Back to Journals » Journal of Pain Research » Volume 18
Dynamic Ultrasound Quantification of Acupuncture-Induced Multifidus Recovery in Lumbar Disc Herniation
Authors Zhang J, Xu J, Wu Q ![]() , Yi X
, Yi X
Received 11 September 2025
Accepted for publication 12 December 2025
Published 19 December 2025 Volume 2025:18 Pages 6921—6929
DOI https://doi.org/10.2147/JPR.S566903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Junfeng Zhang,1,* Jingjing Xu,2,* Qiong Wu,3 Xiaolei Yi3
1Department of Acupuncture, Tuina and Traumatology, Shanghai Sixth People’s Hospital, Shanghai, People’s Republic of China; 2Department of Traditional Chinese Medicine (TCM) Rehabilitation, Nanxiang Town Community Health Service Center, Shanghai, People’s Republic of China; 3Department of Ultrasound in Medicine, Shanghai Sixth People’s Hospital, Shanghai Institute of Ultrasound in Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiong Wu, Email [email protected] Xiaolei Yi, Email [email protected]
Objective: To validate musculoskeletal ultrasound for quantifying real-time morphological changes in multifidus muscles during acupuncture treatment of lumbar disc herniation (LDH).
Methods: Sixty LDH patients received Qi-needling at BL40. Morphological parameters (cross-sectional area [CSA], multifidus muscle thickness [MMT], muscle activation rate [MAR]) were assessed via ultrasound in resting/shrinkage states. Clinical outcomes included Visual Analog Scale (VAS), Japanese Orthopaedic Association (JOA) scores, and infrared thermography of lumbar temperature.
Results: Quantitative ultrasound revealed significant post-acupuncture improvements in multifidus morphology: After acupuncture, CSA at resting-state increased to 251.88mm2 from 190.66mm2, and to 305.28mm2 from 219.22mm2 at shrinkage-state, and MMT at resting-state increased to 11.50mm from 9.15mm, and to 14.04mm from 10.77mm at shrinkage-state. Both results show a significant increase compared to the initial state (P< 0.05). While MAR increased from 18.28% to 22.79% with a statistically significant difference (P< 0.05). Clinically, VAS scores significantly decreased after treatment, dropping from 6.35 to 1.15, while JOA scores increased from 11.77 to 20.62 (P< 0.05). Infrared thermography detected a 1.23°C rise in lumbar temperature (31.09 ± 0.95°C to 32.32 ± 0.85°C, P < 0.05).
Conclusion: Musculoskeletal ultrasound provides objective, dynamic biomarkers for evaluating acupuncture-induced multifidus recovery, enabling precision rehabilitation in LDH.
Keywords: lumbar disc herniation, musculoskeletal ultrasound, acupuncture
Introduction
The multifidus muscle is widely recognized as a crucial stabilizer of the spinal joints, and its condition is often implicated in various lumbar disorders, including low back pain, lumbar disc herniation, and issues with degenerative lumbar anesthesiologists.1 Injuries to this muscle can lead to morphological changes, which may result in decreased strength, compromised function, and impaired core stability, thereby exacerbating pain.2 Therefore, it is of paramount importance to assess the morphological status of the multifidus muscle in patients suffering from low back pain to understand its potential impact on their condition and to devise appropriate treatment strategies.
The application of the QI CI method at the Weizhong acupoint (BL 40) holds significant clinical value in treating lumbar multifidus atrophy in patients with lumbar disc herniation. Traditionally, the morphology of the multifidus muscle has been assessed using imaging techniques such as Computed Tomography (CT) and Magnetic Resonance Imaging (MRI). However, CT scans involve radiation exposure, high costs, and prolonged examination times, posing challenges for repeated monitoring. Additionally, MRI may be limited by patient allergies to contrast agents. Ultrasound has emerged as a promising alternative, offering accurate and sensitive evaluation of musculoskeletal systems.3 Despite its advantages, existing studies have primarily focused on morphological and biomechanical assessments, providing limited objective data to track treatment-related changes. Further research is needed to bridge this knowledge gap and optimize clinical management.
