")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 9
Drug tendering: drug supply and shortage implications for the uptake of biosimilars
Authors Dranitsaris G, Jacobs I, Kirchhoff C, Popovian R, Shane LG
Received 20 April 2017
Accepted for publication 26 August 2017
Published 29 September 2017 Volume 2017:9 Pages 573—584
DOI https://doi.org/10.2147/CEOR.S140063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Samer Hamidi
George Dranitsaris,1 Ira Jacobs,2 Carol Kirchhoff,3 Robert Popovian,4 Lesley G Shane5
1Augmentium Pharma Consulting Inc., Toronto, ON, Canada; 2Global Medical Affairs, Pfizer Inc, New York, NY, 3Global Technology Services, Biotechnology and Aseptic Sciences Group, Pfizer Inc, Chesterfield, MO, 4US Government Relations, Pfizer Inc, Washington, DC, 5Outcomes and Evidence, Global Health and Value, Pfizer Inc, New York, NY, USA
Abstract: Due to the continued increase in global spending on health care, payers have introduced a number of programs, policies, and agreements on pharmaceutical pricing in order to control costs. While incentives to increase generic drug use have achieved significant savings, other cost-containment measures are required. Tendering is a formal procedure to purchase medications using competitive bidding for a particular contract. Although useful for cost containment, tendering can lead to decreased competition in a given market. Consequently, drug shortages can occur, resulting in changes to treatment plans to products that may have lower efficacy and/or an increased risk of adverse effects. Therefore, care must be taken to ensure that tendering does not negatively impact patient care or the health care system. A large and expanding portion of total pharmaceutical expenditure is for biologic therapies. These agents have revolutionized the treatment of many diseases, including cancer and inflammatory conditions; however, patient access to biologic drugs can be limited due to availability, insurance coverage, and cost. As branded biologic therapies reach the end of patent- and data-protection periods, biosimilars are being approved as lower-cost alternatives. Biosimilars are products that are highly similar to the originator product with no clinically meaningful differences in terms of safety, purity, or potency. As more biosimilars receive regulatory approval and adoption increases, these therapies are expected to have an impact on global health care spending and should result in overall savings. However, the use of tendering to maximize the potential benefits of biosimilars has varied across the world. Therefore, the objectives of this review are to examine the drug-tendering process and its implications on drug supply and drug shortages, as well as to describe biosimilars and how tendering may influence their uptake.
Keywords: biosimilars, drug shortages, drug supply, small-molecule drugs, tendering
Introduction
Global spending on medicines is projected to reach US$1.4 trillion by 2020, with up to 60% of this total paid by governments.1,2 For comparison, the total global spending on health care in 2018 is projected to be US$9.3 trillion, with an anticipated increase of 5.2% per year.3 A number of programs, policies, and agreements on medicine pricing and quantity have been enacted to control costs.2 For example, the Affordable Care Act in the US expands the share of pharmaceutical expenditure paid for by the government through funded and mandated programs, which are expected to command substantial discounts from list prices.1 In Japan and many European countries, incentives to increase generic use have been enacted to achieve savings; however, generics account for a large portion of current pharmaceutical expenditure. Therefore, many of the potential savings associated with their use have already been realized.1 Other cost-containment measures have been employed to limit pharmaceutical expenditure: risk-sharing programs (incorporating financial-based models and performance- or outcome-based models/contracting), price reductions, rebates, and changes in value-added tax rates on medicines, guideline-linked reimbursement, copayments, and distribution margins.4–7 In an analysis of the cost-effectiveness of different measures, internal and external reference pricing and the use of generics were considered the most useful policies.8 While changes in cost sharing have increased the use of generics, such policies may have unintended consequences. An increase in cost sharing above a certain threshold can reduce medication adherence, excessively tax vulnerable groups, and/or increase administrative cost on the collection of cost sharing, thus making cost sharing less effective and potentially leading to worsening of patient health and outcomes.8 Therefore, it is important that cost-containment measures do not reduce incentives for using effective products at a lower price.
A large and expanding portion of total pharmaceutical expenditure is for biologic therapies, with projected spending of US$200–$210 billion in 2016.9 Despite biologic therapies revolutionizing the treatment of many diseases, including a variety of cancers and inflammatory diseases, patient access to these drugs can be limited due to availability, insurance coverage, and cost.9–12 As branded biologic therapies reach the end of patent- and data-protection periods (Table 1), biosimilars are being approved as lower-cost alternatives.12 Biosimilars are “highly similar to the [approved, branded] reference product [hereafter referred to as the ‘originator’] notwithstanding minor differences in clinically inactive components” with “no clinically meaningful differences between the biological product and [originator] in terms of the safety, purity, and potency”.13 As more biosimilars receive regulatory approval and adoption increases, these therapies are expected to have an impact on total pharmaceutical expenditure and should result in overall savings.1,9 Indeed, significant savings have been reported with Zarzio®, a biosimilar filgrastim (originator product Neupogen®), with annual savings of €85 million reported across 17 EU countries in 2011.14
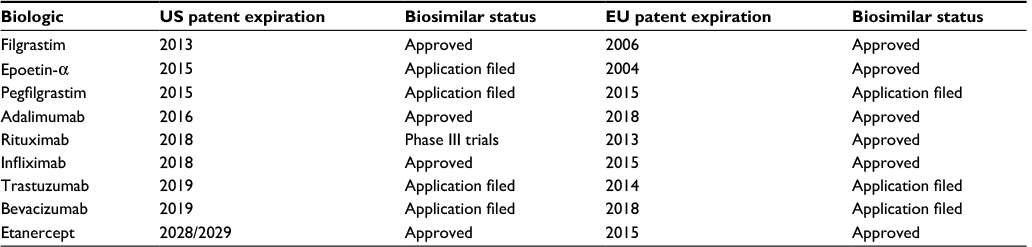 | Table 1 Patent-expiration dates of biologics and development status for some biosimilars64,86–93 Notes: Expiration dates are based on those cited within Genetic Engineering & Biotechnology News,88 although other patent dates may apply; there is no patent that specifically claims the composition of matter of cetuximab. |
This article reviews tendering and current experience with small-molecule drugs. The effect of tendering on drug manufacturers, pricing, and the quality of drugs in a given market, including the implications of drug shortages, is also discussed. Finally, an overview of biosimilars is presented, including the guidelines for biosimilar regulatory approval and the potential impact of tendering on biosimilar uptake.
