Back to Archived Journals » Research and Reviews in Parkinsonism » Volume 6
Drug-induced parkinsonism: diagnosis and management
Authors Blanchet P, Kivenko V
Received 4 June 2016
Accepted for publication 19 July 2016
Published 23 September 2016 Volume 2016:6 Pages 83—91
DOI https://doi.org/10.2147/JPRLS.S99197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Peter Hedera
Pierre J Blanchet,1–3 Veronika Kivenko1–3
1Department of Stomatology, Faculty of Dental Medicine, University of Montreal, 2Andre-Barbeau Movement Disorders Unit, University of Montreal Hospital Center (CHU Montreal), 3Montreal Mental Health University Institute, Montreal, QC, Canada
Abstract: Drug-induced parkinsonism (DIP) has been known for >60 years. It is the second leading cause of parkinsonism, but still underdiagnosis is likely to influence reported incidence figures. Since DIP is clinically undistinguishable from Lewy-body Parkinson’s disease, any new case of parkinsonism should prompt the search for an offending antipsychotic, hidden neuroleptic, or nonneuroleptic agent that may produce DIP. DIP is reversible upon drug withdrawal in most cases. There is no consensus regarding the duration of the recovery period to allow motor signs to fully remit in order to confirm the diagnosis of DIP following removal of the causative agent, but a drug-free interval of at least 6 months is generally recommended. Interestingly, up to 30% of DIP cases may show persisting or worsening motor signs beyond 6 months following drug withdrawal or adjustment, due to complex postsynaptic and presynaptic factors that may variably interact to negatively influence nigrostriatal dopamine transmission in a so-called “double-hit” hypothesis. The condition significantly impacts on quality of life and increases the risks of morbidity and mortality. Management is challenging in psychiatric patients and requires a team approach to achieve the best outcome.
Keywords: neuroleptic drugs, extrapyramidal side effects, second generation antipsychotics, calcium channel blockers, valproic acid, tetrabenazine
Introduction
In view of its prevalence and expected reversibility upon drug withdrawal, drug-induced parkinsonism (DIP) has drawn sustained interest for >60 years. Its causative mechanisms and clinical similarity with Lewy-body Parkinson’s disease (PD) have contributed to our understanding of the latter condition and to the discovery of oral levodopa as symptomatic replacement therapy.1 Although its prevalence is in part related to the aging of the population and expanded polypharmacy,2–4 an individual variation in susceptibility has long been documented.
DIP was initially described in 1954 by Bergouignan and Régnier5 and Steck6 in patients treated with chlorpromazine and reserpine, setting aside first-generation classical antipsychotic drugs and monoamine depleters as high-risk offenders. The list of drugs associated with DIP has grown ever since, to extend to gastrointestinal prokinetics, calcium channel blockers, modern atypical antipsychotics, and antiepileptic drugs that impair dopamine function directly or indirectly.1 Many cases are serious enough to be spontaneously reported to sanitary agencies.7 The condition is not reversible in at least 10% of cases and carries a risk of morbidity and mortality particularly in the elderly,8 especially if neuroleptic malignant syndrome (NMS) develops. Clinicians must remain wary of its development and manage it diligently.
Definition and epidemiology
The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V),9 defines DIP as the presence of resting tremor, muscular rigidity, akinesia, or bradykinesia, developing within a few weeks of starting or raising the dosage of a medication (typically a neuroleptic) or after reducing the dosage of an antiparkinsonian agent. In this definition, the presence of bradykinesia is not mandatory, in contrast to the conventional definition of the parkinsonian syndrome (PS) proposed in the UK Parkinson’s Disease Society Brain Bank (UKPDSBB, Step 1) clinical diagnostic criteria.10 The absolute symmetry of the motor signs is not part of the DSM-V definition, but strictly unilateral signs are unusual in DIP (as detailed in Clinical presentation section). Lack of standard criteria for DIP and misdiagnosis rate undoubtedly have a significant impact on epidemiological data. Several scales are available to document DIP, and the most widely used, the Simpson–Angus Scale, largely excludes bradykinesia as a requirement, shifting emphasis on rigidity.11 Using the DSM classification, Simpson–Angus Scale, and UKPDSBB Step 1 criteria for PS identification in a group of older adults medicated for chronic schizophrenia, the prevalence of PS was 62.5%, 87.5%, and 39.3%, respectively.12 In a single academic center, only one of 24 patients with DIP had been properly diagnosed prior to referral.13 The reasons for underdiagnosis are several-fold, including lack of recognition or attribution of the clinical presentation to PD or the mental illness (as apathy, depression, catatonia, psychogenic condition). In wrongly ascribed cases, the drug profile may inadequately be deemed inoffensive (eg, low-dose classical antipsychotics, use of atypical antipsychotics in monotherapy, or hidden neuroleptics). In contrast to young patients, people over age 50 years with declining dopamine D2 receptors density may display DIP with estimated D2 receptor occupancy levels <80% in the putamen