Back to Journals » Clinical Epidemiology » Volume 18
Ectopic Pregnancy Mortality Trends in BRICS: Age-Period-Cohort Analysis of Global Burden Disease 2021 Data and 2030 Forecast
Authors Xu Y, Liu C, Nan R, Munoz A, Li J
Received 18 November 2025
Accepted for publication 26 February 2026
Published 4 March 2026 Volume 2026:18 582353
DOI https://doi.org/10.2147/CLEP.S582353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Toft Sørensen
Yuting Xu,1,* Chuanna Liu,1,* Ruixing Nan,2 Alvaro Munoz,3 Jiang Li1
1Department of Rehabilitation Medicine, the Third Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2Department of Rehabilitation, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Welfare and Sustainable Development, Centro Universitario Del Norte, Universidad de Guadalajara, Colotlán, Jalisco, Mexico
*These authors contributed equally to this work
Correspondence: Jiang Li, Department of Rehabilitation Medicine, the Third Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China, Email [email protected]
Purpose: Ectopic pregnancy (EP) is a significant contributor to maternal mortality, posing a major burden on women in developing countries. This study examined global trends in EP mortality from 1982 to 2021, focusing on developing nations represented by BRICS countries (Brazil, Russian Federation, India, China, and South Africa).
Methods: Based on the Global Burden Disease (GBD) 2021, an analysis of EP mortality was conducted by location (global and BRICS), age group (15– 49 years), and years (1982– 2021). The age-period-cohort (APC) model was utilized to estimate net drift, local drift, age effects, period effects, and cohort effects from 1982 to 2021. Furthermore, the Autoregressive Integrated Moving Average (ARIMA) model was employed to forecast EP mortality from 2022 to 2030.
Results: Globally, the number of deaths due to EP reached 6442 (95% CI: 5368 to 7796) in 2021, representing a 55.08% increase compared with 1982. Despite rising absolute deaths, the global Age-Standardized Mortality Rate (ASMR) declined by 15.79%, reaching 0.16 per 100,000 population in 2021 (95% UI: 0.14 to 0.20), indicating a reduction in population-level risk after accounting for demographic structure. EP mortality predominantly affected individuals aged 20– 39 years across regions. APC analyses revealed distinct period and cohort effects, with marked heterogeneity across BRICS countries. Net Drift estimates ranged from a substantial annual decline in the Russian Federation (− 10.12%) to a modest decrease in India (− 1.62%), with Brazil, China, and South Africa showing intermediate downward trends.
Conclusion: From 1982 to 2021, varying advancements in managing EP were observed among BRICS nations. Tailored financial allocations and policy measures aided in lowering EP mortality. Enhancing cross-country collaboration and knowledge exchange within BRICS countries is crucial for further ameliorating EP outcomes.
Keywords: ectopic pregnancy, age-period-cohort, mortality, trend, BRICS
Introduction
Ectopic pregnancy (EP) is defined as a pregnancy that implants outside the uterine cavity generally presenting with abdominal pain and vaginal bleeding.1 It is characterized by a rapid onset and progression.2 EP rupture stands as the predominant contributor to maternal mortality in early pregnancy, manifesting in 9% to 14% of instances and accounting for 5% to 10% of total pregnancy-related fatalities.3 Moreover, with women opting to delay childbearing and the expanding utilization of assisted reproductive technology worldwide, the incidence of EP is increasing proportionally.4,5 EP can adversely affect the physical and mental well-being of pregnant women, increasing the risk of infertility and even posing a life-threatening condition.2,6 Therefore, an in-depth analysis of trends in EP mortality is essential for improving prevention and control strategies.
Due to limited healthcare resources and constrained health systems, EP remains a significant challenge in low-and middle-income countries,7 and continues to contribute substantially to disease burden in developing regions.8 The BRICS countries (Brazil, the Russian Federation, India, China, and South Africa) account for approximately 42% of the global population and around 25% of the global economy.9 As large emerging economies undergoing rapid socioeconomic and demographic transitions, BRICS nations face shared structural challenges in strengthening health systems and ensuring equitable access to reproductive health services.10 In addition, these countries are also undergoing epidemiological transitions, with disease burdens increasingly shifting from infectious diseases toward non-communicable and reproductive health-related conditions. At the same time, they differ considerably in population structure, lifestyle patterns, infectious disease burden, sexual behavior, and contraceptive use, which may lead to heterogeneous EP mortality patterns across settings. This combination of a broadly comparable macro-context and substantial inter-country heterogeneity provides a meaningful framework for examining both shared and context-specific temporal trends in EP mortality.
Recent comprehensive reviews have further highlighted the persistent global burden of EP and emphasized ongoing challenges in diagnosis and management despite advances in clinical care.11 Previous studies using the Global Burden Disease 2019 (GBD 2019) database have addressed gaps in epidemiological information on EP, demonstrating a global decline in its disease burden, However, substantial regional heterogeneity persists, and serious challenges remain in low and middle income countries. Moreover, these analyses lacked the capacity to assess potential temporal and cohort-specific trends in EP mortality.7,8 Age-Period-Cohort (APC) modelling is a validated analytical approach that elucidates the complex relationship among age, period and cohort effects on EP mortality. The latest update of the GBD 2021 database provides an important opportunity to examine temporal trends and regional disparities in EP across BRICS countries, thereby deepening understanding of its evolving epidemiological dynamics. The findings from these data may contribute to the development of strategies aimed at improving health outcomes associated with EP and reducing its adverse effects on women.
The aim of this study was to analyze trends in EP mortality in BRICS countries between 1982 and 2021 using the APC model. By comprehensively examining the spatial and temporal variations as well as the geographical characteristics of EP, an Autoregressive Integrated Moving Average (ARIMA) model was also used to predict the mortality due to EP from 2022 to 2030. This study aims to provide evidence to address the significant regional heterogeneity in EP mortality and to inform the rational allocation of medical resources and development of national policies to reduce its disease burden.