Defining tendering and terms of contracts
The ultimate goal of pharmaceutical procurement is to purchase high-quality products with reliable supplier service and the lowest-possible prices.15 One method used to contain spending is tendering, a formal procedure using competitive bidding for a particular contract.15,16 Tendering is used when equivalents for a specific medicine are available, and is defined by the World Health Organization (WHO) Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies as “any formal and competitive procurement procedure through which offers are requested, received and evaluated for the procurement of goods, works or services, and as a consequence of which an award is made to the tenderer whose tender/offer is the most advantageous”.17 Tendering is a major purchasing strategy worldwide for inpatient treatments, but is only used by a few countries for outpatient pharmaceuticals.17 The tendering process for pharmaceuticals typically comprises: determining the tender format and scope; defining the requirements for the medication (including quantities); selecting the suppliers to participate in bidding; preparing and sending the documents; receiving and opening bids; collating bids for adjudication; adjudicating the tender; issuing contracts to the winning bidder(s); monitoring performance and product quality; and enforcing contract terms (as needed).15 The WHO notes that tendering should be conducted with the goal of purchasing high-quality, consistent, and effective products; therefore, the decision on which supplier(s) is awarded the contract should not be based solely on price.18 Similarly, a 2010 report from the European Parliament noted that prioritizing the lowest-cost offers over those that are the most economically advantageous can weaken innovation and global competitiveness.19
Another important consideration that may impact the quality and supply of a drug obtained through tendering systems is whether the tenders are awarded to a single entity or split among multiple suppliers.15 Single-supplier tenders are thought to provide suppliers with an incentive to offer their most competitive pricing, although there can be risk of supplier default (resulting in drug shortages), due to dependence on a single supplier.15,16,20 As a result, some procurement programs split contracts to minimize these risks.15
Tendering can also be defined by whether or not the procurement office can solicit bids from international, competitive suppliers. In some countries, policy requirements and price concessions exist to give preference to local suppliers.15 These policies and practices may not only influence the overall value (price) for a given product but also require a strong registration process to ensure that drug quality is maintained by whatever entities are awarded the tender for a particular product.15,20
Potential impact on pricing, competition, product quality, and health-system economics associated with tendering
The main methods recognized by the WHO for obtaining favorable pricing when purchasing drugs include supplier competition through open tenders, restricted tenders, or competitive negotiation.20 Direct negotiation with a single supplier is less likely to result in optimal pricing; therefore, it is recommended that this practice be limited to very small or emergency purchases.20 Open tendering, which does not require prequalification of suppliers, is most likely to result in the lowest prices, especially when many reputable suppliers are available and are likely to be interested in the contract.15 Restricted tendering can have a favorable impact on the quality of medicines and the sustainability of the market, as the process is limited to those suppliers registered with the appropriate authorities and/or who have qualified based on past performance and demonstration of product quality, thereby keeping unqualified suppliers out of the process.15 Competitive negotiation may result in favorable pricing, and is employed when select suppliers are involved, in emergency situations, or when special terms or restrictions are required.15
Tendering has several positive impacts on pricing. The tendering process is designed to select the most cost-efficient supplier(s) of a particular product.15 Therefore, tendering may achieve important savings when the purchasing power of the procurement office is high and there are several potential suppliers for similar products.21 Short-term savings in pharmaceutical costs due to the use of tendering have been reported.22 A qualitative analysis of tendering in 18 European countries indicated most of the countries had positive experiences with tendering in hospital settings through lower prices for purchasers.23 In Denmark, Germany, and the Netherlands, significant price reductions associated with tendering have been reported.23 For example, in the Netherlands, the introduction of the preference policy in 2008 resulted in close to an 85% reduction compared with the pre-preference policy price. Prices continued to decline to 2012 and averaged a 94% reduction compared with the pre-preference policy price.23 In Germany, there is no publication of rebates or winning prices; however, rebate contracts appear to be the preferred way of procuring generic medicines. Although price information is not available and may vary for the same molecule, it is believed that discounts of >90% are achieved at patent expiry. Additionally, savings from rebates have been estimated to be in the region of €1 billion and might increase further if the totality of the generics market is covered.23
Despite the positive short-term effects on pricing, long-term negative consequences have also been associated with the use of tendering. For example, the achievement of low pricing through tendering can force some manufacturers out of a given market and lead to erosion of competition, which could subsequently lead to higher prices.21,23 A recent study of drug prices in Thailand (a country that employs price negotiations, but not tendering for price control) indicated that single-source drugs had higher prices.24 Recently in the US, some generic-medicine prices increased due to several companies going out of business, owing to low profitability from reduced prices.25,26 For example, the price of digoxin increased from $0.12/tablet in July 2013 to $1.06/tablet in June 2014. Additionally, the price for divalproex sodium extended release increased from $0.27/tablet to $2.38/tablet.26 Also, unintended consequences may occur when tendering is applied to selected medications. For example, a tendering procedure was applied to simvastatin in Belgium, resulting in price reductions and savings for health care payers; however, these savings were offset by increased costs for other statins, eg, atorvastatin and rosuvastatin. Consequently, total statin expenditure increased by 6.5%.27,28
Other long-term negative economic impacts that have been associated with tendering include decreased pharmaceutical investments, resulting in loss of employment and income from taxes, as well as reductions in value-added features, such as improved packaging and programs to support patient compliance.27 Furthermore, tendering procedures can lead to slower development of innovations (to differentiate products) and competition within the generic medicine market.23,25 A robust generic medicine market stimulates originator drug development and life-cycle management, due to the need to replace income lost from losing exclusivity.25 The use of generics allows the addition of more expensive medicines to treatment paradigms while containing costs, leading to savings in health care system pharmaceutical budgets.25 Additionally, innovation in generic medicines includes addressing patient and pharmacist needs to differentiate one generic from another, which could facilitate patient compliance and use of medication through packaging, drug-delivery systems, and devices that are easier to use or understand.25
