Back to Journals » Journal of Pain Research » Volume 18
Early Outcomes of Unilateral Biportal Endoscopic Decompression for Adjacent Segment Disease After Lumbar Fusion
Authors Pi W, Ye L, Gong B, Liu Y, Liu W, Chen H ![]() , Zhao H
, Zhao H
Received 9 August 2025
Accepted for publication 21 November 2025
Published 28 November 2025 Volume 2025:18 Pages 6371—6379
DOI https://doi.org/10.2147/JPR.S559657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Wensen Pi,1,2 Lei Ye,3 Boya Gong,1 Yang Liu,1 Wenjun Liu,1,2 Haidan Chen,1,2 Hongwei Zhao1,2
1Department of Spine Surgery of Yichang Central People’s Hospital, First Clinical Medical College of China Three Gorges University, Yichang, Hubei, 443000, People’s Republic of China; 2Hubei Provincial Clinical Research Center for Elderly Osteoporotic Fractures, Yichang, Hubei, 443000, People’s Republic of China; 3Department of Ophthalmology of Yichang Central People’s Hospital, First Clinical Medical College of China Three Gorges University, Yichang, Hubei, 443000, People’s Republic of China
Correspondence: Wenjun Liu, Department of Spine Surgery of Yichang Central People’s Hospital, First Clinical Medical College of China Three Gorges University, Yichang, Hubei, 443000, People’s Republic of China, Tel/Fax +86 07176488865, Email [email protected]
Purpose: To study the early curative effect of unilateral biportal endoscopy (UBE) in the treatment of adjacent segment disease after lumbar interbody fusion.
Methods: A retrospective analysis of clinical data from 58 patients diagnosed with adjacent segment disease subsequent to lumbar fusion surgery who were treated using the UBE technique between June 2019 and June 2024 at our institution was conducted. The patients’ operation time, intraoperative bleeding, postoperative hospitalization time, and the occurrence of complications were recorded. The visual analogue scale (VAS) for pain, the Japanese Orthopaedic Association (JOA) score, and the Oswestry Dysfunction Index (ODI) for lumbar function were utilised before and after surgery, and the MacNab criteria were employed to evaluate the patient’s outcome at six months after surgery.
Results: The operation time was between 55 and 189 minutes, mean 102.64 minutes, the postoperative drainage flow was between 10 and 110 mL mean 47.81 mL, and the length of hospital stay between 5 and 14 days, mean 9.41 days. VAS scores of pain decreased over time and the ODI index was consistently lower than preoperative at all stages of the postoperative period. JOA scores increased gradually at all postoperative times. All indexes differed statistically at all times (P< 0.05). Surgical efficacy was excellent in 93.1% of cases at 6 months.
Conclusion: The UBE technique is an alternative surgical procedure for the treatment of adjacent segment disease after lumbar fusion, under strict control of the indications.
Keywords: unilateral biportal endoscopic, adjacent segment disease, spine endoscopy, lumbar interbody fusion
Introduction
Lumbar fusion, a well-established procedure for the treatment of lumbar degenerative disease, has been shown to be effective in stabilising the diseased segment. However, the biomechanical changes in the adjacent segments that it causes have been demonstrated to significantly increase the risk of adjacent segment disease (ASD).1 ASD is a degenerative disease that occurs in the adjacent segments of the vertebral body. The condition is characterised by degeneration of the intervertebral discs of the adjacent segments, degeneration of the articular synovial joints, and vertebral instability and slippage. The condition frequently results in complications such as nerve compression, spinal cord injury, and vertebral fracture, manifesting in symptoms including low back pain, neuroradiation pain, and claudication.2 The literature reports that 65 out of 1258 patients (5.2%) who underwent TLIF for degenerative lumbar spine disease developed ASD and underwent surgery.3 Conventional open revision surgery necessitates the extensive stripping of soft tissues and re-fusion fixation, which is not only traumatic and accompanied by a protracted recovery period, but also has the potential to further exacerbate the degeneration of adjacent segments due to rigid fixation, resulting in a vicious cycle of “fusion-degeneration-re-fusion”.4–7 Consequently, the core challenge of ASD treatment is to achieve effective decompression and maintain spinal stability through minimally invasive techniques while preserving the original internal fixation.
Due to the scar tissue coverage and adhesion problems formed by the initial fusion surgery, the adjacent segment degenerative process of the vertebral plate and ligamentum flavum thickening, spinal canal stenosis, take open surgery will increase the risk of dural sac and nerve root injury. In recent years, UBE technology is becoming more mature, which has the advantages of less trauma, faster recovery, fewer complications, etc, and has achieved more satisfactory clinical results in clinical practice.8 However, there is a paucity of studies reporting on the use of UBE for the treatment of adjacent segment degeneration after lumbar fusion, and there is an absence of evidence for its early efficacy. We have used the UBE technique to treat patients with adjacent segmental degeneration after lumbar fusion and have obtained good early results. The relevant clinical data are reviewed and analyzed for reference. The report is as follows.
