Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Economic Evaluation of Molecular Testing for Pulmonary Tuberculosis Diagnosis: A Systematic Review
Authors Chitpim N ![]() , Yoopetch P, Jittikoon J, Udomsinprasert W
, Yoopetch P, Jittikoon J, Udomsinprasert W ![]() , Bunwong K, Mahasirimongkol S, Chaikledkaew U
, Bunwong K, Mahasirimongkol S, Chaikledkaew U
Received 22 May 2025
Accepted for publication 20 September 2025
Published 1 October 2025 Volume 2025:17 Pages 661—671
DOI https://doi.org/10.2147/CEOR.S541923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dean Smith
Natthakan Chitpim,1 Panida Yoopetch,2 Jiraphun Jittikoon,3 Wanvisa Udomsinprasert,3 Kornkanok Bunwong,4,5 Surakameth Mahasirimongkol,6 Usa Chaikledkaew2,7
1Social, Economic and Administrative Pharmacy (SEAP) Graduate Program, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 2Mahidol University Health Technology Assessment (MUHTA) Graduate Program, Mahidol University, Bangkok, Thailand; 3Department of Biochemistry, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 4Department of Mathematics, Faculty of Science, Mahidol University, Bangkok, Thailand; 5Centre of Excellence in Mathematics, MHESI, Bangkok, Thailand; 6Office of Permanent Secretary, Ministry of Public Health, Nonthaburi, Thailand; 7Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand
Correspondence: Usa Chaikledkaew, Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, 447 Sri-Ayudhaya Road, Ratchathewi, Bangkok, 10400, Thailand, Email [email protected]
Purpose: Rapid molecular assays such as Xpert MTB/RIF and TB-LAMP accelerate pulmonary tuberculosis (TB) diagnosis but are more expensive than smear microscopy. This study provided an updated economic synthesis for presumptive adult pulmonary TB in high-burden settings, broadening the evidence from Xpert MTB/RIF to other WHO endorsed tests compared to conventional strategies.
Methods: Medline, Embase and Scopus were searched through March 2025. The strategy combined search terms related to molecular diagnostic tests, pulmonary tuberculosis, and economic evaluation study designs. Full economic evaluations comparing molecular tests with smear microscopy, culture or passive case-finding were eligible. Two reviewers independently screened articles, extracted data, and adjusted costs to 2025 US dollars (USD) using average exchange rates. Reporting quality was appraised using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 checklist. Due to heterogeneity in evaluation criteria, model structures, time horizons, and outcome measures, meta-analysis were not feasible. Therefore, results were synthesized narratively, and incremental cost-effectiveness ratios (ICERs) were contextualized against country-specific cost-effectiveness thresholds to enable meaningful cross-study interpretation.
Results: Eight studies conducted in low- and middle-income countries with high TB burdens were included. All evaluated Xpert MTB/RIF and the Thai studies also examined TB-LAMP. Five studies reported cost per disability-adjusted life years (DALYs) averted or quality-adjusted life years (QALYs) gained, while three used TB cases detected or years of life saved (YLS). CHEERS reporting quality was high (median is 23/28 items). Reported ICERs for molecular testing were either cost-saving or highly cost-effective compared with country-specific thresholds. Probabilistic sensitivity analyses (five studies) indicated ≥ 90% probability of cost-effectiveness in four studies and 6% in one.
Conclusion: Recent evidence supports the cost-effectiveness and cost-saving of Xpert MTB/RIF and TB-LAMP for diagnosing adult pulmonary TB. Policymakers should prioritize reducing cartridge costs and implementing models that capture patient-level benefits to maximize economic benefits.
Keywords: Xpert MTB/RIF, cost-effectiveness, molecular testing, systematic review
Introduction
Tuberculosis (TB) remains a major global health challenge. In 2024, the World Health Organization (WHO) estimated approximately 10.8 million new cases equivalent to 133 per 100,000 population and 1.25 million TB-related deaths.1 Over 80% of this burden occurred in low- and middle-income countries.1 Achieving the End TB Strategy targets, which aim for an 80% reduction in TB incidence and a 90% reduction in mortality by 2030, will require timely and accurate diagnosis as a critical component.2 Conventional sputum-smear microscopy detects fewer than half of active pulmonary TB cases, and mycobacterial culture generally requires several weeks to yield results. Health economic evaluations are essential tools that provide policymakers with the evidence needed to guide resource allocation for TB diagnostics.
Consequently, the WHO now recommends rapid nucleic acid amplification tests (NAATs), including Xpert MTB/RIF Ultra, Truenat, TB-LAMP, and line-probe assays (LPA), as the initial diagnostic options for individuals with presumptive TB.3 These assays demonstrate pooled sensitivities of ≥85% and specificities >95%, significantly reducing the median time from patient presentation to treatment initiation from weeks to days.4,5 However, the substantial capital investment, high cartridge costs, and ongoing maintenance requirements raise concerns about affordability in resource-constrained settings. Table S1 summarizes the strengths and weaknesses of these diagnostic tools.