The requirement for limiting tenders to local or national companies to support economic development can be a challenge to ensure that pharmaceuticals achieve the intended and expected treatment outcomes through meeting sufficiently stringent quality-assurance standards.15,29 In addition, the globalization of pharmaceutical markets has made it more difficult to ensure the quality of imported products.29 For example, while open tendering may increase the number of potential suppliers, complications and delays can often occur post-qualification. The success of open tenders post-qualification depends on the capacity of the procurement program to winnow out unqualified suppliers and poor-quality products after bids have been received; in some cases, from all over the world.15 If routine or “by exception” laboratory testing of products after shipment results in unacceptable failure rates, the supplier should be removed from future tenders.15 While the US Food and Drug Administration (FDA) and other health authorities have tried to harmonize pharmaceutical standards, the failure to establish sufficiently stringent criteria during the tendering process (for qualified suppliers or after tenders have been awarded) could result in products with substandard quality reaching the market.15
In Europe, the EU Public Procurement (EPP) Directive enacted in 2016 outlines general rules governing procurement of supplies (including medicines and medical devices), work, or services by public authorities in EU member states, and awards tenders based on the “most economically advantageous tender” (MEAT).30 The MEAT may include a best price:quality ratio, which enables the contracting authority to take the following factors beyond price into account: qualitative, technical, aesthetic and functional characteristics of the product; accessibility; social, environmental, and innovative characteristics; total life-cycle benefit; trading and delivery conditions; and after-sales service.30 When deemed appropriate to encourage greater quality, the EPP permits any of the 28 EU member states to prohibit or restrict the use of price-only or cost-only criteria when defining the MEAT.30 The European Association for Bioindustries (EuropaBio) considers inclusion of the best price:quality ratio in MEAT the first step toward full inclusion of quality criteria in public procurement.31 Many European countries use public procurement for the provision of medicines, and particularly in hospital settings. National health care systems vary greatly across EU member states, and thus public procurement of medicines, including biosimilars, will also differ considerably across national jurisdictions. These range from largely public-funded health care bodies, such as the National Health Service in the UK, to highly privatized hospitals in countries such as Italy and Cyprus.31
Potential for drug shortages and recalls
A drug shortage is a shortcoming in the supply of a medicinal product that means it is impossible to meet current or projected demand at the patient level.32,33 Drug shortages can cause significant economic and clinical effects at all levels of the health care system, including for patients, pharmacists, clinicians, the pharmaceutical industry, and policy makers.34 Areas of impact include the preparation or dispensing of a drug, patient care through the use of alternative treatments, and overall increased workload to manage the shortage.32,35,36 Of utmost importance, patient care can be severely affected by the lack of drugs or inferior treatment options, eg, alternative options may be prescribed even though there is greater risk of disease progression and/or adverse effects (including death) or increased chance of medication errors and/or decreased compliance.32,35 Additionally, drug shortages can compromise or delay medical procedures or result in medication errors.35,37–40 The Association of Community Cancer Centers issued a statement noting that reductions in production and shortages of critical oncology drugs can create serious implications, such as forcing oncologists to alter or forgo critical treatment regimens.41 In the US and Europe, there have been a number of notable incidents of drug shortages for oncology medications resulting in patients experiencing interruptions or delays to their treatment schedules.34,39,40 In one case, physicians were surveyed afterward, and reported that the alternative regimen had inferior efficacy in 30.4% of cases and greater toxicity in 34.8% of cases compared with the unavailable medication.40 Additionally, there is greater risk of medication errors when clinicians need to treat patients with an unfamiliar or less common alternative therapy. Two patients died when hydromorphone was substituted for morphine because clinicians were unaware of the differences in potency.35,38 In another case, methohexital was substituted for propofol, and one patient fatally overdosed due to an improper dilution.35,38
In recent years, the number of product recalls in some product categories, such as sterile injectables (particularly injectable oncology drugs), has increased.42 The presence of foreign visible or subvisible particulate matter in injectable/parenteral formulations is one of the most common reasons for product recalls.43 Between 2008 and 2012, the FDA reported that 22% of recalls for sterile injectable drugs were due to the presence of visible particles.43 Other reasons were lack of sterility assurance (22%), impurities/degradation (9%), and “other” (47%), such as crystallization and discoloration.44,45 Furthermore, complex manufacturing processes mean that sterile injectables are particularly vulnerable to drug shortages; indeed, in 2010, the most common reasons for injectable-medication shortages were product-quality issues leading to recall or cessation of production.39 While quality/manufacturing issues are a major reason for these shortages, other reasons include production delays at the manufacturer, delays in receiving raw materials and components, and product discontinuations.46 This suggests that there may be a greater risk of supply disruption for products that are more specialized in manufacturing, have fewer manufacturers, have limited production capacity, and/or have longer lead times. Therefore, there may be implications for biologic therapies.
Because suppliers may leave tendered markets due to low pricing, reduced competition associated with tendering has the potential to lead to drug-supply shortages.22,32 There have been a number of reports of drug shortages in various markets and across various drug classes.32,47 Canada has experienced drug shortages of specialized medications, which have been linked to the consolidation of manufacturers to a single supplier.48 Similarly, the European Association of Hospital Pharmacists reported in 2013 that over half of medicine shortages (52.4%) were related to having a limited number of suppliers.49 In Germany, tendering caused a shift in the market from larger to smaller pharmaceutical manufacturers, which has been associated with reports of short-term shortages of medicine.23 This led German pharmacists to criticize the discount contracting system and to increase pressure on lawmakers to prioritize measures to mitigate the supply shortages.50