Previous research indicates that electroacupuncture at the BL40 acupoint enhances regeneration in the early stage of multifidus muscle injury by upregulating the expression of IGF-1 and MyoD.4 Complementing this mechanism, the phosphatidylinositol 3-kinase/protein kinase B (PI3K/Akt) pathway has been shown to promote the proliferation of muscle satellite cells and facilitate myogenic differentiation.5 Together, these findings suggest that acupuncture at key acupoints can effectively regulate and promote the repair of multifidus muscle injuries. To provide imaging-based evidence for evaluating the efficacy of traditional medical interventions, this study investigated the biomechanical characteristics of the lumbar multifidus muscle in its pathological state. Utilizing musculoskeletal ultrasound, we systematically observed the morphological status of the multifidus muscle in patients with chronic low back pain undergoing QI CI treatment at the Weizhong acupoint (BL 40). The findings aim to establish an objective basis for guiding subsequent diagnostic strategies and personalized treatment plans.
Materials and Methods
Patients
This study enrolled a total of 60 patients diagnosed with lumbar disc herniation (LDH) who received treatment at the Department of Acupuncture and Traumatology, Shanghai Sixth People’s Hospital, between August 2023 and January 2024. Prior to treatment, musculoskeletal ultrasound examinations were performed to assess biomechanical parameters of the multifidus muscle, including cross-sectional area (CSA) and thickness. Additionally, clinical evaluations were conducted using the Visual Analog Scale (VAS) for pain, the Japanese Orthopaedic Association (JOA) scores, and measurements of lower lumbar temperature. Subsequently, all participants underwent standardized acupuncture therapy for two consecutive treatment cycles, targeting the lumbar Jiaji acupoints (EX-B2), Shenshu acupoint (BL23), and Yaoyangguan acupoint (DU3). Post-treatment outcomes were evaluated by comparing changes in VAS and JOA scores, lower lumbar temperature, and multifidus muscle CSA and thickness to assess the clinical efficacy of the acupuncture intervention.
Inclusion Criteria:
1. Confirmed diagnosis of lumbar disc herniation based on established medical diagnostic criteria
2. Age between 30 and 55 years
3. MRI confirmation of intervertebral disc protrusion at the L4–L5 or L5–S1 levels
4. No prior treatment received within the past month
5. Provision of signed informed consent.
Exclusion Criteria:
1. History of surgical intervention for lumbar disc herniation
2. Low back pain resulting from lumbar compression fractures, spinal stenosis, spinal tuberculosis, or tumors
3. Presence of severe systemic diseases, coagulation disorders, or pregnancy/lactation
4. Low back pain attributable to other internal medical conditions
5. Participation in other concurrent clinical trials.
Ultrasound Examination
During the initial resting state, the patient is positioned in a prone position with face downward, maintaining normal quiet breathing. Arms are placed alongside the body to relax the back muscles. Mark the L5 spinous process with a marker pen, using the L5 lamina as the bony landmark to ensure precise probe placement and accurate anterior-posterior positioning. Imaging is performed using a Mindray M9 equipped with an L-9 probe. The probe is initially aligned longitudinally at a 90-degree angle to confirm proper orientation. Subsequently, rotate the probe transversely and perform lateral sweeps to image the lateral multifidus muscles of the lumbar region (left or right side). Three ultrasound images are captured and stored for each anatomical location. Finally, instruct the patient to abduct their arms laterally while maintaining quiet breathing. Repeat imaging acquisition using the same technique during shrinkage state to capture dynamic muscle activation patterns.6
All image acquisition and data measurement were performed by the same physician with over ten years of experience. The examiner strictly followed the relevant operating standards to obtain the best ultrasound images.
Clinical Outcomes
JOA scores and VAS were documented before and after the treatment.7,8
(1) The JOA score evaluates the degree of lumbar functional impairment across several dimensions, encompassing subjective symptoms, clinical signs, and restrictions in daily living activities.
(2) The VAS pain index ranges from 0 to 10 points, with a higher score indicating more severe pain and vice versa.
Infrared Thermal Imaging of the Waist: Temperature Difference Analysis
Using an uncooled focal plane infrared thermal image (Fluke Ti480Pro), the room temperature is 25.0 °C, humidity is 60%, and there is no convection or direct sunlight shining on the observation area. After exposing the patient’s waist for 15 minutes, an examination will be conducted about lm away from the thermal image. The infrared thermal image temperature of the waist before treatment will be recorded with the Yaoyangguan point as the center. After the end of the treatment course, the needle will be taken and recorded once, which will be recorded as the temperature value of the first treatment course. After the last treatment, the temperature value of the last treatment will be recorded immediately, and the temperature difference before and after treatment will be analyzed. The corresponding colors of the temperature in the thermal image from high to low are dark red, red, light red, yellow, green, light blue, deep blue, and black in sequence.
Acupuncture Procedure
(1) Patient Positioning & Site Preparation: The patient was placed in the prone position. Acupoints on the affected side were selected and routinely disinfected using 75% alcohol cotton balls.
