Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Drawing Characteristics Associated with Attention-Deficit/Hyperactivity Disorder in Children: Findings from the Synthetic House-Tree-Person Test
Authors Zheng M, Lin X ![]() , Wang S, Zhang X, Li C, Huang R
, Wang S, Zhang X, Li C, Huang R ![]() , Jin X
, Jin X ![]()
Received 11 April 2026
Accepted for publication 1 July 2026
Published 17 July 2026 Volume 2026:22 612297
DOI https://doi.org/10.2147/NDT.S612297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Manman Zheng,1,* Xinya Lin,2,3,* Shao Wang,4 Xuan Zhang,3 Can Li,5 Rong Huang,3 Xiaofeng Jin3,6
1Graduate Work Department, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2Department of Affective Disorder, The Affiliated Brain Hospital, Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 3School of Mental Health, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 4The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 5Department of Psychiatry, The Third People’s Hospital of Xiangshan County, Ningbo, Zhejiang, People’s Republic of China; 6The Affiliated Kangning Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaofeng Jin, School of Mental Health, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Objective: This study aimed to examine drawing characteristics in the Synthetic House-Tree-Person (S-HTP) drawing test among children with attention-deficit/hyperactivity disorder (ADHD) and to explore their associations with ADHD symptom severity.
Methods: A total of 60 children aged 7– 11 years (30 with clinically diagnosed ADHD and 30 healthy controls) completed the S-HTP drawing test and the SNAP-IV scale. Drawing characteristics were independently coded by two trained raters using predefined criteria. Group differences were analyzed using chi-square and rank-sum tests. Logistic regression analyses were performed to evaluate associations with ADHD status, and ROC analyses were used to assess discrimination. FDR correction and bootstrap internal validation were additionally applied.
Results: Six drawing characteristics differed significantly between groups in the initial analyses, of which five remained significant after FDR correction. Seven drawing characteristics showed exploratory associations with SNAP-IV scores. After adjustment for age, gender, family structure, and Raven’s Standard Progressive Matrices scores, three drawing characteristics remained associated with ADHD status: A3 (tracing in shaky lines; OR = 4.31, 95% CI: 1.10– 16.94), A4 (lines jagged and not joined; OR = 5.45, 95% CI: 1.45– 20.49), and A8 (more than seven different colors; OR = 0.20, 95% CI: 0.05– 0.72). Exploratory ROC analyses indicated that combining these characteristics improved discriminatory performance. The combined model achieved an AUC of 0.835. Bootstrap internal validation yielded an optimism-corrected AUC of 0.812, indicating reasonable model stability within the present sample.
Conclusion: Certain S-HTP drawing characteristics were associated with ADHD status and symptom severity in this sample. In particular, A3, A4, and A8 were identified as drawing characteristics of potential interest for future research. However, given the exploratory design, relatively small sample size, and lack of external validation, further studies are required before the clinical utility of these findings can be established.
Keywords: Synthetic House-Tree-Person Drawing Test, attention-deficit hyperactivity disorder, children, drawing characteristics, projective test, assessment
Introduction
Attention-deficit hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders in school-aged children. Global prevalence estimates range from 2% to 18%,1 with a pooled prevalence of 7.2% across the editions of Diagnostic and Statistical Manual of Mental Disorders reported in a meta-analysis of 175 studies.2 As for Chinese children, the overall prevalence of ADHD is 6.3%.3 Given China’s large population, the absolute number of children with ADHD remains substantial, imposing a significant burden on both families and society. The core symptoms of ADHD, including age-inappropriate inattention, impulsivity, and hyperactivity, can lead to learning difficulties, low self-esteem, interpersonal problems, and impaired psychosocial functioning.4–6 Moreover, 60–80% of individuals with childhood ADHD continue to exhibit symptoms into adulthood.7 Recent studies have documented that early management of ADHD symptoms may attenuate adult functioning difficulties.8,9 Therefore, early screening and diagnosis are essential for timely intervention and treatment. Although both genetic and environmental factors are believed to be associated with ADHD, the specific etiology remains contentious.9
Effective treatment of ADHD begins with early screening and diagnosis, which requires a comprehensive approach that gathers information from multiple sources and uses various assessment methods.10 Commonly used instruments include the Achenbach Child Behavior Checklist,11 the Conners’ Parent Rating Scale12 and Swanson Nolan and Pelham, Version IV (SNAP-IV).13 These scales also help distinguish symptoms of inattention, hyperactivity, conduct disorder, and disruptive behavior disorders. In addition to objective scales, information from parents about their child’s behavior at school, home, and in the community is also crucial for making an accurate diagnosis. Thus, parent interviews are a crucial component of ADHD assessment, often employing tools like the Parent Interview for Child Symptoms, a semi-structured interview designed to aid in diagnosing ADHD. While patient interviews should also be included as part of the assessment, they may lack reliability in young children.
