Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Don’t Go: Examining the Relationships Between Meaning, Work Environment and Turnover Intention Across the Entire Healthcare Team
Authors Meese KA ![]() , Boitet LM
, Boitet LM ![]() , Sweeney KL, Gorman CA, Nassetta LB, Patel N, Rogers DA
, Sweeney KL, Gorman CA, Nassetta LB, Patel N, Rogers DA ![]()
Received 30 August 2023
Accepted for publication 4 January 2024
Published 23 January 2024 Volume 2024:17 Pages 353—366
DOI https://doi.org/10.2147/JMDH.S437816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Katherine A Meese,1,2 Laurence M Boitet,1,2 Katherine L Sweeney,2,3 C Allen Gorman,4 Lauren B Nassetta,2,5 Nisha Patel,2 David A Rogers2,6
1Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, AL, USA; 2UAB Medicine Office of Wellness, UAB, Birmingham, AL, USA; 3Department of Sociology, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Management, Information Systems, & Quantitative Methods, University of Alabama at Birmingham (UAB), Birmingham, AL, USA; 5Department of Pediatrics, University of Alabama at Birmingham (UAB), Birmingham, AL, USA; 6Department of Surgery, University of Alabama at Birmingham (UAB), Birmingham, AL, USA
Correspondence: Katherine A Meese, Email [email protected]
Introduction: Healthcare workers tend to have a strong sense of altruism in their work, which may be protective against turnover despite poor working conditions. Due to the increased distress noted during the pandemic, the challenges of working in healthcare and changing attitudes about work may have surpassed the protective effect of meaning and purpose in work. This study empirically examines perceived meaning in work, and specific work-related factors that contribute to employees’ intent to stay and to recommend working at the organization to others as COVID-19 transitions from a pandemic to endemic phase.
Methods: Data from a survey of 4451 clinical and non-clinical healthcare workers were analyzed using regression and dominance analyses to identify specific predictors of turnover intention and net promoter score.
Results: The variables that explained the greatest contribution to variance in turnover intention from highest to lowest were burnout, trust and confidence in senior leadership, perceived organizational support, sense of belonging, and sense of recognition. The variables that explained the greatest overall contribution to variance for net promoter score from highest to lowest were perceived organizational support, trust and confidence in senior leadership, resource availability, sense of recognition, and sense of belonging. While meaning in work was associated with turnover intent, organizational and team level factors such as trust and belonging were more predictive of the outcomes.
Discussion: While meaning and purpose are important job resources, they are not sufficient to retain employees in the absence of trust, organizational support, belonging, recognition and access to necessary resources. Leaders must seek to foster environments that support trust, belonging and recognition in their retention efforts.
Keywords: healthcare, turnover, retention, meaning, work environment
Introduction
Healthcare workers identify with their professional roles strongly and tend to have an altruistic perspective of their work.1 A key characteristic of the healthcare worker is their resolve to heal and help others, which ultimately defines their character and livelihood. Innately, many possess a duty to care. Poor working conditions for clinical workers have been noted for over 20 years and can be felt globally.2,3 The COVID-19 pandemic amplified these challenges as workers were exposed to a deadly virus, threats of physical harm,4 financial instability,5 and widespread staffing shortages6 leading to increased workload. Healthcare worker distress rose sharply, leading to increased risk for suicide, depression, and anxiety across the entire healthcare team.7 Increased rates of distress among healthcare workers were largely explained by work-related factors including heavy workload and long hours, increased job demands and responsibilities,7 perceived inequities, mistreatment from patients,4,8 and moral distress.9 As a result, turnover and intent to leave the field altogether are major concerns industry-wide.10,11
Given the importance of a sense of meaning and purpose in cultivating human flourishing,12 it is likely that healthcare’s meaning and purpose, in tandem with the altruism of the healthcare worker, have been protective against turnover, despite poor working conditions. The Job Demands-Resources Theory (JD-R) emphasizes that job-related stress is affected by both the demands of the work and the resources one has to offset those demands.13 If individuals have sufficient resources to meet their demands (either by increasing resources or reducing demands) there is greater individual motivation, engagement and positive organizational outcomes. If demands exceed resources, negative organizational outcomes result.13
Large studies have examined the drivers of modern employee experience both within and outside of healthcare.14 However, few studies have examined specific factors that may be more salient as the pandemic becomes endemic and the workforce undergoes fundamental changes. Research in healthcare typically occurs in professional siloes but less commonly examines the entire healthcare team, including both clinical and non-clinical employees. Further, little is known about whether a sense of meaning and purpose is sufficient to offset work-related factors that may worsen turnover for a highly altruistic workforce. The purpose of this study therein is to empirically examine perceived meaning in work, and the specific work-related demands and resources that are related to healthcare workers’ intent to leave the organization (turnover intention) or recommend it to others. The main contributions of this study are to explore the factors that have the greatest potential to support recruitment and retention efforts across the entire healthcare team and to understand the contribution of meaningful work relative to other job demands and resources.
Methods
Study Sample and Data Collection
An anonymous, cross-sectional survey was designed and approved by the Institutional Review Board of the University of Alabama at Birmingham in the southeastern United States (IRB #300006629). The survey was developed using JD-R as a theoretical framework and piloted in 2020 and 2021.4,7 From June to July 2022, the survey was distributed via email to 23,697 eligible employees of a large academic medical center for optional participation with informed consent. Reminders to complete the survey were sent weekly for four weeks. Data pertaining to individual and organizational-level demands and resources, turnover intention, and net promoter score were collected using previously validated measures (Table 1). A total of 4827 employees completed the survey.