Two systematic reviews have previously evaluated the economic value of Xpert MTB/RIF. Sagili et al concluded that Xpert MTB/RIF was highly cost-effective across high-burden settings, while noting considerable heterogeneity in costing methods, price-year adjustments, and outcome measures.6 Subsequently, Hao et al updated the evidence to mid-2019 and reached similar conclusions but highlighted a lack of economic evaluations for alternative molecular tests such as TB-LAMP or LPA.7 Although Xpert MTB/RIF, TB-LAMP, and LPA differ in technical performance, infrastructure requirements, and intended use cases, they are frequently considered alternative or complementary options within national TB diagnostic algorithms, particularly in high-burden settings. Since 2019, several comprehensive economic evaluations have emerged, incorporating dynamic transmission or program-level models and accounting for recent reductions in cartridge price.
In response to this evidence gap, we conducted a systematic review to synthesize economic evaluations of all WHO-endorsed rapid molecular diagnostics, ie, Xpert MTB/RIF, TB-LAMP, and LPA compared with conventional diagnostic strategies in presumptive adult pulmonary TB, including individuals with or without HIV infection, using literature published through March 2025. Although operationally distinct, these tests are WHO-recommended initial diagnostics and are often weighed as comparable policy alternatives. By standardizing monetary inputs to 2025 local prices and evaluating reporting quality using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 checklist, this review provides an up-to-date, methodologically consistent synthesis to guide policymakers in scaling-up rapid molecular testing in high-burden, resource-constrained settings.
Methods
This systematic review was conducted in accordance with a pre-registered protocol (PROSPERO registration number: CRD 42022362042) and reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 statement, an updated guideline for reporting systematic reviews.8
Data Sources and Searches
Electronic databases were performed across three electronic databases: MEDLINE (via PubMed), Scopus and Embase, covering all literature published up to March 2025. The search strategy included terms related to interventions (I), outcomes (O) and study design (S), while population (P) and comparators (C) were excluded to allow broader sensitivity and irrelevant results were manually excluded during the selection process. The full search strategies were shown in Table S2.
Search terms for the intervention (I) included: (“Xpert” OR “Cepheid” OR “Genexpert” OR “MTB/RIF”) OR (“loop mediated isothermal amplification” OR “LAMP”) OR (“line probe assay” OR “LPA”). For the population (P), the term used was “tuberculosis”. For the study design (S), terms include: “economic evaluation” OR “cost-effectiveness analysis” OR “cost-utility analysis” OR “cost-benefit analysis” OR “cost-minimization analysis”. Within each domain, search terms were combined using the Boolean operator “OR”, and terms across domains were combined using “AND”.
Selection of Studies
Two independent reviewers (NC and PY) evaluated the eligibility of studies based on titles and abstracts. When eligibility could not be determined, full texts were retrieved and reviewed. Disagreements were resolved through discussion and, if necessary, consultation with a third reviewer (UC). Studies were included if they met the following criteria. Firstly, they were full economic evaluation studies including cost-effectiveness, cost-utility, cost-benefit, or cost-minimization analyses comparing the cost-effectiveness of molecular testing with conventional culture-based strategies considered as a gold standard for diagnosing pulmonary TB. Secondly, studies were included if they involved adult participants (aged ≥15 years, as defined by WHO1) with presumptive pulmonary TB with or without HIV infection. Studies were excluded if they met any of following criteria. Firstly, they were review articles, editorials, or commentaries. Secondly, they lacked both cost and outcome data for the evaluated interventions. Lastly, the full text was not available in English or Thai. These eligibility criteria are summarized in Table 1.
