Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Economic Evaluation of Multiple-Pharmacogenes Testing for the Prevention of Adverse Drug Reactions in People Living with HIV
Authors Turongkaravee S ![]() , Praditsitthikorn N, Ngamprasertchai T
, Praditsitthikorn N, Ngamprasertchai T ![]() , Jittikoon J, Mahasirimongkol S, Sukasem C, Udomsinprasert W
, Jittikoon J, Mahasirimongkol S, Sukasem C, Udomsinprasert W ![]() , Wu O
, Wu O ![]() , Chaikledkaew U
, Chaikledkaew U
Received 22 March 2022
Accepted for publication 28 June 2022
Published 7 July 2022 Volume 2022:14 Pages 447—463
DOI https://doi.org/10.2147/CEOR.S366906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Saowalak Turongkaravee,1 Naiyana Praditsitthikorn,2 Thundon Ngamprasertchai,3 Jiraphun Jittikoon,4 Surakameth Mahasirimongkol,5 Chonlaphat Sukasem,6– 9 Wanvisa Udomsinprasert,4 Olivia Wu,10 Usa Chaikledkaew11,12
1Social, Economic and Administrative Pharmacy (SEAP) Graduate Program, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 2Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand; 3Department of Clinical Tropical Medicine, Faculty of Tropical Medicine; Mahidol University, Bangkok, Thailand; 4Department of Biochemistry, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 5Department of Medical Sciences, Medical Genetics Center, Medical Life Sciences Institute, Ministry of Public Health, Nonthaburi, Thailand; 6Division of Pharmacogenomics and Personalized Medicine, Department of Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 7Laboratory for Pharmacogenomics, Somdech Phra Debaratana Medical Center (SDMC), Ramathibodi Hospital, Bangkok, Thailand; 8Pharmacogenomics and Precision Medicine, The Preventive Genomics & Family Check-Up Services Center, Bumrungrad International Hospital, Bangkok, Thailand; 9MRC Centre for Drug Safety Science, Department of Pharmacology and Therapeutics, Institute of Systems, Molecular and Integrative Biology, University of Liverpool, Liverpool, L69 3GL, UK; 10Health Economics and Health Technology Assessment (HEHTA), Institute of Health and Wellbeing, University of Glasgow, Glasgow, UK; 11Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 12Mahidol University Health Technology Assessment (MUHTA) Graduate Program, Mahidol University, Bangkok, Thailand
Correspondence: Usa Chaikledkaew, Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, 447 Sri-Ayudhaya Road, Rajathevi, Bangkok, 10400, Thailand, Tel +662-644-8679 ext 5317, Fax +662-644-8694, Email [email protected]
Purpose: Pharmacogenetics (PGx) testing is one of the methods for determining whether individuals are at risk of adverse drug reactions (ADRs). It has been reported that multiple-PGx testing, a sequencing technology, has a higher predictive value than single-PGx testing. Therefore, this study aimed to determine the most cost-effective PGx testing strategies for preventing drug-induced serious ADRs in human immunodeficiency virus (HIV)-infected patients.
Patients and Methods: Potential strategies, including 1) single-PGx esting (ie, HLA-B*57:01 testing before prescribing abacavir, HLA-B*13:01 testing before prescribing co-trimoxazole and dapsone, and NAT2 testing before prescribing isoniazid) and 2) multiple-PGx testing as a combination of four single-gene PGx tests in one panel, were all compared to no PGx testing (current practice). To evaluate total cost in Thai baht (THB) and quality-adjusted life years (QALYs) for each strategy-based approach to a societal perspective, a hybrid decision tree and Markov model was constructed. Incremental cost-effectiveness ratios (ICERs) were estimated. Uncertainty, threshold, and scenario analyses were all performed.
Results: Before prescribing HIV therapy, providing single or multiple-PGx testing might save roughly 68 serious ADRs per year, and the number needed to screen (NNS) to avoid one serious ADR was 40. Consequently, approximately 35% and 40% of the cost of ADR treatment could be avoided by the implementation of single- and multiple-PGx testing, respectively. Compared with no PGx testing strategy, the ICERs were 146,319 THB/QALY gained for single-PGx testing and 152,014 THB/QALY gained for multiple-PGx testing. Moreover, the probability of multiple-PGx testing being cost-effective was 45% at the Thai willingness to pay threshold of 160,000 THB per QALY. Threshold analyses showed that multiple-PGx testing remained cost-effective under the range of cost, sensitivity at 0.95– 1.00 and specificity at 0.98– 1.00.
Conclusion: Single and multiple-PGx testing might be cost-effective options for reducing the incidence of drug-induced serious ADRs in people living with HIV.
Keywords: pharmacogenetic, adverse drug reactions, HIV, cost-utility analysis, economic evaluation
Introduction
Human Immunodeficiency Virus (HIV) infection/acquired immunodeficiency syndrome (AIDS) was the fifth leading cause of death and poses a significant disease burden among Thai people.1 The incidence per 1000 population was 0.08 for all ages, with an estimated 5400 new HIV infections per year.2,3 Since 2014, HIV/AIDS guidelines have been developed in collaboration with the Department of Disease Control, Ministry of Public Health and the Thai AIDS Society, with a significant change that people living with HIV can now access antiretroviral treatment (ART) for free and immediately upon diagnosis.4 This was consistent with the recommendation of the United State (US) Department of Health and Human Services (DHHS) panel denoting that ART should be provided to all HIV-positive individuals.5 Until now, people living with HIV have been treated for free through the support of all Thai health insurance schemes. However, drug-related adverse drug reactions (ADRs) frequently lead to non-compliance, virological failure, substantial treatment costs, and poor quality of life, given that people living with HIV are more susceptible to ADRs than the general population. It has been well recognized that HIV therapy consisting of ART and opportunistic infections can cause serious ADRs including abacavir-induced hypersensitivity reaction (HSR), co-trimoxazole-induced Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN), drug-induced rash with eosinophilia and systemic symptoms (DRESS), and isoniazid-induced hepatotoxicity.6
Nowadays, genetic factors are widely known to influence the efficacy and toxicity of pharmacological treatment.7 Supporting this, numerous studies demonstrated significant associations between genetic polymorphisms and drug induced-serious ADRs in not only ART regimens like abacavir, but also opportunistic infection therapy including co-trimoxazole, dapsone, and isoniazid.7,8 In addition to these previous findings, a meta-analysis uncovered that patients who carried HLA-B*57:01 were more likely than non-carriers to develop abacavir-induced HSR.9 Based on this premise, the United States Food and Drug Administration (USFDA) recommended that HLA-B*57:01 genetic screening should be standard practice for all patients receiving abacavir treatment.10 Apart from the significant influence of HLA-B*57:01 associated with abacavir-induced HSR, further meta-analysis and phenotype stratification study revealed a substantial association between HLA-B*13:01 and co-trimoxazole–induced DRESS.11 In Thai people, HLAB*13:01 allele was observed to be significantly associated with co-trimoxazole-induced SJS/TEN when compared to co-trimoxazole-tolerant controls.12 In Thai non-leprosy patients, HLA-B*13:01 was also significantly associated with dapsone-induced severe cutaneous adverse reactions (SCARs). Aside from effects of HLA genetic polymorphisms on drug induced-serious ADRs, several meta-analyses demonstrated that tuberculosis (TB) patients with slow/intermediate N-acetyltransferase 2 (NAT2) acetylators had a higher risk of isoniazid-induced liver injury than those with rapid acetylators.13,14 The aforementioned findings lend support to the notion that identifying genetic polymorphisms of pharmacogenes may pave the way to personalized medicine in the context of ADRs.