Influenced by traditional cultural values, some Chinese parents may overinterpret normal attention lapses as ADHD, while others dismiss symptoms as misbehavior, leading to diagnostic inaccuracies. Inconsistent reporting by parents, influenced by differences in family dynamics, educational environments, and access to healthcare, can further complicate the screening process.14 Although effective diagnosis requires children to communicate their internal states to clinicians, young children often struggle to articulate their experiences clearly. This limitation highlights the need for supplementary, child-friendly assessment tools. Human figure drawing tests have been used as complementary tools in ADHD assessment.15 Drawing tests have also been shown to reveal significant distinctions between children with ADHD and their typically developing peers in terms of emotional issues and impulsive behaviors.16,17 Therefore, there is a need for supplementary assessment approaches that are developmentally appropriate for children.
Drawing transcends its artistic roots to become a profound tool for understanding the human psyche, offering a unique lens into the emotional and psychological realms that are often difficult to articulate through words alone. Engaging in drawing tests allows individuals to bypass the limitations of verbal communication and social expectations, enabling a more authentic expression of personal experiences and feelings. This process illuminates emotional states and personality traits that might otherwise remain concealed. In the context of psychological assessment, drawing serves as a powerful means to uncover and address underlying psychological conditions.18
Projective techniques reveal personality characteristics by eliciting responses to unstructured or ambiguous stimuli. Unlike traditional scales, which participants can consciously manipulate, projective techniques offer a more indirect means of accessing subconscious thoughts and emotions. Drawing provides individuals with a medium to express inner emotions free from societal pressures, reducing the likelihood of deliberate concealment.18 One of the most widely known projective techniques is the Rorschach inkblot test, which uses ambiguous stimuli to explore aspects of personality and emotional functioning.19 Based on the projective technique, Buck proposed the House-Tree-Person drawing test, which is designed to assist clinicians in gathering information.20 It requires subjects to draw a house, a tree, and a person on three separate pages to the best of their ability, without assessing artistic skill. Mikami subsequently developed the Synthetic House-Tree-Person Drawing Test (S-HTP) drawing test,21 which involves drawing these elements on the same sheet of paper, different from the House-Tree-Person drawing test. It enables a more comprehensive assessment of the connections among the house, tree, and person, facilitating clinicians in gaining a deeper insight into the subject’s personality and their interactions with the environment. Although these characteristics have contributed to the use of projective drawing techniques in clinical practice, the clinical utility of projective drawing techniques remains debated, particularly with regard to their diagnostic specificity, psychometric validity, and reproducibility. Therefore, drawing-based assessments are generally considered complementary rather than stand-alone diagnostic tools.
The S-HTP drawing test has been applied in various clinical and research settings and is currently undergoing further standardization.22 It has also been found effective in addressing gender-related issues among adolescents23 and assessing the impact of traumatic events on children’s mental health.24 Certain drawing characteristics have also been reported to be associated with symptoms of anxiety and depression in cancer patients.25,26 Drawing tests, unconstrained by age or cultural background, allow children to independently express their emotions, thereby providing valuable supplementary insights that may be overlooked by conventional verbal or standardized evaluations.
Children with ADHD, however, often exhibit deficits in fine motor control, visuomotor coordination, and sustained attention, all of which are important for drawing performance.27,28 In clinical practice, we have also observed that children with ADHD tend to display distinctive drawing features, such as impulsive strokes or neglect of details, compared with their typically developing peers. These observations suggest that drawing tasks, which naturally integrate motor, perceptual, and attentional components, may provide a sensitive window into the behavioral manifestations of ADHD.
However, the potential of drawing-based tools, such as the S-HTP test, in the assessment of children with ADHD remains underexplored. Given their age-appropriateness, ease of administration, and capacity to engage children actively in the assessment process, such tools may serve as useful adjuncts in the early identification of ADHD. Therefore, this study aimed to investigate whether specific S-HTP drawing characteristics are associated with ADHD status and symptom severity in children. We hypothesize that specific drawing characteristics will significantly differ between children with ADHD and their typically developing peers, thereby providing supplementary information regarding behavioral characteristics associated with ADHD.
Materials and Methods
Participants
All participants in the clinical group had a diagnosis of ADHD and were recruited from the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University in Wenzhou, China. ADHD diagnoses were established by experienced child psychiatrists according to DSM-5 criteria on the basis of comprehensive clinical assessments conducted during the first outpatient visit. Diagnoses were further confirmed using the Mini International Neuropsychiatric Interview for children and adolescents (MINI-KID).29 Information regarding symptom presentation across multiple settings, including home and school environments, was obtained through parental interviews, which incorporated teacher feedback regarding the child’s behavior at school. The S-HTP assessment was conducted for research purposes and was not used in the diagnostic decision-making process. The inclusion criteria were: (1) met the DSM-5 criteria for ADHD;4 (2) a mean subscale score >1 on either the inattention or the hyperactivity/impulsivity subscales of the SNAP-IV; (3) aged 7–11 years, with no sex restriction; (4) Patients were selected at their first consultation, ie, not yet receiving treatment for ADHD. Exclusion criteria: (1) Raven’s Standard Progressive Matrices (SPM) score ≤25th percentile;30 (2) severe or primary comorbid psychiatric or neurological disorders (eg, depressive disorder, generalized anxiety disorder, autism spectrum disorder, or tic disorder); (3) severe physical illnesses. Thirty children were included in the clinical group. The mean age of the clinical group was 8.9 ± 1.2 years; 80.0% (24) were boys, and 20.0% (6) were girls (Table 1).
