Back to Journals » International Journal of General Medicine » Volume 16
E2/E3 and E3/E4 Genotypes of the Apolipoprotein E are Associated with Higher Risk of Diabetes Mellitus in Patients with Hypertension
Authors Han W, Xiong N, Zhong R, Pan Z
Received 14 September 2023
Accepted for publication 18 November 2023
Published 24 November 2023 Volume 2023:16 Pages 5579—5586
DOI https://doi.org/10.2147/IJGM.S438008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Wendao Han,1,2 Nating Xiong,1,2 Renkai Zhong,1,2 Zhongyi Pan1,2
1Department of Blood Transfusion, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Center for Precision Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Wendao Han, Meizhou People’s Hospital, Meizhou, People’s Republic of China, Email [email protected]
Objective: Apolipoprotein E (APOE) plays an important role in the lipid metabolism. APOE polymorphisms have been implicated in susceptibility to diabetes mellitus (DM). However, the association between APOE polymorphisms and the risk of DM among the hypertensive patients remains unclear. Our study aimed to evaluate this relationship to provide clues for further developing DM in hypertensive patients.
Methods: The study included 808 hypertensive patients with DM and 1226 hypertensive patients without DM as controls. The APOE 388T>C (rs429358) and 526C>T (rs7412) polymorphisms were genotyped by polymerase chain reaction (PCR) - microarray. Differences in APOE genotypes between subjects and controls were compared. To analyze the relationship between APOE genotypes and DM risk, multiple logistic regression analysis was performed after adjusting for gender, age, smoking history, and drinking history.
Results: The APOE E2/E4, E3/E3 genotype and ϵ2, ϵ3 allele frequency had significant difference between DM patients and controls (P< 0.05). The DM patients with ɛ4 allele had lower level in high-density lipoprotein cholesterol (HDL-C) and higher level in apolipoprotein B (ApoB) than those with ɛ2 allele. The results of logistic regression analysis indicated that the APOE genotype of E2/E3 with adjusted OR=1.350 (95% Cl=1.009– 1.806, P=0.043) and E3/E4 with adjusted OR=1.325 (95% Cl=1.034– 1699, P=0.026) may be independent risk factors for DM.
Conclusion: APOE E2/E3 and E3/E4 genotypes may be risk factors for developing diabetes mellitus in hypertensive patients.
Keywords: Apolipoprotein E, polymorphism, hypertension, diabetes mellitus
Introduction
As a chronic disease, hypertension (HTN) is very common in China, and its occurrence and development is a serious threat to human health.1–3 It has long been recognized that hypertension is an important risk factor for cardiovascular disease and mortality, the cardiovascular diseases account for 30% of all deaths, and about 13.5% premature deaths and 6.0% disability-adjusted life years has been attributed to high blood pressure worldwide.4 In China, the prevalence of HTN in adults almost doubled from 18% to 34% from 2002 to 2010.5 Diabetes mellitus (DM) is also an important global public health problem with high morbidity and disability rates. The HTN and DM often co-exist in the same individual. Studies have shown that hypertensive patients are more susceptible to DM compared to normotensive subjects.6,7 Both the two diseases are in common in terms of etiology, such as obesity, inflammation, oxidative stress, insulin resistance, and factors associated with increased microvascular and macrovascular damage.8 When hypertensive patients combine with DM, it brings more challenges to the health status of hypertensive patients. Therefore, predicting whether hypertensive patients are at risk of diabetes may be more conducive to the treatment and control of the disease.9
Apolipoprotein E (ApoE) is one of the components of the plasma lipoproteins. It is the structural and functional component of very low-density lipoprotein cholesterol (VLDL-C), high-density lipoprotein cholesterol (HDL-C), which is also the ligand of the binding between lipoprotein and receptor that plays an important role in lipoprotein metabolism.10 The occurrence of hypertension and DM are both associated with dyslipidemia, probably due to insulin resistance affecting the enzymes involved in lipid metabolism.11 ApoE is a protein encoded by the APOE gene. The human APOE gene consists of 3597 nucleotides located on band 2 of region 13 (19q13.2) of human chromosome 19, which is a 34 kD lipid transport-associated protein with 4 exons and 3 introns.12 There are two non-synonymous single-nucleotide polymorphisms (SNP) in the APOE gene, including rs7412 (C4075→T) and rs429358 (C3937→T). And the combination of the two SNPs results in three major alleles (ε2(388T-526T), ε3(388T-526C), and ε4(388C-526C)),13 and form six different genotypes, including three homozygotes (E2/E2, E3/E3, E4/E4) and three heterozygotes (E2/E3, E2/E4, E3/E4).14 Genotype E3/E3 accepted as “wild-type” is the most common isoform of APOE with a frequency of approximately 70–80%, and the other genotypes are deemed to be mutant types.