In support of the above assumption, previously published findings indicated that performing pharmacogenetic (PGx) testing before prescribing medication might help reduce the risk of developing serious ADRs.9,11–14 In Thailand, only HLA-B*15:02 testing is required before prescription carbamazepine for epilepsy patients, and HLA B*57:01 testing is needed before prescription allopurinol for gout patients under the Universal Health Coverage (UHC) scheme, which covers around 80% of Thai population. Despite this, there are over 70 PGx tests accessible at medical school laboratories and 14 regional lab centers operated by the Department of Medical Sciences, Ministry of Public Health.15 To date, technological advancements like a sequencing method have made it possible to test numerous genes in a short period of time, which may have a higher predictive value than single-gene testing. Therefore, multiple-PGx testing will be necessary to explore a variety of potential treatment pathways.16 However, the cost of multiple-PGx testing is still expensive, and no cost-effectiveness information has been provided to assist policymakers in making rationale resource allocation decision. Accordingly, the purpose of this study was to evaluate the cost-utility of single-PGx testing of HLA-B*57:01 before prescribing abacavir to prevent HSR, HLA-B*13:01 before prescribing co-trimoxazole to prevent DRESS, HLA-B*13:01 before prescribing dapsone to prevent SCAR, and NAT2 before prescribing isoniazid to prevent hepatotoxicity in people living with HIV as well as multiple-PGx testing, which is a combination of four aforementioned single-PGx tests compared to no PGx testing as a current practice.
Materials and Methods
Study Design
A hybrid decision tree and Markov model was developed to evaluate a cost-utility of a single- and multiple-PGx testing strategy before starting drug therapy in people living with HIV compared with those prescribed drug therapy without PGx testing. The incremental cost-effectiveness ratio (ICER) was calculated in terms of cost per quality-adjusted life-year (QALY). The assessment was made from a societal perspective.
Target Population
The model simulated cohorts of newly diagnosed HIV patients who received ART and treatment for opportunistic infections such as Pneumocystis jiroveci Pneumonia (PCP) and TB.
Interventions and Comparator
Studied interventions included four single-PGx tests and multiple-PGx testing that merged those single-PGx tests, which were all compared to no PGx testing as a current practice. The following details were provided.
Single-PGx Testing
Single PGx testing included 1) HLA-B*57:01 before starting abacavir to prevent HSR,6 2) HLA-B*13:01 before prescribing co-trimoxazole to prevent DRESS, 3) HLA-B*13:01 before prescribing dapsone to prevent SCAR, and 4) NAT2 before prescribing isoniazid to prevent hepatotoxicity.17 Prior to initiating any medication regimen, newly diagnosed HIV patients were all tested sequentially. Patients who get a positive test result would be prescribed the alternative regimen, whereas those with a negative test result would continue the initial regimen.
Multiple-PGx Testing
Multiple-PGx testing included four single-PGx tests in a single panel. Patients who test positive for each test would be prescribed the alternative regimen, whereas patients who test negative would remain on the initial regimen. All newly diagnosed HIV patients were tested just once before starting drug therapy.
No PGx Testing
Patients newly diagnosed with HIV infection were treated with the first-line ART regimen and opportunistic infection therapy without undergoing PGx testing. Based on the Thailand’s National Guidelines on HIV/AIDS Diagnosis, Treatment, and Prevention 2020/2021,6 the first-line NRTI backbone regimen consists of a combination of tenofovir/emtricitabine (TDF 300 milligram (mg)/FTC 200 mg or TAF 25 mg/FTC 200 mg) plus dolutegravir (DTG) 50 mg, tenofovir-containing regimens. If patients developed serious ADRs due to the first-line treatment, abacavir/lamivudine (ABC 600 mg/3TC 300 mg) with DTG 50 mg, abacavir-containing regimens would be recommended as the second-line ART regimen. If a patient taking abacavir developed a suspected HSR, zidovudine/lamivudine (AZT 600 mg/3TC 300 mg) with DTG 50 mg, zidovudine-containing regimen recommended as the third-line ART regimen. As a result, the ART regimen was provided life-long treatment.
Based on Thailand’s National Guidelines on HIV/AIDS Diagnosis and international guidelines, co-trimoxazole or trimethoprim/sulfamethoxazole (TMP/SMX), 80 mg TMP plus 400 mg SMX (1–2 tablets) daily or 160 mg TMP plus 800 mg SMX three times per week was recommended as the drug of choice for primary prophylaxis of PCP in people living with HIV. Whereas 15 to 20 mg/kg (based on the TMP component) given in 3 or 4 equally divided doses every 6 to 8 hours for up to 14 days was recommended for the treatment of PCP.6,18,19 In patients who had serious ADRs to co-trimoxazole or other sulfa-drugs, either dapsone 100 mg daily or intravenous pentamidine 300 mg monthly could be used as an alternative for PCP prophylaxis.20,21 Moreover, clindamycin 600 mg plus primaquine 30 mg for 21 days could be used as the treatment of PCP.22
Regarding TB infection, the Thailand National Guidelines on TB/HIV and the World Health Organization (WHO) recommended the first-line treatment regimen for TB comprising a combination of isoniazid 5–8 mg/kg (or 300 mg), rifampicin 10 mg/kg (or 450–600 mg), pyrazinamide 25 mg/kg (or 1000–2000 mg), and ethambutol 25 mg/kg (or 800–1200 mg) as an initial treatment regimen for the first two months followed by isoniazid and rifampicin for four months.23,24 In patients who developed hepatotoxicity, half the standard isoniazid dosage for nine months was recommended to prevent hepatotoxicity from isoniazid.25–27
Model Structure
A combination of a hybrid of decision tree and Markov models was constructed based on the clinical practice in accordance with the Thailand’s National Guidelines on HIV/AIDS Diagnosis, Treatment, and Prevention 2020/2021.6 The model was used to determine lifetime costs and health outcomes between people living with HIV receiving either single or multiple PGx testing before starting drug therapy compared with those who did not get PGx testing. From this, the model started with the same adult cohort, individuals newly diagnosed HIV and aged more than 30 years old. The lifetime time horizon was employed with a one-year cycle length. Costs and outcomes were discounted at a rate of 3% per annum based on Thailand’s and the World Health Organization’s guidelines for health technology assessment.28,29
Figure 1A depicts the decision tree model displaying three treatment options for newly diagnosed HIV-infected patients, namely no PGx testing, single-PGx testing, and multiple-PGx testing, which combined four single-PGx tests in a single panel. If the patients had a positive test result of each testing, they would receive the alternative drug regimen. The first-line ART treatment starts with tenofovir-containing regimens; if they develop serious ADRs such as nephrotoxicity or if tenofovir is contraindicated, they are switched to ABC-containing regimens. Afterwards, when the condition progressed, treatment for opportunistic infection was provided.
