Back to Journals » International Journal of General Medicine » Volume 14
Echocardiographic Normal Reference of Left Ventricular Contractile Reserve During Treadmill Exercise Stress Echocardiography in Healthy Chinese Adults – New Non-Sex-Specific Parameter for Left Ventricular Contractile Reserve Evaluation
Authors Wang Y, Li W, Zhang H, Zhang Q, Ding G, Guo Z, Deng Y, Li C, Yin L
Received 15 August 2021
Accepted for publication 12 October 2021
Published 23 October 2021 Volume 2021:14 Pages 7089—7098
DOI https://doi.org/10.2147/IJGM.S334400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yi Wang,1 Wenhua Li,1 Hongmei Zhang,1 Qingfeng Zhang,1 Geqi Ding,1 Zhiyu Guo,2 Yan Deng,1 Chunmei Li,1 Lixue Yin1
1Key Laboratory of Ultrasound in Cardiac Electrophysiology and Biomechanics of Sichuan Province, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2GE Cardiovascular Ultrasound Clinical & Research Department, Chengdu, People’s Republic of China
Correspondence: Lixue Yin
Key Laboratory of Ultrasound in Cardiac Electrophysiology and Biomechanics of Sichuan Province, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, 32#, Xierduan, 1st Ring Road, Chengdu, People’s Republic of China
Tel +86 18981838968
Email [email protected]; [email protected]
Purpose: Left ventricular (LV) contractile reserve is commonly used for LV systolic function assessment, while data on normal LV contractile reserve to exercise and the effect of gender on it are contradictory and limited, especially in Chinese adults. The aims of the present study are to clarify echocardiographic normal reference of LV contractile reserve during treadmill exercise stress echocardiography in healthy Chinese adults and to evaluate the sex-specific impact on it.
Patients and Methods: The study population consisted of 157 healthy Chinese adults. All subjects underwent comprehensive echocardiographic assessment at rest and immediately after a symptom-limited treadmill stress test. The impact of gender on LV contractile reserve was analyzed.
Results: The study population consisted of 157 healthy Chinese adults. All subjects underwent comprehensive echocardiographic assessment at rest and immediately after a symptom-limited treadmill stress test. The impact of gender on LV contractile reserve was analyzed.
Conclusion: Traditional LV contractile reserve of men was much higher than that of women in a healthy Chinese population. The difference might be because of higher BSA in men. ΔGLS was less influenced by METs and CI at rest compared to ΔEF. ΔGLS, and especially the ΔGLS index, might be considered as a more preferable contractile reserve parameter for clinical cardiac function evaluation.
Keywords: stress echocardiography, treadmill stress test, left ventricular contractile reserve, longitudinal strain
Introduction
Left ventricular (LV) systolic function plays an important role in establishing treatment strategy and prognosis in various cardiovascular diseases1,2. Current studies have shown that the LV ejection fraction (LVEF) lacks accuracy and sensitivity in detecting early subclinical impairment. In contrast, recent echocardiographic guidelines recommended routine LV global longitudinal strain (GLS) assessment while evaluating systolic myocardial performance3.
Stressing the heart can unmask subtle alterations in cardiac function that might not be detected during echocardiographic examination at rest. In the early stage of many diseases, resting LV systolic function may remain preserved, but LV contractile reserve for inotropic stimulation may be blunted. Depressed LV contractile reserve has been documented in patients with nonischemic heart diseases, such as mitral regurgitation, aortic regurgitation, hypertrophic cardiomyopathy, and diabetic cardiomyopathy, and is thought to represent an early manifestation of LV dysfunction4–8. The use of LV contractile reserve in pathological conditions implies the need to consider normal reference values derived from a healthy population. Despite showing great clinical potential, there are few data on normal values for LV contractile reserve in healthy individuals. Besides, some studies showed increased, unaltered, or even reduced LV strain during stress testing in healthy controls2,9,10. The latest guideline on ischemic heart disease claimed that optimal speckle-tracking echocardiography (STE) parameters for detection of ischemia remain uncertain, and additional studies are needed to define normal response to dobutamine and exercise stress11. The currently available LV contractile reserve values are mainly derived from North American and European population studies that may not be applicable to the Chinese population. Moreover, no studies have demonstrated whether sex-related differences exist in LV contractile reserve.