Studies have showed that APOE gene polymorphism was established to be related to hypertension and type 2 Diabetes Mellitus (T2DM).15,16 APOE ε4 allele and the E3/E4, E4/E4 genotypes are associated with the increased risk of hypertension, while ε2 allele and the E2/E2, E2/E3 genotypes are not associated with the risk of hypertension.17,18 Furthermore, APOE allele ε4 is associated with the increased risk for the development of T2DM, while allele ε2 is not associated with T2DM.19,20 However, the relationship between the APOE gene polymorphisms and the risk of developing DM in HTN patients remains uncertain. In the current study, we intended to explore the association between APOE gene polymorphisms and the risk of DM in HTN patients.
Materials and Methods
Study Participants
This study was a hospital-based, case-control study of APOE gene polymorphisms in hypertensive patients. A total number of 2034 patients with hypertension were recruited from August 2016 to December 2020. There were 808 patients with hypertension and DM were incorporated in the case group, while 1226 HTN patients without DM were set as a control group. Inclusive criteria of hypertensive patients were the following: (1) a mean systolic blood pressure >140 mmHg and/or a mean diastolic blood pressure >90 mmHg,21 (2) Age ≥18 years old.
Data Collection
Demographic data including gender, age, history of smoking, and history of drinking. Serum lipid levels of the samples were evaluated by an Olympus AU5400 system (Olympus Corporation, Tokyo, Japan). Venous blood was collected on an empty stomach at early morning, and serum lipid levels were detected, including triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), Apolipoprotein A1 (Apo-A1), and Apolipoprotein B (ApoB). T2DM was defined as blood glucose ≥11.1 mol/L at any time or fasting blood glucose ≥7.0 mol/L, or 2-hour postprandial plasma glucose level ≥11.1 mol/L.22
DNA Extraction and Genotyping
A 2 mL venous blood sample was collected from each participant into an ethylene diamine tetraacetic acid (EDTA) sample tube. Genomic DNA was extracted from whole blood using a Blood DNA Isolation Kit (Qiagen GmbH, Germany). The quality and concentration of the DNA were assessed using a Nano-Drop 2000™ spectrophotometer (ThermoFisher Scientific, Waltham, MA, USA). Genotyping of the APOE gene single nucleotide polymorphisms (including rs429358 and rs7412) were amplified by polymerase chain reaction (PCR) - microarray method (Sinochips Bioscience Co., Ltd., Zhuhai, Guangdong, China). The PCR was performed as the following program: 2 minutes at 50 °C, 15 minutes at 95°C for initial denaturation, and 45 thermal cycles (94°C for 30s and 65°C for 45s). The PCR products were subsequently added to the gene chip after PCR amplification, and hybridized with wild-type or mutant probes fixed on the chip. The genotypes of the samples were determined by the hybridization reaction.
Statistical Analysis
All statistical analysis were performed using SPSS statistical software version 21.0 (IBM Inc., USA). Continuous variables were expressed as means ± standard deviations and were compared using either Student’s t-test or the Mann–Whitney U-test. Genotype composition ratios and allele frequencies between groups were analyzed with the Chi-square test. Hardy-Weinberg equilibrium in the DM group and controls was evaluated by Chi-square test. Logistic regression analysis was applied to examine the relationship between APOE gene polymorphisms and DM. P<0.05 was considered to represent statistical significance.
Results
Characteristics of Subjects
A total of 2034 hypertensive subjects were included in this study, consisting of 808 DM patients and 1226 unaffected controls. The case group consisted of 542 (67.1%) male and 266 (32.9%) female patients, while the control group had 805 (65.7%) male and 421 (34.3%) female patients. There were 185 (22.9%) cases with <60 years old and 623 (77.1%) cases with ≥60 years old in DM patients; 300 (24.5%) cases with <60 years old and 926 (75.5%) cases with ≥60 years old in controls. The TG (P<0.001), TC (P<0.001), LDL-C (P=0.002), and Apo-B (P<0.001) levels in the DM subjects were higher than that in controls, while the HDL-C (P<0.001) and Apo-A1 (P=0.001) levels in the DM subjects were lower than that in controls. There were not statistically significant differences in the percentage of subjects with a history of smoking (P=0.918), and alcoholism (P=0.079) (Table 1).