Methods
General Information
Inclusion criteria: ① previous lumbar fusion surgery, adjacent to a single segment degeneration [disc rupture/herniation at the adjacent level (including foraminal or extraforaminal), and/or adjacent segment stenosis (central, lateral recess, foraminal)]; ② symptoms and signs consistent with the imaging of the degenerated segment [symptomatic ASD (ASDis), rather than radiological degeneration (ASDeg)]; ③ strict conservative treatment for at least 3 months is ineffective; ④ postoperative follow-up for more than 6 months.
Exclusion criteria: ① multiple segmental degeneration with multiple nerve compression symptoms; ② lumbar spondylolisthesis, instability (>3 mm translation or >10° angular motion on flexion–extension radiographs), infection, tumor and other lesions. ③ Combination of serious medical diseases cannot tolerate general anesthesia and surgery.
A total of 58 patients admitted to Yichang Central People’s Hospital from June 2019 to June 2024 with adjacent segmental degeneration after lumbar fusion resulting in neurological symptoms in the lower limbs and treated with UBE surgery were retrospectively included in the study. The sample comprised 33 males and 25 females, with an age range from 51 to 85 years and a mean age of 67.76 ± 9.69 years. As illustrated in Table 1, all surgical procedures were carried out by a single surgeon, who utilised pre-defined surgical instruments.
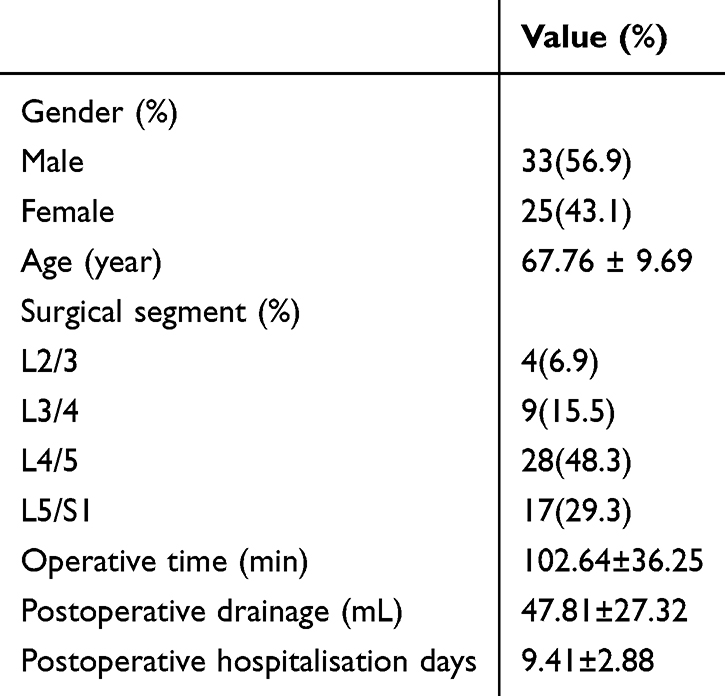 |
Table 1 Patient Basic Information |
Surgical methods
All surgical procedures were performed by the same surgeon. The patient was positioned prone under induced anaesthesia. The target vertebral segment was localised using a C-arm fluoroscopy. Skin markings included a transverse line at the edge of the inferior spinous process and the lamina, and a longitudinal line aligned with the medial border of the pedicle on the operative side. A longitudinal incision was centred over the intersection point and extended 1.0–1.5 cm cranially and caudally. Working and endoscopic trocars were then introduced. Fluoroscopic verification confirmed the alignment of the intersection of the visual and operative channels within the plane of the target intervertebral disc space. After connecting the endoscope, the microscopic bipolar radiofrequency probe, the powered instrumentation system and the saline irrigation interface, the plasma radiofrequency knife was deployed through the working channel. This instrument addressed the lamina, spinous process and overlying soft tissues adhering to the ligamentum flavum. This exposed the inferior margin of the superior lamina, the medial aspect of the inferior articular process and the superior margin of the inferior lamina. These osseous structures were then meticulously abraded using a high-speed drill and residual bone fragments were removed with laminectomy rongeurs until the cranial and caudal attachments of the ligamentum flavum were fully released. The ligament was then dissected free from dural adhesions using a nerve dissector. Removal of the ligamentum flavum then exposed the dural sac and the nerve root passing through it. If present, herniated nucleus pulposus material was excised following gentle nerve root retraction. Meticulous nerve root decompression was performed, followed by careful haemostasis. Finally, a drain was inserted and the incision closed in layers, with a sterile dressing applied.