Therefore, the aims of the present study are to determine echocardiographic normal references for LV contractile reserve during exercise stress echocardiography (SE) in healthy Chinese adults and to evaluate sex-specific impacts on it.
Patients and Methods
Study Population
In a cross-sectional study design, we prospectively enrolled 157 healthy volunteers during the period from May 2018 to December 2019. Subjects were recruited through advertisements and among hospital employees, their relatives, and members of the local community. The participants had blood pressure values within normal reference ranges, had normal resting electrocardiographic results, were not taking any medications, were nonsmokers, and had no history of hypertension, diabetes, or cardiac diseases. All subjects underwent clinical examinations, resting 12-lead electrocardiography, and comprehensive transthoracic echocardiography at rest and immediately after maximal treadmill stress testing. Participants with suboptimal image quality were excluded.
The clinical examination comprised measurements of height, weight, body mass index (BMI) and resting blood pressure. Body surface area (BSA) was calculated according to the DuBois formula12. For the subsequent analysis, subjects were divided into two groups according to sex. Every participant was >18 years of age and was included after providing informed written consent according to the principles of the Declaration of Helsinki. The study was conducted after approval from the local scientific ethics committee of the Sichuan Provincial People’s Hospital.
Echocardiographic Data Acquisition
Transthoracic echocardiographic images were recorded in accordance with current guidelines using a commercially available ultrasound system Vivid E95 equipped with an M5S 3.5-MHz transducer (GE Vivid E95, Vingmed Ultrasound, Horten, Norway) at rest and immediately after exercise in the left lateral decubitus position. Electrocardiogram-triggered echocardiographic data were acquired and digitally stored in a cine-loop format for offline analysis with EchoPac (EchoPac 202, General Electric Vingmed Ultrasound).
LV end-diastolic and end-systolic volumes (LVEDV and LVESV) were measured in the apical two- and four-chamber views, and stroke volume (SV) was calculated from LVEDV and LVESV. The LVEF was calculated using the biplane Simpson’s method13. LVEDV, LVESV, and SV were indexed into BSA (presented as LVEDVI, LVESVI, and SVI, respectively). Cardiac output (CO) (SV * Heart rate (HR)) and cardiac index (CI) (CO/BSA) were calculated.
Speckle Tracking Imaging
Longitudinal myocardial deformation was assessed using a semiautomated 2D speckle tracking technique (EchoPac 202, General Electric Vingmed Ultrasound) with a typical temporal resolution of ≥70 frames/s. After manual tracing of the endocardial border and selecting the appropriate wall thickness, the software automatically identified six segments in each view and tracked the motion of acoustic markers. Segments that failed to track satisfactorily were readjusted manually, and, if this was ineffective, they were excluded from further analysis. The measurements comprised the greatest negative value on the strain curves. The timing of the aortic and mitral valve opening and closure was obtained using single-gated pulsed-wave Doppler traces. GLS was computed as the average value of all LV segments subjected to analysis. Longitudinal strain (LS) at different LV levels was computed as the average value of all segments at basal, middle, or apical level. GLS and LS at different levels were analyzed both at rest and postexercise (Figure 1). In this study, strain and changes in strain are reported in absolute values. All echocardiographic parameters were averaged over three consecutive cardiac cycles.
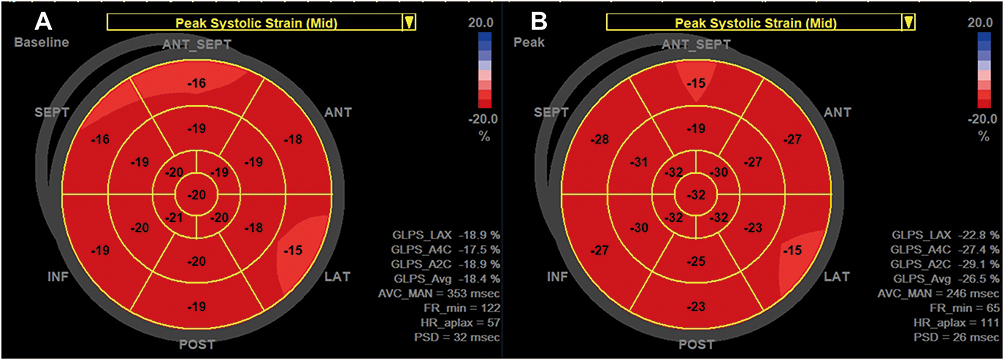 |
Figure 1 LV LS analysis at rest (A) and postexercise (B). LV LS of base, middle and apex were all increased after exercise, especially the apex. Abbreviation: LS, longitudinal strain. |
Exercise Protocol
All participants performed a symptom-limited treadmill (TMX-425, Full Vision Inc, Kansas) exercise test using the standard Bruce protocols.1 Subjects were encouraged to exercise until exhaustion. A baseline 12-lead electrocardiogram (ECG) and noninvasive blood pressure were acquired and repeated at 2-min intervals during the exercise test, at peak exertion, and after exercise. The maximum exercise capacity of metabolic equivalents (METs) was recorded, where 1 MET = 3.5 mL/kg/min oxygen consumption was estimated based on the protocol, speed, and grade achieved14. Exercise duration and ratio of peak HR to target HR (according to the 220-age formula) were also recorded automatically.
