Back to Journals » Clinical Ophthalmology » Volume 15
Drive-by Photoscreening: Plusoptix, 2WIN and Blinq Amblyopia Detection During the COVID-19 Pandemic
Authors Keffalos M, Martin S, Arnold R ![]()
Received 12 January 2021
Accepted for publication 3 February 2021
Published 23 February 2021 Volume 2021:15 Pages 775—782
DOI https://doi.org/10.2147/OPTH.S300871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract of "Drive-by photoscreening during the COVID-19 pandemic" [ID 300871].
Views: 142
Mason Keffalos, 1 Samuel Martin, 2 Robert Arnold 2
1Boise State University, Boise, ID, USA; 2Alaska Blind Child Discovery, Anchorage, AK, USA
Correspondence: Robert Arnold
Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, 3500 Latouche #280, Anchorage, AK, 99508, USA
Tel +1 907561-1917
Fax +1 907563-5373
Email [email protected]
Background: Community photoscreening for amblyopia had successfully been adopted by many communities, however many clinics curtailed screening as a result of the COVID-19 pandemic. We modified three conventional devices and tested them for outdoor, drive-by socially distanced photoscreening and refraction.
Methods: External frames that provide luminance control and focus distance were fashioned for plusoptiX S12 (Nuremberg, Germany), Adaptica 2WIN in Kaleidos case (Padova, Italy) and the Rebion blinq (Boston, USA). Children were screened by each device and then Retinomax (Righton, Japan) before AAPOS guideline validation.
Results: Eighty-eight children average age 8± 7 years had precise refraction and alignment from which 69% AAPOS 2003 risk factors were determined. The sensitivity/specificity/inconclusive rate for plusoptiX was 85%/96%/16%, for 2WIN 79%/89%/5% and for blinq 43%/74%/8%. Blinq improved to 54%/70% when screening for amblyopia ± strabismus. Bland Altman analysis of spherical equivalent showed plusoptiX and 2WIN with less over-minus than Retinomax and J0 and J45 vectors highly reliable for astigmatism determination.
Conclusion: The infrared photorefractors in modified cases reliably screened amblyopia risk factors and refraction. The birefringent scanner provided drive-by results but less reliably with wire-frame opaque case than without the case in a dimly lit room. Modified drive-by photoscreeners could help reduce amblyopia and provide socially distanced refraction during an extended pandemic.
Keywords: amblyopia, photorefraction, ROC curve, Bland Altman, birefringent screen
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
Instrument based objective amblyopia screening has evolved into a valid, public health practice endorsed by the American Academy of Pediatrics (AAP)1 and the United States Preventive Services Task Force (USPSTF).2 Visible or invisible light is projected from the instrument to the patient’s eyes and the reflected light is then analyzed for patterns that correlate with amblyopia risk factors (ARF). The American Association for Pediatric Ophthalmology and Strabismus (AAPOS) has published uniform guidelines of specific levels of refractive errors, strabismus and visual acuity identified during confirmatory exams that should be targeted by screening.3,4 Recently available technology attempts to identify whether both eyes are steadily foveating since instability of fixation correlates with amblyopia.5–7 Conventional vision screeners have required an environment free from excess visible and infrared light8 and free from distractions to allow efficient photoscreening of younger children who are at risk for amblyopia vision impairment.
The COVID-19 pandemic has substantially disrupted public health measures that previously utilized community photoscreening clinics. Concern for spread of novel Corona Virus to patients, family members and screeners has caused photoscreening to be terminated, or in some cases modified. Some clinics have discovered clear plastic barrier screens through which visible or infrared screeners can achieve reasonable results. Others have developed tents or tunnels that shield sunlight. We have modified three different models of commercially available instrument-based screeners for hand-held, portable use in a socially distanced manner with families driving by the outdoor vision screening clinic. This is a proof-of-principal study that describes the modification and limited validation of the adapted devices.
Methods
This study is part of the Alaska Blind Child Discovery which has institutional approval by Providence Hospital (Providence Alaska Medical Center). The study complies with the Declarations of Helsinki and the Health Insurance Portability and Accountability Act. Parents or legal guardians provided written informed consent and older patients provided assent. The parent of the child and all adults in the demonstration video provided written consent for their images to be included in the video. This evaluation of clinical tests has clinical trials registration: NCT0419571. De-identified data are provided and will be maintained indefinitely at the study website: http://www.abcd-vision.org/references/DriveByPhotoscreen%20de-identified.pdf.