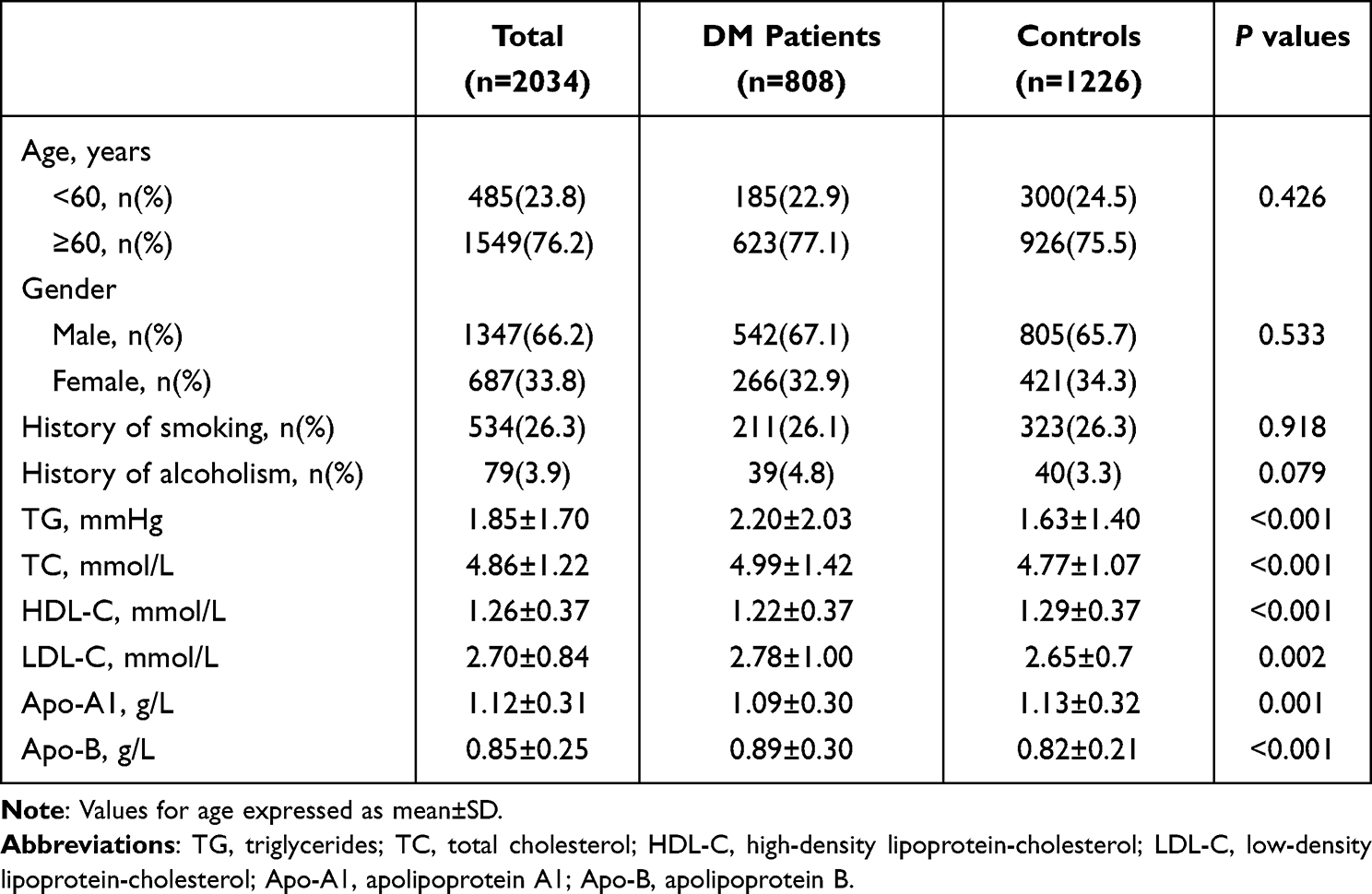 |
Table 1 Clinical Characteristics of DM Patients and Control Participants |
Distribution of the APOE Genotypes and Alleles Between the DM and Control Groups
The allelic distribution of the APOE gene was tested for Hardy-Weinberg equilibrium using the chi-square test, and the APOE genotypes in the DM group (χ2=5.790, P=0.215) and control group (χ2=4.090, P=0.394) confirmed to the Hardy-Weinberg equilibrium, respectively. Compared to the control group, the frequency of the E2/E4 genotype was higher in the DM group (2.1% vs 1.0%, P=0.036), and the frequency of the E3/E3 genotype was lower (67.3% vs 73.7%, P=0.002). The frequency of the ε2 allele was higher (8.0% vs 5.9%, P=0.007) and ε3 allele was lower (81.9% vs 85.5%, P=0.002) in the DM than that in the control group (Table 2).