assessed by positron emission tomography, and a daily dose of risperidone as low as 0.58 mg can achieve 50% maximal receptor occupancy.14 In other missed cases of DIP, the motor signs may have been mild and asymptomatic, unilateral or asymmetric, or delayed in onset or offset. According to the DSM criteria, DIP must become apparent within a few weeks of a change in antipsychotic drug treatment, but there are exceptions. With central dopamine antagonists, most DIP cases develop within 3 months,15,16 but drug exposure up to 12 months may be necessary in the case of calcium channel blockers,16 even longer in valproate users.17 There is no consensus regarding the duration of the recovery period to allow motor signs to fully remit and confirm the diagnosis of DIP following removal of the causative agent, but a drug-free interval of at least 6 months is generally recommended.18 In 17 DIP patients studied retrospectively, ten achieved complete remission after a mean (range 2–19 months) interval of 10 months.13
This proof of reversibility is impractical to fulfill in many psychiatric patients who cannot withdraw their medication easily. Of note, some reversible DIP cases may still show Lewy-body pathology at autopsy to raise a diagnosis of unmasked PD.19,20
Keeping these caveats in mind, it should come as no surprise that the prevalence of DIP is variable between studies and highly dependent on the proportion of older adults in the population under study. In the EUROPARKINSON Collaborative Study, DIP was estimated to contribute to 5% of all cases of PS in Europe.21 The prevalence in patients treated with classical antipsychotics was reported long ago to vary between 4%15 and 40%,22 making comparisons between first- and second- or third-generation antipsychotics difficult. In population studies, DIP is generally considered the second leading cause of PS with 22% (door-to-door survey in central Spain),23 20% (Rochester Epidemiology Project),18 and 37% (Bambuí study)4 of all cases of parkinsonism. In tertiary care movement disorder clinics, the proportion of PS attributed to DIP varies between 4% and 10%.13,24 A preponderance of women is often reported, attributed to drug dosing or interaction issues or hormonal influences.15,16,18,25–28 In addition to old age and female sex, commonly accepted patient-related risk factors for DIP (Table 1) include preexisting extrapyramidal disorder,29 concomitant brain damage and atrophy,30 dementia,29,31 HIV infection,32 severe psychiatric disease,33 severe unexplained hyposmia,34,35 and familial PS,36 while drug-related risk factors include drug potency and dosing maximizing striatal dopamine D2 receptor occupancy in numbers and constancy.
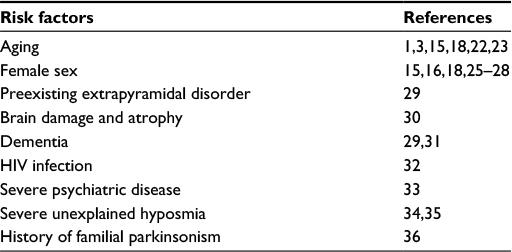 | Table 1 Patient-related risk factors for DIP Abbreviation: DIP, drug-induced parkinsonism. |
In a group of 67 patients with intellectual disability, DIP did not correlate with overt brain damage.37 Dopamine receptor gene variations seem uninvolved.38
Drugs
A strong knowledge of all drugs producing PS is important to raise suspicion about the disorder (Table 2). Many drug classes are implicated, and clinicians should know about the drugs carrying a risk of DIP in their own field of practice in order to advise and monitor patients under treatment adequately. Drugs associated with DIP may be classified as neuroleptic versus nonneuroleptic, according to their propensity for causing PS or in terms of the pathogenic mechanism of interference of dopamine neurotransmission.1,2
 | Table 2 Offending agents causing DIP Abbreviation: DIP, drug-induced parkinsonism. |
Antipsychotic agents
Centrally acting dopamine receptor antagonists accounted for nearly half of all DIP cases in one pharmacovigilance center collecting spontaneous reports.16 Typical, first-generation antipsychotics with high affinity for dopamine D2 receptors constitute a distinct class, including phenothiazines (eg, chlorpromazine, levomepromazine, thioridazine, perphenazine, fluphenazine), thioxanthenes (eg, flupentixol, thiothixene, zuclopenthixol), diphenylbutylpiperidines (eg, pimozide), dibenzoxazepines (eg, loxapine or its metabolite amoxapine), and butyrophenones (eg, haloperidol). Their risk is likely influenced by their antimuscarinic properties. Several second- and third-generation atypical antipsychotics also cause DIP or may unmask and exacerbate PD.39
Causative agents mainly include olanzapine, risperidone, and aripiprazole, drugs also associated with the development of restless legs syndrome. Well-known exceptions include low-to-moderate doses of the atypical drugs quetiapine and clozapine commonly used safely in PD.40–42
Neuroleptics
Besides antipsychotics, other dopamine receptor-blocking agents are well known to induce DIP. Phenothiazine derivatives (eg, prochlorperazine, promethazine, and first-generation H1 antihistamines such as hydroxyzine, alimemazine, and aceprometazine) and benzamide substitutes (eg, metoclopramide, sulpiride, clebopride, veralipride) used for the relief of nausea, vertigo, or post-menopausal syndrome carry an intermediate-to-high risk of producing DIP. Metoclopramide has a great capacity to accumulate in the substantia nigra, even more so in Alzheimer’s disease tissues.43 The gastroprokinetic drug domperidone, which displays strong affinity for dopamine D2 receptors, does not normally cross the blood–brain barrier effectively to block central dopamine transmission.
