Back to Journals » Journal of Pain Research » Volume 18
Does Thunder-Fire Moxibustion Really Augment Therapeutic Efficacy in Knee Osteoarthritis? Methodological Critique of A Recent Pairwise Meta-Analysis [Letter]
Authors Zhao FY ![]() , Fu QQ
, Fu QQ ![]() , Ho YS
, Ho YS
Received 10 July 2025
Accepted for publication 16 July 2025
Published 23 July 2025 Volume 2025:18 Pages 3717—3722
DOI https://doi.org/10.2147/JPR.S551887
Checked for plagiarism Yes
Editor who approved publication: Professor Michael Überall
Fei-Yi Zhao,1–4,* Qiang-Qiang Fu,5,* Yuen-Shan Ho6
1Department of Nursing, School of International Medical Technology, Shanghai Sanda University, Shanghai, 201209, People’s Republic of China; 2School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, 3083, Australia; 3Sydney School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, 2050, Australia; 4Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200071, People’s Republic of China; 5Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China; 6School of Nursing, Faculty of Health and Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuen-Shan Ho, School of Nursing, Faculty of Health and Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China, Tel +852 2766 6410, Fax +852 2364 9663, Email [email protected] Fei-Yi Zhao, Department of Nursing, School of International Medical Technology, Shanghai Sanda University, Shanghai, 201209, People’s Republic of China, Tel +86 5021-0894, Fax +86 5021 0895, Email [email protected] [email protected]
View the original paper by Dr Wei and colleagues
Dear editor
We appreciate Wei et al’s meta-analysis1 assessing Thunder-Fire Moxibustion (TFM) combined with other Traditional Chinese Medicine (TCM) modalities for knee osteoarthritis (KOA). However, we would like to raise some points for further discussion, as we believe that addressing these could enhance future studies and improve the robustness of the evidence in this field.
First, the title’s phrasing “Osteoarthritis Knee” is non-standard. “Knee Osteoarthritis” or “Osteoarthritis of the Knee” are clinically accepted terms.
Second, while the study aimed to evaluate TFM combined with other TCM therapies for KOA through parallel-group RCTs, five included trials used controls that deviate from optimal methodological standards, such as waitlist controls, perfectly matched placebos, or guideline-recommended standard care (eg, land or aquatic exercise, topical/oral NSAIDs, intra-articular corticosteroid injections, or surgical treatment).2 We acknowledge that excluding non-standard comparators is ideal, but may not always be feasible due to ethical or practical considerations. Thus, should the authors opt to include these trials with non-standard controls to enhance review comprehensiveness, a network meta-analysis approach, as discussed later, would be preferable, as it can effectively address inherent heterogeneity and better estimate comparative efficacy among multiple interventions.
Third, the exclusive reliance on clinical efficacy rate as the sole outcome measure is problematic due to substantial heterogeneity in calculation methods across studies and incomplete reporting of derivation procedures in some trials (Table 1). These methodological limitations fundamentally compromise the validity of pooled estimates. More standardized outcome measures, such as the Visual Analog Scale, Numeric Rating Scale, Western Ontario and McMaster Universities Arthritis Index, and Knee Injury and Osteoarthritis Outcome Score, would have better captured clinical efficacy and contributed to mitigating heterogeneity.