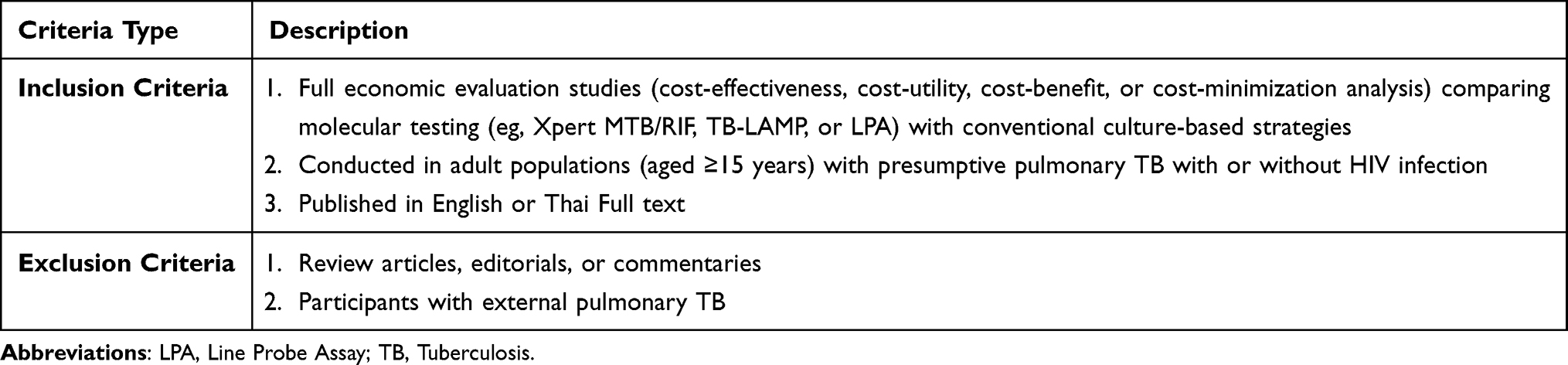 |
Table 1 Inclusion and Exclusion Criteria for Study Selection |
Data Extraction and Quality Assessment
Two independent reviewers (NC and PY) used standardized data extraction forms to collect information relevant to the research question, methodology, and study characteristics. Extracted data were cross-checked and validated for completeness and accuracy. Three key domains were assessed for each included study: methodological variations, transparency of reporting, and quality of input parameters. Extracted study characteristics included first author’s affiliation, funding sources, study setting, type of economic evaluation, models used, cost inputs, perspective, time horizon, cycle length, discount rate, and sensitivity analysis methods.
To evaluate the quality and transparency of reporting, the reviewers applied the CHEERS 2022 checklist,9 the current international standard for health economic evaluations. This updated framework reflects recent methodological advances, provides clearer guidance for consistent and transparent reporting, and ensures comparability across studies, making it preferable to earlier versions of CHEERS or other reporting tools. Detailed results of CHEERS assessment are presented in Table S3.
Data Synthesis and Analysis
This review aimed to compare the cost-effectiveness of Xpert MTB/RIF, TB-LAMP, and LPA in the diagnosis of pulmonary TB across the included studies. However, direct comparison was not feasible due to substantial heterogeneity among studies. Contributing factors included variations in perspectives (eg, societal, healthcare provider, governmental), time horizons, intervention and comparator combinations (eg, Xpert MTB/RIF alone vs Xpert MTB/RIF combined with other diagnostic tools) and outcome measures. Given this heterogeneity, a meta-analysis was not appropriate. Instead, the findings were summarized narratively. In accordance with established systematic review guidelines (eg, PRISMA), a narrative synthesis is an accepted approach when quantitative pooling is not feasible.8 While the synthesis is narrative, this review was conducted using rigorous systematic review methodology, including a registered protocol, comprehensive search strategy, dual independent screening, and formal quality appraisal.
For each study, the reported incremental cost-effectiveness ratios (ICERs) and corresponding cost-effectiveness (CE) thresholds were extracted and presented. These values were contextualized based on the country-specific thresholds or other willingness-to-pay (WTP) benchmarks employed by the study authors. Because the included studies varied in time horizons and outcome measures, eg, quality adjusted life years (QALYs), disability adjusted life years (DALYs), life years (LYs), years of life saved (YLS), we standardized all reported costs to 2025 United States dollars (USD) and compared ICERs against country-specific cost-effectiveness thresholds. This approach enabled consistent interpretation of cost-effectiveness across studies, despite heterogeneity in model structures, time horizons, and outcome metrics. Additionally, the WHO’s list of high TB burden countries1 was used for country classification. For studies that did not explicitly report the year of cost analysis, the year of publication was used as a proxy.
Results
Study Information