(2) Needle Specifications: A sterile filiform needle (0.30 mm diameter × 40 mm length; Gushiyuan Medical Instrument Co., Ltd., China) was used.
(3) Needle Insertion & Manipulation:
- Lumbar Points (BL23, DU3, EX-B2 at L3, L4, L5 levels): Needles were inserted perpendicularly using the finger-press method to a depth of 1.2 cun. Upon obtaining de qi, even reinforcing-reducing manipulation was applied.
- BL40 (Weizhong): The needle was inserted obliquely to a depth of 1.2 cun. After achieving de qi via needle rotation, the tip was slightly withdrawn and angled superiorly. A qi-guiding technique was applied for 30 seconds to propagate the sensation towards the buttocks or lower back, eliciting mild contraction of the lumbar and back muscles.
- Points 0.5 cm Lateral to BL40: Needles were inserted obliquely towards the center of BL40 bilaterally. The needle was slowly inserted and gently twisted to obtain DE qi, then retained for 15 minutes.
(4) Treatment Protocol: Treatments were administered every other day. Ten sessions constituted one treatment course. A total of two courses were completed, with a 7-day interval between courses.
(5) Post-Treatment Evaluation: Following the acupuncture treatment, the patient was re-evaluated using identical assessment parameters.
Statistical Methods
Statistical analyses were performed using SPSS 23.0 software. Continuous count data are presented as mean ± standard deviation. Changes in the cross-sectional area (CSA) and thickness of the multifidus muscle, measured via ultrasound in different positions before and after treatment, were analyzed using two-way analysis of variance (ANOVA).
Paired sample t-tests were used to analyze differences in the JOA Score and VAS before versus after treatment. Similarly, paired sample t-tests were employed to evaluate pre- to post-treatment changes in lower lumbar temperature levels measured by infrared thermography. In all cases, two-tailed P values lower than 0.05 indicated a statistically significant difference.
Results
The study was completed by 60 participants (26 men and 34 women) with a mean age of 39.08 ± 12.20 years, a mean BMI of 22.96 ± 2.70 kg/m2, and a mean symptom duration of 4.78 ± 4.03 years. Among them, 26 presented with unilateral low back pain on the left side and 34 on the right, and the patient’s baseline stratification data (using the Pfirrmann disc degeneration grading system) was shown in Table 1.
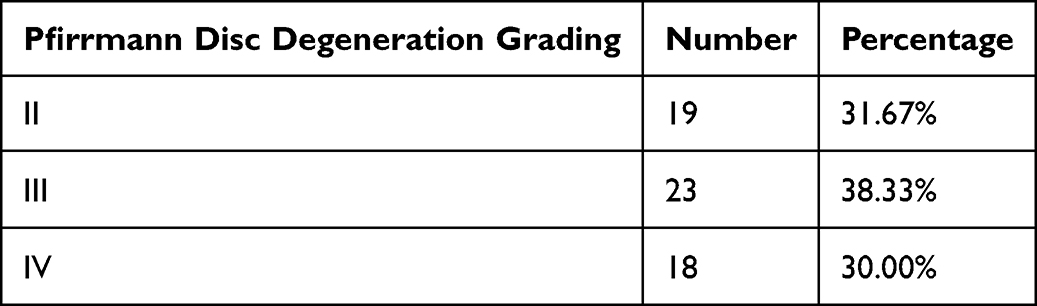 |
Table 1 The Patient’s Baseline Stratification Data |
(1) Changes in multifidus muscle morphometric parameters (affected side) pre-treatment (musculoskeletal ultrasound):
Before treatment, the CSA of the multifidus muscle on the affected side at rest was 190.66 mm2. During muscle contraction induced by changes in body position, the CSA increased to 219.22 mm2, indicating a physiological response to contraction. Following acupuncture treatment, the resting CSA of the multifidus muscle increased to 251.88 mm2, and during contraction, it further increased to 305.28 mm2, both representing significant improvements compared to pre-treatment measurements (Table 2 and Figures 1 and 2).
