")
Back to Journals » OncoTargets and Therapy » Volume 11
Early and late outcomes of bevacizumab plus chemotherapy versus chemotherapy alone as a neoadjuvant treatment in HER2-negative nonmetastatic breast cancer: a meta-analysis of randomized controlled trials
Received 11 September 2018
Accepted for publication 20 November 2018
Published 12 December 2018 Volume 2018:11 Pages 9049—9059
DOI https://doi.org/10.2147/OTT.S186816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Jinli Wei,* Yulin Luo,* Deyuan Fu
Department of Thyroid and Breast Surgery, Northern Jiangsu People’s Hospital, Yangzhou 225001, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Purpose: To better clarify the efficacy of neoadjuvant bevacizumab plus chemotherapy (BEV + CT) vs chemotherapy (CT) alone in the treatment of HER2-negative nonmetastatic breast cancer.
Methods: PubMed, Embase, Web of Science, and Cochrane Library databases were searched for relevant articles published from January 1, 2000 to July 31, 2018. Review Manager software version 5.3 was used to perform this meta-analysis.
Results: Six randomized controlled trials matched the selection criteria, yielding a total of 4,354 patients with early outcomes and 3,777 patients with late outcomes. Pooled pathological complete response (pCR) and 5-year disease-free survival (DFS) rates were higher for the neoadjuvant BEV + CT group (OR =1.37 [1.19, 1.58]; P<0.001 and HR =0.84 [0.72, 0.98]; P=0.020, respectively), but 5-year overall survival (OS) rate showed no significant difference (HR =0.79 [0.55, 1.11]; P=0.180). Subgroup analysis showed that the pCR rate was significantly higher in both patients with hormone receptor (HR)-positive breast cancer (OR =1.30 [1.01, 1.66]; P=0.040) and those with HR-negative breast cancer (OR =1.52 [1.25, 1.83]; P<0.001) in BEV + CT group.
Conclusion: Compared with CT alone, neoadjuvant BEV + CT significantly improved the 5-year DFS rate of HER2-negative breast cancer patients, but showed no benefit in terms of 5-year OS rate.
Keywords: bevacizumab, neoadjuvant chemotherapy, breast cancer, HER2-negative, randomized controlled trial
Introduction
Bevacizumab (BEV), approved by the US Food and Drug Administration in February 26, 2004, is a humanized monoclonal antibody directed against vascular endothelial growth factor, which promotes tumor angiogenesis via proliferation and migration of vascular endothelial cells.1,2 According to a review published in 2014, BEV improves overall survival (OS) and/or progression-free survival (PFS) when used in the first- and second-line treatment of metastatic cancers, such as colorectal cancer and nonsquamous non-small-cell lung cancer, and improves PFS when used in the first-line treatment of advanced renal cell carcinoma, breast cancer, and recurrent platinum-sensitive or platinum-resistant epithelial ovarian, fallopian tube, or peritoneal cancer.3 BEV and paclitaxel were also found to be effective in treating disseminated bone marrow carcinomatosis arising from breast cancer.4 In the case of HER2-negative breast cancer, BEV plus chemotherapy (BEV + CT) regimen resulted in improved PFS in the metastatic setting5–10 and improved pathological complete response (pCR) rate in the neoadjuvant setting.11–15 Similarly, a randomized, Phase III trial demonstrated that BEV, administered in combination with paclitaxel or capecitabine, was effective and may be used as an option for the first-line treatment of patients with HER2-negative metastatic breast cancer if other chemotherapy (CT) regimens, including taxanes or anthracyclines, are not considered appropriate.16 However, no benefit was found by adding BEV for 1 year to standard CT regimen in treating both colon and breast cancers.17–22 There are many factors that cannot be controlled in the studies of BEV as a treatment for advanced breast cancer; thus, some trials found only modest gain in PFS and OS.23–25 On the contrary, comparing the efficacy of BEV + CT regimen to CT-alone regimen for early, operable, or nonmetastatic breast cancer and then evaluating its long-term efficacy is more convincing. In this study, we performed a meta-analysis aimed at comparing the early and late outcomes of these two neoadjuvant chemotherapy (NAC) regimens in HER2-negative nonmetastatic breast cancer.
Methods
Search strategy
Eligible articles published between January 1, 2000 and July 31, 2018 were identified by searching the PubMed, Embase, Web of Science, and Cochrane Library databases. The following medical subject heading terms were used for the search: (breast OR mammary) AND (cancer OR tumo* OR carcinoma* OR neoplasm*) AND (bevacizumab OR avastin) AND (randomized controlled trial [Publication Type] OR randomized [Title/Abstract] OR placebo [Title/Abstract]). There was no language restriction placed on the search. References in the eligible articles were also reviewed to identify relevant citations.
Study selection
Only studies that fulfilled the following criteria were included: 1) randomized controlled trials (RCTs) that compared CT with BEV as a neoadjuvant treatment for nonmetastatic breast cancer patients without any prior cancer-related CT; 2) studies focusing on HER2-negative breast cancer; 3) studies with sufficient data on post-therapy pCR, disease-free survival (DFS), or OS to assess the short- or long-term efficacy of adding BEV to the CT treatment; and 4) articles published in English. There were no limitations on CT regimens.
The following studies were excluded: 1) studies on metastatic breast cancer, 2) non-randomized or single-arm clinical trials, 3) studies focusing on adjuvant CT alone, and 4) studies on HER2-positive breast cancer.
Data extraction and quality assessment
Two reviewers independently assessed all the potentially relevant studies. In the case of any disagreements, consensus was reached by discussion between the two reviewers or decided by senior investigators. Additionally, all authors independently assessed the risk of bias in each eligible trial. The Cochrane tool26 for assessing the risk of bias in randomized clinical trials was used to complete the risk assessment picture using Review Manager software version 5.3. Each study was rated based on the assessment criteria in the Cochrane Handbook for Systematic Reviews of Interventions version 5.3 (Figure 1 and Table 1).