Three instruments were modified for outdoor, drive-by use as described below. Each patient from a pediatric eye practice was screened with each device and also had a confirmatory exam consistent with AAPOS uniform guidelines.3,4 In addition to pre-school-aged children, school-aged children who had accurate phoropter astigmatism determination were included so the 2003 uniform criteria without age stratification was employed. Drive-by autorefraction is beneficial for younger and older children not only for amblyopia screening. The patients were attending a pediatric ophthalmology and strabismus clinic. Their past medical history, visual acuity, recent cycloplegic refraction, stereopsis, ocular suppression, distance and near ocular alignment, anterior and posterior segments were recorded. Each patient’s dry refraction was checked with a Retinomax (Righton, Japan).
PlusoptiX S12: This infrared autorefractor Plusoptix is produced in Nuremberg, Germany and generously provided to Alaska screeners by Christian Schmidt. The front screws of the device were removed and a nylon 21 cm x 20.5 cm board was modified and screwed back in place with longer screws. The plate was fitted with 4 light-weight carbon-fiber poles 85 cm on top and 99 cm on the bottom. Four nylon joining pieces fitted with additional 32 cm carbon-fiber poles formed the “mouth” of the suspended frame (Figure 1). Black, light-weight nylon cloth was then fitted to the frame with an additional fabric drape extending out in front. Six high-strength small magnets were sewn in the top portion of the drape so it could attach to the roof of a car with the remainder of the drape covering the rest of the open car window. At the bottom of the frame, nylon hook-and coil closure allowed opening the plusopitX for change of batteries.
 |
Figure 1 Modified carbon-fiber and nylon board frame for outdoor plusoptix S12 photoscreening. |
Adaptica 2WIN in Kaleidos case: The 2WIN is an infrared autorefractor developed by Mario Angi in Padova, Italy for adult and pediatric refractive estimation. The Kaleidos case activated by way of a WiFi or Blue-tooth tablet provides luminance and focus distance control and an additional battery. The Kaleidos can be tilted in a floor-stand intended for walk-by refractive screening with the patient’s eyes 92 cm from the front of the internally mounted 2WIN. We found that the floor stand and the tablet activation were not practical for Drive-by screening. Therefore, similar to experience in a remote clinic in Burma,9 we bypassed the tablet and sought to activate the incorporated 2WIN photoscreening device manually. Since the Kaleidos holds the 2WIN with a typical camera screw mount tightly to avoid light leakage, finger access to the trigger buttons was not convenient. We carefully cut holes in the right-hand side of the Kaleidos case and through to the front lower right aspect of the 2WIN body (Figure 2). With the 2WIN power augmented by the Kaleidos, high capacity back-up battery flipped open revealing the menu buttons and screen, the activation trigger could be enabled even while the 2WIN was securely attached to the Kaleidos case.
 |
Figure 2 Finger cut-out in the back section of Kaleidos battery case allowing trigger activation of the 2WIN photoscreener. |
Rebion blinq. The Rebion blinq provides binocular birefringent estimation of steady bifoveal fixation and was provided at a generous discount to Alaska screeners by Boston, Massachusetts developer David Hunter. The front, round window on the blinq must be 33 cm from the child’s eyes so a wire-in-plastic frame was bent and constructed with a 22 cm diameter ring fit posterior to the “equator” of the nearly spherical blinq with four 46 cm legs extending forward to the 12 cm wide by 8 cm high front window on the frame (Figure 3). An opaque black plastic covering was attached to the frame that allowed palpation and activation of the trigger buttons on each side of the blinq. The touch screen and the power cord attachment were not obscured by the modified frame for use in Drive-by birefringent screening.
 |
Figure 3 Wire-in-plastic frame to afford opaque covering for the Rebion blinq to be used outdoors. |
For COVID-19 precautions, the patient-end of each modified screener (Figure 4) was wiped with disinfectant cloth between screenings. Parents were able to utilize quick, smart-phone, online quiz registration of each patient while waiting their turn in the drive-by clinic so there was no contamination passed with pen or paperwork between screener and family.