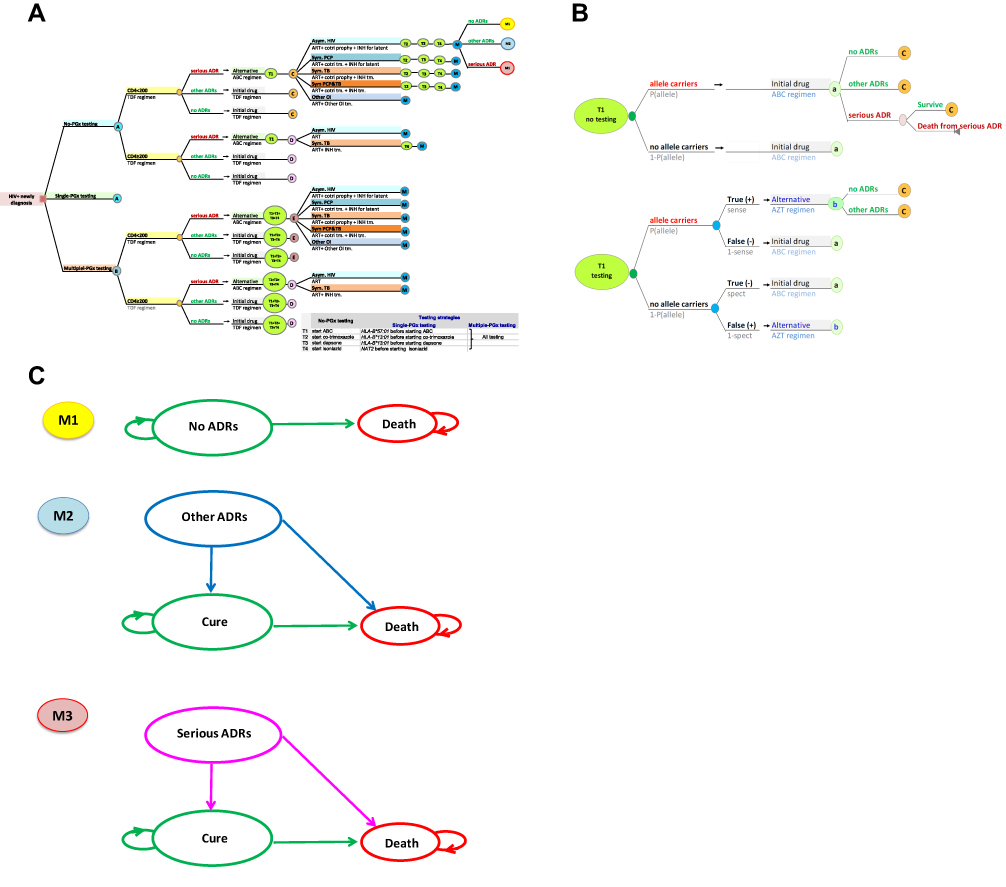 |
Figure 1 (A) Decision tree model. (B) Decision tree model (continue). (C) Markov model. Abbreviations: ABC, abacavir; ADR, adverse drug reaction; ART, Aantiretroviral therapy; Asym, asymptomatic; Cotri, Co-trimoxazole; INH, isoniazid; OI, opportunistic infection; NAT2, N-acetyltransferase 2; PCP, pneumocystis pneumonia; Prophy, prophylaxis; Sym, symptomatic; TB, tuberculosis; TDF, tenofovir; Tm, treatment. |
Five possible events were identified in patients with CD4 counts <200 cells per mm3: 1) asymptomatic HIV infection: patients would initially receive ART, co-trimoxazole prophylaxis and INH for latent TB; 2) symptomatic PCP infection: patients would start with ART, co-trimoxazole treatment and INH for latent TB; 3) symptomatic TB infection: patients would start with ART and INH treatment for TB infection and co-trimoxazole prophylaxis; 4) symptomatic PCP and TB infections: patients would start with ART and co-trimoxazole treatment and INH treatment; and 5) other opportunistic infections: patients would start with ART and other opportunistic infection therapy such as cryptococcal meningitis and toxoplasma encephalitis. For patient with CD4 counts ≥200 cells per mm3, two possible events were identified: 1) asymptomatic HIV infection: patients would start with ART and 2) symptomatic TB infection: patients would start with ART and INH treatment.
All strategies had potential outcomes, including 1) the development of serious ADRs, 2) other ADRs related to drug therapy, and 3) the absence of ADRs. The benefit of PGx testing strategies was to prevent serious ADRs associated with initial drug regimen by modifying the treatment regimen if the test results were positive, while patients with a negative test result would continue to receive the original drug regimen (Figure 1B).
In each strategy, a Markov model was used to represent the lifetime cost and health outcomes associated with the adoption of ART regimen and opportunistic infection therapy (Figure 1C). Patients who did not acquire any ADRs could remain in this health state or die during the next cycle, as shown in Figure 1C (M1). Patients who developed other ADRs could progress to health state of cure or die in the next cycle (Figure 1C, M2), whereas patients who developed serious ADR could progress to health state of cure or die as a result of those serious ADRs, as shown in Figure 1C (M3). Serious ADRs may be fatal if drugs are not promptly discontinued. Therefore, patients who developed serious ADRs (ie, HSR associated with abacavir, DRESS associated with co-trimoxazole, and SCAR associated with dapsone) would be removed off them. Except for hepatotoxicity associated with isoniazid, the dosage was halved for slow acetylators.
Model Assumptions
The following assumptions were used in this study: 1) no difference in the effectiveness between the first-line and alternative regimens (ie, tenofovir, abacavir and zidovudine-containing regimens) was assumed, 2) patients were assumed to adhere to treatment completely, and 3) since no multiple-PGx testing for people living with HIV was available on the market at the time of this study, its sensitivity and specificity were assumed to be equal to 0.99 referred from the PGxOne™,30 the panel testing covering more than 60 PGx tests in one panel from major therapeutic areas including gene-drug pairs in this study (ie, HLA-B*57:01, HLA-B*13:01, and NAT2) and currently available in the market, and 4) The cost of multiple-PGx testing was assumed to be equal to the total cost of four single PGx tests (ie, HLA-B*57:01 before prescribing abacavir, HLA-B*13:01 before prescribing co-trimoxazole and dapsone, and NAT2 before prescribing isoniazid) in the base-case scenario.
Model Parameters
The input parameters used in the model were classified into four major groups: epidemiological data and transition probabilities, effectiveness of testing, costs data, and utility parameters. The parameter values are presented in Table 1.
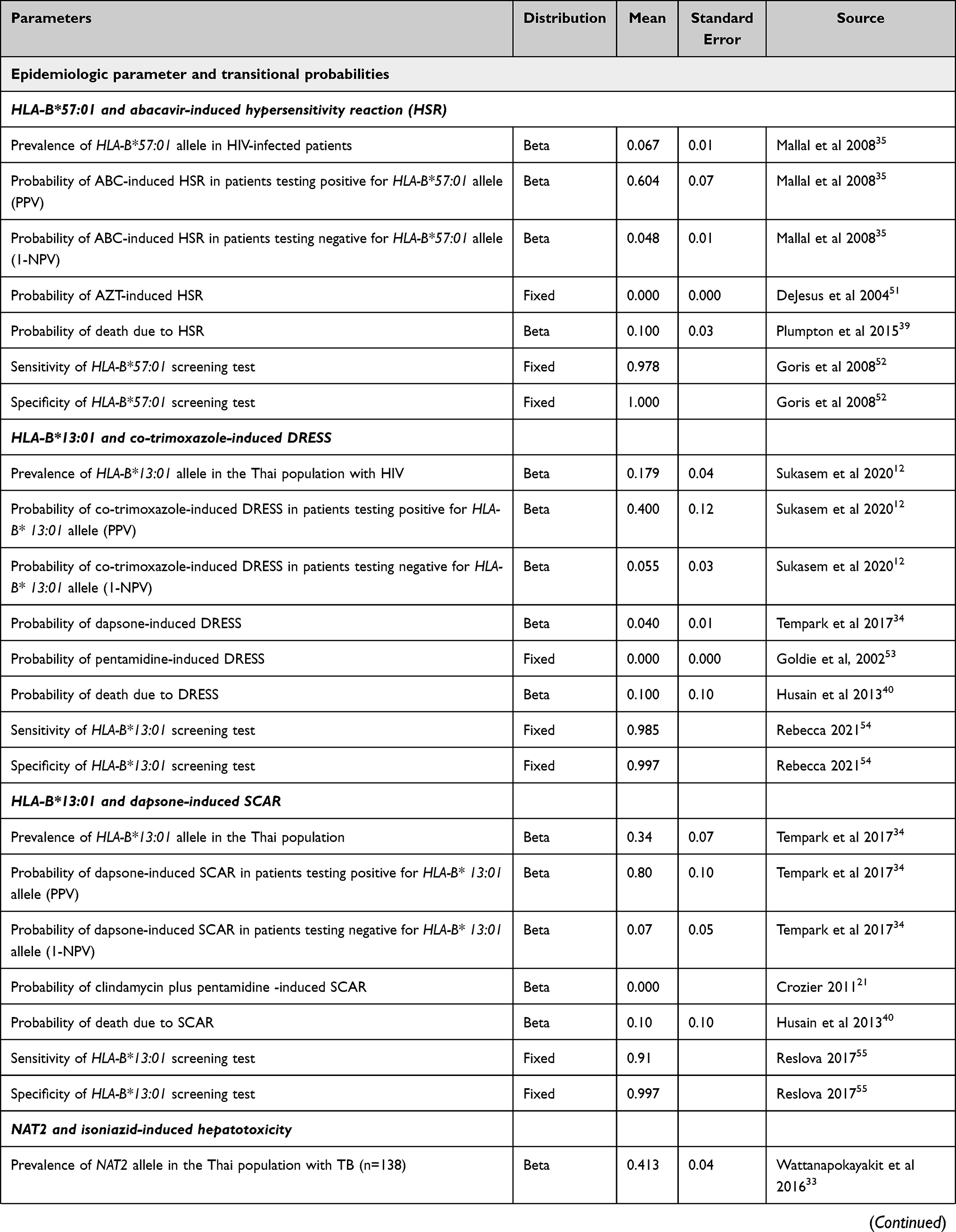 |  | 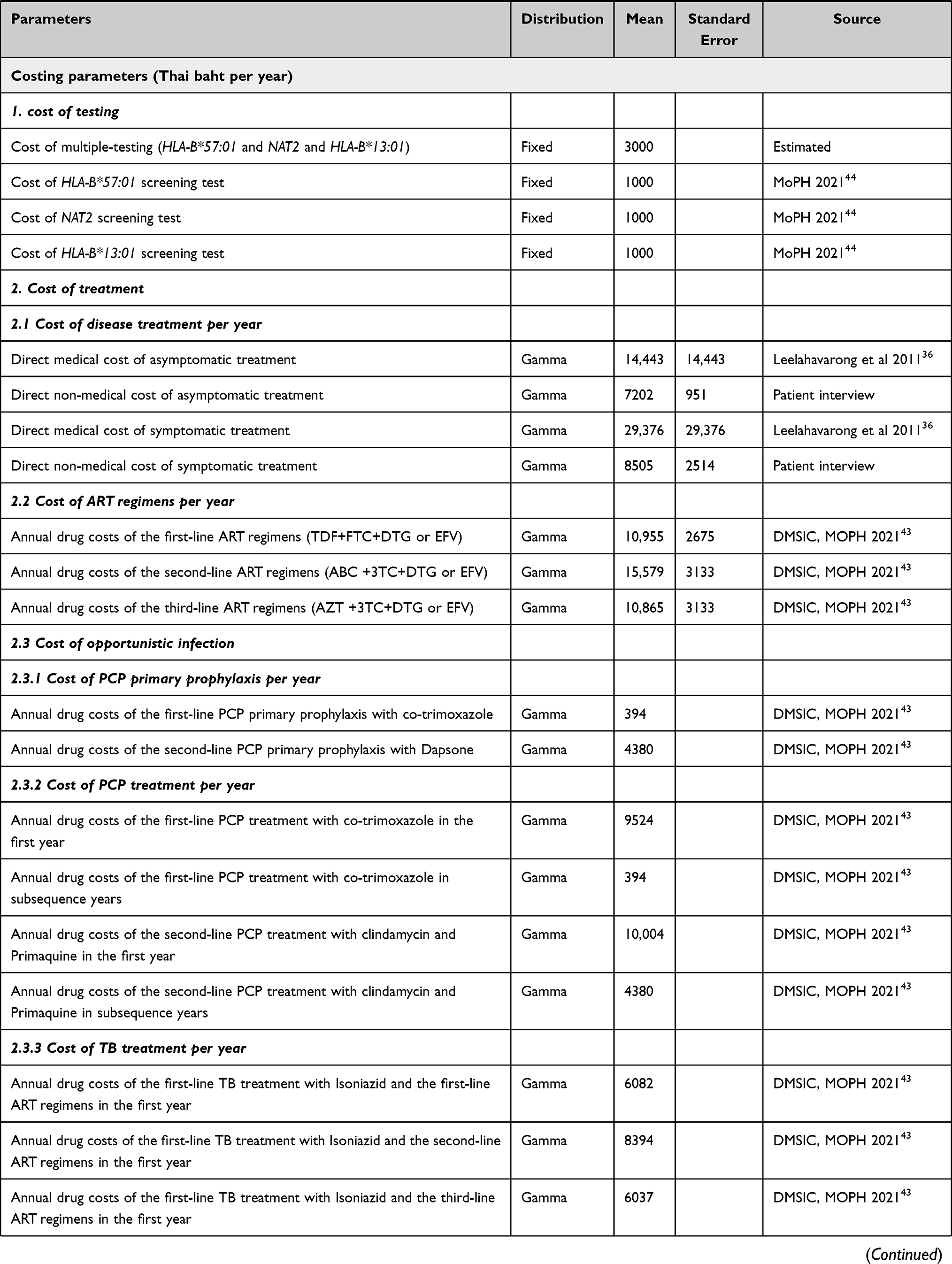 | 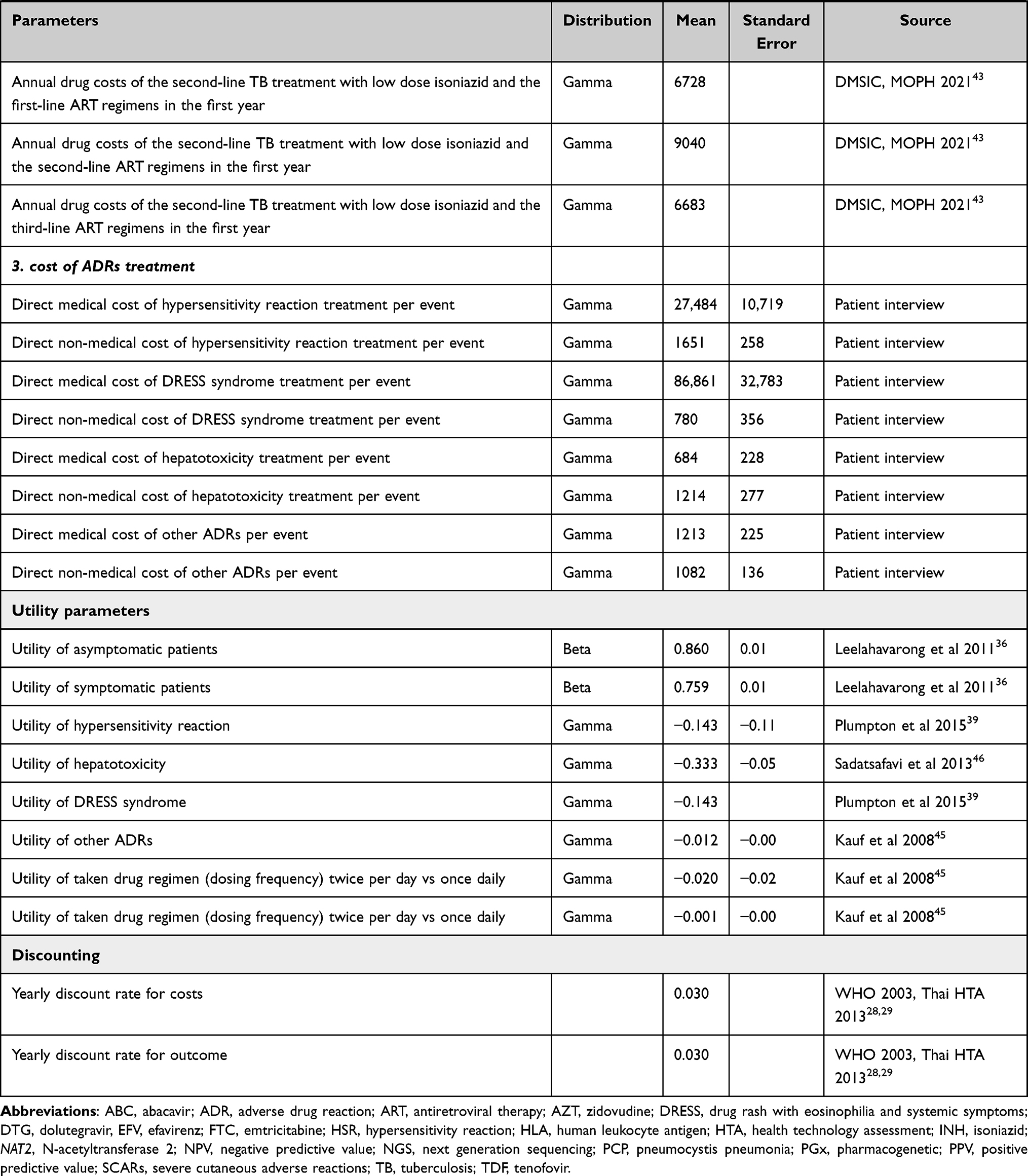 |
Table 1 Model Parameters in the Base-Case Analysis |
Epidemiological Data and Transition Probabilities