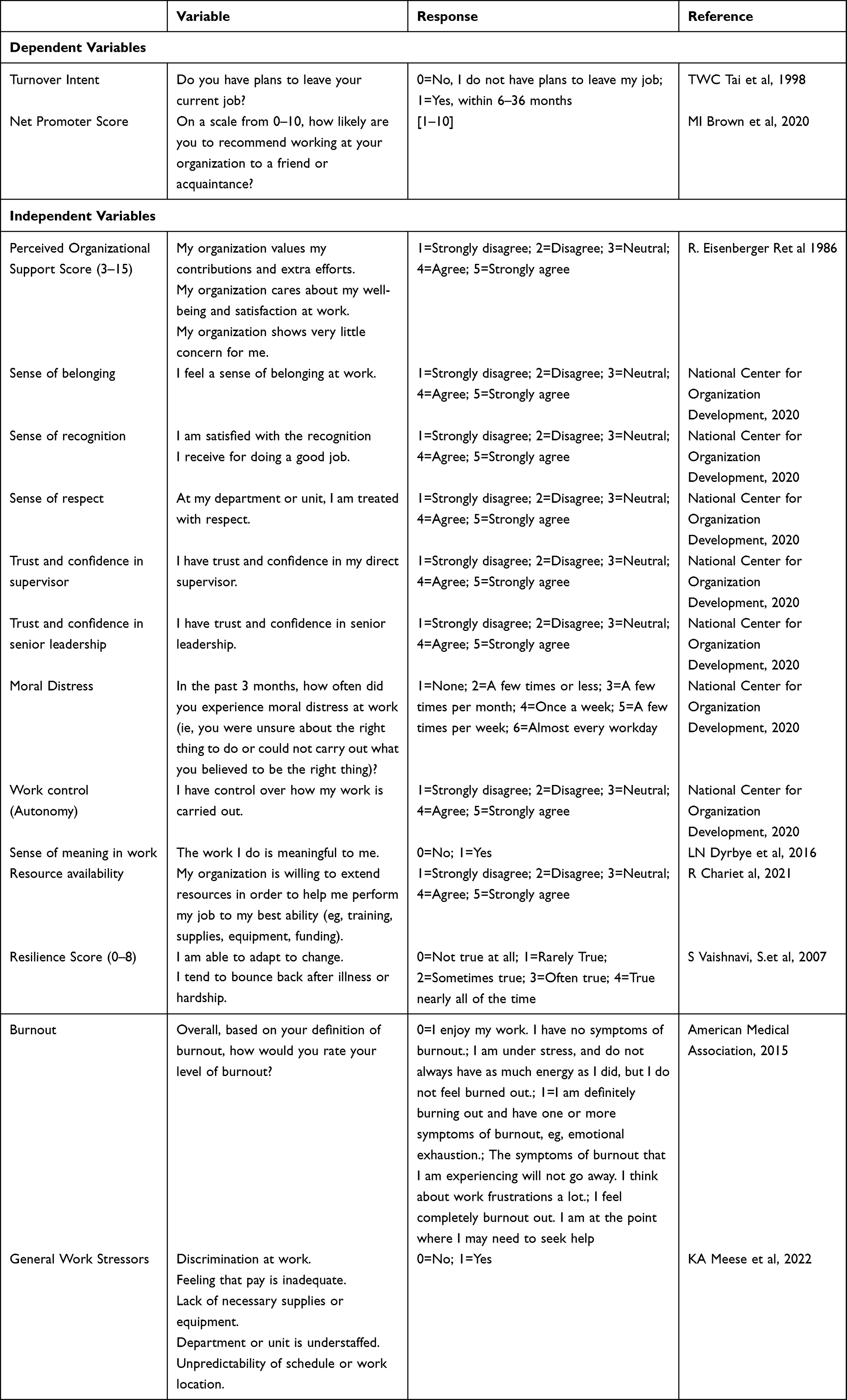 |
Table 1 Definition of Survey Measures |
A total of 6466 employees (27.3% response rate) participated in the survey, of which 1639 were missing at least one variable of interest and omitted using listwise deletion, leaving a final analytic sample of 4827. The sample contained representation from all members of the healthcare team, including administrative and non-clinical staff, advanced practice providers (APP), clinical support staff (clinical laboratory personnel, patient care technicians, social workers, etc.), nurses, physicians and clinicians, basic science personnel (non-clinician faculty and basic science laboratory workers), and other employees (environmental services, nutrition services, maintenance, etc.).
Dependent Variables
To understand factors that influence healthcare worker intent to leave the organization, we used a previously validated measure of turnover intention as an outcome variable (Table 1).15 For the purposes of this study, the responses were recoded as 0 (No, I do not have plans to leave my job) and 1 (Yes, within 6–36 months). Net promoter score was also as an outcome variable as previously described,16 wherein participants ranked their likelihood of recommending their organization on a scale from 1 (Unlikely) to 10 (Extremely likely).
Independent Variables
Explanatory independent variables for each outcome were identified based on literature review as well as stepwise regression and can be found in Table 1. Perceived organizational support was captured and reported as previously described.17,18 Senses of belonging, recognition, and respect, trust and confidence in supervisor and senior leadership, moral distress, and work control (autonomy) were measured and reported as previously described.19 Sense of meaning in work was measured using a single-item measure from the Well-Being Index,20 wherein participant response format ranged from 1 (Strongly disagree) to 5 (Strongly agree) and were combined into +1 (Low level), 0 (neutral level), and −1 (High level), as previously described.20 For the purposes of this study, responses were recoded as 0 (Neutral and low levels) and 1 (High level). Burnout was measured as previously described.21 For this study, responses were recoded as 0 (No burnout) and 1 (Burnout). Resource availability22 and individual resilience23 were measured as previously described.
Participants also selected major general work- and nonwork-related stressors from a predetermined list that was developed with input from over 25 clinical and non-clinical leaders, as previously piloted,4 regarding what they perceived to be the greatest stressors among employees. These included heavy workload, long hours, and unpredictability of schedule or work location. Participants provided demographic information, such as race, gender, age, and job role. A prefer not to answer category was included to capture participants who chose not to disclose their demographics.
Data Analysis
Data were imported into Stata/SE 17.0 (Stata Corp, College Station, TX) for analysis. Variables were stratified by job role and represented by frequency and percentages or mean and standard deviation. Analysis of variance (ANOVA) and chi-square tests were used to determine significance in the variables of interest across job role. Multivariate binary logistic regression was used to predict the odds of turnover intention when considering individual and organizational level factors. Multivariate linear regression was used to analyze the degree to which individual and organizational factors were associated with net promoter score. Significance level was set to 5% and lower. Additionally, stepwise regression, pseudo-R squares, Akaike’s Information Criterion, and Bayesian Information Criterion were used to further confirm the selection of variables for each model. Variance inflation factor values were used to determine absence of problematic multicollinearity. The Stata dominance analysis module24 was conducted to determine the relative dominance of the predictor variables in explaining the variance in turnover intention and net promoter score.
Results
A summary of the sample is presented in Table 2 and significance of any differences in variables that existed among job roles. Turnover intention (p<0.001) was significantly associated with job role, and approximately 31% of the total sample of participants reported plans to leave their job at the time of survey. Nurses reported the highest percentage of turnover intention (39.7%), followed by APP (35.8%). The average net promoter score was 7.03. Administrative and non-clinical staff reported the highest average scores (M=7.63). Most participants identified as a gender or sexual minority (62.56%) and white (54.7%). The majority of participants were between the ages of 25 and 44 (40.0%), followed by 45 to 65 years old (31.8%).