 |
Table 2 Distribution Frequencies of APOE Genotype and Allele in DM Patients and Controls |
Characteristics of DM Patients Stratified by APOE Genotypes and APOE Alleles
Subjects with the E2/E2 genotype (n = 15, 8 patients and 7 controls), the E2/E4 genotype (n = 29, 17 patients and 12 controls) and E4/E4 genotype (n = 17, 4 patients and 13 controls) were excluded from the analysis of the relationship between APOE alleles and lipid levels due to the smaller number of cases. Clinical and laboratory variables were compared among DM patients carried different APOE genotypes and alleles. The DM patients with E3/E4 genotype had higher level in TG (2.49±2.56 mmol/L vs 2.03±1.56 mmol/L, and 2.10±1.89 mmol/L) (P<0.05) and Apo-B (0.95±0.34 g/L vs 0.84±0.26 g/L, and 0.88±0.29 g/L) (P<0.05), while had lower level in HDL-C (1.14±0.41 mmol/L vs 1.25±0.39 mmol/L, and 1.23±0.35 mmol/L) (P<0.05) than those with E2/E3 and E3/E3 genotype. Furthermore, compared with patients carried E3/E3 or E3/E4, the patients carried E2/E3 showed lower level in LDL-C (2.61±0.87 mmol/L vs 2.78±1.00 mmol/L, and 2.89±1.09 mmol/L) (P<0.05). The level of Apo-A1 in patients carried E3/E4 genotype was lower than that in E3/E3 genotype (1.03±0.31 g/L vs 1.10±0.29 g/L) (P<0.05). The clinical characteristics were compared among DM patients carried ɛ2, ɛ3 and ɛ4 allele. The DM patients with ɛ4 allele had lower level in HDL-C (1.14±0.41 mmol/L vs 1.26±0.38 mmol/L) while had higher level in ApoB (0.93±0.33 g/L vs 0.84±0.28 g/L) (all P<0.05) than those with ɛ2 allele. There were no statistically significant differences in the percentage of gender, history of smoking, history of alcoholism, and age, the level of TC and LDL-C among DM patients carried E2/E3, E3/E3 and E3/E4 genotypes, as well as ɛ2, ɛ3 and ɛ4 alleles, respectively (Table 3).
 |
Table 3 Clinical Characteristics of Subjects Stratified by APOE Genotypes and Ɛ2, Ɛ3, Ɛ4 Alleles in DM Patients |
Association of APOE Gene Polymorphisms with DM in Hypertensive Patients
Logistic regression analysis was used to evaluate independent predictors of DM in hypertensive patients. Univariate regression analysis was performed to obtain the unadjusted odds ratio (OR), and multiple logistic regression analysis was performed to obtain the adjusted OR. Subjects with the E2/E4 genotype (n=29) were excluded from the analysis of the relationship between APOE genotypes and characteristics of all patients because of the opposite effects of the ε2 and ε4 alleles in lipid metabolism.15,23 Relative analysis was used to evaluate the association between the APOE genotypes and potential risk factors for DM (Table 4). The APOE genotype of E2/E3 with adjusted OR=1.350 (95% Cl=1.009–1.806, P=0.043) and E3/E4 with adjusted OR=1.325 (95% Cl=1.034–1.699, P=0.026) were independent risk factors for DM. However, the other APOE genotypes were not found to be an independent risk factor for DM in hypertensive patients.
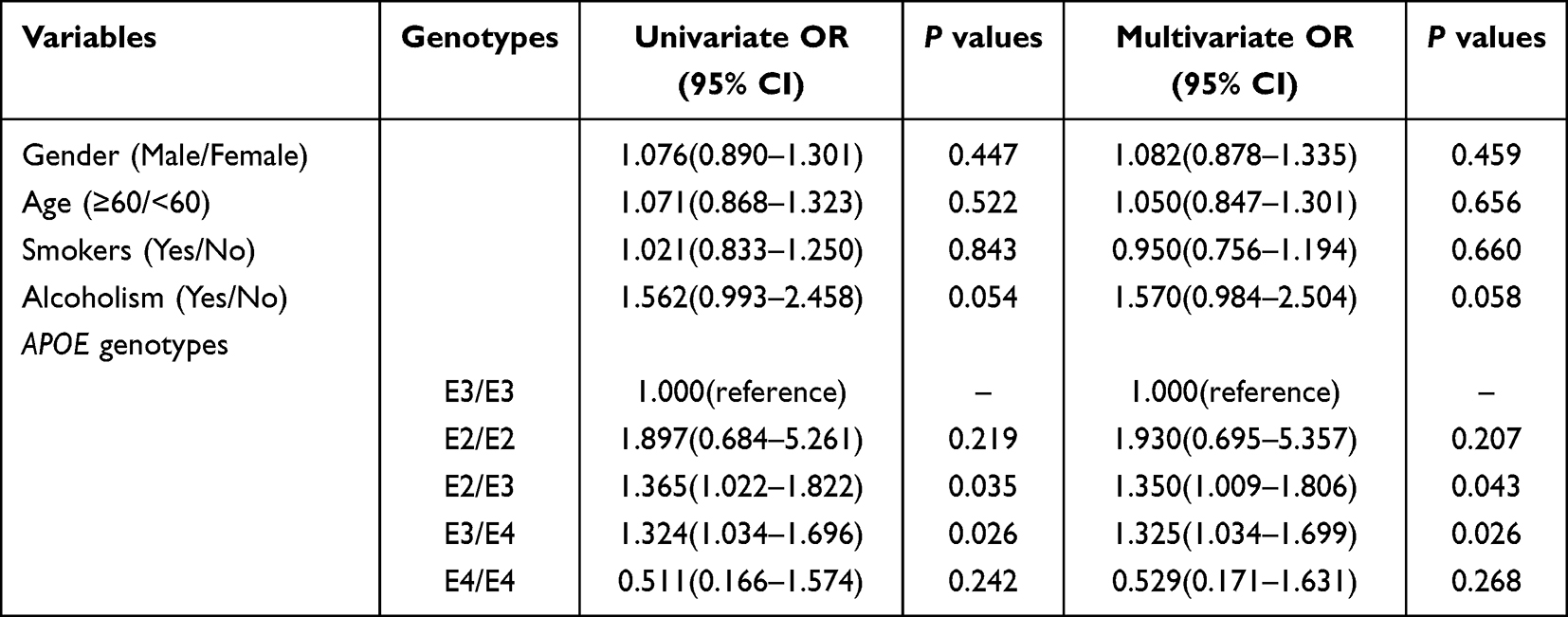 |
Table 4 Multivariate Logistic Regression of Variables Related to DM in Hypertensive Patients |
Discussion
Hypertension and DM share common risk factors and usually co-occur.24 Hypertension is common in patients with DM, and DM is more common in patients with hypertension than in general population.24,25 Studies showed that DM was almost 1.5–2.5 times as likely to develop in patients with hypertension as in those with normal blood pressure.26–28 Lipid levels have been linked to the risk of hypertension and DM, and dyslipidemia is a significant risk factor for hypertension and DM.29,30 ApoE is involved in lipid metabolism, so that the APOE gene polymorphisms are associated with DM and HTN. In this study, we examined the relationship between APOE gene polymorphisms and DM in patients with hypertension.