The incidence of asymptomatic HIV, symptomatic PCP, or TB patients was retrieved from published studies,31,32 which were conducted in Thai people living with HIV before starting ART. The base-case scenario adopted the frequencies of HLA-B*13:01 and NAT2 alleles in Thai HIV-positive people,12,33,34 whereas the frequency of HLA-B*57:01 allele was obtained from white HIV-positive people in Europe and Australia through the PREDICT-1 study.35 Moreover, The annual mortality rates among HIV asymptomatic, HIV symptomatic, and AIDS patients were estimated using data from two cohort studies of 880 people living with HIV in Thailand.36–38 The all-cause mortality rate was derived from the Thai Burden of Disease and Injury Study and was adjusted for age,1 while mortality rate caused by HSR, DRESS, and SCAR was set at 10%, and hepatotoxicity was 1%.39–41
Effectiveness of Testing
In the base-case scenario, the probability of drug-induced serious ADRs in patients testing positive for any allele or positive predictive value (PPV) was retrieved from published genetic association studies mainly focusing on Thai population,12,33 with exception of HLA-B*57:01 study, in which the probability was obtained from PREDICT-1 study.35 Moreover, the sensitivity and specificity of single-PGx testing were specified by the manufacturer, while those of multiple PGx testing were assumed to be equal to 0.99, referred from PGxOne™, which covered more than 60 PGx tests in one panel from major therapeutic areas, including gene-drug pairs in this study, ie, HLA-B*57:01, HLA-B*13:01 and NAT2.30
Cost
All costs were converted and reported in 2022 Thai baht (THB) values using the Thai consumer price index.42 Cost analysis was performed based on a societal perspective, taking into account both direct medical and non-medical costs. Direct medical costs included costs of ART regimens and opportunistic infection therapy, HIV treatment, ADRs management, single- and multiple-PGx testing. Costs of ART regimens and opportunistic infection therapy were calculated using the unit prices based on public hospital’s prevailing acquisition costs in 2022, announced by the Drug and Medical Supply Information Center (DMSIC), Ministry of Public Health.43 In addition, costs associated with HIV treatment including laboratory tests, hospitalization, and outpatient department (OPD) follow-up were obtained from a published study.36 These costs were calculated by multiplying the number of services used by their unit cost. Costs of managing ADRs including abacavir-induced hypersensitivity, co-trimoxazole-induced DRESS, dapsone-induced SCAR, and isoniazid-induced hepatotoxicity were retrieved from Buddhachinaraj Phitsanulok hospital databases containing a total of 465 people living with HIV aged 18 years or older who were hospitalized with serious ADRs in 2015 to 2019. Cost of single-PGx testing was estimated using the reimbursement price of the National Health Security Office (NHSO).44 Due to lack of data on cost of multiple-PGx testing, we assumed that it was equal to the total cost of three single-PGx tests (ie, HLA-B*57:01, HLA-B*13:01, and NAT2). Nevertheless, the cost’s higher and upper bounds were applied to the uncertainty analysis.
Moreover, direct non-medical costs related to ADRs therapy including transportation to hospitals, food for patients and caregivers, paid caregiver, and informal care (unpaid caregiver) were collected through interviews with 93 patients who had experienced serious ADRs in OPD from the aforementioned hospital.
Utility
Health outcomes were represented as quality-adjusted life-years (QALYs), which are calculated by the multiplying life years (LYs) by their utility score. The utility values (0 = death and 1 = full health) for each health state (ie, hypersensitivity and cure) and a decrease in utility (or disutility) in patients who developed ADRs like hypersensitivity syndrome were obtained from published literatures, in addition to treatment attributes such as dosing frequency (more than once per day) and the number of prescribed pills per day that contributed to the disutility.36,39,45,46
Result Presentation