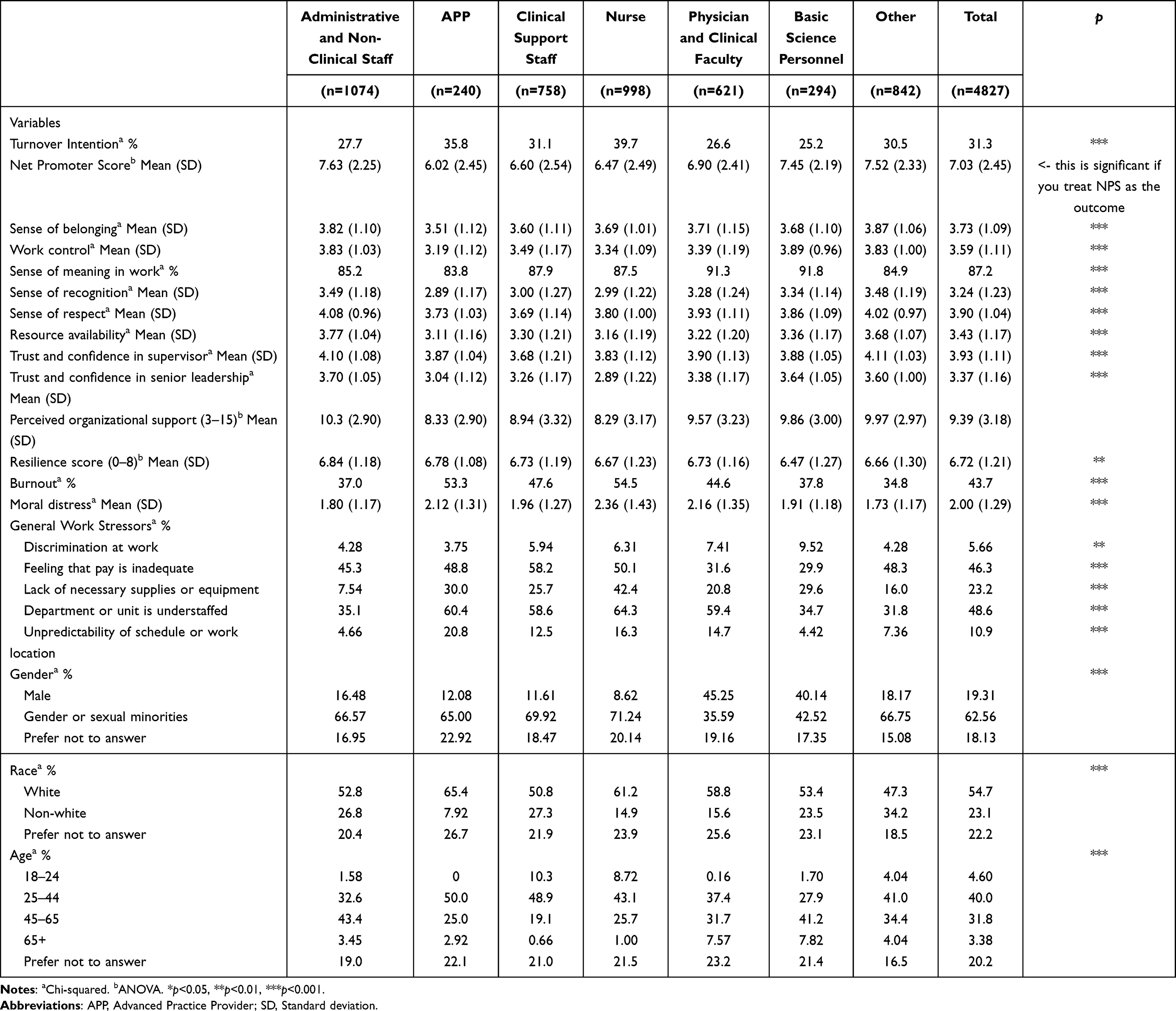 |
Table 2 Characteristics of the Sample (n=4827) |
Table 3 reports the results of the binary logistic regression model predicting the odds of reporting turnover intention. Physician and clinical faculty (OR=0.58, p<0.001), clinical support staff (OR=0.68, p<0.01), and basic science personnel (OR=0.70, p<0.05) showed lower odds of having plans to leave their jobs at the time of survey. Participants who felt a greater sense of belonging (OR=0.80, p<0.001), trust and confidence in senior leadership (OR=0.80, p<0.001), sense of meaning in work (OR=0.67, p<0.01), sense of recognition (OR=0.92, p<0.05), trust and confidence in supervisor (OR=0.91, p<0.01), and perceived organizational support (OR=0.95, p<0.01) had lower odds of turnover intention. Participants who were burnt out (OR=2.1, p<0.001) and reported moral distress at work (OR=1.1, p<0.001) showed higher odds of turnover intention. Of the general work stressors, participants who indicated feelings of inadequate pay (OR=1.6, p<0.001), reported understaffing of their department or unit (OR=1.2, p<0.05), and unpredictability of schedule or work location (OR=1.3, p<0.05) had higher odds of turnover intention. Gender or sexual minorities had lower odds of turnover intention (OR=0.75, p<0.01). Participants who had lower odds of turnover intention were 25–44 (OR=0.45, p<0.001) and 45–65 (OR=0.53, p<0.001) years old, as well as those who preferred not to disclose their age (0.45, p<0.001), compared to the referent group.18–23 On the contrary, participants who were 65 years or older had higher odds of having plans to leave their job (2.5, p<0.001), compared to the referent group. The variables that explained the greatest contribution to variance in turnover intention from highest to lowest were burnout, trust and confidence in senior leadership, perceived organizational support, sense of belonging, and sense of recognition.