In the current study, we observed that the level of TG, TC, LDL-C and Apo-B were higher in the DM group than that in the control group. Research has found that one of the main phenotypes of DM patients is dyslipidemia, especially hypertriglyceridemia and low HDL-C level.31 Apo-A1 and ApoB are two major apoproteins, Apo-A1 is the major lipoprotein associated with HDL-C, and ApoB is associated with LDL-C. Studies have shown that Apo-A1 was negatively correlated with DM and hypertension,32 while ApoB was positively correlated with DM and hypertension.33,34 In addition, the DM patients with ɛ4 allele had lower level in HDL-C than those with ɛ2 allele. A study suggested that APOE polymorphism is highly correlated with lipid levels in Korean population.35 Liu et al showed that LDL-C level was associated with DM in hypertensive patients.36 In T2DM patients, serum lipid levels in ɛ4 group were significantly higher than those in ɛ3 and ɛ2 groups.16 In T2DM patients, there are significant differences in plasma LDL-C levels between ApoE subtypes.37 Chen et al showed that the highest diastolic blood pressure (DBP) and longest hypertension durations in hypertensive patients were independent risk factors for T2DM.28 Among hypertensive patients, a higher level of triglyceride glucose (TyG) index (triglycerides (mg/dl)×fasting blood glucose (mg/dl)/2) was associated with an elevated risk of T2DM.27
In this study, we also found that the APOE E2/E3 and E3/E4 genotypes were independent risk factor for DM in hypertensive patients. Several previous studies have reported that APOE polymorphisms have been linked to impaired glucose metabolism and a high risk of DM and hypertension. Zeng et al found that APOE ε2 and ε4 alleles have specifically been linked to developing diabetes or impaired glucose tolerance.16 The APOE ε2 allele may be a protective factor while the APOE ε4 allele may be risk factors for hypertension.19 The APOE ɛ4 allele may be a risk factor for T2DM.38 Among a Han Chinese population in central China, the APOE E3/E4 genotype is associated with an increased risk of T2DM.16 Our study did not conflict with the results of previous studies, where hypertensive patients carrying the E2/E3 or E3/E4 genotype had a 1.3-fold higher risk of developing DM than the controls. Other studies, on the other hand, have come to different conclusions. Srirojnopkun et al found that APOE polymorphisms might not be the genetic risk factors for T2DM in Southern Thai population.39 Studies have shown that ɛ4 carriers are less likely to develop T2DM.40,41 Santos-Ferreira et al showed that the incidence of T2DM in APOE ɛ2 carriers is approximately tripled.42
Regarding the mechanism of ApoE in the occurrence of diabetes in hypertensive people, on the one hand, chronic inflammation exists in hypertension, and subclinical inflammation and insulin resistance exist in DM patients.43,44 Studies have shown that ApoE−/− mice can produce severe leukocytes and mononucleosis, in ApoE−/− mice, hematopoietic stem cells (HSC) and their precursors lack an important cholesterol efflux mechanism, and their accumulated cholesterol leads to the expression of granulocyte-macrophage colony-stimulating factor (GM-CSF) and interleukin-3 (IL-3) receptor on the plasma membrane.45,46 On the other hand, ApoE may also be related to insulin secretion. In animal experiments, ApoE4 mice showed impaired glucose and insulin tolerance, reduced insulin secretion, and decreased cognitive and sensorimotor characteristics compared to ApoE3 mice, and these changes were associated with central nervous system processes.47 Dyslipidemia is considered to be a risk factor for diabetes,48 so the regulatory effects of ApoE expressed by different APOE genotypes on lipid metabolism are different, which is related to the pathogenesis of diabetes. The mechanism of the relationship between ApoE subtypes and DM risk is unclear and needs more in-depth research to reveal.