 |
Figure 4 Three modified, portable amblyopia screeners, the Rebion blinq (foreground), the plusoptiX s12 (background) and the Adaptica 2WIN in Kaleidos case ready for outdoor, Drive-By photoscreening. |
Sample Size Calculation: From a proportion (sensitivity or specificity) of 70%, to determine a 15% difference with 95% confidence would take a sample size of 74. This proof-of-principal study was limited in time and scope due to COVID-19 restrictions, and therefore is understandably less robust in validation that prolonged, population based validation studies.10
Typical validation statistics (sensitivity, specificity, PPV) were calculated for each screening device. Instrument referral criteria for the infrared autorefractors were modified to provide a sensitive and a specific option as well as a baseline “refer” criteria (Table 1). These correspond to options 1, 3 and 5 for plusoptiX while the baseline is similar to a preschool age option for 2WIN. For cases with inconclusive results either because the patient did not participate, the pupils were not imaged or the device did not provide an interpretation, further validation statistics are provided, namely the ABCD sensitivity and ABCD specificity11,12 which include all inconclusive cases in the denominator for calculations. A receiver operating characteristic (ROC) curve was generated to compare photoscreening validity.
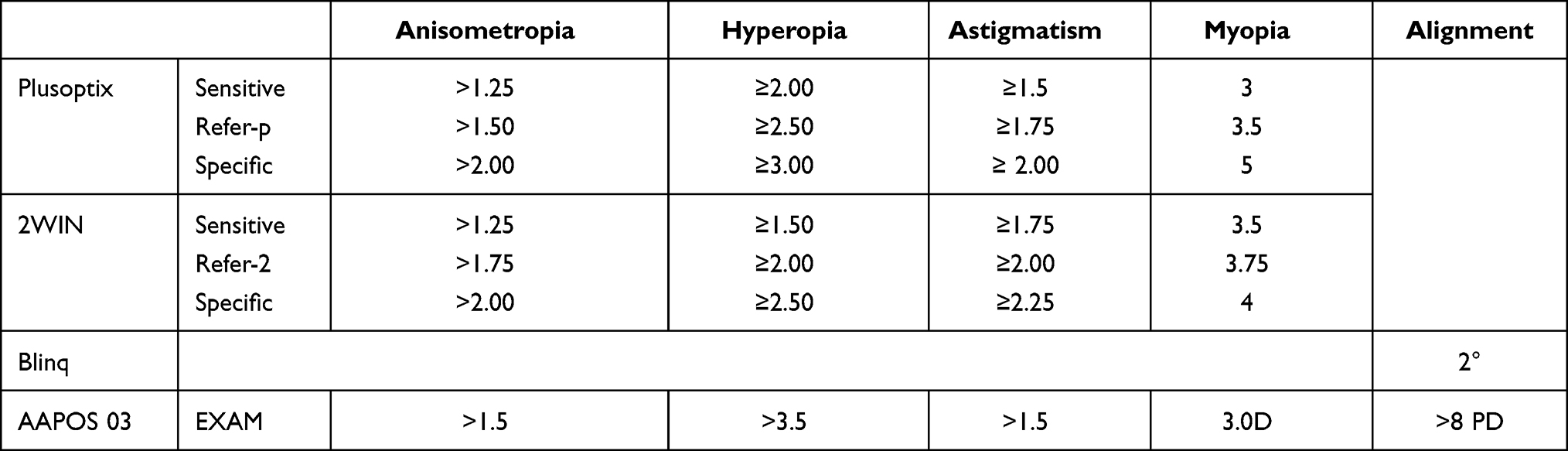 |
Table 1 Instrument Referral Criteria for PlusoptiX and 2WIN: Levels of Refractive and Strabismus Estimates from PlusoptiX, 2WIN and Rebion Blinq That Constitute Instrument Referral Criteria. The Two Infrared Autorefractors Offer at Least Three Sub-Levels of Instrument Referral for More Sensitive and More Specific Options from Which Receiver Operating Characteristic (ROC) Curve (Figure 5) Can Be Drawn. Rebion Blinq Claims to Be Able to Detect a Very Small Angle of Misalignment Whereas Plusoptix and 2WIN Can Be Set to Refer 10 Prism Diopters or More. The Three Sets of Instrument Referral Criteria are Compared with AAPOS 2003 Confirmatory Uniform Exam Guidelines That Match the Oldest Age Triad in the AAPOS 2013 Guidelines |
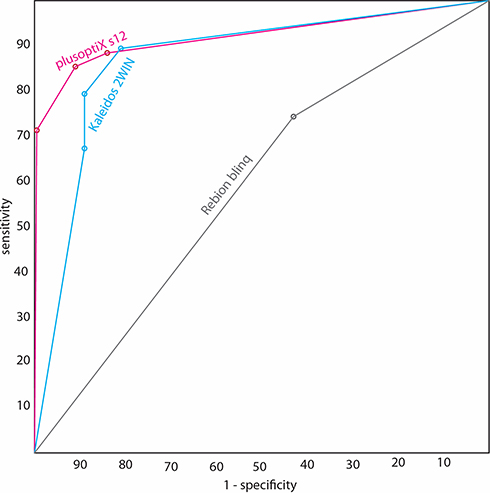 |
Figure 5 Receiver operating characteristic (ROC) curve modified-case infrared photoscreeners plusoptiX s12 and 2WIN in trigger-hole Kaleidos case compared to opaque frame modified Rebion blinq. Gold standard is the 2003 AAPOS guideline which is the older age triad from the AAPOS 2013 guidelines. |
