")
Back to Journals » International Journal of General Medicine » Volume 16
Does Biological Sex Matter in Lyme Disease? The Need for Sex-Disaggregated Data in Persistent Illness
Authors Johnson L, Shapiro M, Janicki S, Mankoff J, Stricker RB
Received 14 February 2023
Accepted for publication 6 June 2023
Published 17 June 2023 Volume 2023:16 Pages 2557—2571
DOI https://doi.org/10.2147/IJGM.S406466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lorraine Johnson,1 Mira Shapiro,2 Sylvia Janicki,3 Jennifer Mankoff,4 Raphael B Stricker5
1MyLymeData, San Ramon, CA, USA; 2Analytic Designers LLC, Bethesda, MD, USA; 3School of Literature, Media and Communications, Georgia Institute of Technology, Atlanta, GA, USA; 4Paul G. Allen School of Computer Science and Engineering, University of Washington, Seattle, WA, USA; 5Union Square Medical Associates, San Francisco, CA, USA
Correspondence: Raphael B Stricker, Tel +1-415-399-1035, Fax +1-415-399-1057, Email [email protected]
Background: Biological sex should be included as an important variable in clinical research studies to identify outcome differences between men and women. Very few Lyme disease studies were designed to consider sex-based differences or gender bias as an important component of the research design.
Methods: To assess sex-based differences in Lyme disease patients who were clinically diagnosed and reported remaining ill for six or more months after receiving antibiotic treatment, we analyzed self-reported clinical data from 2170 patients in the MyLymeData patient registry. We also reviewed previous Lyme disease studies for distribution of patients by biological sex according to stage of illness, data source, and definition of disease used as enrollment criteria.
Results: In MyLymeData, women reported more tick-borne coinfections, worse symptoms, longer diagnostic delays, more misdiagnoses, and worse functional impairment than men. No differences were reported in antibiotic treatment response or side effects. In our review, of clinical research trials and data sources, we identified a smaller percentage of women in studies of acute Lyme disease and a larger percentage of women in studies of persistent illness. Samples and data sources that were more reflective of patients seen in clinical practice had a higher percentage of women than randomized controlled trials and post-treatment Lyme disease studies.
Conclusion: Our results indicate that biological sex should be integrated into Lyme disease research as a distinct variable. Future Lyme disease studies should include sex-based disaggregated data to illuminate differences that may exist between men and women with persistent illness.
Keywords: post-treatment lyme disease, chronic lyme disease, MyLymeData, Borrelia burgdorferi, tick-borne disease, gender bias, sex-based differences
Introduction
An implicit and inaccurate assumption underlying most medical research is that aside from reproductive matters, men and women do not differ substantially in their physiological and pathological response to disease.1 Most research was primarily conducted on men until 2015 when the National Institutes of Health (NIH) began requiring that sex be included as a biological variable factored into research designs and reported in both animal and human studies.2 Consideration of sex is now seen as critical to the interpretation, validation, and generalizability of research findings. However, in the case of Lyme disease, only a handful of papers have meaningfully analyzed differences linked to sex.3
In the USA, Lyme disease, which is caused by the spirochete Borrelia burgdorferi, is transmitted by the black-legged ticks—Ixodes scapularis and Ixodes pacificus. The Centers for Disease Control and Prevention (CDC) estimates that 476,000 new Lyme disease cases occur annually in the USA.4,5 If diagnosed and treated promptly, most patients recover without complications.6 However, even patients who are diagnosed early can remain ill after antibiotic treatment.6 In a recent study, 43% of patients reported persisting symptoms six months or more after early treatment with 14% reporting functional impairment, and only 57% of patients were classified as having recovered from their illness.6 Many patients are not diagnosed and treated early for Lyme disease, which further increases their risk of remaining ill after initial antibiotic treatment.7,8
Clinical studies of patients with persisting Lyme disease symptoms following antibiotic treatment have used different research definitions to enroll patients. A number of NIH-funded studies have used the randomized controlled trial (RCT) design with stringent study entry criteria that excluded 89–99% of patients who sought to enroll.9–12 In 2006, the Infectious Diseases Society of America (IDSA) proposed standardized research criteria based on the CDC surveillance case definition called post-treatment Lyme disease syndrome (PTLDS).13 More recently the name of this clinical category has been simplified to post-treatment Lyme disease (PTLD). Enrollment criteria based on the NIH RCT and IDSA PTLD definitions select for a small subgroup of patients who are clinically diagnosed with persisting illness following Lyme disease diagnosis and treatment.6,8 These restrictive research definitions are collectively referred to in this study as RCT/PTLD.
Unlike RCT/PTLD studies, physician cohort studies depend more on clinical case definitions and use less restrictive inclusion criteria that encompass patients typically seen in clinical practice.14–16 The current analysis focuses on patients who remain ill six or more months after antibiotic treatment, and we refer to these patients as having persistent or chronic Lyme disease (PLD/CLD). This definition conforms more closely with the definitions used by clinicians and represents real world data that is more generalizable to patients seen in clinical practice.
Despite males having a slight predominance in acute Lyme disease (ALD) studies, PLD/CLD appears to be more common among women than men in the clinical treatment trial literature.3,17–19 However, aside from specifying the relative proportion of men and women enrolled, these clinical treatment trials do not offer significant insights into differences between men and women because none of the NIH trials and very few of the other clinical studies conducted to date were designed to consider sex differences or gender bias as an important component in their research design.9,11,12,15,16
To address the lack of information about sex differences and gender bias in PLD/CLD patients, we present an analysis of data from the MyLymeData registry, which includes over 2000 patients with PLD/CLD. The goal of this project is to describe sex-based differences in PLD/CLD related to symptom severity, diagnostic delays, misdiagnosis and functional impairment, as well as treatment response and side effects. We also examine variations in the percentage of women included in clinical studies based on stage of disease and research definitions employed in the studies. To our knowledge, this is the first PLD/CLD study using a large sample that includes sex-based differences as an integral part of the research design.
Materials and Methods
Data Sources
The MyLymeData patient registry was launched in 2015. Participants were recruited through blogs, social media, emails, outreach to clinicians, and professional conferences. Since its launch, the registry has enrolled over 17,000 patients, aggregated an extensive survey response database, and published four peer-reviewed studies.10,20–22 Data used in this study were obtained from the LymeDisease.org patient registry, MyLymeData, Data set dated April 27, 2017. Permission was obtained from the dataset owner LymeDisease.org to access and use the data in the current study.