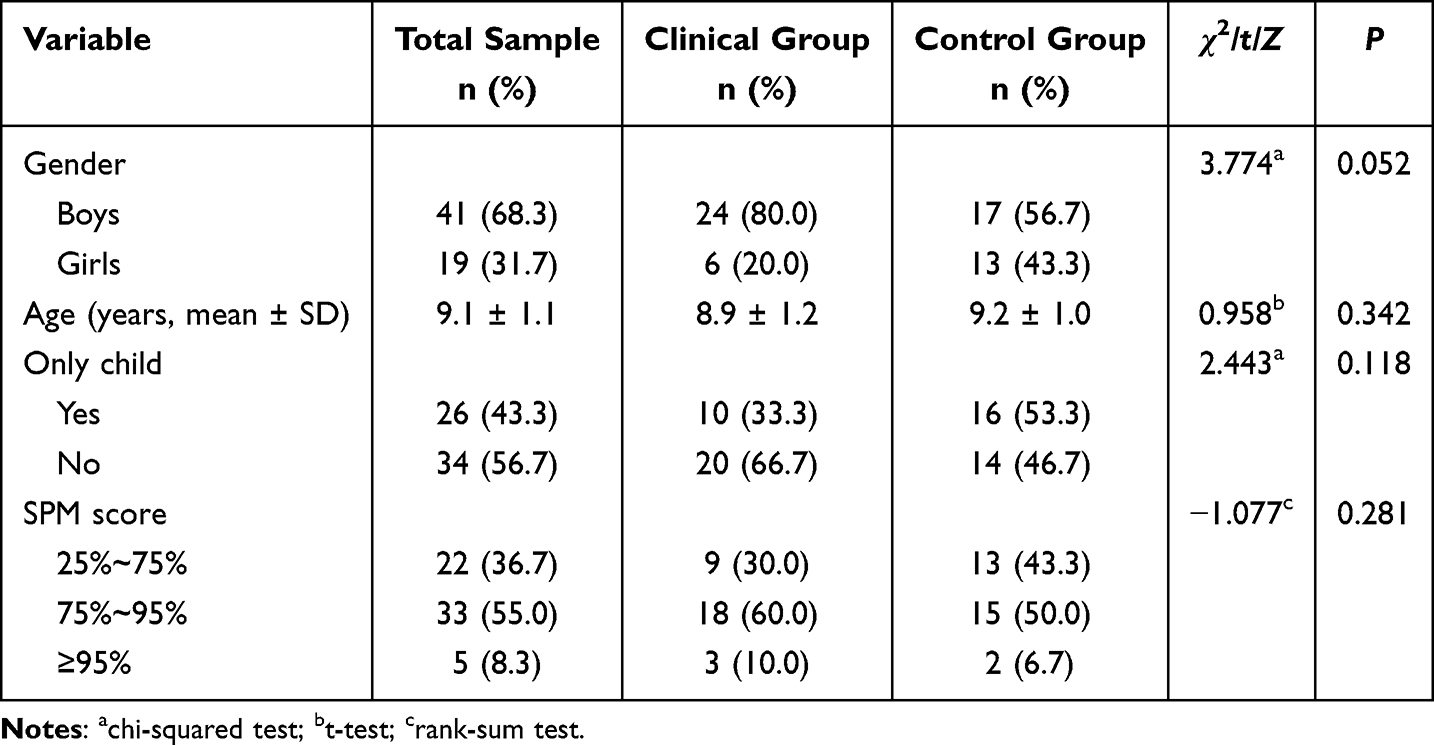 |
Table 1 Demographic and Baseline Characteristics of the ADHD and Control Groups |
Control participants were recruited from the same geographic region as the clinical group. The inclusion criteria were: (1) no history of psychiatric illness; (2) a mean subscale score ≤1 for both the inattention and hyperactivity/impulsivity subscales of the SNAP-IV. Exclusion criteria were the same as the clinical group. Thirty children were included in the control group. The mean age of the control group was 9.2 ± 1.0 years; 56.7% (17) were boys, and 43.3% (13) were girls (Table 1).
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (2025-K-472-01). Written informed consent was obtained from the parents or guardians of each child enrolled in the study.