The database search identified 260 records (PubMed=82, Embase=78, Scopus=100). After removing 135 duplicates, 125 titles/abstracts were screened, resulting in the exclusion of 69 records. Of the 56 full-text articles accessed for eligibility, 48 were excluded, leaving eight studies for qualitative synthesis. The full PRISMA 2020 flow chart is presented in Figure 1. Table 2 presents characteristics of the included studies. Most of the included economic evaluations were conducted in low- and lower-middle-income countries with a high TB burden. Six studies were based in sub-Saharan Africa and South-East Asia—Mozambique,10 India,11 South Africa/Zambia/Zimbabwe/Tanzania,12 Ethiopia,13 Zambia14 and Thailand15—while two additional studies focused on Thailand’s national TB control context.16,17 All eight studies assessed Xpert MTB/RIF as the primary molecular diagnostic. The two Thai studies also examined TB-LAMP as an alternative or add-on diagnostic test.16,17 Of the articles assessed for eligibility, none were economic evaluations of LPA that met the inclusion criteria. In seven of the studies,10–13,15–17 sputum-smear microscopy served as the primary comparator, whereas one Zambian study compared a mobile X-ray plus Xpert screening strategy to passive case finding.14
 |
Figure 1 PRISMA 2020 flow diagram of study selection process. Abbreviations: EE, economic evaluation; HTA, health technology assessment. Note: Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.8 |
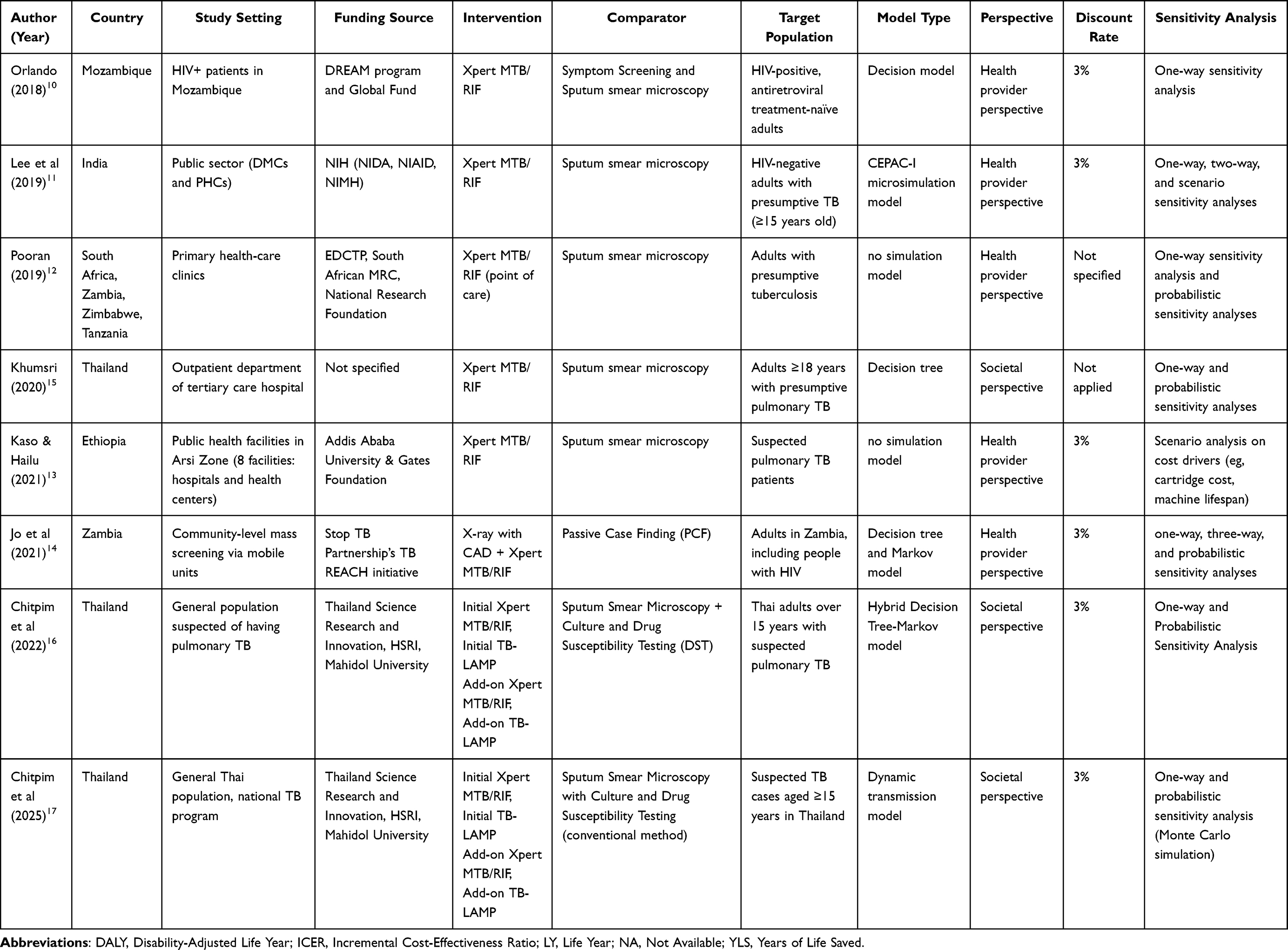 |
Table 2 Characteristics of Included Studies |
In terms of methodology, five studies adopted a cost-utility analysis, reporting outcomes in terms of DALYs or QALYs,10,12,15–17 while three studies presented cost-effectiveness in natural units such as TB cases detected or YLS.11,13,14 Most studies adopted a healthcare provider perspectives,10–14 while three applied a societal perspective to account for patient-incurred costs.15–17 Decision-tree frameworks were the most commonly used modelling approach, employed in three studies.10,13,15 These were complemented by a microsimulation model,11 a hybrid decision-tree–Markov structure,16 a dynamic transmission model17 and pragmatic trial-based or program-specific model.12,14 Time horizons varied: four studies focused on the diagnostic episode or a one-year period,10,12,13,15 one assessed a five-year program cycle;14 another modelled a 15-year horizon;17 and two projected outcomes over a lifetime period.11,16 A 3% annual discount rate was applied in six studies, while two studies did not discount due to short analytic time horizons.12,15 All studies conducted one-way sensitivity analysis, and five included probabilistic sensitivity analyses (PSA) to explore parameter uncertainty.11,14–17
Cost-Effectiveness Analysis Results
Table 3 presents the cost-effectiveness analysis results of all included studies. Rapid molecular testing primarily Xpert MTB/RIF was found to be either economically dominant or highly cost-effective relative to smear microscopy or passive case finding. Three analyses10,13,15 reported that Xpert was cost-saving, reducing total costs by 35–70 USD per patient while improving outcomes in terms of DALYs averted or TB cases detected. The remaining five studies reported favorable ICERs. In low-income, high-burden settings, the cost per DALY averted ranged from cost-saving to 57 USD12 and from 222 USD to 340 USD per YLS,11 well below commonly used WTP thresholds, typically 0.5–1 x GDP per capita. In Thailand, two studies comparing both Xpert and TB-LAMP reported ICERs between 1,290 USD and 1,340 USD per QALY gained,16,17 which remain comfortably within the national threshold of 4,500 USD per QALY gained. A single Zambian study14 evaluating a mobile digital-X-ray combined with Xpert yielded an ICER of 4,254 USD per additional bacteriologically confirmed TB initiation, which is below the country’s WTP threshold.
