Back to Journals » Journal of Pain Research » Volume 18
Early Musculoskeletal Pain Management in the General Practitioner’s Office & E-Referral: A Multidisciplinary Expert Opinion
Authors Gervasoni F ![]() , Farì G, Franco M, Liguori S
, Farì G, Franco M, Liguori S ![]() , Maschietto L, Michieli R, Raimondo E, Scaturro D, Ventriglia G, Magni A
, Maschietto L, Michieli R, Raimondo E, Scaturro D, Ventriglia G, Magni A
Received 3 January 2025
Accepted for publication 11 July 2025
Published 12 August 2025 Volume 2025:18 Pages 3879—3889
DOI https://doi.org/10.2147/JPR.S515501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Fabrizio Gervasoni,1– 3 Giacomo Farì,4 Massimiliano Franco,5 Sara Liguori,6,7 Luca Maschietto,8 Raffaella Michieli,5 Emanuela Raimondo,9 Dalila Scaturro,10 Giuseppe Ventriglia,5 Alberto Magni5
1ASST Fatebenefratelli Sacco, Milan, Italy; 2Home Health Care, ASST Fatebenefratelli Sacco, Milan, Italy; 3Industrial Engineering PhD Program, Industrial Engineering Technologies for Sports Medicine and Rehabilitation, University of Rome Tor Vergata, Rome, Italy; 4Department of Experimental Medicine (Di.Me.S.), University of Salento, Lecce, Italy; 5SIMG (Italian College of General Practitioners and Primary Care), Florence, Italy; 6Department of Medical and Surgical Specialties and Dentistry, University of Campania “Luigi Vanvitelli”, Naples, Italy; 7Department of Mental and Physical Health and Preventive Medicine, University of Campania “Luigi Vanvitelli”, Naples, Italy; 8ASUGI, Trieste, Italy; 9Orthopedics Unit, Casa di Cura San Pio X Humanitas, Milan, Italy; 10Department of Surgical, Oncological and Stomatological Disciplines, University of Palermo, Palermo, Italy
Correspondence: Fabrizio Gervasoni, ASST Fatebenefratelli Sacco, District Municipality 2, Viale Don Orione, 2, Milan, 20132, Italy, Email [email protected]
Purpose: Musculoskeletal pain (MP) is a significant burden in primary care, often presenting challenges for general practitioners (GPs) in providing timely and effective management. Despite MP’s prevalence, GPs face limitations in diagnostic resources and access to specialists, which can delay intervention and increase the risk of pain chronicity. This multidisciplinary expert opinion aims to establish a structured approach for the management of MP within general practice, using three targeted algorithms: (1) early management of acute MP in the GP’s office, (2) post-surgical MP management to support recovery, and (3) MP management following emergency discharge.
Patients and Methods: A panel of GPs, physiatrists, and orthopedists collaborated to develop practical recommendations based on current clinical guidelines, emphasizing early diagnosis, initial pain control, and effective e-referral pathways. During an onsite meeting, they created an algorithm to identify waiting therapy for patients with pain, in order to help GPs in this difficult task.
Results: The first algorithm focuses on early intervention for acute MP in primary care, with recommendations for both pharmacological and non-pharmacological approaches. The second algorithm addresses post-surgical MP management to enhance recovery and reduce complications. The third algorithm outlines post-emergency management strategies, emphasizing immediate pain relief and integrating patient education to support home management. E-referral and teleconsultation are incorporated throughout to enhance care coordination.
Conclusion: These three algorithms provide a structured framework for MP management in primary care, placing GPs at the centre of early intervention. The inclusion of telemedicine and e-referral pathways allows for timely specialist input, ultimately aiming to improve patient outcomes and minimize chronic pain risks.
Keywords: musculoskeletal pain, early pain management, general practice, e-referral, telemedicine, multidisciplinary approach
Introduction and Rationale
Musculoskeletal pain (MP) represents a burdensome issue affecting more than 30% of the global population,1 as one of the main contributors to disability worldwide. MP can be classified into acute or chronic (depending on the pathophysiological activation of pain pathways) or also as focal (localized to a specific area) or diffuse (affecting multiple areas).
In its pathogenesis, MP include disorders affecting several structures such as bones, muscles, ligaments, tendons, and/or related soft tissues. Indeed, MP can occur in the absence of other pathological conditions, known as primary pain, including non-specific low back pain (LBP), or it may be attributable to a specific disease, known as secondary MP, associated with inflammation and/or structural changes due to infection, crystal deposition, or auto-inflammatory pathways.2
Since this paper focuses specifically on musculoskeletal pain, neuropathic pain has not been addressed in the discussion. The latter would require the involvement of neurophysiologists and neurologists, given its distinct pathophysiological mechanisms. Evidence-based therapeutic algorithms for neuropathic pain have already been published in the literature and may serve as reference frameworks in cases involving documented lesions or dysfunctions of sensory neural pathways, as identified through diagnostic tools and validated scales (eg, PainDetect, Douleur Neuropathique en 4 Questions – DN4 –, and the Leeds Assessment of Neuropathic Symptoms – LANSS).3 Consequently, patients with confirmed neuropathic pain were excluded from the analysis, which exclusively addresses pain syndromes within the scope of musculoskeletal disorders.
