Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Dose Escalation Patterns and Associated Costs of Advanced Therapies for Ulcerative Colitis in France and the United Kingdom: A Retrospective Database Analysis
Authors Treuer T, Richards M ![]() , Mert C, Dhesi E
, Mert C, Dhesi E ![]() , Silva L, Tan Y
, Silva L, Tan Y ![]() , Hoque S
, Hoque S
Received 10 September 2024
Accepted for publication 30 January 2025
Published 1 March 2025 Volume 2025:17 Pages 129—146
DOI https://doi.org/10.2147/CEOR.S481730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Tamás Treuer,1 Melissa Richards,1 Can Mert,2 Endip Dhesi,1 Lidia Silva,3 Yubo Tan,4 Sami Hoque5
1International Medical Affairs, Eli Lilly and Company, Indianapolis, IN, USA; 2Statistics, HaaPACS GmbH, Schriesheim, Germany; 3RWE, TFS HealthScience, Madrid, Spain; 4Biostatistics, TFS HealthScience, Toronto, Canada; 5Gastroenterology, Barts Health NHS Trust, London, UK
Correspondence: Tamás Treuer, Eli Lilly and Company, 893 Delaware Street, Indianapolis, IN, USA, Email [email protected]
Background: Dose escalation to optimize advanced therapies is common in ulcerative colitis (UC) to avoid intra-class or inter-class drug switching and maintain clinical response and has impact on costs. Given the limited real-world data available, this study aims to understand real-world dose escalation UC advanced therapies patterns in France and United Kingdom [UK].
Methods: Retrospective study in adult patients with moderate-to-severe UC starting an advanced UC therapy (adalimumab [ADA], golimumab [GOL], infliximab [IFX], tofacitinib [TOF], ustekinumab [UST], or vedolizumab [VED]) with first prescription (and/or dispensation for France) between January 2017 and February 2022 (ie advanced UC therapy new users, by excluding patients who used any of these drugs in the previous 12 months to their index date). Proportions of patients with dose escalation/de-escalation (± 20% versus Summary of Product Characteristics) after maintenance date were estimated using Kaplan–Meier (KM) survival analyses. Clinical response, healthcare resource utilization (HRU) and direct costs related to UC were also analyzed.
Results: Within 6 months after start of maintenance, rate of at least one dose escalation was 74.1%. Overall, 83.9– 89% of patients had dose escalation within the 12– 24 months, respectively, and 61.6% had clinical response [ranging from 56.3% (ADA) to 77.0% (IFX)]. Direct annual HRU costs related to UC ranged between 7426 (IFX) EUR and 22,265 (UST) in France, with mean 11,181 EUR in the dose-escalation group vs 8323 EUR in the de-escalation group (+11.5%). In the UK costs ranged between 5006 (ADA) EUR and 11,975 (UST).
Conclusion: Dose escalation of UC advanced therapies is a common strategy to avoid treatment-switching. Despite dose escalations and their cost to the system, a proportion of patients fail to achieve clinical response. This study highlights the need for more efficacious, durable treatments for moderate-to-severe UC patients, as the initiation of the advanced therapies did not reduce overall systemic/rectal corticosteroid burden.
Keywords: ulcerative colitis, dose escalation, biologics, economic cost, healthcare resource use (HRU)
Introduction
Ulcerative colitis (UC) is an inflammatory bowel disease (IBD) that affects the large intestine (colon and rectum)1 and causes inflammation and ulcers2,3 leading to various debilitating symptoms such as diarrhea, rectal bleeding, bowel urgency, and abdominal pain impacting patient’s quality of life. A characteristic feature of UC is that the disease typically occurs in relapses, with periods of relief (remission) and relapsing acute episodes (acute flare-ups including abdominal cramps and bloody diarrhea) of inflammation limited to the mucosal layer of the colon.3
A study carried out in 2013 estimated the prevalence of UC in Europe between 2.4 and 294 per 100,000 persons, or 1.5 million persons affected by the disease. The incidence and prevalence of this disease continues to rise, resulting in ever-increasing care costs.4 The UC treatment strategy is mainly based on disease severity, and the goal is to induce and maintain long-term remission.2,3,5 Several treatments are available: from the first-line conventional therapies (corticosteroids, 5-aminosalicylates, and immunomodulators such as azathioprine)6 to advanced therapies (biologic therapies and oral small molecules). Advanced therapies are typically recommended when patients with moderate-to-severe UC have an inadequate response to conventional therapy, loss of response, or intolerance to conventional therapy or to another biologic.5 Additionally, up to 30% of UC patients have primary non-response to biologics or small molecules.7,8 While on treatment, due to the nature of the disease and development of antibodies to the biologics, the effectiveness of biologic therapies may decrease over time.9 Among those who respond to biologic therapies, previous studies have indicated that 20–37% of patients lose response over time, with immunogenicity being the leading contributor.10,11
Optimization of UC advanced therapies in terms of dosing, treatment switching, and use of concomitantly prescribed agents have frequently been observed,12 even in patients who achieved clinical remission in the 12 months after therapy initiation.9 This strategy has the advantage of potentially preventing intra-class or inter-class drug switching and maintaining remission. However, dose escalation of advanced therapies has an impact on healthcare resource utilization (HRU) and costs. Different indicators, based on changes in treatment patterns and HRU have been validated as meaningful quality measures for real-world efficacy retrospective analysis of medical records.9 In addition, it has been shown that the data on dose escalation levels, and associated clinical outcomes could be used as the basis for an economic analysis of dose escalation and treatment switching.13
Given the emergence of novel therapeutic approaches to UC in recent years, further studies are needed to assess the impact of UC treatment selection in real-world settings. New therapeutic options available in 2024, such as Etrasimod, Upadacitinib, and Mirikizumab, target different pathways involved in the disease’s pathogenesis14 as opposed to traditional biologic advanced therapies (adalimumab [ADA], golimumab [GOL], infliximab [IFX], tofacitinib [TOF], ustekinumab [UST], and vedolizumab [VED]). Etrasimod, a selective sphingosine 1-phosphate (S1P) receptor modulator, reduces lymphocyte migration to the inflamed gut, thereby decreasing inflammation and promoting mucosal healing. Upadacitinib, a Janus kinase (JAK) inhibitor, selectively targets JAK1 to reduce inflammation, while Mirikizumab, an anti-IL-23 monoclonal antibody, targets the IL-23 cytokine involved in the inflammatory process. These drugs offer improved efficacy, better safety profiles, and greater convenience, providing new hope for UC patients with limited treatment options. To provide better context on real-world dose escalation/de-escalation patterns of traditional biologic advanced therapies just before the availability of these newer drugs, we conducted a retrospective database study in 2023 among patients with moderate-to-severe UC in selected European countries (France and the United Kingdom [UK]). A new-user design was chosen, ie prior use of a biologic treatment was excluded in the 12 months prior to the index date, in order to be able to properly compare the sub-cohorts. The advantages over a prevalent-user design are to minimize potential immortal time bias and treatment/channeling bias, in line with ISPOR Guidelines for comparative effectiveness.15 Secondary study objectives included: 1) to describe clinical characteristics of patients initiating UC advanced drugs in clinical practice; 2) to explore factors predicting dose escalations; 3) to describe the clinical response and the UC-related HRU during the study period; and 4) to estimate annual direct medical costs due to UC in this population.
Materials and Methods
Study Design and Source of Data
This was a retrospective cohort study, based on a subset of patients from The Health Improvement Network (THIN®) database in France and UK. THIN® includes only fully anonymized data (sociodemographic data, disease diagnoses [described using Read codes], diagnostic/laboratory tests, referrals, and drugs prescriptions issued by the physicians) from electronic medical records (EMR) collected voluntarily at the physicians-level and coded using the International Classification of Diseases, 10th Revision (ICD-10) codes.
The research database, THIN®, obtained ethical approval from the French National Data Protection Authority (CNIL) for data collection since 2002. In the UK, ethical approval was granted by the NHS South-East Multicenter Research Ethics Committee in 2003 (ref: 03/01/073) for establishment of the THIN® database, and the approval was extended in 2011 and 2020 (ref: 20/SC/0011). As this was a retrospective study using only fully anonymized patient data, no additional ethical approval was required in these countries, as it no longer constitutes personal data under the UK Data Protection Act 2018 and the Health Research Authority (HRA) Policy, in UK, and under the French Data Protection Act and French Code of Public Health, in France.
Since there are limited data sources available for the purpose of the study objectives within these countries, THIN® was chosen. THIN® France data has been routinely collected by 2000 General Practitioners (GPs) and by hospital specialists, including 130 gastroenterologists, covering more than 4.8 million patients per year. While THIN® UK data has been collected by around 850 GPs (including specialist referrals), covering more than 2.6 million patients per year.