The registry records comprehensive responses of participants’ illness experiences, including symptoms, diagnostic testing, functional impairment, treatment response and side effects. Survey items reflect recommendations from the Agency for Healthcare Research and Quality (AHRQ), and include government survey items derived from the National Health Interview Survey (NHIS), the CDC Behavioral Risk Factor Surveillance System (BRFSS), the Centers for Diseases Control (CDC) Healthy Days Measures, and peer review literature for Lyme disease.23 A beta version of the MyLymeData survey was pilot-tested and adjusted to increase accuracy.
Patient data contributed to the registry are self-reported, de-identified and held confidential. The MyLymeData patient registry uses the same technology and platform that serves NIH patient registries. The registry received ethical approval from the Advarra independent review board and all patients were fully consented and agreed to allow their de-identified data to be used for any and all research projects approved by LymeDisease.org. The analysis of the anonymous survey data for this study was exempted from review by the University of Washington Human Subjects Division Review Board because it did not meet the definition of direct human subject research.
Study Participants
Patients included in this study were United States residents who reported being diagnosed with Lyme disease by a physician and remaining ill for at least six months after antibiotic treatment thereby satisfying the definition for PLD/CLD. Figure 1 shows the original sample of 4719 respondents and the inclusion/exclusion criteria that resulted in a final sample of 2170 PLD/CLD patients, comprised of 1839 women and 331 men.
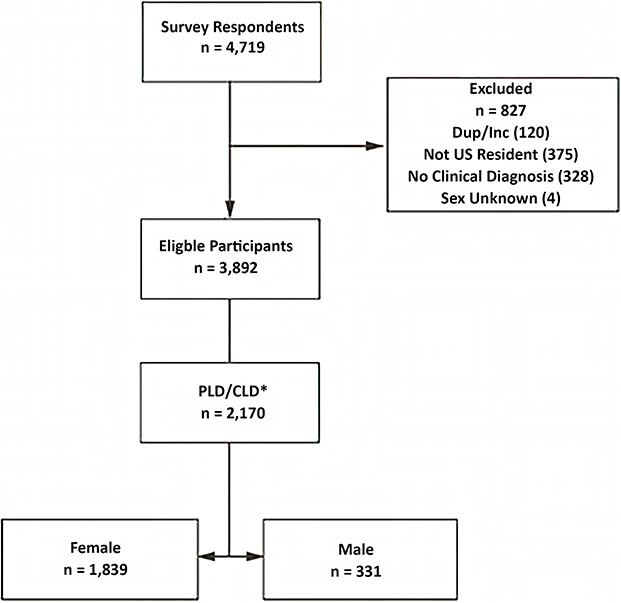 |
Figure 1 Inclusion and exclusion criteria for the MyLymeData study. |
Although a more nuanced approach is sometimes appropriate, the sample in this study was limited to those who defined their biological sex as male or female. Respondents were asked to specify their biological sex as “male, female or other”. Four respondents who identified their sex as “other” were excluded from the sample.
Table 1 shows the demographic characteristics of the sample used in the study, which was predominantly female (85%) with an average age of 49 years. The sample also positively skewed towards higher education and income levels than the general population. These demographics conform with other studies of patients with PLD/CLD.10,14,15,24
 |
Table 1 Demographic Characteristics of Respondents |
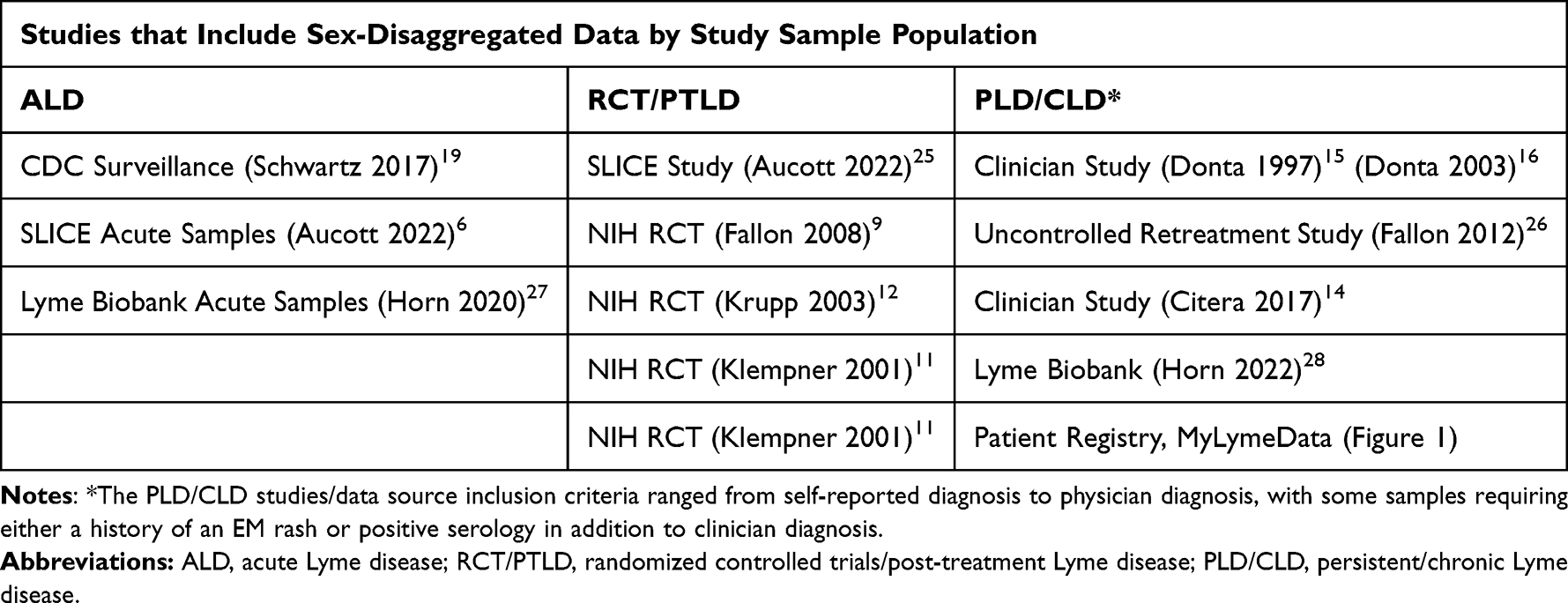 |
Table 2 Data Sources for ALD, RCT/PTLD, and PLD/CLD That Include Sex-Disaggregated Data |
Methodology Overview
The aim of this study using data from the MyLymeData patient registry was to determine whether men and women with PLD/CLD differ significantly with respect to symptom severity, diagnostic delays, misdiagnosis, functional impairment and antibiotic response. Each characteristic of interest was categorized dichotomously as either present or absent or by magnitude using 0/1 coding as more fully described in the findings. For example, the severity of each symptom reported (none or mild, 0, vs moderate to very severe, 1) was analyzed to determine whether men and women reported similar symptom severity.