Despite the high social burden related to MP, it remains an underestimated problem; being such a multifaceted symptom or clinical presentation, clinicians from very different backgrounds face MP in its various forms; therefore, it is not surprising that no consensus about its management has been reached so far.4
The fundamental premise—shared by both General Practitioners and specialists, and endorsed by current clinical practice guidelines as well as national regulations—is the need to quantify musculoskeletal pain using standardized measurement scales that are quick and easy to administer in outpatient settings. The most widely known and commonly used due to their simplicity and rapid application are the Faces Pain Scale-Revised (FPS-R), Verbal Rating Scale (VRS), Numerical Pain Rating Scale (NPRS), and Visual Analogue Scale (VAS).5
These instruments, however, are limited to the quantification of pain intensity and do not provide information on the onset timing (or potential chronification) of the pain, nor on its underlying pathophysiological mechanisms—information that could be better captured by tools such as the DN4 or LANSS, which are specifically designed to identify neuropathic pain.
Italian prevalence of chronic pain referral to general practitioners (GPs) is about one third.6–8 Osteoarthritis (OA) is the most prevalent problem in doctors’ electronic records (18% of patients), while LBP is the second reason for sick leave. Therefore, these conditions have a significant impact not only on the functioning and quality of life of patients, but also on direct and indirect healthcare costs. Despite possessing extensive information about their patients’ clinical history and lifestyle, GPs often struggle to manage these issues effectively. Moreover, patients usually tend to trivialize their condition, preferring to start self-treatment therapies without consulting a doctor. Therefore, effectively managing MP in a GP setting is challenging, given the heterogeneity of underlying conditions and the limitation in healthcare resources, which can restrict access to time-consuming examinations and specialist consultations.
Furthermore, there is a lack of standardized approach to patients with MP. Consequently, the Italian Society of GPs (Società Italiana di Medicina Generale, SIMG) has developed consensus documents to manage and treat the majority of medical conditions causing MP.9,10 Indeed, an early treatment of pain is strongly advised as well appropriated, consistent with the type of pain, to prevent chronification and improve the patient’s psycho-behavioral and cognitive aspects, guaranteeing adequate analgesic coverage also during the rehabilitation process.
In this complex scenario, telemedicine and teleconsultation with a specialist e-referral seems an intriguing option,11 but how and when to use digital tools to facilitate interaction between GPs and specialists is still a matter of debate. Developing a stepwise approach for the diagnostic and therapeutic management of MP, which includes telemedicine for remote consultations, is an important unmet need. This approach should address the appropriate timing for specialist consultations, and clarify when a patient should be referred to a specialist versus when to manage their care with through a shared pathway.
Finally, it is crucial to focus on educating both patients and GPs. This includes training patients in effective pain management and prevention starting from childhood, as well as enhancing doctors’ understanding of managing chronic pain conditions.
This paper presents the findings of a multidisciplinary expert panel consisting of physiatrists, orthopedists, and GPs, which meets onsite to discuss the following topics. The primary goals can be resumed as follows:
- to promote the early management of patients experiencing acute MP, specifically regarding the most common issues encountered in primary care settings;
- to ensure continuity of pain management for patients following hospital discharge, thereby strengthening the integration of hospital and outpatient care;
- to develop a diagnostic and therapeutic algorithm for the early management of MP related to prevalent secondary pain conditions, such as nonspecific LBP and OA pain affecting the knee, hip, hand, and shoulder;
- to establish a standardized patient management process for individuals being discharged from the hospital, which may include those in emergency situations or following surgical procedures;
- to ultimately advocate for the development of protocols focused on the early management of MP.
Unmet Needs in the Patient Journey for MP
MP represents one of the most common reason for visiting general practice (being OA and LBP the first two recorded reasons), although there are several issues faced by GPs. The wideness of the topic and the complexity of diagnostic pathways frequently translate into the lack of tempestive efficacious treatment for MP in the GP setting. In addition, in Western healthcare systems it is still difficult to referring such patients to other specialists in terms of timing.
