Back to Journals » International Journal of Women's Health » Volume 12
Effect of a Health-Education Program Based on the BASNEF Model of Overall Sexual Health Satisfaction and Satisfaction with Quality of Sexual Relationship among Women with Infertility
Authors Shahbazi A ![]() , Behboodi Moghadam Z
, Behboodi Moghadam Z ![]() , Maasoumi R, Saffari M, Mohammadi S, Montazeri A
, Maasoumi R, Saffari M, Mohammadi S, Montazeri A ![]()
Received 7 February 2020
Accepted for publication 20 October 2020
Published 4 November 2020 Volume 2020:12 Pages 975—982
DOI https://doi.org/10.2147/IJWH.S248734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Azade Shahbazi,1 Zahra Behboodi Moghadam,1 Raziyeh Maasoumi,1 Mohsen Saffari,2 Saeed Mohammadi,1 Ali Montazeri3
1Reproductive Health Department, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran; 2Health Research Centre, Life Style Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran; 3Population Health Research Group, Health Metrics Research Center, Iranian Institute for Health Sciences Research, ACECR, Tehran, Iran
Correspondence: Azade Shahbazi; Ali Montazeri Email [email protected]; [email protected]
Introduction: Female infertility is increasing in Iran, encompassing all dimensions of women’s lives. One of the most important effects of infertility is on sexual function. All women have the right to sexual health. Using educational models, one can see a positive effect on women’s sexual function. The present study aimed to investigate the effect of an education program based on the beliefs, attitudes, subjective norms, and enabling factors (BASNEF) model on promoting overall sexual health satisfaction and satisfaction with the quality of sexual relationships among women with infertility.
Methods: This was a quasiexperimental study conducted on 80 infertile women referred to an infertility center affiliated with Tehran University of Medical Sciences, in Tehran, Iran in 2016– 2017. Infertile women with primary infertility were divided into experimental and control groups based on odd and even days. The intervention was carried out based on the BASNEF model over four sessions. Data were collected using a demographic questionnaire, the BASNEF questionnaire, and items on overall sexual health satisfaction and satisfaction with their sexual relationship. The questionnaires were completed before and 4 and 8 weeks after the intervention in the two groups. Friedman, χ2, and t-tests were used for data analysis.
Results: After the educational intervention, BASNEF values and overall sexual function and satisfaction with the quality of sexual relationships had significantly improved in the experimental group (p< 0.05), while changes were not significant in the control group.
Conclusion: The results showed that the BASNEF model–based educational invention improved overall sexual health and satisfaction among intertitle women. Indeed, it seems that using theory-based educational interventions in infertility centers might be helpful.
Keywords: infertility, sexual function, female, reproductive health
Introduction
Infertility is defined by the World Health Organization as “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse”.1 The number of infertile women is constantly increasing. It has been estimated that approximately 72.4 million women worldwide are infertile.2 More than 20% of Iranian couples experience infertility during their reproductive life.3,4 As a medical and social issue, infertility is an important stress for couples.5 Evaluation and treatment of infertility with extensive laboratory workup, serial follow-up ultrasonography, strict coital rules, and unsuccessful cycles can have a detrimental effect on sexual life of couples. It has been reported that health problems, loss of self-esteem, feeling akin to mourning, threat, sexual distress, depression, guilt, anxiety, frustration, emotional distress, and marital problems are all associated with infertility.6
Although infertile women and men are emotionally affected, women seem to experience more stress, pressure, and a higher rate of anxiety and depression.7 During the treatment of infertility, 50%–60% of couples express a marked decrease in sexual satisfaction. Research has shown that lack of sexual health is closely linked to many social problems, such as crime, rape, mental illness, and divorce.8 Studies have shown that infertility is one of the factors affecting sexuality and ultimately the sexual functioning of couples, especially women. In such situations, sexual activity is accompanied by feelings of fear, failure, inefficiency, and loss, or if forced it ultimately leads to loss of sexual desire, lack of orgasm, and other sexual disorders.9 In many cultures, womanhood is defined through motherhood, and infertile women usually carry the blame for a couple’s inability to conceive. Infertile women are frequently stigmatized, resulting in isolation, neglect, domestic violence, and polygamy.10,11
All women should be entitled to sexual and reproductive health. Infertile women are vulnerable because their special sexual and reproductive status.12–14 Sexual health is part of reproductive health, which is a requirement and strategy for achieving the Millennium Development Goals.15 According to the World Health Organization, sexual health is physical, mental, psychological, and social welfare related to sexual desire, and does not just include absence of a disease or disorder. Sexual health is a positive move for sexuality and the possibility of having a safe and desirable sexual experience, away from threats, coercion, discrimination, and violence. In order to achieve and maintain sexual health, everyone’s sexual rights must be recognized, protected, and strengthened.