Patient Selection
The study cohort included adult patients (≥18 years) starting a UC advanced therapy (index date) from January 1, 2017, to February 23, 2022, and with prior UC diagnosis. Patients were required to be new-users, ie they should have not received any biologic UC advanced therapy within 12 months prior to their index date. Therapies of interest were: adalimumab [ADA], golimumab [GOL], infliximab [IFX], tofacitinib [TOF], ustekinumab [UST], and vedolizumab [VED]. New users of UC advanced therapies were identified based on the first prescription (and/or dispensation in France) of these drugs of interest (recorded in their electronic health records (EHRs)) between January 2017 and February 2022. UC diagnosis was identified by the local codes in THIN® France and THIN® UK (Supplementary Table 1). All patients included in this study had been previously treated with conventional systemic therapies for UC before starting UC advanced therapies.
In addition, patients were required to have at least 12 months of data in the EHR system prior to the UC advanced therapy start and have data entered in the EHR after UC advanced therapy start. All available patient data up to February 27, 2023, was extracted.
Patients were excluded from the analysis if they had any of the following: a diagnosis of an alternative indication of the index therapy drug prior to the index date, prescription or dispensation for any of the UC advanced therapies of interest in the 12-month prior to the first prescription period, prescription or dispensation for a second UC advanced therapy drug at index date.
Study Period
The index date was the first prescription date of any of the UC advanced therapy drugs of interest. The observation period for case identification (new users of UC advanced therapies) in the THIN® database ranged between January 2017 and February 2022. The baseline period (covariate assessment period) comprised 12 months prior to the index date, ranging from January 2016 to February 2022. The follow-up period (outcome assessment period) comprised the period to collect outcomes information from index date up to last date of recorded patient activity on the EHR, death, or end of data availability, whichever occurred first, ranging January 2017 to February 2023. The complete study period was from baseline period until end of follow-up period (from January 1, 2016, and February 27, 2023).
Statistical Analysis
Data were collected and analyzed at baseline, at maintenance date (after induction period of each advanced therapy drug, see Supplementary Table 2), and every 6 months after maintenance date until end of follow-up. Descriptive analyses were performed for all baseline demographic and clinical characteristics and outcomes of interest. For continuous variables, the distribution of each of the study variables was summarized in terms of the mean, standard deviation (SD), median, and range of values. For categorical variables, the number and proportion at each level of the variable, with 95% confidence intervals (CI) around the proportion, were reported. Time-to-event outcomes were analyzed by using Kaplan–Meier (KM) survival function. Multivariate Cox regression was used to compare dose escalation between treatments. Inverse propensity score weights (IPTW) were used to balance the cohorts by their baseline and clinical characteristics (age, weight, gender, index year, prior and concomitant medications, comorbidities, erythrocyte sedimentation rate [ESR], and hemoglobin). IPTW was calculated using a logistic regression model for multiple treatment groups.16
In the main analyses, missing data were not imputed (observed case approach). Only for clinical response and dose escalation/de-escalation analysis, a “non-responder imputation” (NRI) was performed.
Patients were followed in an “as-treated” (AT) approach from their index date until the occurrence of earliest of the following: discontinuation of UC advanced therapy (defined as a gap of 60 days in continuous exposure, ie from end of last supply to start of subsequent supply), switch/addition of another UC advanced therapy, death, end of follow-up (defined as a gap of 60 days without having any healthcare data registered), end of data source availability (up to February 27, 2023). In the analysis of UC-related HRU and direct costs by country, patients were followed in an “intention to treat” (ITT) manner, ie without excluding information after discontinuation or switch of UC Advanced therapy, to allow assessment of the 12-month impact.
All analyses were conducted using commercially available statistical software (SAS version 9.2; SAS Institute Inc., Cary, NC, USA).
Baseline characteristics included: age (at index date), gender, race (only for UK, not available for France), height, weight, prior and concomitant medication (at index date), prior UC therapies (and duration) and associated comorbidities.
UC patients’ exposure was assessed during the induction period and during the maintenance period independently. The induction period was calculated based on the induction period specified in the Summary of Product Characteristics (SPC) of the UC drugs (Supplementary Table 2). The maintenance period was calculated from the index date.
Assessment of Dose Escalation
Escalation or de-escalation was determined by comparing the prescribed daily dose with the lowest SPC recommended daily dose during the maintenance period for adult patients with UC. Consequently, a patient might undergo multiple escalations and de-escalations during the follow-up period (non-excluding events). Any increase or decrease of at least 20% of the dose (due to dose increase/decrease or change in dosing interval/schedule) during the maintenance period compared to the recommended dose in the SPC was considered dose escalation or de-escalation, respectively. For infliximab, since dosing is weight-based, in case weight was not available from data source, the index dose was used to derive an average daily baseline maintenance dose. This was calculated by dividing the total quantity prescribed at index day by 56 (based on the labelled maintenance dose frequency of 8 weeks, or 56 days).
Daily dose calculation used details from the prescription (including number of boxes, duration, frequency, quantity, and other labelling information). Daily dose (mg/day) was computed using two methods. When both the number of boxes ( ) and duration of the prescription (
) and duration of the prescription ( ) were recorded:
) were recorded:
Where  referred to the amount of drug substance in mg per box.
referred to the amount of drug substance in mg per box.
If the duration of the prescription was missing, it was estimated based on the days until the next identical prescription. Due to the nature of the prescription, the estimated duration was rounded to the nearest full week, imputing the duration in increments of 7 days. When the number of boxes was missing in the prescription, daily dose was calculated as:
where  represented the prescribed quantity (number of syringes, tablets, etc, depending on the drug product),
represented the prescribed quantity (number of syringes, tablets, etc, depending on the drug product),  was the amount of drug substance for each unit, and
was the amount of drug substance for each unit, and  was the prescribed frequency in days for taking the drugs, for example, weekly (7 days), bi-weekly (14 days), or monthly (30 days).
was the prescribed frequency in days for taking the drugs, for example, weekly (7 days), bi-weekly (14 days), or monthly (30 days).
According to the definition of the variables in the dataset, the daily doses calculated from these two formulas should ideally be identical. If daily dose could be calculated through either method, and if there were discrepancies between the two calculated doses, the dose closer to the SPC recommended dose was selected.
For patients with repeated prescriptions with the same product, if the daily dose could not be computed for certain entries, a carry-forward imputation method was applied. Any prescriptions where the daily dose could not be determined by either formula or carried forward was marked as missing. There were no alternative imputation methods utilized in this analysis.
The proportion of patients with dose escalation during the maintenance period, therefore excluding the induction period, was assessed. While the SPC can suggest different doses, primary analyses were based on a less stringent criteria for dose escalation/de-escalation, and the lowest SPC recommended dose for the maintenance period was used to identify the dose escalation/de-escalation; as a sensitivity analysis, a more stringent criterion was applied by using the highest SPC dose as reference (Supplementary Table 3). For the subgroup analyses, patients with at least one escalation in the first 6 months were categorized into the escalation group, even if they experienced several dose de-escalations during this time. Conversely, patients without any escalations but with at least one de-escalation in the first 6 months were placed in the de-escalation group. Those without escalation or de-escalations were considered to have a stable dose.
Clinical Response
Responders to a UC advanced therapy drug were defined as patients with all three following surrogate endpoints: no hospitalization related to UC nor colectomy; no treatment discontinuation, no switch to or addition of another UC advanced therapy; and no exposure to systemic corticosteroids. The proportion of patients with clinical response was assessed at maintenance date and every 6 months thereafter until the end of data availability.
UC-Related Healthcare Resource Utilization and Direct Costs
Healthcare resource utilization (HRU) (UC-related consultations, hospitalizations, ER admissions, diagnostic tests, UC drugs, and non-drug interventions [eg dietary, lifestyle]) during the study period (ITT-approach) was described as number and proportion of subjects with at least 1 use and, among these, mean (SD) number of uses. Direct yearly costs were then estimated by applying unit costs to each patient´s HRU and described separately by country and index therapy cohort, when possible (Supplementary Table 4). To account for the censoring bias due to patients lost to follow-up, and in order to be able to estimate the yearly cost per patient with minimum bias, Lin’s method,17 which utilizes Kaplan–Meier survival estimates for re-weighting, was employed. In this approach, the yearly cost per patient was derived by averaging monthly costs, each weighted by the likelihood of survival for that specific month. More specifically, the full follow-up period was divided into K months and the weighted yearly average for HRU was calculated as

Where  is the survival probability estimated from Kaplan–Meier estimator for the kth month after index date and
is the survival probability estimated from Kaplan–Meier estimator for the kth month after index date and  is the estimated cost averaged across patients still under study. In this study, patients were assumed to be censored at the end of each month. Using the formula above, two approaches were applied to estimate the yearly cost. In the first approach, the monthly cost was calculated solely based on patients who had experienced at least one HRU event. In the second approach, costs were averaged across all patients who remained in the study (with any HRU data available). The costs were additionally examined both by individual HRUs and in aggregate. Given that the survival analysis was based on the overall follow-up status of patients, the survival probabilities estimated for the calculations remained consistent across all types of HRUs. Direct UC-related costs were also estimated by subgroups based on dose escalation/de-escalation/stable dose during the AT follow-up, when the dose information was available.
is the estimated cost averaged across patients still under study. In this study, patients were assumed to be censored at the end of each month. Using the formula above, two approaches were applied to estimate the yearly cost. In the first approach, the monthly cost was calculated solely based on patients who had experienced at least one HRU event. In the second approach, costs were averaged across all patients who remained in the study (with any HRU data available). The costs were additionally examined both by individual HRUs and in aggregate. Given that the survival analysis was based on the overall follow-up status of patients, the survival probabilities estimated for the calculations remained consistent across all types of HRUs. Direct UC-related costs were also estimated by subgroups based on dose escalation/de-escalation/stable dose during the AT follow-up, when the dose information was available.
