Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Does Interprofessional Scenario-Based Simulation Training Change Attitudes Towards Interprofessional Learning – A Pretest-Posttest Study
Authors Reime MH ![]() , Aarflot M, Kvam FI
, Aarflot M, Kvam FI
Received 9 April 2022
Accepted for publication 1 July 2022
Published 19 July 2022 Volume 2022:15 Pages 1527—1532
DOI https://doi.org/10.2147/JMDH.S370100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marit Hegg Reime,1 Morten Aarflot,2 Fred-Ivan Kvam1
1Department of Health and Caring Sciences, Western Norway University of Applied Sciences, Bergen, Norway; 2Oslo University Hospital, Oslo, Norway
Correspondence: Marit Hegg Reime, Department of Health and Caring Sciences, Western Norway University of Applied Sciences, Post Box 7030, Inndalsveien 28, Bergen, 5020, Norway, Tel +4755585505, Email [email protected]
Purpose: To investigate readiness for interprofessional learning (IPL) among Norwegian health-care students at bachelor-, postgraduate- and master’s level, before and after participating in a one-day scenario-based simulation-training course.
Participants and Methods: A pretest-posttest study using readiness for interprofessional learning scale (RIPLS) was conducted with bachelor nursing students (n = 123, 4th semester), postgraduate nursing students from anesthesia, operating theatre and intensive care (n = 61, 1st semester) and medical students (n = 78, 10th semester).
Results: Bachelor nursing students and postgraduate nursing students scored significantly higher in the posttest on all four subscales and on the total scale. Between professions, medical students scored significantly higher on subscale 1 (teamwork and collaboration) and subscale 3 (positive professional identity) and significantly lower on subscale 4 (roles and responsibilities) in the pretest. In the posttest bachelor nursing students scored significantly higher on subscale 2 (negative professional identity) and medical students scored significantly lower on subscale 4. The internal consistency for RIPLS was acceptable, except for subscale 4.
Conclusion: The study indicates readiness for IPL in our sample of Norwegian health-care students. RIPLS had the ability to measure significant changes in attitudes both within each profession and between professions.
Keywords: interprofessional education, pretest-posttest study, RIPLS, simulation
Introduction
Understanding various roles and responsibilities and the ability to interact towards common goals is essential for strengthening health-care students’ ability for interprofessional cooperation within the professional field.1 In Norway, the curricula for bachelor and master degrees within the health and social field share common learning outcomes regarding interprofessional cooperation and communication,2 but training together still remains challenging due to logistics. Studies on Norwegian health-care students’ attitudes towards interprofessional learning (IPL) are therefore scarce.3 The Readiness for Interprofessional Learning Scale (RIPLS) measures attitudes towards interprofessional shared learning. However, studies have shown inconsistency in the scale’s ability to measure change in attitudes in pretest-posttest studies.3–5
Interprofessional education (IPE) takes place when two or more professions learn about, from and with each other to enable effective collaboration and improve attitudes and health outcomes.6,7 Several studies have found that nursing students present more positive beliefs about teamwork and collaboration compared to medical students.7–11 Other reports describe difficulties in engaging medical students in IPL because of development of a mono-professional identity,12 favoring uniprofessional learning at the expense of interprofessional learning. Fisher, King13 conclude that there is a strong need to further research student’s opinion of IPE.
Aim
The aim of this study was to investigate readiness for IPL among Norwegian health-care students at bachelor-, postgraduate- and master’s level, before and after participating in a one-day scenario-based simulation-training course. Bringing these three different study level programs together on the same training course represents a novelty in IPL research.
Materials and Methods
Design and Participants
A pretest-posttest study was conducted with bachelor nursing students (n = 123, 4th semester), postgraduate nursing students from anesthesia, operating theatre and intensive care (n = 61, 1st semester) and medical students (n = 78, 10th semester).
Instrument
The revised version of the 19 item RIPLS with four subscales (teamwork and collaboration, negative professional identity, positive professional identity, roles and responsibilities) was chosen,14 because it is the most widely used scale measuring attitudes towards IPL.5 The items are scored on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = undecided, 4 = agree, 5 = strongly agree). Given the reverse scoring of items in subscale two and four, higher scores on each subscale suggest more positive attitudes to IPE. RIPLS has been translated into several languages, including Norwegian.3,15
Intervention
The intervention consisted of a one-day scenario-based simulation-training course. The 262 students were divided into 44 interprofessional teams, each team comprising 5–6 students. The training took place in a hospital clinical skills laboratory and the course extended over a period of seven weeks. Four scenarios were developed for the training: hypovolemic shock, anaphylactic reaction, a child with fever seizure and low blood sugar and a trauma patient losing consciousness due to increasing intracranial pressure. The facilitator group was interprofessional and consisted of six trained facilitators. Skills in patient observation, clinical reasoning, problem-solving, leadership, teamwork, communication, prioritization, delegation, and medication practice were the subjects of the training. All students experienced being both in the participant role and the observer role. Each course day started and ended with filling in a paper-based RIPLS questionnaire.