Due to the fact that our sample is predominantly female, we compare the sex-specific proportions in our analysis. Because the variables of interest are categorical in nature and there are substantially more women than men, we tested for statistical significance using the Fisher’s Exact Test, which is nonparametric and therefore requires no underlying distribution assumptions. The assumption of fixed row and column totals required for Fisher’s Exact Test is met with our analysis.
The null hypothesis under consideration for our study was that men and women do not differ for the attribute under review. An alpha threshold of 0.05 was used to determine statistical significance. In most of the cases where statistical significance was demonstrated, the observed p-value was much less than this threshold. All analyses were performed using SAS® JMP® 16.0.
We also compare the percentage of women included in US studies based on whether their Lyme disease was acute or persistent, and whether the data sample was clinically oriented (eg, PLD/CLD) or reflected a more restrictive research focus (eg, RCT/PTLD). Data sources were chosen that contained disaggregated data on the proportion of men and women in the sample or outcome and were characteristic of the category at issue (eg CDC surveillance data and acute disease). The sources include both traditional research samples (eg randomized control trials) and real world data.
Two stages of disease were evaluated: patients with ALD and patients whose symptoms persisted for six or more months after treatment. Data sources involving patients who remained ill for six months or more following antibiotic treatment were further divided into studies/sources that used restrictive RCT/PTLD eligibility criteria (eg randomized controlled trials or PTLD studies) and physician cohort studies that used less restrictive inclusion criteria and encompass patients typically seen in clinical practice.14–16 Table 2 lists the data sources for ALD, RCT/PTLD and PLD/CLD.
Results
Our study used data from the MyLymeData patient registry to explore the sex-based differences in PLD/CLD patients for the following attributes:
- Diagnosis, diagnostic delays, and misdiagnosis
- Symptom severity
- Functional impairment and activity limitations
- Antibiotic response and side effects
- Distribution of women in research samples and data sets
These categories provide a framework to evaluate the differences between men and women with PLD/CLD.
Diagnosis, Diagnostic Delays, and Misdiagnosis
Table 3 shows the diagnostic and clinical characteristics of the sample broken down by biological sex, including recollection of a rash, existence of positive laboratory tests, diagnostic delays and presence of tick-borne coinfections (Babesia, Anaplasma, Ehrlichia, Bartonella, Rickettsia, Mycoplasma and Tularemia) as previously described.21 There was no statistically significant difference between the sexes on either rash rates or positive laboratory tests, although six percent more men reported a rash than women. The rate of tick-borne coinfections for men was 75% compared to 81% for women (p=0.020).
 |
Table 3 Clinical and Diagnostic Characteristics of MyLyme Data Sample |
Diagnostic delays were common. Nearly three-quarters of those included in our sample reported that they were not diagnosed until six or more months following symptom onset, more than half reported diagnostic delays of 3 or more years, and about a third visited 10 or more clinicians before receiving a Lyme disease diagnosis. Women were more likely to have been diagnosed at late stage (83% versus 76%, p=0.0019), to have waited three or more years from symptom onset to diagnosis (57% versus 49%, p=0.0036), and to have seen 10 or more physicians before being diagnosed (36% versus 25%, p=<0.001). There was no statistically significant difference between women and men who were diagnosed within one month when treatments are more likely to be effective, but very few participants in our sample (<10%) were diagnosed this early.
As Table 4 describes, 79% of participants reported being initially misdiagnosed with another condition and 76% reported specifically being misdiagnosed with myalgic encephalomyelitis/chronic fatigue syndrome (CFS) (46%), fibromyalgia (FMS) (47%), and/or a psychiatric illness (55%). Women were more likely than men to report being misdiagnosed initially (80% versus 71%, p=0.0006) and to have been misdiagnosed with CFS (48% versus 39%, p=0.0081), FMS (50% versus 26%, p=<0.0001) or with a psychiatric condition (56% versus 46%, p=0.0024).
 |
Table 4 Misdiagnosis |
Symptom Severity
Participants were asked about the severity of each of twelve common symptoms of Lyme disease (fatigue, muscle aches, joint pain, sleep impairment, neuropathy, cognitive impairment, memory loss, psychiatric symptoms, gastrointestinal distress, headache, twitching, and heart-related conditions). Patient responses were categorized as a binary variable (none/mild versus moderate/severe/very severe). Men and women were compared for symptoms rated moderate to very severe. These results are illustrated in Figure 2.
 |
Figure 2 Symptom severity in men versus women. Upper bars: women; Lower bars: men. Women reported greater symptom severity that was statistically significant for six symptoms: fatigue (p=0.0210), muscle aches (p=0.00006), joint pain (p=0.0001), sleep impairment (p=0.0108), gastrointestinal complaints (p=0.0202) and headache (p=0.0007). |
Women reported greater symptom severity for all but twitching, cognitive impairment, and heart-related conditions. Results were statistically significant for six of these symptoms: fatigue (85% versus 80%, p=0.0210), muscle aches (73% versus 64%, p=0.00006), joint pain (71% versus 60%, p=0.0001), sleep impairment (68% versus 61%, p=0.0108), gastrointestinal complaints (52% versus 46%, p=0.0202), and headache (49% versus 39%, p=0.0007). The percentage of women experiencing more severe symptoms for neuropathy, memory loss, and psychiatric illness was higher than for men, while a higher percentage of men reported more severe twitching, cognitive impairment, and heart-related conditions. However, these differences were not statistically significant.
Functional Impairment and Activity Limitations
In Table 5, we describe the degree of functional impairment of participants using survey items pertaining to self-rated health status, bed days, and use of special equipment (for example a cane or special bed). These questions were derived from government questionnaires (eg NHIS, the CDC Healthy Days Measures, and the BRFSS) and extensive population-level data exists on these measures. We also assessed disability status in a question asking participant to identify their primary form of work.