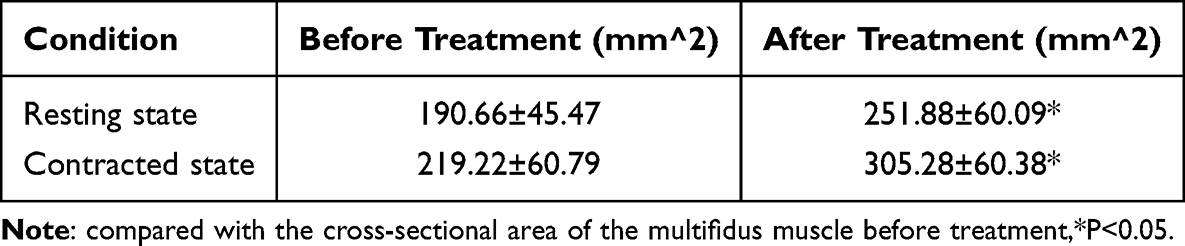 |
Table 2 Comparison of CSA of the Multifidus Muscle on the Affected Side in Different Body Positions Before and After Treatment |
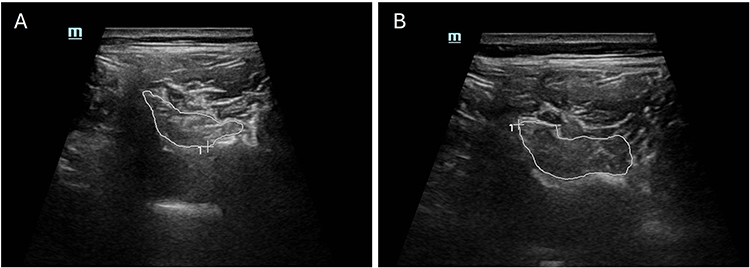 |
Figure 1 The morphology of the multifidus muscle was traced with a white brush under ultrasound, and its CSA was calculated. (A) Multifidus muscle CSA before treatment. (B) Multifidus muscle CSA after treatment. |
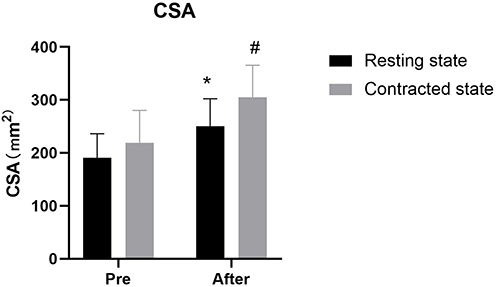 |
Figure 2 The CSA of multifidus muscle in different body positions of the affected side was compared before and after treatment. Notes: *Significant difference was found in the CSA of the multifidus muscle before and after treatment in the resting state. # Significant difference was found in the CSA of the multifidus muscle before and after treatment in the contracted state. |
(2) Evaluation of the Multifidus Muscle Thickness (MMT) and Muscle Activation Rate(MAR) on the Affected Side Before and After Treatment Using Musculoskeletal Ultrasound:
The MMT on the affected side was 9.15mm at resting state, and 10.77mm at contracted state before treatment.
After acupuncture treatment, the MMT at resting-state increased to 11.50mm, and 14.04mm at contracted state. Both results show a significant increase compared to the initial state.
The results presented in the table indicate that after treatment, the MAR of the multifidus muscle on the affected side increased from 18.28% to 22.79%,which significantly increased in MAR after treatment (P<0.05) (Table 3 and Figure 3).
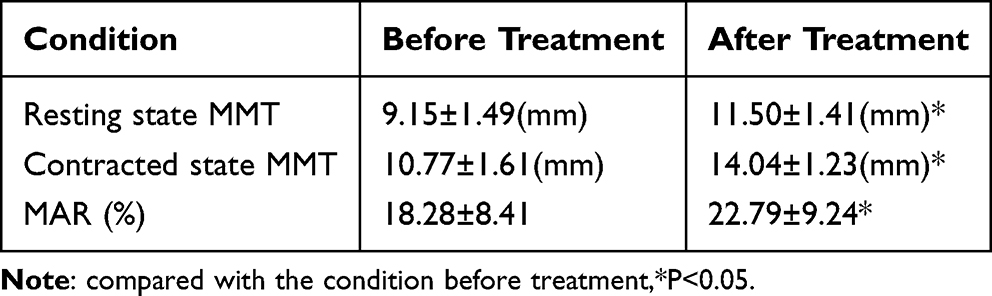 |
Table 3 Comparison of MMT and MAR on the Affected Side Before and After Treatment |
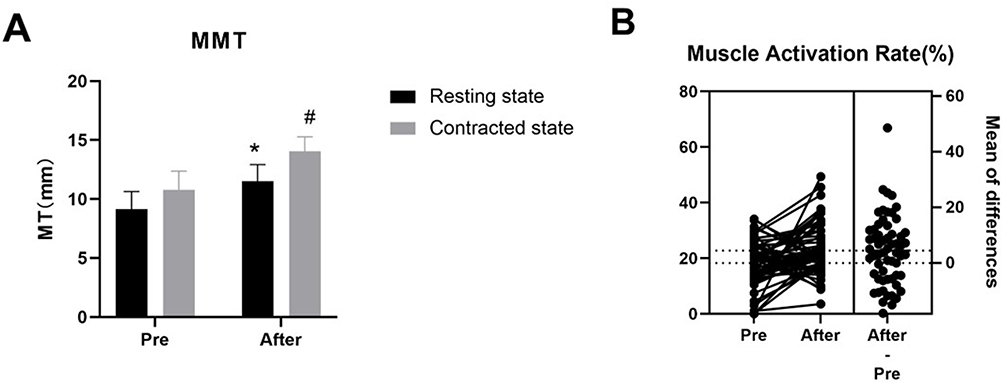 |
Figure 3 The MMT and MAR in different positions of the affected side. (A) * Significant difference was found in the MMT before and after treatment in the resting state. # Significant difference was found in the MMT before and after treatment in the contracted state. (B) Significant difference was found in the mean value of MAR before and after acupuncture treatment. The mean value after treatment increased by 12.31% compared with pre-treatment (95% confidence interval: 1.73 to 7.70). |
Muscle activation rate9 = (Thickness at contracted state- Thickness at resting-state) / Thickness at resting-state * 100%
(3) Lumbar function was evaluated using the Japanese Orthopaedic Association (JOA) scores, and pain intensity was assessed with the Visual Analog Scale (VAS) before and after treatment. Changes in lower lumbar temperature were monitored using infrared thermography. Following treatment, the VAS score decreased significantly from 6.35 to 1.15, and JOA scores increased from 11.77 to 20.62. Additionally, the lower lumbar temperature rose from 31.09°C to 32.32°C. All observed differences before and after treatment were statistically significant (P < 0.05) (Table 4 and Figures 4 and 5).