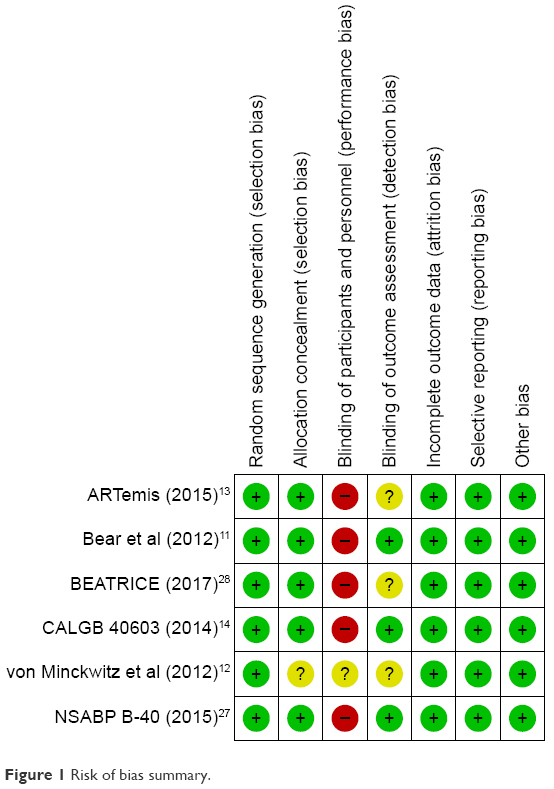 | Figure 1 Risk of bias summary. |
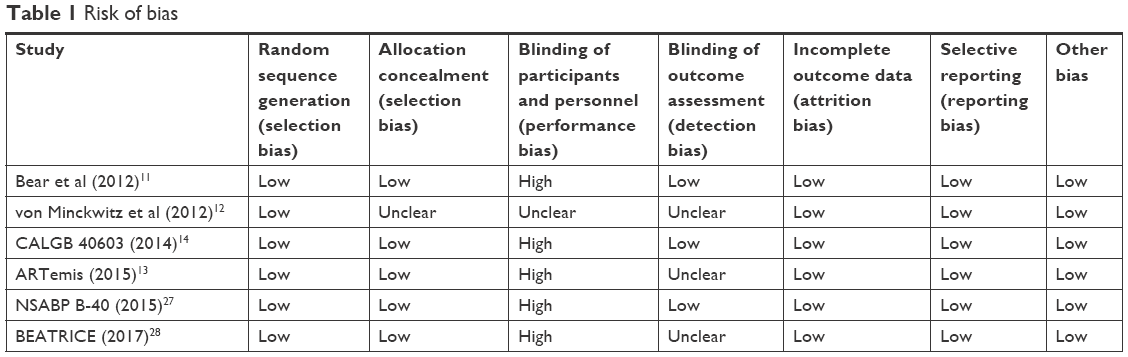 | Table 1 Risk of bias |
Statistical analysis
The Review Manager 5.3 statistical package was used to analyze the data on study variables; four of them were dichotomous variables expressed as ORs, and two of them were generic inverse variance variables expressed as HRs. To measure overall heterogeneity, we used the I2 statistic. I2 values greater than 50% indicated high heterogeneity. First, random-effect model was used for meta-analysis, and then heterogeneity was judged. If I2 value was less than 50%, then fixed-effect model was used instead of the random-effect model. Results were reported with 95% CIs, and a P-value of less than 0.05 was considered statistically significant; that is, the 95% CI did not include the value “1”.
Our study adhered to the PRISMA guidelines.
Results
Study quality and characteristics
A total of 1,041 records related to BEV and CT were retrieved by searching the PubMed, Embase, Web of Science, and Cochrane Library databases. After removing duplicate articles, 695 studies were found eligible, of which 15 full-text articles met the inclusion criteria. Of these 15 articles, two non-RCTs, two single-arm clinical trials, four HER2-positive breast cancer studies, and one study focusing on adjuvant CT alone were excluded. Finally, a total of six studies were included in the meta-analysis.11–14,27,28 The selection process is depicted in the flow diagram (Figure S1).
Table 2 presents the baseline characteristics of the six studies used for meta-analysis. A total of four RCTs assessed the early outcomes of 4,354 patients given CT alone (50.1%) and BEV + CT (49.9%), and two RCTs assessed the late outcomes of 3,777 patients given CT alone (49.9%) and BEV + CT (50.1%). In three of the six RCTs, patients were divided into several subgroups based on their CT regimens.11,14,27 Four RCTs, including seven subgroups, provided data on pCR,11–14 and two RCTs, including four subgroups, estimated DFS and OS.27,28 All the trials focused on patients without metastatic disease diagnosed by core needle biopsy of breast and lymph nodes (T1-4d, N0-3). Details about clinical nodal (CN) status and HR status were available in all six trials for all the subgroups. For approximately 1% of patients, CN status was unknown. All CT regimens included anthracycline and taxane, while some also included cyclophosphamide, capecitabine, gemcitabine, carboplatin, and fluorouracil (Table 2).