Research Tools
Swanson Nolan and Pelham, Version IV (SNAP-IV)
The Chinese version of SNAP-IV has been validated and is widely used in clinical practice.31,32 The SNAP-IV comprises three subscales: the inattention scale (items 1 to 9), the hyperactivity/impulsivity scale (items 10 to 18), and the oppositional disobedience scale (items 19 to 26). For the purpose of this study, only the first two subscales were used. Each item is rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (very much), completed by parents. For each subscale, the item scores were summed and divided by the number of items to obtain a mean subscale score. According to previous validation studies, a mean score of 1 is the recommended cut-off value,33 which was adopted as part of the participant selection criteria in the present study.
Synthetic House-Tree-Person Drawing Test (S-HTP)
All participants were given a blank sheet of A4-sized paper, a black pen and a set of 12 shades of colored markers. They were instructed to draw a house, a tree, a person, and any additional elements they wish to include. Participants were given 10–15 minutes to complete the drawing. Erasers and replacement sheets of paper were not permitted. After completing the drawings, all participants were asked to write down their age and gender on the reverse side of the sheet. Following completion of the drawing, each participant was involved in a semi-structured interview,20 which was conducted by a trained researcher and a psychiatrist with relevant qualifications. This was to acquire their own description of the contents of the painting and the message they were trying to convey. Interview responses were transcribed and were subsequently available to raters when scoring characteristics requiring contextual interpretation.
House-Tree-Person Drawing Test Scoring System
The S-HTP scoring procedure consisted of two steps. In the first step, we included 21 drawing characteristics based on previous research16,17,34 and clinical experience. Characteristics reported to be related to impulsivity, inattention, and emotional instability were retained, whereas those primarily reflecting psychotic symptoms, neurotic traits, or unrelated personality constructs were excluded. Several characteristics frequently observed during clinical assessments of children with ADHD were also incorporated. In the second step, drawings were independently scored by two raters who had received professional training in drawing-based psychological assessment and had relevant scoring experience. The raters were blinded to participants’ diagnostic status, SNAP-IV scores, and other clinical information throughout the scoring process. To facilitate interpretation of ambiguous drawing elements, raters were allowed to refer to the post-drawing interview records, which consisted solely of the child’s descriptions and explanations of the drawings and did not contain diagnostic or clinical information. A dichotomous coding system was used (1 = present; 0 = absent). Detailed operational definitions of all drawing characteristics are provided in Supplementary Table S1. For characteristics requiring contextual interpretation (eg, “person at odds”), ratings were informed by the child’s post-drawing descriptions obtained during the drawing interview.
Data Analysis
Depending on variable type and distribution, t-tests, chi-square tests, and Mann–Whitney U-tests were used to compare demographic and baseline characteristics between groups. Inter-rater reliability for the S-HTP drawing characteristics was assessed using Cohen’s kappa coefficient. Pearson correlation analysis was used to examine the association between total S-HTP drawing scores and SNAP-IV scores. The Mann–Whitney U-test was used to compare total drawing scores between the ADHD and control groups. Chi-square tests were performed to compare the frequencies of individual drawing characteristics between groups. To reduce the risk of false-positive findings arising from multiple comparisons, FDR correction was applied to the primary group-comparison analyses. Mann–Whitney U-tests were used to examine associations between individual drawing characteristics and SNAP-IV total and subscale scores. Univariate binary logistic regression analyses were performed to examine the association between each drawing characteristic and ADHD status (ADHD = 1, control = 0). Drawing characteristics showing significant associations were subsequently entered into multivariable logistic regression analyses using a forward selection procedure. Age, gender, family structure, and SPM score were included as covariates. ROC curve analyses were conducted to evaluate the ability of individual and combined drawing characteristics to distinguish children with ADHD from healthy controls. To assess model stability and potential overfitting, bootstrap internal validation with 1000 resamples was performed for the final ROC model, and optimism-corrected AUC estimates were obtained. Statistical analyses were primarily conducted using SPSS version 26.0. FDR correction and bootstrap internal validation were performed in R version 4.5.2. A two-sided P value < 0.05 was considered statistically significant.
Results
The inter-rater reliability for the S-HTP drawing characteristics exceeded 0.600 for all characteristics except “Messy hair” (κ = 0.348, P = 0.006). This finding suggests limited reliability for the “Messy hair” indicator and should therefore be interpreted with caution. The Pearson correlation coefficient between the total drawing score and the SNAP-IV score was r = 0.342 (P = 0.008), indicating a positive association between the overall number of identified drawing characteristics and ADHD symptom severity. In addition, the Mann–Whitney U-test revealed a significant difference in total drawing scores between the ADHD group and the control group (U = 232.50, P = 0.001), with higher scores observed in the ADHD group.