This study found that APOE E2/E3 and E3/E4 genotypes may be risk factors for developing diabetes in hypertensive patients. This study suggests that hypertensive patients with APOE E2/E3 and E3/E4 genotypes need to be monitored for diabetes risk. However, there are several limitations that should be pointed out as follows. First, this case-control study was hospital-based, therefore the selection bias is inevitable. Second, this study did not analyze the relationship between blood glucose levels and ApoE subtypes in diabetic patients. Third, in addition to the indicators included in this study, other patients’ lifestyle habits and environmental factors that may be related to the development of diabetes were not included in the analysis. In the future, larger sample sizes and more genetic factors will need to be included to investigate this relationship.
Conclusion
In summary, the APOE E2/E3 and E3/E4 genotypes may be risk factors for developing DM in hypertensive patients. It provides evidence that APOE gene polymorphisms are linked to the risk of DM in hypertensive patients.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
Since this study was a retrospective study and it was impossible for all subjects to return to the hospital to sign informed consent, the research procedures and objectives were informed in verbal form through telephone communication, and the consent of all subjects was obtained, which approved by the Ethics Committee of the Meizhou People’s Hospital. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital (Clearance No.: 2021-A-60).
Acknowledgments
The authors would like to thank their colleagues who were not listed in the authorship of the Department of Laboratory Medicine, Meizhou People’s Hospital, for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Meizhou (Grant No.: 2019B0202001).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bromfield S, Muntner P. High blood pressure: the leading global burden of disease risk factor and the need for worldwide prevention programs. Curr Hypertens Rep. 2013;15(3):134–136. doi:10.1007/s11906-013-0340-9
2. Pickering GW. The natural history of hypertension. Br Med Bull. 1952;8(4):305–309. doi:10.1093/oxfordjournals.bmb.a074193
3. Yin R, Yin L, Li L, et al. Hypertension in China: burdens, guidelines and policy responses: a state-of-The-art review. J Hum Hypertens. 2022;36(2):126–134. doi:10.1038/s41371-021-00570-z
4. Hedner T, Kjeldsen SE, Narkiewicz K. State of global health--hypertension burden and control. Blood Press. 2012;21 Suppl 1(sup1):1–2. doi:10.3109/08037051.2012.704786
5. Liu S, Yuan H, Jiang C, Xu J, Qiu X, Luo J. The blood pressure control and arteriosclerotic cardiovascular risk among Chinese community hypertensive patients. Sci Rep. 2021;11(1):19066. doi:10.1038/s41598-021-98745-8
6. Gregg EW, Buckley J, Ali MK, et al. Improving health outcomes of people with diabetes: target setting for the WHO Global Diabetes Compact. Lancet. 2023;401(10384):1302–1312. doi:10.1016/S0140-6736(23)00001-6
7. Conen D, Ridker PM, Mora S, Buring JE, Glynn RJ. Blood pressure and risk of developing type 2 diabetes mellitus: the Women’s Health Study. Eur Heart J. 2007;28(23):2937–2943. doi:10.1093/eurheartj/ehm400
8. Moreno B, de Faria AP, Ritter AMV, et al. Glycated hemoglobin correlates with arterial stiffness and endothelial dysfunction in patients with resistant hypertension and uncontrolled diabetes mellitus. J Clin Hypertens. 2018;20(5):910–917. doi:10.1111/jch.13293
9. Wang J, Ma JJ, Liu J, Zeng DD, Song C, Cao Z. Prevalence and risk factors of comorbidities among hypertensive patients in China. Int J Med Sci. 2017;14(3):201–212. doi:10.7150/ijms.16974
10. Singh PP, Singh M, Mastana SS. APOE distribution in world populations with new data from India and the UK. Ann Hum Biol. 2006;33(3):279–308. doi:10.1080/03014460600594513
11. Alidu H, Dapare PPM, Quaye L. Insulin resistance in relation to hypertension and dyslipidaemia among men clinically diagnosed with type 2 diabetes. Biomed Res Int. 2023;2023:8873226. doi:10.1155/2023/8873226