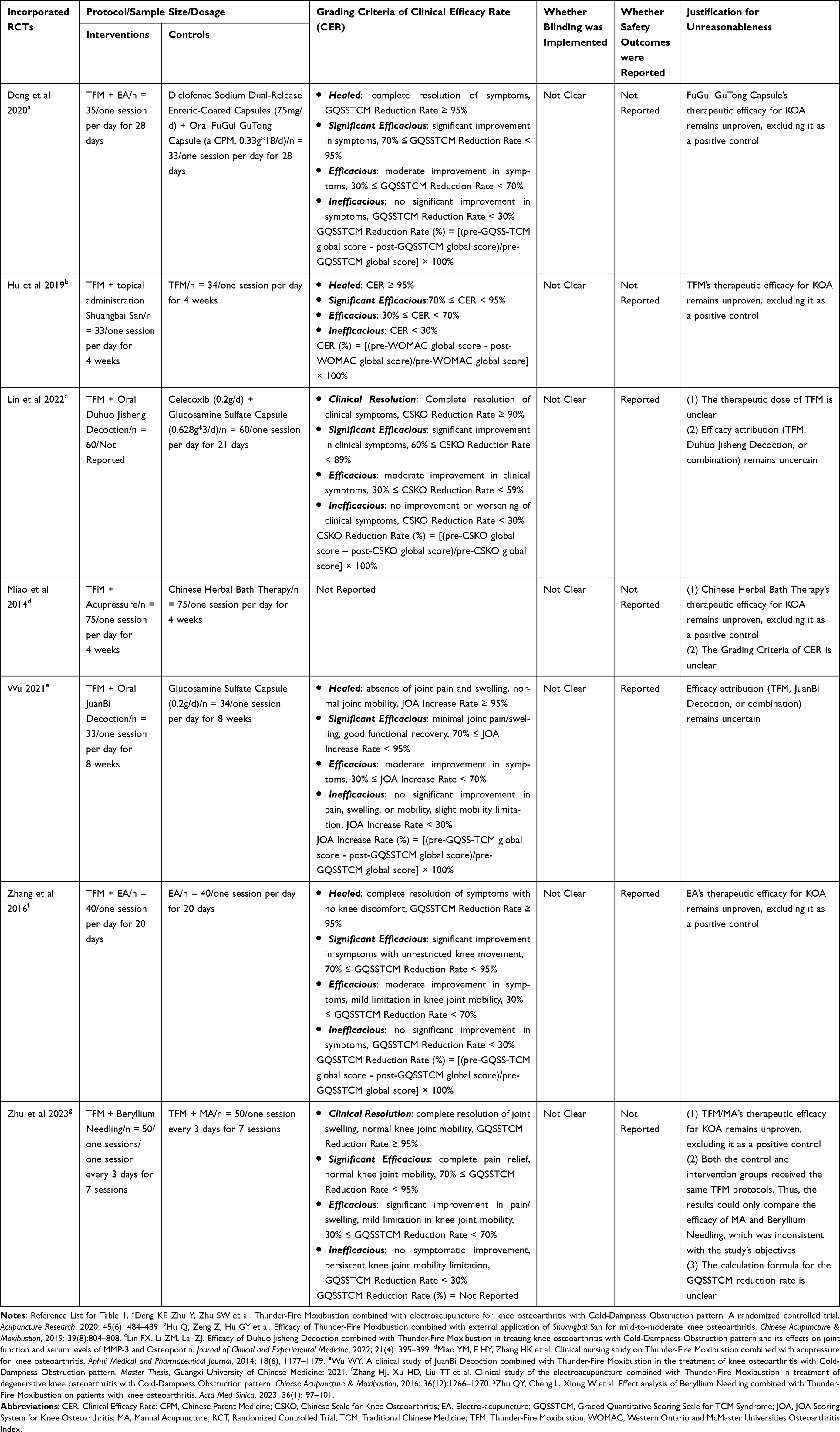 |
Table 1 Evaluation of Methodological Limitations in the Seven RCTs Included by Wei et al |
Fourth, in Wei et al’s meta-analysis, heterogeneous TCM modalities (eg, various topical and oral herbal medicines, and different acupuncture or acupressure methods) were combined into broad subgroups, with minimal justification provided for this aggregation. This approach, coupled with the mixing of conventional and traditional medicine controls, poses challenges to clinical comparability and undermines the interpretability of effect estimates. We recommend clearer subgrouping with sufficient justification or the adoption of a network meta-analysis approach to establish efficacy hierarchies when addressing such clinical diversity. Notably, even though the intervention and control groups included multiple therapies, Wei et al’s analysis reported minimal heterogeneity (I² = 0%).
