientist. 2016;22(6):563–578. doi:10.1177/1073858416654453
10. Ondrejkovicova A, Petrovics G, Svitkova K, et al. Why acupuncture in pain treatment? Neuro Endocrinol Lett. 2016;37(3):163–168.
11. Kim SY, Min S, Lee H, et al. Changes of local blood flow in response to acupuncture stimulation: a systematic review. Evid Based Complement Alternat Med. 2016;2016:9874207. doi:10.1155/2016/9874207
12. Di Carlo M, Beci G, Salaffi F. Pain changes induced by acupuncture in single body areas in fibromyalgia syndrome: results from an open-label pragmatic study. Evid Based Complement Alternat Med. 2021;2021:9991144. doi:10.1155/2021/9991144
13. Di Carlo M, Beci G, Salaffi F. Acupuncture for fibromyalgia: an open-label pragmatic study on effects on disease severity, neuropathic pain features, and pain catastrophizing. Evid Based Complement Alternat Med. 2020;2020:9869250. doi:10.1155/2020/9869250
14. Langhorst J, Klose P, Musial F, et al. Efficacy of acupuncture in fibromyalgia syndrome-A systematic review with a meta-analysis of controlled clinical trials. Rheumatology. 2010;49(4):778–788. doi:10.1093/rheumatology/kep439
15. Deare JC, Zheng Z, Xue CC, et al. Acupuncture for treating fibromyalgia. Cochrane Database Syst Rev. 2013;2013(5):Cd007070.
16. Zhang XC, Chen H, Xu WT, et al. Acupuncture therapy for fibromyalgia: a systematic review and meta-analysis of randomized controlled trials. J Pain Res. 2019;12:527–542. doi:10.2147/JPR.S186227
17. Kim J, Kim SR, Lee H, et al. Comparing verum and sham acupuncture in fibromyalgia syndrome: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2019;2019:8757685. doi:10.1155/2019/8757685
18. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. doi:10.1002/art.1780330203
19. Deluze C, Bosia L, Zirbs A, et al. Electroacupuncture in fibromyalgia: results of a controlled trial. BMJ. 1992;305(6864):1249–1252. doi:10.1136/bmj.305.6864.1249
20. Sprott H. Efficiency of acupuncture in patients with fibromyalgia. Clin Bull Myofascial Therapy. 1998;3(1):37–43. doi:10.1300/J425v03n01_05
21. Assefi NP, Sherman KJ, Jacobsen C, et al. A randomized clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. Ann Intern Med. 2005;143(1):10–19. doi:10.7326/0003-4819-143-1-200507050-00005
22. Harris RE, Tian X, Williams DA, et al. Treatment of fibromyalgia with formula acupuncture: investigation of needle placement, needle stimulation, and treatment frequency. J Altern Complement Med. 2005;11(4):663–671. doi:10.1089/acm.2005.11.663
23. Martin DP, Sletten CD, Williams BA, et al. Improvement in fibromyalgia symptoms with acupuncture: results of a randomized controlled trial. Mayo Clin Proc. 2006;81(6):749–757. doi:10.4065/81.6.749
24. Harris RE, Zubieta JK, Scott DJ, et al. Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on mu-opioid receptors (MORs). Neuroimage. 2009;47(3):1077–1085. doi:10.1016/j.neuroimage.2009.05.083
25. Harte SE, Clauw DJ, Napadow V, et al. Pressure pain sensitivity and insular combined glutamate and glutamine (Glx) are associated with subsequent clinical response to sham but not traditional acupuncture in patients who have chronic pain. Med Acupunct. 2013;25(2):154–160. doi:10.1089/acu.2013.0965
26. Vas J, Santos-Rey K, Navarro-Pablo R, et al. Acupuncture for fibromyalgia in primary care: a randomised controlled trial. Acupunct Med. 2016;34(4):257–266. doi:10.1136/acupmed-2015-010950
27. Uğurlu FG, Sezer N, Aktekin L, et al. The effects of acupuncture versus sham acupuncture in the treatment of fibromyalgia: a randomized controlled clinical trial. Acta Reumatol Port. 2017;42(1):32–37.
28. Zucker NA, Tsodikov A, Mist SD, et al. Evoked pressure pain sensitivity is associated with differential analgesic response to verum and sham acupuncture in fibromyalgia. Pain Med. 2017;18(8):1582–1592. doi:10.1093/pm/pnx001
29. Karatay S, Okur SC, Uzkeser H, et al. Effects of acupuncture treatment on fibromyalgia symptoms, serotonin, and substance P levels: a randomized sham and placebo-controlled clinical trial. Pain Med. 2018;19(3):615–628. doi:10.1093/pm/pnx263
30. Mawla I, Ichesco E, Zöllner HJ, et al. Greater somatosensory afference with acupuncture increases primary somatosensory connectivity and alleviates fibromyalgia pain via insular γ-aminobutyric acid: a randomized neuroimaging trial. Arthritis Rheumatol. 2021;73(7):1318–1328. doi:10.1002/art.41620
31. Stival RS, Cavalheiro PR, Stasiak CE, et al. Acupuncture in fibromyalgia: a randomized, controlled study addressing the immediate pain response. Rev Bras Reumatol. 2014;54(6):431–436. doi:10.1016/j.rbr.2014.06.001
32. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale: Lawrence Erlbaum Associates. 1988:1007.
33. Madsen MV, Gøtzsche PC, Hróbjartsson A. Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ. 2009;338:a3115. doi:10.1136/bmj.a3115
34. Zhang R, Lao L, Ren K, et al. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
35. Anand P, Whiteside G, Fowler CJ, et al. Targeting CB2 receptors and the endocannabinoid system for the treatment of pain. Brain Res Rev. 2009;60(1):255–266. doi:10.1016/j.brainresrev.2008.12.003
36. Kim DJ, Lim M, Kim JS, et al. Structural and functional thalamocortical connectivity study in female fibromyalgia. Sci Rep. 2021;11(1):23323. doi:10.1038/s41598-021-02616-1
37. Chou XL, Fang Q, Yan L, et al. Contextual and cross-modality modulation of auditory cortical processing through pulvinar mediated suppression. Elife. 2020;9:e54157. doi:10.7554/eLife.54157
38. Fang Q, Chou XL, Peng B, et al. A differential circuit via retino-colliculopulvinar pathway enhances feature selectivity in visual cortex through surround suppression. Neuron. 2020;105(2):355–369.e356. doi:10.1016/j.neuron.2019.10.027
39. Ibrahim LA, Mesik L, Ji XY, et al. Cross-modality sharpening of visual cortical processing through Layer-1-Mediated inhibition and disinhibition. Neuron. 2016;89(5):1031–1045. doi:10.1016/j.neuron.2016.01.027
40. Froesel M, Cappe C, Ben Hamed S. A multisensory perspective onto primate pulvinar functions. Neurosci Biobehav Rev. 2021;125:231–243. doi:10.1016/j.neubiorev.2021.02.043
41. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998;352(9125):364–365. doi:10.1016/S0140-6736(97)10471-8
42. Derry C, Derry S, McQuay H, et al. Systematic review of systematic reviews of acupuncture published 1996–2005. Clin Med. 2006;6(4):381–386. doi:10.7861/clinmedicine.6-4-381
43. Moher D, Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.