The results were compared to the number needed to screen (NNS) for PGx testing in order to prevent one occurrence of serious ADRs. Total cost, Lys, and QALYs of three alternatives were estimated. The incremental cost-effectiveness ratio (ICER) was calculated by incremental cost divided by incremental QALY of single-PGx or multiple-PGx testing and compared to that of no testing. As recommended by the guidelines for health technology assessment in Thailand,29 the Thai societal willingness-to-pay threshold (WTP) of 160,000 THB per QALY gained was applied.
Uncertainty Analysis
Parameter Uncertainty
To address the uncertainty of all input parameters and assess their effects on the model, one-way deterministic sensitivity analysis (DSA) and multivariate probabilistic sensitivity analysis (PSA) were performed. DSA was performed by varying each input parameter within its 95% CI, and the Tornado diagram was used to display the range of ICER values. Moreover, PSA using a 1000-time Monte Carlo simulation was conducted to evaluate uncertainty of all parameters simultaneously with appropriate statistical distributions for each parameter, namely the beta-distribution for risks and utility and the gamma distribution for costs parameters. The cost-effectiveness acceptability curve (CEAC) was used to illustrate the probabilities of each alternative being cost-effective relative to a specified WTP threshold.
Scenario Analysis
The scenario analyses were performed by varying the prevalence and PPV of HLA-B*57:01, HLA-B*13:01, and NAT2, as these parameters might have an impact on the ICER values. The prevalence was estimated using the extreme values at the higher and lower bounds of prevalence in other setting. The prevalence of HLA-B*57:01 was estimated to be 9.5% in Eastern Europe ethnicity47 and 1.1% in Han Chinese.48 For HLA-B*13:01, 28% of Papuans and Australian aborigines and 0% of European and African populations49 were considered. For NAT2, 66% of the UK Caucasian and 10% of Korean population50 were utilized. Additionally, upper and lower bounds for the PPV were set at 50% of the base case values.
Threshold Analysis
Threshold analysis was undertaken to determine the ICER, in which the cost of multiple-PGx testing and the range of its sensitivity and specificity were varied. This analysis sought to determine the threshold at which point the decision would be altered (ie, where the ICER showed that the testing was no longer cost-effective).
Results
Base-Case Analysis
Compared with no PGx testing, PGx testing prior to initiating drug therapy could avoid the number of serious ADR cases (ie, abacavir-induced HSR, co-trimoxazole-induced DRESS, dapsone-induced SCAR and isoniazid-induced hepatotoxicity) by approximately 68 cases per year (Figure 2). Furthermore, the number needed to screen (NNS) showed that 40 patients needed to be tested for these PGx tests to prevent one case of serious ADR.
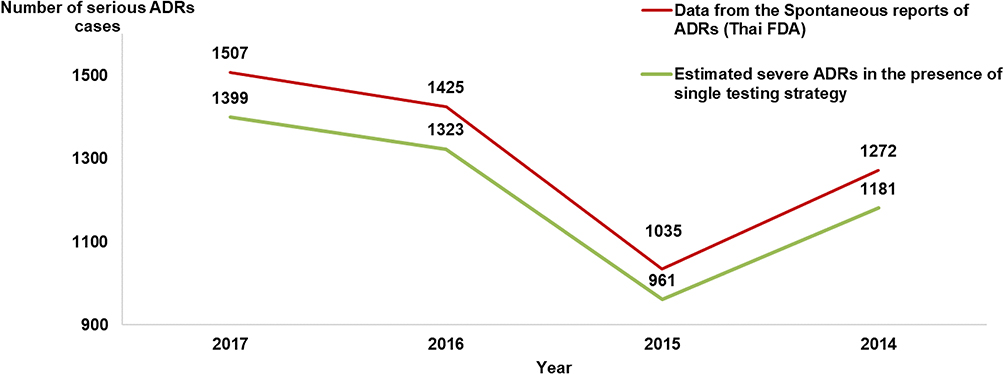 |
Figure 2 The incidence of serious ADRs relevant to Abacavir, co-trimoxazole and isoniazid when providing the multiple-pharmacogenetic testing. Abbreviations: ADRs, adverse Ddrug reactions; FDA, Food and Drug Administration. |
The total lifetime cost, LYs, QALYs, and ICER based on the societal perspective are detailed in Table 2. Compared with no PGx testing, single and multiple-PGx testing were both found to increase LYs and QALYs. Total LYs and QALYs were 24.87 LYs and 20.83 QALYs in the absence of PGx testing, 24.92 LYs and 20.88 QALYs for single-PGx testing, and 24.96 LYs and 20.91 QALYs for multiple-PGx testing. The lifetime costs of single-PGx and multiple-PGx testing were increased by approximately 8101 and 13,171 THB per patient, respectively, whereas QALYs were increased by 0.06 and 0.09, respectively, as compared with no PGx testing. These results indicated that single- and multiple-PGx tests were more slightly higher costs and more advantageous than initiating drug therapy without PGx testing, owing to the cost savings associated with ADR treatment. Consequently, approximately 35% and 40% of the cost of ADR treatment could be avoided by the implementation of single- and multiple-PGx testing, respectively.
 |
Table 2 Results of Total Lifetime Costs and Health Outcomes from the Base-Case Analysis Using a Societal Perspective |
The incremental cost-effectiveness ratio was estimated at 146,319 THB/QALY gained for single-PGx testing strategy and 152,014 THB/QALY gained for multiple-PGx testing compared with no PGx testing.