Nonneuroleptic agents
Drugs interfering with central catecholamines vesicular storage (tetrabenazine, reserpine) or synthesis (α-methyldopa) are regarded as high-risk offenders for DIP. Other drugs are in the high-risk category of drugs liable to produce DIP, particularly, the calcium channel antagonists flunarizine and cinnarizine, two drugs bearing a piperazine nucleus displaying dopamine receptor blockade properties and affecting presynaptic dopamine storage and release mechanisms.44 Two decades ago, they were leading offending drugs in Japan45 and Spain.27 In comparison, the risk is much lower with other cardiotropic calcium channel antagonists such as verapamil and diltiazem, incriminated in a few DIP reports. This may be due to disordered calcium homeostasis affecting vesicular dopamine storage and release and/or to dopamine receptor-blocking properties. Lithium and anticonvulsant drugs (valproic acid in particular and phenytoin) convey an intermediate risk. Lithium adverse motor events may be due to a number of effects, including inhibition of the enzyme glycogen synthase kinase-3 shared with neuroleptics. Chronic lithium administration in older adults has been associated with a higher incidence of antiparkinsonian agent cotreatment.46 DIP has been observed in up to 6% of chronic valproate users, representing a tenfold rise in PS compared to the general population.47
Lower estimates in the order of 1.37% have also been documented in patients under valproate for 2.5–10 months.48 Diagnosis is difficult due to the insidious onset and highly variable treatment interval before motor manifestations emerge, extending to years of valproate exposure in some cases. Patients may even respond to levodopa.17 The underlying molecular mechanisms remain elusive, possibly involving mitochondrial dysfunction and impaired oxidative phosphorylation.49 Serotonergic (5-HT) antidepressants have long been associated with an intermediate risk of DIP (8%),16 either in monotherapy or with concomitant medications (antipsychotics in particular). Reported cases have involved all classes.50,51 These medications do not block postsynaptic dopamine receptors but have been shown to decrease striatal dopamine concentrations in animal studies.52 Combination of the antidepressant with an atypical antipsychotic blocking 5-HT2A receptors is not preventive and, to the contrary, may even increase the risk of DIP. Pharmacokinetic interaction at the level of CYP450 metabolism may contribute to raise plasma antipsychotic concentrations.51 Interestingly, antidepressants have also caused or aggravated restless legs syndrome. Miscellaneous nonneuroleptic drugs have been associated with a low risk of DIP: antiarrhythmics (amiodarone, procaine), acetylcholinesterase inhibitors, antibacterial (rifampicin), antiviral (acyclovir, vidarabine, antiretrovirals), and antifungal (amphotericin B) antibiotics, and hormones (thyroxine).1,2,16 The thiazolidinedione derivative pioglitazone, a peroxisome proliferator-activated receptor-gamma and -alpha receptor agonist, has been reported to negatively have an impact on the motor benefit derived from levodopa in a primate model of parkinsonism,53 but no report of DIP or aggravation of motor symptoms in PD subjects under oral hypoglycemic agents has been published. Anticancer agents generally do not interact with dopamine receptors.54 Methotrexate has been shown to reduce brain dopamine levels in rats,55 but no DIP cases have been reported to date. The oral 5-fluorouracil prodrug capecitabine reportedly caused an acute dystonic reaction,56 but no DIP. Thalidomide worsened PD in one case.57 Tamoxifen did not worsen motor function in animal PD models, while relieving levodopa-induced dyskinesia.58
Diagnosis and management
Clinical presentation and associated features
It cannot be emphasized enough that DIP is clinically similar to PD, although strictly unilateral motor signs occur in only 4% of DIP cases.59 A subacute onset as mentioned in the DSM criteria and typically bilateral signs from the outset raise a suspicion of DIP, but signs are reportedly symmetric in 61% of patients.59 In another series of 26 autopsy-lacking consecutive patients, motor signs were found asymmetric on the Webster rating scale in 14 (54%) cases.60 Thus, asymmetric PS is part of the DIP spectrum and does not necessarily represent underlying PD. Resting tremor is common particularly in the upper limbs (up to 60% in one series15) but occasionally restricted to the lower lip and jaw (so-called “rabbit syndrome”). An action tremor in both hands may be observed alone or in association with resting tremor. Axial involvement (postural instability, gait disturbance) depends on the severity of the presentation and comorbid brain damage. Slowing of gait is frequent, but freezing is unusual. Almost one-half of DIP cases display additional signs of tardive dyskinesia or akathisia.13,60 Pisa syndrome may also be seen, but its frequency is unclear.