Postoperative Management
Postoperative treatment involved the administration of methylcobalamin and B vitamins, as well as neurotrophic drugs. The drainage tube was removed, and straight leg raising training commenced on the second day after surgery. The patient was permitted to wear a waist cuff in order to facilitate mobilisation without manifesting obvious discomfort. Postoperative lumbar intervertebral disc CT and MRI scans were repeated. Patients were subjected to regular follow-up procedures in the post-operative period.
Observation Index
The following parameters were recorded: gender, age, body mass index, operative segment, operative time, postoperative drainage, postoperative hospitalization time, and the occurrence of complications. The visual analogue score (VAS) for pain, the Japanese Orthopaedic Association (JOA) score, and the Oswestry Dysfunction Index (ODI) were utilised to evaluate the degree of pain before surgery and at 3 days, 1 month, 3 month, and 6 months after surgery. The modified MacNab criteria were employed to evaluate the clinical outcomes at 6 months after surgery. The modified MacNab criteria categorised patients’ postoperative outcomes into four grades: excellent (complete disappearance of symptoms, return to work and life), good (mild symptoms, mild activity limitation, no impact on work and life), acceptable (symptomatic reduction, activity limitation, impact on normal work and life), and poor (no difference between pre- and post-treatment, or even worse).
Statistical Analysis
The IBM SPSS Statistics Ver. 26.0 (IBM Co., Armonk, NY, USA) was used for statistical analysis. Data are presented as mean ± standard deviation or frequency. The comparison of scores before and after surgery was analysed by repeated measures ANOVA. Count data is expressed in numbers or percentages, using x 2 test. A statistically significant difference was defined as p < 0.05.
Results
The present study encompasses a cohort of fifty-eight patients who underwent surgical intervention and met the inclusion criteria. It is worthy of note that all patients were subjected to the surgical plan that had been meticulously devised in accordance with the scheduled protocol. The surgical time exhibited a range from 55 to 189 minutes, with a mean of 102.64 minutes; the postoperative drainage volume ranged from 11 to 110 mL, with a mean of 47.81 mL; and the postoperative hospital stay ranged from 5 to 14 days, with a mean of 9.41 days. Patients were given a minimum of six-month follow-up after surgery. (Table 1).
The data demonstrated significant variations in VAS scores for low back pain in patients at the time points of 3 days, 1 month, 3 months, and 6 months postoperatively. The scores exhibited a marked decrease compared to the preoperative scores at all stages postoperatively, and the differences underwent a gradual improvement over time, which was statistically significant. A significant difference in the ODI index was observed at each postoperative time point. The index demonstrated a gradual reduction in dysfunction, with a significant decrease observed when comparing the index at all stages of the postoperative period to the preoperative index. However, there was no significant difference between the 1-month and 3-month results. The JOA scores demonstrated a marked increase at each postoperative time point, including three days, one month, three months and six months following surgery. Notably, these scores exhibited a higher magnitude