12. Marais AD. Apolipoprotein E in lipoprotein metabolism, health and cardiovascular disease. Pathology. 2019;51(2):165–176. doi:10.1016/j.pathol.2018.11.002
13. Khalil YA, Rabès JP, Boileau C, Varret M. APOE gene variants in primary dyslipidemia. Atherosclerosis. 2021;328:11–22. doi:10.1016/j.atherosclerosis.2021.05.007
14. Seripa D, D’Onofrio G, Panza F, Cascavilla L, Masullo C, Pilotto A. The genetics of the human APOE polymorphism. Rejuvenation Res. 2011;14(5):491–500. doi:10.1089/rej.2011.1169
15. Rao H, Wu H, Yu Z, Huang Q. APOE genetic polymorphism rs7412 T/T genotype may be a risk factor for essential hypertension among Hakka People in Southern China. Int J Hypertens. 2022;2022:8145896. doi:10.1155/2022/8145896
16. Zeng Y, Wen S, Huan L, Xiong L, Zhong B, Wang P. Association of ApoE gene polymorphisms with serum lipid levels and the risk of type 2 diabetes mellitus in the Chinese Han population of central China. PeerJ. 2023;11:e15226. doi:10.7717/peerj.15226
17. Niu W, Qi Y, Qian Y, Gao P, Zhu D. The relationship between apolipoprotein E epsilon2/epsilon3/epsilon4 polymorphisms and hypertension: a meta-analysis of six studies comprising 1812 cases and 1762 controls. Hypertens Res. 2009;32(12):1060–1066. doi:10.1038/hr.2009.164
18. Niu WQ, Qi Y. Meta-based evidence for apolipoprotein E epsilon2/epsilon3/epsilon4 polymorphism in association with hypertension among Chinese. J Hum Hypertens. 2011;25(12):725–731. doi:10.1038/jhh.2010.116
19. Shi J, Liu Y, Liu Y, et al. Association between ApoE polymorphism and hypertension: a meta-analysis of 28 studies including 5898 cases and 7518 controls. Gene. 2018;675:197–207. doi:10.1016/j.gene.2018.06.097
20. Chen DW, Shi JK, Li Y, Yang Y, Ren SP. Association between ApoE polymorphism and type 2 diabetes: a meta-analysis of 59 studies. Biomed Environ Sci. 2019;32(11):823–838. doi:10.3967/bes2019.104
21. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in china: results from the China Hypertension Survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
22. Benhalima K, Van Crombrugge P, Moyson C, et al. Risk factor screening for gestational diabetes mellitus based on the 2013 WHO criteria. Eur J Endocrinol. 2019;180(6):353–363. doi:10.1530/EJE-19-0117
23. Liu Q, Wu H, Yu Z, Huang Q, Zhong Z. APOE gene ɛ4 allele (388C-526C) effects on serum lipids and risk of coronary artery disease in southern Chinese Hakka population. J Clin Lab Anal. 2021;35(9):e23925. doi:10.1002/jcla.23925
24. Selby JV, Peng T, Karter AJ, et al. High rates of co-occurrence of hypertension, elevated low-density lipoprotein cholesterol, and diabetes mellitus in a large managed care population. Am J Manag Care. 2004;10(2 Pt 2):163–170. PMID: 15005509.
25. Kim MJ, Lim NK, Choi SJ, Park HY. Hypertension is an independent risk factor for type 2 diabetes: the Korean genome and epidemiology study. Hypertens Res. 2015;38(11):783–789. doi:10.1038/hr.2015.72
26. Jia G, Sowers JR. Hypertension in diabetes: an update of basic mechanisms and clinical disease. Hypertension. 2021;78(5):1197–1205. doi:10.1161/HYPERTENSIONAHA.121.17981
27. Deng H, Hu P, Li H, et al. Novel lipid indicators and the risk of type 2 diabetes mellitus among Chinese hypertensive patients: findings from the Guangzhou Heart Study. Cardiovasc Diabetol. 2022;21(1):212. doi:10.1186/s12933-022-01660-z
28. Chen Y, Ma J, Lu D, Fang Y. The risk factors of type 2 diabetes in hypertensive subjects. Front Endocrinol. 2022;13:901614. doi:10.3389/fendo.2022.901614
29. Ariyanti R, Besral B. Dyslipidemia associated with hypertension increases the risks for coronary heart disease: a case-control study in Harapan Kita Hospital, National Cardiovascular Center, Jakarta. J Lipids. 2019;2019:2517013. doi:10.1155/2019/2517013
30. Verdecchia P, Reboldi G, Angeli F, et al. Systolic and diastolic blood pressure changes in relation with myocardial infarction and stroke in patients with coronary artery disease. Hypertension. 2015;65(1):108–114. doi:10.1161/HYPERTENSIONAHA.114.04310