Patients often present not only because of the intensity of the pain, but also because of the impact on their quality of life and social participation, such as the inability to work or manage family responsibilities. In addition to identifying the type of pain, it is crucial to distinguish the course of the pain, especially when it changes from acute to chronic. This can manifest itself as a latent chronicity or a fluctuation that fuels the fear of new attacks, negatively influencing social participation, work and family habits, as well as the patient’s expectations. Fear of movement (kinesiophobia) and the resulting psychological limitations represent a key element in the vicious cycle of chronic pain.12
Consequently, from the GP perspective several unmet needs still exist in the management of MP. Firstly, making a tempestive diagnosis is crucial since early intervention is generally essential, and diagnostic processes must not delay treatment. Then, understand the nature of the disease is pivotal to the following clinical pathway. Indeed, a critical aspect is understanding the underlying reasons for the patient’s pain, which may not always correspond to its maximum intensity but rather to its debilitating impact on the patient’s daily life. Thirdly, considering the gender and age differences is one of reasons for complexity: women often exhibit greater sensitivity to symptoms and possess a more nuanced ability to articulate their pain experiences, influenced by factors such as pregnancy and other life situations.13 Indeed, a personalized approach that recognizes these differences can significantly improve pain management and treatment outcomes.
The implementation of an algorithm for the early management of musculoskeletal pain by General Practitioners offers several clinical and organizational advantages that extend beyond the algorithm’s structure alone. Specifically, it facilitates timely and appropriate specialist referral and intervention, thereby improving the overall timing of care and potentially preventing the chronification of pain. Early or inappropriate access to diagnostic imaging (eg, X-rays, MRI) may delay the initiation of effective analgesic therapy. Moreover, incidental findings that are common in asymptomatic adults—such as intervertebral disc protrusions—may be identified but lack clinical relevance to the patient’s current symptomatology. Such findings, when not clinically indicated, can lead to patient overemphasis on structural deficits or degenerative changes, thereby undermining efforts to empower the patient toward necessary behavioral and lifestyle modifications, which are often key contributors to musculoskeletal pain. Therefore, the use of the algorithm promotes diagnostic and therapeutic appropriateness, ensures timely initiation of the treatment pathway, and supports the selection of the most suitable healthcare professional to manage the patient’s care effectively.
The Specialists Contribute on the Management of MP Conditions
Specialists’ approach to MP has a different point of view, as the priority is identification of the nature of the problem, to set up a correct therapy and to prevent long life consequences of MP.
Firstly, specialists suggest starting from education and prevention, to fully exploit the potential of current technologies and pain treatment methods. Prevention is key, but is currently overlooked. It is important to educate the patient from a pediatric age to prevent future musculoskeletal pathologies. For instance, a good postural education and regular physical activity is deemed to prevent LBP. Promoting good postural and movement practices by the GPs can significantly reduce the incidence of these pathologies. On the other hand, self-management for chronic diseases such as OA is pivotal and should be encouraged by GPs. Educating patients on aspects such as weight loss, exercise and self-management of symptoms may be a key element to review and implement in follow-up.10
The specialists’ goal is the rapid and correct treatment of MP. Improving knowledge at all levels to quickly arrive at a correct diagnosis is necessary, as patients can bypass their GP and turn directly to non-medical specialists, further complicating the patient journey. Indeed, the multidisciplinary approach is fundamental in the management of MP. At this regard, the physiatrist should be a point of reference in the management of MP, working closely with GPs and orthopedists.
To support the GP in parallel with his evaluation, which must contain first level tests and scales for an appropriate diagnosis, teleconsultation tools can be useful. The objective of teleconsultation for GPs should be to rely on the specialist in case of doubts about diagnoses and requests for further information. Furthermore, it is necessary to set clear objectives for contact with the specialist, determining what is expected from this collaboration. The collaboration between different professional figures and the use of shared protocols represent a stimulating and innovative method to improve care for patients with pain, both acute and chronic. It is essential to consider what we expect from any intervention or test offered to the patient, as these can change the therapeutic path. The shared idea is that pain should no longer be treated only based on its intensity. The old WHO three-step ladder is outdated, and a bio-psycho-social approach must be adopted to correctly set the therapy. Thorough proper shared diagnostic intervention, including imaging and specialist consultations, it is possible to control pain while waiting for a complete diagnostic assessment. This approach allows to effectively treat pain while furthering diagnosis. Furthermore, the use of digital is crucial. Sharing a complete medical history via the electronic health record can improve patient management. If the primary care physician detects critical data during semeiological maneuvers specific to the pathology underlying the pain and the type of pain, this can be shared with specialists, who can then decide the timing and appropriateness of treatment. This collaboration and data sharing can optimize pain diagnosis and treatment.
Similarly, all these considerations can be applied also in the preparatory approach to conditions favoring MP. Prehabilitation or pre-operative preparation is a controversial field in which GPs should have a greater role. Prehabilitation is considered crucial, as it helps manage pain and prepare the patient for possible surgical interventions, improving joint and muscle condition and reducing post-operative rehabilitation times. The need for effective pharmacological management, possibly supported by digital platforms and therapeutic exercise, is highlighted. The problem of some inadequate approaches is also highlighted, such as the failure to prescribe painkillers, which can worsen the patient’s situation.