Assessment of LV Contractile Reserve
LVEF and LV GLS were analyzed at rest and postexercise. LV contractile reserve was calculated as the difference in LVEF and LV GLS between rest and postexercise values (presented as ΔEF and ΔGLS, respectively).
LV contractiles at different levels were calculated from LV LS change at the base, middle, and apex of LV. ΔEF and ΔGLS were also indexed to BSA as the LV contractile reserve index.
Statistical Analysis
Normally distributed data are presented as the mean±SD. Skewed data are presented as median (interquartile range [IQR]). Histograms and Q-Q plots were used to check continuous values for normality. Comparison of continuous variables between sexes was done using unpaired Student’s t-tests. The 95% confidence interval was calculated as ±1.96 SDs from the mean. The lowest (2.5th percentile) and highest (97.5th percentile) expected values for skewed data were estimated in 1000 bootstrap samples to generate the sampling distribution. To identify correlations of LV contractile reserve, univariable linear regression analysis was carried out. After excluding variables showing collinearity, all the variables that were significant in univariable analysis were entered into a stepwise multivariable regression analysis. P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 23.0 (SPSS, Armonk, NY).
Intraobserver and Interobserver Variability Analysis
GLS analyses at baseline and immediately after exercise were repeated in 10 randomly selected patients at least 4 weeks after the initial analysis by the original investigator and by a second investigator who were both blinded to the original measurements to assess intraobserver and interobserver variability. Intraclass correlations (ICCs) were evaluated.
Results
Characteristics of the Population
Resting and treadmill exercise SE were performed in 157 healthy volunteers (55% women; aged 45.3±13.0 years; age range, 22–74 years). All subjects were in sinus rhythm during examination. The clinical characteristics of the study population are displayed in Table 1. As expected, men were significantly taller and had larger BSA than women.
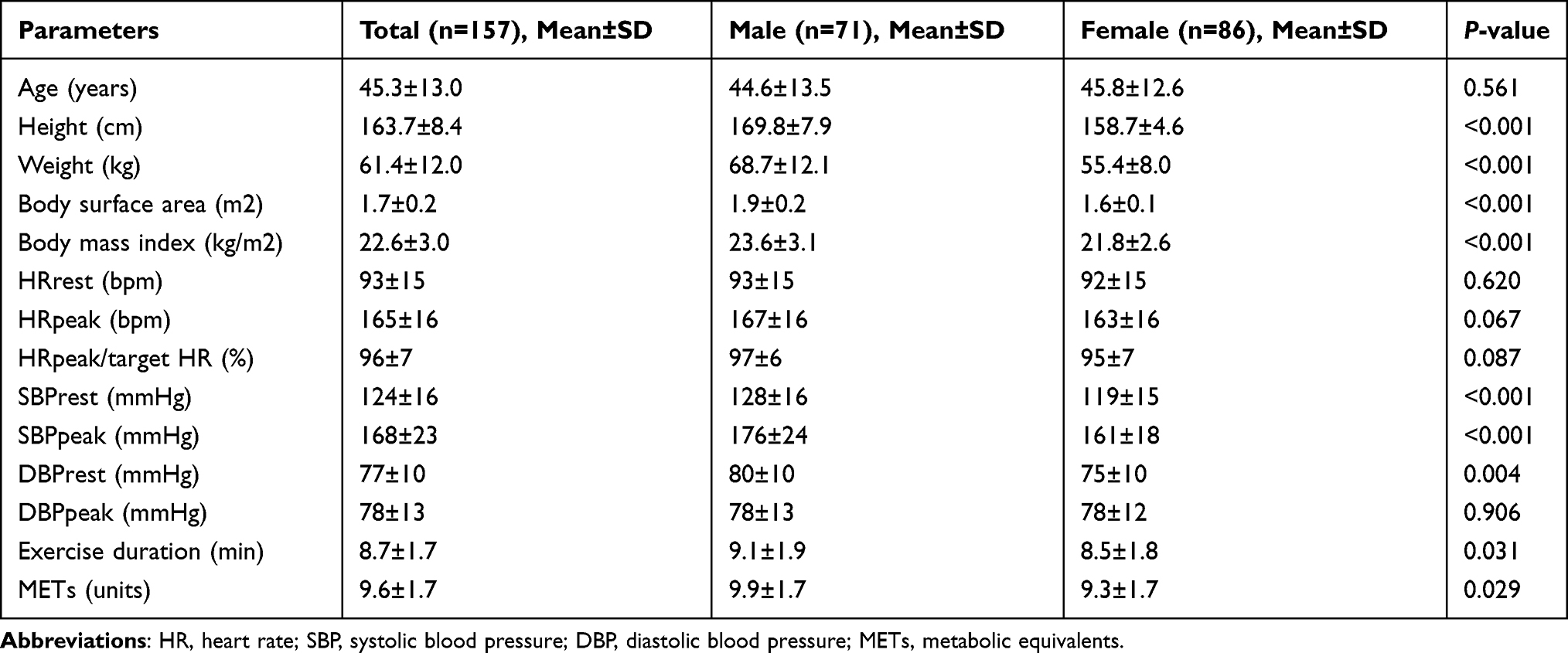 |
Table 1 Characteristics of the Population |
There were no statistically significant differences in HR at rest or at the peak of exercise. Systolic blood pressure (SBP) in men was higher compared with women both at rest and at the peak of exercise. The male group also showed longer exercise duration and higher exercise capacity.
Feasibility of Speckle Tracking Analysis