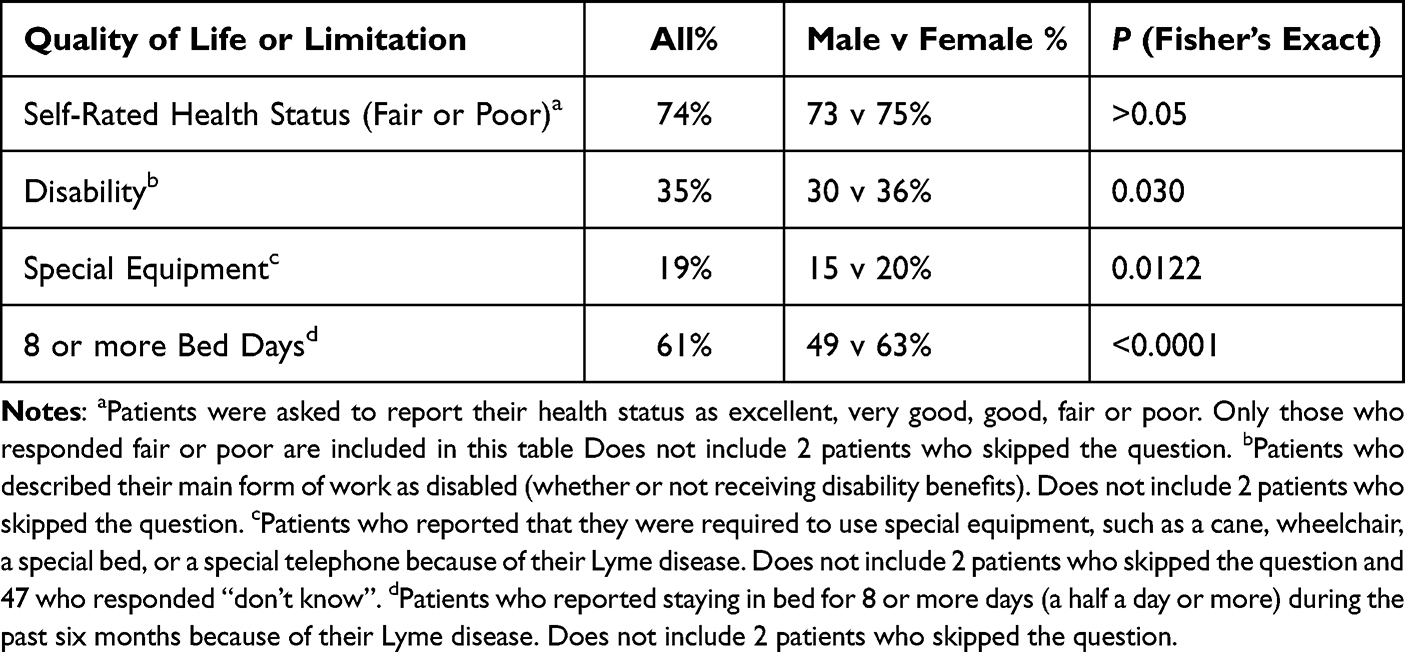 |
Table 5 Quality of Life Impairment, Activity Limitations and Functional Impairment |
The number of bed days reported in our study greatly exceeds those reported for the general population. More specifically, only 8% of the general population report 8 or more bed days annually, while 61% of our PLD/CLD population report 8 or more bed days over a six-month period.29
Similarly, the percentage of participants who report having to rely on special equipment due to their Lyme disease is quite high (> 19%) compared to the US general population (11%).29 Three-quarters of participants reported fair/poor self-rated health status compared to 15% of the general population and 33% of patients with fibromyalgia.30,31
Self-rated health status is the first question in the SF-36 instrument and is considered to be a highly prognostic single question method to predict mortality and healthcare utilization.32 This single question item was also used in the Krupp NIH-funded Lyme disease retreatment study.12 Men and women did not differ substantially in their reported rates of fair/poor self-rated health status. However, in all other cases, women fared worse than men on a statistically significant basis. Women were more likely to report that as a result of their Lyme disease, they were disabled (36% versus 30%, p=0.030); required to use special equipment (20% versus 15%, p=0.0122) or had to spend more time in bed over the last six months (63% versus 49%, p=<0.0001).
Antibiotic Treatment Response and Side Effects
We assessed treatment effectiveness using two questions: One focused on the effectiveness for the patient’s current antibiotic treatment, while the other focused on effectiveness of treatment over time since antibiotics were first initiated. Nearly half (45%) of those respondents on antibiotics reported that their current antibiotic treatment was moderately to very effective and more than half (57%) reported improvement over time from antibiotics since initiation.
The existence of side effects was assessed with two questions. The first question pertained to side effects associated with current treatment, while the second assessed whether patients who were not taking antibiotics did not do so because of side effects. Approximately 8% reported troubling side effects associated with their current antibiotic. Twenty-percent of those who reported not taking antibiotics did not do so because of side effects. No significant differences between the sexes was observed in treatment effectiveness or side effects associated with treatment.
Distribution of Women in Research Samples and Data Sets
Figure 3 illustrates the percentage of women included in US studies categorized based on whether the stage of disease was acute or persistent and whether the data sample was more clinically oriented (PLD/CLD) or reflected the more restrictive research enrollment criteria of RCT/PTLD studies. Research definitions used in any single study vary, but, in general samples included in PLD/CLD studies are more heterogenous than samples of RCT/PTLD because sample inclusion criteria are less restrictive. As shown in Figure 3, there is substantial variation in the percentage of women included in research and data samples associated with different disease stages and research designs. ALD studies enrolled the lowest percentage of women (mean 42%, range 37–47%); RCT/PTLD studies enrolled a greater percentage of women (mean 58%, range 44–72%), and PLD/CLD samples, which used broader enrollment criteria, included the highest percentage of women (mean 77%, range 66–88%).
 |
Figure 3 Average percentage of women by study and disease category. *Horn 1= EM rash; Horn 2 = Symptoms & diagnosis (no rash); Klempner 1= Seronegative w EM rash; Kempner 2 = Seropositive; Citera 1= Clinician diagnosed; Citera 2 = Internet survey; Citera 3 = Clinician diagnosed AND validated EM rash OR + lab test). **Personal communications with authors 2022. See data sources in Table 2 for references. Abbreviations: RCT/PTLD, Randomized controlled trial/post-treatment Lyme disease; PLD/CLD, Persistent Lyme disease/chronic Lyme disease. |
Discussion
As recently recognized by the NIH, basic and medical research should include biological sex as one of the variables in study design.2 Biological sex has been shown to influence susceptibility to infection, pathophysiology, immune responses, clinical presentation, disease severity, and response to treatment.33 Biological sex can directly impact initial response to pathogens as well as the course of disease progression through different genetic pathways (including the role of X and Y chromosomes), anatomic niches, immunological profiles, and hormonal environments.34
In our study, women more often reported tick-borne coinfections, diagnostic delays, misdiagnosis, greater symptom severity, and functional impairment (Tables 3–5). No significant difference in treatment effectiveness or side effects was seen. Our sample consists of patients with PLD/CLD and is predominantly female.
Looking across different studies and data sources in Lyme disease, we also noted a smaller percentage of women enrolled in ALD studies compared to studies of persistent illness, coupled with a greater percentage of women enrolled in more clinically-oriented studies compared to those using restrictive research definitions common in RCTs and PTLD (Figure 3).