In recent years, nonmotor features have been examined with the objective to distinguish DIP from PD. Anosmia and rapid eye movement sleep behavior disorder are not typical of DIP.34,61 Abnormal olfactory testing in DIP correctly predicted those subjects displaying persistent signs after drug withdrawal35 or abnormal 123I-metaiodobenzylguanidine (sympathetic neuron imaging ligand) cardiac scintigraphy suggestive of an underlying neurodegenerative process.61 Rapid eye movement sleep behavior disorder is reported in 15%–60% of PD patients and is suggestive of the diagnosis, although it may be triggered or aggravated by various antidepressants or acetylcholinesterase inhibitors.62 Autonomic complaints, including constipation and urinary and sexual dysfunction, are more common in PD than in DIP35,63 and relatively more frequent in persistent DIP than in reversible DIP.63 The prevalence of restless legs syndrome in DIP relative to PD is unknown.
Approach
Prevention is the best approach to avoid the acute as well as long-term complications that may occur with all neuroleptic drugs, particularly in subjects at greater risk (Table 1). The indications for antipsychotic drug prescription have broadened tremendously within the last 20 years, in children and in adults alike. In institutionalized elderly with dementia living in Ontario (Canada), the rate of prescription of antipsychotics used for behavioral management has been steadily over 30% in the last decade.64 In general, the indication for psychotropic drug dispensing should be reevaluated periodically, and in the case of symptomatic DIP, the drug should be discontinued whenever possible, a recommendation admittedly more easily applicable in nonpsychotic patients. For those who must be kept on antipsychotic drug treatment, prescribers must be aware that polypharmacy with psychotropic drug combinations may raise the risk of DIP due to unanticipated pharmacodynamic and/or pharmacokinetic factors. A change in drug class to a low-dose atypical agent, ideally quetiapine or clozapine, would offer the best chance to reverse the condition and facilitate management in the long run. In the event, DIP remains symptomatic; a team approach with the treating psychiatrist and individualized treatment should be proposed, taking into account the patient age, the severity of the motor condition, and impact on quality of life. Prescribing antiparkinsonian medications may threat the underlying psychopathology and cognition or exacerbate tardive dyskinesia. The clinical response highly depends on the robustness of the antipsychotic drug regime left in place for maintenance therapy. Thus, mild DIP is probably best left untreated. For the others, an anticholinergic drug or amantadine may be used in individuals under or over 60 years of age, respectively.65 Levodopa may be added but reported benefit is variable and often modest,60 but those with valproate-induced parkinsonism may respond.17 Dopamine agonists have also been used,66 but detailed studies regarding tolerability are lacking. Physical therapy should be proposed particularly in those with disordered posture and gait.
Other clinical issues
Persistent parkinsonism following neuroleptic exposure
Up to 30% of DIP cases may show persistent or worsening motor signs beyond 6 months following drug withdrawal or adjustment.67–69 In a French elderly cohort of 2,991 noninstitutionalized individuals, neuroleptic exposure increased 3.2-fold the risk to develop probable PD.70 The risk was significant for benzamides and the calcium channel blockers flunarizine and cinnarizine. The estimated population-attributable fraction of PD associated with drug exposure suggested that avoidance of drug exposure would yield a 21.7% reduction in the number of new cases of PD. In the last 15 years, studies using single photon emission computed tomography and dopamine transporter ligands have examined the integrity of the nigrostriatal dopamine terminals in DIP, revealing reduced binding capacity in >40% of cases.71 The underlying pathogenic explanation for these results is lacking, since several autopsy cases of DIP patients under long-term antipsychotic drugs have shown no significant substantia nigra pathology.19,20 Thus, postsynaptic and presynaptic factors may variably interact to influence nigrostriatal dopamine transmission and contribute to persistent DIP in the context of chronic neuroleptic exposure. In a recent review, this “double-hit” hypothesis was proposed to involve drug-induced neurotoxic cell death with inhibition of the mitochondrial respiratory chain, free radicals production, and lack of trophic support.72 Further studies are required to shed light on the mechanisms at play.