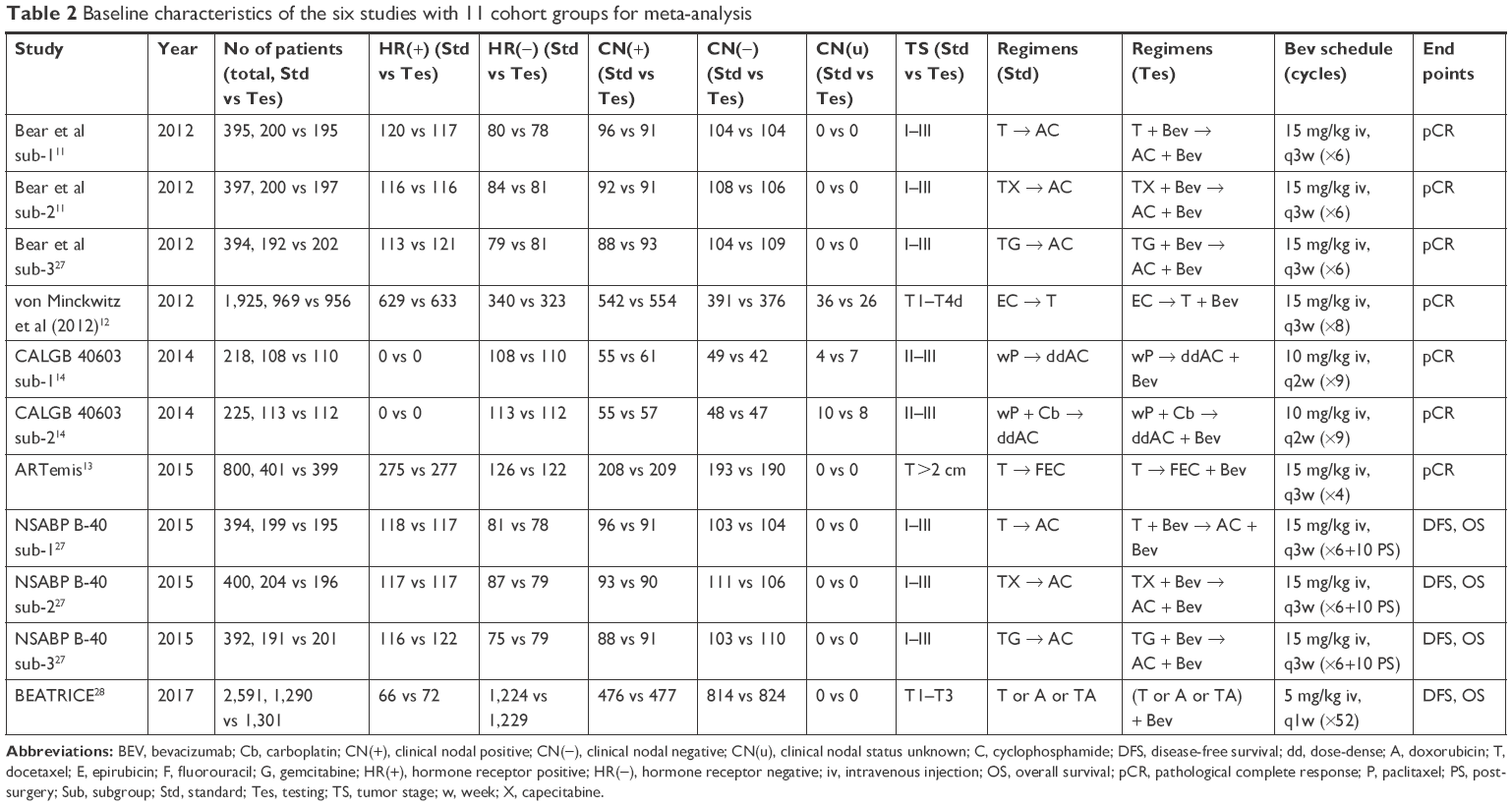 | Table 2 Baseline characteristics of the six studies with 11 cohort groups for meta-analysis |
Outcomes of interest
A total of 4,354 patients were included in pCR analysis. pCR was classified into two types after NAC: 1) pCR breast, which was defined as the absence of residual invasive disease with or without ductal carcinoma in situ regardless of nodes (ypT0/isN0/+) and 2) pCR breast/axillary which was defined as pCR breast and the absence of any tumor deposit ≥0.2 mm in sampled axillary nodes (ypT0/isN0). Invasive disease-free survival (IDFS) in the BEATRICE trial was classified as DFS.
The pooled event rates of pCR breast (ypT0/isN0/+) for the BEV + CT and CT-alone groups were 29% and 23%, respectively. Based on our analysis, the pooled estimate of OR was 1.37, and the 95% CI was 1.19–1.58 (P<0.001) (Figure 2A). Similar results were obtained when further subgroup analysis was performed (Figure 2B), suggesting that BEV + CT group showed distinctly improved rate of pCR in breast regardless of the presence or absence of axillary tumors (ypT0/isN0/+). With regard to pCR breast/axillary (ypT0/isN0), a higher incidence of pCR was also observed in the BEV + CT group (25%). The pooled estimate of OR was 1.32, and the 95% CI was 1.14–1.53 with or without subgroup analysis (P<0.001) (Figure 3A and B). This result suggests that BEV + CT group showed distinctly improved rate of pCR not only in breast but also in axillary nodes. In terms of HR status, pooled pCR was higher in triple-negative breast cancer (TNBC) (OR =1.52 [1.25, 1.83]; P<0.001) (Figure 4A) and HR-positive breast cancer (OR =1.30 [1.01, 1.66]; P=0.040) (Figure 4B) treated with BEV + CT.