Diagnosis, Diagnostic Delays, and Misdiagnosis
Until recently, most research was conducted primarily on men and our current medical knowledge is based on a male-centric research perspective used to diagnose and treat patients. Over the last decade, it has become increasingly clear that women are more likely than men to experience diagnostic delays or misdiagnosis for a wide range of conditions.35
Sometimes misdiagnosis occurs because men and women have distinct biological systems and women fall outside the established symptoms, physical findings or diagnostic laboratory reference values that were based on male-centric research.36 Women are also misdiagnosed or treated differently than men based on gender bias, which is largely a societal construct.36 For example, women with acute myocardial infarction are more likely than men to have their symptoms characterized as “atypical”, receive less thorough evaluations and fewer medical interventions, have lower hospital admission rates and suffer poorer outcomes.36,37 They are also twice as likely to have cardiac symptoms misdiagnosed as a mental illness.38
In Lyme disease, research has suggested that sex-based biological differences may occur with rash presentation and test positivity rates used to diagnose the disease. One recent study found that in Lyme disease men have larger rashes than women, with male rashes averaging 2.18 cm larger than female rashes.39 Similarly, some research suggests that commercial Lyme disease testing favors men over women, with men having more positive ELISA tests and Western blots.3,17,33,40,41 CDC surveillance test requirements that specify five positive bands on a Lyme Western blot and require that rashes equal or exceed 5 cm in diameter potentially underestimate female cases.33 Thus clinicians who follow the CDC surveillance definition for diagnosis may misdiagnose more women than men.
In our study, a larger percentage of men (51%) than women (44%) recollected an EM rash, although this result was not statistically significant. We also did not find a significant difference between men and women in positive laboratory test rates. However, our survey question asked patients whether they had received “any” positive test result and answers may reflect multiple laboratory tests. Our sample’s high rate of positive laboratory tests (82%) suggests this possibility. As a result, our data cannot tell us whether women needed more tests than men before testing positive, or whether laboratory tests are more sensitive in men than in women, as the literature suggests.
Gender bias appears to be important in Lyme disease. In our study, women were more likely than men to experience diagnostic delays and/or to be misdiagnosed with FMS, CFS, and/or a psychiatric illness (Table 4). Lyme disease is frequently confused with other female-dominated conditions such as CFS, FMS, and psychiatric illness.42,43 Although some symptoms of these conditions overlap, the pattern of symptoms in PLD/CLD differs from that seen in FMS, CFS and depression.44
Unlike Lyme disease, FMS and CFS have unknown etiologies, no diagnostic testing, and no curative treatments. They are diagnosed by ruling out similar illnesses.42,45 The high risk of misdiagnosis, 82% positive laboratory test rate, and 45% rash rate seen in our study suggest that Lyme disease is not being eliminated as a potential cause before CFS or FMS are diagnosed. Similar issues may be at play in the misdiagnosis of Lyme disease as a psychiatric illness, because neuropsychiatric symptoms are common in Lyme disease.3 The IDSA PTLD enrollment criteria specifically exclude from research samples anyone who was diagnosed with FMS or CFS “before the onset of Lyme disease”.13 As our study indicates, it is important to identify patients initially misdiagnosed with CFS, FMS, or psychiatric disorder after the onset of Lyme disease symptoms and ensure that they are not inappropriately excluded from research studies.
Since misdiagnosis and diagnostic delays postpone treatment of the underlying illness, the biases documented in our study may increase the development of PLD/CLD in women disproportionately.
Symptom Severity
Some PLD/CLD symptoms are common in the general population; however, recent studies have found that patients with PLD/CLD experience these symptoms more frequently and with greater severity.6,8,46,47 A recent study by Aucott discovered that, even with early diagnosis and treatment, women are four times more likely than men to meet the research criteria for PTLD.6 Our analysis lends support to these findings. Women had more severe symptoms than men for all but three of the twelve symptoms, six of which were statistically significant. A study of 235 patients with EM rash or positive Lyme serology identified no sex-based variations in PLD/CLD symptoms.24 However, the study’s male sample was small (40 men vs 123 men in the Aucott study and 331 men in our study). Small sample size is known to increase the risk of reporting false-negative findings.48
The reason women have worse symptoms is unknown, but may be related to sex-based differences in cytokine response to Lyme disease infection.49 Emerging research on the role of cytokines in chronic pain and fatigue that focuses on the immune system interaction with the peripheral and central nervous systems may help us learn more in this area.50
Functional Impairment and Activity Limitations
The proportion of subjects in our sample who reported functional impairment substantially exceeded those in the general population. Significantly more patients reported fair/poor self-rated health than either the general population or patients diagnosed with FMS. The functional impairment reported here is consistent with the findings of other researchers that patients with PLD/CLD may suffer a degree of disability equivalent to that of patients with congestive heart failure.11
With the exception of self-rated health status, women reported more limitations than men on all other measures, including bed days, disability, and the need to use special equipment (Table 5). This may reflect the greater symptom severity experienced by women (Figure 2).
Although self-rated health status, bed days, and equipment limitations are included in major government population health surveys, they are not widely used to assess functional limitations in Lyme disease. The fact that responses to all of these questions substantially exceeded the rates reported in the general population, however, suggests that these highly validated and widely used single-item survey measures should be used more broadly in Lyme disease research.
Antibiotic Treatment Response and Side Effects
The high antibiotic treatment response rate in this study is noteworthy, with nearly half of the sample indicating that their current medication was moderately to very effective and more than half (57%) reporting some improvement with antibiotic treatment over time. This conforms with our previous study using the broadly used and highly validated Global Rating of Change (GROC) scale with a separate MyLymeData sample. In that study 52% reported some improvement and 34% reported improving moderately to a very great deal.10
Our findings are also in line with the 64% level of fatigue improvement reported in the Krupp et al study.12 The Fallon et al study results also suggest that for a subgroup of patients with more severe impairment in pain or physical functioning, a course of repeated IV antibiotic therapy can result in sustained long-term benefit.9,26 Although these studies used different outcome measures and entry criteria, it is important that the real world evidence of our studies support the results of these two NIH funded RCTs. The concordance of these studies underscores the effectiveness of antibiotic treatment approaches for some patients with PLD/CLD in clinical practice. The risk/benefit trade-off of any treatment approach should be considered in the individualized context of shared medical decision making.
It is well known that sex-based differences may affect treatment outcomes and adverse events in men and women.34,51 However, in our sample, no significant differences between men and women were observed in reported effectiveness or side effects from antibiotic treatment. Donta’s two clinical trials comparing male vs female antibiotic response yielded mixed results.15,16 Our investigation focused on any antibiotic treatment as opposed to individual antibiotics, and a study of individual antibiotics may provide different results.