at all stages of the postoperative period when compared to the preoperative period. This observation signifies a gradual recovery of neurological function, and the statistical significance of this finding underscores the reliability of the study’s outcomes. The VAS scores for the leg also demonstrated a significant decrease at each time point (3 days, 1 month, 3 months and 6 months postoperatively). Furthermore, the scores at all stages postoperatively were lower than the preoperative values, indicating that the pain relief effect was significant and continued to improve with the rehabilitation process. The difference was found to be statistically significant (Table 2).
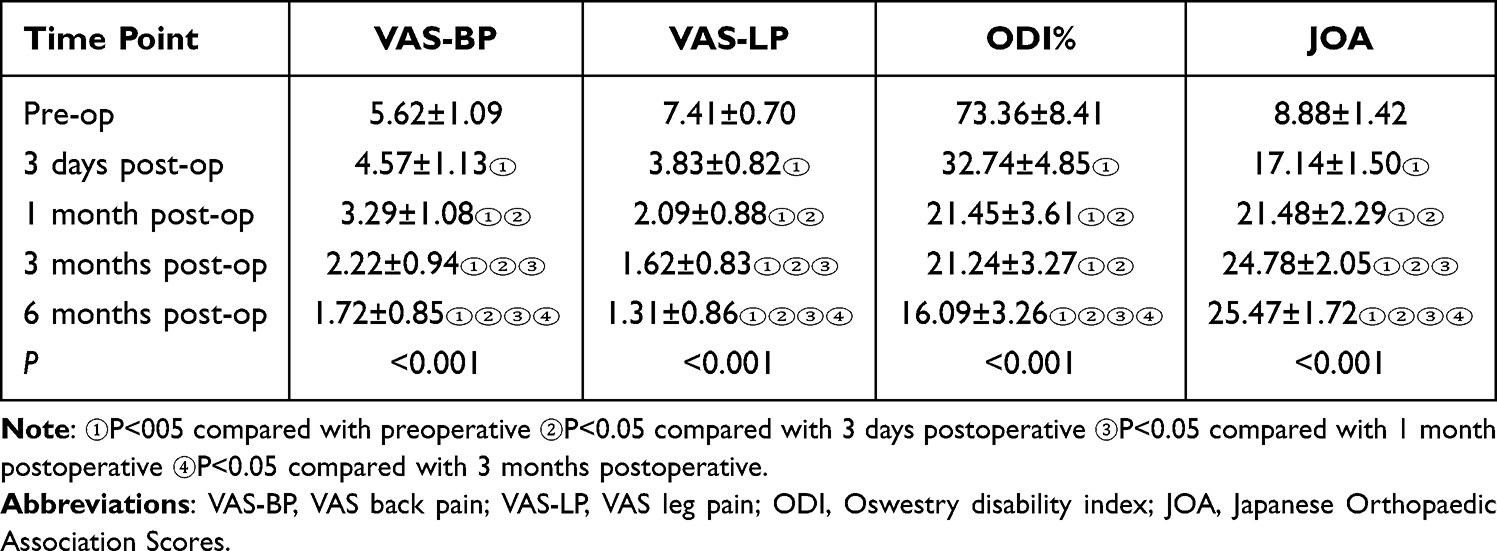 |
Table 2 Comparison of Patients’ Preoperative and Postoperative Back Pain and Leg VAS Scores, as Well as ODI Index and JOA at Each Time Point (Mean ± Standard Deviation) |
The surgical efficacy was evaluated in accordance with the MacNab criteria at the 6-month postoperative stage. The analysis revealed that 44 cases were classified as excellent, 10 cases were designated as good, and 4 cases were deemed to be feasible, thereby yielding an exceptional rate of 93.10%. (Table 3) Intraoperative spinal dural rupture and dural tear with herniation of the cauda equina occurred in three cases. These were converted to open surgery intraoperatively, and the dural sacs were repaired. All three patients achieved satisfactory clinical results. Typical cases are illustrated in Figures 1 and 2.
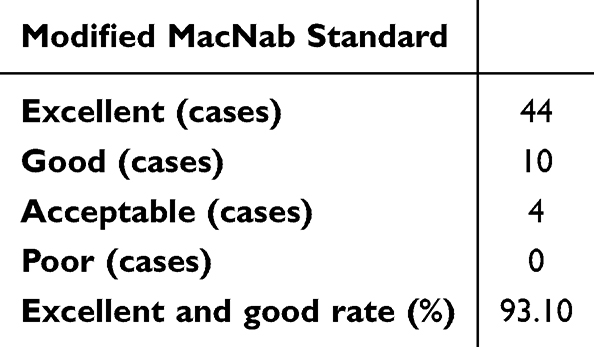 |
Table 3 The Surgical Efficacy Was Evaluated in Accordance with the MacNab Criteria at the 6-month Postoperative Stage |
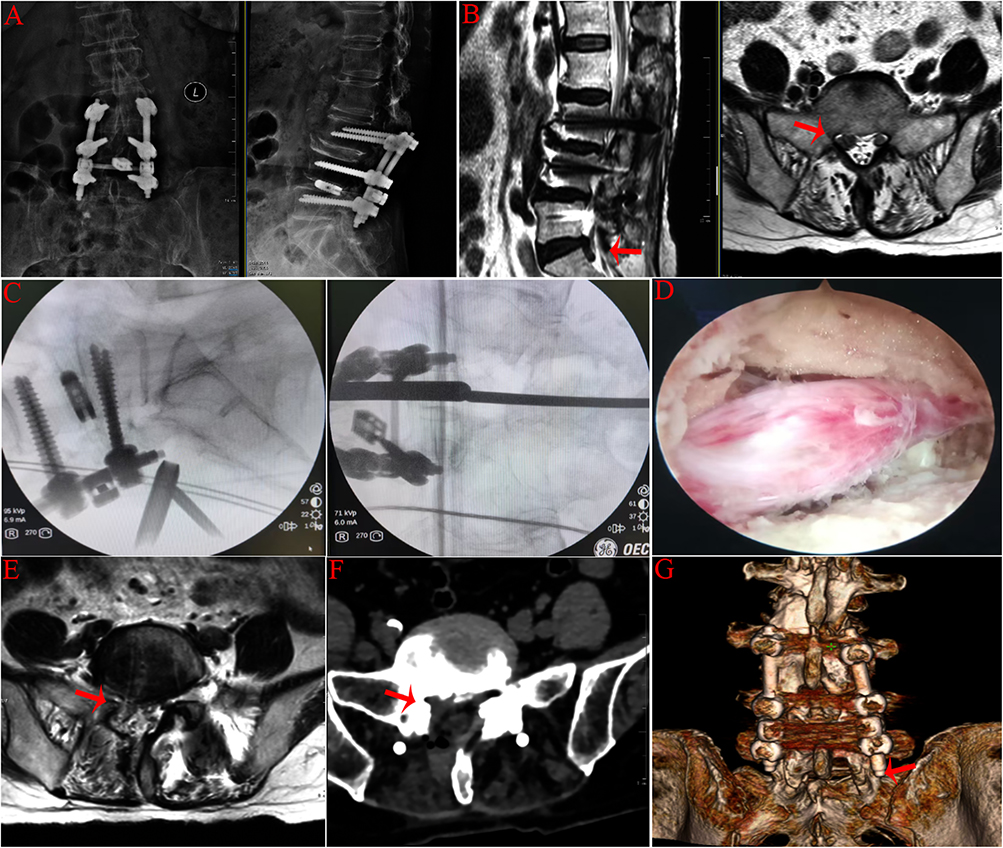 |
Figure 1 Typical case 1. A 72-year-old female patient underwent lumbar 3/4 and lumbar 4/5 fusion and fixation surgery for lumbar spine disease eight years ago. Over a period of six months, the patient exhibited symptoms of pain and numbness in her right lower limb. Following an unsuccessful course of conservative management, she underwent an additional UBE decompression surgery. (A) preoperative orthostatic/lateral DR; (B) preoperative MRI, suggesting L5/S1 right disc prolapse with nerve compression (red arrow: herniated disc); (C) Fluoroscopy of C-arm to determine the surgical segment after placement of the channel; (D) intraoperative picture after nerve decompression; Postoperative follow-up MRI (E) and CT (F) suggest adequate nerve root decompression (red arrows: the black signal intensity decreases); (G) Postoperative 3D CT suggests the extent of the laminar opening with excellent preservation of the zygapophyseal joint. (The red arrow indicates the location of the zygapophyseal joint). |
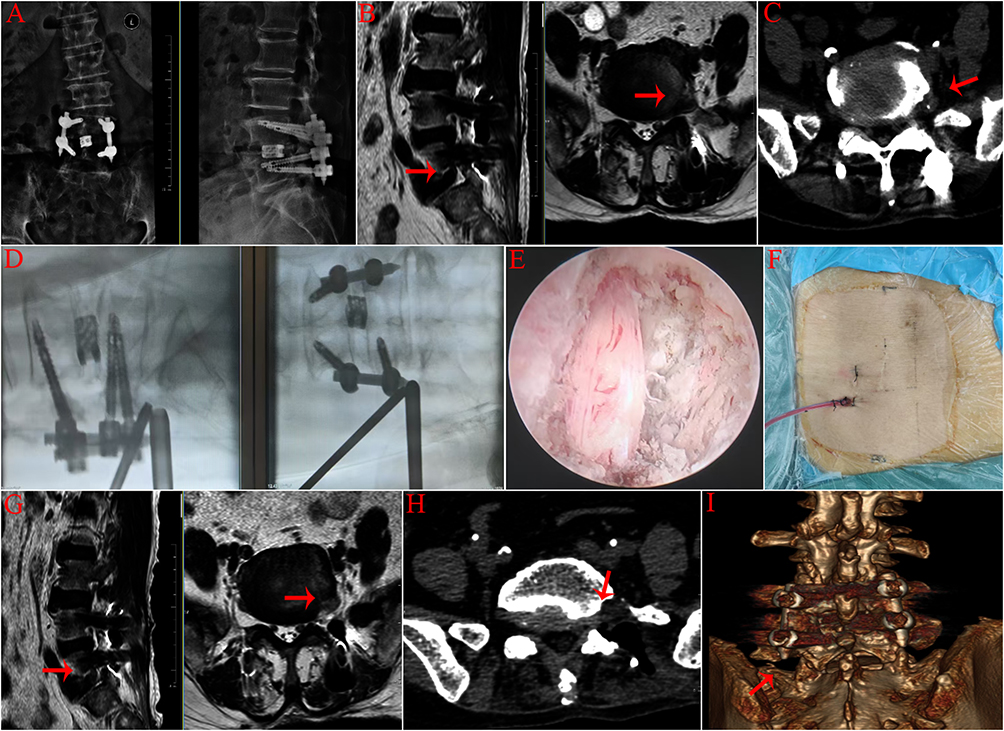 |
Figure 2 Typical case 2. A 69-year-old female patient, one year following lumbar fusion, exhibited a 8-month duration of pain and discomfort in the left lower extremity, which resulted in a limitation of walking activities. A preoperative examination indicated the presence of an L5/S1 left extreme lateral disc herniation, accompanied by nerve compression. This condition was addressed through surgical intervention, employing the UBE technique. (A) preoperative orthostatic/lateral DR; (B) Preoperative MRI indicates the presence of an L5/S1 left extreme lateral disc herniation, accompanied by nerve compression. (red arrow: herniated disc); (C) Preoperative CT suggests L5/S1 left extreme lateral disc herniation with nerve compression; (D) Fluoroscopy of C-arm to determine the surgical segment after placement of the channel; (E) intraoperative picture after nerve decompression; (F) Placing a drain in the surgical incision; Postoperative follow-up MRI (G) and CT (H) suggest adequate nerve root decompression (red arrows: the black signal intensity decreases); (I) Postoperative 3D CT showed good preservation of the zygapophyseal joint (The red arrow indicates the location of the zygapophyseal joint). |
