Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Does Baseline Cognitive Function Predict the Reduction Rate in HDRS-17 Total Scores in First-Episode, Drug-Naïve Patients with Major Depressive Disorder?
Authors Jiao Q, Dong Y, Ma X, Ji SS ![]() , Liu X, Zhang J, Sun X, Li D, Luo X
, Liu X, Zhang J, Sun X, Li D, Luo X ![]() , Zhang Y
, Zhang Y
Received 5 December 2023
Accepted for publication 6 February 2024
Published 23 February 2024 Volume 2024:20 Pages 353—361
DOI https://doi.org/10.2147/NDT.S453447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Qingyan Jiao,1,* Yeqing Dong,2,* Xiaojuan Ma,3 Shiyi Suzy Ji,4 Xinyu Liu,1 Jian Zhang,1 Xia Sun,1 Dazhi Li,1 Xingguang Luo,5 Yong Zhang1
1Unit of Bipolar Disorder, Tianjin Anding Hospital, Tianjin, 300222, People’s Republic of China; 2Institute of Mental Health, Tianjin Anding Hospital, Mental Health Center of Tianjin Medical University, Tianjin, 300222, People’s Republic of China; 3Tianjin Medical College, Tianjin, 300222, People’s Republic of China; 4Teachers College, Columbia University, New York, NY, USA; 5Department of Psychiatry, Yale University School of Medicine, New Haven, CT, 06511, USA
*These authors contributed equally to this work
Correspondence: Yong Zhang, Unit of Bipolar Disorder, Tianjin Anding Hospital, 13 Liulin Road, Hexi District, Tianjin, 300222, People’s Republic of China, Tel/Fax +86 22 8818 8258, Email [email protected]
Purpose: Major depressive disorder (MDD) is associated with worse cognitive functioning. We aim to examine the association between baseline cognitive functioning and the reduction rate in HDRS-17 total scores and to highlight the predictors of the reduction rate in HDRS-17 total scores in MDD with first-episode, drug-naïve (FED) patients.
Patients and Methods: Ninety FED patients were recruited consecutively and evaluated using the 17-item Hamilton Depression Rating Scale (HDRS-17), the 14-item Hamilton Anxiety Scale (HAMA-14), the Functioning Assessment Short Test (FAST) and the MATRICS Consensus Cognitive Battery (MCCB) at baseline and again at week 8.
Results: Eighty-four FED patients completed the study. Comparison showed that response group had significantly higher T scores in TMT-A, BACS-SC, WMS-III, BVMT-R, MSCEI and CPT-IP, but showed significantly lower scores in FAST total scores including autonomy, occupational functioning, cognitive functioning, interpersonal relationship than non- response group (all p’s< 0.05). Partial correlation analysis also found that the reduction rate in HDRS-17 total scores could be negatively associated with autonomy, cognitive functioning and interpersonal relationship domains as well as total FAST scores, also was further positively associated with T-scores of BACS-SC, CPT-IP and MSCEI in MCCB, even when accounting for potential confounders. Furthermore, the levels of cognitive function domain, autonomy domain in FAST, and BACS-SC, CPT-IP in MCCB may predict the reduction rate in HDRS-17 total scores in FED patients (all p’s< 0.05).
Conclusion: Our findings underscore significant correlations between baseline functioning and the reduction rate in HDRS-17 total scores in FED patients. Moreover, better baseline cognitive function, autonomy, speed of processing and attention/vigilance are more likely to predict patients’ response to antidepressant treatment, indicating pre-treatment better cognitive functioning may be predictors to treatment response in FED.