Results
Figure 1 summarizes the patient disposition. Of the 2446 patients with UC diagnosis in the THIN® database between January 2017 and February 2022, 1663 (68%) patients met the eligibility criteria (777 and 886 patients for UK and France, respectively). The mean (SD) follow-up time was 155 (259) days in the AT approach, and 462 (488) days in the ITT approach (Supplementary Table 5). Only 26.6% of patients in the UK were still on follow-up at the start of maintenance, compared to 71.2% in France. Beyond 6 months, the main reason for study drop-out was discontinued follow-up (Figure 1).
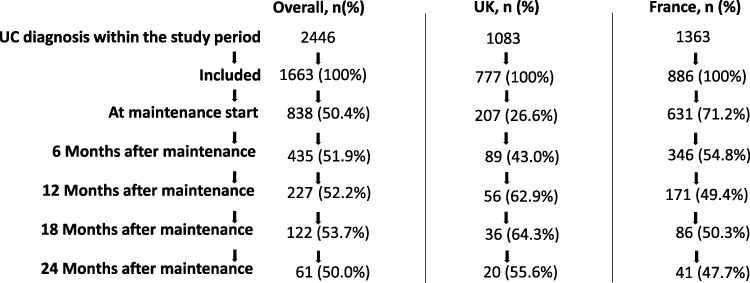 |
Figure 1 Cohort Flow Diagram by Countries. |
Baseline Characteristics
Patient demographics, comorbidities, and concomitant medications, by treatment cohort, are shown in Table 1. Overall, all treatment cohorts were similar in mean (SD) age (range from 43 (15.6) IFX to 47 (18.5) years old VED), and female/male distribution (from 44.6% to 56.8% of females in IFX and GOL, respectively). Most patients initiated the index UC therapy drug in 2020–2021 (942 [56.6%] patients). The number of patients initiating UC therapy drug increased through time reaching a peak in 2021 (545 [32.8%] patients). Prior and concomitant UC therapies prescribed at index date were similar among treatment cohorts. Main prior and concomitant therapy taken was systemic/rectal corticosteroids (913 [55.0%] and 875 [52.6%] patients, respectively). A total of 1240 [75.0%] patients had no comorbidity in their medical records and 414 (25.0%) had any comorbidities. Mean time between symptoms onset and UC diagnosis was 377 (433) days (Table 1).
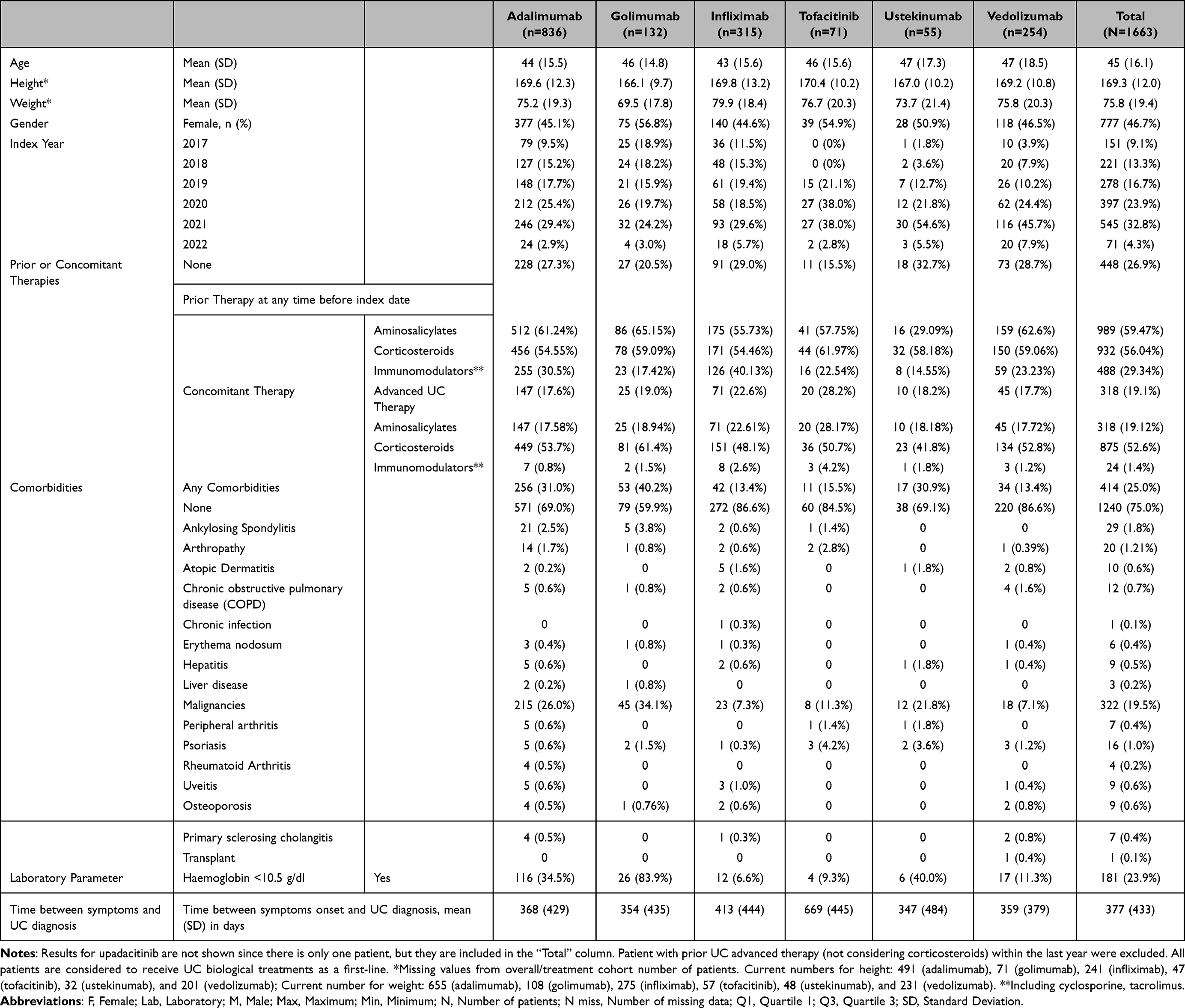 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients Starting First-Line UC Advanced Therapies in France and in UK Between January 2017 and February 2022 |
Dose Escalations and De-Escalations
Within the first 6 months after the start of maintenance period, KM-estimated mean (95% CI) rates of at least one dose escalation and at least one dose de-escalation were 74.1% (71.2–77.1%) and 57.8% (54.5–61.1%), respectively (Figure 2A and Supplementary Figure 1A). Overall, only 14.5% of subjects did not have any escalation or de-escalation (stable dose). Within the first 12 months after start of maintenance period, KM-estimated rate of at least one dose escalation was 83.9%. Dose escalation rates were higher in patients initiating UST, GOL, and ADA whereas patients initiating IFX showed the lowest rate (Figure 2A). At 18 months, all patients (100%) with UST had a dose escalation, and all patients treated with GOL and TOF had a dose escalation by 24 months (Figure 2A). For dose de-escalation, the highest rate was observed with IFX and ADA whereas patients initiating UST showed the lowest rate of dose de-escalation (Supplementary Figure 1A). Up to 24 months, 89% of patients (range 33% [IFX] to 100% [GOL, TOF, and UST]) had dose escalation, with a median % dose increase ranging from +15% [VED] to +198% [GOL] (Figure 2A).