Fifth, methodological concerns exist in RoB assessment using RoB 2.0 Tool:3 (1) Three RCTs failing to report safety outcomes were incorrectly rated as low RoB for “Selective Outcome Reporting”; and (2) Four trials without reported outcome assessor blinding were judged as having low risk for “Measurement of Outcomes”, when “Some Concerns” would have been more appropriate.
Sixth, the application of the GRADE framework4 could be further refined. Given the substantial heterogeneity across included RCT designs, the “Indirectness” domain might warrant downgrading, contrary to the authors’ assertion that “no downgrade was needed”. Moreover, the absence of standard controls and inadequate blinding in the included trials warrant downgrading in the “Limitations” domain. Even under the authors’ own criteria, “Incidence of Adverse Reactions” outcome presents multiple concerns across domains and should have been rated as “Very Low” certainty rather than “Low”.
Seventh, based on the inclusion criteria outlined by Wei et al, we identified at least five eligible RCTs—without applying a formal search strategy—that were not included in their analysis (Table 2). This suggests that a substantial number of relevant studies may have been overlooked. Such omissions significantly affect the validity and outcomes of their meta-analysis.
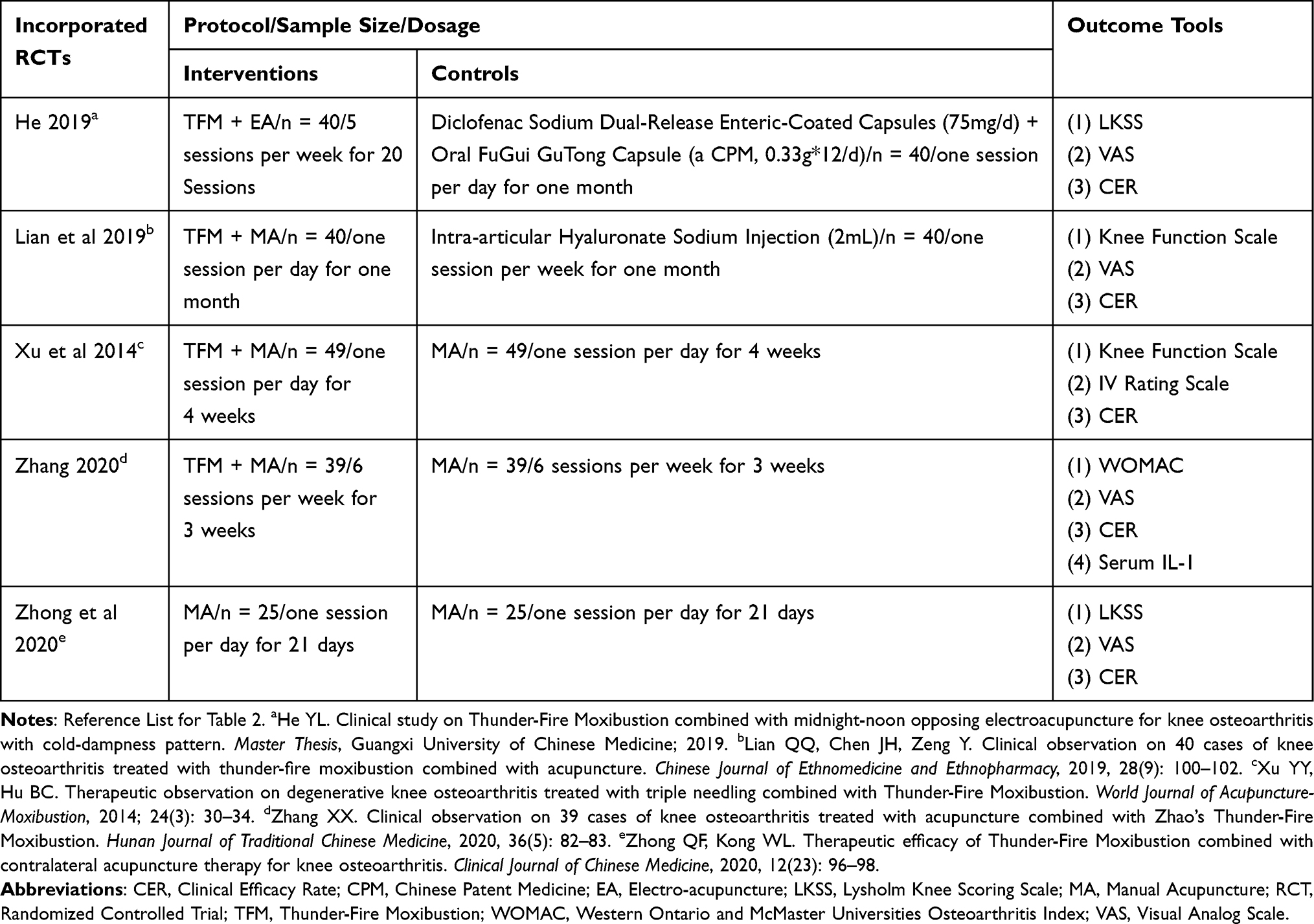 |
Table 2 Eligible RCTs Meeting Wei et al’s Inclusion Criteria but Omitted from Their Meta-Analysis |
Lastly, we encourage future systematic reviews to register their protocols in advance. Protocol registration enhances transparency, reduces research duplication, and minimizes selective reporting, thereby improving the overall credibility of the review process.5
In conclusion, while Wei et al’s study offers preliminary evidence for TMF combined with other TCM therapies in KOA, its methodological limitations necessitate resolution for more robust and clinically translatable findings. Future studies should: (1) adopting stricter inclusion criteria to ensure high-quality evidence