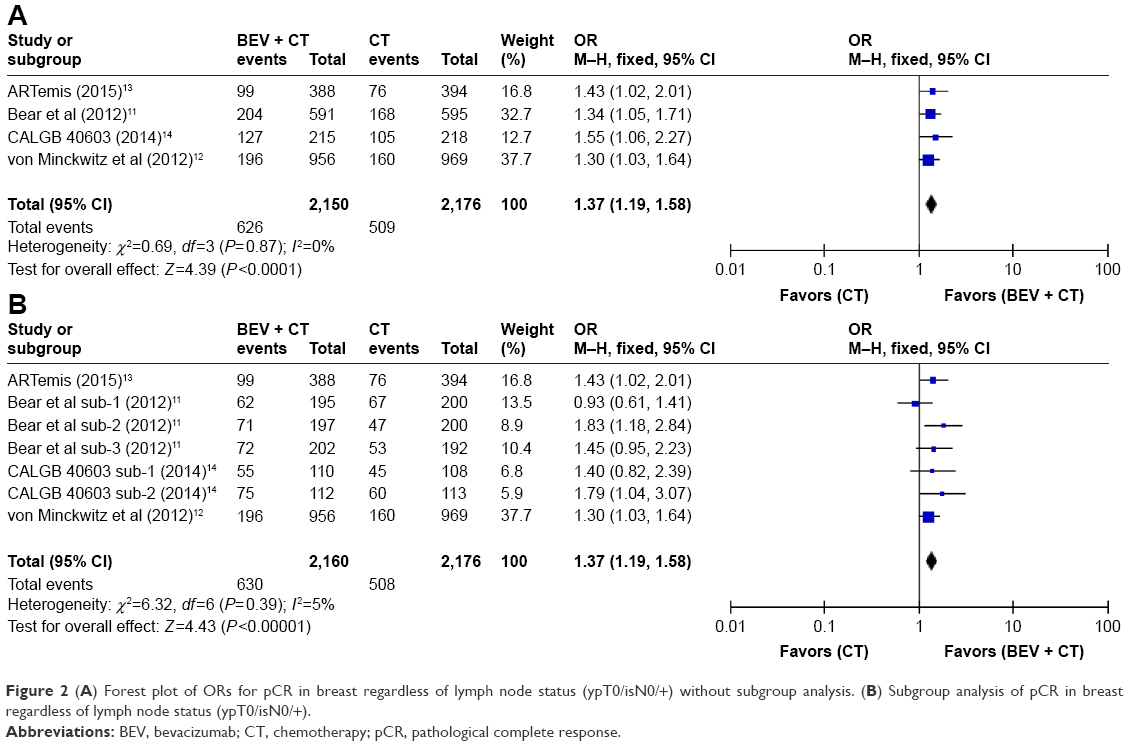 | Figure 2 (A) Forest plot of ORs for pCR in breast regardless of lymph node status (ypT0/isN0/+) without subgroup analysis. (B) Subgroup analysis of pCR in breast regardless of lymph node status (ypT0/isN0/+). |
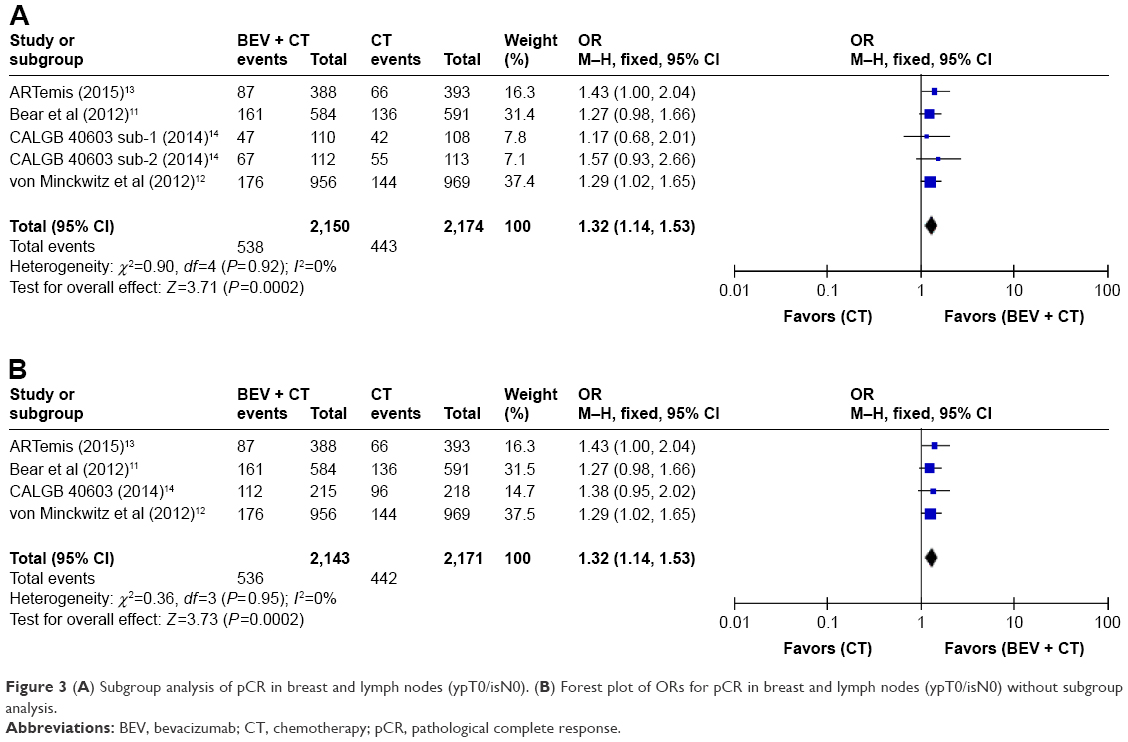 | Figure 3 (A) Subgroup analysis of pCR in breast and lymph nodes (ypT0/isN0). (B) Forest plot of ORs for pCR in breast and lymph nodes (ypT0/isN0) without subgroup analysis. |
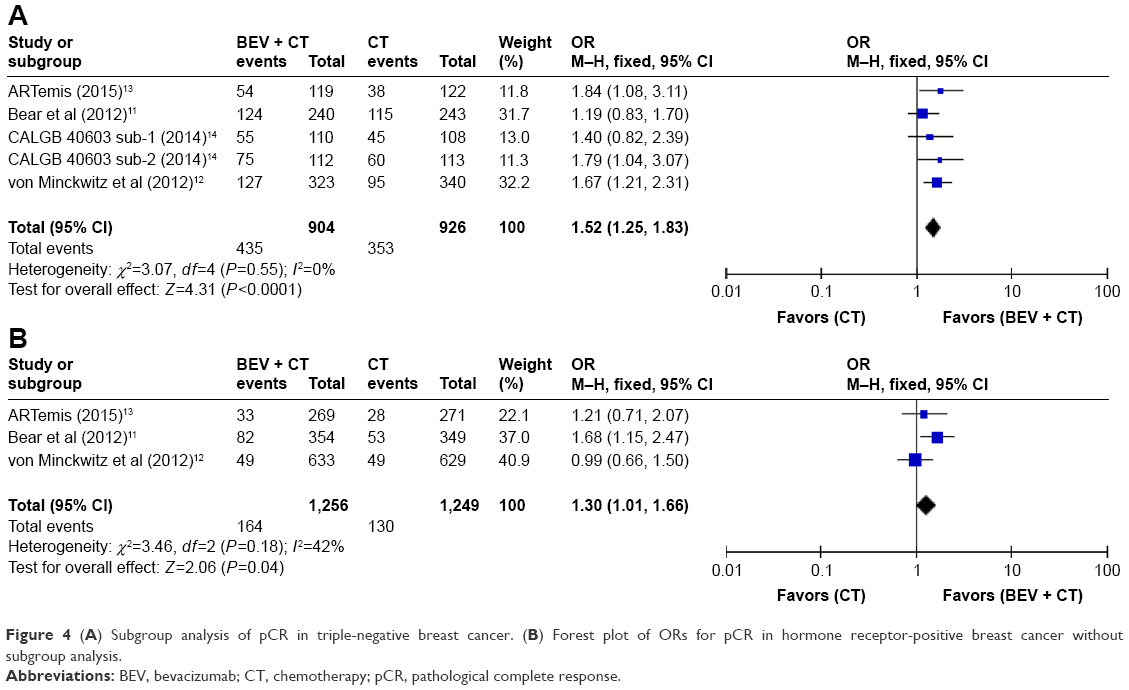 | Figure 4 (A) Subgroup analysis of pCR in triple-negative breast cancer. (B) Forest plot of ORs for pCR in hormone receptor-positive breast cancer without subgroup analysis. |
Two trials including 3,777 patients reported 5-year late-outcome data for OS and DFS. The final efficacy results of the BEATRICE trial published in April 2017 made it possible to evaluate the efficacy of neoadjuvant BEV in HER2-negative nonmetastatic breast cancer within 5 years.28 In order to make the index consistent, IDFS in the BEATRICE trial was defined as DFS. The percentage of the total number of patients with no follow-up information was 7.11% in the 5-year OS analysis (Table 3A) and 7.16% in the 5-year DFS analysis (Table 3B). There was no significant difference in 5-year OS between treatment groups (HR =0.79, 95% CI 0.55–1.11; P=0.180) (Figure 5A). However, BEV + CT was associated with better DFS (HR =0.84, 95% CI 0.72–0.98; P=0.020) (Figure 5B).