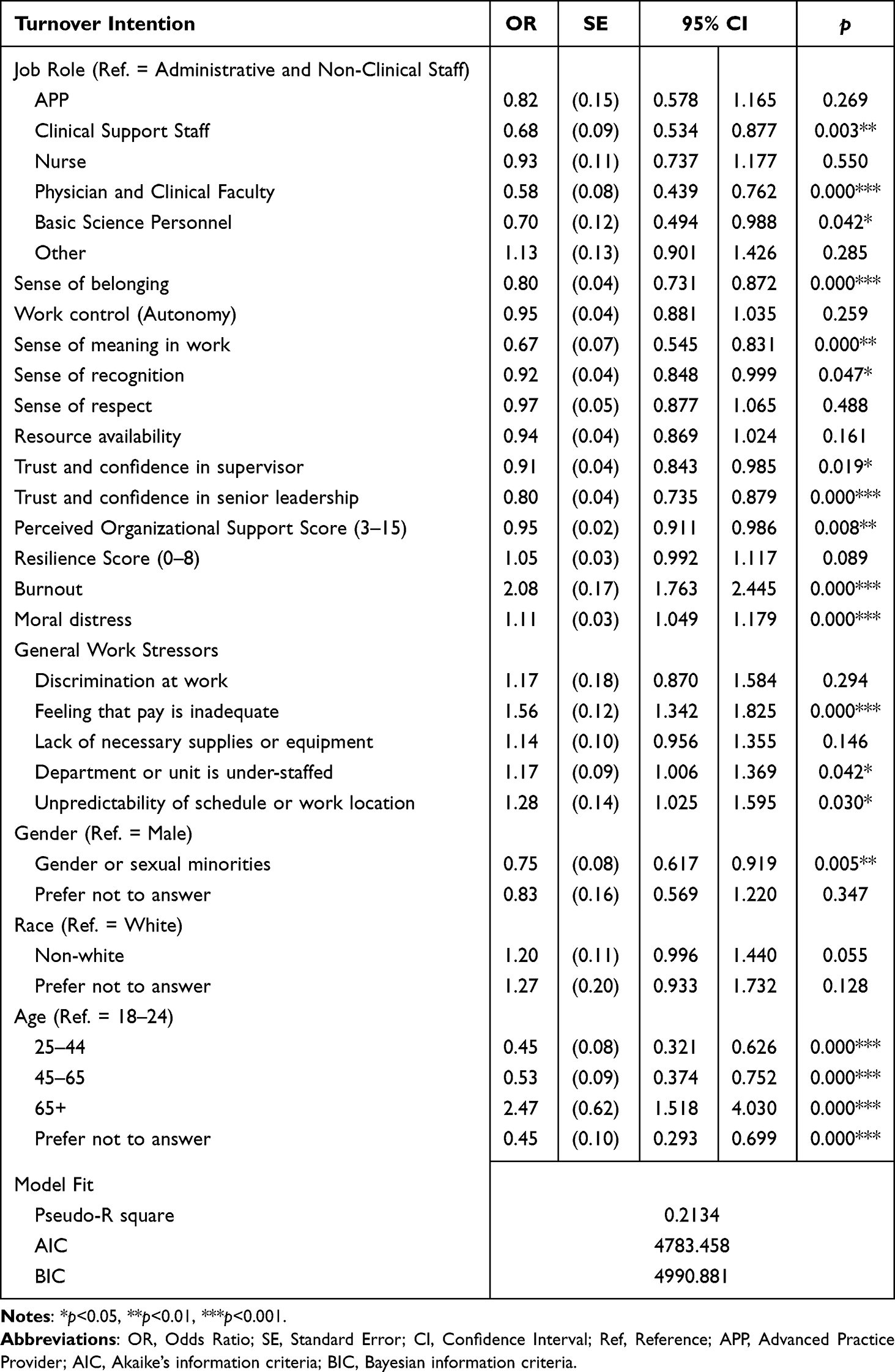 |
Table 3 Logistic Regression Predicting the Odds of Turnover Intent Across the Entire Healthcare Team (n=4827) |
Table 4 presents the results of the linear regression model predicting NPS. APPs (β=−0.43, p<0.01), clinical support staff (β=−0.18, p<0.05), and physician and clinical faculty (β=−0.16, p<0.05) on average reported lower net promoter scores and were less likely to recommend their organization to a friend or acquaintance. Factors associated with lower NPSs on average were burnout (β=−0.39, p<0.001), and moral distress at work (β=−0.08, p<0.001). Participants who indicated a sense of belonging (β=0.17, p<0.001), work control or autonomy (β=0.06, p<0.05), sense of meaning in work (β=0.25, p<0.01), and sense of recognition (β=0.08, p<0.01) reported higher NPSs on average. Participants were also more likely to recommend the organization to friends or acquaintances if they reported resource availability (β=0.2, p<0.001), and trust and confidence in their direct supervisor (β=0.15, p<0.001) as well as trust in senior leadership (β=0.28, p<0.001). Participants who reported higher perceived organizational support scores (β=0.30, p<0.001) and higher resilience scores (β=0.04, p<0.05) were also more likely to report higher NPSs, on average. Of the general work stressors, those reporting feeling that pay is inadequate (β=−0.13, p<0.01) and unpredictability of schedule or work location (β=−0.18, p<0.05) were less likely to recommend the organization to friends or acquaintances. Additionally, those who selected “prefer not to answer” for their race reported lower NPSs on average (β=−0.22, p<0.05), compared to the referent group (white). The variables that explained the greatest overall contribution to variance for NPS from highest to lowest were perceived organizational support score, trust and confidence in senior leadership, resource availability, sense of recognition, and sense of belonging.
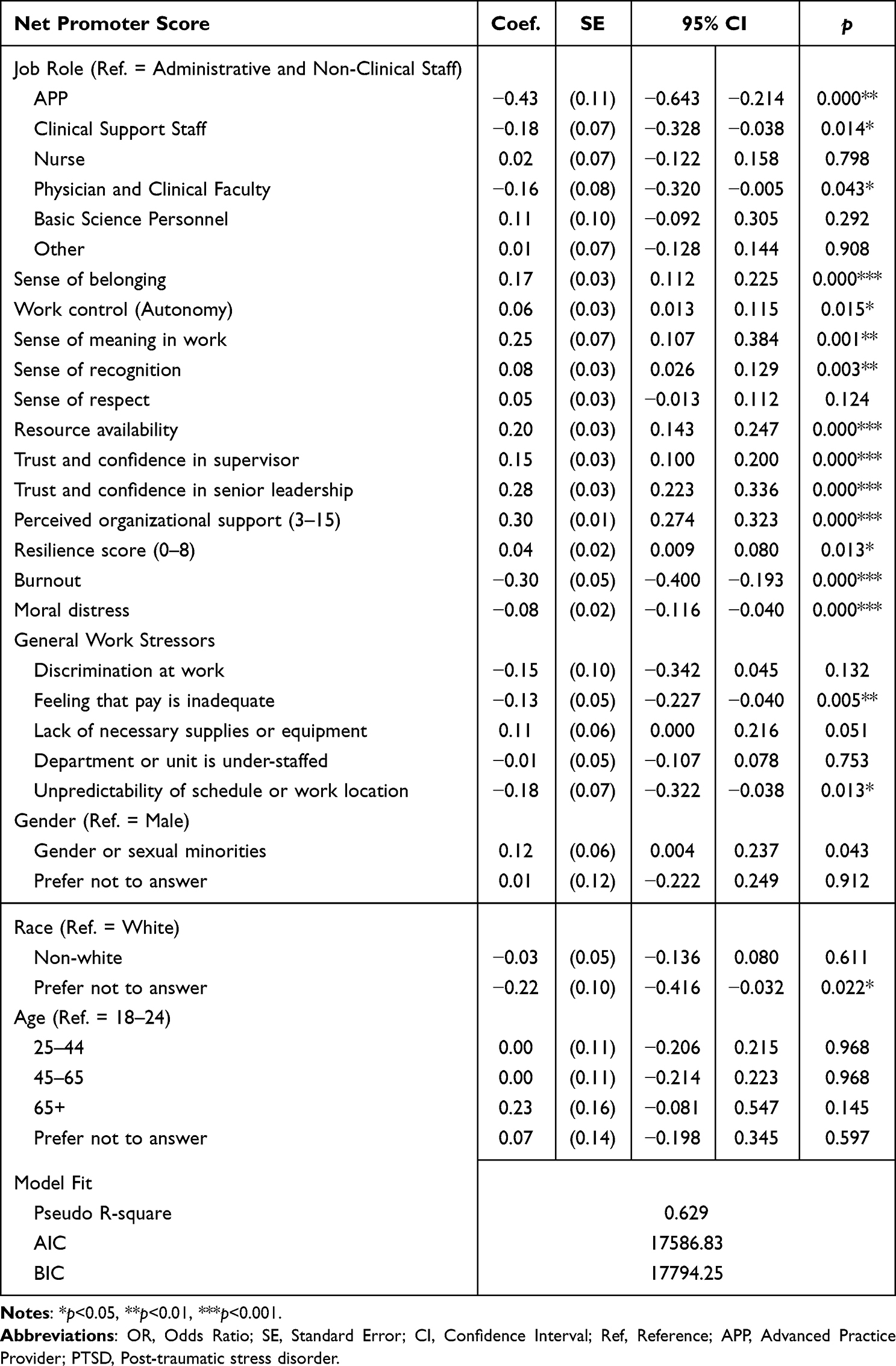 |
Table 4 Linear Regression Predicting Net Promoter Score Across the Entire Healthcare Team (n=4827) |
Discussion
Despite the many challenges facing healthcare workers and institutions, specific identifiable factors are associated with employees’ intent to stay in their current roles and recommend working at the organization. Understanding what might predict employees’ intent to leave is essential in decreasing turnover, which has clear financial implications and impacts the quality of patient care.25 Additionally, net promotor scores serve two evaluative purposes. The first is to assess the probability of employees recruiting others in their network to the organization. More subtly, it also reflects employees’ pride in the organization, and desire for others to be a part of the experience at work. Factors associated with turnover intention and NPS are discussed at the organizational, team, and individual levels.
Organizational Level Factors
We found that employee perceptions of activities at the highest level of the organization are significantly associated with their intentions to remain with the organization and recommend it to others as an employer. Specifically, employee perceptions of organizational support and whether they had trust and confidence in senior leadership were among the top three contributors to the overall variance for both turnover intention and NPS. The role of the direct supervisor in employee turnover is often highlighted in the literature;26,27 however, our findings emphasize the importance of individual employee perceptions of organization-wide and senior-level support. In large hierarchical organizations, there are many levels between the employee and the senior leadership team. These findings suggest that building trust with employees remains a key role for senior leaders and cannot be fully relegated to direct supervisors in the efforts to recruit and retain the workforce. It is important to note that the perceived organizational support score included elements of feeling seen and valued by the organization and believing that the organization cares about the individual employee’s well-being. This is consistent with other research that has identified that workers prioritize organizations that are willing to invest in their well-being.28–30 Similarly, those identifying a negative or toxic work environment as a major stressor were less likely to recommend the organization. This perception of culture is likely a combination of both team-level interactions and broader organizational experiences, the organization’s leadership holds responsibility for the leaders in place and the systems of accountability, or lack thereof, that allow toxic cultures to persist.