Speckle tracking analysis was feasible in all subjects. A total of 5338 segments were analyzed at rest and postexercise, of which 96 segments were excluded because of inadequate tracking quality (ie, lung interference). The remaining 5242 segments (98.2%) had successful tracking. Three of 314 LV GLS calculations were done by hand because of poor tracking of three of 17 segments. No LV GLS calculation was based on <14 segments.
Exercise Stress Echocardiography
Conventional treadmill exercise SE parameters for LV are summarized in Table 2. All subjects had normal LV geometry. The male group had a larger LV volume at rest. Significant differences were also found in LV SV, SVI, CO, and CI at rest. After exercise, no significant differences were found in LV EDV, EDVI, ESV, SVI, or CI. For LV systolic function, there is no significant difference in the traditional parameter EF at rest. With exercise, EF increased much higher in men compared to women.
 |
Table 2 Conventional Treadmill Exercise Stress Echocardiographic Parameters of the Left Ventricle |
GLS and LS at different levels were increased after exercise of course (Table S1). GLS in the female group was much higher than that in the male group at rest, whereas no significant difference was found in the two groups at postexercise (Table S1, Figure S1). The strain gradient at different levels of LV did not change either at rest or postexercise, with the highest LS at apex and the lowest LS at the base of LV (Figure 2). At rest, LS at the base and middle of LV was higher in women, but no significant difference was found in LS at the apex between groups. While at post-exercise, there were significant differences in LS at all three levels (Figure S1).
 |
Figure 2 LS changes during exercise at different levels of LV. The strain gradient at different levels of LV did not change either at rest or postexercise, with the highest LS at apex and the lowest LS at the base of LV. The LS of the apex increased much more than the other two levels. Abbreviations: LS, longitudinal strain; LV, left ventricle. |
LV Contractile Reserve
Details of LV contractile reserve are listed in Table 3. ΔEF and ΔGLS were much higher in men than women. After adjustment for BSA, no significant difference was found in ΔEFI and ΔGLSI between the two groups. The lowest expected values of LV contractile reserve were 0.03/m2 for ΔEFI and 0.52%/m2 for ΔGLSI. There were no significant differences in ΔLS in basal segments and middle segments between the two groups. ΔLS at the apex was much higher in males.