Discussion
As the population ages and the incidence of degenerative spinal diseases increases, there is an increasing need for research in this field. Spinal fusion represents the most prevalent surgical intervention for the management of degenerative spinal diseases in clinical practice.9 Adjacent segment disease (ASD) is characterised by degenerative imaging of the cephalad and/or caudal portion of the fused segment, accompanied by the manifestation of corresponding clinical syndromes.1 The incidence of imaging adjacent segment degeneration (ASDeg) and symptomatic adjacent segment disease (ASDis) after lumbar fusion and reoperation rates have been reported in the literature to be 27.8%, 7.6%, and 4.6%, respectively.10 A retrospective study involving 568 patients found that the most significant surgical factor leading to ASD is decompression beyond the fusion level.11
Historically, the management of adjacent segment disease primarily involved open decompression procedures. In cases where this was accompanied by lumbar instability or slippage, the extension of the fusion segment was considered a relevant consideration. However, the initial surgery, due to the extensive exposure and substantial decompression, would result in anatomical structure destruction and scar proliferation and adhesion. Consequently, reopening the surgery would be a highly traumatic procedure, accompanied by significant bleeding, protracted recovery, and an increased risk of complications.12 This approach represented a substantial challenge not only for the surgeon but also for the patient. The development of spinal surgery has been characterised by a gradual shift towards minimally invasive treatments, as conventional surgical methods have increasingly come under scrutiny from patients.
A number of studies have reported the utilisation of single-channel endoscopy for the treatment of ASD,13–16 yielding satisfactory outcomes. However, the limited operating space and angle of single-channel endoscopy may result in insufficient decompression, especially in patients with combined spinal stenosis. In such cases, the intervertebral foramenoscope is unable to enlarge the spinal canal for decompression, which limits the use of this procedure.17,18 In the study by Wei Zhang et al,19 three patients diagnosed with ASD following lumbar spine surgery were treated with the UBE technique, yielding favourable outcomes. Similarly, the report by Shreenidhi Kulkarni et al20 details a case of a 72-year-old female patient with ASD who underwent surgery 12 years prior and was treated with the UBE technique, also resulting in positive outcomes. A further study reported a high rate of joint preservation and a low incidence of reoperation in the treatment of ASD with the UBE technique. These findings serve to highlight this technique as a compelling alternative treatment for ASD.21 A recent retrospective study also reported satisfactory short-term results in 18 patients with ASD after lumbar spine surgery treated with the UBE technique.22