Keywords: FED, FAST, MCCB, treatment response, the reduction rate in HDRS-17 total scores
Introduction
Major depressive disorder (MDD) is a chronic, recurrent disease that affects 350 million people worldwide annually. Depression is estimated to be the second leading chronic cause of disability.1,2 According to the World Mental Health Survey, the 12-month prevalence rates for major depressive episodes (MDE) vary internationally, from 2.2% in Japan to 10.4% in Brazil, with averages of 5.5% in developed countries and 5.9% in developing ones.3 In China, the lifetime and 12-month prevalence have been documented at 3.9% and 2.3%, respectively.4 MDD, a common psychiatric disorder, is characterized by heterogeneous clinical performance and functional impairment. Impairments of social and neurocognitive function have been evidenced in MDD patients.5,6 Further explorations determined that work capacity, home management, social activity, and personal relationships could be closely related to depressive symptoms.7 MDD patients also continue to present significant moderate cognitive deficits in executive function, memory and attention even in remission, suggesting that cognitive impairment occurs separately from depressive symptoms.8 Significant cognitive deficits are already identifiable during a FED, with some functions showing persistent impairment upon remission. Clinicians must consider cognitive impairment alongside mood symptoms to ensure functional recovery from the MDD, especially first-episode, drug-naïve (FED) patients.9,10 Previous studies have revealed that this persistent and clinically significant functional damage may exist in part due to biomechanisms of brain functional connectivity, such as changes in the left dorsolateral cortex, anterior cingulate cortex activation, left hippocampus and orbitofrontal cortex as observed in resting-state functional magnetic resonance imaging (rsfMRI).11–13 These areas support changes of cognitive processes in unmedicated or first-onset MDD.
Several findings have elaborated on the relationships between treatment outcomes and clinical and functional variables in MDD.14–17 However, the predictive value of baseline functioning in treatment response remains less clear. Existing literature indicated that severe depressive severity and clinical global impression (CGI), suicidal ideation at prior treatment, more MDD episodes, significant medical comorbidities and early response by week 6 were less likely to achieve response or remission.18–21 A recent finding reported that self-reported better working capacity may facilitate the improvement of functioning after treatment with vortioxetine.22 Improvement in verbal memory and scores of Sheehan disability scale (SDS) can predict psychosocial function after antidepressant treatment in adults with MDD.23,24 Only one finding showed early changes in neurocognition could predict response after 8-week vortioxetine treatment in MDD patients.25
So far, few studies have examined the relationship between functioning and treatment response based on whole neurocognitive and psychosocial domains, and no study has explored the discriminant ability of cognitive measures in FED from healthy controls. This gap highlights the need for further investigation into how baseline functioning could predict treatment outcomes in FED patients. Therefore, we propose the hypothesis that baseline cognitive function may be associated with treatment response to antidepressants, and baseline neurocognitive and psychosocial functioning will predict response after 8-week treatment in FED patients.
Materials and Methods
Participants
Ninety-one FED patients aged 18–60 years and ninety-two healthy controls (HCs) were continuously recruited from the Tianjin Anding Hospital between March 2018 and March 2019. All MDD (FED) patients have met the diagnosis of the major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorder-Fifth Edition criteria (DSM-5) and were rated as having baseline scores equal to or exceeding 18 on the 17-item Hamilton Depression Rating Scale (HDRS-17). Exclusion criteria included presence of physical diseases, any history of comorbid alcohol or drug abuse, or presence of some severe psychiatric diseases. Moreover, we excluded MDD patients who received medications and formal psychotherapy prior to enrollment.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study protocol was granted by the Ethics Committee of Tianjin Anding Hospital. Written informed consent was obtained from all participants.
Assessments and Materials
Participants’ demographic details, including age, gender, educational background, duration of FED, and medication history, were collected through structured interviews. The severity of depressive and anxious symptoms was measured using the HDRS-17 and the 14-item Hamilton Anxiety Scale (HAMA-14). We then measured neurocognitive and functional impairment in MDD patients using the MATRICS Consensus Cognitive Battery (MCCB) and the Functioning Assessment Short Test (FAST).