Materials and Methods
Study Source
This study used data from the GBD 2021 public database (http://ghdx.healthdata.org/gbd-results-tool; accessed on July 8, 2024). All data are anonymous and publicly available, with ethical approval for exemption from informed consent granted by the Human Research Ethics Committee at the University of Washington. The GBD 2021 provides epidemiological estimates for 371 diseases and injuries across 21 regions and 204 countries and territories spanning from 1980 to 2021. We extracted data on EP-related deaths, crude mortality, and age-standardized mortality rate (ASMR) for women aged 15–49 years, categorized into seven age groups (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, and 45–49 years). The data were obtained from diverse origins, spanning vital registration systems, verbal autopsy assessments, population censuses, household surveys, disease registries, health service utilization data, and other pertinent repositories.1 To ensure the reliability of historical data across diverse countries, GBD 2021 employs a standardized data-processing pipeline. This includes the redistribution of “garbage codes” (nonspecific causes) and the use of the Cause of Death Ensemble Model (CODEm), which accounts for variations in data quality and availability by integrating diverse covariates and weighting sources based on their predictive validity. The use of 95% uncertainty intervals (UIs) further reflects the confidence level of these estimates in relation to data density and quality in each country.12 According to the International Classification of Diseases (ICD) 9th and 10th editions, EP is defined by codes 633 and O00, respectively.1 In the study, the age groups below 15 years and above 50 years were excluded due to the rarity or absence of EP mortality rates within these age ranges.12 Although isolated cases may occur in settings with early marriage or advanced maternal age, mortality counts in these groups were extremely low in the GBD dataset and were unlikely to materially influence age-effect estimation.
Statistical Analysis
Age–Period–Cohort Analysis
In our study, we utilized the APC model, with age, period, and cohort as independent variables, to investigate the probability distribution of event occurrence rates in the population. The APC model evaluated the independent effects of age, period, and birth cohort on EP burden, revealing longitudinal age distribution, period-relative risk, and cohort-relative risk. The APC model, which is based on the poisson distribution, is widely employed in epidemiological studies of diseases in the scientific community.13
Age refers to the age of women at the time of data collection, with age effects capturing variations across different age groups. Period represents the year of data collection, with period effects reflecting temporal changes that influence all age groups simultaneously. Cohort denotes the birth cohort of participants, representing differences in outcomes among individuals born in the same period.14
The APC analysis was performed using the National Cancer Institute (NCI) APC web tool (https://analysistools.cancer.gov/apc/), which applies a log-linear Poisson regression model with a log link and an offset for the log of the population at risk.15 Parameter estimation was based on the Intrinsic Estimator (IE) method, which addressed the identification problem arising from the linear dependency among age, period, and cohort (cohort = period – age). This method provided unbiased and efficient parameter estimates without arbitrary constraints on model parameters.16,17 The relative risk (RR) of the mortality can be obtained through the natural logarithm transformation of the effect coefficient. Model adequacy was evaluated using Wald chi-square tests for age, period, and cohort effects, along with inspection of the coefficient estimates and their 95% confidence intervals.15 Model fit was evaluated using deviance and information criteria as reported by the Web Tool, and the resulting estimates of longitudinal age curves, and period and cohort effects were used for interpretation and plotting in R statistical software program (version 4.3.2).
Data Arrangement
In order to control the number of parameters in the APC model and to achieve smooth temporal effect curves, the APC model requires equal intervals between age and period groups. In this study, the population aged 15 to 49 years was subdivided into seven groups (15–19,20-24,25–29,30-34,35–39,40-44, and 45–49 years), and the periods were defined as 1982–1986, 1987–1991., 2017–2021. The starting year (1982) was selected based on the earliest year with complete and stable GBD mortality estimates across BRICS countries and to construct balanced five-year intervals required for APC modeling. Considering that the birth cohort was determined by the age of the subjects and the year of events (cohort = period – age),18 the corresponding birth cohorts ranged from 1933–1941 (with a median year of 1937) to 1998–2006 (with a median year of 2002). To ensure model identifiability, the reference period (1997–2001) and reference cohort (1963–1971) were located around the midpoint of the observation window, providing a stable baseline that minimizes boundary bias and facilitates interpretation of relative effects.19–21
Auto-Regressive Integrated Moving Average Forecasting
The ARIMA model integrates autoregressive (AR) and moving average (MA) models to analyze time series data. It characterizes time-dependent random variables and has the capacity to forecast future values based on past observations.22 In this study, a log-transformation was applied to the GBD 1982–2021 dataset to predict the ASMR for EP during the period 2022–2030.
To ensure data stationarity, each country’s time series was first examined using the Augmented Dickey–Fuller (ADF) and Kwiatkowski–Phillips–Schmidt–Shin (KPSS) tests. The optimal ARIMA model was automatically selected based on the minimum Bayesian Information Criterion (BIC), implemented via the auto.arima() function in R (version 4.3.2) with ic = “bic” and seasonal = FALSE. The original data were used for ARIMA modeling, as they yielded a lower BIC and provided a better balance between model fit and parsimony. Model adequacy was evaluated through diagnostic analyses, including autocorrelation (ACF) and partial autocorrelation (PACF) plots, residual normality (Q-Q plot), residual independence (Ljung–Box test), and residual–fitted value plots. A non-significant Ljung–Box test (p > 0.05) indicated that the residuals satisfied the white noise assumption, suggesting an adequate model fit. The final ARIMA model orders (p, d, q), transformation type, and BIC values for each series were summarized in Table S1, with detailed diagnostic plots presented in Figure S1. The data analyses and visualizations were created utilizing the R statistical software program (version 4.3.2).
Uncertainty Handling in Modeling
Mean point estimates from GBD 2021 were used in the modeling analyses because neither the APC Web Tool nor conventional ARIMA frameworks support the direct incorporation of UIs. Although uncertainty propagation via Monte Carlo simulation is theoretically feasible, such an approach would generate an intractable number of parameter combinations across countries, age groups, and time periods, substantially increasing computational complexity and limiting the feasibility and interpretability of the results. Therefore, the projections presented in this study should be interpreted as point estimates rather than probabilistic forecasts.
Results
Globally and in BRICS Countries Trends in EP Mortality 1982-2021
In 2021, the global number of deaths due to EP was 6442 (95% UI: 5368 to 7796), representing a 55.08% increase compared to 1982. The global ASMR for EP was 0.16 per 100,000 individuals (95% UI: 0.14 to 0.20) in 2021, showing a decrease of 15.79% from 1982. According to the APC model, the net drift of the global EP mortality from 1982 to 2021 was −0.30 (95% UI: −0.41 to −0.19) (Table 1).