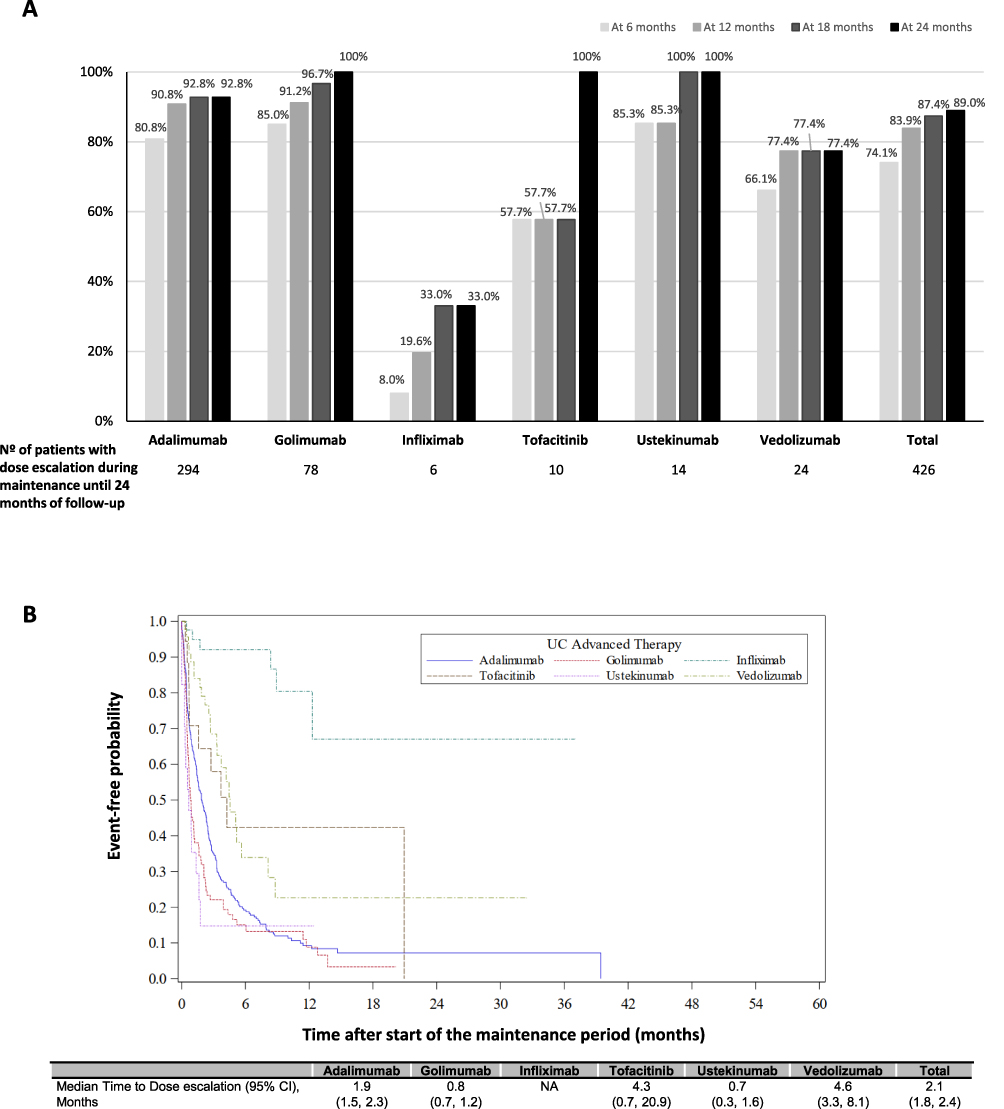 |
Figure 2 (A) Kaplan Meier (KM)-estimated percentages of patients with dose escalation (ie, received an average daily dose >20% higher than specified in the label) during the maintenance phase until 24 months of follow-up, by treatment cohort (As-Treated [AT] approach). (B) KM Curve for Time to First Dose Escalation by treatment cohort (AT approach). |
With the more stringent criteria (ie versus highest recommended dose in the SPC), dose escalation and de-escalation rates at 6 months were 36.0% and 83.7%, respectively (Supplementary Figure 2).
Kaplan–Meier (KM) estimates of overall median (95% CI) time before first dose escalation and de-escalation were 2.1 (1.8, 2.4), and 4.0 (3.1, 4.5) months, respectively. While the median time before first dose escalation for IFX was not estimable due to lack of events, for other therapies, the shortest median time to dose escalation was found in the UST cohort (0.7 [0.3–1.6] months), and the longest time in the VED cohort (4.6 [3.3–8.1] months) (Figure 2B). Regarding dose de-escalation, the shortest time observed in the IFX, and the longest in the GOL (Supplementary Figure 1B). After discontinuation of the index UC drug, 110 subjects (17.8% of the total sample and 48.5% of patients under follow-up at 12 months post-maintenance) received a subsequent line of advanced therapy, of whom 79 (72%) required at least one dose escalation.
Factors Associated with Dose Escalation
In a multivariate Cox model predicting the risk of first-dose escalation, pairwise comparisons between all advanced therapies drugs were performed, adjusting also by additional confounders (only the use of concomitant medication remained as independent predictor factor). Using IPTW to adjust for potential baseline confounding, ADA and GOL were significantly associated with higher risk of dose escalation vs IFX (HR [95% CI]: 17.9 [5.5,58.1], and 23.5 [7.1,77.8], respectively) and vs VED (HR [95% CI]: 2.8 [1.4,5.3], and 3.7 [1.8,7.3], respectively); UST was associated with higher risk vs VED (HR [95% CI]: 9.0 [3.6,22.7]). ADA and GOL were significantly (p<0.05) associated with lower risk of dose escalation vs UST (HR [95% CI]: 0.3 [0.2,0.6], and 0.4 [0.2,0.8], respectively); IFX vs TOF, UST, and VED (HR [95% CI]: 0.1 [0.02,0.4], 0.02 [0.00,0.1], and 02 [0.04,0.6], respectively); and TOF vs UST (HR [95% CI]: 0.2 [0.1,0.6]). Having at least 1 concomitant UC medication was associated with 40% higher risk of dose escalation (HR [95% CI]: 1.4 [1.1, 1.8]) (Supplementary Table 6).
Clinical Response
Overall, 516 (61.6%) patients achieved clinical response definition (no UC-related hospitalization, no colectomy; no treatment discontinuation/switch or addition of another UC advanced therapy; and no systemic corticosteroids exposure) during the study. Up to 6 months after maintenance start, 571 (68.1%) out of 838 patients had clinical response to UC advanced therapies. Proportions of patients with clinical response, based on the number of patients in study at each time point, increased up to 18 months and remained stable afterwards (Table 2). For patients with at least one escalation, 58.2% experienced a clinical response (range from 50.7% [GOL] to 77.8% [TOF]) during the whole study follow-up; for patients with no escalation, a similar percentage was observed (56% overall; range from 43.8% [ADA] to 83.3% [TOF]) (Figure 3). A total of 52.6% of patients were treated concomitantly with systemic/rectal corticosteroids during UC advanced therapy, with similar percentages to those reported before UC advanced therapy start, except for TOF and UST (Supplementary Figure 3).