 |
Table 3 Changes in Exercise Characteristics |
Factors Influencing LV Contractile Reserve
ΔEF showed moderate correlation with BSA (r = 0.21, P = 0.004, Figure 3) and significant but weak correlations with BMI, METs, and CI at rest (r = 0.16, P = 0.023; r = 0.18, P = 0.013; r = −0.15, P = 0.029, respectively). In the multivariable analysis, ΔEF was independently associated with BSA (β = 0.23, P = 0.003), METs (β = 0.21, P = 0.006) and CI at rest (β = −0.31, P = 0.001).
 |
Figure 3 Correlation between parameters of LV contractile reserve and BSA. LV, left ventricle; BSA, body surface area; EF, ejection fraction; GLS, global longitudinal strain; %ΔEF, percentage of EF increase compared to rest; %ΔGLS, percentage of GLS increase compared to rest. |
The relative increase in EF (ΔEF to rest) showed moderate correlation with BSA (r = 0.21, P = 0.008, Figure 3), and significant but weak correlations with BMI (r = 0.17, P = 0.033), HRpeak/target HR (r = 0.19, P = 0.017), METs (r = 0.18, P = 0.024), and CI at rest (r = −0.178, P = 0.026). In the multivariable analysis, the relative increase in EF was independently associated with BSA (β = 0.23, P = 0.002), HR at rest (β = 0.31, P < 0.001), CI at rest (β = −0.35, P < 0.001), and METs (β = 0.21, P = 0.005).
ΔGLS showed significant correlations with BMI and BSA (r = 0.16, P = 0.025, and r = 0.23, P = 0.015, respectively, Figure 3). In the multivariable analysis, ΔGLS was only independently associated with BSA (β = 0.18, P = 0.03).
The relative increase of GLS (ΔGLS to rest) showed moderate correlations with BMI (r = 0.24, P = 0.003) and BSA (r = 0.27, P = 0.001, Figure 3). In the multivariable analysis, the relative increase in GLS was also only independently associated with BSA (β = 0.27, P = 0.001).
Intra- and Interobserver Reproducibility
The ICC for intraobserver variability was 0.92 for GLS at baseline and 0.84 for GLS at postexercise. The ICC for interobserver variability was 0.91 for GLS at baseline and 0.85 for GLS at postexercise.
Discussion
The present prospective study provides contemporary normal reference values for LV contractile reserve in different sexes in a large cohort of healthy Chinese volunteers. Our study showed that LV contractile reserve in men was much higher than that in women. The difference might be due to larger BSA of men. After adjusting for BSA, no significant difference was found in LV contractile reserve between sexes. In addition, the augmentation of systolic function is mostly driven by the apex. And ΔGLS, as well as the relative increase of the GLS, was less influenced by other parameters compared to ΔEF. ΔGLS, especially ΔGLS index, might be considered a more stable contractile reserve parameter for clinical applications.
Feasibility and Reproducibility of Speckle-Tracking Analysis
In our study, we achieved high (98.2%) feasibility of segmental speckle tracking during exercise. The reason for the high feasibility of our study might be that only normal subjects with a priori satisfactory image quality were enrolled.
Resting LV GLS measurements have proved robust and reproducible with low intra- and interobserver variability,2 which is in accordance with our findings in the present study. Although it decreased after exercise, ICC was still more than 0.80. Good reproducibility at different stages reinforces the possibility of a promising application of this echocardiographic parameter in daily clinical practice.
LV Contractile Reserve During Exercise SE
During the early stages of disease process, global LV functional parameters of volume and EF are usually preserved.3,4 Unless there has been a previous infarction or stunning of the myocardium, regional wall motion abnormalities are not evident at rest, and noninvasive detection of ischemia by transthoracic echocardiography requires stress provocation. Myocardial functional reserve between peak stress and rest reflects the recruitment of myocardial function during stress testing, which allows adequate adaptation of LV forward stroke volume and cardiac output to central and peripheral demands. In addition to chronotropic adaptation, LV improves contractility with an increase in longitudinal shortening, circumferential, and radial thickening.