Neuroleptic malignant syndrome
Parkinsonism as part of the NMS is an infrequent drug side effect, with prevalence estimates averaging 0.991 cases per thousand people.73
Rigidity typically coexists with fluctuating delirium, fever, and dysautonomia and is associated with a rise in creatine phosphokinase (usually >1,000 IU/L) and white blood cell count in most cases.74 Like DIP, NMS commonly arises within the first few days or months following drug initiation or upward titration, but it can occur at any time point during exposure. All neuroleptics may trigger NMS, and high dosing as well as polypharmacy (combination of antipsychotics or adjunct therapy with lithium or carbamazepine) constitutes pharmacological risk factors, whereas environmental factors include physical restraint and dehydration. Profoundly altered dopamine transmission due to extensive D2 receptor occupancy in the basal ganglia75 and hypothalamus (disturbing thermoregulation), as well as musculoskeletal fiber toxicity, are thought to contribute, but current knowledge on precise mechanisms is lacking. Prompt recognition and withdrawal of the offending drug are important to prevent complications and mortality. Supportive treatment and use of dantrolene and dopamine agonists are common practice.76 Other agents such as amantadine, levodopa, and benzodiazepines have been tested. Dantrolene should be stopped as soon as possible, and the dopamine agonist maintained for 10 days (if harmful neuroleptic oral) or 2–3 weeks (if harmful neuroleptic depot). Reintroducing an antipsychotic may be considered at least 2 weeks after clinical recovery.
Conclusion
The motor features of DIP are clinically indistinguishable from Lewy-body PD. Thus, DIP requires a high index of suspicion and knowledge of the diverse offending drugs in order to be managed effectively. The condition significantly impacts on quality of life and increases the risks of morbidity and mortality. It is more complex than heretofore believed, with acute and chronic pictures documented and a variable interplay between nigrostriatal presynaptic and postsynaptic mechanisms implicated in different patients. Nonmotor features such as anosmia and cardiac denervation examined by 123I-metaiodobenzylguanidine scintigraphy may distinguish pure reversible DIP from PD. Autopsy findings in reversible or irreversible DIP have shown Lewy-body midbrain pathology and neuronal loss in a fraction of cases only, leaving many cases unexplained. DIP management is challenging and requires a team approach with the treating psychiatrist to achieve the best outcome.
Disclosure
In the last 3 years, PJB has received honoraria as consultant and speaker from UCB Pharma Canada, and as speaker from Novartis Pharma Canada. VK reports no conflicts of interest in this work.
References
Friedman JH, Trieschmann ME, Fernandez HH. Chap. 6: Drug-induced parkinsonism. In: Factor SA, Lang AE, Weiner WJ, editors. Drug Induced Movement Disorders. 2nd ed. Madden, MA: Blackwell Publishing; 2005:103–139. | ||
Thanvi B, Treadwell S. Drug induced parkinsonism: a common cause of parkinsonism in older people. Postgrad Med J. 2009;85(1004):322–326. | ||
López-Sendón J, Mena MA, de Yébenes JG. Drug-induced parkinsonism. Expert Opin Drug Saf. 2013;12(4):487–496. | ||
Barbosa MT, Caramelli P, Maia DP, et al. Parkinsonism and Parkinson’s disease in the elderly: a community-based survey in Brazil (the Bambuí study). Mov Disord. 2006;21(6):800–808. | ||
Bergouignan M, Régnier G. Aspect parkinsonien réversible au cours d’une cure de Largactil pour vomissements gravidiques [Reversible parkinsonism in the course of largactil therapy of vomiting in pregnancy]. J Med Bord. 1954;131(7):678–679. | ||
Steck H. Le syndrome extrapyramidal et diencéphalique au cours des traitements au largactil et au serpasil [Extrapyramidal and diencephalic syndrome in the course of largactil and serpasil treatments]. Ann Med Psychol (Paris). 1954;112(25):737–744. | ||