 | Table 3 Five-year OS data and 5-year DFS data |
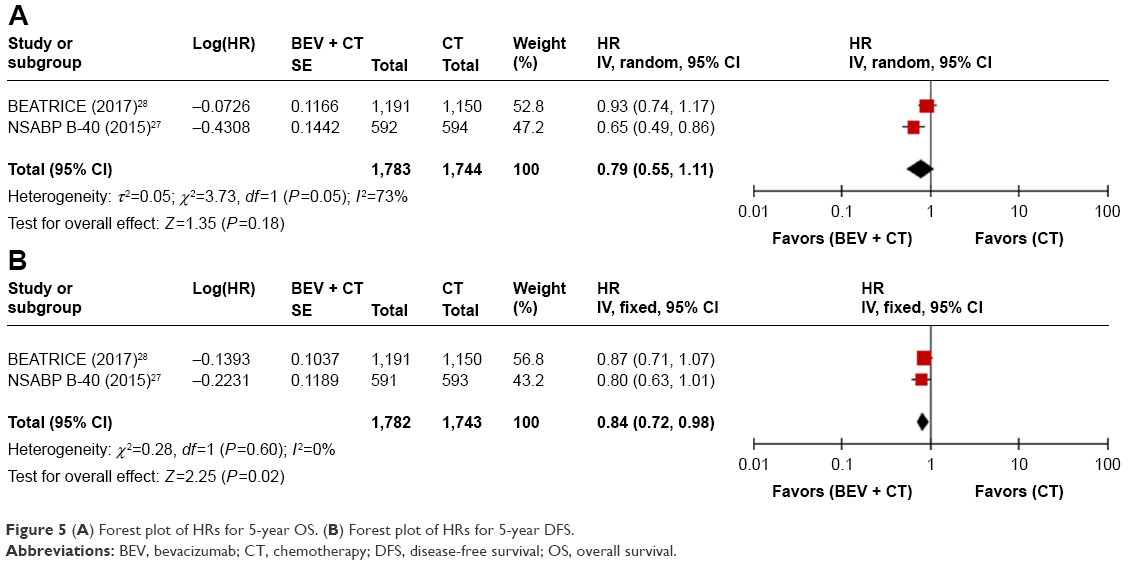 | Figure 5 (A) Forest plot of HRs for 5-year OS. (B) Forest plot of HRs for 5-year DFS. |
Publication bias
In the process of making forest plots, we conducted a sensitivity and heterogeneity analysis of the inclusion and elimination of each study. In essence, each study had no effect on outcome, and heterogeneity was less than 50%. We assessed publication bias using funnel plots (Figure 6).