For the devices designed to estimate refractive error, each was compared to recent cycloplegic refraction and also to Retinomax under non-cyclopleged conditions. Refractive values were converted to spherical equivalent M (sphere + cylinder/2) and astigmatism was vector converted to J0 (Horizontal Jackson cross) and J45 (oblique meridian Jackson cross) power transformations.13 Then, Plusoptix, 2WIN and Retinomax M, J0 and J45 were compared to cycloplegic refraction using Bland Altman analysis.
Results
Screening with the three modified photoscreeners (Figure 4) was attempted for 88 children each of whom successfully gave a Retinomax refractive reading. The mean and standard deviation age was 8.1±6.7 years comprising 6 toddlers less than age 3, 32 pre-school less than age 6, 23 primary school-aged, and 27 teen-aged patients. Eighteen were referred by photoscreening and ten by visual acuity screening. Sixteen had some form of developmental delay including 7 with attention deficit hyperactivity disorder and 2 with autism. Concerning racial and ethnic background, 2 were black, 7 were Asian, 11 were Hispanic, 6 were Alaska Natives, 7 were Pacific Islanders and 54 were white. A total of 61 out of the 88 (69%) had amblyopia risk factors. Their spherical equivalent cycloplegic refraction, right eyes ranged from −9.75 to +6.5 with mean +0.15 and standard deviation 2.7 diopters. There were 39 myopic, 39 hyperopic and 10 emmetropic from −0.25 to +0.25 diopters. Fifteen had amblyopia of 20/40 or worse.
Table 2 shows validation statistics for the modified photoscreeners against three different gold-standard outcomes. The primary outcome is the AAPOS 2013 older subset of refractive criteria combined with strabismus and visual acuity determination of amblyopia.3 Since the Rebion blinq is not intended as a refractive screener, the additional exam outcome of visual acuity-defined amblyopia and/or strabismus is compared for each photoscreener. The refractive screeners are also compared with pure AAPOS 2013 refractive amblyopia risk factors. Table 1 also shows three different instrument referral criteria (specific, baseline refer and specific) from which the ROC curve can be drawn (Figure 5). It is very important to clearly separate instrument referral criteria from gold-standard exam outcome guidelines (Table 1).14 By sensitive instrument referral criteria, plusoptiX and 2WIN in Kaleidos performed essentially the same (sensitivity 88–89%, specificity 81–85%) but the plusoptiX was a bit better for baseline refer and specific instrument referral criteria. However, the plusoptiX had 16% inconclusive results compared to 5% for 2WIN so the ABCD-sensitivity and ABCD-specificity were higher (73%, 78%) for 2WIN compared to plusoptiX (66%, 63%). The baseline sensitivity and specificity from the modified blinq (38%, 59%) were lower than the infrared photorefractors but improved when screening for amblyopia and/or strabismus alone (54%, 70%).