The UBE technique, with its dual-channel design, facilitates the operator’s ability to achieve a clear and expansive surgical field, thereby enabling precise localisation of the diseased tissue and complete decompression of the compressed nerve. The C-arm fluoroscopy is utilised for the purpose of identifying the responsible segment prior to surgery, and the puncture handle is employed to directly penetrate the scar tissue and enter the bony structure of the vertebral plate. This approach serves to prevent substantial bleeding during the open surgical exposure process and the collateral injuries that are often caused by a lack of anatomical clarity. The dual-channel design facilitates the simultaneous execution of dynamic irrigation and fine manipulation, thereby significantly reducing intraoperative field of vision blockage. The UBE procedure achieves bilateral decompression through a unilateral approach, preserving the spinous process, interspinous ligament, and posterolateral structures of the articular eminence to the greatest extent possible, thereby reducing the risk of spinal instability of medical origin. It is imperative to note that, during the operation, only the ventral aspect of the contralateral vertebral plate and part of the medial aspect of the articular process require abrading. This is to be done in such a manner as to avoid extensive resection of bony structures. This approach is to be adopted in order to maintain the biomechanical integrity of the spine.23–26 In comparison with single-channel endoscopy, UBE has been shown to be more efficient in the management of bilateral bony hyperplasia and hypertrophy of the ligamentum flavum, particularly in cases of combined central canal stenosis or complex lateral saphenous stenosis.27,28
The postoperative lumbar/lower extremity VAS scores, postoperative ODI scores, and lumbar JOA scores of the patients in this study demonstrated significant improvement in comparison with the preoperative scores. The excellent therapeutic outcome rate was 93.10%, which provides substantial evidence for the feasibility of the UBE procedure in the treatment of adjacent segment disease. No patients required reoperation during the follow-up period, though this may be limited by the short follow-up duration (6 months). In cases of intravertebral stenosis accompanied by thickened adhesions of the ligamentum flavum, the surgical intervention may result in the occurrence of a dural tear, with the likelihood of such an event being higher than that of the initial operation. Dural tears accompanied by herniation of the cauda equina occurred in three cases. The operating team swiftly transitioned to an open surgical approach, undertaking dural sac repair. Not all patients with dural tears require conversion to open surgery. We only consider converting to open surgery when the dural defect is large, the cauda equina nerve herniation is severe, and neural decompression has not yet been completed. The UBE technique is characterised by the presence of a single operating channel, a factor that can complicate the intraoperative microscopic suturing of the dura. Furthermore, large dural tears frequently entail difficulties in nerve retraction, which may culminate in irreversible nerve injury if left untreated. ASD revision surgery is associated with heavy intraoperative tissue adhesions and is prone to large dural tears. We therefore recommend immediate conversion to open surgery.