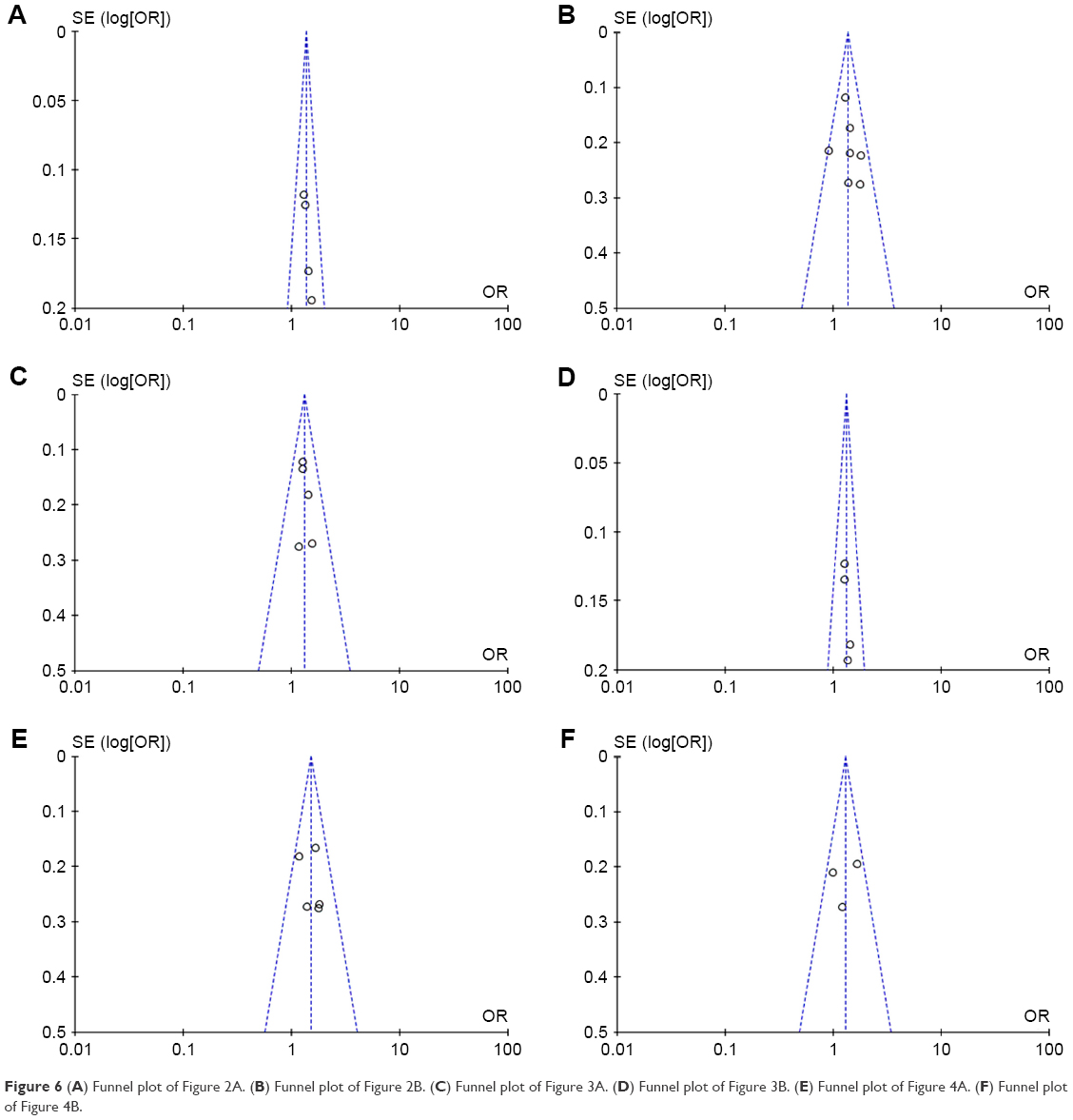 | Figure 6 (A) Funnel plot of Figure 2A. (B) Funnel plot of Figure 2B. (C) Funnel plot of Figure 3A. (D) Funnel plot of Figure 3B. (E) Funnel plot of Figure 4A. (F) Funnel plot of Figure 4B. |
Discussion
Randomized studies have shown that BEV + CT improves DFS and overall response rate compared to CT alone in metastatic breast cancer, but the relative efficacy of BEV + CT in early breast cancer is still controversial, especially for TNBC, which has a poor clinical outcome owing to limited treatment. Thus, we performed this meta-analysis aimed at comparing the early and late outcomes of these two NAC regimens in HER2-negative nonmetastatic breast cancer.
Of the four trials11–14 consisting of seven subgroups which reported pCR in breast while ignoring axillary lymph nodes status (ypT0/isN0/+), only Bear et al sub-1 reported a decreased pCR rate (1.5%) for BEV + CT group. Both Bear et al sub-3 and CALGB 40603 sub-1 reported a nonsignificant increase in pCR rate for the BEV + CT group. However, both the study of Bear et al and CALGB 40603 trials (without subgroup analysis) showed increased pCR rates for the BEV + CT group, which contradicts the results of the subgroup analysis. These conflicting results suggest that BEV + TX (docetaxel + capecitabine) → AC (doxorubicin + cyclophosphamide) was more effective than BEV + docetaxel (T) → AC and BEV + TG (docetaxel + gemcitabine) → AC, whereas BEV + wP (weekly paclitaxel) + carboplatin (Cb) → ddAC (dose-dense doxorubicin + cyclophosphamide) was more effective than BEV + wP → ddAC (Table 2).
In four trials11–14 which included five subgroups, pCR in breast and axillary lymph nodes (ypT0/isN0) was determined (Figure 3A and B). In CALGB 40603 sub-1, CALGB 40603 sub-2, CALGB 40603, and Bear et al study, a higher pCR rate in the BEV + CT group was not observed. However, ARTemis and von Minckwitz et al showed increased pCR rates for BEV + CT group, which were in accordance with the results of the total analysis shown in Figure 3A and B. These conflicting results suggest that the addition of neoadjuvant BEV to EC (epirubicin + cyclophosphamide) → T or T → FEC (fluorouracil + epirubicin + cyclophosphamide) was more effective than the addition of BEV to T → AC, T → AC (with capecitabine or gemcitabine), and wP → ddAC (with or without Cb) (Table 2).
We tried to determine which group of patients, HR positive or HR negative, benefited more from the addition of BEV to NAC. As shown in Figure 4A and B, CALGB 40603 reported pCR in HR-negative patients only; ARTemis, Bear et al, and von Minckwitz et al reported pCR in both HR-positive and HR-negative patients. Subgroup analysis in the Bear et al study (Figure 4B) showed that the effect of BEV on pCR was greater in HR-positive patients (OR =1.68 [1.15, 2.47]; P=0.008), and there was no statistically significant difference in TNBC patients (OR =1.19 [0.83, 1.70]; P=0.340) (Figure 4A). However, in the von Minckwitz et al trial, the opposite trend was found in the effect of BEV on pCR rate when HR levels were considered. Bear et al demonstrated that adding BEV to T → AC (with or without capecitabine or gemcitabine) was more effective in HER2-negative/HR-positive patients. In addition, von Minckwitz et al demonstrated that adding BEV to EC → T was more effective in TNBC patients. In conclusion, regardless of the HR levels or CT regimens, the rate of pCR was higher in the BEV + CT group than the CT-alone group.