 |
Table 2 Validation for Drive-by Photoscreening; the Validation Statistics Sensitivity, Specificity, Positive Predictive Value (PPV) and ABCD Sensitivity (Sens) and ABCD Specificity (Spec) are Given in the Right-Hand Columns. A 3 x 2 Matrix of Validation Variables includes Conventional A, B, C and D with Additional E (Inconclusive Exam True) and F (Inconclusive Exam Normal). Exam Failure Criteria (Exam Fail?) Include Three Subsets; AAPOS 2003 Refractive Only (Refract Only), Cases with Visual Acuity Defined Amblyopia and/or Constant Strabismus (Strab/Ambly) and the AAPOS 2003 Which Combines Cycloplegic Refraction Guideline Levels Plus Strabismus Plus Amblyopia. There are Three Levels of Instrument Referral Criteria for plusoptiX and 2WIN Shown in Table 1 Offering Sensitive (Sens), Baseline (Refer) and Specific (Spec) Screen Interpretations |
Figure 6 gives Bland Altman analysis for modified plusoptiX and Kaleidos 2WIN compared to dry Retinomax when each is directly compared with cycloplegic refraction. There was a high correlation for each comparison; the interclass correlation coefficient (ICC) ranged from 0.49 to 0.91 for each and is superimposed on Figure 6. Almost all (88%) the cycloplegic refractions were done with precise astigmatism determination on a phoropter whereas the remaining 12% younger patients had SBARS refractions.15 For spherical equivalent, both 2WIN and plusoptiX tended to underestimate for patients with higher levels of hyperopia, whereas Retinomax tended to over-minus patients with mild levels of myopia or hyperopia (green oval on Figure 6). All devices gave good estimates of vector transformed astigmatism with the 2WIN overestimating higher levels of J0 (purple oval on Figure 6).
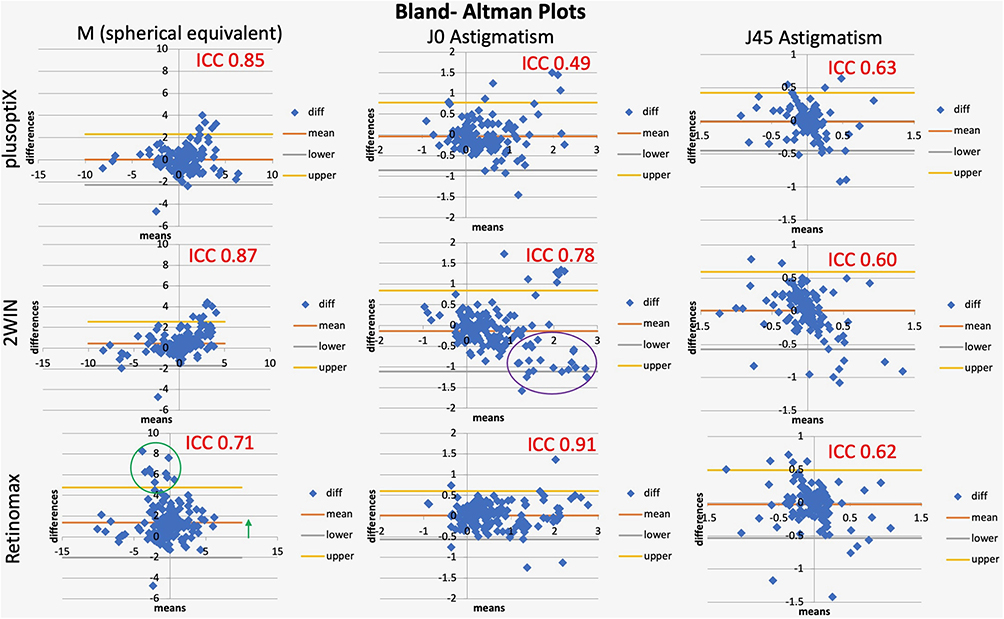 |
Figure 6 Bland Altman plots comparing three autorefractors plusoptiX s12 (top), Adaptic 2WIN in Kaleidos (middle row) and Righton Retinomax (bottom row). The left column is spherical equivalent, the middle column J0 vector transformation and the right column J45 oblique vector transformation of astigmatism. Intraclass correlation coefficient (ICC) is superimposed on each in red. The green oval and arrow indicate how Retinomax over-estimated myopia while the purple oval shows how 2WIN overestimates J0 for higher amounts of astigmatism. Clinical Ophthalmology: Drive-By Photoscreening. |
Discussion
Three commercially available, instrument-based vision screeners were successfully modified so they yield results during an out-door, drive-by photoscreening clinic in older children with a high prevalence of disease. Both plusoptiX and 2WIN gave highly reliable sphero-cylindrical refractive estimates. Our black covered frame on the Rebion blinq allowed many patients to give a “refer” or “pass” reading however it also obscured the red aiming laser beams that are intended to rest directly between the patient’s eyes. Compared to previous experience with unmodified Rebion blinq that yielded 75% sensitivity and 68% specificity for AAPOS 2003 amblyopia risk factors,16 the outdoor modifications appear to have hindered validity.