Organizations have faced challenging supply shortages across industries, and global supply chains have been disrupted. Additionally, financial pressures may lead to reduced training and professional development budgets and internal funding mechanisms, making access to these resources no less crucial, but increasingly difficult to provide. We demonstrate that employees equipped with adequate resources to do their jobs to the best of their abilities were more likely to recommend the workplace. These resources included training, supplies, equipment, or funding. This aligns with McGregor’s Theory Y view that employees generally self-motivated to perform at a high level and take pride in their work.31 Therefore, when employees do not feel that they have adequate resources allowing them to do so, they are less likely to view their organization as a desirable place to work.
Understaffing within the organization may also create difficulty in an employee being able to perform to the best of their ability. In both clinical and non-clinical areas, the ability of employees to pursue meaning and purpose in their work is largely dependent on having a reasonable workload and being able to use their higher-level skills. When staffing shortages occur, it often means taking on more work, and sometimes performing tasks that do not require their training or talents. For example, it has been noted that during the pandemic, staffing shortages required nurses to take on heavy patient loads, but also to do tasks typically handled by other team members such as respiratory therapists, patient care technicians, and food and nutrition services.32 In the present study, identifying understaffing as a major stressor was associated with a greater intent to leave the organization. More people leaving the organization may exacerbate understaffing, leading to further departures and a perpetuating cycle of turnover.
As healthcare organizations continue to experience financial pressures because of the COVID-19 pandemic, the mechanisms used in other industries to entice employees to stay, including increased wages and benefits, are largely untenable. Those that viewed inadequate pay or compensation as a major stressor were more likely to leave and less likely to recommend the organization to others. It is important to note that while adequacy of pay was significantly related to turnover and NPS, it was ranked 6th and 12th on the list in terms of its contribution to explaining the variance in those measures, respectively. This finding suggests that pay is an important consideration, but that it is not the leading cause of turnover or low NPS. This is consistent with research finding that toxic corporate culture was 10.4 times more likely to predict turnover than compensation.33,34 This suggests that in financially constrained settings where raises are infeasible, addressing the toxic culture elements and may represent another mechanism for retention.
Team Level Factors
An employee’s experience at work is a combination of experiences and perceptions at the organization-level and interactions within their own teams, with supervisors, and with colleagues. Therefore, it is not surprising that given the frequency of interaction with one’s supervisor, those who had a trusting relationship were more likely to stay and recommend the organization. Trust becomes the lens through which every other interaction is viewed and interpreted, making it a critical element of the supervisor–employee relationship. Employees that were satisfied with their recognition in the workplace reported higher NPSs on average. Together, these findings confirm the importance of supervisor behaviors in the aim to recruit and retain employees.