Bondon-Guitton E, Perez-Lloret S, Bagheri H, Brefel C, Rascol O, Montastruc JL. Drug-induced parkinsonism: a review of 17 years’ experience in a regional pharmacovigilance center in France. Mov Disord. 2011;26(12):2226–2231. | ||
Wilson JA, MacLennan WJ. Review: drug-induced parkinsonism in elderly patients. Age Ageing. 1989;18(3):208–210. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth ed. Arlington, VA: American Psychiatric Association; 2013. | ||
Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1988;51(6):745–752. | ||
Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl. 1970;212:11–19. | ||
Blanchet PJ, Rompré PH. Clinimetric evaluation of the Simpson-Angus Scale in older adults with schizophrenia. J Clin Psychopharmacol. 2014;34(1):36–39. | ||
Esper CD, Factor SA. Failure of recognition of drug-induced parkinsonism in the elderly. Mov Disord. 2008;23(3):401–404. | ||
Uchida H, Kapur S, Mulsant BH, Graff-Guerrero A, Pollock BG, Mamo DC. Sensitivity of older patients to antipsychotic motor side effects: a PET study examining potential mechanisms. Am J Geriatr Psychiatry. 2009;17(3):255–263. | ||
Ayd FJ Jr. A survey of drug-induced extrapyramidal reactions. JAMA. 1961;175:1054–1060. | ||
Bondon-Guitton E, Perez-Lloret S, Bagheri H, Brefel C, Rascol O, Montastruc JL. Drug-induced parkinsonism: a review of 17 years’ experience in a regional pharmacovigilance center in France. Mov Disord. 2011;26(12):2226–2231. | ||
Silver M, Factor SA. Valproic acid-induced parkinsonism: levodopa responsiveness with dyskinesia. Parkinsonism Relat Disord. 2013;19(8):758–760. | ||
Bower JH, Maraganore DM, McDonnell SK, Rocca WA. Incidence and distribution of parkinsonism in Olmsted County, Minnesota, 1976–1990. Neurology. 1999;52(6):1214–1220. | ||
Bower JH, Dickson DW, Taylor L, Maraganore DM, Rocca WA. Clinical correlates of the pathology underlying parkinsonism: a population perspective. Mov Disord. 2002;17(5):910–916. | ||
Shuaib UA, Rajput AH, Robinson CA, Rajput A. Neuroleptic-induced parkinsonism: clinicopathological study. Mov Disord. 2016;30(3):360–365. | ||
de Rijk MC, Rocca WA, Anderson DW, Melcon MO, Breteler MM, Maraganore DM. A population perspective on diagnostic criteria for Parkinson’s disease. Neurology. 1997;48(5):1277–1281. | ||
Hall RA, Jackson RB, Swain JM. Neurotoxic reactions resulting from chlorpromazine administration. J Am Med Assoc. 1956;161(3):214–218. | ||
Benito-León J, Bermejo-Pareja F, Rodríguez J, Molina JA, Gabriel R, Morales JM. Neurological Disorders in Central Spain (NEDICES) Study Group. Prevalence of PD and other types of parkinsonism in three elderly populations of central Spain. Mov Disord. 2003;18(3):267–274. | ||
Gershanik OS. Drug-induced parkinsonism in the aged. Recognition and prevention. Drugs Aging. 1994;5(2):127–132. | ||
Tarsy D. Neuroleptic-induced extrapyramidal reactions: classification, description, and diagnosis. Clin Neuropharmacol. 1983;6(Suppl 1):S9–S26. | ||
Llau ME, Nguyen L, Senard JM, Rascol O, Montastruc JL. Syndromes parkinsoniens d’origine médicamenteuse: expérience d’un centre régional de pharmacovigilance sur dix ans [Drug-induced parkinsonian syndromes: a 10-year experience at a regional center of pharmaco-vigilance]. Rev Neurol (Paris). 1994;150(11):757–762. | ||
Errea-Abad JM, Ara-Callizo JR, Aibar-Remón C. Parkinsonismo inducido por fármacos. Aspectos clínicos comparativos con la enfermedad de Parkinson [Drug-induced parkinsonism. Clinical aspects compared with Parkinson disease]. Rev Neurol. 1998;27(155):35–39. | ||
Wenning GK, Kiechl S, Seppi K, et al. Prevalence of movement disorders in men and women aged 50-89 years (Bruneck Study cohort): a population-based study. Lancet Neurol. 2005;4(12):815–820. | ||
Caligiuri MP, Lacro JP, Jeste DV. Incidence and predictors of drug-induced parkinsonism in older psychiatric patients treated with very low doses of neuroleptics. J Clin Psychopharmacol. 1999;19(4):322–328. | ||