During the COVID-19 Pandemic, direct face-to-face patient care was severely restricted in pediatric and ophthalmology clinics. Compared to the year before, far fewer children had photoscreening as an integral aspect of regularly scheduled, well-child visits. During that same time, many pediatric eye exams were converted to telemedicine.17 One striking limitation of telemedicine eye exams is the inability to perform refractions. The development of valid drive-by photorefractive screening with social distancing offers a good option for both pediatric well-child vision screening and also ophthalmology telemedicine care.
Once referred by a screening, patients with amblyopia risk factors still need care during a pandemic. Providing the estimation of refraction with valid photorefractors in a drive-by paradigm is a beneficial step. Visual acuity can be checked at home by a phone-based18 or paper download19 method. Further referral toward expert pediatric ophthalmic specialty care must be balanced with community needs for pandemic isolation.20,21
These two infrared autorefracting photoscreeners and blinq, without modifications, have not yet all been directly compared, but some paired comparisons have been published. The PlusoptiX S09 had sensitivity/specificity/inconclusive rate of 85%/73%/12% compared to 73%/76%/8% for an early effort by 2WIN.22 Racano in 142 children found sensitivity/specificity/inconclusives for 2WIN of 67%/84%/5% compared to 73%/96%/11% for plusoptiX A12R.23 2WIN in the Kaleidos case achieved 87% sensitivity, 84% specificity and 8% inconclusives in remote clinics.9 From children with 63% prescreening prevalence of 2003 AAPOS risk factors, Plusoptix S09 had sensitivity/specificity/inconclusive rate of 84%/94%/13% while SPOT had 82%/68%/11%.12 Zhang et al combined 21 studies with 5022 patients to determine sensitivity/specificity of 87.7%/78% for SPOT compared to plusoptiX 89.4/89.9%.24 The 2WIN in a group with 56% 2003 AAPOS risk factors achieved 68% sensitivity, 84% specificity and only 1% inconclusive rate and vector-transformed refractions that closely matched Retinomax.25 From 321 preschool children Retinomax had sensitivity/specificity/inconclusives of 95%/94%/0% compared to plusoptiX S12 86%/84%/15%.26 In patients with 64% 2003 amblyopia risk factors, sensitivity/specificity/inconclusive rate for 2WIN was 91%/70%/3% and for blinq 70%/72%/13%.16
Strengths of this study include direct head-to-head comparison of the three modified devices in the same groups of patients who also had Retinomax autorefraction in addition to confirmatory exam. The study was completed in a short period during a pandemic with a desire to make information on blindness reduction available quickly. The patients include a wide distribution of ethnicity, eye color and neurodevelopment. A weakness of this study is the relatively small sample size obtainable during COVID-19 clinic scheduling. The study is a proof-of-concept more than a precise validation. The smart phone, in-auto registration of patients was contact free and practical; however, the patients did not electronically feed directly into any of the screening devices. Each device allowed storage of screening results on flash drives or internal memory.