Uncertainty Analysis Results
The parameters influencing sensitivity of the ICER for multiple-PGx testing were the cost of ABC-containing regimens, the cost of TDF-containing regimens and probability of death from DRESS, respectively (Figure S1 in Supplementary Materials). Furthermore, when the WTP was 160,000 THB per QALY gained, probability of multiple-PGx testing being cost-effective was 45%, compared to no PGx testing (42%) and single-PGx testing (13%). Moreover, it is important to note that the cost-effectiveness of the multiple-PGx testing increased in correlation with the WTP threshold (Figure 3). The cost-effectiveness plane showed that single- and multiple-PGx testing were more expensive and more effective than no testing (Figure S2 in Supplementary Materials). Additionally, results suggested that there are several uncertainties around the mean of the ICER.
 |
Figure 3 Cost-effectiveness acceptability curves comparing the probabilities of being cost-effective at different willingness-to-pay of the non-PGx testing, single-PGx testing, and multiple-PGx testing. Abbreviations: PGx, pharmacogenetic; QALY, quality-adjusted life-year; THB, Thai baht. |
The scenario analyses were performed by varying the value of prevalence and PPV of HLA-B*57:01, HLA-B*13:01, and NAT2. Results from scenario analyses indicated that increases in prevalence and PPV of those tests might result in slightly increased the cost and QALYs of single-PGx testing. However, most scenarios continue to be cost-effective (Table S1 in Supplementary Materials).
Table 3 presents results of threshold analysis upon the ICER of each scenario when the cost of multiple-PGx testing and a range of sensitivity and specificity were varied. Compared to no PGx testing, multiple-PGx testing was shown to be cost-effective under the range of specificity at 0.98–1.00 and sensitivity at 0.95–1.00 as well as the range cost of multiple-PGx testing. For example, if sensitivity and specificity of multiple-PGx testing were both 0.99, multiple-PGx testing would be cost-effective when the cost was less than 3000 THB, but not when the cost exceeded 3000 THB.
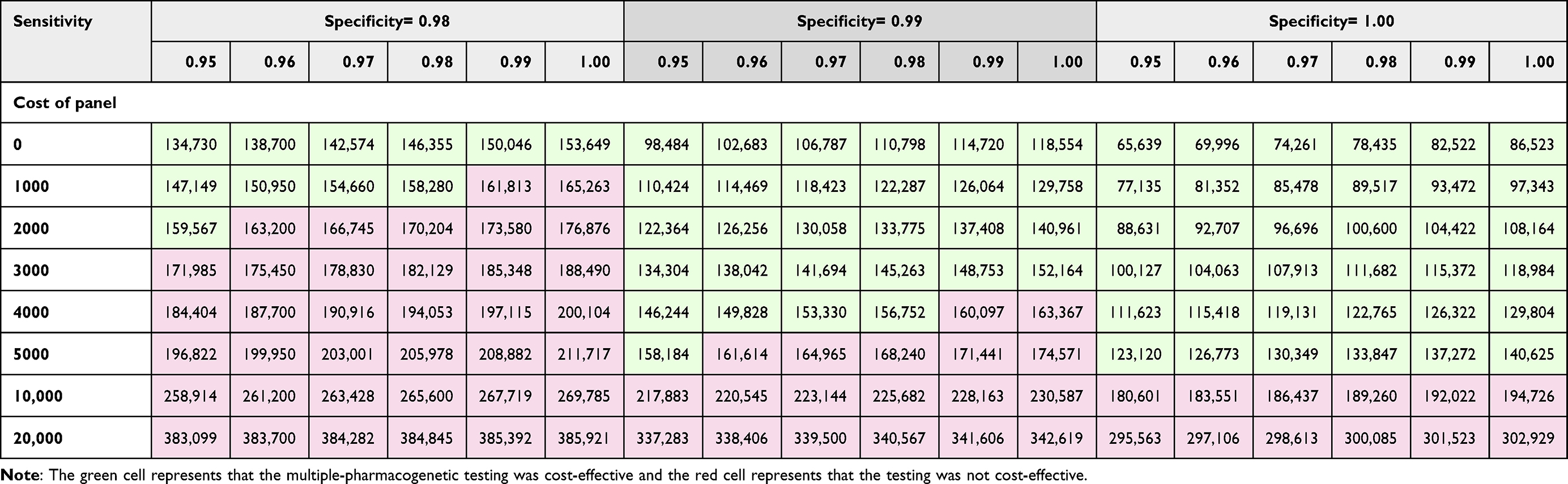 |
Table 3 Threshold Analysis Showing the Incremental Cost-Effectiveness Ratios (ICER) of Each Scenario, Classified by Cost, Sensitivity and Specificity of Multiple-Pharmacogenetic Testing |
Discussion
To the best of our knowledge, this study was the first to investigate the cost-utility of single- and multiple-PGx testing before starting drug therapy in people living with HIV compared to no PGx testing as a current practice. Our results suggested that both single- and multiple-PGx testing could help prevent serious ADRs and reduce the costs of ADR treatment. Moreover, the NNS demonstrated that 40 patients needed to be tested for those PGx to prevent one case of serious ADR. From a societal perspective, both single- and multiple-PGx testing were cost-effective strategies, indicating that they were more expensive and more effective than initiating drug therapy without PGx testing. Moreover, the probability of multiple-PGx testing being cost-effective was 45% compared to no PGx testing (42%) and single-PGx testing (13%) at the Thai willingness to pay threshold of 160,000 THB per QALY.
Currently, although four single PGx testing are available in Thailand and should be performed only once in a lifetime of people living with HIV, there is still low coverage rate of these PGx testing given that these tests have not been included in the UCS health benefit as a result of limited cost-effectiveness information. Hence, the findings from this study could be used to guide policymakers on whether to include either single- or multiple-PGx testing in the UCS health benefit package. These PGx tests may aid in not only identifying the multiple causative genes, but also in developing optimal treatment strategies based on the National Thai HIV treatment guidelines. In addition to this, capacity of PGx services in terms of a referral pathway and genetic counselling services should be considered, while implementing PGx. Alongside this, threshold analysis revealed that multiple-PGx testing was still cost-effective compared to no PGx testing under the range of sensitivity at 0.95–1.00 and specificity at 0.98–1.00 as well as the range cost of multiple-PGx testing. This information can be used to aid in the development of multiple-PGx testing before starting drug therapy in people living with HIV. In parallel with threshold analysis, given that the scenario analysis using a wide range of important parameter values were performed, the finding would be generalizable to other settings. Additionally, the developed method for determining the cost-effectiveness of multiple-PGx testing for preventing drug-induced serious ADRs in people living with HIV may be applied to assess value for money test in other clinical settings.
This study also provided supporting data on host genetic factors in ADRs, which may be helpful in reducing the detrimental effect of drug-induced serious ADRs. Our findings may be considered an extension of traditional approach for treating a disease, which allows clinicians to choose a medication therapy or intervention based on a patient’s genetic profile, a process known as personalized medicine. Furthermore, PGx testing has a significant impact on the rational use of drugs by reducing the development of side effects and preventing inappropriate treatment adjustment. This may have both therapeutic and economic benefits.