The European Federation of Pharmaceutical Industries and Associations has reported that many European countries, including the UK, France, Italy, Spain, Portugal, Greece, Poland, the Czech Republic, Hungary, Romania, and Slovakia, have felt compelled to take action in the last few years.51 For example, in 2014, Greece moved from a single supplier to a three-supplier model for hospital procurement, as the previous model had resulted in significant shortages.52 The adapted procurement mechanisms allowed for a greater number and diversity of suppliers to mitigate their risk of shortages.52 However, in more recent years, it is important to note that other factors, including economic and political factors, have contributed to drug shortages in Greece.53–56 Additionally, France became the first country to introduce legal obligations and sanctions for pharmaceutical companies and pharmacy wholesalers to fight against drug shortages.57 Measures include: the identification of major therapeutic-interest drugs or classes of drugs for which shortage-management plans must be prepared; the requirement for pharmaceutical companies to develop and implement these shortage-management plans; if there are major therapeutic-interest drugs in shortage or in potential shortage outside of France, then wholesalers cannot sell them to wholesale distributors for drug export; and in the case of a breach of an obligation, pharmaceutical companies may be administratively and financially sanctioned.57
Drug shortages have been associated with several economic factors, including the stoppage of drug production for economic reasons.32 In the US, drug shortages have become more frequent and have been linked to the consolidation of manufacturers. This has resulted in a reduction of products, leaving only a few manufacturers for older, less profitable products, which are often maintained in lower inventories.39,58 In the Netherlands, the number and average duration of reported drug shortages increased from 2004 to 2011; the majority (69%) of the longer shortages were due to economic factors.59 In Europe, economic causes (eg, reduced profitability and market attractiveness) behind drug shortages are generally not reported, because this can lead to a negative perception about the marketing-authorization holder.32 A reduction in the number of manufacturers in a market, whether it is due to consolidation or awarding of single-source tenders, can limit the ability to redistribute or increase supplies, eg, as a consequence of increased demand or to cover manufacturing or supply issues experienced by the main supplier.15,16
Tendering can also be associated with drug shortages through shifts in demand for certain drugs. Consolidation of generic-drug buyers and the use of group-purchasing and procurement programs have led to changes in purchasing patterns that can have an impact on distribution and inventories.39,58 Unforeseen and unexpected increases in demand (eg, due to disease outbreaks), changes in clinical practice, and parallel trade can also be associated with drug shortages.22 In addition, should issues arise with production or distribution when single-source tendering is used, the ability for another manufacturer to step in is eliminated.48 Splitting tender awards allows the maintenance of drug-supply capacity and adequate competition, while avoiding dependence on a single supplier.15 However, while this secures the drug supply, it may undercut the level of savings associated with tendering, because the economy of scale is usually reduced and bidders may not necessarily offer the lowest prices.15,48
Biosimilars
As more branded biologic therapies reach the end of patent- and data-protection periods, biosimilars are being developed and approved for use. Biosimilars are not considered generics of biologic drugs.13,60,61 The recommendation for regulatory approval is based on the “totality of the evidence”, and includes a comprehensive data package from all stages of development (analytical, nonclinical, and clinical similarity assessment) that demonstrates biosimilarity to the originator biologic product.13,60,61 As with all biologic products, postmarketing pharmacovigilance is critical to monitor the safety of biosimilars.62 To date, more than 20 biosimilars have been approved by the European Medicines Agency since the development of specific recommendations for their evaluation (Table 2).60,63 The FDA approved its first biosimilar (a biosimilar to filgrastim) in 2015, and the first biosimilar monoclonal antibody (a biosimilar to infliximab) in 2016 (Table 2).64
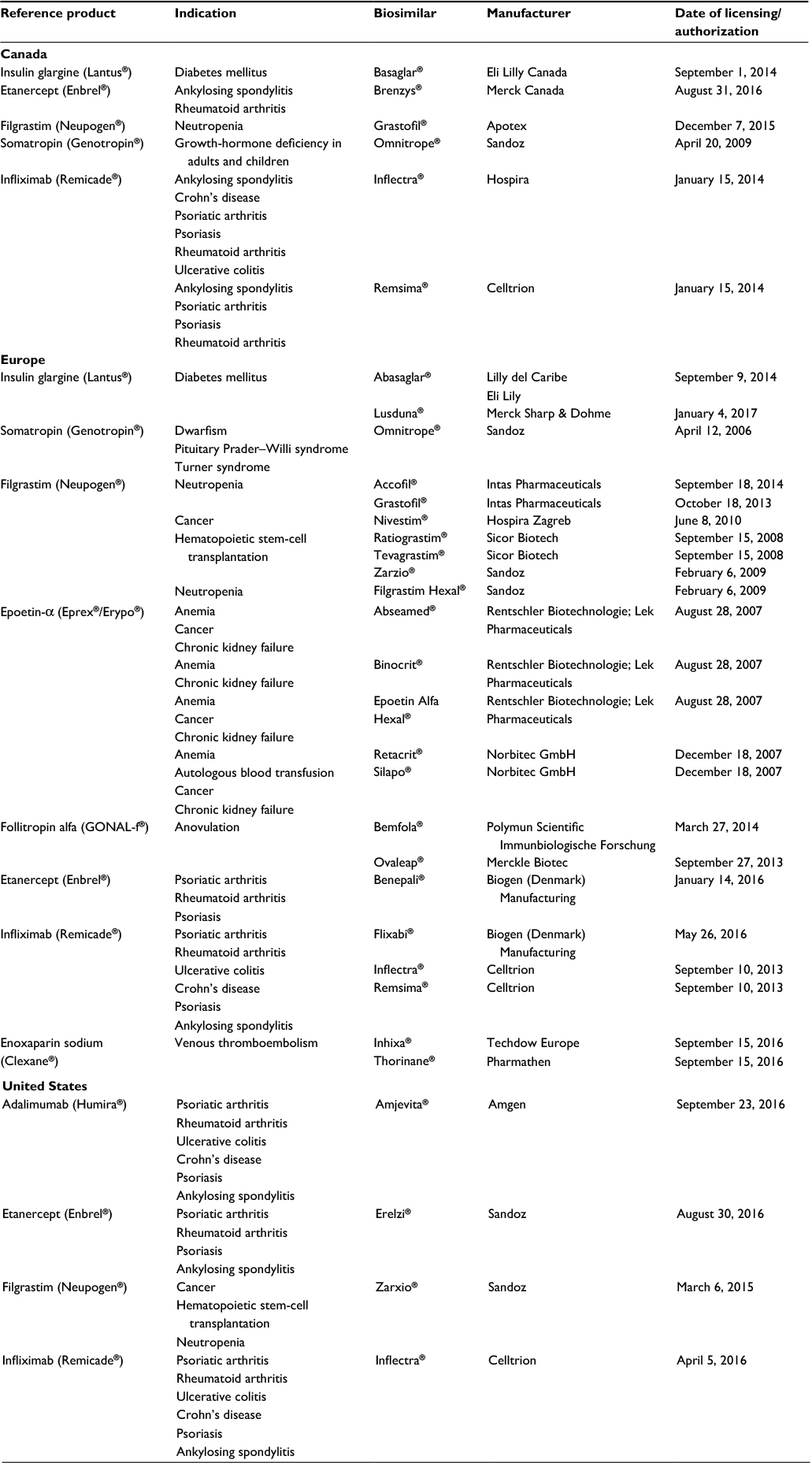 | Table 2 Biosimilar availability in Canada, Europe, and the US63,64,94 Notes: Availability as of February 28, 2017. |
Although biosimilar usage is growing rapidly in most EU countries, the uptake of biosimilars has varied considerably across the EU, mostly due to variations in incentives, distribution channels, medical practice, and the education of key stakeholders.65–72 For example, the education of physicians and implementation of measures to stimulate biosimilar prescribing has led to Germany being among the most successful countries to capitalize on the benefits of biosimilars.65–68,70–72 However, it must be highlighted that the penetration of biosimilars in Germany is very heterogeneous and depends on therapeutic class and region.66,67,70–72 Compared with other markets, the uptake of biosimilars of erythropoietin has been especially successful in Germany, and is largely due to incentives for biosimilar use.66,67 In 2014, the uptake of biosimilars of erythropoietin was 8.3%, 21.7%, 23% and 2.4% in France, Italy, Spain and the UK, respectively, compared with 32.9% in Germany.66 However, biosimilar uptake in European countries varies by product class, and the performance of a biosimilar in one product class does not necessarily predict the performance of biosimilars in other product classes. For example, the penetration rates for granulocyte colony-stimulating factor (G-CSF) biosimilars in 2014 was 12.8%, 11.8%, 25.2%, 56.8% and 40.7% in Germany, France, Italy, Spain and the UK, respectively.66 Spain, the UK, and Italy are countries with dominant hospital markets compared with France (dominant retail market) and Germany (distribution mix), thus accounting for the high uptake of G-CSF biosimilars in these countries.66 Greater acceptance of G-CSF biosimilars in Italy may also be the consequence of medical considerations and/or reimbursement policies.72 Additionally, greater G-CSF uptake compared with erythropoietin uptake in the UK may have been due to large discounts by originator erythropoietin product brands prior to biosimilar entry.72
In contrast, Austria’s mandatory price reductions have led to the exclusion of some biosimilars from their market and discouraged biosimilar competition.65,72 For example, the first biosimilar that is launched must be priced at 52% of the originator product, the second at 44%, and the third at 40%. Upon entry of the third biosimilar, the originator product and other two biosimilars must be priced at 40% of the originator’s original price.72 Additionally, due to uncertainties and a lack of confidence toward biosimilars, as well as a hospital-financing system that discourages the use of biosimilars, there has been limited uptake of biosimilars in Belgium.69 Therefore, not all stakeholders have used competition and incentives to maximize the potential benefits of biosimilars.65 In Norway, public tendering for medicines is very competitive, leading suppliers to offer substantial discounts on biosimilars (up to 50%–70% lower than the originator), resulting in significant penetration of biosimilars to the market.72,73 The Norwegian Medicines Agency was very candid in addressing concerns surrounding biosimilars, such as switching. Motivated by savings and the attitude of the Norwegian Medicines Agency, many hospital departments in Norway initiated switching of patients from originator infliximab to the biosimilar infliximab (Remsima®) before results from the NOR-SWITCH trial were available.74,75 Consequently, as of April 2016, the biosimilar infliximab (Remsima®) had obtained 92.9% of the market share in Norway.74 Prompted by the response in Norway, the Dutch authorities began funding a similar trial (BIO-SWITCH) to study the effects of switching from Remicade® to an infliximab biosimilar.72