Distribution of Women in Research Samples and Data Sets
A greater percentage of men than women are represented in CDC surveillance data.19 In contrast, results from a variety of studies show that women are more likely than men to develop PLD/CLD or PTLD after antibiotic treatment for Lyme disease.3,18 In other diseases, men and women vary in their biological response to infectious diseases.34,52 Different bacterial pathogens exhibit a sex preference in acute infection, with most showing a male bias.33 In some infectious disorders, women have a heightened antiviral, inflammatory, and cellular immune response, which is crucial for pathogen clearance but may produce more severe symptoms and symptoms that persist longer in women than in men following acute infection.34 Both HIV/AIDS and COVID exhibit this tendency.34,52 In one COVID study, 69% of participants developed long COVID. Despite making up only 36% of total patients in that study, 82% of women developed long COVID.53 In Lyme disease, women may produce more inflammatory and inhibitory cytokines than men in response to Borrelia infection, increasing the risk of PLD/CLD.49
Instances where data from both acute and persistent illness samples are available from a single data source may provide the best insights into the distribution of women in research studies or data sets. In one longitudinal investigation, the female population was 47% in ALD, but 72% in PTLD.6,25 This significant disparity in gender representation suggests that biological factors may play a role, given that strict research definitions were used for both ALD admission requirements and PTLD outcome characterization.6 The Lyme Biobank samples also include more women in their PLD/CLD samples than in their ALD samples (37–41% ALD vs 88% PLD/CLD).27,28 A major insurance claims analysis reported a relatively even proportion of males (49%) and females (51%) in the ALD sample, but substantially more females (68%) than males (58%) with PTLD-related diagnosis defined by fatigue, musculoskeletal symptoms, peripheral neuropathy, arthropathy, and other non-specific signs or symptoms.46
Strengths and Limitations
The strengths and limitations of this study in large measure reflect the factors inherent in observational trials and the use of single point-in-time self-reported data from patient registries where samples are self-selected. A strength of patient registries is that they are more generalizable than RCTs because they have fewer inclusion and exclusion criteria and reflect real-world behavior and practices.54 Even though observational research cannot prove cause and effect or supplant rigorous RCTs, leveraging data generated by patient registries can play a critical role in developing the evidence base that informs decisions made by patients, providers, and policy makers to improve patient outcomes.55
The sample used here does not represent the full spectrum of disease in Lyme patients because the registry primarily attracts patients with PLD/CLD. These patients may be more likely to develop PLD/CLD as a result of diagnostic delays, may be more severely ill and may experience greater functional impairment. However, this sample is clinically appropriate for the analysis conducted here on PLD/CLD. A systematic literature review of all ALD, PLD/CLD, and PTLDS studies is beyond the scope of this paper. Hence, the studies and data sources delineated in Table 2 are not intended to be exhaustive, but rather to exemplify sex-based differences between the different data sources generally.
It has been observed that women have a greater willingness to engage in internet surveys.56 A recent study analyzed the proportion of males and females that participated in symptom tracker studies for eight different diseases and concluded that participation rates also depend on sex-based disease prevalence.57
There was no outside physician diagnostic confirmation of patient reported data in the registry. However, self-reported information may improve the accuracy of patient data and has been found to have acceptable levels of reliability when compared to medical chart information.58 Most government population-based surveys, such as the BRFSS and NHIS, rely on self-reported data, as do many clinical trial outcome measures, including the SF-36 used in NIH-funded PLD/CLD trials.
Finally, our data did not include a sufficient sample of people across races or who identify across the gender spectrum.
Conclusion
Few Lyme disease studies have reported or analyzed sex on a disaggregated basis. In this study, we found:
- Women had higher rates of coinfections.
- Women had longer diagnostic delays, saw more doctors before receiving a diagnosis, and were diagnosed at a later stage of illness than male patients. They were also more likely to be misdiagnosed in general, and were more likely to be misdiagnosed with CFS, FMS, or a psychiatric disorder in particular (or any combination of these conditions).
- Women had more severe symptoms and were more likely than men to report being disabled, spending more days in bed, and requiring special equipment as a result of their PLD/CLD. Self-reported health status was equally impaired for men and women.
- There was no statistically significant difference between men and women in treatment response and side effects from antibiotic treatment, with the majority of both men and women reporting some improvement in symptoms since the beginning of their antibiotic treatment.
- A smaller proportion of women are included in ALD samples, while a larger proportion are included in samples for persisting illness. Clinically-oriented PLD/CLD samples had a higher proportion of women than samples from RCT/PTLD studies using more restrictive inclusion/exclusion criteria.
The substantial variation in the proportion of women included in data for ALD compared to RCT/PTLD or PLD/CLD data sources indicate that there is a compelling need for use of sex-disaggregated sample inclusion data as well as outcome data in future studies to increase our knowledge of the role of sex-based differences in Lyme disease. The greater rates of diagnostic delays and misdiagnosis in women illustrated here likely play a large role in the fact that more women than men develop PLD/CLD. The extent to which biological factors also contribute to the greater prevalence of PLD/CLD in women should be a central focus of future research.
Abbreviations
AHRQ, Agency for Healthcare Research and Quality; BRFSS, Behavioral Risk Factor Surveillance System; CDC, Centers for Disease Control and Prevention; IDSA, Infectious Diseases Society of America; NIH, National Institute of Health; PLD/CLD, Persistent or chronic Lyme disease; PTLD, Post-treatment Lyme Disease; SRHS, Self-Rated Health Status; SF-36, 36-Item Short Form Survey.
Data Sharing Statement
Data used in the preparation of this article were obtained from the LymeDisease.org patient registry, MyLymeData, Phase 1 April 27, 2017. The data and supporting calculations in this study are available from the corresponding author upon request.
Acknowledgments
The authors wish to thank the patients participating in MyLymeData, who have the power to accelerate Lyme disease research and without whom this research would not have been possible. We also thank Christine Green, Erica Lehman, Dorothy Leland, and Phyllis Mervine for their thoughtful comments and research insights.
Author Contributions
Conceptualization, L.J.; Data curation, M.S.; Formal analysis, M.S., R.B.S., S.J., and J.M.; Investigation, L.J. and R.B.S.; Methodology, L.J. and M.S.; Supervision, J.M.; Writing—original draft, S.J., L.J., J.M. and M.S.; Writing—review & editing, L.J., M.S., R.B.S., J.M., and S.J. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work”.
Funding
Funding for this work was provided in part by grants from the Bill and Marion Cook Foundation, the Bruce Lindorf Memorial Foundation and the Peterson Family Foundation, Orem, UT. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Ms Lorraine Johnson reports general funding support for the MyLymeData patient registry project from Bruce Lindorf Memorial Foundation, during the conduct of the study. The authors declare no other conflict of interest.