31. Kane JP, Pullinger CR, Goldfine ID, Malloy MJ. Dyslipidemia and diabetes mellitus: role of lipoprotein species and interrelated pathways of lipid metabolism in diabetes mellitus. Curr Opin Pharmacol. 2021;61:21–27. doi:10.1016/j.coph.2021.08.013
32. Domingo-Espín J, Nilsson O, Bernfur K, Del Giudice R, Lagerstedt JO. Site-specific glycations of apolipoprotein A-I lead to differentiated functional effects on lipid-binding and on glucose metabolism. Biochim Biophys Acta Mol Basis Dis. 2018;1864(9 Pt B):2822–2834. doi:10.1016/j.bbadis.2018.05.014
33. Malyala R, Rapi L, Nash MM, Prasad GVR. Serum apolipoprotein B and A1 concentrations predict late-onset posttransplant diabetes mellitus in prevalent adult kidney transplant recipients. Can J Kidney Health Dis. 2019;6:2054358119850536. doi:10.1177/2054358119850536
34. Baszczuk A, Musialik K, Kopczyński J, et al. Hyperhomocysteinemia, lipid and lipoprotein disturbances in patients with primary hypertension. Adv Med Sci. 2014;59(1):68–73. doi:10.1016/j.advms.2013.08.001
35. Seo JY, Youn BJ, Cheong HS, Shin HD. Association of APOE genotype with lipid profiles and type 2 diabetes mellitus in a Korean population. Genes Genomics. 2021;43(7):725–735. doi:10.1007/s13258-021-01095-y
36. Liu L, Shen G, Huang JY, et al. U-shaped association between low-density lipid cholesterol and diabetes mellitus in patients with hypertension. Lipids Health Dis. 2019;18(1):163. doi:10.1186/s12944-019-1105-5
37. Wu L, Zhang Y, Zhao H, et al. Dissecting the association of apolipoprotein e gene polymorphisms with type 2 diabetes mellitus and coronary artery disease. Front Endocrinol. 2022;13:838547. doi:10.3389/fendo.2022.838547
38. Gao C, Fu X, Chu Q, Li J, Shu G. Relationship between the apoe gene polymorphism and type 2 diabetes mellitus complications. Genet Test Mol Biomarkers. 2021;25(2):111–115. doi:10.1089/gtmb.2020.0130
39. Srirojnopkun C, Kietrungwilaikul K, Boonsong K, Thongpoonkaew J, Jeenduang N. Association of APOE and CETP TaqIB polymorphisms with type 2 diabetes mellitus. Arch Med Res. 2018;49(7):479–485. doi:10.1016/j.arcmed.2019.02.005
40. Pitchika A, Markus MRP, Schipf S, et al. Longitudinal association of Apolipoprotein E polymorphism with lipid profile, type 2 diabetes and metabolic syndrome: results from a 15 year follow-up study. Diabetes Res Clin Pract. 2022;185:109778. doi:10.1016/j.diabres.2022.109778
41. Galal AA, Abd Elmajeed AA, Elbaz RA, Wafa AM, Elshazli RM. Association of Apolipoprotein E gene polymorphism with the risk of T2DM and obesity among Egyptian subjects. Gene. 2021;769:145223. doi:10.1016/j.gene.2020.145223
42. Santos-Ferreira C, Baptista R, Oliveira-Santos M, Costa R, Pereira Moura J, Gonçalves L. Apolipoprotein E2 genotype is associated with a 2-fold increase in the incidence of type 2 diabetes mellitus: results from a long-term observational study. J Lipids. 2019;2019:1698610. doi:10.1155/2019/1698610
43. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
44. Yousef H, Khandoker AH, Feng SF, Helf C, Jelinek HF. Inflammation, oxidative stress and mitochondrial dysfunction in the progression of type II diabetes mellitus with coexisting hypertension. Front Endocrinol. 2023;14:1173402. doi:10.3389/fendo.2023.1173402
45. Yvan-Charvet L, Pagler T, Gautier EL, et al. ATP-binding cassette transporters and HDL suppress hematopoietic stem cell proliferation. Science. 2010;328(5986):1689–1693. doi:10.1126/science.1189731
46. Murphy AJ, Akhtari M, Tolani S, et al. ApoE regulates hematopoietic stem cell proliferation, monocytosis, and monocyte accumulation in atherosclerotic lesions in mice. J Clin Invest. 2011;121(10):4138–4149. doi:10.1172/JCI57559
47. Koren-Iton A, Salomon-Zimri S, Smolar A, Shavit-Stein E. Central and peripheral mechanisms in ApoE4-driven diabetic pathology. Int J Mol Sci. 2020;21(4):1289. doi:10.3390/ijms21041289
48. Shi LJ, Tang X, He J, Shi W. Genetic evidence for a causal relationship between hyperlipidemia and type 2 diabetes in mice. Int J Mol Sci. 2022;23(11):6184. doi:10.3390/ijms23116184
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.