The motto “A woman’s pathway to health” is the special attention to sexual health education.16 Given that one of the goals of education can be behavioral change, the understanding of behavior afforded by various behavior-change theories provides insight into the formulation of effective teaching methods for this purpose.17,18 One of these models is the beliefs, attitudes, subjective norms, and enabling factors (BASNEF), model as explained by John Hubley, which includes beliefs regarding behavioral outcomes, attitudes toward behavior, subjective norms and enabling factors. This model is a combination of the Precede–Proceed model and expectancy-value theory.19,20 The most significant construct of the BASNEF model is the behavior change.19 Beliefs and attitudes are influenced by culture, values, traditions, education, the media, and personal experiences. Subjective norms include family, society, social media, and peer pressure. Enabling factors can be income, women’s status, time, and skills.19,21 This model can be proposed as a new educational method.22 In developing countries, the BASNEF model is used to meet the health-education needs of society.19 However, since infertility is one of the major causes of sexual dysfunction and marital dissatisfaction, it is necessary to pay attention to the relationship between marital satisfaction and positive moods, such as happiness.23,24 The present study was conducted to determine the effect of education based on the BASNEF model on promoting overall sexual health satisfaction and satisfaction with quality of sexual relationships among infertile women.
Methods
Design
This was a quasiexperimental clinical trial including an experimental and a control group conducted at an infertility center affiliated with Tehran University of Medical Sciences in Tehran, Iran in 2016–2017 (IRCT registration IRCT201301189463N12). The trial commenced on October 22, 2016, but registration was not finalized until January 2, 2017.
Participants
Women with primary infertility were eligible for the study. Inclusion criteria were history of at least 4 years of primary infertility, no history of participation in educational or counseling classes focusing on sexual function, no alcohol or drug use, no chronic disease, no psychological disorder, and not taking medication for sexual functioning. Women were excluded if they had been pregnant or did not wish to participate in educational sessions. Continuous sampling was carried out on a daily basis. Those attending the center on even days were assigned to the experimental group, and those attending on odd days were assigned to the control group. All subjects signed a written informed-consent form.
Intervention
The content of the intervention was prepared based on pretesting and using validated scientific resources. The experimental group was divided into groups of five to ten. Four sessions of 60–90 minutes were held once a week. At the first session, the women’s awareness of infertility, their sexual health, and their attitudes toward these issues were considered. At the second session, subjective norms, ie, social pressures, were discussed. The third session covered topics on enabling factors, such as marital counseling, and introducing. During the final session, the contents were reviewed and summarized. A manual was provided to the control group after completion of the study.
Study Instrument
Data were collected using a questionnaire containing three sections:
- Demographics, including items on age, marriage, and infertility duration.
- Items based on the BASNEF model, containing questions on beliefs, attitudes, subjective norms, and enabling factors. The questionnaire was developed after an extensive literature review. Content validity was evaluated by ten experts on reproductive health and health education, and Cronbach’s α was estimated to assess the reliability of the BASNEF questionnaire in the target group. The questionnaire was distributed to a sample of 20 women, and it was found that it had good internal consistency (α=0.84).
- Regarding sexual health satisfaction and satisfaction with quality of sexual relationships, a single item was used to assess whether women were satisfied with their sexual health or not. Additionally, we assessed satisfaction with quality of sexual relationships using a single item. Response categories for both items were in “yes and no” format.
The questionnaire was administered to both groups before and at 1 and 2 months after the intervention.
Sample Size

assuming that a 35% improvement in sexual health among the intervention group and a 5% improvement among the control group would occur, it was estimated that a study with 80% power at 5% significance needed at least need 34 women per group. Considering a 20% dropout rate, we recruited 40 women per group. A study flowchart is presented in Figure 1.