Statistical Analysis
The Statistical Package for the Social Science (SPSS) version 24 was used for statistical analysis. The Kruskal–Wallis test compared the difference between professions on each subscale, the Wilcoxon signed-rank test compared pretest-posttest data for each subscale and the Mann–Whitney U test compared the difference between pretest and posttest data within dichotomous variables. Cronbach’s alpha measured internal consistency of RIPLS and its subscales. A two-tailed significance level of p < 0.05 was used for all tests.
Ethical Considerations
All students gave written informed consent for participation in the study. The Norwegian Centre for Research Data approved the study (No.23713).
Results
All 262 students answered the pretest, and 260 the posttest (99%). Characteristics of participants according to profession are reported in Reime, Kvam, Johnsgaard, Aarflot.16 When looking at scores between pretest and posttest within each profession, bachelor nursing students and postgraduate nursing students scored significantly higher in the posttest, on three subscales or on all four subscales, respectively, in addition to the total score (Table 1).
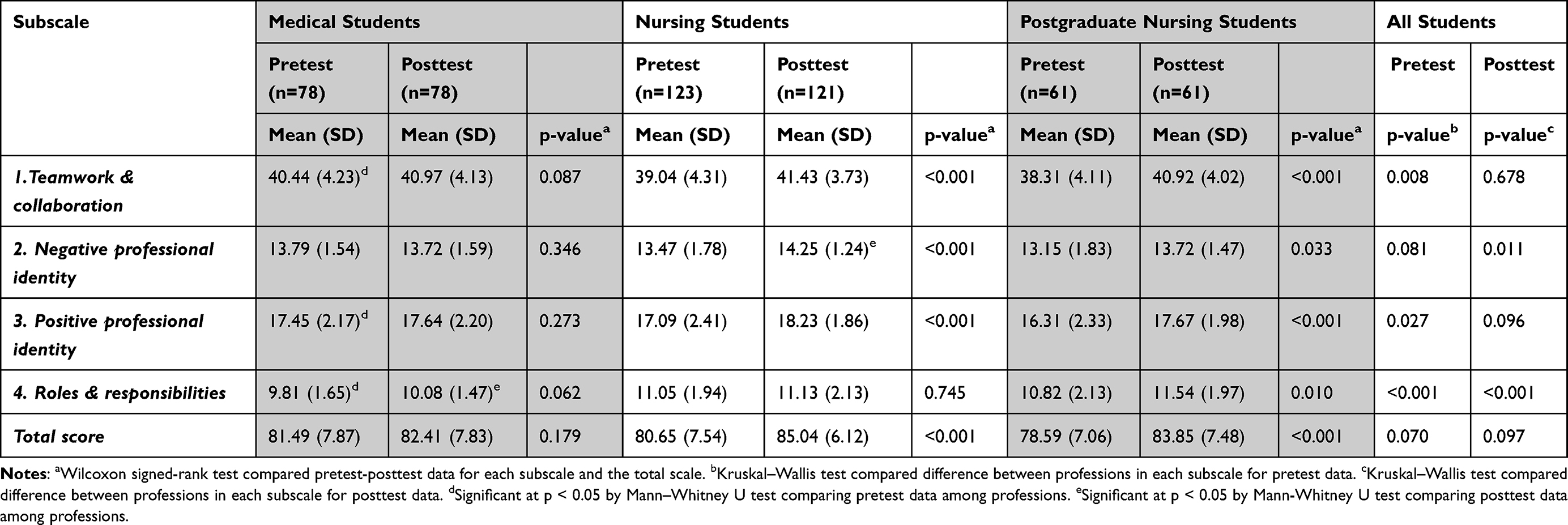 |
Table 1 Comparison of RIPLS Scores Between Professions for Subscales and for the Total Scale at Baseline (Pretest) and After Intervention (Posttest) |
When looking at scores between professions, medical students scored significantly higher on subscale 1 and subscale 3 and significantly lower on subscale 4 in the pretest. After intervention, bachelor nursing students scored significantly higher on subscale 2 and medical students scored significant lower on subscale 4 (Table 1). The internal consistency for RIPLS was acceptable except for subscale 4 (Table 2).17
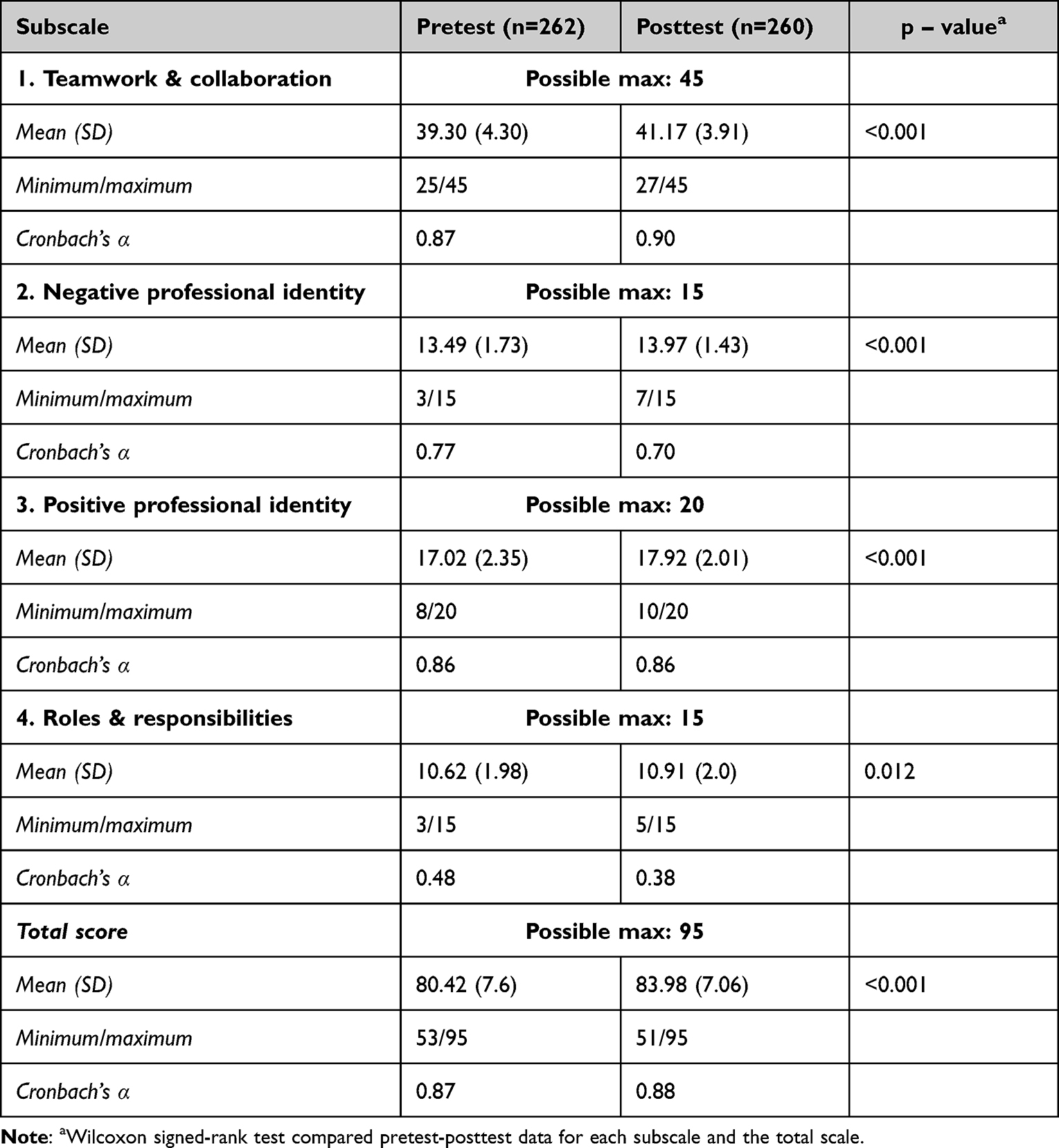 |
Table 2 Comparison of Total and Subscale Scores of RIPLS at Baseline (Pretest) and After Intervention (Posttest) |
Discussion
Our study found that medical students scored significantly higher on teamwork and collaboration in the pretest compared to the two nursing professions, deviating from studies showing that nursing students presented more positive beliefs on this domain.7–11 One explanation may be that medical students were in their final year of education and that clinical placement experiences had given them positive attitudes regarding cooperation with the