References
1. Blair ML. Sex-based differences in physiology: what should we teach in the medical curriculum? Adv Physiol Educ. 2007;31:23–25. doi:10.1152/advan.00118.2006
2. Arnegard ME, Whitten LA, Hunter C, Clayton JA. Sex as a biological variable: a 5-year progress report and call to action. J Womens Health. 2020;29:858–864. doi:10.1089/jwh.2019.8247
3. Rebman A, Soloski M, Aucott J. Sex and Gender Impact Lyme Disease Immunopathology, Diagnosis and Treatment. In: Klein S, Roberts C, editors. Sex and Gender Differences in Infection and Treatments for Infectious Diseases. Switzerland: Springer International Publishing; 2015. doi:10.1007/978-3-319-16438-0_12.
4. Kugeler KJ, Schwartz AM, Delorey MJ, Mead PS, Hinckley AF. Estimating the frequency of lyme disease diagnoses, United States, 2010–2018. Emerg Infect Dis. 2021;27:616–619. doi:10.3201/eid2702.202731
5. Schwartz AM, Kugeler KJ, Nelson CA, Marx GE, Hinckley AF. Use of commercial claims data for evaluating trends in lyme disease diagnoses, United States, 2010–2018. Emerg Infect Dis. 2021;27:499–507. doi:10.3201/eid2702.202728
6. Aucott JN, Yang T, Yoon I, Powell D, Geller SA, Rebman AW. Risk of post-treatment Lyme disease in patients with ideally-treated early Lyme disease: a prospective cohort study. InterJ Infect Dis. 2022;116:230–237. doi:10.1016/j.ijid.2022.01.033
7. Hirsch AG, Poulsen MN, Nordberg C, et al. Risk factors and outcomes of treatment delays in lyme disease: a population-based retrospective cohort study. Front Med. 2020;7. doi:10.3389/fmed.2020.560018
8. Rebman AW, Bechtold KT, Yang T, et al. The clinical, symptom, and quality-of-life characterization of a well-defined group of patients with posttreatment lyme disease syndrome. Front Med. 2017;4. doi:10.3389/fmed.2017.00224
9. Fallon BA, Keilp JG, Corbera KM, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology. 2008;70:992–1003. doi:10.1212/01.WNL.0000284604.61160.2d
10. Johnson L, Shapiro M, Mankoff J. Removing the mask of average treatment effects in chronic Lyme disease research using Big Data and subgroup analysis. Healthcare. 2018;6. doi:10.3390/healthcare6040124
11. Klempner M, Hu L, Evans J, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001;345:85–92. doi:10.1056/NEJM200107123450202
12. Krupp LB, Hyman LG, Grimson R, et al. Study and treatment of post Lyme disease (STOP-LD): a randomized double masked clinical trial. Neurology. 2003;60:1923–1930. doi:10.1212/01.WNL.0000071227.23769.9E
13. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1089–1134. doi:10.1086/508667
14. Citera M, Freeman PR, Horowitz RI. Empirical validation of the Horowitz multiple systemic infectious disease syndrome questionnaire for suspected lyme disease. Int J Gen Med. 2017;10:249–273. doi:10.2147/IJGM.S140224
15. Donta ST. Tetracycline therapy for chronic Lyme disease. Clin Infect Dis. 1997;25(1):S52–56. doi:10.1086/516171
16. Donta ST. Macrolide therapy of chronic Lyme Disease. Med Sci Monit. 2003;9:I136–142.
17. Rebman AW, Crowder LA, Kirkpatrick A, Aucott JN. Characteristics of seroconversion and implications for diagnosis of post-treatment Lyme disease syndrome: acute and convalescent serology among a prospective cohort of early Lyme disease patients. Clin Rheumatol. 2015;34:585–589. doi:10.1007/s10067-014-2706-z
18. Wormser GP, Shapiro ED. Implications of gender in chronic Lyme disease. J Womens Health. 2009;18:831–834. doi:10.1089/jwh.2008.1193
19. Schwartz AM, Hinckley AF, Mead PS, Hook SA, Kugeler KJ. Surveillance for Lyme Disease - United States, 2008–2015. MMWR Surveill Summ. 2017;66:1–12. doi:10.15585/mmwr.ss6622a1
20. Johnson L, Shapiro M, Stricker RB, Vendrow J, Haddock J, Needell D. Antibiotic treatment response in chronic lyme disease: why do some patients improve while others do not? Healthcare. 2020;8. doi:10.3390/healthcare8040383
21. Johnson L, Wilcox S, Mankoff J, Stricker RB. Severity of chronic Lyme disease compared to other chronic conditions: a quality of life survey. In PeerJ. 2014;2:e322. doi:10.7717/peerj.322
22. Vendrow J, Haddock J, Needell D, Johnson L. Feature selection from lyme disease patient survey using machine learning. Algorithms. 2020;13:334. doi:10.3390/a13120334
23. Gliklich R, Leavy DN. Registries for Evaluating Patient Outcomes: A User’s Guide.
24. Scotti JM. Sex Differences in Lyme Disease Symptomatology in the Northeast United States. Walden University; 2020.
25. Aucott JN. Personal Communication. Email “Re: your 2022 Study”. (PTLD unpublished data for 32 patients). Received by L. Johnson; 2022.
26. Fallon BA, Petkova E, Keilp J, Britton C. A reappraisal of the U.S. clinical trials of post-treatment lyme disease syndrome. Open Neurol J. 2012;6:79–87. doi:10.2174/1874205X01206010079
27. Horn EJ, Dempsey G, Schotthoefer AM, et al. The Lyme disease biobank: characterization of 550 patient and control samples from the east coast and upper midwest of the United States. J Clin Microbiol. 2020;58. doi:10.1128/jcm.00032-20
28. Horn EJ. Personal Communication. Email “Re: gender in LDB”. (PLD/CLD unpublished data for 73 patients). Received by L. Johnson; 2022.
29. Centers for Disease Control and Prevention. Summary Health Statistics: National Health Interview Survey, 2018. Age-adjusted percent distribution (with standard errors) of work-loss days in the past 12 months among employed adults aged 18 and over, and age-adjusted percent distribution (with standard errors) of bed days in the past 12 months among all adults aged 18 and over, by selected characteristics: United States; 2018. Availabe from: https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2018_SHS_Table_A-9.pdf.