Demars JP. Neuromuscular effects of long-term phenothiazine medication, electroconvulsive therapy and leucotomy. J Nerv Ment Dis. 1966;143(1):73–79. | ||
McKeith I, Fairbairn A, Perry R, Thompson P, Perry E. Neuroleptic sensitivity in patients with senile dementia of Lewy body type. BMJ. 1992;305(6855):673–678. | ||
Hriso E, Kuhn T, Masdeu JC, Grundman M. Extrapyramidal symptoms due to dopamine-blocking agents in patients with AIDS encephalopathy. Am J Psychiatry. 1991;148(11):1558–1561. | ||
Chakos M, Mayerhoff D, Loebel A, Alvir J, Lieberman J. Incidence and correlates of acute extrapyramidal symptoms in first episode of schizophrenia. Psychopharmacol Bull. 1992;28(1):81–86. | ||
Bovi T, Antonini A, Ottaviani S, et al. The status of olfactory function and the striatal dopaminergic system in drug-induced parkinsonism. J Neurol. 2010;257(11):1882–1889. | ||
Morley JF, Pawlowski SM, Kesari A, Maina I, Pantelyat A, Duda JE. Motor and non-motor features of Parkinson’s disease that predict persistent drug-induced parkinsonism. Parkinsonism Relat Disord. 2014;20(7):738–742. | ||
Myrianthopoulos NC, Kurland AA, Kurland LT. Hereditary predisposition in drug-induced parkinsonism. Arch Neurol. 1962;6(1):5–9. | ||
Rao JM, Cowie VA, Mathew B. Neuroleptic-induced parkinsonian side effects in the mentally handicapped. J Ment Defic Res. 1989;33(pt 1):81–86. | ||
Knol W, van Marum RJ, Jansen PA, et al. Genetic variation and the risk of haloperidol-related parkinsonism in elderly patients: a candidate gene approach. J Clin Psychopharmacol. 2013;33(3):405–410. | ||
Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs. 2002;16(1):23–45. | ||
Desmarais P, Massoud F, Filion J, Nguyen QD, Bajsarowicz P. Quetiapine for psychosis in Parkinson disease and neurodegenerative parkinsonian disorders: a systematic review. J Geriatr Psychiatry Neurol. 2016;29(4):227–236. | ||
Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. | ||
Lutz UC, Sirfy A, Wiatr G, et al. Clozapine serum concentrations in dopamimetic psychosis in Parkinson’s disease and related disorders. Eur J Clin Pharmacol. 2014;70(12):1471–1476. | ||
Chen S, Seeman P, Liu F. Antipsychotic drug binding in the substantia nigra: an examination of high metoclopramide binding in the brains of normal, Alzheimer’s disease, Huntington’s disease, and Multiple Sclerosis patients, and its relation to tardive dyskinesia. Synapse. 2011;65(2):119–124. | ||
Mena MA, de Yébenes JG. Drug-induced parkinsonism. Expert Opin Drug Saf. 2006;5(6):759–771. | ||
Kuzuhara S. [Drug-induced parkinsonism]. Nihon Rinsho. 1997;55(1):112–117. | ||
Marras C, Herrmann N, Fischer HD, et al. Lithium use in older adults is associated with increased prescribing of Parkinson medications. Am J Geriatr Psychiatry. 2016;24(4):301–309. | ||
Easterford K, Clough P, Kellett M, Fallon K, Duncan S. Reversible parkinsonism with normal beta-CIT-SPECT in patients exposed to sodium valproate. Neurology. 2004;62(8):1435–1437. | ||
Ristić AJ, Vojvodić N, Janković S, Sindelić A, Sokić D. The frequency of reversible parkinsonism and cognitive decline associated with valproate treatment: a study of 364 patients with different types of epilepsy. Epilepsia. 2006;47(12):2183–2185. | ||
Mahmoud F, Tampi RR. Valproic acid-induced parkinsonism in the elderly: a comprehensive review of the literature. Am J Geriatr Pharmacother. 2011;9(6):405–412. | ||
Madhusoodanan S, Alexeenko L, Sanders R, Brenner R. Extrapyramidal symptoms associated with antidepressants--a review of the literature and an analysis of spontaneous reports. Ann Clin Psychiatry. 2010;22(3):148–156. | ||
Hawthorne JM, Caley CF. Extrapyramidal reactions associated with serotonergic antidepressants. Ann Pharmacother. 2015;49(10):1136–1152. | ||
Dewey SL, Smith GS, Logan J, et al. Serotonergic modulation of striatal dopamine measured with positron emission tomography (PET) and in vivo microdialysis. J Neurosci. 1995;15(1 pt 2):821–829. | ||