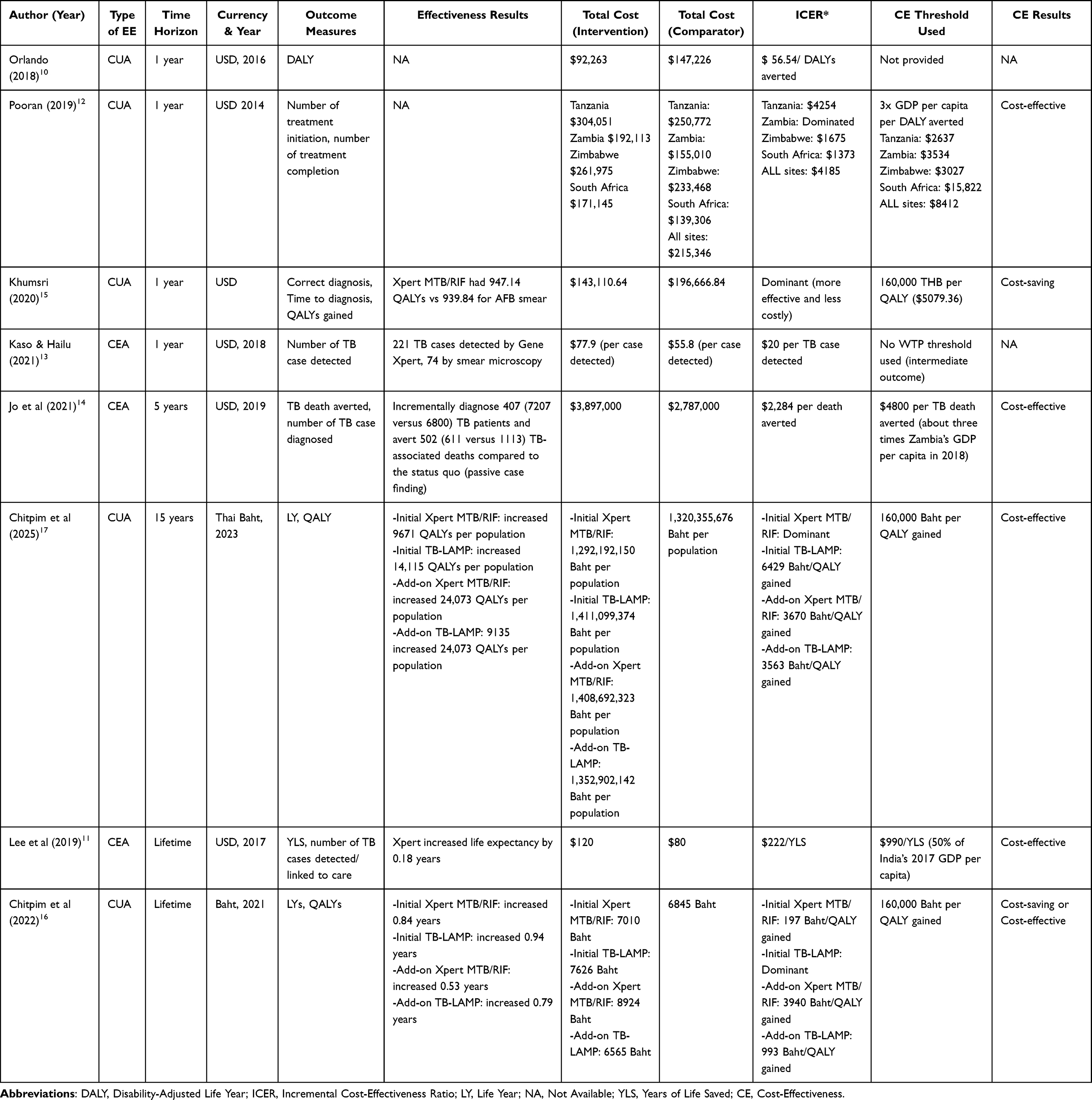 |
Table 3 Cost-Effectiveness Results of Included Studies |
PSA conducted in five studies consistently supported the base-case results. For example, Jo14 demonstrated a 97% probability that the mobile-X-ray plus Xpert intervention would be cost-effective at a WTP of 4,800 USD per TB death averted in Zambia. Both Thai studies16,17 revealed more than 95% probability of cost-effectiveness below the national threshold of 4,500 USD per QALY gained. Khumsri15 found Xpert to be economically dominant in all 1,000 Monte-Carlo simulations. Moreover, the analysis by Pooran12 was comparatively more uncertain, demonstrating a 61% probability of cost-effectiveness at its DALY-based WTP threshold. Across all PSA, the parameters with the greatest influence on ICERs were the price of diagnostic cartridge, the underlying prevalence of TB, and the costs associated with downstream treatment. Nevertheless, even under plausible variations in these parameters, molecular testing rarely exceeded country-specific WTP thresholds.