Because EF and visual assessment of regional wall motion are based on radial thickening of the endocardial border, these parameters are less sensitive to detecting early ischemia.5,6 Furthermore, LVEF may overestimate LV systolic function due to the presence of the regurgitant volume in the left atrium, and could not reflect regional systolic function unless 3D echocardiography is used.7 In our study, ΔEF was influenced by lots of factors, which restricts its application in LV contractile reserve assessment. Magne et al found that the first consequences of LV myocardial damage primarily occur in longitudinal function before impairment of circumferential or radial function.8 Therefore, longitudinal strain, which has a predominant contribution from the endocardial layer, more accurately detects early derangement of cardiac function caused by ischemia, hypoxia and higher wall stress associated with hemodynamic overload.9 In patients with normal EF and absence of wall motion abnormalities, the discriminatory presence of reduced GLS provides incremental diagnostic value for detecting underlying coronary artery disease and other nonischemic diseases.4,6,10,11 In heart failure patients, a reduced contractile reserve could also be used for outcome prediction.12,13
In the early stage of many diseases, resting systolic function may remain preserved, but contractile reserve for isotropic stimulation may be blunted. Depressed contractile reserve is thought to represent an early manifestation of LV dysfunction.8,14–17 However, there is a paucity of data about myocardial strain change between rest and post-exercise in healthy adults.18 In healthy individuals, inotropic myocardial reserve usually increases myocardial deformation during exercise. Larsen et al found that the average absolute numeric LVGLS rises by approximately 5% in healthy subjects,18 which is the same as in our study.
Different Regional LS Change Between Rest and Post-Exercise During Exercise SE
Evaluation of LS at different levels may provide additional clinical value to GLS. Certain cardiac diseases, such as hypertrophic obstructive cardiomyopathy and amyloidosis, display a characteristic relative apical sparing pattern.19 Therefore, knowing the normal relative difference in apical, middle and basal LS allows comparison. In this study, the strain gradient at different LV levels did not change either at rest or postexercise, with the highest LS at apex and the lowest LS at the base of LV. The significant difference in GLS between groups was mostly driven by the change in apex of LV. Marwick et al showed a significant increase in LV LS from the LV base to apex also, which has been attributed to the specific curvature and architecture of the LV apical fibers.20 This specific structure might account for regional differences in LV mechanics that are responsible for the different distribution of contractile reserve across the LV.
Interestingly, a study showed LS changes observed during dobutamine SE displayed different region-related dispersion, with an increase in the apex, but decrease in the base and middle LV segments.21 This opposite direction of changes in regional deformation at different LV levels indicates the need for differentiation of segment-specific cut-off values for deformation-based ischemia detection during dobutamine SE. However, the LS of all three levels increased after exercise in our research, probably because we used exercise SE and all subjects were healthy volunteers, not patients with high coronary risk profiles.
Correlates of LV Contractile Reserve
We examined the impact of clinical characteristics and LV dynamic parameters on LV contractile reserve. Multivariable analysis showed that ΔEF was independently associated with BSA, METs, and CI at rest. While ΔGLS and the relative increase of GLS were only independently associated with BSA. This finding restricts the multiple factor influenced ΔEF as a stable parameter to evaluate LV contractile reserve. Other research found that exercise-induced changes in regurgitant volume influenced LV EF and might mask abnormal contractility.22 This finding also emphasizes that the assessment of myocardial contractile function by a volume-based functional parameter has important limitations in the setting of LV volume overload.
Cognet et al found that longitudinal strain reserve was significantly higher in overweight patients after dipyridamole infusion. After a multivariate analysis, only age remained independently associated with a decrease in longitudinal strain reserve. While the mean age of that study was 70 ± 11 years ranging from 46 to 90 years old, which is much higher than that in our research.23 However, we did not find any association between age and LV contractile reserve, probably due to different stresses and age distribution.
It is well known that the differences in cardiac chamber and great arterial dimensions among different racial and sex groups are attributable largely to variations in body size.24 In the present study, lots of parameters in men were significantly higher than in women, which suggests that it is important to take into account the impacts of sex on LV contractile reserve parameters, and it is more appropriate to use sex-specific reference values in clinical practice. At the same time, it should be noted that men had larger BSA than women in our research. There is a significant correlation between LV contractile reserve and BSA. In addition, ΔGLS and the relative increase of GLS were only independently associated with BSA. After adjusting for BSA, no significant difference was found in LV contractile reserve between sexes. Therefore, there is no need to use sex-specific references for LV contractile reserve. ΔGLS adjusted for BSA could be considered as a “one size fits all” LV contractile reserve index.