30. Kaiser Family Foundation. Adult self-reported health status analysis of the centers for disease control and prevention (CDC)’s 2020 Behavioral Risk Factor Surveillance System (BRFSS). Timeframe; 2020. Availabe from: https://www.kff.org/other/state-indicator/adult-self-reported-healthstatus/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
31. S.C. Department of Health and Environmental Control (DHEC). BRFSS SC: health problems requiring special equipment; 2014. Availabe from: https://scdhec.gov/sites/default/files/docs/Health/docs/BRFSSreports/2015/8-C.pdf.
32. DeSalvo KB, Fan VS, McDonell MB, Fihn SD. Predicting mortality and healthcare utilization with a single question. Health Serv Res. 2005;40:1234–1246. doi:10.1111/j.1475-6773.2005.00404.x
33. Dias SP, Brouwer MC, van de Beek D. Sex and gender differences in bacterial infections. Infect Immun. 2022;e0028322. doi:10.1128/iai.00283-22
34. Vom Steeg LG, Klein SL. SeXX matters in infectious disease pathogenesis. PLoS Pathog. 2016;12:e1005374–e1005374. doi:10.1371/journal.ppat.1005374
35. Shansky RM, Murphy AZ. Considering sex as a biological variable will require a global shift in science culture. Nat Neurosci. 2021;24:457–464. doi:10.1038/s41593-021-00806-8
36. Mehta LS, Beckie TM, DeVon HA, et al. Acute Myocardial Infarction in Women. Circulation. 2016;133:916–947. doi:10.1161/CIR.0000000000000351
37. Banco D, Chang J, Talmor N, et al. Sex and race differences in the evaluation and treatment of young adults presenting to the emergency department with chest pain. J Am Heart Assoc. 2022;11:e024199. doi:10.1161/JAHA.121.024199
38. Maserejian NN, Link CL, Lutfey KL, Marceau LD, McKinlay JB. Disparities in physicians’ interpretations of heart disease symptoms by patient gender: results of a video vignette factorial experiment. J Womens Health. 2009;18:1661–1667. doi:10.1089/jwh.2008.1007
39. Rebman AW, Yang T, Mihm EA, et al. The presenting characteristics of erythema migrans vary by age, sex, duration, and body location. Infection. 2021;49:685–692. doi:10.1007/s15010-021-01590-0
40. Feder HM Jr, Gerber MA, Luger SW, Ryan RW. Persistence of serum antibodies to Borrelia burgdorferi in patients treated for Lyme disease. Clin Infect Dis. 1992;15:788–793. doi:10.1093/clind/15.5.788
41. Schwarzwalder A, Schneider MF, Lydecker A, Aucott JN. Sex differences in the clinical and serologic presentation of early Lyme disease: results from a retrospective review. Gend Med. 2010;7:320–329. doi:10.1016/j.genm.2010.08.002
42. Centers for Disease Control and Prevention. What is ME/CFS? Availabe from: https://www.cdc.gov/me-cfs/about/index.html.
43. National Center for Complementary and Integrative Health. Fibromyalgia: in Depth. Availabe from: https://www.nccih.nih.gov/health/fibromyalgia-in-depth.
44. Cairns V, Godwin J. Post-Lyme borreliosis syndrome: a meta-analysis of reported symptoms. Int J Epidemiol. 2005;34:1340–1345. doi:10.1093/ije/dyi129
45. National Institute of Arthritis and Musculoskeletal and Skin Diseases. Fibromyalgia: diagnosis, treatment, and steps to take. Availabe from: https://www.niams.nih.gov/health-topics/fibromyalgia/diagnosis-treatment-and-steps-to-take.
46. Adrion ER, Aucott J, Lemke KW, Weiner JP. Health care costs, utilization and patterns of care following Lyme disease. PLoS One. 2015;10:e0116767. doi:10.1371/journal.pone.0116767
47. Ursinus J, Vrijmoeth HD, Harms MG, et al. Prevalence of persistent symptoms after treatment for lyme borreliosis: a prospective observational cohort study. Lancet Reg Health. 2021;6:100142. doi:10.1016/j.lanepe.2021.100142
48. Biau DJ, Kernéis S, Porcher R. Statistics in brief: the importance of sample size in the planning and interpretation of medical research. Clin Orthop Relat Res. 2008;466:2282–2288. doi:10.1007/s11999-008-0346-9
49. Jarefors S, Bennet L, You E, et al. Lyme borreliosis reinfection: might it be explained by a gender difference in immune response? Immunology. 2006;118:224–235. doi:10.1111/j.1365-2567.2006.02360.x
50. Vanderwall AG, Milligan ED. Cytokines in pain: harnessing endogenous anti-inflammatory signaling for improved pain management. Front Immunol. 2019;10:3009. doi:10.3389/fimmu.2019.03009
51. Heidari S, Babor TF, De Castro P, Tort S, Curno M. Sex and Gender Equity in Research: rationale for the SAGER guidelines and recommended use. Res Integr Peer Rev. 2016;1:2. doi:10.1186/s41073-016-0007-6
52. Sylvester SV, Rusu R, Chan B, Bellows M, O’Keefe C, Nicholson S. Sex differences in sequelae from COVID-19 infection and in long COVID syndrome: a review. Curr Med Res Opin. 2022;38:1391–1399. doi:10.1080/03007995.2022.2081454
53. Bai F, Tomasoni D, Falcinella C, et al. Female gender is associated with long COVID syndrome: a prospective cohort study. Clin Microbiol Infect. 2022;28:611.e619–611.e616. doi:10.1016/j.cmi.2021.11.002
54. Dreyer N, Franklin P, Haynes K. Direct-to-Patient Registry and Other Patient-Centric Designs. In: Century Patient Registries: Registries for Evaluating Patient Outcomes: A User’s Guide.
55. Howie L, Hirsch B, Locklear T, Abernethy AP. Assessing the value of patient-generated data to comparative effectiveness research. Health Aff. 2014;33:1220–1228. doi:10.1377/hlthaff.2014.0225
56. Fowler FJ Jr, Cosenza C, Cripps LA, Edgman-Levitan S, Cleary PD. The effect of administration mode on CAHPS survey response rates and results: a comparison of mail and web-based approaches. Health Serv Res. 2019;54:714–721. doi:10.1111/1475-6773.13109
57. Pratap A, Neto EC, Snyder P, et al. Indicators of retention in remote digital health studies: a cross-study evaluation of 100,000 participants. npj Dig Med. 2020;3:21. doi:10.1038/s41746-020-0224-8
58. Bayliss M, Rendas-Baum R, White MK, Maruish M, Bjorner J, Tunis SL. Health-related quality of life (HRQL) for individuals with self-reported chronic physical and/or mental health conditions: panel survey of an adult sample in the United States. Health Qual Life Outcomes. 2012;10:154.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.