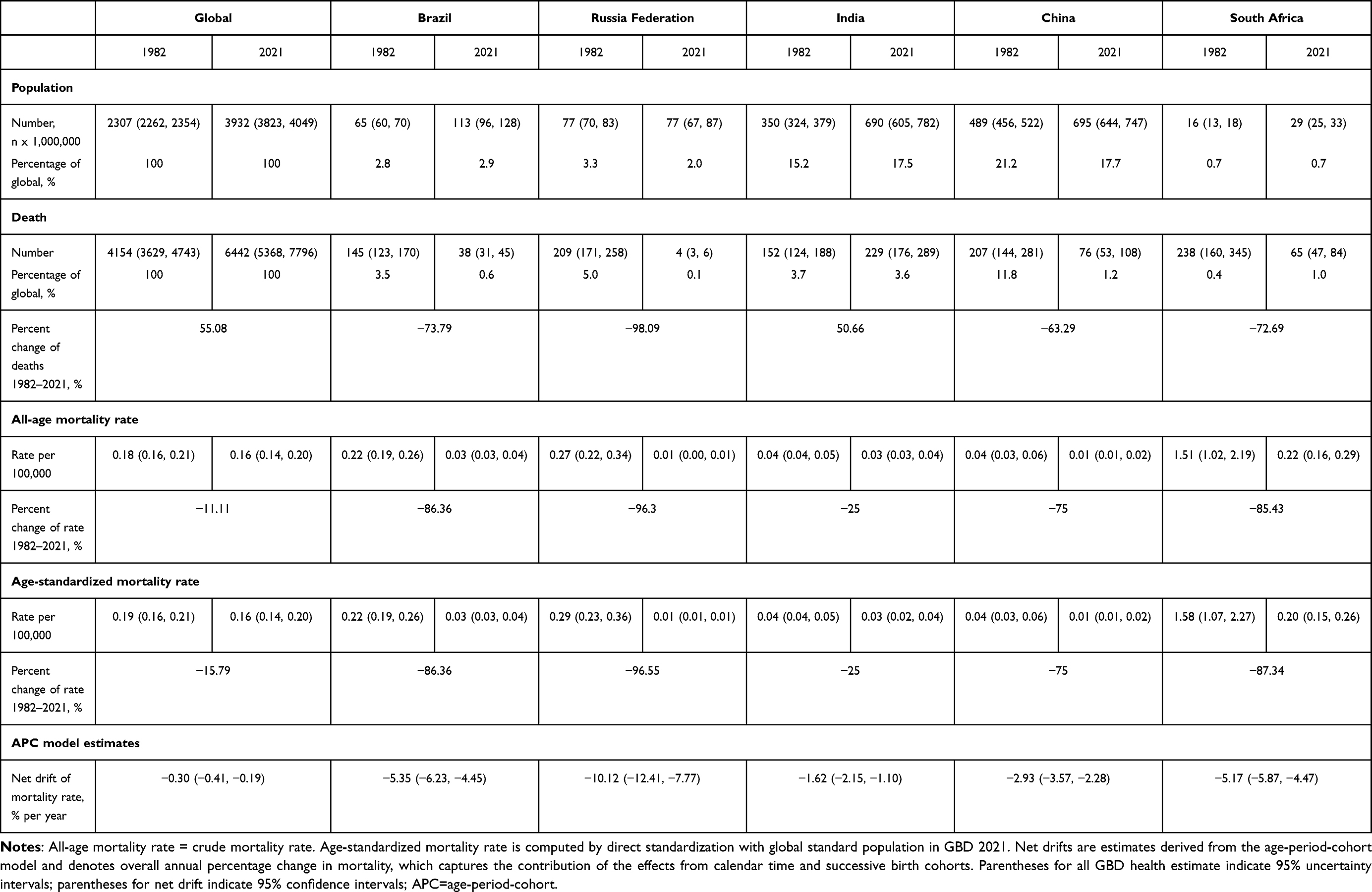 |
Table 1 Trends in the Mortality of Ectopic Pregnancy Across BRICS, 1982–2021 |
From 1982 to 2021, the number of EP deaths in the BRICS countries declined to varying degrees, while India stood out with a 50.66% increase. This apparent paradox reflects the distinction between absolute disease burden and age-standardized risk, whereby rapid population growth and demographic expansion can drive increases in total deaths even as mortality risk declines. It was noteworthy that during this period, both the global and BRICS countries showed a decreasing trend in mortality and age-specific mortality across all age groups. Additionally, the range of decline in the ASMR among the BRICS countries varied from −25% in India to −96.55% in the Russian Federation. The mortality drift in the BRICS countries also demonstrated varying degrees of decrease, with the largest decline observed in Russian Federation at −10.12% (95% UI: −12.41 to −7.77), and the smallest decline in India at −1.62% (95% UI: −2.15 to −1.10) (Table 1).
Time Trends in EP Mortality Across Different Age Groups
Figure 1A illustrated the annual percentage changes in EP mortality across different age groups. In Brazil, China, India, the Russian Federation, and South Africa, the local drift values were predominantly negative across nearly all age groups, indicating declining EP mortality in the BRICS countries. However, globally, the local drift values before the age of 25–30 were greater than 0, suggesting an increase in EP mortality globally before the age of 25–30, followed by a gradual decline (Figure 1A).