The FAST contains 24 items with six domains of functioning: autonomy, occupational functioning, cognitive functioning, financial issues, interpersonal relationships and leisure time. The FAST is rated on a 4-point scale (0–3) ranging from no difficulty to severe difficulty, with higher scores indicating more severe functional impairment. The Chinese version of the FAST has excellent psychometric characteristics in patients with bipolar disorder.26
The MCCB was originally developed for schizophrenia, but our recent finding showed that the Chinese version of the MCCB also displayed better psychometric properties in MDD patients.27 The Chinese MCCB version comprises 9 tasks across 7 cognitive domains, including speed of processing (Trail Making Test-Part A, TMT-A; Brief Assessment of Cognition in Schizophrenia, Symbol Coding sub-test, BACS-SC; Animal Naming, Fluency), verbal learning (Hopkins Verbal Learning Test-Revised, HVLT-R), visual learning (Brief Visuospatial Memory Test-Revised, BVMT-R), reasoning and problem solving (Neuropsychology Assessment Battery, Mazes), working memory (Wechsler Memory Scale-III, WMS-III), attention/vigilance (Continuous Performance Test-Identical Pairs version, CPT-IP) and social cognition (Salovey–Caruso Emotional Intelligence Test, MSCEI). In this study, we calculate the T-scores of each task across 7 cognitive domains. A lower score indicates more impaired cognition.
Procedures and Treatments
FED patients underwent evaluations both at baseline and week 8 by an experienced psychiatrist. Then, according to the HDRS-17 scores before and after antidepressant treatment for eight weeks, the reduction rate in HDRS-17 total scores is calculated as a measure of the prognostic effects of antidepressant treatment. We defined “response” with 50% reduction (including 50%) in HDRS-17 total scores from baseline to the endpoint after 8-week treatment. Lower than 50% reduction in HDRS-17 total scores was defined as “non-response”.28,29
We chose selective serotonin reuptake inhibitors (SSRIs) including sertraline, fluoxetine, escitalopram or citalopram, and serotonin-norepinephrine reuptake inhibitors (SNRIs) including duloxetine and venlafaxine as treatment medications. All antidepressants were kept within flexible dose according to treatment guidelines for MDD.30 Some sedative-hypnotic medications needed for insomnia including zopiclone (7.5mg/per day) and zolpidem (5–10mg/per day), but other hypnotic medications, such as clonazepam and alprazolam, could not be used because of the presence of cognitive impairment.
This study’s registration details can be found on http://www.chictr.org.cn/ (Identifier number: ChiCTR-IIR-17010453).
Data Analysis
The demographic and clinical cognition information between two groups (MDD vs HC; response vs non-response) was analyzed by the independent sample t-tests for continuous variables and chi-square tests (Fisher Exact Test) for categorical variables. The partial correlation analysis between the HDRS reduction rate and cognitive variables was performed, with general information including baseline HDRS-17, HAMA-14, age, gender, educational levels and duration of FED as covariations. Using stepwise linear regression analysis, we further analyzed the potential predictors of the HDRS reduction rate in FED patients. In this analytical model, we chose the reduction rate in HDRS-17 total scores as the dependent variable, and other clinical related variables and demographic factors, including baseline HDRS-17 score, baseline HAMA-14 score, age, gender, education levels and FAST scores in all dimensions and all neurocognitive tests, etc., were chosen as the independent variables. All statistical analyses were performed by Software SPSS 16.0, and all tests were two-tailed (p< 0.05).
Results
Demographic Characteristics
Six participants were excluded because of unwillingness to continue for treatment (4 patients) or failing to complete all assessments (2 patients and 4 HCs). Finally, 84 patients with FED and 88 HCs completed all assessments in our study. There were no significant differences between the MDD and HC groups in gender ratio, age, and education level (all p’s>0.05). The total FAST score of the MDD group was significantly higher than that in HCs, and the scores of FAST total score, autonomy, occupational functioning, cognitive functioning, interpersonal relationships (p<0.001) and leisure time (p=0.001) were significantly higher than those in HC group. While six domains of the neurocognitive function in the MDD group were significantly lower than those in the HC group, TMT-A, BACS-SC, HVLT-R, Fluency, CPT-IP and MSCEI (all p’s<0.001). See Table 1.
 |
Table 1 Demographic and Baseline Cognitive Function in MDD Patients and HCs |
The FED patients with response totalled 74 (88.1%) while those with non-response totalled 10 patients (11.9%). The antidepressants prescribed to the FED patients were sertraline (16.7%, range = 100–150mg, Mean = 110.7, SD = 21.3mg), fluoxetine (10.7%, range = 20–40mg, Mean = 23.3, SD = 7.1mg), escitalopram (28.6%, range = 10–20mg, Mean = 14.0, SD = 4.7mg), citalopram (10.7%, range = 20–40mg, Mean = 25.6, SD = 8.8mg), duloxetine (25.0%, range = 30–90mg, Mean = 62.9, SD = 18.8mg) and venlafaxine (8.3%, range = 75–225mg, Mean = 139.3, SD = 51.6mg).