nursing profession. Compared to results in the study of McFadyen, Webster, Maclaren, O’neill,18 our students reported higher mean scores on all four domains. A high score on the subscale negative professional identity should be interpreted as strong support against a negative attitude.18 On this subscale, all professions had high mean scores, but nursing students had significantly higher scores in the posttest compared to the other professions. However, our results indicate that both on subscale 2 and subscale 3 all student groups found it highly valuable learning together with other professions, which opposes preferences for mono-professional groups.12 Regarding subscale 4, medical students had significant lower scores both in the pretest and the posttest compared to the two nursing groups. This subscale concerns roles and responsibility and may reflect that medical students think they have to acquire much more knowledge and skills than other health-care students. Looking at the total score, the mean score in the pretest ranged from 83% to 86%, and in the posttest from 87% to 90% of the possible maximum of the whole scale (derived from data in Table 1). This indicate positive attitudes to shared learning among all student groups. The two nursing groups had significantly higher scores in the posttest, indicating that scenario-based simulation and ad hoc interprofessional teams had strengthened attitudes towards shared learning. This is in line with findings from Burford, Greig, Kelleher, Merriman, Platt, Richards, Davidson, Vance.19
The RIPLS is still the most used scale measuring IPL attitudes.5 However, low internal consistency on the subscale Roles and Responsibility, questions the scale’s reliability.20 Our result shows that subscale 1, 2 and 3 have satisfactory internal consistency, but not subscale 4 (Table 2). This is in line with other studies using RIPLS,21–26 as any α<0.60 should be thought unacceptable.27
Methodological Considerations
This study was limited to two educational institutions. Caution is also required as RIPLS is a self-report questionnaire. Doing pretest-posttest studies the same day may lead to complacency of respondents. Other research methods than using attitude scales may be needed to fully account for attitudes when participating in IPE activities, in addition to assessing if these attitudes are sustained.28
Conclusion