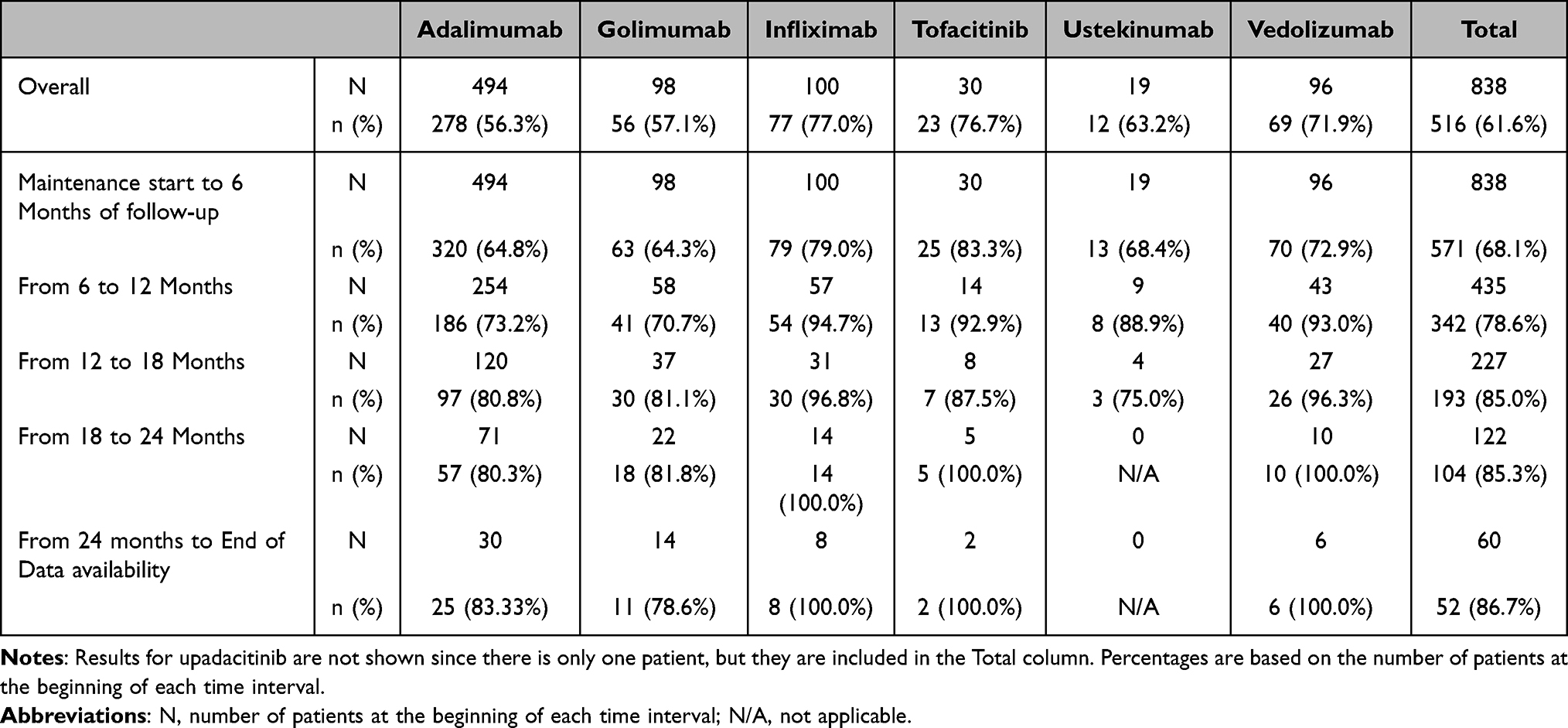 |
Table 2 Clinical Response by Time Interval and Treatment Cohort From Maintenance Start to End of Data Availability (AT Approach) |
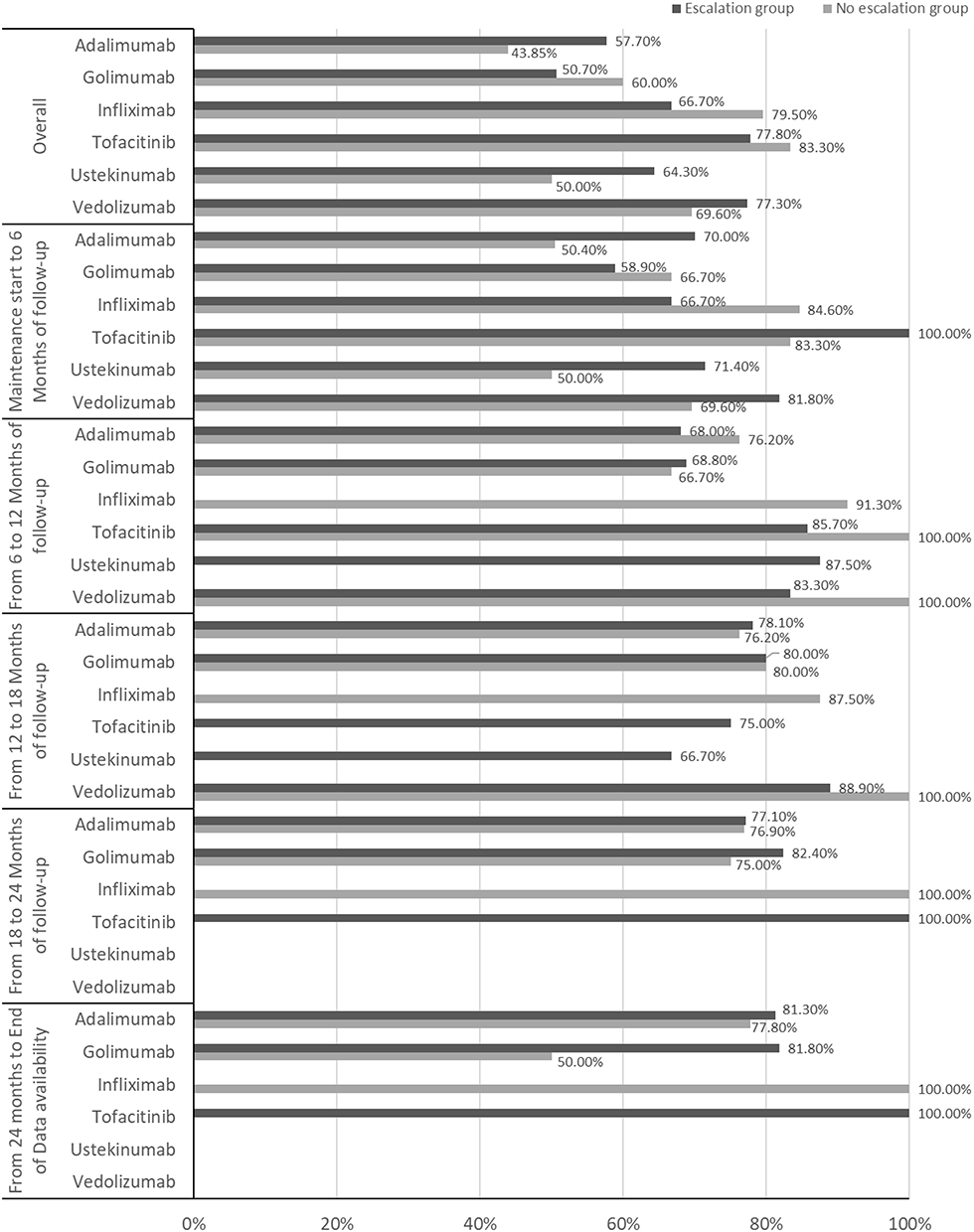 |
Figure 3 Clinical response in escalated patient versus non escalated patients, by treatment cohort (As-Treated approach). |
UC-Related Health Care Resource Utilization and Direct Costs
Table 3 summarizes the UC-related HRU (consultations [visits to general practitioners (GP) or specialists], hospitalizations or ER, diagnostic tests, UC drugs and non-drug interventions) during the study period (ITT approach) by country and treatment cohort. Mean (SD) number of consultations in UK was 27 (25.1), over a mean (SD) follow-up of 355.1 (446.9) days, whereas mean (SD) number of consultations for France was 10 (9.4), over a mean [SD] of 555.5 [503.1] days. In both countries (UK and France), UST and GOL were associated with lowest and highest number of consultations, respectively (mean [SD]: 19 [17.0] and 7 [7.3] vs 57 [47.0] and 11 [9.7]). Due to lack of information on specialized care in the UK database, only GP consultations were captured. In France, most consultations were from hepatologists/gastroenterologists (59.8%). In the UK, 273 (35.1%) patients were hospitalized, and 233 (26.3%) in France. Emergency room (ER) visits were recorded for a total of 70 (9.0%) patients in the UK, whereas only two patients had ER visits recorded in France [ADA and GOL cohorts]). A total of 366 (47.1%) and 190 (21.4%) patients in the UK and France, respectively, underwent UC-related diagnostic tests (including laboratory tests, endoscopies, biopsy, and radiologic imaging tests), and 522 (67.2%) and 563 (63.5%), respectively received other UC therapies (Table 3). These rates are underestimated as discussed further in the discussion section.
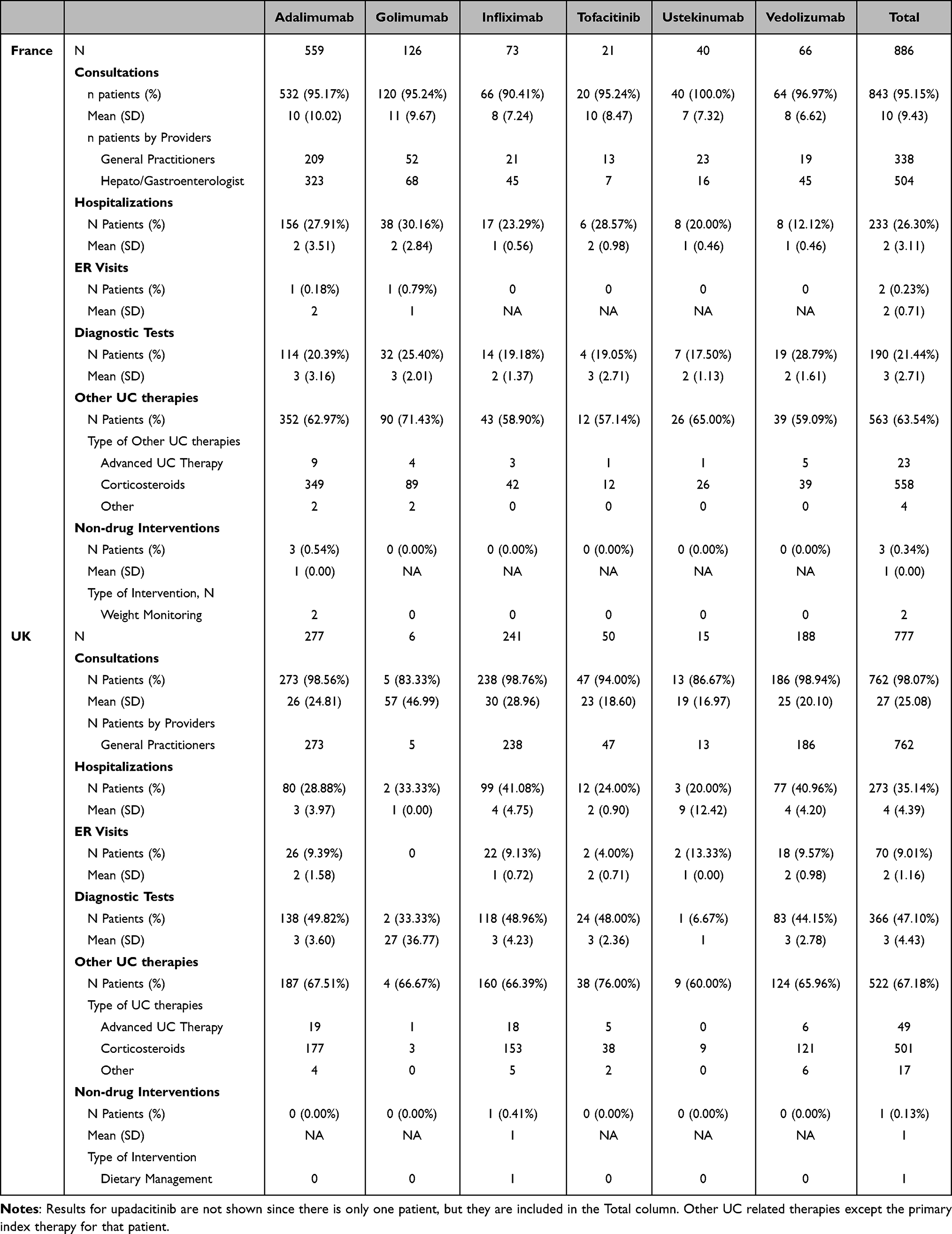 |
Table 3 Healthcare Resource Utilization (ITT Approach) |
Total direct mean (95% CI) UC-related costs per year per patient was estimated to be 6071.0 EUR and 10,025.6 EUR, in UK and France, respectively (Table 4). In UK, the main cost drivers were hospitalization (36.6%), consultations (34.8%), and UC drugs (27.7%). In France, the main cost driver was UC drugs (91.8%), followed by consultations (5.4%) and hospitalizations (2.8%) whatever the treatment cohort considered. In France, there was an overall increase in costs in the dose escalation group of 11.5% on average (corresponding to +1155.2 EUR), with treatment cohort variations ranging from −42.6% (−3159.8 EUR) in the case of IFX to +22.8% (+2991.7 EUR) in the case of TOF (Table 4). These differences are mainly driven by an increase in hospitalization (in overall with an increase of +22.3% between escalation and all patients, data not shown) and in UC drug costs (+11.8% between escalation group and all patients, data not shown). Data was insufficient in the UK to make reliable subgroup comparisons. The treatment associated with the highest direct costs was UST in both countries, whereas IFX was associated with the lowest costs in both countries, and ADA and TOF in the UK (Figure 4).