Teleconsult and e-Referral
Disrupting this pattern is crucial, and in this context digital platforms and digital health can play an important role. These tools can guide the patient towards greater autonomy and awareness, providing information on what to do and what to avoid. Digital platforms can also facilitate monitoring and follow-up, reducing the need for frequent doctor visits and providing a seamless point of contact between the patient, GP and specialists. Furthermore, they can offer support in accessing non-pharmacological and interventional therapies, improving overall pain management.
The decision regarding the initial therapeutic approach and the timing of referrals can be enhanced through teleconsultation, which allows for timely and precise evaluations, thereby prioritizing data movement over patient relocation.14 However, there is currently no standardized pathway for subsequent care following diagnostic evaluations, encompassing both pharmacological and non-pharmacological management.
In this complex scenario, it is important to highlight the concerns surrounding current medical education, which often neglects the essential training needed to effectively address intricate conditions. At the same time, we must acknowledge the invaluable contributions of specialists in managing these complex health issues. Collaboration between GPs and specialists is essential, particularly in cases where patient progress is unsatisfactory or in understanding pain causes.
Interestingly, physical referrals to specialists are not always necessary; their expertise can also be leveraged through digital tools, promoting efficient, mediated contact. However, while technology presents new opportunities for patient interaction, the physical presence and direct care offered by a practitioner remain indispensable.
Ultimately, the concept of continuous patient care is fundamental. It is not only crucial to alleviate pain but also to monitor the patient over time to ensure sustainable improvement. This approach necessitates effective coordination among all specialists involved in the patient’s treatment, under the GP’s guidance.
To avoid its inappropriate use, GPs and specialists should keep in mind that teleconsultation can have different purposes and roles,15 which can be resumed as:
- Possible rapid evaluation for emergent referral to hospitals;
- Definition of timing and appropriateness of the clinical path (eg, physiotherapy);
- Tele-cooperation in the diagnostic path;
- Sharing of the therapeutic path;
- Request for instrumental exams and their interpretation or rapid sharing;
- Educational issues and shared research.
Although being out of the aim of this paper, it is to acknowledge that teleconsultation, and more in general telemedicine, has precise medico-legal issues to be kept in mind when the service is organized and forwarded. In addition, telemedicine should be cost-efficacious, as it can shorten diagnostic and therapeutic delays, foster GP-specialist cooperation and save time both for patients and for doctors.15
Early Management of Acute Pain Due to Musculoskeletal Conditions (LBP and OA)
Specialists have developed a framework for the patient’s pain through codified steps that culminate in an adequate therapy.10 The goal of this paper is to create an algorithm to identify waiting therapy for patients with pain, in order to help GPs in this difficult task. It is essential to decide who takes care of the patient, as current systems are overloaded and lack appropriateness criteria. A teleconsultation can act as a first educational filter to better manage patients. Confusion over who should do what leads to inefficiencies in the healthcare system. The implementation of guidance pathways for patients with acute diseases, such as LBP, requires the identification and adoption of effective and safe pharmacological therapies. Most practitioners follow therapies coded for safety and duration of therapy, but there is a lack of training in chronic pain management.
The algorithm suggested by experts regarding the early management of acute or acute-on-chronic MP is resumed in Figure 1.
 |
Figure 1 Algorithm on the early management of acute or acute-on-chronic MP. |
As first step, the GP must carry out an anamnestic evaluation (pain at night or at rest, specific irradiation, trauma, non-response to first-line drug therapy, indicators of the likelihood of becoming chronic, including contextual factors, patient’s history, age, working, and social conditions), also by means of phone or web contact. If red flags are identified (eg, trauma, infection, neurologic disease), e-referral or in-person referral are necessary. On the contrary, while awaiting the appointment, the patient should be advised with behavioral indications and can start pain killers. Paracetamol is firstly indicated as a safe and versatile choice, also possibly in association with other drugs (NSAIDs or steroids) depending on the type of pain, the patient’s response and comorbidities.10,16–19 Therapeutic exercise, physical therapies (such as heat therapy) and postural education are also an integral part of the treatment.20 The doctor should provide practical advice to the patient on how to manage pain at home. It is important to educate patients on the importance of movement and appropriate drug treatment.