The frequency of drawing characteristics and chi-square test results were shown in Table 2. In the initial analyses, six drawing characteristics differed significantly between the ADHD and control groups. After FDR correction, five characteristics remained significant: tracing in shaky lines (A3), lines jagged and not joined (A4), coloring beyond the edges (A6), brushwork in chaos (A7), and more than seven different colors (A8). Children with ADHD were more likely to exhibit A3, A4, A6, and A7, whereas A8 was less common in the ADHD group.
 |
Table 2 Comparison of Drawing Characteristics Between the Clinical and Control Groups |
The results of the rank-sum analyses examining associations between the 21 drawing characteristics and SNAP-IV scores are presented in Table 3. Children exhibiting characteristics A2, A3, A4, A6, A7, and B3 had significantly higher SNAP-IV total scores than those without these characteristics (P < 0.05), whereas children with characteristic A8 had lower scores (P < 0.001). Regarding SNAP-IV subscales, characteristics A2, A3, A4, and A8 were significantly associated with inattention scores, while A2, A3, A6, A7, and A8 were significantly associated with hyperactivity/impulsivity scores (P < 0.05). Except for A8, the presence of these characteristics was generally associated with higher symptom scores.
 |
Table 3 Comparison of Drawing Characteristics and SNAP-IV Scores Between Two Groups |
In univariate binary logistic regression analysis, six drawing features were found to be significantly associated with ADHD (P < 0.05). After controlling for gender, age, family structure, and SPM score, these characteristics remained significant (P < 0.05) (Table 4). Furthermore, a multivariate binary logistic regression model was used to consider all the selected drawing characteristics while controlling for confounding factors. As shown in Table 5, tracing in shaky lines (A3) (P = 0.036) and lines jagged and not joined (A4) (P = 0.012) were positively associated with ADHD status, whereas A8 was inversely associated with ADHD status (P = 0.014). The Hosmer-Lemeshow test indicated an acceptable model fit (χ2 = 4.909, P = 0.556).
 |
Table 4 Individual Logistic Regression Analyses of Drawing Characteristics and ADHD |
 |
Table 5 Multivariable Logistic Regression Analysis of Selected Drawing Characteristics and ADHD |
Figure 1 shows the ROC curves of the drawing characteristics. The corresponding AUCs, sensitivities, and specificities are presented in Table 6. A3 (P = 0.008), A4 (P = 0.004), and A8 (P = 0.004) demonstrated acceptable discriminatory ability, with AUCs of 0.700, 0.717, and 0.717, respectively. A combined model incorporating A3, A4, and A8 achieved an AUC of 0.835 (P < 0.001). Bootstrap internal validation using 1000 resamples yielded an optimism-corrected AUC of 0.812 (bootstrap percentile 95% CI: 0.762–0.941), suggesting acceptable model stability within the present sample. Exploratory analyses further suggested that inclusion of A6 and A7 in the combined model yielded a slightly higher AUC of 0.859. However, because these characteristics were not retained in the final multivariable logistic regression model, this finding should be interpreted cautiously and requires confirmation in larger independent samples.
 |
Table 6 Results of ROC Curve Analysis of Drawing Characteristics Associated with ADHD |
 |
Figure 1 Receiver operating characteristic curve of drawing characteristics associated with attention-deficit hyperactivity disorder. |
Discussion
This study identified several S-HTP drawing characteristics that were more frequently observed among children with ADHD than among typically developing controls. Five drawing characteristics remained significantly different between groups after FDR correction, and among these features, A3, A4, and A8 remained independently associated with ADHD status in the adjusted logistic regression analyses. ROC analyses suggested that combinations of these drawing characteristics demonstrated greater discriminatory performance than individual features alone. Although the combined model achieved an AUC of 0.835 in the present sample, bootstrap internal validation yielded an optimism-corrected AUC of 0.812, indicating that the model retained acceptable discriminatory performance after accounting for potential overfitting. These findings suggest that certain drawing characteristics may be associated with ADHD and warrant further investigation in larger, independent samples.
Children with ADHD more frequently exhibited jagged, incomplete, or unstable lines (A3, A4). Previous studies have reported impairments in fine motor coordination and handwriting performance among children with ADHD.35,36 These findings are consistent with the possibility that some drawing characteristics may be related to motor difficulties reported in previous ADHD research. Children with ADHD were also more likely to exhibit chaotic brushwork (A7), which may be related to difficulties in impulse control reported in previous studies. These drawing errors resemble those reported in free-drawing tasks among ADHD children, where poor planning and rapid execution led to decreased structural coherence.37 However, the present study did not directly assess motor function, executive functioning, or underlying neurobiological mechanisms, and therefore these interpretations should be viewed as hypotheses requiring further investigation.
An unexpected result was the reduced use of colors by children with ADHD. This finding stands in contrast to Rajabpour Azizi,16 who reported more vivid and diverse color use in ADHD drawings. The reasons for this discrepancy remain unclear. Several explanations may account for this discrepancy. First, cultural or contextual differences may influence children’s approach to drawing tasks, as prior studies were conducted in different sociocultural settings. Second, task instructions may have influenced outcomes; while previous studies emphasized creativity and expressiveness, our study focused on structural completion, possibly leading ADHD children to minimize color use to reduce task demands. Furthermore, motivational factors should also be considered. Children with ADHD often display reduced persistence in effortful tasks. It is plausible that, rather than engaging in time-consuming color choices, they opted for simplified strategies to complete the task more quickly. However, because the present study did not directly assess motivation, task engagement, or color preference, these explanations remain speculative. Further studies are needed to clarify the mechanisms underlying reduced color use in ADHD drawings.