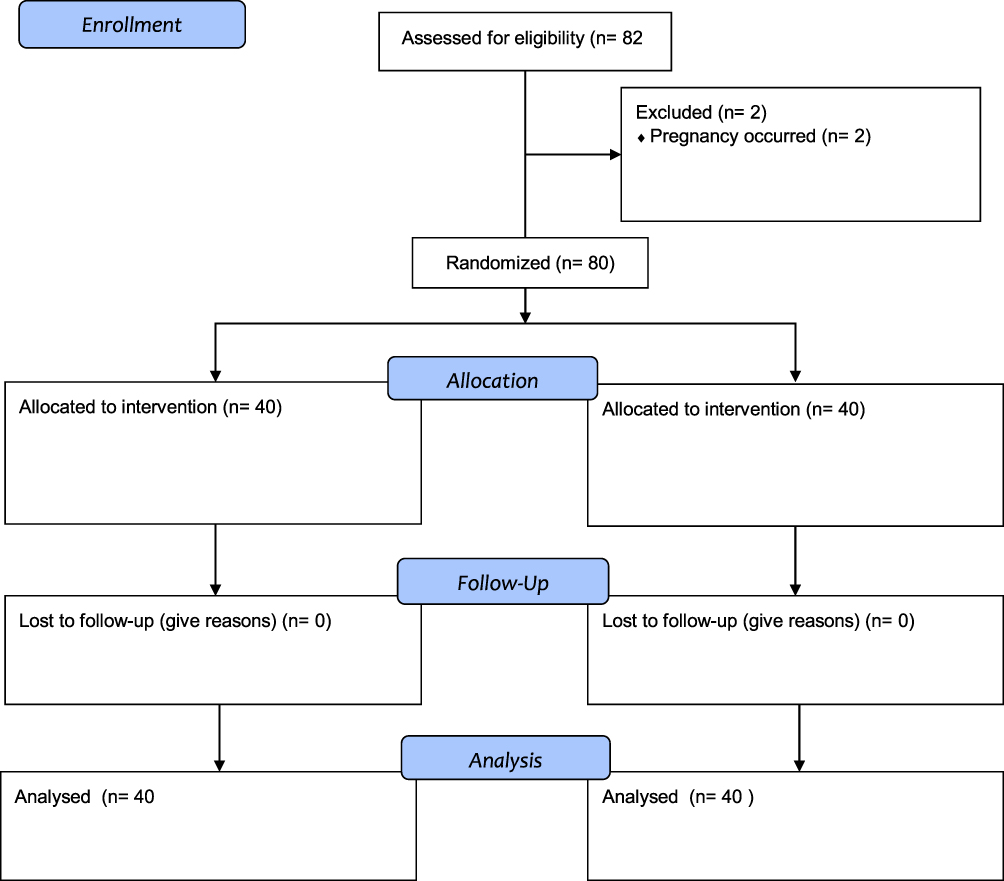 |
Figure 1 Study flowchart. |
Statistical Analysis
Data analysis was performed using SPSS version 20.IBM, Armonk, NY). Descriptive statistics, — frequency, percentage, and means ± SD — was used to explore the data. To compare data within groups, repeated-measure analysis for qualitative data and Friedman’s test for quantitative data wer performed. Between-group comparisons were carried out using χ2 and t-tests. Significance level set at P<0.05.
Ethics
The study was carried out with accordance with the Declaration of Helsinki. The ethics committee of Tehran University of Medical Sciences approved the study (IR.TUMS.FNM.REC.1395.596). All participants signed informed consent.
Results
Characteristics of Subjects
Characteristics of the study samples are shown in Table 1. There were no significant differences between the experimental and control groups. The mean age in the two groups was 31 years and that of the husband 35 years (P>0.05). Furthermore, there were no significant differences in lifetime frequency of infertility treatment between the groups. The majority in both groups were housewives.