The goal of the first GP visit is trying to define the type of pain and to reach a diagnosis. A detailed clinical exam (dynamic examination of the back and segmental examination of the lumbar area; palpation spinal curvatures; irritation maneuvers such as Lasègue or Wasserman, looking at the buttocks and feet). Evaluation of the type of pain, and a neurological examination to assess sensory function can provide important clues to the type of pain.9 In addition, also multidimensional evaluation scale using validated scores (ie, ODI for LBP, WOMAC for OA) can help quantifying the associated disability. It is essential to overcome the treatment of pain based only on intensity and adopt an etiopathogenetic approach to correctly set the therapy. Again, if red flags are identified, instrumental exams and e-referral/in-person referral are indicated. If a diagnosis is made by the GP (namely, specific pain for LBP), therapy should follow the appropriate guidelines, including those of neuropathic pain. Patients should be monitored regularly to evaluate the effectiveness of treatment and the evolution of pain. In this case, specialist’s visit or e-referral should be requested, when necessary, namely if pain persists. If a diagnosis is missed (namely, nonspecific pain), the patient should continue the pain treatment and e-referral should be an option. Consequently, when the doctor cannot characterize the pain or if the initial treatment is not effective, a teleconsultation with a specialist can provide further guidance. Telemedicine can be a useful tool for follow-up without the need for in-person visits. Including advice on exercises, correct postures, and other physical therapies that the patient can do at home is essential to improve the condition and prevent relapses. It is crucial to provide the patient with clear information on what to do, what to avoid and how to manage pain independently, possibly through educational portals or information materials. Considering the factors that triggered the pain and the patient’s lifestyle habits can help prevent further episodes. An educational portal to provide guidelines on preventive exercises and behaviors is also useful.
Patient Management After Hospital Discharge: The Post-Surgery Period
The immediate post-surgery period is a vulnerable phase for orthopedic elective patients. Fragile subjects are directly to a rehabilitation ward. The remaining are discharged home with a tailored rehabilitation program. In this regard, an effective and substantial pain therapy is pivotal to guarantee the patient’s immediate mobility. Indeed, in cases of post-surgical pain, especially in patients with osteoporosis and musculoskeletal problems, it is crucial that the patient is able to move as soon as possible. There is no univocal protocol for pain therapy in this context, however paracetamol is again the first choice, sometimes in combination with NSAIDs or opioids, for the first two weeks after surgery, with the aim of minimize pain and enhance post-operative mobility.10,21 Moreover, in hospital settings, post-operative blocks and a combination of paracetamol with