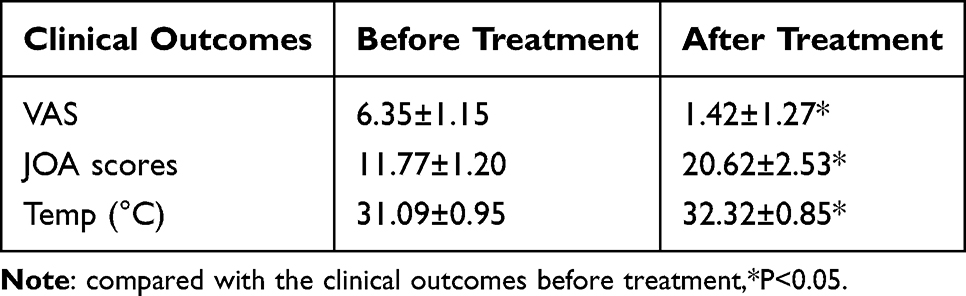 |
Table 4 Comparison of VAS, JOA Scores and Temperature of LDH Patients Before and After Treatment |
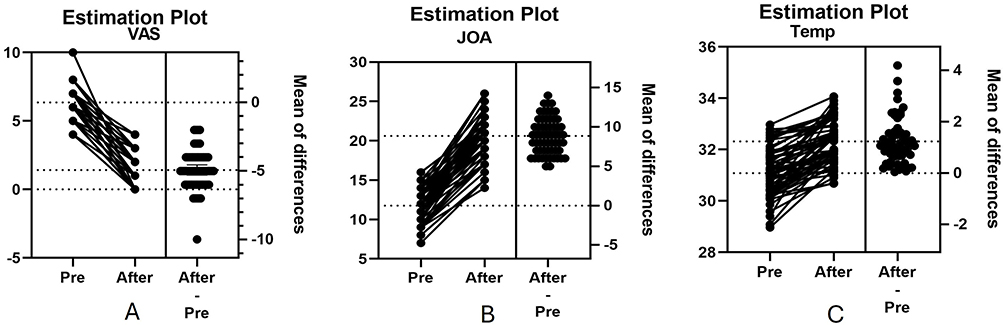 |
Figure 4 VAS, JOA score and temperature of LDH patients. (A) Significant difference was found in the mean value of VAS score before and after acupuncture treatment, and the mean VAS decreased by 4.933 (95% confidence interval: −5.307 to −4.559). (B) Significant difference was found in the mean value of JOA score before and after acupuncture treatment, and the mean JOA increased by 8.850 (95% confidence interval: 8.260 to 9.440). (C) Significant difference was found in the mean value of temperature of Yaoyangguan (GV3) before and after acupuncture treatment, and the mean temperature of GV3 increased by 1.230 (95% confidence interval: 0.9988 to 1.461). |
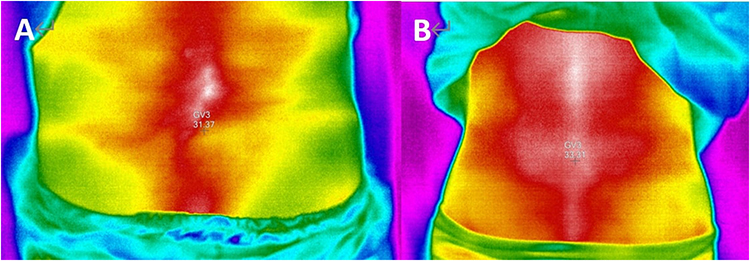 |
Figure 5 Infrared thermography of Yaoyangguan acupoint (GV3). (A) before-treatment (31.37°C). (B) after treatment (33.31°C). |
Discussion
The lumbar multifidus muscle, intrinsic to spinal stability, spans the lumbar spine and sacrum. Previous studies have shown that various lumbar disorders such as lumbar disc herniation, chronic low back pain, and degenerative spondylolisthesis are strongly associated with bio-mechanical changes and pathological morphological characteristics of the lumbar multifidus muscle.10,11 Observations of the multifidus muscle using magnetic resonance imaging (MRI) in subjects of different age groups revealed that with increasing age, the muscle begins to gradually atrophy and inter muscular gaps gradually appear, exhibiting significant age-related degenerative changes.12 Chua et al retrospectively analyzed case data of patients who underwent minimally invasive decompression surgery for lumbar spinal stenosis, showing that postoperative patients had varying degrees of atrophy and fatty infiltration in the multifidus muscle, leading to dysfunction in lumbar motion.13 Ogon et al used MRI spectroscopy to analyze the fat content in the multifidus muscle of patients with chronic low back pain, and the results showed a significant increase in intramuscular lipid levels.14 The pathological morphological changes of the lumbar multifidus muscle can easily lead to muscle atrophy.15 Critically, extensive research supports a correlation between multifidus atrophy and the development of chronic low back pain. Consequently, evaluating multifidus morphology state in patients with low back pain provides a valuable biomarker for assessing therapeutic efficacy during both treatment and rehabilitation.