Practical experience with Drive-By photoscreening: The Kaleidos case was most readily adapted needing only a means of activating the forward-facing trigger buttons on the 2WIN infrared photoscreener. Inside the Kaleidos case, the flashing fixation lights and sound are subdued however patients were able to fixate sufficiently for quick results with a low number of inconclusives. The additional battery in Kaleidos is a distinct advantage if a power cord is not available at the screening site. The Kaleidos was the only device to directly contact the patient’s face; however, sterilizing cloth wipes were simple. The plusoptiX required the largest and most extensive modification for a screening “tunnel’ with the cloth hood attaching to the car roof with magnets that did not scratch any paint. Wind and weather impacted the plusoptiX cloth and frame similar to a kite. Wind could make flaps of cloth brush over the patient’s face during screening. The wire frame fit over the Rebion blinq with no screws removed, but small shifts made the focusing laser beams slightly off center. Younger patients were less likely to glance around the room with the blinq framed hood; however, we noted a decrease in accuracy in children screened with the hood compared to prior experience without the hood in a quiet, dim exam room. Care must be used to avoid dropping the photoscreeners during outdoor, drive-by clinics, especially the blinq with its complete lack of handles. The LCD screens on all devices were harder to view in bright sunlight.
Conclusion
External modifications to account for luminance and focus distance allowed conventional amblyopia screening devices to collect valid data for amblyopia screening and remote autorefraction during Drive-By clinics. A craftsman could reproduce these modifications to conventional instrument screeners; however, we hope the manufacturers would provide them if pandemic contact restrictions are not eased in the near future.
Disclosure
Dr. Arnold is a board member of Glacier Medical Software that markets ROP-Check could-based NICU software. Dr. Arnold is a board member of PDI Check that makes a vision screening game for autostereoscopic screens on Nintendo 3DS. Dr. Arnold is the coordinator of the Alaska Blind Child Discovery which has received discounted vision screen technology from several vendors. Dr. Arnold is an investigator and protocol developer for the NIH-supported Pediatric Eye Disease Investigator Group (PEDIG). Dr. Arnold is a non-paid advisor to GoCheck Kids, plusoptiX, Adaptica and iScreen. The authors report no other conflicts of interest in this work.
References
1. Miller JM, Lessin HR. AAP: instrument-based pediatric vision screening policy statement. Pediatrics. 2012;130(5):983–986.
2. Grossman DC, Curry SJ, Owens DK, Force USPST. Vision screening in children aged 6 months to 5 years: US preventive services task force recommendation statement. JAMA. 2017;318(9):836–844. doi:10.1001/jama.2017.11260
3. Donahue SP, Arthur B, Neely DE, Arnold RW, Silbert D, Ruben JB. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013;17(1):4–8. doi:10.1016/j.jaapos.2012.09.012
4. Donahue S, Arnold R, Ruben JB. Preschool vision screening: what should we be detecting and how should we report it? Uniform guidelines for reporting results from studies of preschool vision screening. J AAPOS. 2003;7(5):314–316. doi:10.1016/S1091-8531(03)00182-4
5. Gramatikov BI, Guyton DL. A no-moving-parts sensor for the detection of eye fixation using polarised light and retinal birefringence information. J Med Eng Technol. 2017;41(4):249–256. doi:10.1080/03091902.2017.1281357
6. Gramatikov BI. Detecting central fixation by means of artificial neural networks in a pediatric vision screener using retinal birefringence scanning. Biomed Eng Online. 2017;16(1):52. doi:10.1186/s12938-017-0339-6
7. Gramatikov BI, Irsch K, Wu YK, Guyton DL. New pediatric vision screener, part II: electronics, software, signal processing and validation. Biomed Eng Online. 2016;15:15. doi:10.1186/s12938-016-0128-7
8. Arnold RW, Stark L, Leman R, Arnold KK, Armitage MD. Tent photoscreening and patched HOTV visual acuity by school nurses: validation of the ASD-ABCD protocol. (Anchorage School District – Alaska Blind Child Discovery program). Binocul Vis Strabismus Q. 2008;23(2):83–94.
9. Martin SJ, Htoo HE, Hser N, Arnold RW. Performance of two photoscreeners enhanced by protective containers. Clin Ophthalmol. 2020;14:1427–1435. doi:10.2147/OPTH.S251451
10. Varma R, Deneen J, Cotter S. The multi-ethnic pediatric eye disease study: design and methods. Ophthalmic Epidemiol. 2006;13(4):253–262. doi:10.1080/09286580600719055
11. Arnold RW. Highly specific photoscreening at the Alaska State Fair. Valid Alaska Blind Child Discovery photography and interpretation.. Alaska Med. 2003;45(2):34–40.