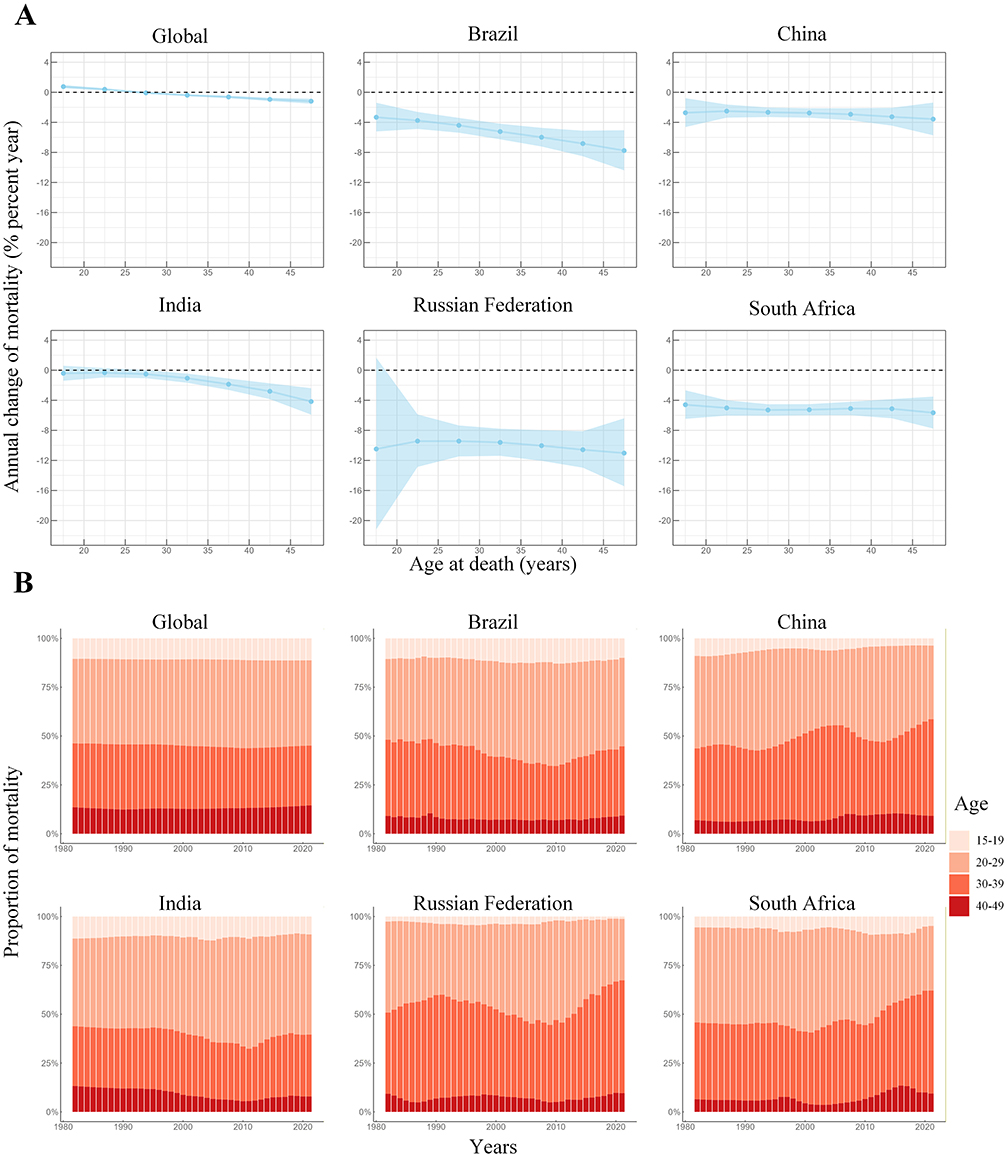 |
Figure 1 Trends and age distribution of ectopic pregnancy mortality in global and BRICS from 1982 to 2021. (A) Local drifts of ectopic pregnancy mortality rate (estimates from age-period-cohort models) for 7 age groups (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, and 45–49). The dots and shaded areas indicate the annual percentage change of mortality rate (% per year) and the corresponding 95% confidence intervals (CIs). (B) Age distribution of mortality from ectopic pregnancy. Age distribution of mortality is represented as temporal change in the relative proportion of mortality across age groups during 1982–2021. |
Figure 1B depicted the temporal changes in the age distribution of EP mortality. From 1982 to 2021, both globally and in the BRICS countries, the distribution of deaths was predominantly concentrated within the 20–39 age group (exceeding 70%),with a smaller proportion observed in the 15–19 and 40–49 age groups. The proportion of deaths attributed to EP remained stable across age groups globally, with Brazil and India showing a similarly sustained stability over time. In China, the Russian Federation, and South Africa, an evident shift in EP mortality distribution occurred from younger (20–29 years) to older age groups (30–39 years) (Figure 1B).
Age, Period, and Cohort Effects on EP Mortality
The age effect revealed that both globally and within the BRICS nations, EP mortality showed an increasing trend among individuals aged 15–25, with the highest rates observed in the 20–25 age group, followed by a decline among women aged 25–49 years. A distinctive pattern was evident in Russian Federation, where EP mortality rapidly decreased among women aged 35–49, surpassing all other countries. Of concern was the consistently higher EP mortality across all age groups in South Africa compared with other nations (Figure 2A).
Figure 2 continued. Figure 2 Age, period and cohort effects on ectopic pregnancy mortality in global and BRICS. (A) Age effects are shown by the fitted longitudinal age curves of mortality rate (per 100,000 person-years) adjusted for period deviations. (B) Period effects are shown by the relative risk of mortality rate (mortality rate ratio) and computed as the ratio of age-specific rates from 1982–1986 (1984.5) to 2017–2021 (2019.5), with the referent period set at 1997–2001 (1999.5). (C) Cohort effects are shown by the relative risk of mortality rate and computed as the ratio of age-specific rates from the 1933–1941 (1937) cohort to the 1998–2006 (2002) cohort, with the referent cohort set at 1963–1971 (1967). The dots and shaded areas denote mortality rates or rate ratios and their corresponding 95% CIs.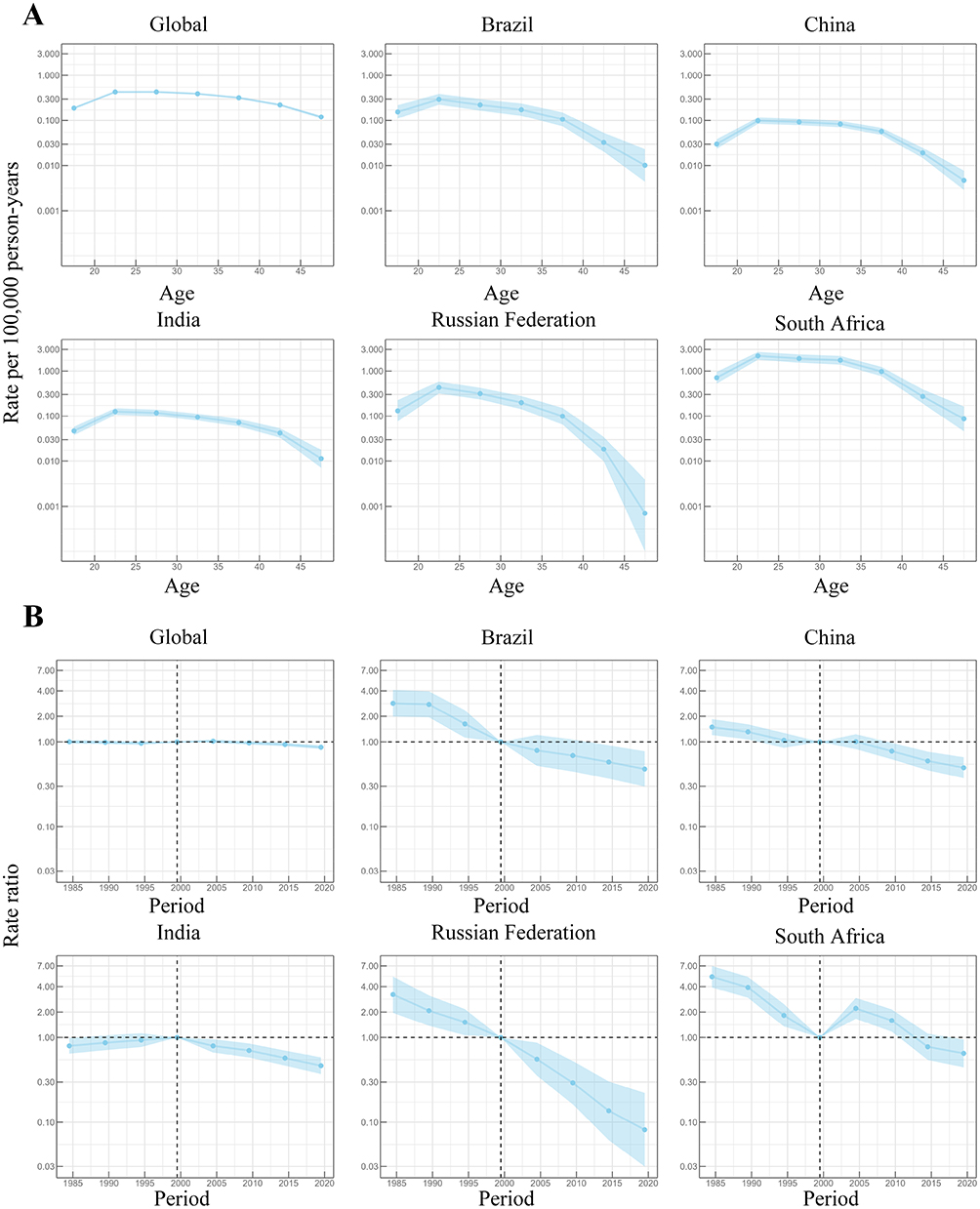
The period effect indicated a relatively consistent global pattern in mortality risk, suggesting limited improvement over time. Following the reference period (1997–2001), EP mortality risk continued to decrease in Brazil and the Russian Federation, while China showed slight and temporary increase between 1997–2006, followed by a declining trend from 2007 to 2021. South Africa displayed a pattern similar to that of China, characterized by a longer period of increasing mortality risk. South Africa experienced a more pronounced and sustained increase in mortality risk from 1997 to 2011, followed by a decreasing trend from 2012 to 2021. It was noteworthy that India experienced a continuous decrease in mortality risk from 1982 to 2021 (Figure 2B).