BL 40 (Kunlun) is an acupoint located on the Foot Taiyang Bladder Meridian. Stimulation at BL 40 has been shown to reduce apoptosis in lumbar muscle cells, enhance sarcoplasmic reticulum function, and improve local blood circulation; While focusing on spinal cord injury, the work of Choi et al sheds light on a potential anti-inflammatory pathway through which acupuncture promotes functional recovery, a mechanism that could be applicable to multifidus muscle repair.16 More directly, Sarafraz et al utilized ultrasound imaging to show that acupuncture significantly improves the functional status of the multifidus muscle in patients with lumbar disc herniation, lending direct empirical support to the role of BL40 in this process.17 However, evaluating the therapeutic effect of interventions targeting the multifidus muscle presents challenges due to its complex morphology. Currently, there is a lack of convenient and cost-effective imaging-based methods for this specific assessment. Clinical evaluation of paraspinal muscles in patients with low back pain primarily relies on modalities such as computed tomography (CT) and magnetic resonance imaging (MRI). The widespread application of these techniques is limited by factors such as high cost and, in the case of CT, ionizing radiation exposure. Conversely, ultrasonography offers significant advantages for musculoskeletal examination, including high accuracy, sensitivity, and the ability to assess biomechanical parameters dynamically. Consequently, ultrasound holds considerable promise as a practical modality for evaluating multifidus muscle morphology. Its implementation could provide a valuable diagnostic basis for managing low back pain and objectively assessing treatment efficacy.17
Özcan-Eksi et al18 identified significant bilateral asymmetry in morphological and mechanical parameters of the multifidus muscle within the same spinal segment of individual patients. This asymmetric atrophy of the lumbar multifidus is closely associated with intervertebral joint displacement in patients with low back pain.19 Such displacement places the multifidus muscle on the affected side under abnormal passive stretch, initially causing localized edema. Prolonged passive stretch leads to muscle dysfunction. Conversely, the contralateral muscle, subjected to chronic disuse, undergoes atrophy. Supporting this, Miki et al documented atrophy in the cross-sectional area (CSA) of the lumbar multifidus muscle specifically at levels corresponding to L4-L5 disc degeneration.20
Chan et al21 demonstrated the dynamic nature of the lumbar multifidus using musculoskeletal ultrasound in healthy adults, showing its biomechanical parameters change with posture. For instance, multifidus CSA increased from 190.66 mm2 at rest to 219.22 mm2 during postural change, reflecting muscle contraction. This underscores ultrasound’s value in evaluating multifidus morphology and its critical role in postural balance, where biomechanical parameters adapt dynamically.