NSAIDs are often used to manage pain and improve patient’s autonomy. Notably, although some studies suggest that they may slow tissue healing, NSAIDs are still used for their effectiveness in controlling pain and inflammation, taking into consideration the potential associated risks.10,21 Generally, most patients are able to independently manage pain therapy in the first post-operative two weeks. Nevertheless, it is important that GPs are informed and able to monitor and support patients during the recovery period, intervening if necessary. Indeed, after 7–14 days blood count is advised to exclude the development of heparin-induced thrombocytopenia (HIT) and anemia. Usually, a specialist’s visit takes place after one month together with X-ray control. It should be anticipated only in case of refractory pain, required wound care or anemia. It can be suggested to use e-referral to avoid unnecessary visits and promptly solve some problems. In case of refractory pain, a rescue therapy is needed, once excluded surgical complication, to favor rehabilitation and movement. Otherwise, paracetamol alone after two weeks of multimodal therapy is advised. The algorithm suggested by experts regarding the early management of MP is resumed in Figure 2.
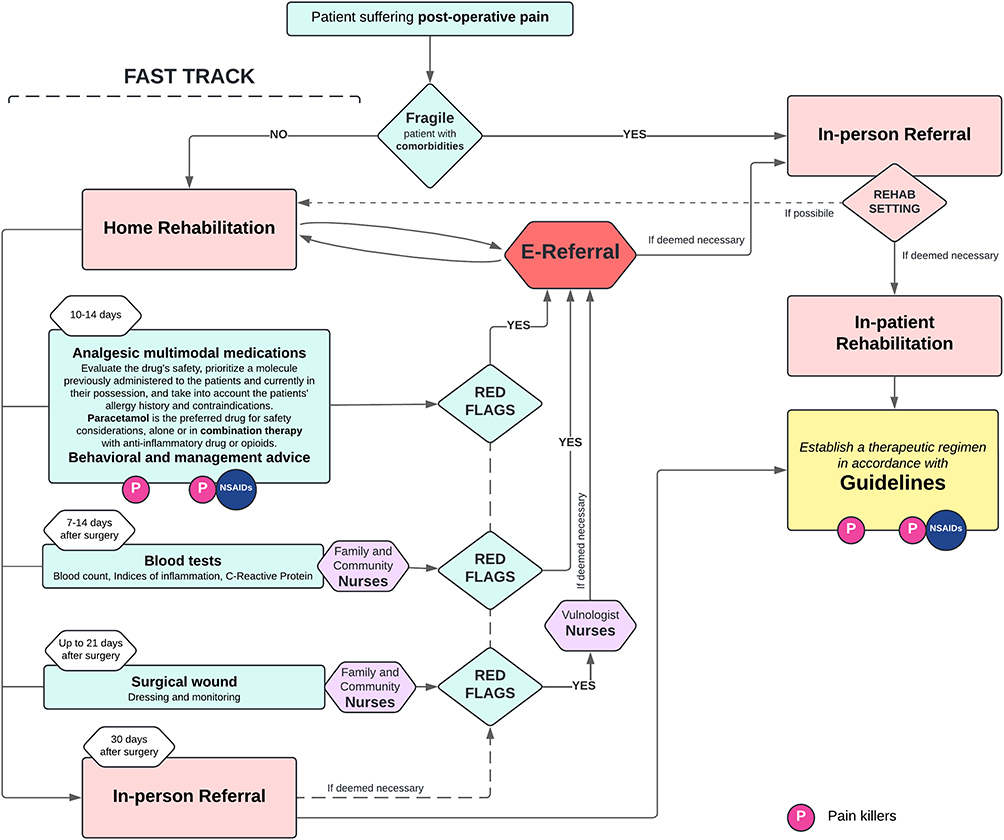 |
Figure 2 Algorithm on patient after surgery. |
Patient Management After Hospital Discharge: The Post-Emergency Period
Emergency situations involve patients who may present trauma, fractures, or soft tissue injuries. Surgical patients are dealt with the previous paragraph. In case of trauma, patients must necessarily be evaluated on-site by the specialist and subsequently an adequate therapeutic regimen should be established based on guidelines. In non-traumatic case, analgesic treatment should be initiated as soon as possible, as well. Paracetamol alone or in combination with NSAIDs or opioids is the first choice, for both situations. In the emergency room not all patients with musculoskeletal injuries should necessarily undergo X-ray exams, especially in cases of minor sprains. This approach aims to reduce unnecessary exposure to X-rays. Using specific criteria to determine when an X-ray exam is truly necessary is advocated. Once a fracture has been ruled out by negative imaging, pain management may include the use of paracetamol or codeine. In mild pain (NRS 1–3) paracetamol represents the first choice, in its oral formulation at a dosage of 1g 3 times per day.10 It can also be used in its orosoluble formulation, for a simple and easily applicable protocol, based on the immediate assessment of pain by nurses, allowing the achievement of satisfactory analgesia during the stay in the emergency department.
For greater pain (NRS > 3), paracetamol can be used at a dosage of 1 g up to 3 per day, in association with opioids in order to reduce their consumption. In case the intravenous formulation is chosen, paracetamol can be used at a dosage of 1 g i.v. up to 3 or 4 doses per day (according to national indications), allowing to reduce opioid consumption.22