Employees with control over how their work is carried out, on average, were more likely to recommend the organization to others. Autonomy has been identified as an important human motivator.35 The empowering model of leadership seeks to help followers become self-leaders and encourages independent action, thereby offering supervisors a framework for increasing autonomy.36 Some elements of autonomy may be restricted in the clinical setting, where external bodies often regulate process requirements and rigid protocols can prevent harm. However, where possible, employees should be given autonomy to best conduct their work. For example, scheduling or flexibility in work location may represent an opportunity to increase autonomy while still meeting organizational needs. Those identifying unpredictability of schedule were less likely to recommend the organization. However, many organizations have embraced self-scheduling for portions of their workforce that allows employees some autonomy in choosing which shifts they will cover, offering some sense of control and predictability.37
Lastly, employees with a sense of belonging were less likely to indicate turnover intention and reported higher NPSs on average. Feeling a sense of belonging is likely a combination of interactions with colleagues, leaders, and even patients. However, the supervisor has an important role in creating a culture where team members feel included, are encouraged to participate, and where destructive behaviors such as discrimination, gossip, or micro-aggressions are not tolerated.
Individual Level Factors
A defining feature of healthcare is the deep sense of altruism, meaning and purpose that many find in their work. In this study, 87% of employees finding their work to be meaningful. This gives healthcare organizations an advantage over other industries, particularly as generations entering the workforce may place a higher value on meaningful work.38,39 However, this feature also has the potential to allow poor work design to persist. As such, workers may tolerate certain conditions because they feel so connected to the purpose in their work, whereas other industries may have to deliver a better employee experience to recruit and retain without the allure of meaningful work. These results suggest that while meaning in work is associated with improved turnover and NPSs, it is not enough to counteract low-trust or unsupportive environments. Furthermore, as production pressures increase, there is the potential to further erode the protective effect of meaning and purpose in the recruitment and retention equation. Similarly, those experiencing moral distress were more likely to leave, and less likely to recommend the organization. Because of the great sense of meaning in their work, when an employee feels unable to do what they believe to be right, the conflict may be even more jarring.
Burnout was the greatest predictor of intention to leave and was also associated with lower NPSs. Burnout among specific healthcare worker populations has been well documented,40–42 but our findings reiterate the relative importance of burnout on the recruitment and retention process. The toll of the COVID-19 pandemic and other societal stressors during that time-period were notable in the data, with employees reporting at least one symptom of PTSD from events from 2020 until 2022 showing a lower likelihood to recommend the organization. Interestingly, individuals who reported a higher count of nonwork stressors were more likely to report higher NPSs on average. Past research has demonstrated that, while work and nonwork stressors both contribute to common mental disorders, nonwork stressors are not associated with greater susceptibility to work stress.43 We postulate that, given the high levels of work meaning and purpose reported in the study sample, perhaps their jobs give them temporary reprieve from the stress of their homes and personal lives. Furthermore, given these many stressors and traumatic events, those with greater individual resilience were more likely to recommend the organization to others, though it explained little of the overall variance. Individual resilience was not statistically significantly associated with intention to leave.
In addition to these individual characteristics, some demographic features predicted turnover intention. Other than employees over age 65, for which retirement is an expected source of turnover, all age groups had lower turnover intent compared to the 18–24 age group. This is concerning as younger workers are vital to addressing the growing health needs of an aging population. The departure of this age group, coupled with an aging workforce, poses substantial challenges in maintaining a sustainable workforce. Non-white employees were more likely to intend to stay, while females and gender or sexual minorities were more likely to have intent to leave the organization. This is consistent with findings from McKinsey et al, who demonstrated that women in the workforce are more likely to leave for organizations than men and highly value organizations that have more flexibility, opportunities to advance, a reasonable workload and supportive managers.38 Demographic characteristics were largely insignificant for NPS, although those who declined to disclose their race reported lower NPSs on average. More research is needed to understand this dynamic.
Implications for Practice
Increased turnover intention in healthcare workers ignited by the COVID-19 pandemic continues to be an issue in the “post-pandemic” era.10,11 Thus, understanding what other non-monetary factors may facilitate recruitment and retention of this workforce is vital. In the present study, the findings of the importance of trust in direct supervisor and trust in top leadership for both turnover intentions and NPSs have direct implications for healthcare practice.
First, healthcare organizations must recognize and appreciate the importance of trust in their organizations for establishing and maintaining employee well-being and job satisfaction. In times of crisis, such as the COVID-19 pandemic, employees tend to look to their managers and senior leadership for guidance and support.44 Unfortunately, many managers are also experiencing burnout and distress,7 so their ability to provide emotional support to others may be strained. We suggest supervisors and leaders prioritize recognition of their employees and teams. Frequent interactions with employees offer leaders opportunities to listen to employee frustrations and ideas, and subsequently build relationships and trust. For senior leaders that cannot feasibly have individual meetings with all employees, frequent and high-quality rounding is a practice that can lead to a variety of positive outcomes. A large study with over 16,000 observations noted that high-quality leader rounding is associated with higher workforce engagement, readiness for improvement, and lower burnout.45
Second, our results point to the importance of timely and frequent communication for the development of trust. Research has consistently demonstrated the importance of open communication for establishing trust in organizations.46,47 Especially in times of crisis, leaders must be open and honest about what is known and not known within the organization. Communication with employees should increase as crisis and stress levels rise. Employees need to feel connected and have a shared sense of purpose during times of crisis. When communication levels are low during periods of high stress, employees tend to look to other sources for information and guidance, which can often be wrong and confusing for employees.
Third, our findings that autonomy predicted NPS support the assertion that employees today demand more flexibility and autonomy. This has become more pronounced in the pandemic-fueled Great Resignation48,49 and, similar to other industries, healthcare workers are voting with their feet. Unfortunately, flexibility can be difficult in the patient-driven medical field; however, one potential solution might be to introduce more opportunities for job crafting to increasing feelings of autonomy. Job crafting is a process by which employees make changes to the resources or demands of the job to improve the fit between the job and their skills, abilities and interests.50 For example, a physician preferring telemedicine may be able to conduct more telemedicine visits by trading with a physician that misses more in-person interaction with patients. In this example, both individuals get more enjoyment in their work and the organizational objectives are still met. Overall, healthcare leaders should encourage their employees to job craft and find other meaningful ways to add autonomy and flexibility to their already stressful and overwhelming jobs.
Finally, our results further solidify the importance of effective leadership in healthcare organizations, as evidenced by the findings that both trust in direct supervisor and trust in top leadership were significant predictors of both turnover intention and NPS. Leadership has taken center stage since the pandemic, and the importance of effective leadership in healthcare organizations cannot be overstated. Leadership consistently ranks as one of the most important factors in employee job satisfaction,51,52 and our findings suggest that healthcare leadership is critical in the current healthcare landscape. Leadership is also accountable for toxic work environments, which were identified as important to turnover intentions in the present sample. Healthcare organizations should continue to invest in leadership development opportunities and training for their managers and leaders. Moreover, given the state of the current healthcare employment crisis, healthcare organizations should promote and reward managers who effectively create positive work environments and trusting relationships with employees.