Following acupuncture treatment at BL 40 (Kunlun), significant improvements were observed in multifidus muscle parameters on the affected side: CSA: Increased from 190.66 mm2 to 251.88 mm2 at rest and from 219.22 mm2 to 305.28 mm2 during contraction (P<0.05 for both). Muscle Thickness (MMT): Increased from 9.15 mm to 11.50 mm at rest and from 10.77 mm to 14.04 mm during contraction (P<0.05 for both). Muscle Activity Ratio (MAR): Increased from 18.28% to 22.79% (P<0.05). These findings indicate that acupuncture enhances multifidus thickness, cross-sectional area, and contractile activity (MAR), thereby improving spinal motion stability. Concomitant clinical improvements were also observed: VAS Pain Score: Decreased significantly from 6.35 to 1.15 (P<0.05). JOA Score: Increased significantly from 11.77 to 20.62 (P<0.05). Lower Lumbar Skin Temperature: Increased significantly from 31.09°C to 32.32°C (P<0.05). Acupuncture at BL40 is posited to promote Qi circulation and enhance local blood perfusion, which increases lumbar skin temperature and contributes to pain relief. These physiological effects are directly reflected in the ultrasound parameters: the improved perfusion underlies the structural restoration indicated by increases in CSA and MMT, while the enhanced neuromuscular regulation associated with Qi circulation corresponds to the functional improvement captured by the rise in the MAR. Consequently, the alleviation of clinical symptoms aligns with the coordinated recovery in both morphological and functional properties of the multifidus muscle.
This investigation has several noteworthy limitations. Firstly, the single-center design and modest cohort size may introduce selection bias and limit the generalizability of our findings. Secondly, the open-label study design without a sham-control group prevents us from discerning the specific therapeutic effects of acupuncture from potential placebo responses. From a methodological perspective, our reliance on 2D ultrasound imaging restricts comprehensive morphological assessment; future studies would benefit from employing 3D reconstruction for volumetric analysis. Furthermore, the absence of ultrasound elastography limited our ability to quantify tissue stiffness and characterize the muscle’s mechanical properties more comprehensively. Finally, future investigations could leverage artificial intelligence techniques to elucidate the complex relationships between global postural alignment, multifidus mechanical parameters, and therapeutic outcomes.
Conclusion
In summary, the lumbar multifidus muscle is essential for lumbar stability. Acupuncture stimulation at BL 40 (Kunlun) effectively mitigates multifidus atrophy in patients with lumbar disc herniation. Ultrasound imaging provides a valuable, non-invasive modality for objectively evaluating therapeutic efficacy during rehabilitation. This facilitates the development of more targeted treatment and rehabilitation strategies.
Data Sharing Statement
- The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request for 12 months. The authors do not intend to share individual deidentified participant data.
- No specific clinical trial data will be made available.
- Other study documents available: None.
- The corresponding authors will respond to valid requests and provide the study protocol immediately following the publication of this manuscript, with no predefined end date for availability.
Ethics Approval and Consent to Participate
This study has been reviewed and approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2023-106-[1]), and this randomized parallel group study was registered at www.chictr.org.cn (no. ChiCTR2300075092). All the patients signed the informed consent form. The trial was conducted in accordance with the Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests in this work.
References
1. Kassem H, Urits I, Hasoon J, et al. Images in practice: multifidus muscle dysfunction characterized by fat infiltration in a patient with chronic lumbar back pain. Pain therap. 2020;9(1):341–343. doi:10.1007/s40122-019-00141-8
2. Parkkola R, Rytökoski U, Kormano M. Magnetic resonance imaging of the discs and trunk muscles in patients with chronic low back pain and healthy control subjects. Spine. 1993;18(7):830–836. doi:10.1097/00007632-199306000-00004
3. Qiuchen H, Desheng L, Yuying Z, et al. The reliability of rehabilitative ultrasound imaging of the cross-sectional area of the lumbar multifidus muscles in the pnf pattern. J. Phys. Ther. Sc. 2014;26(10):1539–1541. doi:10.1589/jpts.26.1539
4. Peng YY, Liu T, P CY, et al. Effects of electroacupuncture at “Weizhong” (BL 40) on regeneration and morphology in rats with bupivacaine-induced multifidus muscle injury. Chin Acupuncture Moxibustion. 2016;36(3):287–294.