Limitations
This study reflects a single-center experience with a moderate sample size of 157 healthy patients. However, compared to most of the published studies to assess LV contractile reserve, the sample size of the present study exceeds previously reported data. And we will expand the sample size in the future to investigate the difference in LV contractile reserve among different age groups.
Second, we cannot rule out the presence of asymptomatic cardiovascular disease. Nevertheless, all patients demonstrated normal physiological responses to exercise on the standard hemodynamic and echocardiographic measures.
Third, certain limitations inherent to the technique of speckle tracking echocardiography, such as image quality dependency, are amplified during exercise stress test. Concurrently, increased heart rate reduces temporal resolution and strain accuracy. However, none of the patients were excluded because of inadequate imaging.
Conclusion
Speckle tracking imaging is feasible during exercise SE. In normal exercise SE studies, both global and regional strains increase during exercise, with the highest value of LV apical LS and the lowest value of LV basal LS. The LV contractile reserve of men was much higher than that of women in healthy Chinese adults. The difference might be because of the higher BSA of men. While ΔGLS was not influenced by METs, and CI at rest compared to ΔEF. After LV contractile reserve was adjusted by BSA, no significant difference was found between the two groups. ΔGLS, and especially the ΔGLS index and the relative increase of GLS, emerged beyond ΔEF as promising and more preferable contractile reserve parameters for noninvasive assessment of LV systolic function.
Ethics Approval and Informed Consent
Every participant was >18 years of age and was included after providing informed written consent according to the principles of the Declaration of Helsinki. The study was conducted after approval from the local scientific ethics committee of the Sichuan Provincial People’s Hospital.
Consent for Publication
Consent for publication was obtained from all the participants.
Acknowledgments
We are very grateful to all the participants in this research project.
Funding
This work was supported by a research grant from the National Natural Science Foundation of China (grant number: 81901762).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pellikka PA, Arruda-Olson A, Chaudhry FA, et al. Guidelines for performance, interpretation, and application of stress echocardiography in ischemic heart disease: from the American Society of Echocardiography. J Am Soc Echocardiography. 2020;33(1):1–41.e48.
2. Alcidi GM, Esposito R, Evola V, et al. Normal reference values of multilayer longitudinal strain according to age decades in a healthy population: a single-centre experience. Eur Heart J Cardiovasc Imaging. 2018;19(12):1390–1396.
3. Galli E, Lancellotti P, Sengupta PP, Donal E. LV mechanics in mitral and aortic valve diseases: value of functional assessment beyond ejection fraction. JACC Cardiovasc Imaging. 2014;7(11):1151–1166. doi:10.1016/j.jcmg.2014.07.015
4. Morris DA, Otani K, Bekfani T, et al. Multidirectional global left ventricular systolic function in normal subjects and patients with hypertension: multicenter evaluation. J Am Soc Echocardiography. 2014;27(5):493–500. doi:10.1016/j.echo.2014.01.017
5. Hanekom L, Cho GY, Leano R, Jeffriess L, Marwick TH. Comparison of two-dimensional speckle and tissue Doppler strain measurement during dobutamine stress echocardiography: an angiographic correlation. Eur Heart J. 2007;28(14):1765–1772. doi:10.1093/eurheartj/ehm188
6. Tops LF, Delgado V, Marsan NA, Bax JJ. Myocardial strain to detect subtle left ventricular systolic dysfunction. Eur J Heart Fail. 2017;19(3):307–313. doi:10.1002/ejhf.694
7. De Luca A, Stolfo D, Caiffa T, et al. Prognostic value of global longitudinal strain-based left ventricular contractile reserve in candidates for percutaneous correction of functional mitral regurgitation: implications for patient selection. J Am Soc Echocardiography. 2019;32(11):1436–1443. doi:10.1016/j.echo.2019.07.006