Comparison of the Related Variables Between Response and Non- Response Group of FED
Our findings showed that response had significantly higher T scores in TMT-A, BACS-SC, WMS-III, BVMT-R, MSCEI and CPT-IP, compared with non-response [36.04(13.03) vs 27.20 (11.30), t= −2.041, p= 0.044], [44.78(11.12) vs 31.8(13.60), t= −3.374, p= 0.001], [44.23(10.39) vs 35.10(10.93), t= −2.593, p= 0.011], [42.57(9.62) vs 34.20(10.54), t= −2.554, p= 0.013], [37.72(9.86) vs 28.60 (8.24), t= −2.791, p= 0.007], [42.28(11.32) vs 34.50(11.72), t = −2.033, p = 0.045]. Furthermore, response showed significantly lower scores in FAST total scores including autonomy, occupational functioning, cognitive functioning, interpersonal relationship than non-response [24.61(9.42) vs 39.20(11.39), t= 4.486, p= 0.000], [2.70(1.83) vs 4.30(1.83), t= 2.586, p= 0.011], [4.46(3.45) vs 8.80(5.37), t= 3.47, p= 0.001], [6.72(2.96) vs 10.30(3.34), t= 3.538, p= 0.001], [6.54(3.74) vs 10.10(3.76), t= 2.822, p= 0.006]. No significant differences in age, educational level, duration of FED, baseline HAMA-14 and HDRS-17, and financial issues, leisure time domains in FAST, or HVLT-R, Fluency, Mazes measures in MCCB (all p’s > 0.05).
Relationships Between the Reduction Rate in HDRS-17 Total Scores and Cognitive Variables in FED Group
The relationships were analyzed between the reduction rate in HDRS-17 total scores and baseline FAST total scores including its six domains and baseline T scores of seven neurocognitive tasks by Pearson’s correlation analysis. After