NSAIDs are not recommended for non-fracture sprains (except of the first 48 hours) and ice is used in the first 5 days, as indicated in the PEACE&LOVE protocol.23
Generally, if the patient is discharged, paracetamol treatment should be maintained only when necessary 48 hours after the injury, and the rehabilitation program should be activated promptly. The involvement of the patient in a rehabilitation process is mandatory, typically by means of the activation of an orthopedic and physiatric referral. Also in this context, availability and accessibility of rehabilitation services are limited, so the panel emphasizes the need to train GPs to recognize and adequately manage non-fracture injuries, also using e-referral as a tool. Indeed, accurate diagnosis and timely initiation of rehabilitation are crucial to avoid long-term complications and improve patient’s outcome. In case of non-fracture pathologies, MRI is indicated no earlier than 14 days. E-referral is also useful in case of persistent pain or red flags found in instrumental investigations. The algorithm suggested by experts regarding the early management of MP is resumed in Figure 3.
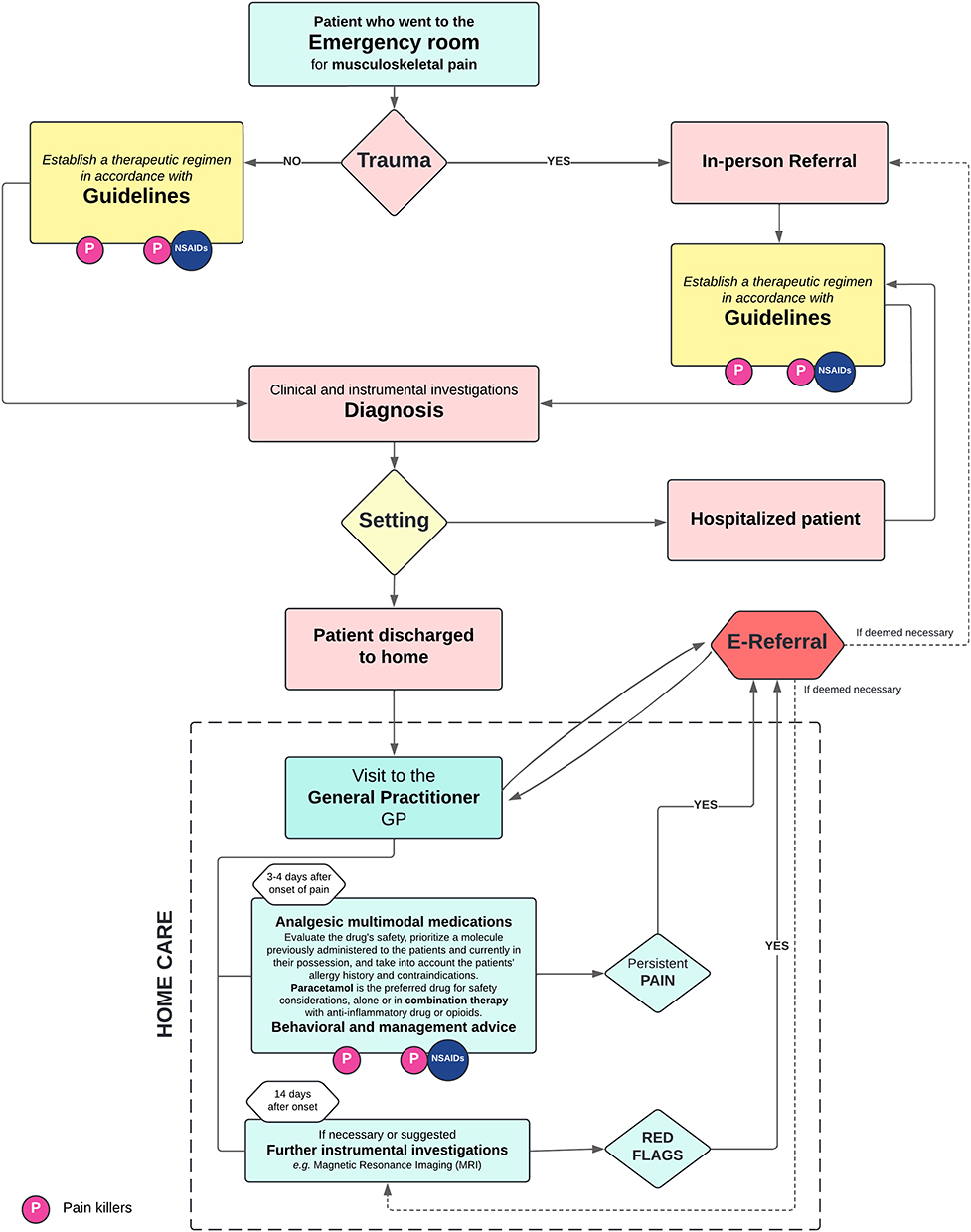 |
Figure 3 Algorithm on patient management after emergency. |
Conclusion
This expert opinion emphasizes a systematic, three-algorithm approach for managing musculoskeletal pain (MP) within primary care, focusing on early intervention and coordinated care pathways.
The first algorithm supports early management of acute MP directly in the GP’s office, outlining safe and accessible treatment options. The second algorithm focuses on post-surgical MP management, which plays a critical role in controlling pain, aiding recovery, and enabling early mobilization. The third algorithm addresses MP management following discharge from emergency settings, prioritizing immediate pain relief and patient education on self-management to avoid unnecessary follow-ups.
E-referral and teleconsultation are integral across these protocols, enabling GPs to collaborate effectively with specialists and streamline patient care. This structured approach positions GPs as primary coordinators in MP management, reducing pain chronicity and enhancing patient outcomes. In conclusion, the integration of early pain management protocols with telemedicine tools and e-referral pathways offers a comprehensive framework to improve patient outcomes and optimize healthcare resource allocation.
Funding
This study was sponsored by an unconditional contribution from Angelini Pharma.
Disclosure
Fabrizio Gervasoni: Teaching, editorial, dissemination, and/or clinical research activities in collaboration with: Angelini Pharma S.p.A., Abiogen Pharma, GlaxoSmithKline Consumer Healthcare Srl Unipersonale, Saluber MD srl, Gruppo Humantech, Pharmanutra, IBSA, Italfarmaco, Guna, ITECH Medical Division, Podartis, Laborest, Kyowa Kirin S.r.l., Ortopedia Castagna, Società Aziende Chimiche Riunite Angelini Francesco A.C.R.A.F. S.p.A, Chiesi Italia S.p.A., Exphy Srl (PHEX), Haleon. Giacomo Farì reports personal fees from Ethos s.r.l. Alberto Magni reports grants from Angelini Pharma. The other authors have nothing to disclose.