Quality Assessment of Reporting
Reporting quality was generally high among the included studies. Application of the 28-item CHEERS 2022 checklist revealed a median compliance of 23 items (82%), with individual scores ranging from 21/28 (75%) to 25/28 (89%). The most comprehensive reporting was observed in Lee,11 which fulfilled 25 items (89%), followed by Jo14 with 24 items (86%). Five studies10,11,13,14,16,17 exceeded the 80% “good” reporting threshold, whereas two studies12,15 were categorized as “moderate” at 75% (Table S3).
All studies consistently reported key elements, including the title, abstract, background and objectives, study population, setting, comparators, perspective, time horizon, currency and price date, resource-use measurement, and uncertainty analysis. However, no study provided a pre-published health-economic analysis plan (item 4) or discussed stakeholder engagement (item 20). Only one study11 mentioned the public availability of analytic code or data (item 28). Justification of model structure (item 16) and formal assessment of heterogeneity (item 18) were either missing or only briefly addressed in approximately half of the studies. Additionally, two studies with short time horizon did not report discounting.12,15
Discussion
This study presents the most-updated systematic review of economic evaluations of all WHO-endorsed molecular TB diagnostics, specifically Xpert MTB/RIF, TB-LAMP and LPA compared to conventional diagnostic strategies in presumptive adult pulmonary TB. Building upon previous systematic reviews, including those by Sagili et al and Hao et al, this review extends the evidence base to include studies published through March 2025.6,7 Notably, it significantly updates the last comprehensive review by Hao et al,7 which included studies only up to mid-2020. Over the past five years, the evidence base has become more refined. While earlier reviews included numerous heterogeneous conference abstracts, our analysis incorporated eight peer-reviewed journal articles, five of which were published after 2020. These studies provide more robust and detailed evaluations of both cost and effectiveness. Importantly, this review is the first to include dynamic transmission models and programmatic-level evaluations for TB-LAMP and for mobile X-ray combined with Xpert MTB/RIF, providing a more nuanced perspective on large scale implementation scenarios and their long-term public health impact.
Our review revealed that all eight eligible economic evaluation studies were conducted in Mozambique,10 India,11 South Africa, Zambia, Zimbabwe, Tanzania,12 Ethiopia,13 Zambia14 and Thailand,15–17 countries classified as low-, lower-middle-, or middle-income countries with a high-TB-burden. According to the WHO’s latest classification for 2021–2025, 30 countries are designated as high-burden for TB, accounting for nearly 87% of global TB cases.18 However, only nine of these countries have conducted economic evaluations of diagnostic tests for pulmonary TB. This highlights a significant gap in the evidence base and raises concerns about the lack of such studies in many high-burden countries.
To enable meaningful cross-country comparisons, an element lacking in previous reviews, we adjusted all ICER values to local prices, converted to 2025 USD, and compared them against country specific cost-effectiveness thresholds. Although our findings indicated that rapid molecular testing was either cost-saving or highly cost-effective across all studies,10–17 the key drivers of parameter uncertainty were cartridge price, underlying TB prevalence, and downstream treatment costs. These findings underscore the need for caution when generalizing economic evaluation results across countries, as differences in epidemiological contexts, health system capacity, and cost structures can significantly influence outcomes. Beyond the methodological considerations of the economic models, real-world implementation faces significant challenges, including infrastructural needs, logistical hurdles with supply chains, and the requirement for trained personnel. Overcoming these barriers is crucial to ensure the effective uptake of these molecular tests.