The limitations of this study are as follows: firstly, there is an absence of long-term follow-up results that could illustrate the long-term clinical efficacy and recurrence rate of the UBE technique for the treatment of adjacent segment disease after lumbar spinal fusion. Secondly, it is a retrospective study with low quality of evidence, and there is a possibility of selection bias due to the small number of ASD cases included. Thirdly, the study did not encompass adjacent spondylolisthesis. Further studies are necessary to better understand the efficacy of UBE surgery in symptomatic ASD patients.
Conclusion
In conclusion, a retrospective analysis was conducted to summarise the neurological decompression effect of the UBE technique in the treatment of ASD following lumbar spinal fusion. The UBE technique is an alternative surgical procedure for the treatment of adjacent segment disease after lumbar fusion, under strict control of the indications. However, it should be noted that there is a risk of dural tear during the operation, and that larger dural tears with herniation of the cauda equina may require conversion to open surgery.
Data Sharing Statement
The data used and analyzed during the current study are available from the corresponding author (Wenjun Liu) on reasonable request. All data files mentioned in this manuscript are available.
Human Ethics and Consent to Participate Declarations
This retrospective study was reviewed by the ethics committee of Yichang Central People’s Hospital following the Declaration of Helsinki.
Consent for Publication
Informed consent was taken from all patients for their participation in the study. All published medical histories and photographs have been signed with informed consent from patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. McDonald CL, Alsoof D, Glueck J, et al. Adjacent segment disease after spinal fusion. JBJS Rev. 2023;11(6). doi:10.2106/JBJS.RVW.23.00028.
2. Virk SS, Niedermeier S, Yu E, et al. Adjacent segment disease. Orthopedics. 2014;37(8):547–555. doi:10.3928/01477447-20140728-08
3. Ye J, Yang S, Wei Z, et al. Incidence and risk factors for adjacent segment disease after transforaminal lumbar interbody fusion in patients with lumbar degenerative diseases. Int J Gen Med. 2021;14:8185–8192. doi:10.2147/IJGM.S337298
4. Rubio-Haro R, de Andrés-Serrano C, Noriega González DC, et al. Adjacent segment syndrome after failed back surgery: biomechanics, diagnosis, and treatment. Minerva Anestesiol. 2022;88(4):282–292. doi:10.23736/S0375-9393.21.15939-5
5. Miwa T, Sakaura H, Yamashita T, et al. Surgical outcomes of additional posterior lumbar interbody fusion for adjacent segment disease after single-level posterior lumbar interbody fusion. Eur Spine J. 2013;22(12):2864–2868. doi:10.1007/s00586-013-2863-9
6. Kanno H, Aizawa T, Hahimoto K, et al. Minimally invasive discectomy for lumbar disc herniation: current concepts, surgical techniques, and outcomes. Int Orthop. 2019;43(4):917–922. doi:10.1007/s00264-018-4256-5
7. Chang F, Zhang T, Gao G, et al. Comparison of the minimally invasive and conventional open surgery approach in the treatment of lumbar stenosis: a systematic review and a meta-analysis. Ann Acad Med Singap. 2017;46(4):124–137. doi:10.47102/annals-acadmedsg.V46N4p124
8. Feng Z, Zhao Z, Cui W, et al. Unilateral biportal endoscopic discectomy versus microdiscectomy for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2024;33(6):2139–2153. doi:10.1007/s00586-023-08116-2
9. Keum BR, Kim HJ, Kim G-H, et al. Osteobiologies for spinal fusion from biological mechanisms to clinical applications: a narrative review. Int J Mol Sci. 2023;24(24):17365. doi:10.3390/ijms242417365
10. Donnally CR, Patel PD, Canseco JA, et al. Current incidence of adjacent segment pathology following lumbar fusion versus motion-preserving procedures: a systematic review and meta-analysis of recent projections. Spine J. 2020;20(10):1554–1565. doi:10.1016/j.spinee.2020.05.100
11. Maragkos GA, Motiei-Langroudi R, Filippidis AS, et al. Factors predictive of adjacent segment disease after lumbar spinal fusion. World Neurosurg. 2020;133:e690–e694. doi:10.1016/j.wneu.2019.09.112