Economic analyses of budgetary impacts of biosimilars have been conducted, and biosimilars are more cost-efficient overall with significant savings.14,76,77 For example, in the London health-authority region, switching from originator filgrastim to the biosimilar filgrastim (Zarzio®) resulted in purchasing costs being reduced from £3.3 million in 2010 to £2.3 million in 2011, a £1 million annual saving.14 These savings were predicted to increase to £2 million in 2012 as the switch to Zarzio® continued. Furthermore, in the Southern Health Care region in Sweden, the introduction of Zarzio® was associated with net savings of €2 million, representing savings of 4%–5% of the total budget for all drugs.14 In 2011, it was reported that the use of Zarzio®, rather than originator filgrastim, led to annual savings of €85 million across 17 EU countries.14 In an economic analysis of filgrastim, biosimilar filgrastim, and pegfilgrastim in Germany, France, Italy, Spain, and the UK, the biosimilar was consistently more cost-efficient than filgrastim or pegfilgrastim, with estimated savings of €457.84 for a 14-day regimen of treatment.76 Similarly, in a budget-impact analysis of a biosimilar to infliximab in Bulgaria, the Czech Republic, Hungary, Poland, Romania, and Slovakia, assuming the retail price for the infliximab biosimilar was 75% (25% discount) of the originator product, the projected estimated savings would be €15.3–€20.8 million in the first 3 years.77 An estimate on biosimilar-related savings between 2007 and 2020 for eight European countries (Germany, France, the UK, Italy, Spain, Sweden, Poland, and Romania) varied from €11.8 billion (slow penetration and minimal price reduction) to €33.4 billion (fast penetration and maximal price reduction).68
The development of biosimilars offers many potential benefits to patients, health care providers, and hospitals, including enhanced affordability and increased access to biologic treatments, without compromising on efficacy and safety. For example, in a pooled analysis of five postapproval studies across 12 European countries, Zarzio® was shown to be effective for the prevention of chemotherapy-induced neutropenia in clinical practice across a variety of cancers.14 Since its launch in 2009, the estimated exposure to Zarzio® is approximately 7 million patient-days (as of the FDA-approval date), and clinical experience has reported no prominent or new safety signals. Furthermore, no neutralizing antibodies were detected in any of the clinical studies in healthy volunteers or patients with cancer. Additionally, no reports of neutralizing antibodies have occurred during the ongoing pharmacovigilance of Zarzio® in clinical use.14,62,78 Similarly, patients with a variety of autoimmune diseases who were switched from originator infliximab (Remicade®) to the biosimilar infliximab (Remsima®) in clinical practice reported satisfactory outcomes, sustained efficacy, and no sign of increased immunogenicity or any other safety concerns.79,80 Furthermore, a long-term extension of the pivotal PLANETRA study reported comparable efficacy and tolerability in patients with rheumatoid arthritis who switched from originator infliximab to Remsima® for an additional year and in those who had long-term Remsima® treatment for 2 years.81 In Norway, recent data from the NOR-SWITCH trial in adult patients with spondyloarthritis, rheumatoid arthritis, psoriatic arthritis, Crohn’s disease, ulcerative colitis, or psoriasis demonstrated that switching from Remicade® to Remsima® was not inferior to continued treatment with Remicade®.82
Markets with the greatest benefit from biosimilars are functioning and competitive, with manufacturers motivated to participate and physicians who can determine the appropriate use of biosimilars for their patients.65 Consistent with an earlier analysis of vaccine tendering in Italy, a regional analysis of biosimilar tendering demonstrated that an increase in the number of competitors was associated with lower awarded prices, and that savings can be generated using tenders if the bid is designed to allow more than one manufacturer to supply the biologic.21,83 Similarly, the WHO recommends that competition should be increased to the point at which drug prices are as low as possible.20 Furthermore, the “rule of five” for pharmaceutical pricing states that prices typically reach their minimum when at least five alternatives are on the market; additional bids generally do not result in further lowering of prices.20 For biosimilars, the European Trade Association of biopharmaceutical companies, European Biopharmaceutical Enterprises, recognizes that tendering and procurement practices are used to achieve the best-possible value and outcomes; however, they recommend that tendering practices for biologics and biosimilars include a variety of selection criteria and not be based solely on price.84 Instead, tendering should provide for a sufficiently broad choice of products.84 As discussed previously, disruptions in the availability of medicines can negatively impact both patients and the health system, eg, by increased costs in sourcing alternative supplies and/or by increased vulnerability of the supply chain due to suppliers who may provide substandard products.85 To ensure the best outcomes, scientific committees involved in decision making about tendering and awards should include physicians and respect and safeguard their decisions in the clinical choice of appropriate treatment for any patient.84
Biologic drugs have a complex and specialized manufacturing process involving multiple stages, each with the potential to impact the safety and effectiveness of the biologic product, that can add risk to a manufacturer’s ability to produce high-quality biologics and meet existing (or potentially increasing) clinical demand.36 As a result of this specialization, the capacity of production plants is limited, and it is more difficult to increase the scale of production of biologic drugs rapidly if a sudden increase in demand occurs. While there are measures that biologic drug manufacturers can implement to reduce the risk of incurring shortages of biologics, the possibility that tendering processes may lead to decreased supplier options should be closely monitored to ensure drug shortages do not occur. Regulatory approval of high-quality biosimilars, developed in compliance with published biosimilar guidelines, may also help prevent shortages of biologic drugs in future by increasing the number of suppliers.36
Conclusion
Biosimilars have the potential to expand treatment options for many diseases. As observed with small-molecule generic drugs, maximizing the potential benefits of biosimilars can be significantly impacted by the policies and practices used to achieve the best value in patient care. Additionally, any tendering policy should be evaluated annually to ensure that multiple companies are still manufacturing the tendered biologics to avoid drug shortages, as well as market failures leading to market manipulation and exorbitant prices. The positive and negative aspects of tendering for small-molecule generic drugs can be critically assessed now as additional biosimilars become available to inform pricing policy.
Acknowledgments
Medical writing support was provided by Christina McManus, PhD and Anne Marie Reid, PhD of Engage Scientific Solutions and funded by Pfizer Inc.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
IJ, CK, RP, and LGS are employees of Pfizer Inc. The authors report no other conflicts of interest in this work.