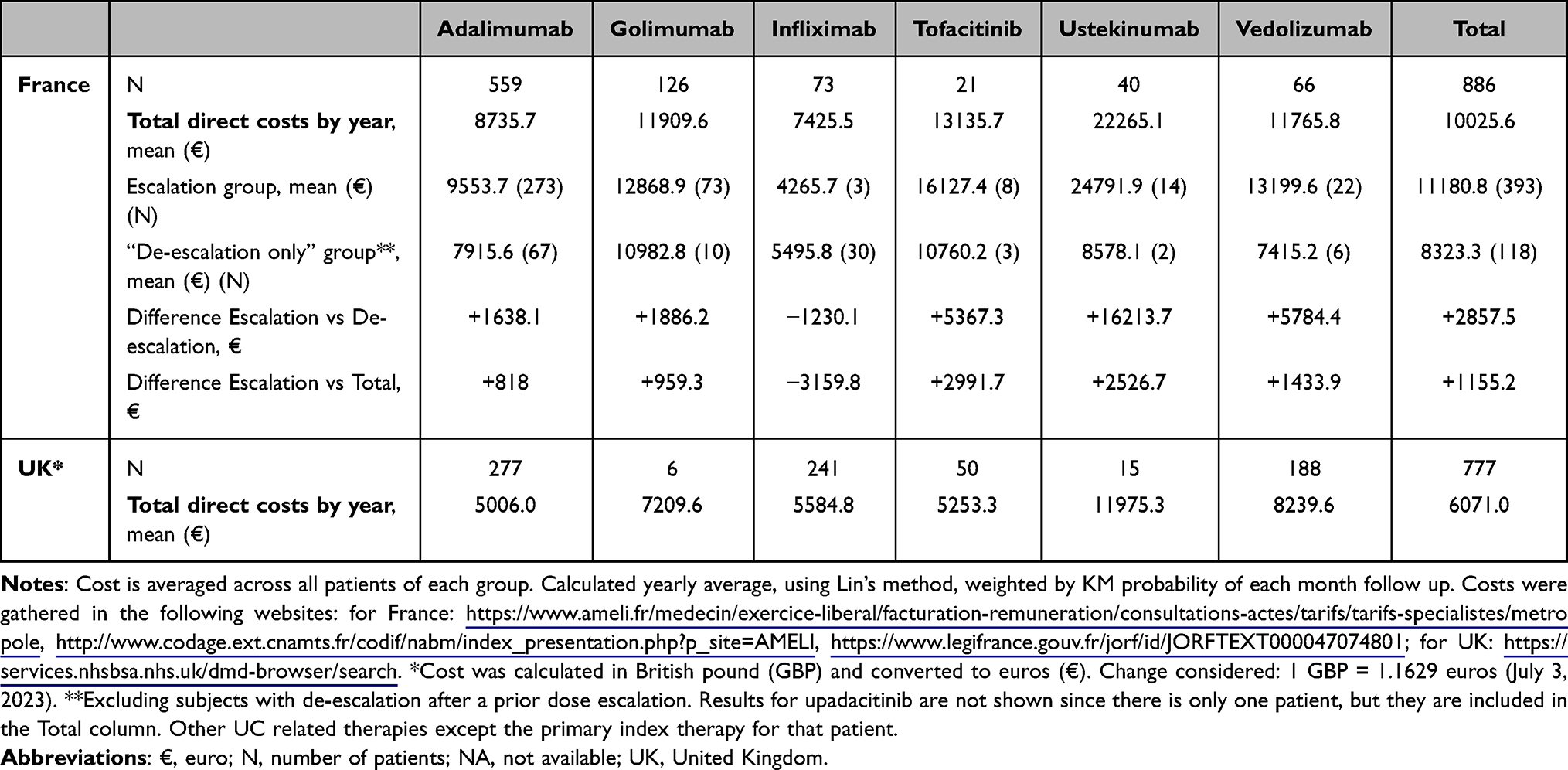 |
Table 4 Total Direct Cost in France and UK by Treatment Cohort and Overall, and by Escalation/“De-Escalation Only” Groups (ITT Approach) All Tables – Please Ensure the Table Footnotes are Presented Beneath the Table to Which They Relate, Not Formatted as the Last Lines of the Table |
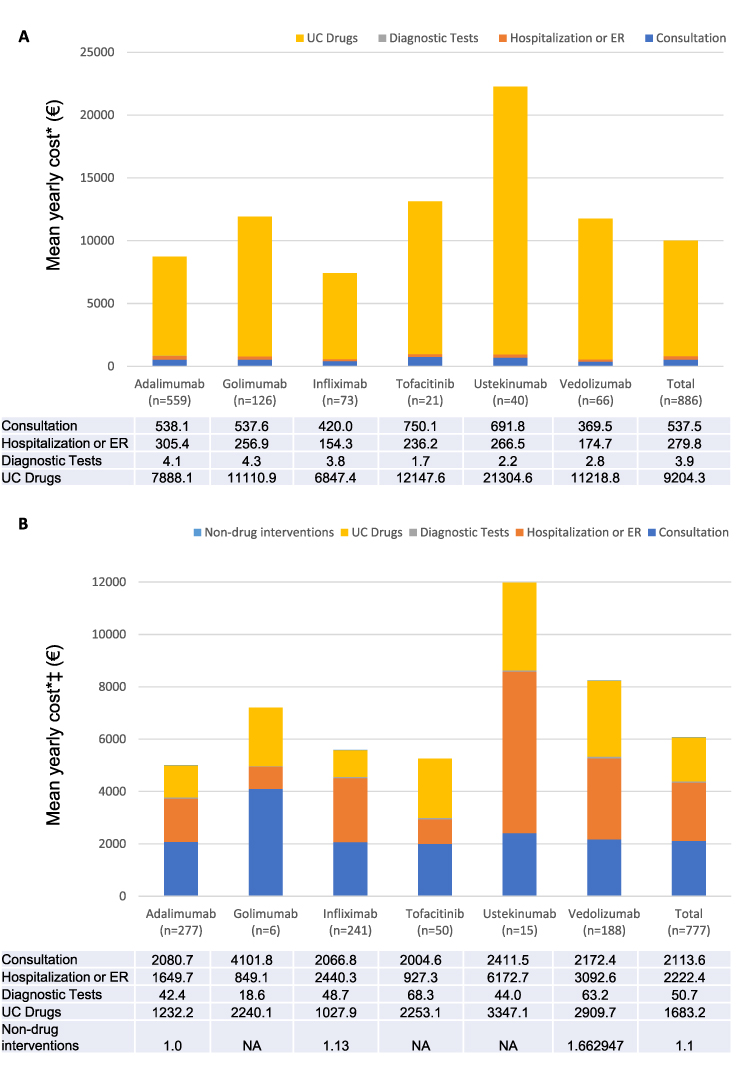 |
Figure 4 Mean yearly direct medical costs by patient. (A) France and (B) UK. Results for upadacitinib are not shown since there is only one patient, but they are included in the Total column. *Cost is averaged across all patients. Cost was calculated yearly average, using Lin’s method, weighted by KM probability of each month follow up. ‡ Cost were calculated in British pound (GBP) and converted to euros (€). Change considered: 1 GBP = 1,1629 euros (July 3, 2023). |
Discussion
This was a retrospective database study of real-world dose escalation/de-escalation patterns of advanced therapies among a relatively large cohort of patients with moderate-to-severe UC from France and the UK. All patients included in this study had been previously treated with conventional systemic therapies for UC before starting UC advanced therapies, in line with ECCO guidelines, and were new-users of biological therapies. This may have resulted in exclusion of more refractory UC patients (ie those who need a “second-line” advanced therapy), and underestimation of real-world dose-escalations. However, allowing prior advanced therapy use would have induced treatment/channeling bias (by comparing different treatment lines between sub-cohorts) or made the study unfeasible (if we had required the same line across sub-cohorts). Overall, the results of this study showed that dose escalation and de-escalation are commonly required among patients receiving advanced UC therapies, with 74.1% and 57.8% of patients escalating or de-escalating, respectively, within the first 6 months after the start of maintenance treatment. Despite this, clinical response over the study period was achieved by 61.6% of subjects, with rates varying from 56.3% with ADA to 77.0% with IFX. This result is a bit higher than the one reported by Dignass et al18 of less than the half achieving remission, although our definition based on absence of clinical events instead of disease activity score could have overestimated true response.19 The economic impact resulted in total direct mean annual costs per patient of 10,026 EUR in France and 6071 EUR in UK, mainly driven by drug costs, hospitalizations, and consultations.