The cohort effect demonstrated a overall stability globally, indicating limited improvement in EP mortality risks across different birth cohorts. Following the reference cohort (1963–1971), Brazil, China, the Russian Federation, and South Africa experienced sustained declines in EP mortality risks. In contrast, in India, mortality risk remained relatively stable across birth cohorts after the reference cohort (Figure 2C).
Figure 3 presents the ARIMA-based forecast of ASMR for EP from 2022 to 2030.At the global level, the ASMR of EP is projected to show a slight upward trend over the forecast period. In contrast, declining trajectories are observed in Brazil, the Russian Federation, and China, with China exhibiting a more pronounced decrease. India and South Africa are projected to remain relatively stable, showing minimal variation in ASMR throughout the forecast horizon.
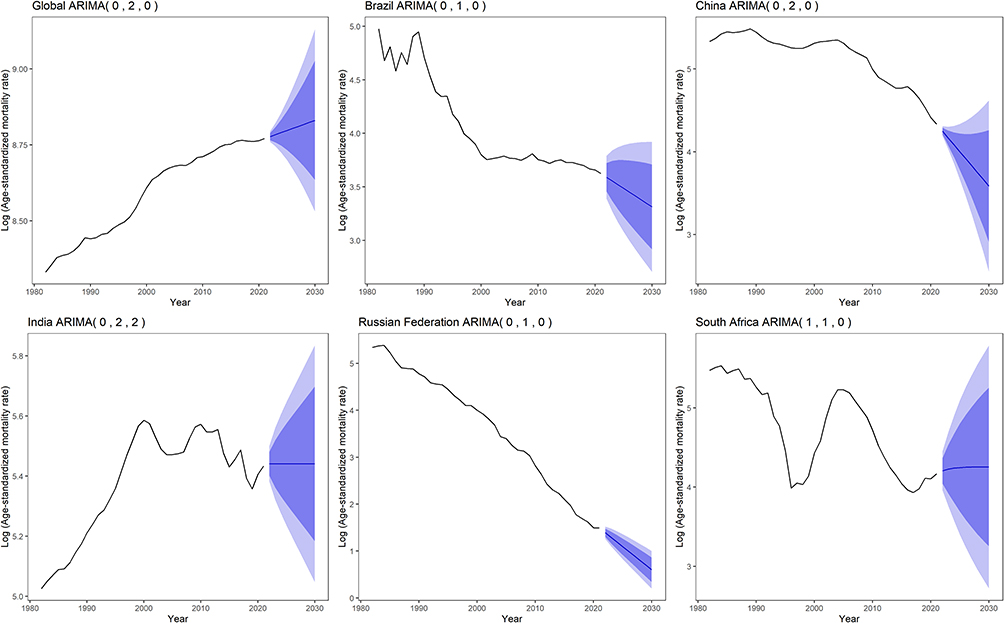 |
Figure 3 Forecast of age-standardized mortality rates with ectopic pregnancy from 2022–2030 through ARIMA. The blue line indicates the predicted value, the dark blue area indicates the 95% CI (confidence interval) of the predicted value, and the light blue is the 80% CI. |
Discussion
To our knowledge, few studies have applied the APC model to analyzing EP mortality and to predict EP-related mortality from 2022 to 2030 using the ARIMA model. Compared to previous GBD 2019 publications,7,8,23 our study provides a more detailed examination of age, period, and cohort effects and offers projections that may inform future public health planning.
Although the global number of EP-related deaths increased between 1982 and 2021, this pattern should be interpreted alongside the concurrent decline in the ASMR. This divergence highlights the distinction between absolute mortality burden and population-level risk, whereby demographic expansion and population growth may drive increases in total deaths even when underlying mortality risk decreases. The downward ASMR trend may be consistent with multiple coinciding factors, including improvements in early recognition, broader access to obstetric care, and advances in diagnostic practices.23–25 For example, expanded antenatal care (ANC) coverage during this period may have facilitated earlier clinical contact and referral opportunities,26 while technological developments—such as the wider availability of transvaginal ultrasound and sensitive serum β-hCG testing—may have contributed to more timely identification of EP before catastrophic complications occur.27,28 EP mortality was predominantly concentrated in the 20–39 age group, likely reflecting peak reproductive activity.8 The gradual shift toward older reproductive age groups observed in several countries may be consistent with delayed childbearing patterns.29 Between 2022 and 2030, the projected global increase in EP ASMR may be partly related to population aging and shifts toward older maternal age, alongside delayed childbearing patterns observed globally. The stable patterns predicted for India and South Africa may suggest that underlying risk structures and health-system conditions will remain broadly unchanged over the forecast horizon. By contrast, the declining trajectories in Brazil, the Russian Federation, and China may be consistent with sustained improvements in access to early diagnosis and clinical management. These heterogeneous projections underscore the importance of strengthening early diagnostic capacity and reproductive healthcare strategies across settings.