Regarding aggressive content, previous studies have reported that children with ADHD may be more likely to include violent or aggressive elements in their drawings.17 However, such features were not significantly associated with ADHD in the present study. This discrepancy may be related to differences in sample characteristics, cultural context, or study design. Further research with larger samples is needed to clarify the relevance of aggressive drawing content to ADHD.
Collectively, these findings suggest that certain S-HTP drawing characteristics may reflect behavioral features commonly observed in children with ADHD. The S-HTP drawing task provides an additional source of behavioral information that may complement information obtained from conventional assessments. Its simplicity, low cost, and nonverbal format may make it a potentially useful source of supplementary observation for children who are reluctant or unable to articulate their emotions. Moreover, we observed that several children with ADHD exhibited off-task behaviors such as restlessness and looking around during the drawing process. Although these observations were not systematically recorded or analyzed, they suggest that the drawing process itself may provide additional behavioral information. Future research should aim to establish standardized criteria for evaluating not only the drawing product but also the drawing process itself. Incorporating behavioral observations and temporal measures may help clarify how drawing behavior differs between children with and without ADHD and may contribute to a better understanding of the potential role of drawing-based assessments in psychological evaluation.
Beyond its potential research value, the S-HTP test may provide useful qualitative information during psychological assessment. In outpatient settings, analysis of drawing content can offer insights into children’s perceptions of their family relationships and potential sources of emotional conflict, which are sometimes overlooked in parental reports. Moreover, certain drawing themes may raise questions regarding possible emotional or behavioral difficulties that warrant further assessment. Given that ADHD often co-occurs with family stress and emotional dysregulation,38 the S-HTP may provide a child-friendly context in which behavioral and emotional expressions can be observed. However, the interpretation of drawing content remains inherently subjective and should not be regarded as a stand-alone indicator of psychological functioning. Future research is needed to determine the reliability, validity, and potential applications of the S-HTP in clinical and research settings.
Despite its exploratory findings, this study has several limitations. First, the sample size was relatively small, and no formal a priori power analysis was conducted, which may have limited statistical power and contributed to instability in some effect estimates. Second, although FDR correction was applied to the primary group-comparison analyses, multiple exploratory analyses were conducted and the possibility of false-positive findings cannot be completely excluded. Third, the regression and ROC analyses were exploratory in nature. Variable selection and model evaluation were performed using the same sample, increasing the risk of overfitting and potentially yielding optimistic estimates of model performance. Although bootstrap internal validation yielded an optimism-corrected AUC of 0.812, no external validation cohort was available. Therefore, the reported discriminatory performance should be considered preliminary and requires confirmation in larger independent samples. The ROC analyses were intended to evaluate discriminatory performance rather than to establish clinically applicable screening thresholds. No pre-specified or externally validated decision thresholds were available; therefore, the reported sensitivity and specificity values should not be interpreted as clinically validated screening criteria.
In addition, although gender differences between groups were not statistically significant, the ADHD group contained a higher proportion of boys than the control group. While gender was included as a covariate in the adjusted analyses, residual confounding cannot be completely excluded, particularly given the relatively small sample size. Furthermore, participants were recruited from a single clinical center within one geographic region of China, which may limit the generalizability of the findings to other populations and settings. Although most drawing characteristics demonstrated acceptable inter-rater reliability, some indicators may still involve subjective interpretation. In particular, the characteristic “Messy hair” showed relatively low inter-rater agreement, highlighting the need for more refined operational definitions and standardized scoring procedures. Notably, this characteristic was not significantly associated with ADHD status or SNAP-IV scores and did not contribute to the subsequent regression analyses. Furthermore, the S-HTP scoring system relied primarily on dichotomous judgments of observable features and did not incorporate quantitative or process-based indices. Future studies with larger and more diverse samples, including clinically relevant comparison groups, should establish standardized scoring systems, evaluate drawing processes in greater detail, and further examine the reliability, validity, specificity, and potential applications of the S-HTP in both research and clinical settings.
Conclusion
Research on the application of the S-HTP drawing test in ADHD remains limited. In the present study, several drawing characteristics were observed more frequently in children with ADHD than in typically developing controls and were associated with ADHD symptom severity. Among these features, A3 (tracing in shaky lines), A4 (lines jagged and not joined), and A8 (more than seven different colors) remained associated with ADHD status in the exploratory regression analyses. These findings suggest that certain drawing characteristics may provide additional information regarding behavioral features commonly observed in children with ADHD. However, given the exploratory nature of the study, the small sample size, and the lack of external validation, further research in larger independent samples is required before the clinical utility of these findings can be established.