References
IMS Institute for Healthcare Informatics. Global medicines use in 2020: outlook and implications. 2015. Available from: http://www.imshealth.com/en/thought-leadership/ims-institute/reports/global-medicines-use-in-2020. Accessed February 20, 2017. | ||
Lu Y, Hernandez P, Abegunda D, Edejer T. The World Medicines Situation 2011: Medicine Expenditures. Geneva: World Health Organization; 2011. Available at: http://apps.who.int/medicinedocs/documents/s18767en/s18767en.pdf. Accessed February 20, 2017. | ||
Deloitte. 2015 Global health care outlook: common goals, competing priorities. 2015. Available from: http://www2.deloitte.com/content/dam/Deloitte/global/Documents/Life-Sciences-Health-Care/gx-lshc-2015-health-care-outlook-global.pdf. Accessed February 20, 2017. | ||
Adamski J, Godman B, Ofierska-Sujkowska G, et al. Risk sharing arrangements for pharmaceuticals: potential considerations and recommendations for European payers. BMC Health Serv Res. 2010; 10:153. | ||
Schnipper LE, Smith TJ, Raghavan D, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: the top five list for oncology. J Clin Oncol. 2012;30(14):1715–1724. | ||
Vogler S, Zimmermann N, Habl C, Piessnegger J, Bucsics A. Discounts and rebates granted to public payers for medicines in European countries. South Med Rev. 2012;5(1):38–46. | ||
Vogler S, Zimmermann N, Leopold C, de Joncheere K. Pharmaceutical policies in European countries in response to the global financial crisis. South Med Rev. 2011;4(2):69–79. | ||
Carone G, Schwierz C, Xavier A. Cost-containment policies in public pharmaceutical spending in the EU. 2012. Available from: http://ec.europa.eu/economy_finance/publications/economic_paper/2012/pdf/ecp_461_en.pdf. Accessed December 20, 2016. | ||
IMS Institute for Healthcare Informatics. The Global Use of Medicines: Outlook Through 2016. Parsippany (NJ): IMS Health; 2012. Available at: www.imshealth.com/files/web/IMSH%20Institute/Reports/The%20Global%20Use%20of%20Medicines%20Outlook%20Through%202016/Medicines_Outlook_Through_2016_Report.pdf. Accessed February 20, 2017. | ||
Baer II WH, Maini A, Jacobs I. Barriers to the access and use of rituximab in patients with non-Hodgkin’s lymphoma and chronic lymphocytic leukemia: a physician survey. Pharmaceuticals (Basel). 2014;7(5):530–544. | ||
Lammers P, Criscitiello C, Curigliano G, Jacobs I. Barriers to the use of trastuzumab for HER2+ breast cancer and the potential impact of biosimilars: a physician survey in the United States and emerging markets. Pharmaceuticals (Basel). 2014;7(9):943–953. | ||
McCamish M, Woollett G. The state of the art in the development of biosimilars. Clin Pharmacol Ther. 2012;91(3):405–417. | ||
US Food and Drug Administration. Scientific considerations in demonstrating biosimilarity to a reference product: guidance for industry. 2015. Available from: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm291128.pdf. Accessed May 20, 2015. | ||
Gascón P, Tesch H, Verpoort K, et al. Clinical experience with Zarzio® in Europe: what have we learned? Support Care Cancer. 2013;21(10):2925–2932. | ||
Management Sciences for Health. Managing the tender process. In: Embrey M, Ryan M, editors. MDS-3: Managing Access to Medicines and Health Technologies. Arlington (VA): MSH; 2012:401–428. | ||
Management Sciences for Health. Managing procurement. In: Embrey M, Ryan M, editors. MDS-3: Managing Access to Medicines and Health Technologies. Arlington (VA): MSH; 2012:321–348. | ||
World Health Organization. Operational principles for good pharmaceutical procurement. 1999. Available from: http://www.who.int/3by5/en/who-edm-par-99-5.pdf. Accessed February 20, 2017. | ||
World Health Organization. WHO Expert Committee on Specifications for Pharmaceutical Preparations. World Health Organ Tech Rep Ser. 2014;(986):1–387. Available at: http://apps.who.int/medicinedocs/en/d/Js21464en/. Accessed November 30, 2016. | ||
European Parliament. Report on new developments in public procurement (2009/2175[INI]) 2010. Available from: http://www.europarl.europa.eu/sides/gETDOC.DO?PUBREF=-//EP//NONSGML+REPORT+A7-2010-0151+0+DOC+PDF+V0//EN. Accessed September 8, 2017. | ||
World Health Organization. Operational principles for good pharmaceutical procurement. 1999. Available from: http://www.who.int/3by5/en/who-edm-par-99-5.pdf. Accessed February 20, 2017. | ||
Garattini L, Van de Vooren K, Freemantle N. Tendering and value-based pricing: lessons from Italy on human papilloma virus vaccines. J R Soc Med. 2014;107(1):4–5. | ||
Dylst P, Vulto A, Simoens S. Tendering for outpatient prescription pharmaceuticals: what can be learned from current practices in Europe? Health Policy. 2011;101(2):146–152. | ||
Kanavos P, Seeley L, Vandoros S. Tender systems for outpatient pharmaceuticals in the European Union: evidence from the Netherlands, Germany and Belgium. 2009. Available from: http://ec.europa.eu/DocsRoom/documents/7607/attachments/1/translations/en/renditions/pdf. Accessed February 20, 2017. | ||
Ngorsuraches S, Chaiyakan K. Equitable prices of single-source drugs in Thailand. Appl Health Econ Health Policy. 2015;13(4):389–397. | ||
Dylst P, Vulto A, Simoens S. Societal value of generic medicines beyond cost-saving through reduced prices. Expert Rev Pharmacoecon Outcomes Res. 2015;15(4):701–711. | ||
Generics and Biosimilars Initiative. Generics makers to be penalized for huge price hikes. 2015. Available from: http://www.gabionline.net/Policies-Legislation/Generics-makers-to-be-penalized-for-huge-price-hikes. Accessed February 17, 2017. | ||
Dylst P, Simoens S. Generic medicine pricing policies in Europe: current status and impact. Pharmaceuticals (Basel). 2010;3(3):471–481. | ||
Generics and Biosimilars Initiative. Tendering for medicines in ambulatory care. 2011. Available from: http://www.gabionline.net/layout/set/print/content/view/full/1446. Accessed February 15, 2017. | ||
Management Sciences for Health. Quality assurance for pharmaceuticals. In: Embrey M, Ryan M, editors. MDS-3: Managing Access to Medicines and Health Technologies. Arlington (VA): MSH; 2012:348–371. | ||
EU Minister for Public Expenditure and Reform. European Union (Award of Public Authority Contracts) regulations 2016. 2016. Available from: http://etenders.gov.ie/Media/Default/SiteContent/LegislationGuides/european_union_award_of_public_authority_contracts_regulations_082016.pdf. Accessed December 20, 2016. | ||
EuropaBio. White paper on public procurement of biological medicines. 2015. Available from: http://www.europabio.org/sites/default/files/europabio_white_paper_on_public_procurement_of_biological_medicines_final.pdf. Accessed December 20, 2016. | ||