12. Arnold RW, Arnold AW, Armitage MD, Shen JM, Hepler TE. Pediatric photoscreeners in high risk patients 2012: a comparison study of Plusoptix, iScreen and SPOT. Binoc Vis Strabismus Quart. 2013;28(1):20–28.
13. Miller JM. Clinical applications of power vectors. Optom Vis Sci. 2009;86(6):599–602. doi:10.1097/OPX.0b013e3181a6a211
14. Robert W Arnold MD. Introduction to amblyopia vision screening validation; 2018. Available from: https://www.aao.org/annual-meeting-video/introduction-to-amblyopia-vision-screening-validat.
15. Arnold AW, Arnold SL, Sprano JH, Arnold RW. School bus accommodation-relaxing skiascopy. Clin Ophthalmol. 2019;13:1841–1851. doi:10.2147/OPTH.S219031
16. Arnold RW. Comparative AAPOS validation of the blinq birefringent amblyopia screener with isolated small-angle strabismus. Clin Ophthalmol. 2020;14:325–329. doi:10.2147/OPTH.S242335
17. Arnold RW, LaMattina KC, Taylormoore J, Nelson LB. Experiences in Telemedicine for Pediatric Ophthalmology. JPOS. 2020;57(6):344–347. doi:10.3928/01913913-20200819-02
18. Silverstein E, Williams JS, Brown JR, Bylykbashi E, Stinnett SS. Teleophthalmology: evaluation of Phone-based Visual Acuity in a Pediatric Population. Am J Ophthalmol. 2021;221:199–206. doi:10.1016/j.ajo.2020.08.007
19. Tsao WM, Armitage MD, Trujillo C, Trujillo A, Arnold LE, Tsao WL. Portable acuity screening for any school: validation of patched HOTV with amblyopic patients and Bangerter normals. BMC Ophthalmol. 2017;17(1):232. doi:10.1186/s12886-017-0624-y
20. Tamez-Tamez VE, Ruiz-Lozano RE. Evaluating amblyopia during the era of COVID-19. Graefes Arch Clin Exp Ophthalmol. 2020;258(12):2857–2859. doi:10.1007/s00417-020-04817-2
21. Saxena R, Singh D, Jethani J, Sharma P, Sinha R, Sharma N. Sachdev Writing Committee MS, Prepared in Association with the APa: pediatric ophthalmology, strabismus and neuro-ophthalmology practice in the COVID-19 era: all India Ophthalmological Society guidelines. Indian J Ophthalmol. 2020;68(7):1300–1305. doi:10.4103/ijo.IJO_1789_20
22. Kirk S, Armitage MD, Dunn S, Arnold RW. Calibration and Validation of the 2WIN Photoscreener Compared to the PlusoptiX S12 and the SPOT. J Pediatr Ophthalmol Strabismus. 2014;51(5):1–4. doi:10.3928/01913913-20140701-01
23. Racano E, Alessi S, Pertile R. Comparison of 2WIN and plusoptiX A12R refractometers with Retinomax handheld autorefractor keratometer. J AAPOS. 2019;23(5):276e271–276 e275. doi:10.1016/j.jaapos.2019.05.017
24. Zhang X, Wang J, Li Y, Jiang B. Diagnostic test accuracy of Spot and Plusoptix photoscreeners in detecting amblyogenic risk factors in children: a systemic review and meta-analysis. Ophthalmic Physiol Opt. 2019;39(4):260–271. doi:10.1111/opo.12628
25. Arnold SL, Arnold AW, Sprano JH, Arnold RW. Performance of the 2WIN photoscreener with “CR” strabismus estimation in high risk patients. Am J Ophthalmol. 2019;207:195–203. doi:10.1016/j.ajo.2019.04.016
26. Kinori M, Molina I, Hernandez EO, Robbins SL, Granet DB, Coleman AL. The PlusoptiX Photoscreener and the Retinomax Autorefractor as Community-based Screening Devices for Preschool Children. Curr Eye Res. 2018;1–5.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.