Huot P, Johnston TH, Fox SH, Brotchie JM. Pioglitazone may impair L-DOPA anti-parkinsonian efficacy in the MPTP-lesioned macaque: results of a pilot study. Synapse. 2015;69(3):99–102. | ||
Peroutka SJ. Chemotherapeutic agents do not interact with neurotransmitter receptors. Cancer Chemother Pharmacol. 1987;19(2):131–132. | ||
Madhyastha S, Somayaji SN, Rao MS, Nalini K, Bairy KL. Effect of intracerebroventricular methotrexate on brain amines. Indian J Physiol Pharmacol. 2005;49(4):427–435. | ||
van Pelt-Sprangers MJ, Geijteman EC, Alsma J, Boere IA, Mathijssen RH, Schuit SC. Oromandibular dystonia: a serious side effect of capecitabine. BMC Cancer. 2015;15:115. | ||
Crystal SC, Leonidas J, Jakubowski A, Di Rocco A. Thalidomide induced acute worsening of Parkinson’s disease. Mov Disord. 2009;24(12):1863–1864. | ||
Smith CP, Oh JD, Bibbiani F, Collins MA, Avila I, Chase TN. Tamoxifen effect on L-DOPA induced response complications in parkinsonian rats and primates. Neuropharmacology. 2007;52(2):515–526. | ||
Hassin-Baer S, Sirota P, Korczyn AD, et al. Clinical characteristics of neuroleptic-induced parkinsonism. J Neural Transm (Vienna). 2001;108(11):1299–1308. | ||
Hardie RJ, Lees AJ. Neuroleptic-induced Parkinson’s syndrome: clinical features and results of treatment with levodopa. J Neurol Neurosurg Psychiatry. 1988;51(6):850–854. | ||
Lee PH, Yeo SH, Yong SW, Yun JK. Odour identification test and its relation to cardiac 123I-metaiodobenzylguanidine in patients with drug induced parkinsonism. J Neurol Neurosurg Psychiatry. 2007;78(11):1250–1252. | ||
Howell MJ. Parasomnias: an updated review. Neurotherapeutics. 2012;9(4):753–775. | ||
Kim JS, Youn J, Shin H, Cho JW. Nonmotor symptoms in drug-induced parkinsonism and drug-naïve Parkinson disease. Can J Neurol Sci. 2013;40(1):36–41. | ||
Vasudev A, Shariff SZ, Liu K, et al. Trends in psychotropic dispensing among older adults with dementia living in long-term care facilities: 2004–2013. Am J Geriatr Psychiatry. 2015;23(12):1259–1269. | ||
Fann WE, Lake CR. Amantadine versus trihexyphenidyl in the treatment of neuroleptic-induced parkinsonism. Am J Psychiatry. 1976;133(8):940–943. | ||
Friedman JH. Managing idiopathic Parkinson’s disease in patients with schizophrenic disorders. Parkinsonism Relat Disord. 2011;17(3):198–200. | ||
Klawans HL, Gegen D, Bruyn GW. Prolonged drug-induced parkinsonism. Confin Neurol. 1973;35:368–377. | ||
Martí-Massó JF, Poza JJ. Cinnarizine-induced parkinsonism: ten years later. Mov Disord. 1998;13(3):453–456. | ||
Brigo F, Erro R, Marangi A, Bhatia K, Tinazzi M. Differentiating drug-induced parkinsonism from Parkinson’s disease: an update on non-motor symptoms and investigations. Parkinsonism Relat Disord. 2014;20(8):808–814. | ||
Foubert-Samier A, Helmer C, Perez F, et al. Past exposure to neuroleptic drugs and risk of Parkinson disease in an elderly cohort. Neurology. 2012;79(15):1615–1621. | ||
Tinazzi M, Cipriani A, Matinella A, et al. [123I]FP- CIT single photon emission computed tomography findings in drug-induced parkinsonism. Schizophr Res. 2012;139(1–3):40–45. | ||
Erro R, Bhatia KP, Tinazzi M. Parkinsonism following neuroleptic exposure: a double-hit hypothesis? Mov Disord. 2015;30(6):780–785. | ||
Gurrera RJ, Simpson JC, Tsuang MT. Meta-analytic evidence of systematic bias in estimates of neuroleptic malignant syndrome incidence. Compr Psychiatry. 2007;48(2):205–211. | ||
Tse L, Barr AM, Scarapicchia V, Vila-Rodriguez F. Neuroleptic malignant syndrome: a review from a clinically oriented perspective. Curr Neuropharmacol. 2015;13(3):395–406. | ||
Jauss M, Krack P, Franz M, et al. Imaging of dopamine receptors with [123I]iodobenzamide single-photon emission-computed tomography in neuroleptic malignant syndrome. Mov Disord. 1996;11(6):726–728. | ||
Berman BD. Neuroleptic malignant syndrome: a review for neurohospitalists. Neurohospitalist. 2011;1(1):41–47. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.