controlling for baseline HDRS-17, HAMA-14, age, gender, educational levels and duration of FED, the results of partial correlation analysis showed that the reduction rate in HDRS-17 total scores was negatively associated with autonomy, cognitive functioning and interpersonal relationship domains as well as total FAST scores. Additionally, the reduction rate in HDRS-17 total scores was positively associated with T-scores of BACS-SC, CPT-IP and MSCEI in MCCB. See Table 2.
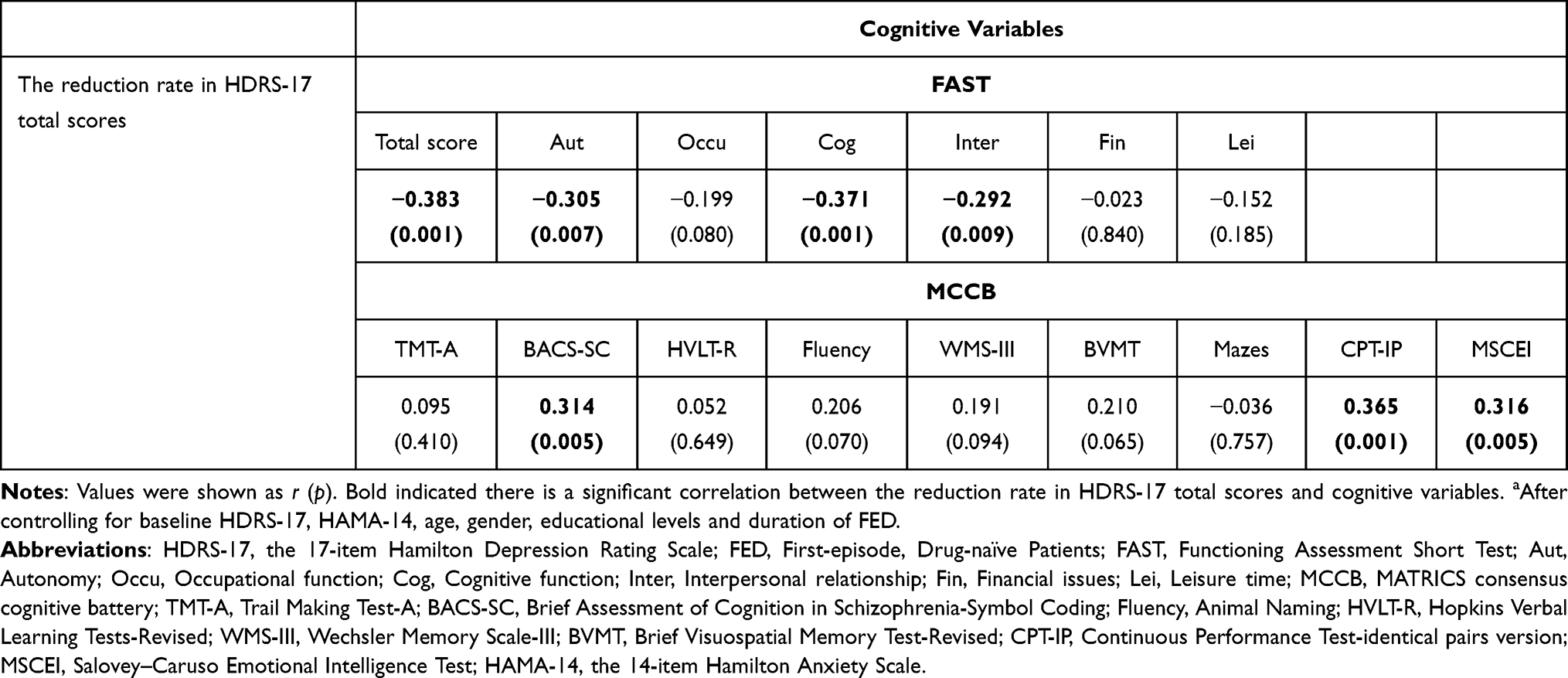 |
Table 2 The Partial Correlation of the Reduction Rate in HDRS-17 Total Scores and Cognitive Variables in Patients with FED (n=84)a |
Stepwise Linear Regression Analysis of the Reduction Rate in HDRS-17 Total Scores in FED Group
Using linear regression analysis, we explored the potential predictors of the reduction rate in HDRS-17 total scores in FED patients. In this analytical model, the reduction rate in HDRS-17 total scores was chosen as the dependent variable, and other clinical related variables (baseline HDRS-17 score, baseline HAMA-14 score, FAST scores in all dimensions and all neurocognitive tests) and partial demographic factors (age, gender and education level) were chosen as the independent variables. The results showed that the cognitive functioning domain (β=−0.013, p= 0.001), autonomy (β= −0.023, p= 0.001), BACS-SC (β= 0.004, p= 0.001), and CPT-IP (β= 0.003, p= 0.018) were identified as predictive factors for the reduction rate in HDRS-17 total scores in FED patients. See Table 3.