12. Lambrechts MJ, Toci GR, Siegel N, et al. Revision lumbar fusions have higher rates of reoperation and result in worse clinical outcomes compared to primary lumbar fusions. Spine J. 2023;23(1):105–115. doi:10.1016/j.spinee.2022.08.018
13. Li T, Zhang B. Early application of bilateral decompression under single channel endoscopic laminectomy in patients with adjacent vertebrae after lumbar fusion. Zhongguo Gu Shang. 2024;37(12):1153–1157. doi:10.12200/j.issn.1003-0034.20240245
14. Han J, Wei Tang MD, Guanghui Li, et al. Comparison of percutaneous endoscopic transforaminal and interlaminar approaches in treating adjacent segment disease following lumbar decompression surgery: a clinical retrospective study. Pain Physician. 2023;26(7):E833–E842. doi:10.36076/ppj.2023.26.E833
15. Feng P, Kong Q, Zhang B, et al. Percutaneous full endoscopic lumbar discectomy for symptomatic adjacent segment disease after lumbar fusion in elderly patients. Orthop Surg. 2023;15(7):1749–1755. doi:10.1111/os.13725
16. Shan X, An J, Li L, et al. An innovative minimally invasive technique for lumbar adjacent segment disease: a retrospective comparative analysis between extreme-oblique lumbar interbody fusion combined with percutaneous endoscopic lumbar discectomy (XOLIF-PELD) and posterior lumbar interbody fusion (PLIF) revision. J Orthop Surg Res. 2025;20(1):609. doi:10.1186/s13018-025-06011-8
17. Fan N, Yuan S, Du P, et al. Complications and risk factors of percutaneous endoscopic transforaminal discectomy in the treatment of lumbar spinal stenosis. BMC Musculoskelet Disord. 2021;22(1):1041. doi:10.1186/s12891-021-04940-z
18. Li L, Hai Y, Yang J, et al. Correlation between preoperative CT imaging parameters and clinical outcome of lumbar spinal stenosis treated with endoscopic transforaminal decompression. J Int Med Res. 2020;48(4):300060519894078. doi:10.1177/0300060519894078
19. Zhu C, Zhang Y, Sun S, et al. A case report: unilateral biportal endoscopic revision for adjacent segmental disease: case presentations and literature review. Medicine. 2023;102(40):e35466. doi:10.1097/MD.0000000000035466
20. Sakhrekar R, Ha JS, Don H, et al. Unilateral biportal endoscopic approach for symptomatic adjacent segment disease: case report and technical note. J Orthop Case Rep. 2023;13(12):172–177. doi:10.13107/jocr.2023.v13.i12.4122
21. Lee DH, Park CK, Jang J-W, et al. Safety and utility of bilateral-contralateral decompression for adjacent segment stenosis after lumbar interbody fusion using unilateral biportal endoscopy. Clin Spine Surg. 2025. doi:10.1097/BSD.0000000000001777
22. Feng F, Li G, Meng H, et al. Clinical efficacy of unilateral biportal endoscopic technique for adjacent segment pathology following lumbar fusion. J Orthop Surg Res. 2025;20(1):628. doi:10.1186/s13018-025-06034-1
23. Park DK, Weng C, Zakko P, et al. Unilateral biportal endoscopy for lumbar spinal stenosis and lumbar disc herniation. JBJS Essent Surg Tech. 2023;13(2). doi:10.2106/JBJS.ST.22.00020.
24. Sellier A, Lechanoine F, Lonjon G, et al. How to begin unilateral biportal endoscopy (UBE) for segmental lumbar degenerative disease: a step-by-step guide to perfect patient positioning and surgical approach, avoiding common pitfalls. Neurosurg Rev. 2024;47(1):593. doi:10.1007/s10143-024-02674-9
25. Zhang Y, Tian L, Hu P, et al. Research progress of unilateral biportal endoscopy technique in treatment of lumbar related diseases. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022;36(10):1234–1240. doi:10.7507/1002-1892.202205087
26. Li K, Zhang Z, Ran J, et al. Unilateral endoscopic and unilateral biportal endoscopic surgery for lumbar spinal stenosis: a systematic review and meta-analysis. Front Surg. 2025;12:1585783. doi:10.3389/fsurg.2025.1585783
27. Yuan C, Wen B, Lin H. Clinical analysis of minimally invasive percutaneous treatment of severe lumbar disc herniation with UBE two-channel endoscopy and foraminal single-channel endoscopy technique. Oxid Med Cell Longev. 2022;2022:9264852. doi:10.1155/2022/9264852
28. He BL, Zhu Z-C, Lin L-Q, et al. Comparison of biportal endoscopic technique and uniportal endoscopic technique in unilateral laminectomy for bilateral decompression (ULBD) for lumbar spinal stenosis. Asian J Surg. 2024;47(1):112–117. doi:10.1016/j.asjsur.2023.05.068
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.