Seventy-five percent of patients required at least one dose escalation within the first 6 months after start of maintenance. Dose escalation was highest in patients initiating GOL (85%), ADA (81%), and UST (85%), even after adjusting by differences in baseline characteristics. These findings were similar or slightly higher than those previously reported in the literature.13,20–22 For instance, Ylisaukko-Oja et al, in a Finnish UC cohort, found dose escalation rates of 71%, 63%, and 52–54%, for UST, ADA, and GOL.20 In our cohort, IFX showed the lowest dose escalation rates. Dose escalation of IFX at 18 and 24 months (both 33%) were similar to those observed at one year in the study by Long et al.21 Time to dose escalation among UC patients was 2.1 (1.8, 2.4) months. These findings are consistent with the range reported by the studies included in the systematic review by Singh et al.13 De-escalation rates, which are also associated with direct costs themselves, were also in line (58% in our cohort vs 17–81% in Singh et al), although results are not entirely comparable since many of these studies considered only de-escalations in patients with initial-dose escalation (as opposed to our definition, considering all subjects).
Clinical response varied between UC advanced therapies, but, at minimum, approximately 60% fulfilled the three criteria (no hospitalization, drug switch/addition or systemic corticosteroids use) within the first 6 months of maintenance. For subjects still on treatment at 24 months (less than 20% of the cohort) the long-term response attained 80%. Results regarding clinical response were aligned with those previously reported in systematic reviews13,23 and observational studies.24,25 Several studies based on real-world data found clinical response rates of 73–80% for IFX24 (with same definition as in our study) and 68.5% for GOL25 (using Mayo Score and reduction in corticosteroids use). Noticeably, within the first 6 months after maintenance, there were no relevant differences in clinical response rates between subjects who underwent dose escalation and those who did not, but, interestingly, between 12 and 18 months, rates of clinical response were similar or slightly higher for non-escalated patients. These results are likely due to patients achieving therapeutic benefit not requiring dose escalation. Overall, despite treatment with an advanced therapy, 52.6% of patients in this analysis received systemic/rectal corticosteroids as a concomitant medication for UC treatment, and, as expected, this was associated with dose-escalation of advanced therapy. The concomitant use of corticosteroids observed in this study is low compared with some studies in UC26 and IBD27 but high compared to the one found in the German cohort by Dignass et al.18
Direct annual medical costs related to UC ranged from 7426 to 22,265 EUR in France and, from 5006 to 11,975 EUR in the UK, being lower than those previously reported in the same countries by Lawton et al18,28 and Black et al18,28 Differences could be explained by several reasons such as inclusion of biosimilars on the market,28 or potential underestimation in our study due to incomplete follow-up information (particularly in the UK cohort) and/or missing public hospitalization costs (particularly in France), due to the nature of the THIN® database mainly capturing data from private healthcare (France) and from GPs (UK). Importantly, a limitation of this study is that GPs in UK are not the clinicians responsible for UC Advanced therapies selection and prescription. Both prior studies analyzed data before 2018, before biosimilars for different UC advanced therapies (such as ADA and IFX) were approved, marketed, and used in the clinical practice, which led to a reduction in the cost of treatment with biologics. This argument is reinforced by the fact that, in this study, ADA and IFX are among the treatment cohorts associated to the lowest prices on both countries, compared to data by Lawton et al (ADA [14,058€] and IFX [12,347€]),28 and Dignass et al (ADA [24,151€] and IFX [24,462€], at 12 months of follow-up).18 By comparing the costs according to the different dosing patterns (escalation or de-escalation), an overall increase in costs between the escalation vs all patients and escalation vs de-escalation group is observed. Once an advanced therapy is dose escalated, there may be subsequent additional visits required to de-escalate the dose. This study’s results are in line with the literature,21,29 even though the cost differences may differ from one study to another. Only IFX seems to follow a different pattern compared to previous studies, with higher overall costs for de-escalation.
Our results also showed that, for France and some UK UC treatment cohorts, drug costs were the major cost driver, in line with previous studies.18,28,30 In France, cost driven by UC advanced drugs reached up to 90%. A previous French study in IBD patients showed similar results, with drugs accounting for 84% of the total direct cost, while hospitalization represented only a minor part of the costs.28 For UK, in this study, half of the direct HRU costs were driven by UC advanced drugs in contrast with the 96.5% reported in a previous real-word data analysis of UC patients treated with ADA.30 Between 2017 and 2022, both France and the UK implemented significant changes in their health insurance policies, which have had a notable impact on drug prices. In France, the introduction of new pricing regulations aimed at controlling healthcare costs led to stricter price negotiations and reimbursement criteria for new drugs. The French National Health Authority (HAS) played a crucial role in assessing the therapeutic value of new medications, which influenced their pricing and reimbursement status. These measures resulted in more competitive pricing and increased pressure on pharmaceutical companies to demonstrate the cost-effectiveness of their products. In the UK, the National Institute for Health and Care Excellence (NICE) continued to refine its health technology assessment (HTA) processes, emphasizing value-based pricing. The introduction of the Voluntary Scheme for Branded Medicines Pricing and Access (VPAS) in 2019 replaced the previous Pharmaceutical Price Regulation Scheme (PPRS). VPAS aimed to cap the growth of branded medicine spending, ensuring that any expenditure above the agreed cap would be refunded by pharmaceutical companies. This policy shift encouraged the adoption of innovative pricing models, such as outcome-based agreements, and fostered a more sustainable approach to drug pricing. These policy changes in both countries have led to a more rigorous evaluation of drug prices, ensuring that new therapies provide significant clinical benefits relative to their costs. Consequently, pharmaceutical companies have had to adapt their pricing strategies to align with the evolving regulatory landscape, ultimately impacting the affordability and accessibility of advanced therapies for patients with ulcerative colitis.
Limitations
There are several limitations associated with this study, and some results should be interpreted with appropriate caution. Just as any study using secondary data, the findings were highly dependent on information (and quality) entered into the THIN® database by physicians. In some cases, incomplete or improper recording of some variables (like UC symptoms) or diagnoses may take place, potentially leading to misclassification of some patients into escalation/de-escalation subgroups or to the inability to dose analysis. For instance, information on dose strength and frequency was lacking in some subjects, particularly in the UK. Therefore, multiple imputations were performed to get meaningful dose information, but this may have added bias in the interpretation of the data. Sensitivity analysis gone using more stringent criteria to try to quantify potential bias with the imputations, showed that we could overestimate dose escalations by 35%.
For dose escalation, it is important to highlight that the dose escalation/de-escalation results in this study come mainly from the French cohort, as in the UK cohort only 50% of patients had information on index UC advanced therapy upon the start of maintenance period. This is due to the fact that the THIN® database in UK only captures data from GPs. However, it should be noted that HRU analyses by country suggest that the UK cohort was quite similar to the French one, with more hospitalizations (35% vs 26%) and diagnostic tests done (47% vs 21%), despite a shorter median follow-up time. This suggests that the dose escalations in this UK cohort, if a longer follow-up would have been available, would be even more frequently required than in the French cohort.
Regarding HRU, hospitalizations could be underestimated. In the UK, hospitalizations in THIN® include only those registered by GPs and, in France, due to reimbursement history, mainly only private hospitalizations are registered. Moreover, the source dataset did not allow identification of whether resource utilization was directly related to UC, so UC-related hospitalizations were selected based on the diagnostic labels; therefore, some cases could have been missed. On the other side, costs could be overestimated due to lack of visibility of prices of advanced therapies in each country.