5. Liu T, Yu JN, Zou DH, et al. Effect of electroacupuncture serum on proliferation of cultured multifidus muscle satellite cells and expression of pax-7,myod and p-akt. Acupuncture Res. 2016;41(5):402–409.
6. Varol U, Sánchez-Jiménez E, A LEA, et al. Correlation between body composition and inter-examiner errors for assessing lumbar multifidus muscle size, shape and quality metrics with ultrasound imaging. Bioengineering. 2023;10(2):133. doi:10.3390/bioengineering10020133
7. Haro H, Ebata S, Inoue G, et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lumbar disc herniation, third edition - secondary publication. J Orthop Sci. 2022;27(1):31–78. doi:10.1016/j.jos.2021.07.028
8. B NM, Steinfeld Y, Badash S, et al. Association between type of face mask and visual analog scale scores during pain assessment. Pain Manag Nurs. 2022;23(3):370–373. doi:10.1016/j.pmn.2021.09.005
9. Ehsani F, M AA, Jaberzadeh S, et al. Ultrasound measurement of deep and superficial abdominal muscles thickness during standing postural tasks in participants with and without chronic low back pain. Manual Ther. 2016;23:98–105. doi:10.1016/j.math.2016.01.003
10. Alikemal Y, Tuba Y. The relationship between the degeneration and asymmetry of the lumbar multifidus and erector spinae muscles in patients with lumbar disc herniation with and without root compression. J Orthopaedic Surg Res. 2022;17(1):541. doi:10.1186/s13018-022-03444-3
11. Shi L, Yan B, Jiao Y, et al. Correlation between the fatty infiltration of paraspinal muscles and disc degeneration and the underlying mechanism. BMC Musculoskelet Disord. 2022;23(1):509. doi:10.1186/s12891-022-05466-8
12. Gökşen A, Kocaman H, Merve Arman G, et al. Comprehensive analysis of muscles wasting in disc herniation. J biomech. 2022;145:111391. doi:10.1016/j.jbiomech.2022.111391
13. Chua M, Hochberg U, Regev G, et al. Gender differences in multifidus fatty infiltration, sarcopenia and association with preoperative pain and functional disability in patients with lumbar spinal stenosis. Spine J. 2022;22(1):58–63. doi:10.1016/j.spinee.2021.06.007
14. Ogon I, Takebayashi T, Takashima H, et al. Multifidus muscles lipid content is associated with intervertebral disc degeneration: a quantitative magnetic resonance imaging study. Asian Spine J. 2019;13(4):601–607. doi:10.31616/asj.2018.0258
15. Padwal J, Berry DB, Hubbard JC, et al. Regional differences between superficial and deep lumbar multifidus in patients with chronic lumbar spine pathology. BMC Musculoskelet Disord. 2020;21(1). doi:10.1186/s12891-020-03791-4
16. C CD, Y LJ, Moon YJ, et al. Acupuncture-mediated inhibition of inflammation facilitates significant functional recovery after spinal cord injury. Neurobiol Dis. 2010;39(3):272–282. doi:10.1016/j.nbd.2010.04.003
17. Sarafraz H, R HM, Ayoobi Yazdi N, et al. Neuromuscular morphometric characteristics in low back pain with unilateral radiculopathy caused by disc herniation: an ultrasound imaging evaluation. Musculoskeletal Sci Pract. 2019;40:80–86. doi:10.1016/j.msksp.2019.01.016
18. E O-E-E, S EM, U TV, et al. Reciprocal relationship between multifidus and psoas at L4-L5 level in women with low back pain. Br J Neurosurg. 2021;35(2):220–228. doi:10.1080/02688697.2020.1783434
19. Özcan-Eksi EE, Börekci A, Eksi MS. Facet joint orientation/tropism could be associated with fatty infiltration in the lumbar paraspinal muscles. World Neurosurg. 2023;173:E606–E615. doi:10.1016/j.wneu.2023.02.111
20. Takahiro M, Fujita N, Hiroyuki T, et al. Associations between paraspinal muscle morphology, disc degeneration, and clinical features in patients with lumbar spinal stenosis. Progress Rehabilitation Med. 2020;5. doi:10.2490/prm.20200015
21. Chan ST, Fung PK, Ng NY, et al. Dynamic changes of elasticity, cross-sectional area, and fat infiltration of multifidus at different postures in men with chronic low back pain. Spine J. 2012;12(5):381–388. doi:10.1016/j.spinee.2011.12.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.