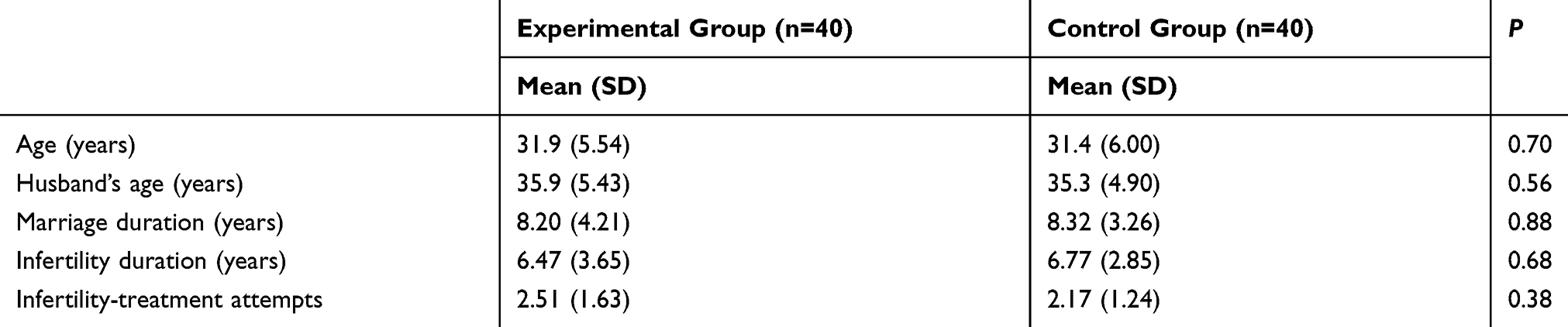 |
Table 1 Demographic Characteristics of Study Subjects |
Findings for BASNEF Constructs
Mean scores for beliefs in the experimental and control groups were not significantly different before intervention, while after the end of the intervention, belief scores had increased significantly in the experimental group (Table 2). Attitude scores increased in the experimental group, and these changes were significant compared to the control group (Table 3). For the construct of subjective norms assessed by perceived changes in husband’s behavior, the results showed no significant differences in either groups before, 1 month, or two months after the intervention. The results are presented in Table 4. For the construct of enabling factors evaluated by the women’s intention to seek sexual counseling, a significant improvement was observed for the experimental group, but not for the control group. The results are shown in Table 5.
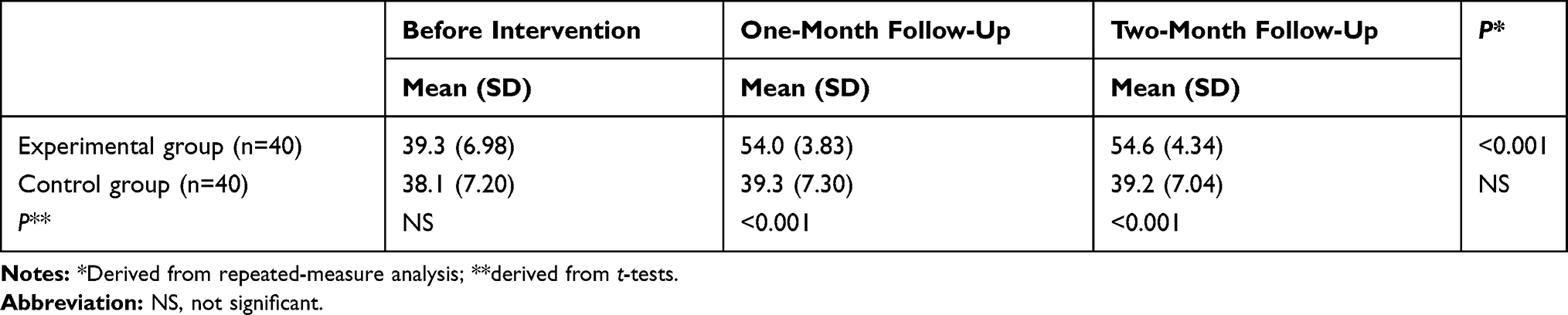 |
Table 2 Comparison of Belief Scores in Experimental and Control Groups |
 |
Table 3 Comparison of Attitude Scores in Experimental and Control Groups |
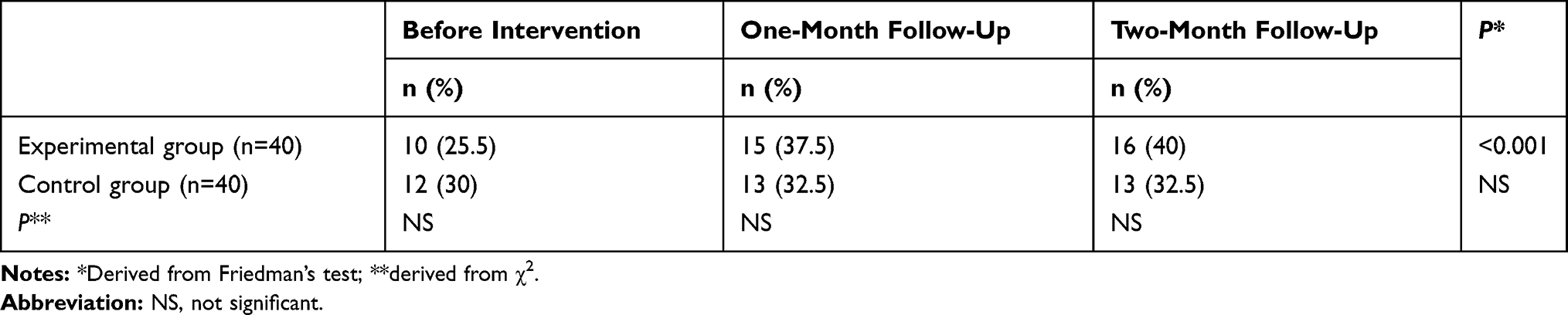 |
Table 4 Comparison of Subjective Norms (Perceived Changes in Husband’s Behavior) in Experimental and Control Groups (Frequency of Positive Responses) |
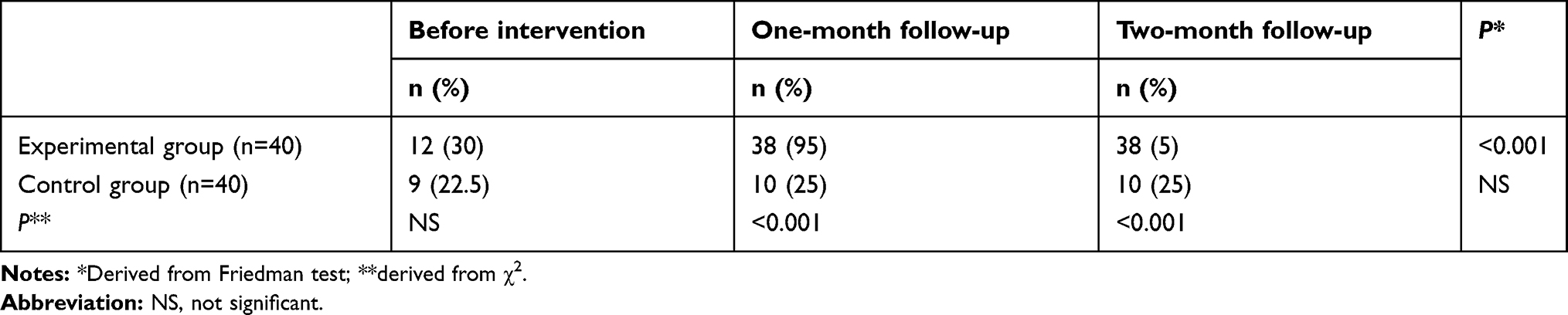 |
Table 5 Comparing Enabling Factors (Intent for Sexual Counseling) in Experimental and Control Groups (Frequency of Positive Responses) |
Overall Sexual Health Satisfaction and Satisfaction with Quality of Sexual Relationships
The results showed significant improvements for overall sexual health satisfaction and satisfaction with quality of sexual relationships among women in the experimental group, whereas no differences were observed in the control group. The results are shown in Tables 6 and 7. increase in