Lastly, low sample size in some treatment cohorts could lead to insufficient precision to properly describe some outcomes. Also, due to the observational nature of this study, selection bias and unmeasured confounding (related to missing key sociodemographic and clinical variables) may affect and limit the outcomes description and interpretation.
Conclusion
Dose escalation of advanced therapies for UC is a common strategy to avoid treatment-switching. Despite dose escalations and associated cost, a proportion of patients fail to achieve clinical response. This study highlights the need for more efficacious and durable treatments for patients with moderate-to-severe UC, as the initiation of the advanced therapies studied did not reduce overall systemic/rectal corticosteroid burden.
Disclosure
Dr Tamás Treuer and Dr Dhesi are employees and minor shareholders in Eli Lilly & Company, during the conduct of the study. Ms Lidia Silva reports payment made to TFS (as CRO) by contracting the data analysis and writing of respective manuscript to TFS from Eli Lilly, during the conduct of the study. The authors report no other conflicts of interest in this work. The abstract of this paper was presented at the 19th Congress of ECCO Stockholm -Sweden (on February 21–24, 2024) as a poster presentation with interim findings. The poster’s abstract was published in Volume 18, Issue Supplement_1, January 2024, Page i1667, of the Journal of Crohn’s and Colitis: https://doi.org/10.1093/ecco-jcc/jjad212.1042. A Real-World Evidence Study of Dose Escalation and Associated Costs of Advanced Therapies for Ulcerative Colitis in France and United Kingdom.
References
1. Vermeire S, Van Assche G, Rutgeerts P. Classification of inflammatory bowel disease: the old and the new. Curr Opin Gastroenterol. 2012;28:321–326. doi:10.1097/MOG.0b013e328354be1e
2. Ramos L, Teo-Loy J, Barreiro-de Acosta M. Disease clearance in ulcerative colitis: setting the therapeutic goals for future in the treatment of ulcerative colitis. Front Med. 2022;9:1102420. doi:10.3389/fmed.2022.1102420
3. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel J-F. Ulcerative colitis. Lancet. 2017;389:1756–1770. doi:10.1016/S0140-6736(16)32126-2
4. Burisch J, Jess T, Martinato M, Lakatos LP. The burden of inflammatory bowel disease in Europe. J Crohn’s Colitis. 2013;7(4):322–337. doi:10.1016/j.crohns.2013.01.010
5. Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis. 2017;11:769–784. doi:10.1093/ecco-jcc/jjx009
6. Armuzzi A, DiBonaventura MC, Tarallo M, et al. Treatment patterns among patients with moderate-to-severe ulcerative colitis in the United States and Europe. PLoS One. 2020;15:e0227914. doi:10.1371/journal.pone.0227914
7. Yamamoto-Furusho JK, Al Harbi O, Armuzzi A, et al. Incidence of suboptimal response to tumor necrosis factor antagonist therapy in inflammatory bowel disease in newly industrialised countries: the EXPLORE study. Digestive Liver Dis. 2020;52:869–877. doi:10.1016/j.dld.2020.05.031
8. Zhao M, Larsen L, Dige A, et al. P405 primary non-response and loss-of-response to first-line biological therapies are more common in patients with Ulcerative Colitis than Crohn’s Disease – preliminary results from the Danish IBD Biobank Project. J Crohn’s Colitis. 2022;16:i397–i398. doi:10.1093/ecco-jcc/jjab232.532
9. Lindsay JO, Picker N, Kromer D, Smyth M, Patel H. The incidence of remission and indicators of inadequate response to advanced therapy in patients with ulcerative colitis: results from medical charts in the United Kingdom. Curr Med Res Opin. 2023;39:1–23. doi:10.1080/03007995.2023.2194782
10. Vincent FB, Morand EF, Murphy K, Mackay F, Mariette X, Marcelli C. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis. 2013;72:165–178. doi:10.1136/annrheumdis-2012-202545
11. Vermeire S, Gils A, Accossato P, Lula S, Marren A. Immunogenicity of biologics in inflammatory bowel disease. Therap Adv Gastroenterol. 2018;11:1756283X17750355. doi:10.1177/1756283X17750355
12. Panaccione R, Lee W-J, Clark R, et al. Dose escalation patterns of advanced therapies in Crohn’s disease and ulcerative colitis: a systematic literature review. Adv Ther. 2023;40:2051–2081. doi:10.1007/s12325-023-02457-6
13. Singh H, Wilson L, Tencer T, Kumar J. Systematic literature review of real-world evidence on dose escalation and treatment switching in ulcerative colitis. Clinicoecon Outcomes Res. 2023;15:125–138. doi:10.2147/CEOR.S391413
14. Seni K, Saini A, Debnath R, Singh A. Advancements in ulcerative colitis management: a critical assessment of etrasimod therapy. Health Sci Rev. 2024;12:100196. doi:10.1016/j.hsr.2024.100196
15. Berger ML, Dreyer N, Anderson F, Towse A, Sedrakyan A, Normand S-L. Prospective observational studies to assess comparative effectiveness: the ISPOR good research practices task force report. Value Health. 2012;15:217–230. doi:10.1016/j.jval.2011.12.010
16. Leslie S, Thiebaud P. Using Propensity Scores to Adjust For Treatment Selection Bias. San Diego, CA: MedImpact Healthcare Systems, Inc.; 2007.
17. Lin DY, Feuer EJ, Etzioni R, Wax Y. Estimating medical costs from incomplete follow-up data. Biometrics. 1997;53:419. doi:10.2307/2533947
18. Dignass A, Waller J, Cappelleri JC, et al. Living with ulcerative colitis in Germany: a retrospective analysis of dose escalation, concomitant treatment use and healthcare costs. J Med Econ. 2020;23:415–427. doi:10.1080/13696998.2019.1707210
19. Dignass A, Redondo I, Streit P, et al. Clinical profiles and outcomes in patients with inflammatory bowel disease receiving standard and escalated doses of targeted therapies: findings from a global real-world study. Curr Med Res Opin. 2023;39:1695–1705. doi:10.1080/03007995.2023.2278695
20. Ylisaukko-Oja T, Puttonen M, Jokelainen J, et al. Dose-escalation of Adalimumab, golimumab or ustekinumab in inflammatory bowel diseases: characterization and implications in real-life clinical practice. Scand J Gastroenterol. 2022;57:415–423. doi:10.1080/00365521.2021.2014950
21. Long MD, Cohen RD, Smith TW, et al. Retrospective database analysis: dose escalation and adherence in patients initiating biologics for ulcerative colitis. Dig Dis. 2022;40:553–564. doi:10.1159/000521299
22. Kathe N, Umashankar K, Mirchandani K, et al. Dose escalation of biologic therapies in biologic treatment-naïve adult patients with ulcerative colitis: results from the Odessa database study. Inflamm Bowel Dis. 2022;28:S9–S10. doi:10.1093/ibd/izac015.015
23. Yang H, Li B, Guo Q, et al. Systematic review with meta-analysis: loss of response and requirement of ustekinumab dose escalation in inflammatory bowel diseases. Aliment Pharmacol Ther. 2022;55:764–777. doi:10.1111/apt.16802
24. Kirchgesner J, Desai RJ, Schneeweiss MC, Beaugerie L, Kim SC, Schneeweiss S. Emulation of a randomized controlled trial in ulcerative colitis with US and French claims data: infliximab with thiopurines compared to infliximab monotherapy. Pharmacoepidemiol Drug Saf. 2022;31:167–175. doi:10.1002/pds.5356
25. Macaluso FS, D’Antonio E, Fries W, et al. Safety and effectiveness of tofacitinib in ulcerative colitis: data from TOFA-UC, a SN-IBD study. Dig Liver Dis. 2023;55:S178. doi:10.1016/j.dld.2023.08.061
26. Patel H, Lissoos T, Rubin DT. Indicators of suboptimal biologic therapy over time in patients with ulcerative colitis and Crohn’s disease in the United States. PLoS One. 2017;12:e0175099. doi:10.1371/journal.pone.0175099
27. Lindsay JO, Armuzzi A, Gisbert JP, et al. Indicators of suboptimal tumor necrosis factor antagonist therapy in inflammatory bowel disease. Dig Liver Dis. 2017;49:1086–1091. doi:10.1016/j.dld.2017.07.010
28. Lawton J, Achit H, Pouillon L, et al. Cost-of-illness of inflammatory bowel disease patients treated with anti-tumour necrosis factor: a French large single-centre experience. United Eur Gastroenterol J. 2019;7:908–913. doi:10.1177/2050640619853448
29. Pöllinger B, Schmidt W, Seiffert A, Imhoff H, Emmert M. Costs of dose escalation among ulcerative colitis patients treated with Adalimumab in Germany. Eur J Health Econ. 2019;20:195–203. doi:10.1007/s10198-017-0953-z
30. Black CM, Yu E, McCann E, Kachroo S. Dose escalation and healthcare resource use among ulcerative colitis patients treated with adalimumab in English hospitals: an analysis of real-world data. PLoS One. 2016;11:e0149692. doi:10.1371/journal.pone.0149692
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.