High mean values on RIPLS for all students’ groups on all four subscales indicate readiness for IPL in our sample of Norwegian health-care students. RIPLS had the ability to measure significant changes in attitudes both within each profession and between professions.
Acknowledgments
We wish to thank the participating students and the facilitators leading the scenario-based simulations. We also thank Western Norway University of Applied Sciences for supporting the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Patient safety research. A guide to developing training programmes; 2012. Available from: http://apps.who.int/iris/bitstream/10665/75359/1/9789241503440_eng.pdf.
2. Ministry of Education and Research. National Curriculum Regulations for Norwegian Health and Welfare Education (RETHOS); 2019. Available from: https://www.regjeringen.no/no/tema/utdanning/hoyere-utdanning/utvikling–av–nasjonale–retningslinjer–for–helse—og–sosialfagutdanningene/id2569499/.
3. Torsvik M, Johnsen HC, Lillebo B, Reinaas LO, Vaag JR. Has “The ceiling” Rendered the readiness for interprofessional learning scale (RIPLS) outdated? J Multidiscip Healthc. 2021;14:523. doi:10.2147/JMDH.S296418
4. Oates M, Davidson M. A critical appraisal of instruments to measure outcomes of interprofessional education. Med Educ. 2015;49(4):386–398. doi:10.1111/medu.12681
5. Berger-Estilita J, Fuchs A, Hahn M, Chiang H, Greif R. Attitudes towards interprofessional education in the medical curriculum: a systematic review of the literature. BMC Med Educ. 2020;20(1):1–17. doi:10.1186/s12909-020-02176-4
6. Interprofessional Education Collaborative Expert Panel. Core competencies for interprofessional collaborative practice: report of an expert panel. Interprofessional Education Collaborative Expert Panel; 2011.
7. Aziz Z, Teck LC, Yen PY. The attitudes of medical, nursing and pharmacy students to inter-professional learning. Procedia Soc Behav Sci. 2011;29:639–645. doi:10.1016/j.sbspro.2011.11.287
8. Keshtkaran Z, Sharif F, Rambod M. Students’ readiness for and perception of inter-professional learning: a cross-sectional study. Nurse Educ Today. 2014;34(6):991–998. doi:10.1016/j.nedt.2013.12.008
9. Hood K, Cant R, Baulch J, et al. Prior experience of interprofessional learning enhances undergraduate nursing and healthcare students’ professional identity and attitudes to teamwork. Nurse Educ Pract. 2014;14(2):117–122.