In addition, all included studies assessed Xpert MTB/RIF as the primary molecular diagnostic test,10–17 while two studies from Thailand16,17 also examined TB-LAMP, either as an alternative or as an add-on test compared with sputum-smear microscopy. These findings are consistent with WHO recommendations, which advocate the use of Xpert MTB/RIF Ultra, Truenat, and TB-LAMP as the initial diagnostic options for individuals with presumptive TB.3 Remarkably, our reviewed suggested that the majority of studies (5 out of 6 studies) applied a cost-utility analysis, reporting outcomes in terms of DALYs or QALYs, which are particularly relevant for informing policy decisions regarding the inclusion of TB diagnostic tests in healthcare benefit packages.10,12,15–17 Moreover, decision-tree models were the most commonly used modelling approach,10,13,15 followed by pragmatic trial-based or program-specific model,12,14 microsimulation model,11 a hybrid decision-tree–Markov structure,16 and a dynamic transmission model.17 Despite TB being an infectious disease with person-to-person transmission, only one study applied a dynamic transmission model to account for both the direct and indirect effects of TB transmission.17 This model specifically evaluated the potential impact of diagnostic delays such as differences in turnaround time between testing with molecular diagnostic tests and sputum-smear microscopy on disease spread within the community.17 However, conducting such dynamic models is often challenging due to their significant complexity and extensive data requirements, particularly for country-specific transmission parameters that are frequently unavailable. These findings suggest that future economic evaluation studies should incorporate dynamic transmission models to more accurately reflect the epidemiological and public health implications of diagnostic strategies.
In terms of quality assessment based on the 28-item CHEERS 2022 checklist, we excluded grey literature that did not meet minimum methodological standards, resulting in a more reliable evidence base. Overall, the reporting quality was generally high among the included studies. However, several important elements consistently lacking, including a pre-published health-economic analysis plan (item 4), stakeholder engagement (item 20), justification of model structure (item 16) and a formal assessment of heterogeneity (item 18). Future economic evaluations should aim to incorporate these components to enhance the transparency, methodological rigor and relevance to decision-makers.
It is important to acknowledge the limitations of our study. First, we included only English-language full-text articles and excluded grey literatures, which may contain valuable local insights on economic evaluation of molecular tests. Second, we assessed reporting quality solely using the CHEERS 2022 checklist. Although existing guidelines for quality assessment of health economics models have been published by the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) and the National Institute for Health and Care Excellence (NICE),19–21 we did not apply them in this review. Future studies should consider incorporating multiple quality appraisal tools to strengthen the robustness of their assessments.
Conclusion
In summary, this systematic review synthesized current evidence on the cost-effectiveness of rapid molecular diagnostics for presumptive adult pulmonary TB, including Xpert MTB/RIF, TB-LAMP and LPA, compared with conventional strategies, covering studies published up to March 2025. Eight studies were identified, all from high TB burden low- and lower-middle-income countries. Across diverse settings, these molecular tests were consistently found to be cost-saving or highly cost-effective. By contextualizing ICERs against country-specific thresholds, our review enabled meaningful interpretation across studies despite heterogeneity in time horizons, model structures, and outcome measures. In addition, key drivers of parameter uncertainty included cartridge prices, TB prevalence and downstream treatment costs. Based on the CHEERS 2022 checklist, the overall reporting quality of included studies was relatively high. However, our review also highlights a continued lack of economic evaluation studies of molecular diagnostic tests in many high-burden countries. Moreover, the generalizability of economic evaluation results across different settings should be approached with caution in policy decision making, given variations in epidemiological and health system contexts. Overall, our findings provide evidence to guide national TB programs in adopting rapid molecular diagnostics as cost-effective tools to optimize resource allocation in high-burden settings. This offers a strong economic rationale for policymakers to prioritize funding and scale-up of these diagnostics over conventional methods. To strengthen the evidence base, future research should incorporate dynamic transmission models and assess the equity implications of diagnostic strategies to ensure benefits reach the most vulnerable populations. Linking such evidence into national policy frameworks and donor funding priorities will be critical to accelerate adoption, maximize health gains, and support sustainable investments in TB control.
Acknowledgment
We also extend our sincere thanks to Dr. Pattara Leelahavarong at Siriraj Health Policy Unit, Faculty of Medicine Siriraj Hospital, Mahidol University for her invaluable guidance, technical advice, and unwavering support throughout the course of this study.
Funding
This research was supported by multiple funding sources. The Royal Golden Jubilee Ph.D. Scholarship (Grant No. PHD/0104/2559) was awarded to N.C. and U.C. by the Thailand Science Research and Innovation (TSRI), Ministry of Higher Education, Science, Research and Innovation. Additional support was provided by the Health Systems Research Institute (HSRI) and Mahidol University (Fundamental Fund: fiscal year 2024 by the National Science Research and Innovation Fund (NSRF)).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2024. 2025.
2. World Health Organization. The end TB strategy. 2015.
3. World Health Organization. Molecular WHO-recommended rapid diagnostics for screening. Available from: https://tbksp.who.int/en/node/1409?utm_source=chatgpt.com.
4. Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005–1015. doi:10.1056/NEJMoa0907847
5. Menzies NA, Cohen T, Lin -H-H, Murray M, Salomon JA. Population health impact and cost-effectiveness of tuberculosis diagnosis with Xpert MTB/RIF: a dynamic simulation and economic evaluation. PLoS Med. 2012;9(11):e1001347–e1001347. doi:10.1371/journal.pmed.1001347
6. Sagili KD, Muniyandi M, Nilgiriwala KS, et al. Cost-effectiveness of GeneXpert and LED-FM for diagnosis of pulmonary tuberculosis: a systematic review. PLoS One. 2018;13(10):e0205233. doi:10.1371/journal.pone.0205233
7. Hao X, Lou H, Bai J, Ding Y, Yang J, Pan W. Cost-effectiveness analysis of Xpert in detecting mycobacterium tuberculosis: a systematic review. Review. Int J Infect Dis. 2020;95:98–105. doi:10.1016/j.ijid.2020.03.078
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
9. CHEERS 2022 ISPOR Good Research Practices Task Force (2022); Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Int J Technol Assess Health Care. 2022;38(1):e13. doi:10.1017/S0266462321001732
10. Orlando S, Triulzi I, Ciccacci F, et al. Delayed diagnosis and treatment of tuberculosis in HIV+ patients in Mozambique: a cost-effectiveness analysis of screening protocols based on four symptom screening, smear microscopy, urine LAM test and Xpert MTB/RIF. PLoS One. 2018;13(7):e0200523. doi:10.1371/journal.pone.0200523
11. Lee DJ, Kumarasamy N, Resch SC, et al. Rapid, point-of-care diagnosis of tuberculosis with novel truenat assay: cost-effectiveness analysis for India’s public sector. Article. PLoS One. 2019;14(7):e0218890. doi:10.1371/journal.pone.0218890
12. Pooran A, Theron G, Zijenah L, et al. Point of care Xpert MTB/RIF versus smear microscopy for tuberculosis diagnosis in Southern African primary care clinics: a multicentre economic evaluation. Lancet Glob Health. 2019;7(6):e798–e807. doi:10.1016/s2214-109x(19)30164-0
13. Kaso AW, Hailu A, Quinn F. Costs and cost-effectiveness of Gene Xpert compared to smear microscopy for the diagnosis of pulmonary tuberculosis using real-world data from Arsi zone, Ethiopia. PLoS One. 2021;16(10):e0259056. doi:10.1371/journal.pone.0259056
14. Jo Y, Kagujje M, Johnson K, et al. Costs and cost-effectiveness of a comprehensive tuberculosis case finding strategy in Zambia. PLoS One. 2021;16(9):e0256531. doi:10.1371/journal.pone.0256531
15. Khumsri J, Hanvoravongchai P, Hiransuthikul N, Chuchottaworn C. Cost-effectiveness analysis of Xpert MTB/RIF for multi-outcomes of patients with presumptive pulmonary tuberculosis in Thailand. Value Health Reg Issues. 2020;21:264–271. doi:10.1016/j.vhri.2019.09.010
16. Chitpim N, Jittikoon J, Udomsinprasert W, Mahasirimongkol S, Chaikledkaew U. Cost-utility analysis of molecular testing for tuberculosis diagnosis in suspected pulmonary tuberculosis in Thailand. Clinicoecon Outcomes Res. 2022;14:61–73. doi:10.2147/ceor.S350606
17. Chitpim N, Praditsitthikorn N, White LJ, et al. Economic evaluation of diagnostic tests for Thai patients with tuberculosis: a dynamic transmission model approach. PLoS One. 2025;20(3):e0315772. doi:10.1371/journal.pone.0315772
18. World Health Organization. WHO releases new global lists of high-burden countries for TB, HIV-associated TB and drug-resistant TB. 2025. Available from: https://www.who.int/news/item/17-06-2021-who-releases-new-global-lists-of-high-burden-countries-for-tb-hiv-associated-tb-and-drug-resistant-tb?utm_source=chatgpt.com.
19. Weinstein MC, O’Brien B, Hornberger J, et al. Principles of good practice for decision analytic modeling in healthcare evaluation: report of the ISPOR task force on good research practices--modeling studies. Value Health. 2003;6(1):9–17. doi:10.1046/j.1524-4733.2003.00234.x
20. Drummond M, Barbieri M, Cook J, et al. Transferability of economic evaluations across jurisdictions: ISPOR good research practices task force report. Value Health. 2009;12(4):409–418. doi:10.1111/j.1524-4733.2008.00489.x
21. Excellence NIfHa C. Methods for the development of NICE public health guidance (third edition). Available from: https://www.nice.org.uk/process/pmg4/chapter/appendix-i-quality-appraisal-checklist-economic-evaluations.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review and Statistical Analysis of Factors Influencing the Cost-Effectiveness of Transcatheter Aortic Valve Implantation for Symptomatic Severe Aortic Stenosis
Heathcote L, Srivastava T, Sarmah A, Kearns B, Sutton A, Candolfi P
ClinicoEconomics and Outcomes Research 2023, 15:459-475
Published Date: 14 June 2023