Pauwels K, Huys I, Casteels M, Simoens S. Drug shortages in European countries: a trade-off between market attractiveness and cost containment? BMC Health Serv Res. 2014;14:438. | ||
US Food and Drug Administration. Manual of policies and procedures. MAPP 4190.1 Rev. 2: drug shortage management. 2014. Available from: http://www.fda.gov/downloads/aboutfda/centersoffices/officeofmedicalproductsandtobacco/cder/manualofpoliciesprocedures/ucm079936.pdf. Accessed February 20, 2017. | ||
De Weerdt E, Simoens S, Casteels M, Huys I. Clinical, economic and policy implications of drug shortages in the European Union. Appl Health Econ Health Policy. 2017;15(4):441–445. | ||
Fox ER, Sweet BV, Jensen V. Drug shortages: a complex health care crisis. Mayo Clin Proc. 2014;89(3):361–373. | ||
Li E, Subramanian J, Anderson S, Thomas D, McKinley J, Jacobs IA. Development of biosimilars in an era of oncologic drug shortages. Drug Des Devel Ther. 2015;9:3247–3255. | ||
American Society of Health-System Pharmacists. Current shortages: drug shortages. Available from: http://www.ashp.org/shortages. Accessed December 8, 2016. | ||
Mazer-Amirshahi M, Pourmand A, Singer S, Pines JM, van den Anker J. Critical drug shortages: implications for emergency medicine. Acad Emerg Med. 2014;21(6):704–711. | ||
Ventola CL. The drug shortage crisis in the United States: causes, impact, and management strategies. P T. 2011;36(11):740–757. | ||
Becker DJ, Talwar S, Levy BP, et al. Impact of oncology drug shortages on patient therapy: unplanned treatment changes. J Oncol Pract. 2013;9(4):e122–e128. | ||
Association of Community Cancer Centers. Chemotherapy drug shortages. 2011. Available from: https://accc-cancer.org/advocacy/pdf/2011-Chemo-Drug-Shortages.pdf. Accessed December 8, 2016. | ||
Office of Science and Data Policy - U.S. Department of Health and Human Services. Economic analysis of the causes of drug shortages. 2011. Available from: https://aspe.hhs.gov/sites/default/files/pdf/108986/ib.pdf. Accessed December 9, 2016. | ||
Tawde SA. Particulate matter in injectables: main cause for recalls. J Pharmacovigilance. 2014;3(1):1000e128. | ||
Shabushnig JG. Particulate matter and visual inspection: industry trends 2015. 2015. Available from: https://www.pda.org/docs/default-source/website-document-library/chapters/presentations/ireland/particulate-matter-and-visual-inspection---industry-trends-2015.pdf?sfvrsn=4. Accessed February 28, 2017. | ||
Shabushnig JG. Particles in injectable pharmaceuticals: industry trends and regulatory requirements. 2017. Available from: https://websites.godaddy.com/blob/631aa03c-05c1-4540-a27c-adad80e127a5/downloads/05%20-%20PRPQA%202017%20-%20Shabushnig%201-4-2017.pdf?87be8821. Accessed February 28, 2017. | ||
US Food and Drug Administration. Frequently asked questions about drug shortages. 2016. Available from: https://www.fda.gov/Drugs/DrugSafety/DrugShortages/ucm050796.htm#q3. Accessed February 28, 2017. | ||
De Weerdt E, Simoens S, Hombroeckx L, Casteels M, Huys I. Causes of drug shortages in the legal pharmaceutical framework. Regul Toxicol Pharmacol. 2015;71(2):251–258. | ||
Hollis A, Grootendorst P. Tendering generic drugs: what are the risks? Available from: http://canadiangenerics.ca/wp-content/uploads/ 2016/10/TenderingGenericDrugs-WhatAretheRisks_FINAL.pdf. Accessed September 4, 2017. | ||
International Pharmaceutical Federation (FIP). Report of the International Summit on Medicines Shortage. The Hague: FIP; 2013. Available at: www.fip.org/files/fip/publications/FIP_Summit_on_Medicines_Shortage.pdf. Accessed December 8, 2016. | ||
IHS Markit. German pharmacists criticise discount contracts amid mounting drug shortages concerns. 2013. Available from: https://www.ihs.com/country-industry-forecasting.html?ID=1065983862. Accessed December 6, 2016. | ||
European Federation of Pharmaceutical Industries and Associations. Policy proposals to minimise medicine supply shortages in Europe. 2014. Available from: https://www.efpia.eu/media/15427/policy-proposals-to-minimise-medicine-supply-shortages-in-europe-march-2014.pdf. Accessed September 4, 2017. | ||
IHS Global Insights. Greek MoH introduces three-supplier model for hospital drugs to avoid shortages. 2014. March 30, 2017. | ||
IHS Global Insights. Major shortages reported across a wide range of drug groups in Greece. 2017. March 30, 2017. | ||
IHS Global Insights. Greek pharmacies “threatened with closure” over drug shortages. 2016. March 30, 2017. | ||
IHS Global Insights. Pharmaceutical industry commits to continued supply of Greek market amid referendum uncertainty. 2015. March 30, 2017. | ||
IHS Global Insights. Situation in Greek hospitals deteriorates, causing shortages of supplies and staff. 2016. March 30, 2017. | ||
Bocquet F, Degrassat-Théas A, Peigné J, Paubel P. The new regulatory tools of the 2016 Health Law to fight drug shortages in France. Health Policy. 2017;121(5):471–476. | ||
Schweitzer SO. How the US Food and Drug Administration can solve the prescription drug shortage problem. Am J Public Health. 2013;103(5):e10–e14. | ||
Postma D, de Wolf LM. Drug shortages in the Netherlands: monitored by Farmanco. Eur J Hosp Pharm. 2013;20 Suppl 1:A90. | ||
European Medicines Agency. Guideline on similar biological medicinal products. 2014. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/10/WC500176768.pdf. Accessed February 1, 2016. | ||
World Health Organization. Guidelines on evaluation of similar biotherapeutic products (SBPs). 2009. Available from: http://www.who.int/biologicals/areas/biological_therapeutics/BIOTHERAPEUTICS_FOR_WEB_22APRIL2010.pdf. Accessed February 1, 2016. | ||
Daller J. Biosimilars: a consideration of the regulations in the United States and European Union. Regul Toxicol Pharmacol. 2016;76:199–208. | ||
European Medicines Agency. European public assessment reports by type (biosimilars). 2016. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search.jsp&mid=WC0b01ac058001d124&searchTab=searchByAuthType&keyword=Enter%20keywords&searchType=name&alreadyLoaded=true&status=Authorised&status=Withdrawn&status=Suspended&status=Refused&jsenabled=false&searchGenericType=biosimilars&orderBy=status&pageNo=1. Accessed April 26, 2016. | ||
US Food and Drug Administration. Center for Drug Evaluation and Research: list of licensed biological products with (1) reference product exclusivity and (2) biosimilarity or interchangeability evaluations to date. 2016. Available from: https://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/UCM560162.pdf. Accessed September 8, 2017. | ||