8. Magne J, Mahjoub H, Dulgheru R, Pibarot P, Pierard LA, Lancellotti P. Left ventricular contractile reserve in asymptomatic primary mitral regurgitation. Eur Heart J. 2014;35(24):1608–1616. doi:10.1093/eurheartj/eht345
9. Brecker SJ. The importance of long axis ventricular function. Heart. 2000;84(6):577–579. doi:10.1136/heart.84.6.577
10. Plana JC, Galderisi M, Barac A, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2014;15(10):1063–1093. doi:10.1093/ehjci/jeu192
11. Shimoni S, Gendelman G, Ayzenberg O, et al. Differential effects of coronary artery stenosis on myocardial function: the value of myocardial strain analysis for the detection of coronary artery disease. J Am Soc Echocardiography. 2011;24(7):748–757. doi:10.1016/j.echo.2011.03.007
12. Daros CB, Ciampi Q, Cortigiani L, et al. Coronary Flow, Left Ventricular Contractile and Heart Rate Reserve in Non-Ischemic Heart Failure. J Clin Med. 2021;10:15. doi:10.3390/jcm10153405
13. Pugliese NR, Deb N, Balletti A, et al. Characterisation of haemodynamic and metabolic abnormalities in the heart failure spectrum: the role of combined cardiopulmonary and exercise echocardiography stress test. Minerva Cardiol Angiol. 2021. doi:10.23736/S2724-5683.21.05743-4
14. Mahfouz RA, El Zayat A, Yousry A. Left ventricular restrictive filling pattern and the presence of contractile reserve in patients with low-flow/low-gradient severe aortic stenosis. Echocardiography. 2015;32(1):65–70. doi:10.1111/echo.12586
15. Cadeddu C, Nocco S, Piano D, et al. Early impairment of contractility reserve in patients with insulin resistance in comparison with healthy subjects. Cardiovasc Diabetol. 2013;12:66. doi:10.1186/1475-2840-12-66
16. Lancellotti P, Pellikka PA, Budts W, et al. The clinical use of stress echocardiography in non-ischaemic heart disease: recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur Heart J Cardiovasc Imaging. 2016;17(11):1191–1229. doi:10.1093/ehjci/jew190
17. Wu XP, Li YD, Zhang M, et al. Impaired left ventricular mechanics and functional reserve are associated with reduced exercise capacity in patients with hypertrophic cardiomyopathy. Echocardiography. 2019;36(2):266–275. doi:10.1111/echo.14241
18. Larsen AH, Clemmensen TS, Wiggers H, Poulsen SH. Left Ventricular Myocardial Contractile Reserve during Exercise Stress in Healthy Adults: a Two-Dimensional Speckle-Tracking Echocardiographic Study. J Am Soc Echocardiography. 2018;31(10):1116–1126.e1111. doi:10.1016/j.echo.2018.06.010
19. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: an Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016;17(12):1321–1360. doi:10.1093/ehjci/jew082
20. Marwick TH, Leano RL, Brown J, et al. Myocardial strain measurement with 2-dimensional speckle-tracking echocardiography: definition of normal range. JACC Cardiovasc Imaging. 2009;2(1):80–84. doi:10.1016/j.jcmg.2007.12.007
21. Wierzbowska-Drabik K, Plewka M, Kasprzak JD. Variability of longitudinal strain in left ventricular segments supplied by non-stenosed coronary artery: insights from speckle tracking analysis of dobutamine stress echocardiograms in patients with high coronary risk profile. Arch Med Sci. 2017;13(1):82–92. doi:10.5114/aoms.2016.60603
22. Lancellotti P, Cosyns B, Zacharakis D, et al. Importance of left ventricular longitudinal function and functional reserve in patients with degenerative mitral regurgitation: assessment by two-dimensional speckle tracking. J Am Soc Echocardiography. 2008;21(12):1331–1336. doi:10.1016/j.echo.2008.09.023
23. Cognet T, Vervueren PL, Dercle L, et al. New concept of myocardial longitudinal strain reserve assessed by a dipyridamole infusion using 2D-strain echocardiography: the impact of diabetes and age, and the prognostic value. Cardiovasc Diabetol. 2013;12:84. doi:10.1186/1475-2840-12-84
24. Yao GH, Deng Y, Liu Y, et al. Echocardiographic measurements in normal Chinese adults focusing on cardiac chambers and great arteries: a prospective, nationwide, and multicenter study. J Am Soc Echocardiography. 2015;28(5):570–579. doi:10.1016/j.echo.2015.01.022
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.