synthesis, ideally using network meta-analysis to compare intervention effects, and (2) unbiasedly evaluating the efficacy and safety of TMF as a monotherapy and as an adjunct to standard care separately. We hope these constructive suggestions foster further academic dialogue and methodological refinement within this field.
Abbreviations
GRADE, Grades of Recommendation, Assessment, Development, and Evaluation; KOA, Knee Osteoarthritis; NSAID(s), Non-Steroidal Anti-Inflammatory Drug(s); RCT(s), Randomized Controlled Trials; RoB, Risk of Bias; RoB 2.0 Tool, Revised Cochrane Risk-of-Bias Tool for Randomized Trials; TCM, Traditional Chinese Medicine; TFM, Thunder-Fire Moxibustion.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author Contributions
Fei-Yi Zhao: Conceptualization, Investigation, Formal analysis, Writing - original draft. Qiang-Qiang Fu: Methodology, Formal analysis, Writing - review & editing. Yuen-Shan Ho: Conceptualization, Methodology, Formal analysis, Writing - review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no competing interests in this communication.
References
1. Wei W, Qin Y, Lin J. Effectiveness of combination of thunder fire moxibustion with other forms of traditional Chinese medicine for osteoarthritis knee: a meta-analysis. J Pain Res. 2025;18:3087–3099. doi:10.2147/JPR.S502457
2. Langworthy M, Dasa V, Spitzer AI. Knee osteoarthritis: disease burden, available treatments, and emerging options. Ther Adv Musculoskelet Dis. 2024;16:1759720X241273009. doi:10.1177/1759720X241273009
3. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
4. Phillips M. Healthcare recommendations: grades of recommendation, assessment, development, and evaluation (GRADE) approach. Evidence-Based Orthopedics. 2021;19–23. doi:10.1002/9781119413936.ch4
5. Tawfik GM, Giang HTN, Ghozy S, et al. Protocol registration issues of systematic review and meta-analysis studies: a survey of global researchers. BMC Med Res Methodol. 2020;20(1):213. doi:10.1186/s12874-020-01094-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.