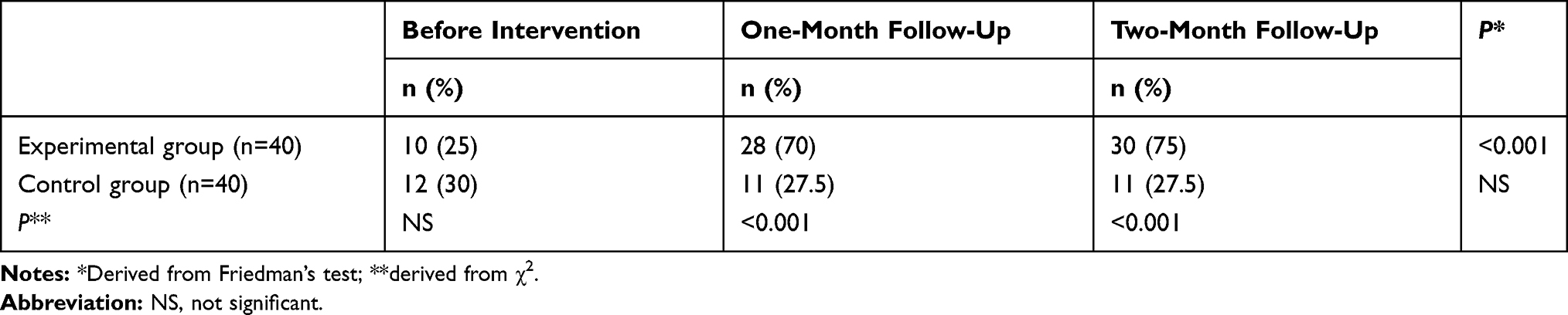 |
Table 6 Overall Sexual Health Satisfaction in Experimental and Control Groups (Frequency of Positive Responses) |
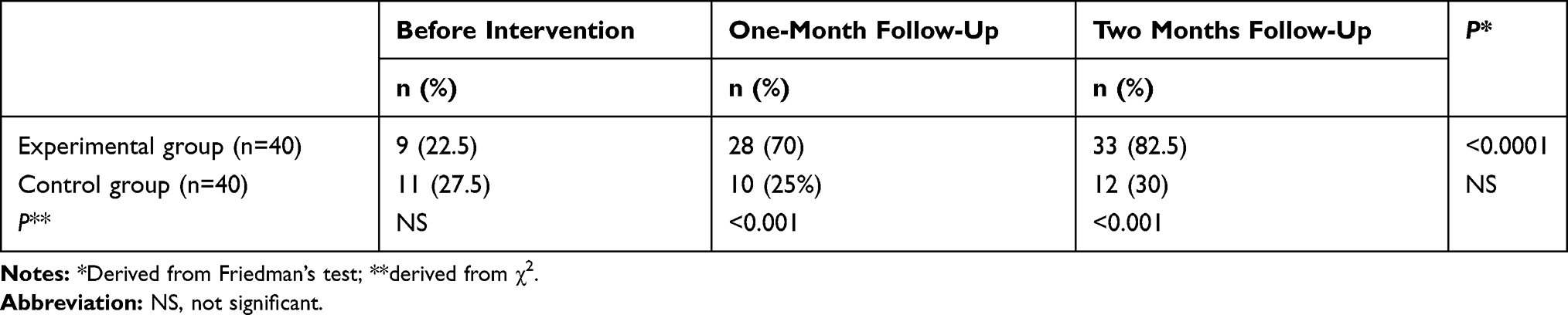 |
Table 7 Satisfaction with Quality of Sexual Relationship (Frequency of Positive Responses) |
Discussion
The findings from this study indicate that educational interventions are potentially able to improve sexual satisfaction among infertile women. In a study by Winkelman et al, younger age and infertility due to female problems were the main causes of sexual dysfunction in infertile women.25 Bayar et al found that infertility was one of the major causes of sexual dysfunction and indicated that it is necessary to pay attention to this issue.26 In general, the BASNEF model has been found to be a useful framework for change in beliefs and attitudes.27 We also found that the educational intervention based on the BASNEF model increased belief and attitude scores. Perhaps these occurred because during the sessions, we discussed topic that changed attitudes toward sexual health and altered thoughts about infertility. Concerning subjective norms, the results were promising. However, based on the observations of the main investigator in the educational sessions, infertile women had problems in sexual self-regulation and sexual self-efficacy. Because of feeling deficient, these women stayed away from sexual relationships. It has been argued that individual factors, such as stress, false beliefs, and self-blame, have various effects on sexual health that in turn can affect sexual activity. In a study on the effect of sexual education based on the theory of planned behavior on sexual functioning in women, there was no significant difference in the subjective norms of the two groups after the intervention.28
Enabling factors were assessed with regard to seeking sexual counseling. The two groups were homogeneous before the study. However, after the intervention and understanding of subjects about the need to seek help from experienced experts, the intervention group showed significant improvement. We think this happened because of improvements in their capacity for effective communication with their partner as a powerful factor. Similar observations have been reported by other investigators.29–31 Overall sexual health satisfaction and satisfaction with sexual relationships significantly increased among the intervention group. In general, as indicated by other investigators, BASNEF-based educational programs are usually successful in changing behaviors or intentions. For instance, in one study on the effect of educational intervention based on the BASNEF model in promoting the physical activity of women after childbirth, significant behavior and intention changes occurred in the experimental group.32 It clearly indicated that educational programs can lead to satisfaction in marital relationships. Another study showed that after a 12-week intervention, the overall sexual performance of women in the experimental group had improved.33
Limitations
This study had some limitations. One was the short follow-up. Future studies need to follow women for longer. Also, randomization was not complete. We assigned infertile women into the study groups based on odd and even days during a week, and this might have biased the findings. Finally, it seems that a bigger sample is needed to reach firm conclusions.