IMS Institute for Healthcare Informatics. Delivering on the potential of biosimilar medicines: the role of functioning competitive markets. 2016. Available from: http://www.imshealth.com/files/web/IMSH%20Institute/Healthcare%20Briefs/Documents/IMS_Institute_Biosimilar_Brief_March_2016.pdf. Accessed February 20, 2017. | ||
Bocquet F, Loubière A, Fusier I, Cordonnier AL, Paubel P. Competition between biosimilars and patented biologics: learning from European and Japanese experience. Pharmacoeconomics. 2016;34(11):1173–1186. | ||
Bocquet F, Paubel P. A long war begins: biosimilars versus patented biologics. J Med Econ. 2015;18(12):1071–1073. | ||
Farfan-Portet MI, Gerkens S, Lepage-Nefkens I, Vinck I, Hulstaert F. Are biosimilars the next tool to guarantee cost-containment for pharmaceutical expenditures? Eur J Health Econ. 2014;15(3):223–228. | ||
Dylst P, Vulto A, Simoens S. Barriers to the uptake of biosimilars and possible solutions: a Belgian case study. Pharmacoeconomics. 2014;32(7):681–691. | ||
Bocquet F, Paubel P, Fusier I, Cordonnier AL, Le Pen C, Sinègre M. Biosimilar granulocyte colony-stimulating factor uptakes in the EU-5 markets: a descriptive analysis. Appl Health Econ Health Policy. 2014;12(3):315–326. | ||
Bocquet F, Paubel P, Fusier I, Cordonnier AL, Sinègre M, Le Pen C. Biosimilar versus patented erythropoietins: learning from 5 years of European and Japanese experience. Appl Health Econ Health Policy. 2015;13(1):47–59. | ||
Mestre-Ferrandiz J, Towse A, Berdud M. Biosimilars: how can payers get long-term savings? Pharmacoeconomics. 2016;34(6):609–616. | ||
Palmer E. Deep discounts allow Remicade biosimilar to grab 50% of Norway’s market. 2015. Available from: http://www.fiercepharma.com/m-a/deep-discounts-allow-remicade-biosimilar-to-grab-50-of-norway-s-market. Accessed February 20, 2017. | ||
Welch AR. The Norwegian biosimilar phenomenon: from biosimilar to “biogeneric”. 2016. Available from: https://www.biosimilardevelopment.com/doc/the-norwegian-biosimilar-phenomenon-from-biosimilar-to-biogeneric-0001. Accessed February 17, 2017. | ||
Dorner T, Strand V, Cornes P, et al. The changing landscape of biosimilars in rheumatology. Ann Rheum Dis. 2016;75(6):974–982. | ||
Aapro M, Cornes P, Abraham I. Comparative cost-efficiency across the European G5 countries of various regimens of filgrastim, biosimilar filgrastim, and pegfilgrastim to reduce the incidence of chemotherapy-induced febrile neutropenia. J Oncol Pharm Pract. 2012;18(2):171–179. | ||
Brodszky V, Baji P, Balogh O, Pentek M. Budget impact analysis of biosimilar infliximab (CT-P13) for the treatment of rheumatoid arthritis in six Central and Eastern European countries. Eur J Health Econ. 2014;15 Suppl 1:S65–S71. | ||
US Food and Drug Administration. FDA Oncologic Drugs Advisory Committee meeting: Zarxio (filgrastim). 2015. Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee/UCM428782.pdf. Accessed September 4, 2017. | ||
Danese S, Bonovas S, Peyrin-Biroulet L. Biosimilars in IBD: from theory to practice. Nat Rev Gastroenterol Hepatol. 2017;14(1):22–31. | ||
Braun J, Kudrin A. Switching to biosimilar infliximab (CT-P13): evidence of clinical safety, effectiveness and impact on public health. Biologicals. 2016;44(4):257–266. | ||
Yoo DH, Prodanovic N, Jaworski J, et al. Efficacy and safety of CT-P13 (biosimilar infliximab) in patients with rheumatoid arthritis: comparison between switching from reference infliximab to CT-P13 and continuing CT-P13 in the PLANETRA extension study. Ann Rheum Dis. 2017;76(2):355–363. | ||
Goll GL, Olsen IC, Jorgensen KK, et al. Biosimilar infliximab (CT-P13) is not inferior to originator infliximab: results from a 52-week randomized switch trial in Norway. Poster presented at: 2016 ACR/ARHP Annual Meeting; November 11–16, 2016; Washington, DC. | ||
Curto S, Ghislandi S, van de Vooren K, Duranti S, Garattini L. Regional tenders on biosimilars in Italy: an empirical analysis of awarded prices. Health Policy. 2014;116(2–3):182–187. | ||
European Biopharmaceutical Enterprises. Directive of the European Parliament and of the Council on Public Procurement COM (2011) 896: EBE position paper on tendering of biosimilars/biologicals. 2012. Available from: https://qed.eu/old-files-dir/EBEPositionPaper.pdf. Accessed June 8, 2016. | ||
American Chamber of Commerce to the European Union. Improving access to medicines in the European Union: value, measured outcomes and innovation crucial to fostering sustainable healthcare systems. 2016. Available from: http://www.amchameu.eu/system/files/position_papers/improving_access_to_medicines_in_the_eu_amcham_eu_healthcare_june_2016.pdf. Accessed February 17, 2017. | ||
European Medicines Agency. Human medicines. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages%2Fmedicines%2Flanding%2Fepar_search.jsp&mid=WC0b01ac058001d124&searchTab=searchByAuthType&alreadyLoaded=true&isNewQuery=true&status=Authorised&status=Withdrawn&status=Suspended&status=Refused&keyword=Enter+keywords&searchType=name&taxonomyPath=&treeNumber=&searchGenericType=biosimilars&genericsKeywordSearch=Submit. Accessed February 20, 2017. | ||
Generics and Biosimilars initiative. Biosimilars approved in the US. 2016. Available from: http://www.gabionline.net/Biosimilars/General/Biosimilars-approved-in-the-US. Accessed February 17, 2017. | ||
Genetic Engineering & Biotechnology News. Biosimilars: 11 drugs to watch. 2016. Available from: http://www.genengnews.com/the-lists/biosimilars-11-drugs-to-watch/77900135?page=2. Accessed February 17, 2017. | ||
Generics and Biosimilars Initiative. Biosimilars of rituximab. 2015. Available from: http://www.gabionline.net/Biosimilars/General/Biosimilars-of-rituximab. Accessed April 19, 2017. | ||
Generics and Biosimilars Initiative. Biosimilars of trastuzumab. 2014. Available from: http://gabionline.net/Biosimilars/General/Biosimilars-of-trastuzumab. Accessed April 19, 2017. | ||
Generics and Biosimilars Initiative. Biosimilars of bevacizumab. 2014. Available from: http://gabionline.net/Biosimilars/General/Biosimilars-of-bevacizumab. Accessed April 19, 2017. | ||
Generics and Biosimilars Initiative. Biosimilars of pegfilgrastim. 2014. Available from: http://www.gabionline.net/Biosimilars/General/Biosimilars-of-pegfilgrastim. Accessed April 19, 2017. | ||
Generics and Biosimilars Initiative. Biosimilars of epoetin alfa. 2014. Available from: http://www.gabionline.net/Biosimilars/General/Biosimilars-of-epoetin-alfa. Accessed April 19, 2017. | ||
Generics and Biosimilars Initiative. Subsequent entry biologics approved in Canada. 2014. Available from: http://www.gabionline.net/Biosimilars/General/Subsequent-entry-biologics-approved-in-Canada. Accessed February 28, 2017. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.