Abbreviations
ADHD, attention-deficit hyperactivity disorder; S-HTP, Synthetic House-Tree-Person Drawing Test; SNAP-IV, Swanson, Nolan, and Pelham, Version IV; SPM, Standard Progressive Matrices; ROC, receiver operating characteristic curve; AUC, area under the curve.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Ethics Statement
The study was approved by the Ethics Committee of The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (2025-K-472-01). Written informed consent was obtained from the parents or guardian of each child enrolled in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Online Course Construction and Teaching Research Program for Graduate Students in Medicine and Pharmacy (B_YXC2024-02-03_10), the Second Batch of Provincial Graduate Teaching Reform Projects during the 14th Five-Year Plan Period in Zhejiang Province (JGCG2024303), the “Social Sciences Empowering High-Quality Development in Wenzhou” Special Research Project (Project No. 44), and The Summit Advancement Disciplines of Zhejiang Province (Wenzhou Medical University – Pharmaceutics).
Disclosure
Dr Rong Huang reports patents issued for a device for rehabilitation training of children with ADHD and a device for auxiliary detection and attention training of ADHD. The authors declare no other competing interests in this work.
References
1. Luo Y, Weibman D, Halperin JM, Li X. A review of heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD). Front Hum Neurosci. 2019;13:42. doi:10.3389/fnhum.2019.00042
2. Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–12. doi:10.1542/peds.2014-3482
3. Liu A, Xu Y, Yan Q, Tong L. The prevalence of attention deficit/hyperactivity disorder among Chinese children and adolescents. Sci Rep. 2018;8(1):11169. doi:10.1038/s41598-018-29488-2
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Vol. 5. Washington, DC: American Psychiatric Association; 2013.
5. Faraone SV, Rostain AL, Blader J, et al. Practitioner Review: emotional dysregulation in attention-deficit/hyperactivity disorder - implications for clinical recognition and intervention. J Child Psychol Psychiatr. 2019;60(2):133–150. doi:10.1111/jcpp.12899
6. Rajaprakash M, Leppert ML. Attention-deficit/hyperactivity disorder. Pediatr Rev. 2022;43(3):135–147. doi:10.1542/pir.2020-000612
7. Ren Y, Fang X, Fang H, et al. Predicting the adult clinical and academic outcomes in boys with ADHD: a 7- to 10-year follow-up study in China. Front Pediatr. 2021;9:634633. doi:10.3389/fped.2021.634633
8. Roy A, Hechtman L, Arnold LE, et al. Childhood predictors of adult functional outcomes in the multimodal treatment study of Attention-Deficit/Hyperactivity Disorder (MTA). J Am Acad Child Adolesc Psychiatry. 2017;56(8):687–695.e687. doi:10.1016/j.jaac.2017.05.020
9. Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet. 2016;387(10024):1240–1250. doi:10.1016/S0140-6736(15)00238-X
10. De Los Reyes A, Augenstein TM, Wang M, et al. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol Bull. 2015;141(4):858–900. doi:10.1037/a0038498
11. Raiker JS, Freeman AJ, Perez-Algorta G, Frazier TW, Findling RL, Youngstrom EA. Accuracy of achenbach scales in the screening of attention-deficit/hyperactivity disorder in a community mental health clinic. J Am Acad Child Adolesc Psychiatry. 2017;56(5):401–409. doi:10.1016/j.jaac.2017.02.007
12. Conners CK. Conners’ rating scales-revised. 1997.
13. Swanson J, Deutsch C, Cantwell D, et al. Genes and attention-deficit hyperactivity disorder. Clin Neurosci Res. 2001;1(3):207–216. doi:10.1016/S1566-2772(01)00007-X
14. May T, Birch E, Chaves K, et al. The Australian evidence-based clinical practice guideline for attention deficit hyperactivity disorder. Aust N Z J Psychiatry. 2023;57(8):1101–1116. doi:10.1177/00048674231166329
15. Perets-Dubrovsky S, Kaveh M, Deutsh-Castel T, Cohen A, Tirosh E. The human figure drawing as related to attention-deficit hyperactivity disorder (ADHD). J Child Neurol. 2010;25(6):689–693. doi:10.1177/0883073809344122
16. Rajabpour Azizi M, Rajabpour Azizi Z, Akhavan Tafti M, Mohamadzadeh S. Comparing the graphic performance of students with and without SLDs and ADHD based on FEATS. Art Therapy. 2022;39(3):146–156. doi:10.1080/07421656.2022.2030621
17. Haghighi M, Khaterizadeh M, Chalbianloo G, Toobaei S, Ghanizadeh A. Comparing the drawings of children with attention deficit hyperactivity disorder with normal children. Iran J Psychiatry. 2014;9(4):222–227.
18. Gu S, Liu Y, Liang F, et al. Screening depressive disorders with tree-drawing test. Front Psychol. 2020;11:1446. doi:10.3389/fpsyg.2020.01446
19. Rorschach H. Psychodiagnostics. 1942.
20. Buck JN. The HTP test. J Clin Psychol. 1948;4(2):151–159. doi:10.1002/1097-4679(194804)4:2<151::AID-JCLP2270040203>3.0.CO;2-O
21. Mikami N. The S-HTP technique: the clinical and developmental approach in Synthetic-H–T–P Test. Seishinshobo, Tokyo; 1995.