Conclusion
The results indicated that education based on the BASNEF model had positive effects on sexual health and quality of sexual relationships in infertile women.
Data-Sharing Statement
All data for this study are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank the infertility clinic of Valiasr hospital and Dr Baghery.
Funding
No external funding was received for this paper.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. International Committee for Monitoring Assisted Reproductive T, World Health O. International committee for monitoring assisted reproductive technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92:1520–1524. doi:10.1016/j.fertnstert.2009.09.009
2. Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Hum Reprod. 2007;22(6):1506–1512. doi:10.1093/humrep/dem046
3. Direkvand Moghadam A, Delpisheh A, Sayehmiri A. The prevalence of infertility in Iran, a systematic review. Iran J Obstetrics Gynecol Infertility. 2013;16:1–7.
4. Kazemijaliseh H, Ramezani Tehrani F, Behboudi-Gandevani S, Hosseinpanah F, Khalili D, Azizi F. The prevalence and causes of primary infertility in Iran: a population-based study. Glob J Health Sci. 2015;7:226–232. doi:10.5539/gjhs.v7n6p226
5. Lee TY, Sun GH, Chao SC. The effect of an infertility diagnosis on the distress, marital and sexual satisfaction between husbands and wives in Taiwan. Hum Reprod. 2001;16:1762–1767. doi:10.1093/humrep/16.8.1762
6. Edelmann RJ, Connolly KJ. Psychological aspects of infertility. Br J Med Psychol. 1986;59:209–219. doi:10.1111/j.2044-8341.1986.tb02686.x
7. Schweiger U, Wischmann T, Strowitzki T. Mental disorders and female infertility. Nervenarzt. 2012;6:6.
8. Eren N The effect of perceived social support in infertile couples on infertility related stress and marriage harmony [master’s thesis]. Ankara, Turkey: Gazı University, Ankara; 2008
9. Monga M, Alexandrescu B, Katz SE, Stein M, Ganiats T. Impact of infertility on quality of life, marital adjustment, and sexual function. Urology. 2004;63–126.
10. Eftekhar-Ardabily H, Behboodi-Moghadam Z, Salsali M, Ramezanzadeh F, Nedjat S. Prevalence and risk factors for domestic violence against infertile women in an Iranian setting. Int J Genecol Obstetrics. 2011;112:15–17. doi:10.1016/j.ijgo.2010.07.030
11. Araoye MO. Epidemiology of infertility: social problems of the infertile couple. West African J Med. 2003;22:190–196.
12. World Health Organization. WHO. Defining Sexual Health. Report of a Technical Consultation on Sexual Health 2002. World Health Organization; 2006. Available from: http //www.who.int/reproductivehealth/publications/se xual_health/defining_sexual_health.pdf.
13. Farajkhoda T, Roudsari RL, Abbasi M. Ethical performance in delivery of sexual and reproductive health services: a Delphi study focused on the right of confidentiality. Health Med. 2012;6:3385–3394.
14. Farajkhoda T, Latifnejad Roudsari R, Abbasi M. An exploratory study to develop a practical ethical framework for reproductive health research. Iran J Reprod Med. 2013;11:31–38.