However, it should be noted that some inherent limitations of this study need to be taken into account. First, our analysis did not consider the possibility of different treatment regimens, drug resistance, and poor adherence, which are all conceivable in real practice. Besides this, each serious ADRs and other ADRs related to drug therapy occurred only once during the first year, and we did not consider lifelong ADRs or complications. This may lead to an underestimated value of the one-off testing. Second, due to the scarcity of local data, two input parameters were gathered from other countries. Another caveat is the fact that the prevalence of HLA-B*57:01 was obtained from the PREDICT-1 trial,35 a randomized, multicenter, double-blind trial of HLAB*57:01 genotyping abacavir-related HSRs in white Caucasians or Europeans. However, HLA-B*57:01 testing was included in this study, because abacavir-containing regimen would be a crucial component of an ART backbone regimen as a second-line treatment option for patients who had severe ADRs due to tenofovir or for whom tenofovir was contraindicated. In addition, the Thailand National Guidelines on HIV/AIDS mentioned that HLA-B*57:01 should be tested before starting abacavir to prevent HSR.6 In order to account for this constraint, we performed an uncertainty analysis to assess its effects on the ICER. For the other parameter, dosage adjustments of isoniazid were made in Europe and Japan based on NAT2 genotype-guided regimen to avoid hepatotoxicity.25–27 Taking these limitations into account, however, we conducted one-way and PSA to examine the effect of each parameter on the ICER results. Lastly, we were unable to determine the affordability and ability to implement PGxs testing. To address this challenge, budget impact and feasibility analyses should be executed in a future study.
Conclusion
Our findings indicated that both multiple- and single-PGx testing before prescribing HIV therapy could prevent serious ADRs and reduce the costs of ADR treatment. Collectively, given that genetic polymorphisms of several pharmacogenes have been shown to be involved in drug-induced serious ADRs, single- and multiple-PGx testing would be cost-effective options for preventing drug-induced serious ADRs in people living with HIV.
Ethics Approval
This study used anonymized and aggregated data related to the cost of managing ADRs conducted by our research team. All participants were required to provide written informed consent before enrolling and the commencement of the study. Ethical approval was granted by the Institutional Review Boards (IRB), Mahidol University (COA.No.MU-DT/PY-IRB 2020/016.1603) through the expedited review procedure. All procedures performed in the study complied with international guidelines for human research protection, such as the Declaration of Helsinki and the Belmont Report.
Acknowledgments
This work is a part of a study in Doctor of Philosophy program in Social, Economic and Administrative Pharmacy (SEAP), Faculty of Pharmacy, Mahidol University, Bangkok. Besides, this study was supported by grants from the International Research Network-The Thailand Research Fund (IRN60W003) and Health Systems Research Institute (HSRI61-080), Thailand. However, the funders had no role in the design, conduct of the study; collection, management, analysis and interpretation of data, and preparation of the manuscript. We would like to thank Miss. Waranya Rattanavipapong for her valuable advice. Our gratitude is also extended to all patients who participated in this study.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. The Thai Working Group on Burden of Disease and Injuries. Burden of disease and injuries in Thailand; 2002.
2. Country factsheets Thailand; 2019. Available from: https://www.unaids.org/en/regionscountries/countries/Thailand.
3. HIV Epidemic. Available from: https://hivhub.ddc.moph.go.th/epidemic.php.
4. Manosuthi W, Ongwandee S, Bhakeecheep S, et al. Guidelines for antiretroviral therapy in HIV-1 infected adults and adolescents 2014, Thailand. AIDS Res Ther. 2015;12:12. doi:10.1186/s12981-015-0053-z
5. Adolescents PoAGfAa. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services. Available from: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
6. Department of Disease Control, Ministry of Public Health. Thailand National Guidelines on HIV/AIDS Diagnosis, Treatment and Prevention 2020/2021. Thailand: Department of Disease Control, Ministry of Public Health; 2020.
7. Rodríguez-Nóvoa S, Barreiro P, Jiménez-Nácher I, Soriano V. Overview of the pharmacogenetics of HIV therapy. Pharmacogenomics J. 2006;6(4):234–245. doi:10.1038/sj.tpj.6500374
8. Whirl-Carrillo M, Huddart R, Gong L, et al. An evidence-based framework for evaluating pharmacogenomics knowledge for personalized medicine. Clin Pharmacol Ther. 2021;110(3):563–572. doi:10.1002/cpt.2350
9. Tangamornsuksan W, Lohitnavy O, Kongkaew C, et al. Association of HLA-B*5701 genotypes and Abacavir-induced hypersensitivity reaction: a systematic review and meta-analysis. J Pharm Pharm Sci. 2015;18(1):68–76. doi:10.18433/j39s3t
10. US Food and Drug Administration. Table of pharmacogenetic associations. Available from: https://www.fda.gov/medical-devices/precision-medicine/table-pharmacogenetic-associations.
11. Wang C-W, Tassaneeyakul W, Chen C-B, et al. Whole genome sequencing identifies genetic variants associated with co-trimoxazole hypersensitivity in Asians. J Allergy Clin Immunol. 2021;147(4):1402–1412. doi:10.1016/j.jaci.2020.08.003
12. Sukasem C, Pratoomwun J, Satapornpong P, et al. Genetic association of co-trimoxazole-induced severe cutaneous adverse reactions is phenotype-specific: HLA class I genotypes and haplotypes. Clin Pharmacol Ther. 2020;108(5):1078–1089. doi:10.1002/cpt.1915
13. Wang PY, Xie SY, Hao Q, Zhang C, Jiang BF. NAT2 polymorphisms and susceptibility to anti-tuberculosis drug-induced liver injury: a meta-analysis. Int J Tuberc Lung Dis. 2012;16(5):589–595. doi:10.5588/ijtld.11.0377
14. Richardson M, Kirkham J, Dwan K, Sloan DJ, Davies G, Jorgensen AL. NAT2 variants and toxicity related to anti-tuberculosis agents: a systematic review and meta-analysis. Int J Tuberc Lung Dis. 2019;23(3):293–305. doi:10.5588/ijtld.18.0324
15. Sukasem C, Jantararoungtong T, Koomdee N. Pharmacogenomics research and its clinical implementation in Thailand: lessons learned from the resource-limited settings. Drug Metab Pharmacokinet. 2021;39:100399. doi:10.1016/j.dmpk.2021.100399
16. Payne K, Shabaruddin FH. Cost-effectiveness analysis in pharmacogenomics. Pharmacogenomics. 2010;11(5):643–646. doi:10.2217/pgs.10.45
17. Department of Medical Services; Ministry of Public Health AND Infectious Disease Association of Thailand. Clinical Practice Guideline (CPG) of Tuberculosis Treatment in Thailand. Department of Medical Services; Ministry of Public Health; 2018.
18. Thomas CF, Limper AH. Pneumocystis pneumonia. N Engl J Med. 2004;350(24):2487–2498. doi:10.1056/NEJMra032588
19. Hughes WT, Rivera GK, Schell MJ, Thornton D, Lott L. Successful intermittent chemoprophylaxis for Pneumocystis carinii pneumonitis. N Engl J Med. 1987;316(26):1627–1632. doi:10.1056/nejm198706253162604
20. Awad WB, Asaad A, Al-Yasein N, Najjar R. Effectiveness and tolerability of intravenous pentamidine for Pneumocystis carinii pneumonia prophylaxis in adult hematopoietic stem cell transplant patients: a retrospective study. BMC Infect Dis. 2020;20(1):400. doi:10.1186/s12879-020-05127-y
21. Crozier F. Pneumocystis carinii pneumonia prophylaxis: current therapies and recommendations. J Pediatr Oncol Nurs. 2011;28(3):179–184. doi:10.1177/1043454211408101
22. World Health Organization. Guidelines on Co-Trimoxazole Prophylaxis for HIV-Related Infections Among Children, Adolescents and Adults: Recommendations for a Public Health Approach. World Health Organization; 2006.