The NSABP B-4027 and BEATRICE28 trials reported data on OS (Table 3A). Though the pooled 5-year OS did not differ significantly between the BEV + CT group and CT-alone group, the two trials did yield contrary results (Figure 5A). In the BEATRICE trial, there was no statistically significant difference in OS between the two treatment arms in either the total population (HR =0.93 [0.74, 1.17]; P=0.520) or the pre-specified subgroups.28 In addition, high heterogeneity could not be ignored (I2=73%). The different results and high heterogeneity in the two trials may be due to differences in HR status, CN status, regimens, and BEV dose. First and most importantly, there was a distinct difference in HR status: the proportion of HR-positive patients was 59.6% in NSABP B-40 vs 5.3% in BEATRICE. Second, the proportion of patients with positive axillary nodes was 50% in NSABP B-40 vs 36% in BEATRICE. Third, the additional drugs (cyclophosphamide or capecitabine or gemcitabine) in the NSABP B-40 trial (Table 2) may have played an important role. Fourth, in BEATRICE, patients were randomized 1:1 and received either BEV for 52 weeks (5 mg/kg/week equivalent) or four of more cycles of CT (T or A or TA) alone after definitive surgery, whereas in NSABP B-40 patients received BEV for 48 weeks (15 mg/kg every 3 weeks for six cycles of NAC plus 10 doses given postoperatively).
There are several limitations of this meta-analysis that need to be addressed. First, this is a retrospective study, resulting in selective reporting and failure to exclude incomplete outcome data. Second, the number of RCTs included was relatively small, especially in the analysis of OS and DFS. Third, the definition of pCR and DFS varied from trial to trial. Fourth, there were no specific causes of death reported in the BEATRICE and NSABP B-40 trials. Fifth, for the subgroup of HR-positive patients, a follow-up of only 5 years was short to find differences in OS in stages II–III. Despite these limitations, a meta-analysis is needed to determine which subgroup could benefit most from NAC with the addition of BEV.29–31 To obtain more convincing results, we suggest that more large trials with long-term follow-up to be conducted.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferrara N. Vascular endothelial growth factor as a target for anticancer therapy. Oncologist. 2004;9(Suppl 1):2–10. | ||
Ferrara N. Vascular endothelial growth factor: basic science and clinical progress. Endocr Rev. 2004;25(4):581–611. | ||
Keating GM. Bevacizumab: a review of its use in advanced cancer. Drugs. 2014;74(16):1891–1925. | ||
Kamata A, Hagiwara H, Koizumi M, et al. A case of disseminated bone marrow carcinomatosis arising from breast cancer for which paclitaxel and bevacizumab treatment was effective. Gan To Kagaku Ryoho. 2016;43(1):103–106. | ||
Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. | ||
Miles DW, Chan A, Dirix LY, et al. Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol. 2010;28(20):3239–3247. | ||
Miles D, Cameron D, Bondarenko I, et al. 1866 First results from the double-blind placebo (PL)-controlled randomised phase III MERiDiAN trial prospectively evaluating plasma (p)VEGF-A in patients (pts) receiving first-line paclitaxel (PAC) +/− bevacizumab (BV) for HER2-negative metastatic breast cancer (mBC). Eur J Cancer. 2015;51(3):S287–S288. | ||
Robert NJ, Diéras V, Glaspy J, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J Clin Oncol. 2011;29(10):1252–1260. | ||
Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized, double-blind, placebo-controlled, phase III trial evaluating the efficacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol. 2011;29(32):4286–4293. | ||
von Minckwitz G, Puglisi F, Cortes J, et al. Bevacizumab plus chemotherapy versus chemotherapy alone as second-line treatment for patients with HER2-negative locally recurrent or metastatic breast cancer after first-line treatment with bevacizumab plus chemotherapy (TANIA): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1269–1278. | ||
Bear HD, Tang G, Rastogi P, et al. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. N Engl J Med. 2012;366(4):310–320. | ||
von Minckwitz G, Eidtmann H, Rezai M, et al; German Breast Group; Arbeitsgemeinschaft Gynäkologische Onkologie–Breast Study Groups. Neoadjuvant chemotherapy and bevacizumab for HER2-negative breast cancer. N Engl J Med. 2012;366(4):299–309. | ||