There are a few limitations to this study. First, the data is collected from a single organization, and therefore may not be generalizable to other organizations. Additionally, the study is cross-sectional, and therefore no causality can be implied in the findings. Lastly, we measure only intent to stay within an organization, not whether people actually stayed or left. Despite these limitations, this study provides important insight for healthcare leaders working to retain their current employees and recruit for the future in the face of massive historic worker shortages and financial pressures.
Conclusion
This study meets a gap in the literature by exploring factors associated with retention of the entire healthcare team, including both clinical and non-clinical employees in the post-pandemic period. Further, this study contributes to the understanding of the role of meaningful work as a job resource in healthcare and the relative contribution of that resource compared to other job resources and demands. Encouragingly, this study emphasizes the importance of many non-monetary elements of the employee experience which may offer financially constrained leaders with feasible options for improvement. The findings suggest that leadership behaviors and relationships, autonomy, and reasonable workload through improved staffing remain high-impact opportunities for improving recruitment and retention across the entire healthcare team. The strong sense of meaning and purpose in healthcare is not sufficient to overcome unhealthy cultures and overwork. To further understand the complexity of healthcare workers’ intentions to stay within an organization and recommend it to others, we suggest more research using qualitative and mixed methods approaches are needed. Further research is needed on whether these factors also predict actual departure from the organization, beyond one’s stated intentions.
Disclosure
David A. Rogers has received funding from ProAssurance. Laurence M. Boitet has received funding from an NIH/NIGMS Institutional Research and Academic Career Development Award (K12 GM088010 to LMB). Katherine A. Meese has received book royalties from Jones & Bartlett Publishers; speaker honoraria from American College of Healthcare Executives. For the remaining authors, none are declared.
References
1. Missel M, Bernild C, Dagyaran I, Christensen SW, Berg SK. A stoic and altruistic orientation towards their work: a qualitative study of healthcare professionals’ experiences of awaiting a COVID-19 test result. BMC Health Serv Res. 2020;20(1):1031. doi:10.1186/s12913-020-05904-0
2. Caruso CC, Arbour MW, Berger AM, et al. Research priorities to reduce risks from work hours and fatigue in the healthcare and social assistance sector. Am J Ind Med. 2022;65(11):867–877. doi:10.1002/ajim.23363
3. Aiken LH, Sloane DM, Clarke S, et al. Importance of work environments on hospital outcomes in nine countries. Int J Qual Health Care. 2011;23(4):357–364. doi:10.1093/intqhc/mzr022
4. Meese KA, Colón-López A, Montgomery AP, Boitet LM, Rogers DA, Patrician PA. Rules of engagement: the role of mistreatment from patients in the nurse, physician and advanced practice provider experience. Patient Exp J. 2022;9(2):36–45. doi:10.35680/2372-0247.1719
5. Millenbach L, Crosby FE, Niyirora J, et al. Impact of COVID-19 pandemic on nurses: where is the financial safety net? Online J Issues Nurs. 2021;26(2). doi:10.3912/OJIN.Vol26No02Man01
6. Andel SA, Tedone AM, Shen W, Arvan ML. Safety implications of different forms of understaffing among nurses during the COVID‐19 pandemic. J Adv Nurs. 2022;78(1):121–130. doi:10.1111/jan.14952
7. Meese KA, Colón-López A, Singh JA, Burkholder GA, Rogers DA. Healthcare is a team sport: stress, resilience, and correlates of well-being among health system employees in a crisis. J Healthc Manag. 2021;66(4):304–322. doi:10.1097/JHM-D-20-00288
8. Dyrbye LN, West CP, Sinsky CA, et al. Physicians’ Experiences with mistreatment and discrimination by patients, families, and visitors and association with burnout. JAMA Netw Open. 2022;5(5):e2213080. doi:10.1001/jamanetworkopen.2022.13080
9. Meese KA, Colon-Lopez A, Dill R, Naik GA, Cendoma PJ, Rogers DA. Perceptions of inequitable compensation reductions among healthcare workers during covid-19. J Health Care Finance. 2021;2021;1.
10. Maurer R. Turnover ‘tsunami’ expected once pandemic ends; 2021. Available from: http://www.deltapeo.com/wp-content/uploads/2021/03/Turnover-‘Tsunami-Expected-Once-Pandemic-Ends.pdf.
11. Hendrickson RC, Slevin RA, Hoerster KD, et al. The impact of the COVID-19 pandemic on mental health, occupational functioning, and professional retention among health care workers and first responders. J Gen Intern Med. 2022;37(2):397–408. doi:10.1007/s11606-021-07252-z
12. Seligman M. Flourish: a visionary new a understanding of happiness and well-being. Policy. 2011;27(3):60–61.
13. Bakker AB, Demerouti E. The job demands-resources model: state of the art. J Manage Psychol. 2007;22(3):309–328. doi:10.1108/02683940710733115
14. Pangallo A, Atwell T, Roe K, Boissy A. Understanding modern drivers of the employee experience in healthcare. Patient Exp J. 2022;9(2):46–61. doi:10.35680/2372-0247.1710
15. Tai TW, Bame SI, Robinson CD. Review of nursing turnover research, 1977–1996. Soc Sci Med. 1998;47(12):1905–1924. doi:10.1016/S0277-9536(98)00333-5
16. Brown MI. Comparing the validity of net promoter and benchmark scoring to other commonly used employee engagement metrics. Hum Resour Dev Q. 2020;31(4):355–370. doi:10.1002/hrdq.21392
17. Eisenberger R, Huntington R, Hutchison S, Sowa D. Perceived organizational support. J Appl Psychol. 1986;71(3):500–507. doi:10.1037/0021-9010.71.3.500
18. Ogbonnaya C, Tillman CJ, Gonzalez K. Perceived organizational support in health care: the importance of teamwork and training for employee well-being and patient satisfaction. Group Organ Manag. 2018;43(3):475–503. doi:10.1177/1059601118767244
19. National Center for Organization Development. VA All Employee Survey. U.S. Department of Veterans Affairs; 2020.
20. Dyrbye LN, Satele D, Shanafelt T. Ability of a 9-item well-being index to identify distress and stratify quality of life in US workers. J Occup Environ Med. 2016;58(8):810–817. doi:10.1097/JOM.0000000000000798
21. American Medical Association. AMA STEPS Forward Mini Z Burnout Survey. American Medical Association; 2015.
22. Chari R, Chang -C-C, Sauter SL, Patrun Sayers EL, Huang W, Fisher GG. NIOSH Worker Well-Being Questionnaire (Wellbq). U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH); 2021.