22. Guo H, Feng B, Ma Y, et al. Analysis of the screening and predicting characteristics of the house-tree-person drawing test for mental disorders: a systematic review and meta-analysis. Front Psychiatry. 2022;13:1041770. doi:10.3389/fpsyt.2022.1041770
23. Soll BMB, Brandelli Costa A, Vaitses Fontanari AM, et al. Use of the house-tree-person projective drawings and parental styles inventory in the global psychological evaluation of transgender youth who seek healthcare at the gender identity program. Front Psychol. 2019;10:2488. doi:10.3389/fpsyg.2019.02488
24. Roysircar G, O’Grady K. Children’s disaster trauma in Haiti: configurations of similarities and dissimilarities in experiences. Psychol Serv. 2022;19(4):698–709. doi:10.1037/ser0000569
25. Yang G, Zhao L, Sheng L. Association of synthetic house-tree-person drawing test and depression in cancer patients. Biomed Res Int. 2019;2019:1478634. doi:10.1155/2019/1478634
26. Sheng L, Yang G, Pan Q, Xia C, Zhao L. Synthetic house-tree-person drawing test: a new method for screening anxiety in cancer patients. J Oncol. 2019;2019:5062394. doi:10.1155/2019/5062394
27. Li D, Luo X, Dang C, et al. Impaired sensory-motor integration in children with attention-deficit/hyperactivity disorder during visual search. J Child Psychol Psychiatr. 2025;67:17–26. doi:10.1111/jcpp.70004
28. Bowler A, Arichi T, Fearon P, et al. Phenotypic and genetic associations between preschool fine motor skills and later neurodevelopment, psychopathology, and educational achievement. Biol Psychiatry. 2024;95(9):849–858. doi:10.1016/j.biopsych.2023.11.017
29. Sheehan DV, Sheehan KH, Shytle RD, et al. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J Clin Psychiatry. 2010;71(3):313–326. doi:10.4088/JCP.09m05305whi
30. Zhang H, Wang X. Raven’s standard progressive matrices revised in China. Acta Psychologica Sinica. 1989;21:113–120.
31. Gau SSF, Shang CY, Liu SK, et al. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, version IV scale–parent form. Int J Methods Psychiatr Res. 2008;17(1):35–44. doi:10.1002/mpr.237
32. Zhou J, Guo L, Chen Y. Reliability and validity of the Chinese version of Swanson, Nolan, and PelhamVersion IV Rating Scale-Parent Form for attention-deficit/hyperactivity disorder. Chin Ment Heal J. 2013;27:424–428.
33. Yin H, Yang D, Yang L, Wu G. Relationship between sleep disorders and attention-deficit-hyperactivity disorder in children. Front Pediatr. 2022;10:919572. doi:10.3389/fped.2022.919572
34. Marzolf SS, Kirchner JH. House-Tree-Person drawings and personality traits. J Pers Assess. 1972;36(2):148–165. doi:10.1080/00223891.1972.10119740
35. Borella E, Chicherio C, Re AM, Sensini V, Cornoldi C. Increased intraindividual variability is a marker of ADHD but also of dyslexia: a study on handwriting. Brain Cogn. 2011;77(1):33–39. doi:10.1016/j.bandc.2011.06.005
36. Muñoz-Organero M, Powell L, Heller B, Harpin V, Parker J. Automatic extraction and detection of characteristic movement patterns in children with ADHD based on a Convolutional Neural Network (CNN) and acceleration images. Sensors. 2018;18(11):3924. doi:10.3390/s18113924
37. Hyde C, Sciberras E, Efron D, Fuelscher I, Silk T. Reduced fine motor competence in children with ADHD is associated with atypical microstructural organization within the superior longitudinal fasciculus. Brain Imaging Behav. 2021;15(2):727–737. doi:10.1007/s11682-020-00280-z
38. Copeland W, Shanahan L, Costello EJ, Angold A. Configurations of common childhood psychosocial risk factors. J Child Psychol Psychiatr. 2009;50(4):451–459. doi:10.1111/j.1469-7610.2008.02005.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Improving Diagnostic Strategies for Pediatric Anxiety Disorders: Advice for the Clinician
Hilliard W, Kearney K, Lucas S, Flores MED
Psychology Research and Behavior Management 2024, 17:4035-4042
Published Date: 25 November 2024
The ADHD Assessment Quality Assurance Standard for Children and Teenagers (CAAQAS)

Young S, Absoud M, Al-Attar Z, Ani C, Colley W, Cortese S, Crame J, Gudjonsson G, Hill P, Hollingdale J, Mukherjee RAS, Ozer S, Partridge G, Smith J, Woodhouse EL, Lewis A
Neuropsychiatric Disease and Treatment 2024, 20:2603-2628
Published Date: 24 December 2024