23. World Health Organization. Guidelines for treatment of tuberculosis, 4th ed. Available from: http://www.who.int/tb/publications/2010/9789241547833/en/.
24. Department of Disease Control, Ministry of Public Health. Thailand National Guidelines on TB/HIV 2017. Thailand: Department of Disease Control, Ministry of Public Health; 2020.
25. Azuma J, Ohno M, Kubota R, et al. NAT2 genotype guided regimen reduces isoniazid-induced liver injury and early treatment failure in the 6-month four-drug standard treatment of tuberculosis: a randomized controlled trial for pharmacogenetics-based therapy. Eur J Clin Pharmacol. 2013;69(5):1091–1101. doi:10.1007/s00228-012-1429-9
26. Kinzig-Schippers M, Tomalik-Scharte D, Jetter A, et al. Should we use N-acetyltransferase type 2 genotyping to personalize isoniazid doses? Antimicrob Agents Chemother. 2005;49(5):1733–1738. doi:10.1128/aac.49.5.1733-1738.2005
27. Kubota R, Ohno M, Hasunuma T, Iijima H, Azuma J. Dose-escalation study of isoniazid in healthy volunteers with the rapid acetylator genotype of arylamine N-acetyltransferase 2. Eur J Clin Pharmacol. 2007;63(10):927–933. doi:10.1007/s00228-007-0333-1
28. Tan-Torres Edejer T, Baltussen R, Adam T, et al. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis. World Health Organization; 2003.
29. Chaikledkaew U, Teerawattananon Y. Guidelines for Health Technology Assessment in Thailand.
30. Admera Health PGxOne™ Plus. Genetic testing registry. NCBI. Available from: https://www.ncbi.nlm.nih.gov/gtr/tests/567653/performance-characteristics/.
31. Ningsanon P, Supawitkul S, Srisongsom S, Boason T, Nutchom K. CD4 monitoring in HIV infected patients not eligible for receiving ARV in 2004–2006. Dis Control J. 2008;34(1):11–21.
32. Rojanawiwat A, Tsuchiya N, Pathipvanich P, et al. Impact of the National Access to Antiretroviral Program on the incidence of opportunistic infections in Thailand. Int Health. 2011;3(2):101–107. doi:10.1016/j.inhe.2010.12.004
33. Wattanapokayakit S, Mushiroda T, Yanai H, et al. NAT2 slow acetylator associated with anti-tuberculosis drug-induced liver injury in Thai patients. Int J Tuberc Lung Dis. 2016;20(10):1364–1369. doi:10.5588/ijtld.15.0310
34. Tempark T, Satapornpong P, Rerknimitr P, et al. Dapsone-induced severe cutaneous adverse drug reactions are strongly linked with HLA-B*13: 01 allele in the Thai population. Pharmacogenet Genomics. 2017;27(12):429–437. doi:10.1097/fpc.0000000000000306
35. Mallal S, Phillips E, Carosi G, et al. HLA-B*5701 screening for hypersensitivity to Abacavir. N Engl J Med. 2008;358(6):568–579. doi:10.1056/NEJMoa0706135
36. Leelahavarong P, Teerawattananon Y, Werayingyong P, et al. Is a HIV vaccine a viable option and at what price? An economic evaluation of adding HIV vaccination into existing prevention programs in Thailand. BMC Public Health. 2011;11:534. doi:10.1186/1471-2458-11-534
37. Maleewong U, Kulsomboon V, Teerawattananon Y. The cost-effectiveness analysis of initiating HIV/AIDS treatment with efavirenz-based regimens compared with nevirapine-based regimens in Thailand. J Med Assoc Thai. 2008;91(Suppl 2):S126–38.
38. Leelukkanaveera Y. An Economic Evaluation of Routine Offer HIV Counseling and Testing of Out Patients at Community Hospitals in Thailand. Chulalongkorn University; 2009.
39. Plumpton CO, Yip VL, Alfirevic A, Marson AG, Pirmohamed M, Hughes DA. Cost-effectiveness of screening for HLA-A*31:01 prior to initiation of carbamazepine in epilepsy. Epilepsia. 2015;56(4):556–563. doi:10.1111/epi.12937
40. Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part I. Clinical perspectives. J Am Acad Dermatol. 2013;68(5):
41. Mo P, Zhu Q, Teter C, et al. Prevalence, drug-induced hepatotoxicity, and mortality among patients multi-infected with HIV, tuberculosis, and hepatitis virus. Int J Infect Dis. 2014;28:95–100. doi:10.1016/j.ijid.2014.06.020
42. Ministry of Commerce. Report for consumer price index of Thailand. Available from: http://www.indexpr.moc.go.th/price_present/TableIndexG_region.asp?table_name=cpig_index_country&province_code=5&type_code=g&check_f=i&year_base=2562&nyear=2552.
43. Ministry of Public Health. Drug And Medical Supply Information Center. Available from: http://dmsic.moph.go.th/index/drugsearch/1.
44. Department of Medical Sciences MoPH. Service fee for analysis and service. Availabe from: https://www3.dmsc.moph.go.th/.
45. Kauf TL, Roskell N, Shearer A, et al. A predictive model of health state utilities for HIV patients in the modern era of highly active antiretroviral therapy. Value Health. 2008;11(7):1144–1153. doi:10.1111/j.1524-4733.2008.00326.x
46. Sadatsafavi M, Marra C, Marra F, Moran O, FitzGerald JM, Lynd L. A quantitative benefit-risk analysis of isoniazid for treatment of latent tuberculosis infection using incremental benefit framework. Value Health. 2013;16(1):66–75. doi:10.1016/j.jval.2012.09.006
47. Wolf E, Blankenburg M, Bogner JR, et al. Cost impact of prospective HLA-B*5701-screening prior to Abacavir/lamivudine fixed dose combination use in Germany. Eur J Med Res. 2010;15(4):145–151. doi:10.1186/2047-783X-15-4-145
48. Kapoor R, Martinez-Vega R, Dong D, et al. Reducing hypersensitivity reactions with HLA-B*5701 genotyping before Abacavir prescription: clinically useful but is it cost-effective in Singapore? Pharmacogenet Genomics. 2015;25(2):60–72. doi:10.1097/fpc.0000000000000107
49. Satapornpong P, Jinda P, Jantararoungtong T, et al. Genetic diversity of HLA class I and Class II alleles in Thai populations: contribution to genotype-guided therapeutics. Front Pharmacol. 2020;11:78. doi:10.3389/fphar.2020.00078
50. Retno WS, Kinasih P, Intan R, Syukrini B, Rika Y. High frequency of NAT2 slow acetylator alleles in the Malay population of Indonesia: an awareness to the anti-tuberculosis drug induced liver injury and cancer. Med J Indones. 2017;26(1). doi:10.13181/mji.v26i1.1563
51. DeJesus E, Herrera G, Teofilo E, et al. Abacavir versus zidovudine combined with lamivudine and efavirenz, for the treatment of antiretroviral-naive HIV-infected adults. Clin Infect Dis. 2004;39(7):1038–1046. doi:10.1086/424009
52. Goris A, Walton A, Ban M, Dubois B, Compston A, Sawcer S. A Taqman assay for high-throughput genotyping of the multiple sclerosis-associated HLA-DRB1*1501 allele. Tissue Antigens. 2008;72(4):401–403. doi:10.1111/j.1399-0039.2008.01101.x
53. Goldie SJ, Kaplan JE, Losina E, et al. Prophylaxis for human immunodeficiency virus-related Pneumocystis carinii pneumonia: using simulation modeling to inform clinical guidelines. Arch Intern Med. 2002;162(8):921–928. doi:10.1001/archinte.162.8.921
54. Rebecca E. Sanger sequencing: past successes and current applications. Available from: https://www.cytivalifesciences.com/en/us/news-center/sanger-sequencing-past-and-present-10001.
55. Reslova N, Michna V, Kasny M, Mikel P, Kralik P. xMAP technology: applications in detection of pathogens. Front Microbiol. 2017;8:55. doi:10.3389/fmicb.2017.00055
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.