10. Wilhelmsson M, Ponzer S, Dahlgren L-O, Timpka T, Faresjö T. Are female students in general and nursing students more ready for teamwork and interprofessional collaboration in healthcare? BMC Med Educ. 2011;11(1):15. doi:10.1186/1472-6920-11-15
11. Reid R, Bruce D, Allstaff K, McLernon D. Validating the readiness for interprofessional learning scale (RIPLS) in the postgraduate context: are health care professionals ready for IPL? Med Educ. 2006;40(5):415–422. doi:10.1111/j.1365-2929.2006.02442.x
12. Visser CL, Wilschut JA, Isik U, van der Burgt SM, Croiset G, Kusurkar RA. The association of readiness for interprofessional Learning with empathy, motivation and professional identity development in medical students. BMC Med Educ. 2018;18(1):1–10. doi:10.1186/s12909-018-1248-5
13. Fisher D, King L. An integrative literature review on preparing nursing students through simulation to recognize and respond to the deteriorating patient. J Adv Nurs. 2013;69(11):2375–2388. doi:10.1111/jan.12174
14. McFadyen A, Webster V, Strachan K, Figgins E, Brown H, McKechnie J. The readiness for interprofessional learning scale: a possible more stable sub-scale model for the original version of RIPLS. J Interprof Care. 2005;19(6):595–603. doi:10.1080/13561820500430157
15. Villagrán I, Jeldez P, Calvo F, et al. Spanish version of the readiness for interprofessional learning scale (RIPLS) in an undergraduate health sciences student context. J Interprof Care. 2021;36(2):318–326.
16. Reime MH, Kvam FI, Johnsgaard T, Aarflot M. Comparison of peer assessment and faculty assessment in an interprofessional simulation-based team training program. Nurse Educ Pract. 2020;42:102666. doi:10.1016/j.nepr.2019.102666
17. Pallant J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using SPSS. McGraw-Hill International; 2010.
18. McFadyen A, Webster V, Maclaren WM, O’neill M. Interprofessional attitudes and perceptions: results from a longitudinal controlled trial of pre-registration health and social care students in Scotland. J Interprof Care. 2010;24(5):549–564. doi:10.3109/13561820903520369
19. Burford B, Greig P, Kelleher M, et al. Effects of a single interprofessional simulation session on medical and nursing students’ attitudes toward interprofessional learning and professional identity: a questionnaire study. BMC Med Educ. 2020;20(1):1–11. doi:10.1186/s12909-020-1971-6
20. Mahler C, Berger S, Reeves S. The readiness for interprofessional learning scale (RIPLS): a problematic evaluative scale for the interprofessional field. J Interprof Care. 2015;29(4):289–291. doi:10.3109/13561820.2015.1059652
21. Mahler C, Rochon J, Karstens S, Szecsenyi J, Hermann K. Internal consistency of the readiness for interprofessional learning scale in German health care students and professionals. BMC Med Educ. 2014;14(1):145. doi:10.1186/1472-6920-14-145
22. Schmitz CC, Brandt BF. The readiness for interprofessional learning scale: to RIPLS or not to RIPLS? That is only part of the question. J Interprof Care. 2015;29(6):525–526. doi:10.3109/13561820.2015.1108719
23. Ataollahi M, Amini M, Delavari S, Bazrafkan L. Reliability and validity of the Persian version of readiness for inter-professional learning scale. Int J Med Educ. 2019;10:203. doi:10.5116/ijme.5da4.37c2
24. Lauffs M, Ponzer S, Saboonchi F, Lonka K, Hylin U, Mattiasson AC. Cross cultural adaptation of the Swedish version of readiness for interprofessional learning scale (RIPLS). Med Educ. 2008;42(4):405–411. doi:10.1111/j.1365-2923.2008.03017.x
25. Ergonul E, Baskurt F, Yilmaz ND, et al. Reliability and validity of the readiness for interprofessional learning scale (RIPLS) in Turkish speaking health care students. Acta Med Mediterr. 2018;34(3):797–803.
26. Li Z, Sun Y, Zhang Y. Adaptation and reliability of the readiness for inter professional learning scale (RIPLS) in the Chinese health care students setting. BMC Med Educ. 2018;18(1):1–6. doi:10.1186/s12909-018-1423-8
27. DeVellis RF. Scale Development: Theory and Applications. Sage Publications: Vol. 26; 2011.
28. Miller A, Morton S, Sloan P, Hashim Z. Can a single brief intervention improve participants’ readiness for interprofessional learning? J Interprof Care. 2013;27(6):532–533. doi:10.3109/13561820.2013.805736
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimizing Interprofessional Simulation with Intentional Pre-Briefing and Debriefing
Penn J, Voyce C, Nadeau JW, Crocker AF, Ramirez MN, Smith SN
Advances in Medical Education and Practice 2023, 14:1273-1277
Published Date: 10 November 2023