Earl HM, Hiller L, Dunn JA, et al; ARTemis Investigators. Efficacy of neoadjuvant bevacizumab added to docetaxel followed by fluorouracil, epirubicin, and cyclophosphamide, for women with HER2-negative early breast cancer (ARTemis): an open-label, randomised, phase 3 trial. Lancet Oncol. 2015;16(6):656–666. | ||
Sikov WM, Berry DA, Perou CM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33(1):13–21. | ||
Nahleh ZA, Barlow WE, Hayes DF, et al. SWOG S0800 (NCI CDR0000636131): addition of bevacizumab to neoadjuvant nab-paclitaxel with dose-dense doxorubicin and cyclophosphamide improves pathologic complete response (pCR) rates in inflammatory or locally advanced breast cancer. Breast Cancer Res Treat. 2016;158(3):485–495. | ||
Allegra CJ, Yothers G, O’Connell MJ, et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J Clin Oncol. 2011;29(1):11–16. | ||
Allegra CJ, Yothers G, O’Connell MJ, et al. Bevacizumab in stage II–III colon cancer: 5-year update of the National Surgical Adjuvant Breast and Bowel Project C-08 trial. J Clin Oncol. 2013;31(3):359–364. | ||
Cameron D, Brown J, Dent R, et al. Adjuvant bevacizumab-containing therapy in triple-negative breast cancer (BEATRICE): primary results of a randomised, phase 3 trial. Lancet Oncol. 2013;14(10):933–942. | ||
Slamon DJ, Swain SM, Buyse M, et al. Abstract S1-03: Primary results from BETH, a phase 3 controlled study of adjuvant chemotherapy and trastuzumab±bevacizumab in patients with HER2-positive, node-positive or high risk node-negative breast cancer. Cancer Research. 2013;73(24 Supplement):S1–03. | ||
Miller K, O’Neill AM, Dang CT. Bevacizumab (Bv) in the adjuvant treatment of HER2-negative breast cancer: Final results from Eastern Cooperative Oncology Group E5103. J Clin Oncol. 2014;32(Suppl 1):500. | ||
Zielinski C, Láng I, Inbar M, et al. Bevacizumab plus paclitaxel versus bevacizumab plus capecitabine as first-line treatment for HER2-negative metastatic breast cancer (TURANDOT): primary endpoint results of a randomised, open-label, non-inferiority, phase 3 trial. Lancet Oncol. 2016;17(9):1230–1239. | ||
de Gramont A, Van Cutsem E, Schmoll HJ, et al. Bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for colon cancer (AVANT): a phase 3 randomised controlled trial. Lancet Oncol. 2012;13(12):1225–1233. | ||
Dickler MN, Barry WT, Cirrincione CT, et al. Phase III trial evaluating letrozole as first-line endocrine therapy with or without bevacizumab for the treatment of postmenopausal women with hormone receptor-positive advanced-stage breast cancer: CALGB 40503 (Alliance). J Clin Oncol. 2016;34(22):2602–2609. | ||
Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. | ||
Aalders KC, Tryfonidis K, Senkus E, Cardoso F. Anti-angiogenic treatment in breast cancer: Facts, successes, failures and future perspectives. Cancer Treat Rev. 2017;53:98–110. | ||
Jørgensen L, Paludan-Müller AS, Laursen DR, et al. Evaluation of the Cochrane tool for assessing risk of bias in randomized clinical trials: overview of published comments and analysis of user practice in Cochrane and non-Cochrane reviews. Syst Rev. 2016;5:80. | ||
Bear HD, Tang G, Rastogi P, et al. Neoadjuvant plus adjuvant bevacizumab in early breast cancer (NSABP B-40 [NRG Oncology]): secondary outcomes of a phase 3, randomised controlled trial. Lancet Oncol. 2015;16(9):1037–1048. | ||
Bell R, Brown J, Parmar M, et al. Final efficacy and updated safety results of the randomized phase III BEATRICE trial evaluating adjuvant bevacizumab-containing therapy in triple-negative early breast cancer. Ann Oncol. 2017;28(4):754–760. | ||
Metcalfe KA, Lubinski J, Ghadirian P, et al; Hereditary Breast Cancer Clinical Study Group. Predictors of contralateral prophylactic mastectomy in women with a BRCA1 or BRCA2 mutation: the Hereditary Breast Cancer Clinical Study Group. J Clin Oncol. 2008;26(7):1093–1097. | ||
Adkisson CD, Bagaria SP, Parker AS, et al. Which eligible breast conservation patients choose mastectomy in the setting of newly diagnosed breast cancer? Ann Surg Oncol. 2012;19(4):1129–1136. | ||
Valachis A, Nearchou AD, Lind P. Surgical management of breast cancer in BRCA-mutation carriers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2014;144(3):443–455. |
Supplementary material
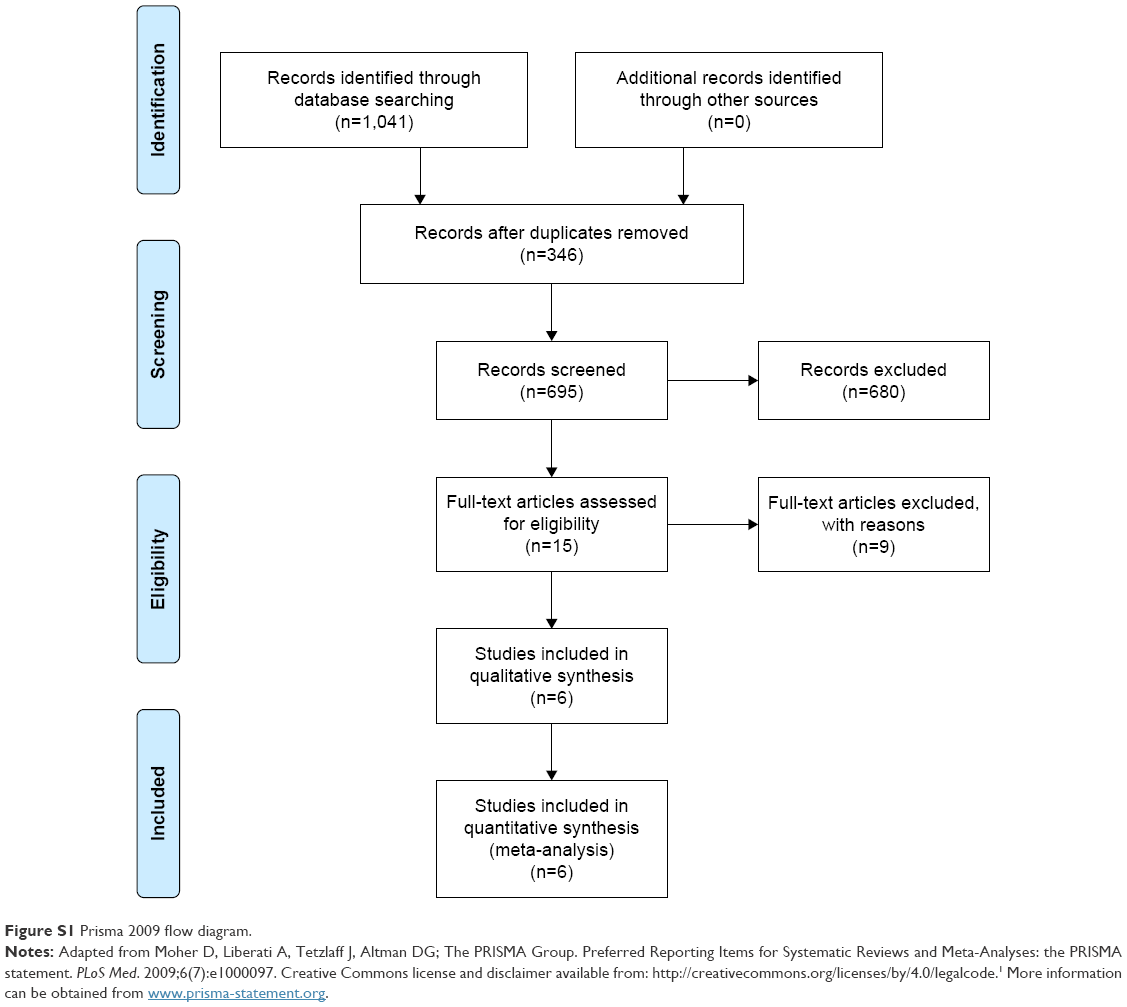 | Figure S1 Prisma 2009 flow diagram. |
Reference
Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.