References
1. GBD. Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Puntillo F, Giglio M, Paladini A, et al. Pathophysiology of musculoskeletal pain: a narrative review. Ther Adv Musculoskelet Dis. 2021;13:1759720X21995067. doi:10.1177/1759720X21995067
3. Bates D, Schultheis BC, Hanes MC, et al. Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019;20(Suppl 1):S2–S12. doi:10.1093/pm/pnz075
4. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The Global Burden of Musculoskeletal Pain-Where to From Here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
5. Ranzatto ADDS, Chaves TC, Martins MN, et al. Pain intensity scales: a cross-sectional study on the preferences and knowledge of physiotherapists and participants with musculoskeletal pain. Musculoskelet Sci Pract. 2024;73:103162. doi:10.1016/j.msksp.2024.103162
6. Koleva D, Krulichova I, Bertolini G, Caimi V, Garattini L. Pain in primary care: an Italian survey. Eur J Public Health. 2005;15(5):475–479. doi:10.1093/eurpub/cki033
7. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
8. Del Giorno R, Frumento P, Varrassi G, Paladini A, Coaccioli S. Assessment of chronic pain and access to pain therapy: a cross-sectional population-based study. J Pain Res. 2017;10:2577–2584. doi:10.2147/JPR.S136292
9. Bonezzi C, Fornasari D, Cricelli C, Magni A, Ventriglia G. Not All Pain is Created Equal: basic Definitions and Diagnostic Work-Up. Pain Ther. 2020;9(Suppl 1):1–15. doi:10.1007/s40122-020-00217-w
10. Bonezzi C, Fornasari D, Cricelli C, Magni A, Ventriglia G. Pharmacological Management of Adults with Chronic Non-Cancer Pain in General Practice. Pain Ther. 2020;9(Suppl 1):17–28. doi:10.1007/s40122-020-00218-9
11. Boriani G, Maisano A, Bonini N, et al. Digital literacy as a potential barrier to implementation of cardiology tele-visits after COVID-19 pandemic: the INFO-COVID survey. J Geriatr Cardiol. 2021;18(9):739–747.
12. Yerlikaya T, Bağkur M, Özkader HB. Assessment of kinesiophobia levels in patients with musculoskeletal pathologies: a demographic, physical, and clinical perspective. Int J Orthop Trauma Nurs. 2024;54:101105. doi:10.1016/j.ijotn.2024.101105
13. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013;111(1):52–58. doi:10.1093/bja/aet127
14. Brizio A, Faure V, Baudino F. Medical semiotics in the telemedicine era: the birth of telesemiotics. Int J Med Inform. 2022;157:104573. doi:10.1016/j.ijmedinf.2021.104573
15. Ministry of Health. TELEMEDICINA Linee di indirizzo nazionali [TELEMEDICINE National guidelines]. Available from: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2129_allegato.pdf.
16. Chou R, Deyo R, Friedly J, et al. Systemic Pharmacologic Therapies for Low Back Pain: a Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017;166(7):480–492. doi:10.7326/M16-2458
17. Verkleij SP, Luijsterburg PA, Willemsen SP, Koes BW, Bohnen AM, Bierma-Zeinstra SM. Effectiveness of diclofenac versus paracetamol in knee osteoarthritis: a randomised controlled trial in primary care. Br J Gen Pract. 2015;65(637):e530–e537. doi:10.3399/bjgp15X686101
18. Vannacci A, Lombardi N, Simonetti M, et al. Regular use of Acetaminophen or acetaminophen-codeine combinations and prescription of rescue therapy with non-steroidal anti-inflammatory drugs: a population-based study in primary care. Curr Med Res Opin. 2017;33(6):1141–1148. doi:10.1080/03007995.2017.1308920
19. Kolasinski SL, Neogi T, Hochberg MC, et al. American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res). 2020;72(2):149–162. doi:10.1002/acr.24131
20. Vlaeyen JWS, Maher CG, Wiech K, et al. Low back pain. Nat Rev Dis Primers. 2018;4(1):52. doi:10.1038/s41572-018-0052-1
21. Helmerhorst GTT, Zwiers R, Ring D, Kloen P. Pain Relief After Operative Treatment of an Extremity Fracture: a Noninferiority Randomized Controlled Trial. J Bone Joint Surg Am. 2017;99(22):1908–1915. doi:10.2106/JBJS.17.00149
22. Gruppo di Studio “Emergenza” (Area Culturale Medicina dell’Emergenza) e del Gruppo di Studio “Dolore acuto e cronico” (Area Culturale Medicina del Dolore e Cure Palliative) [“Emergency” Study Group (Emergency Medicine Cultural Area) and the “Acute and Chronic Pain” Study Group (Pain Medicine and Palliative Care Cultural Area)]. Raccomandazioni Intersocietarie Italiane (SIAARTI, SIMEU, SIS 118, AISD, SIARED, SICUT, IRC) sulla gestione del dolore in emergenza [Italian Intercompany Recommendations (SIAARTI, SIMEU, SIS 118, AISD, SIARED, SICUT, IRC) on emergency pain management]. Available from: https://d1c2gz5q23tkk0.cloudfront.net/assets/uploads/3019636/asset/Raccomandazioni_gestione_del_dolore_in_emergenza.pdf?1607086718.
23. Dubois B, Esculier JF. Soft-tissue injuries simply need PEACE and LOVE. Br J Sports Med. 2020;54(2):72–73. doi:10.1136/bjsports-2019-101253
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.