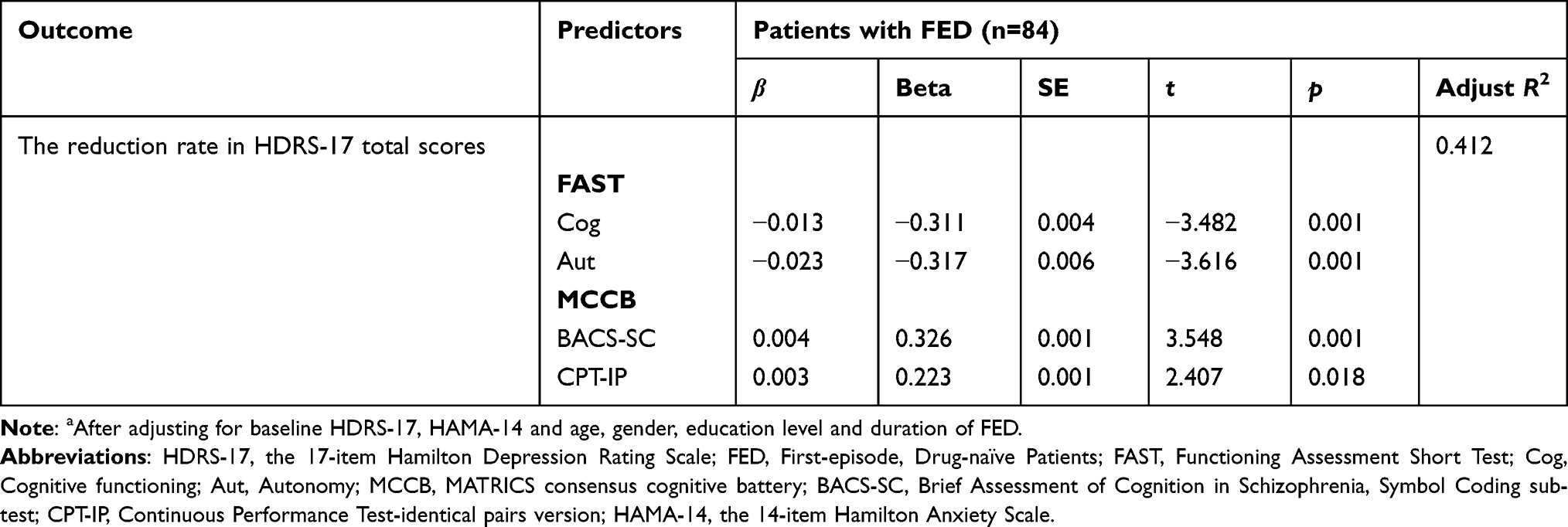 |
Table 3 Stepwise Linear Regression Analysis of the Reduction Rate in HDRS-17 Total Scores in FED (n=84)a |
Discussion
This study was a descriptive analysis study with a case–control design. We found that patients with depression had significantly lower social and neurocognitive functions than healthy controls. In FED patients, the response group had significantly higher scores in some domains in MCCB, but showed significantly lower scores in FAST total scores including autonomy, occupational functioning, cognitive functioning, interpersonal relationship than non-response group. Moreover, the reduction rate of HDRS-17 could be negatively associated with autonomy, cognitive functioning and interpersonal relationship domains as well as total FAST scores, was further positively associated with T-scores of BACS-SC, CPT-IP and MSCEI in MCCB. Furthermore, the cognitive functioning domains, autonomy, BACS-SC, and CPT-IP were identified as predictive factors for the reduction rate in HDRS-17 total scores. Our results are largely consistent with the study hypothesis, and underscore significant correlations between baseline functioning and the reduction rate in HDRS-17 total scores in FED patients with MDD.
These findings align with numerous studies on impairments of cognitive or social functioning in MDD.31–35 A recent meta-analysis also affirmed this adverse condition for total functioning in MDD.9 Our findings supported same outcomes in FED patients again. Importantly, comparisons showed that response group had significantly higher T scores in TMT-A, BACS-SC, WMS-III, BVMT-R, MSCEI and CPT-IP, compared with non-response group in FED. However, response group suggested significantly lower scores in FAST total scores including autonomy, occupational functioning, cognitive functioning, interpersonal relationship than non-response group. This is consistent with literature indicating that cognitive dysfunction is a strong predictor of occupational and social dysfunction in MDD adults. The persistence of cognitive deficits after remission of depressive symptoms has been shown to contribute to the inability of patients with MDD to achieve full functional recovery.36,37 Recent research has also shown that objective cognitive dysfunction can negatively impact organizational, occupational, and social functioning and can lead to poor treatment outcomes and recurrence of MDD.38
In our study, the partial correlation analysis demonstrated that the reduction rate in HDRS-17 total scores was associated significantly with autonomy, cognitive and interpersonal relationship domains, as well as total FAST scores, speed of processing, attention/vigilance and social cognition. This finding remained significant even after adjusting for baseline depression, anxiety and demographic confounders. Similar findings have reported these associations between treatment response and better depression-related functioning and quality of life in MDD.16,39 One strength of the current study was that we examined this relationship between treatment response and functional measures based on broad range of psychosocial and neurocognitive functioning in FED patients. We found that ability to self-manage and interpersonal relationships may be more predictive for treatment response to antidepressants. Our previous finding also revealed that employed bipolar depressed patients displayed greater social functioning, better verbal learning performance and speed of processing than unemployed those patients.40 Therefore, we speculate that persistent work status and interpersonal activity could attribute to better psychosocial and cognitive functioning, and self-management in daily life, working capacity and interpersonal activity are more likely to promote the ability to memorize and learn new information in the real world,41 which may further facilitate treatment response in FED patients.