15. Jan Ghorban R, Latifnejad Roodsari R, Taghipoor A, Abbasi M. An overview of the concept and structure of sexual and reproductive rights in international instruments on human rights. J Obstet Gynecol Infertil. 2014;17(100):16–26.
16. Petraten H, Sofia T, Andrea N, Michaela Michel R, Nester T, Bokosi R. Midwifery 2030ʹ: a woman’s pathway to health. What does this mean? Midwifery. 2016;32::1–6. doi:10.1016/j.midw.2015.10.014
17. Giampietro O, Virgone E, Carneglia L, Griesi E, Calvi D, Matteucci E. Anthropometric indices of school children and familiar risk factors. Prev Med. 2002;35(5):492–498. doi:10.1006/pmed.2002.1098
18. Lytle LA. Chapter 4 Nutrition education for school-aged children. J Nutr Educ. 1995;27(6):298–311. doi:10.1016/s0022-3182(12)80090-2
19. Hubley J. Communicating Health. An Action Guide to Health Education and Health Promotion.
20. Hubley J. Understanding behavior: the key to successful health education. Trop Doct. 1988;18(3):134–138. doi:10.1177/004947558801800316
21. Reimers P The influence of the workplace environment on breastfeeding practice of working mothers returning to work: A case study of two companies in KwaZulu-Natal. Dissertation. 2009. Available from: http://ir.dut.ac.za/handle/10321/448?show=full.
22. Hazavehei S, Sharifirad G, Kargar M. The comparison of educational intervention effect Using BASNEF and classic models on improving assertion skill level. J Res Health Sci. 2008;8(1):1–11.
23. Sooky Z, Keramat A, Sharifi K, et al. Investigating happiness and its related factors in married women referred to health centers of shahroud city. Iran Red Crescent Med J. 2014;16:e22211. doi:10.5812/ircmj.22211
24. Monga M, Alexandrescu B, Katz SE, Stein M, Ganiats T. Impact of infertility on quality of life, marital adjustment, and sexual function. Urology. 2004;63:126–130. doi:10.1016/j.urology.2003.09.015
25. Winkelman WD, Katz PP, Smith JF, Rowen TS. Infertility outcomes program project group: the sexual impact of infertility among women seeking fertility care. Sexual Med. 2016;4:e190–7. doi:10.1016/j.esxm.2016.04.001
26. Bayar U, Basaran M, Atasoy N, et al. Sexual dysfunction in infertile couples: evaluation and treatment of infertility. Sexual Dysfunction J Pak Med Assoc. 2014;64:138–145.
27. Ahmadi S, Kazemi F, Masoumi SZ, Parsa P, Roshanaei G. Intervention based on BASNEF model increases exclusive breastfeeding in preterm infants in Iran: a randomized controlled trial. Int Breastfeed J. 2016;11:30. doi:10.1186/s13006-016-0089-2
28. Ebrahimipour H, Jalambadany Z, Peyman N, Ismaili H, Vafaii Najjar A. Effect of sex education, based on the theory of planned behavior, on the sexual function of the woman attending Mashhad health centers. J Birjand Univ Med Sci. 2013;20:58–67.
29. Zareipour MA, Mahmoodi H, Valizadeh R, Ghelich Ghorooji M, Rezaie Moradali M, Zare F. Impact of an educational intervention based on the BASNEF model on skin cancer preventive behavior of college students. Asian Pac J Cancer Prev. 2018;19(10):2717–2722.
30. Rostami Moez M, Hazavehei SM, Moeini B, Karimi Shahanjarini A, Roshanaei G. Effectiveness of educational program based on BASNEF model for using safe contraception methods. J Res Health. 2014;4(2):705–713.
31. Shahnazi H, Koon PB, Talib RA, et al. Can the BASNEF model help to develop self-administered healthy behavior in Iranian youth? Iran Red Crescent Med J. 2016;18:3. doi:10.5812/ircmj.23847
32. Mahububi Rad A, Tol A, Shojaeizadeh D, Yaseri M. The study of the effect of educational intervention based on the BASNEF model in promoting the physical activity of postpartum women. Payesh. 2016;15:462–469.
33. Behboodi Moghadam Z, Rezaei E, Khaleghi Yalegonbadi F, et al. The effect of sexual health education program on women sexual function in Iran. J Res Health Sci. 2015;15:124–128.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.