23. Vaishnavi S, Connor K, Davidson JR. An abbreviated version of the Connor-Davidson Resilience Scale (CD-RISC), the CD-RISC2: psychometric properties and applications in psychopharmacological trials. Psychiatry Res. 2007;152(2–3):293–297. doi:10.1016/j.psychres.2007.01.006
24. Luchman J. DOMIN: stata module to conduct dominance analysis; 2023.
25. Poon Y-SR, Lin YP, Griffiths P, Yong KK, Seah B, Liaw SY. A global overview of healthcare workers’ turnover intention amid COVID-19 pandemic: a systematic review with future directions. Human Resour Health. 2022;20(1):1–18. doi:10.1186/s12960-022-00764-7
26. Fukui S, Wu W, Salyers MP. Impact of supervisory support on turnover intention: the mediating role of burnout and job satisfaction in a longitudinal study. Adm Policy Ment Health Ment Health Serv Res. 2019;46(4):488–497. doi:10.1007/s10488-019-00927-0
27. Ilyas A, Khan AH, Zaid F, Ali M, Razzaq A, Khan WA. Turnover intention of employees, supervisor support, and open innovation: the role of illegitimate tasks. J Open Innov. 2020;6(4):128. doi:10.3390/joitmc6040128
28. Meister J. The future of work is employee well-being; 2021. Available from: https://www.forbes.com/sites/jeannemeister/2021/08/04/the-future-of-work-is-worker-well-being/?sh=4befcf884aed.
29. Stewart WF, Ricci JA, Chee E, Morganstein D. Lost productive work time costs from health conditions in the United States: results from the American productivity audit. J Occup Environ Med. 2003;45(12):1234–1246. doi:10.1097/01.jom.0000099999.27348.78
30. McKinsey & Company. Companies need to hold on to the leaders shaping the future of work; 2022. Available from: https://leanin.org/women-in-The-workplace/2022/companies-need-to-hold-on-to-The-leaders-shaping-The-future-of-work.
31. Lawter L, Kopelman RE, Prottas DJ. McGregor’s theory X/Y and job performance: a multilevel, multi-source analysis. J Managerial Issues. 2015;2015;84–101.
32. Colón-López A, Meese KA, Montgomery AP, Patrician PA, Rogers DA, Burkholder GA. Unique stressors in a global pandemic: a mixed methods study about unique causes of distress among healthcare team members during COVID-19. J Hosp Manag Health Policy. 2022;6:23. doi:10.21037/jhmhp-21-69
33. Sull D, Sull C, Cipolli W, Brighenti C. Why every leader needs to worry about toxic culture; 2022. Available from: https://sloanreview.mit.edu/article/why-every-leader-needs-to-worry-about-toxic-culture/.
34. Sull D, Sull C, Zweig B. Toxic culture is driving the great resignation. MIT Sloan Manage Rev. 2022;63(2):1–9.
35. Pink DH. Drive: The Surprising Truth About What Motivates Us. Penguin; 2011.
36. Pearce CL, Sims HP Jr. Vertical versus shared leadership as predictors of the effectiveness of change management teams: an examination of aversive, directive, transactional, transformational, and empowering leader behaviors. Group Dyn Theory Res Pract. 2002;6(2):172.
37. Wynendaele H, Gemmel P, Pattyn E, Myny D, Trybou J. Systematic review: what is the impact of self‐scheduling on the patient, nurse and organization? J Adv Nurs. 2021;77(1):47–82. doi:10.1111/jan.14579
38. Casic AP. Gen Z in the workplace: what matters to young professionals at work — and what turns them off; 2022. Available from: https://www.talentlms.com/research/gen-z-workplace-statistics#what-matters-to-Gen-Z.
39. Deloitte. The Deloitte global 2021 gen Z and millennial survey; 2021. Available from: https://www.deloitte.com/content/dam/assets-shared/legacy/docs/insights/2022/2021-deloitte-global-millennial-survey-report.pdf.
40. Melnikow J, Padovani A, Miller M. Frontline physician burnout during the COVID-19 pandemic: national survey findings. BMC Health Serv Res. 2022;22(1):365. doi:10.1186/s12913-022-07728-6
41. Murthy VH. Confronting health worker burnout and well-being. N Engl J Med. 2022;387(7):577–579. doi:10.1056/NEJMp2207252
42. Sinsky CA, Shanafelt TD, Dyrbye LN, Sabety AH, Carlasare LE, West CP. Health care expenditures attributable to primary care physician overall and burnout-related turnover: a cross-sectional analysis.
43. Clark C, Pike C, McManus S, et al. The contribution of work and non-work stressors to common mental disorders in the 2007 adult psychiatric morbidity survey. Psychol Med. 2012;42(4):829–842. doi:10.1017/S0033291711001759
44. McKinsey & Company. Communications get personal: how leaders can engage employees during a return to work; 2020. Available from: https://www.mckinsey.com/capabilities/people-and-organizational-performance/our-insights/communications-get-personal-how-leaders-can-engage-employees-during-a-return-to-work.
45. Sexton JB, Adair KC, Leonard MW, et al. Providing feedback following Leadership WalkRounds is associated with better patient safety culture, higher employee engagement and lower burnout. BMJ Qual Saf. 2018;27(4):261–270. doi:10.1136/bmjqs-2016-006399
46. Guzzo RF, Wang X, Madera JM, Abbott J. Organizational trust in times of COVID-19: hospitality employees’ affective responses to managers’ communication. Int J Hospitality Manage. 2021;93:102778. doi:10.1016/j.ijhm.2020.102778
47. Jem R. How effective communication improves employee trust and engagement; 2020. Available from:: https://www.hrcloud.com/blog/how-effective-communication-improves-employee-trust-and-engagement.
48. Oladipupo S. More evidence lack of flexibility drives the great resignation; 2022. Available from: https://www.hcmtechnologyreport.com/more-evidence-lack-of-flexibility-drives-The-great-resignation/.
49. Patton C. 2 keys to stopping the ‘great resignation’? Flexibility and trust; 2021. Available from; https://hrexecutive.com/2-keys-to-stopping-The-great-resignation-flexibility-and-trust/.
50. Dubbelt L, Demerouti E, Rispens S. The value of job crafting for work engagement, task performance, and career satisfaction: longitudinal and quasi-experimental evidence. Eur J Work Org Psychol. 2019;28(3):300–314. doi:10.1080/1359432X.2019.1576632
51. Leimbach M, Worldwide WL. Redefining employee satisfaction. Wilson Learn. 2006;2006:1.
52. Belias D, Koustelios A. Leadership and job satisfaction--a review. Eur Sci J. 2014;10(8):1.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Workplace Belonging of Women Healthcare Professionals Relates to Likelihood of Leaving
Schaechter JD, Goldstein R, Zafonte RD, Silver JK
Journal of Healthcare Leadership 2023, 15:273-284
Published Date: 26 October 2023