In Brazil and China, the relatively higher EP mortality observed among younger women may be consistent with reproductive-age risk concentration, as EP events inherently occur during periods of highest fertility.30 Age-specific differences in younger populations may also reflect variations in healthcare-seeking behavior, contraceptive access, or early recognition of pregnancy complications rather than biological factors alone.31,32 The subsequent reductions in mortality risk observed after the reference period may coincide with broader transitions in healthcare systems, expansion of reproductive health services, and improvements in diagnostic capacity. In Brazil, these patterns may be interpreted in light of major health-system developments, including the implementation of the National Comprehensive Women’s Health Care Policy (PNAISM), launched in 2004.33 In China, long-term family planning policies may plausibly be related to expanded access to reproductive health education and contraception,34,35 a mechanism that has been linked to lower EP risk in prior studies.36 Since the early 2000s, China has also experienced substantial expansion of maternal and child health services, particularly in antenatal and obstetric care coverage, which may have facilitated earlier detection and management of pregnancy-related complications.30 Cohort patterns observed in Brazil and China may likewise be viewed within the context of broader public health initiatives, including Brazil’s Women’s Comprehensive Healthcare Program (PAISM) and Unified Health System (SUS), as well as China’s Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCAH) program.30,37,38 Collectively, these interpretations are consistent with prior literature emphasizing the potential role of healthcare infrastructure, service accessibility, and diagnostic improvements in shaping EP-related mortality patterns.25,39
In the Russian Federation, the age effect was similar to that of Brazil and China, however, there was a more rapid decline in EP mortality among women aged 35–49. This pattern may plausibly be interpreted in the context of demographic shifts, as the Russian Federation has experienced sustained declines in fertility rates and progressive population aging.40 The decline in EP mortality observed after the 2000s coincided with broader behavioral and public health transitions, including documented reductions in alcohol consumption among women of reproductive age.41 Previous research has indicated that low to moderate alcohol intake is associated with an increased risk of EP.42 Alcohol consumption exceeding 10 g/day was associated with a 1.5-fold higher risk compared with non-drinkers, and the authors raised the possibility that cigarette smoking and alcohol intake could play a role in the etiology of EP through altering the motility of normal fallopian tubes.43 However, since the late 2000s, the Russian Federation has intensified efforts to promote alcohol abstinence during pregnancy, resulting in a significant increase in the percentage of pregnant women who completely abstain from alcohol, from 46.8% during 2006–2011 to 54.6% during 2012–2018.41 This shift may have contributed to the decline in EP mortality risk observed after the reference period (1997–2001). Furthermore, cohort effects in the Russian Federation may plausibly be associated with long-term improvements in women’s education. As successive birth cohorts emerged with higher levels of education,44 there was a corresponding decrease in EP mortality risk, likely due to increased knowledge about contraception and reproductive health. This trend underscores the importance of women’s education in reducing maternal health risks, including EP.45
India and South Africa exhibited age-related patterns broadly comparable to those observed in Brazil and China. In South Africa, the persistently elevated EP mortality across age groups may plausibly be interpreted in the context of the country’s well-recognized dual burden of infectious diseases and structural healthcare constraints. HIV infection and sexually transmitted infections (STIs), which remain highly prevalent in this setting, have been associated with an increased risk of tubal damage and subsequent EP in prior studies.46–48 Regarding period effects, the continuous decline in EP mortality risk observed in India may coincide with long-standing expansions in family planning programs and contraceptive access initiated in the mid-20th century.49,50 Improvements in reproductive health awareness, earlier clinical contact, and gradual strengthening of maternal healthcare services may also have contributed to this pattern. In South Africa, the observed temporal changes may be viewed alongside national public health initiatives, including the National Health Promotion Policy (NHPP) introduced in 2015, which was designed to improve population and maternal health indicators. From a cohort perspective, the relatively stable mortality patterns observed in India may reflect persistent structural and social determinants, including inequalities in women’s autonomy, education, and healthcare accessibility,51,52 which have been widely recognized as influential factors in reproductive health outcomes. In South Africa, cohort-level variations may plausibly be related to long-term demographic, epidemiological, and health-system transitions rather than any single policy intervention. Long-term population and reproductive health strategies, including the National Population Development Program (PDP), established in 1984, may have influenced healthcare utilization patterns and broader reproductive health dynamics over time.53 Even under a relatively stable projected trajectory, persistent structural pressures on the healthcare system may remain relevant for interpreting EP-related mortality patterns.
Importantly, EP represents a broader reproductive health challenge beyond maternal mortality. In addition to fatal outcomes, EP is associated with infertility, recurrent EP, chronic pelvic morbidity, and psychological distress.54 Therefore, mortality reduction captures only part of the overall disease burden, and prevention strategies should be integrated within comprehensive reproductive health frameworks.
Despite its contributions, this study has several limitations. First, GBD-based estimates are derived from heterogeneous data sources across countries, and variations in data quality, diagnostic practices, and reporting systems may introduce bias, particularly in settings with limited healthcare capacity where EP mortality may be underestimated. Second, this study used the mean point estimates of mortality from GBD 2021 without incorporating the corresponding 95% UIs into the APC and ARIMA models, which may underestimate overall statistical uncertainty and lead to overconfidence in point projections. In addition, ARIMA modeling assumes time-series stationarity after differencing; residual non-stationarity cannot be entirely excluded and may affect the robustness of long-term projections. In some age–country strata, relatively small numbers of deaths in certain years may have affected the stability of age-specific mortality rate estimates despite age standardization. Furthermore, although five-year grouping is standard in APC modeling, this approach may reduce sensitivity to subtle temporal variations Finally, the study’s reliance on the ARIMA model, a univariate time-series approach, limits its ability to account for external factors.While we have addressed this by shortening the forecast horizon to 2030 and applying log-transformations to enhance model stability, these statistical projections should be interpreted as a baseline trend under the assumption of historical continuity rather than a definitive prediction of future outcomes.
Conclusions
From 1982 to 2021, the ASMR of EP declined globally, indicating a reduction in population-level mortality risk, yet substantial heterogeneity persisted across BRICS countries. While most nations exhibited declining or stable patterns, South Africa remained a comparatively high-risk setting, with projections suggesting a potential upward tendency through 2030. APC analyses further indicated that EP mortality was concentrated among women of reproductive age, particularly those aged 20–24 years. These findings highlight pronounced cross-country disparities and age-related vulnerabilities that may not be fully captured by aggregate trends.
Overall, the observed and projected patterns underscore the importance of context-specific prevention strategies. Sustained improvements in early diagnosis, timely clinical management, and equitable access to reproductive healthcare services may be essential for mitigating EP-related mortality, particularly in higher-burden settings.
Data Sharing Statement
The data utilized in this study originate from the 2021 Global Burden of Disease database, accessible via the link hosted by the Institute for Health Metrics and Evaluation at Washington University: http://ghdx.healthdata.org/gbd-results-tool. The GBD dataset is managed by this institution. Access to the provided GBD research database link does not require additional permission from IHME for data usage. Data verification can be provided upon request. For any inquiries regarding data availability, please contact the corresponding authors.
Ethics Approval and Informed Consent
This study was conducted using publicly available data from the GBD 2021 study. According to the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (issued on February 18, 2023), Article 32, Items 1 and 2, research using legally obtained public data that does not involve identifiable personal information may be exempt from ethical review. After consultation with the Ethics Committee of the Third Xiangya Hospital, Central South University, this study was determined to be exempt from ethical approval.
Acknowledgments
Thanks to the IHME and the Global Burden of Disease study collaborations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 82401939 to L.J.), Natural Science Foundation of Hunan Province (grant number 2023JJ40892 to L.J.), and Natural Science Foundation of Changsha City (grant number kq2208352 to L.J.). The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Collaborators GDaI. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–14. doi:10.1016/s0140-6736(24)00757-8.
2. Ren N, Dela Rosa RD, Chen Z, et al. Research progress on psychological distress in patients with ectopic pregnancy in China. Neuropsychiatr Dis Treat. 2023;19:1633–1639. doi:10.2147/ndt.S410320
3. Mullany K, Minneci M, Monjazeb R, CC O. Overview of ectopic pregnancy diagnosis, management, and innovation. Women’s Health. 2023;19:17455057231160349. doi:10.1177/17455057231160349
4. Correa-de-Araujo R, Yoon SS (Sarah). Clinical outcomes in high-risk pregnancies due to advanced maternal age. J Womens Health. 2021;30(2):160–167. doi:10.1089/jwh.2020.8860
5. Zhu S, Fan Y, Lan L, Deng T, Zhang Q. Heterotopic pregnancy secondary to in vitro fertilization-embryo transfer: risk factors and pregnancy outcomes. Front Med Lausanne. 2022;9:864560. doi:10.3389/fmed.2022.864560
6. Al Naimi A, Moore P, Brüggmann D, Krysa L, Louwen F, Bahlmann F. Ectopic pregnancy: a single-center experience over ten years. Reprod Biol Endocrinol. 2021;19(1):79. doi:10.1186/s12958-021-00761-w
7. Bo W, Qianyu Z, Mo L. Global, regional, and national burden of ectopic pregnancy: a 30-year observational database study. Int J Clin Pract. 2023;2023:3927337. doi:10.1155/2023/3927337
8. Zhang S, Liu J, Yang L, Li H, Tang J, Hong L. Global burden and trends of ectopic pregnancy: an observational trend study from 1990 to 2019. PLoS One. 2023;18(10):e0291316. doi:10.1371/journal.pone.0291316
9. Liu Z, Wang Z, Xu M, Ma J, Sun Y, Huang Y. The priority areas and possible pathways for health cooperation in BRICS countries. Global Health Res Policy. 2023;8(1):36. doi:10.1186/s41256-023-00318-x
10. Romaniuk P, Poznańska A, Brukało K, Holecki T. Health system outcomes in BRICS countries and their association with the economic context. Front Public Health. 2020;8:80. doi:10.3389/fpubh.2020.00080
11. Papageorgiou D, Sapantzoglou I, Prokopakis I, Zachariou E. Tubal ectopic pregnancy: from diagnosis to treatment. Biomedicines. 2025;13(6):1465. doi:10.3390/biomedicines13061465
12. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
13. Bell A. Age period cohort analysis: a review of what we should and shouldn’t do. Ann Hum Biol. 2020;47(2):208–217. doi:10.1080/03014460.2019.1707872
14. Wang Z, Hu S, Sang S, Luo L, Yu C. Age–period–cohort analysis of stroke mortality in China. Stroke. 2017;48(2):271–275. doi:10.1161/strokeaha.116.015031
15. Rosenberg PS, Check DP, Anderson WF. A web tool for age–period–cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2014;23(11):2296–2302. doi:10.1158/1055-9965.Epi-14-0300
16. Yang Y, Lai X, Li C, et al. Focus on the impact of social factors and lifestyle on the disease burden of low back pain: findings from the global burden of disease study 2019. BMC Musculoskelet Disord. 2023;24(1):679. doi:10.1186/s12891-023-06772-5
17. Yang Y, Schulhofer‐Wohl S, Fu W, Land KC. The intrinsic estimator for age-period-cohort analysis: what it is and how to use it. Am J Sociol. 2008;113(6):1697–1736. doi:10.1086/587154
18. Yang Y, Land KC, Ko, CW. Review of age-period-cohort analysis: new models, methods, and empirical applications, by Y. Yang and KC Land, journal of the American statistical association, 109, 865: comment by Fienberg, Hodges, and Luo and replies REPLY. J Am Stat Assoc. 2015;110(509):457. doi:10.1080/01621459.2015.1008843
19. Jing X, Wang Y, Zhang Y, et al. Global, regional, and national burden of neck pain in young population, 1990-2021: an age-period-cohort analysis and projections to 2050 based on the global burden of disease study 2021. Global Spine J. 2025:21925682251352847. doi:10.1177/21925682251352847.
20. Yan X, Wu D, Li R, et al. Temporal trends in prevalence for depressive disorders among women of childbearing age: age-period-cohort analysis 2021. J Affect Disord. 2025;380:124–134. doi:10.1016/j.jad.2025.03.108
21. Wang X, Xu Y, Ma X, Nan R, Wu Y, Cheng P. Epidemiological trends and age-period-cohort effects on periodontal diseases incidence across the BRICS from 1992 to 2021. BMC Oral Health. 2025;25(1):434. doi:10.1186/s12903-025-05796-8
22. Vollset SE, Goren E, Yuan C-W, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396(10258):1285–1306. doi:10.1016/s0140-6736(20)30677-2
23. He D, Wang T, Ren W. Global burden of pelvic inflammatory disease and ectopic pregnancy from 1990 to 2019. BMC Public Health. 2023;23(1):1894. doi:10.1186/s12889-023-16663-y
24. WHO Guidelines Approved by the Guidelines Review Committee. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization; 2016.
25. Creanga AA, Shapiro-Mendoza CK, Bish CL, Zane S, Berg CJ, Callaghan WM. Trends in ectopic pregnancy mortality in the United States: 1980-2007. Obstetrics Gynecol. 2011;117(4):837–843. doi:10.1097/AOG.0b013e3182113c10
26. Moller A-B, Petzold M, Chou D, Say L. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. Lancet Glob Health. 2017;5(10):e977–e983. doi:10.1016/s2214-109x(17)30325-x
27. Varma R, Gupta J. Tubal ectopic pregnancy. BMJ Clin Evid. 2009;2009:1406.
28. Practice Committee of the American Society for Reproductive Medicine. Medical treatment of ectopic pregnancy: a committee opinion. Fertil Sterility. 2013;100(3):638–644. doi:10.1016/j.fertnstert.2013.06.013
29. Chouinard M, Mayrand M-H, Ayoub A, Healy-Profitós J, Auger N. Ectopic pregnancy and outcomes of future intrauterine pregnancy. Fertil Steril. 2019;112(1):112–119. doi:10.1016/j.fertnstert.2019.03.019
30. Qiao J, Wang Y, Li X, et al. A lancet commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet. 2021;397(10293):2497–2536. doi:10.1016/s0140-6736(20)32708-2
31. Andola S, Kumar RR, Desai RM, k SA. Study of Risk factors and treatment modalities of ectopic pregnancy. J Family Med Prim Care. 2021;10(2):724–729. doi:10.4103/jfmpc.jfmpc_1279_20
32. Liang M, Simelane S, Fortuny Fillo G, et al. The state of adolescent sexual and reproductive health. J Adolesc Health. 2019;65(6):S3–s15. doi:10.1016/j.jadohealth.2019.09.015
33. Sorpreso ICE, Dos Santos Figueiredo FW, Ramos JLS, et al. Brazilian national policy of comprehensive women’s health care and mortality during climacteric period: has anything changed? BMC Public Health. 2021;21(1):518. doi:10.1186/s12889-021-10556-8
34. Zeng Y, Hesketh T. The effects of China’s universal two-child policy. Lancet. 2016;388(10054):1930–1938. doi:10.1016/s0140-6736(16)31405-2
35. Wang C. Trends in contraceptive use and determinants of choice in China: 1980–2010. Contraception. 2012;85(6):570–579. doi:10.1016/j.contraception.2011.10.014
36. Schultheis P, Montoya MN, Zhao Q, Archer J, Madden T, Peipert JF. Contraception and ectopic pregnancy risk: a prospective observational analysis. Am J Clin Exp Obstet Gynecol. 2021;224(2):228–229. doi:10.1016/j.ajog.2020.10.013
37. Diniz CSG, Cabral CDS. Reproductive health and rights, and public policies in Brazil: revisiting challenges during covid-19 pandemics. Global Public Health. 2022;17(11):3175–3188. doi:10.1080/17441692.2021.1995463
38. Osis M. Paism: um marco na abordagem da saúde reprodutiva no Brasil. Cadernos de Saúde Pública. 1998;14(suppl 1):25–32. [Paism: um marco na abordagem da saúde reprodutiva no Brasil]. doi:10.1590/S0102-311X1998000500011
39. GCoD C. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/s0140-6736(24)00367-2
40. Shcherbakova EM. Population dynamics in russia in the context of global trends. Stud Russ Econ Dev. 2022;33(4):409–421. doi:10.1134/s1075700722040098
41. Kotelnikova Z. Prevalence of self-reported alcohol consumption among pregnant women in Russia between 1994 and 2018. Alcoholism. 2022;46(5):825–835. doi:10.1111/acer.14798
42. Wang S, Mitsunami M, Ortiz-Panozo E, et al. Prepregnancy healthy lifestyle and adverse pregnancy outcomes. Obstetrics Gynecol. 2023;142(6):1278–1290. doi:10.1097/aog.0000000000005346
43. Bronson R. Ectopic pregnancy—still a challenge. Fertil Sterility. 2018;110(7):1265–1266. doi:10.1016/j.fertnstert.2018.09.008
44. Perelli-Harris B, Gerber TP. Nonmarital childbearing in Russia: second demographic transition or pattern of disadvantage? Demography. 2011;48(1):317–342. doi:10.1007/s13524-010-0001-4
45. Rogne T, Gill D, Liew Z, et al. Mediating factors in the association of maternal educational level with pregnancy outcomes: a Mendelian randomization study. JAMA Network Open. 2024;7(1):e2351166. doi:10.1001/jamanetworkopen.2023.51166
46. Amin A. Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. J Int AIDS Soc. 2015;18(Suppl 6S5):20302. doi:10.7448/ias.18.6.20302
47. Hufstetler K, Llata E, Miele K, Quilter LAS. Clinical updates in sexually transmitted infections, 2024. J Women’s Health. 2024;33(6):827–837. doi:10.1089/jwh.2024.0367
48. Ravindran TKS, Govender V. Sexual and reproductive health services in universal health coverage: a review of recent evidence from low- and middle-income countries. Sexual Reprod Health Matters. 2020;28(2):1779632. doi:10.1080/26410397.2020.1779632
49. Bansal A, Dwivedi LK, Ali B. The trends of female sterilization in India: an age period cohort analysis approach. BMC Women’s Health. 2022;22(1):272. doi:10.1186/s12905-022-01857-0
50. Ledbetter R. Thirty years of family planning in India. Asian Survey. 1984;24(7):736–758. doi:10.2307/2644186
51. Singh P, Das A, William J, Bruckner T. Fertility, economic development, and suicides among women in India. Social Psychiatry Psychiatric Epidemiol. 2021;56(10):1751–1759. doi:10.1007/s00127-021-02054-4
52. Kumar A. The transformation of the indian healthcare system. Cureus. 2023;15(5):e39079. doi:10.7759/cureus.39079
53. Chimere-Dan O. Population policy in South Africa. Stud Fam Plann. 1993;24(1):31–39. doi:10.2307/2939212
54. Papageorgiou D, Sapantzoglou I, Zachariou E, Antsaklis P, Daskalakis G, Pergialiotis V. Impact of ectopic pregnancy on the outcomes of the subsequent pregnancy: a systematic review and meta-analysis. J Clin Med. 2025;14(12):4112. doi:10.3390/jcm14124112
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.