So far, few studies have focused on the correlation between functional impairment and treatment response, and no study on prediction of pre-treatment functioning to treatment response has been established in FED patients. An fMRI study identified that brain functional connectivity (FC) between the dorsolateral prefrontal cortex (DLPFC) and the subgenual anterior cingulate cortex (sgACC) may predict the efficacy of antidepressant treatment among medication-free patients with MDD,42 while these brain functional areas could be core region related to cognitive functioning.43 A recent finding also revealed that better baseline verbal memory may predict the 8-week treatment response in medicated MDD patients with anxious symptom,44 partially demonstrating the predictive value of baseline cognitive performance to treatment response. Additionally, information processing speed and attention, the most important cognitive functions thought to be core domains of cognitive impairment in schizophrenia, have also been shown to be stronger predictors for MDD.45 Another research in elderly MDD patients has suggested that better word learning is related to higher remission rates after antidepressant treatment.46 Our findings highlighted that better cognitive functioning, autonomy, speed of processing and attention/vigilance are more likely to predict a patient’s response to antidepressant treatment, indicating pre-treatment better cognitive functioning may be predictors to the reduction rate in HDRS-17 total scores in FED. These results may have indirectly elucidated possible predictions of cognitive function to treatment response in FED.
Several limitations should be taken into account in this study. First, due to an unbalanced sample size, our findings on differences of clinical variables between response and non-response group should be cautiously elucidated, this is likely to attenuate our findings when we analyze the correlations between treatment response and functioning variables, and it is difficult to exclude the impact of the possible confounders by the multivariable analysis because of this insufficient and unbalanced sample size, so the prediction may be biased. Second, a shorter time period of 8 weeks for medication intervention may impede the predictive value of treatment response, thus our current findings are not able to represent long-term outcome. Third, our predictive value was not strong, implying possible risks or protective factors need to be considered, such as instances of poorer social adjustment.47 Additionally, some biomarkers may predict final treatment outcome and should be involved in future studies. Last, some medications including zopiclone and zolpidem could worsen cognitive performance, although clonazepam and alprazolam could not be used in the study, the possible effect of other sedative-hypnotic medications on cognitive performance should be considered.48
Conclusion
Our findings underscore relationships between baseline functioning and the reduction rate in HDRS-17 total scores in FED patients and mainly revealed that the baseline cognitive level, including cognitive function, autonomy, speed of processing and attention/vigilance have better predictive value for the prognosis of antidepressant treatment in FED patients.
Acknowledgments
We acknowledge the medical staff of Tianjin Anding Hospital for their helps in the collection of samples, especially all participants and their family members for their excellent cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-033A).
Disclosure
The authors report no conflicts of interest in connection with this manuscript.
References
1. Lu J, Xu X, Huang Y, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2021;8(11):981–990. doi:10.1016/s2215-0366(21)00251-0
2. Wang Q. The social determinants of depressive disorders in China. Lancet Psychiatry. 2021;8(11):939–940. doi:10.1016/s2215-0366(21)00389-8
3. Ferrari AJ, Somerville AJ, Baxter AJ, et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychological Med. 2013;43(3):471–481. doi:10.1017/s0033291712001511
4. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/s2215-0366(18)30511-x
5. Evans VC, Iverson GL, Yatham LN, Lam RW. The relationship between neurocognitive and psychosocial functioning in major depressive disorder: a systematic review. J Clini Psych. 2014;75(12):1359–1370. doi:10.4088/JCP.13r08939
6. Knight MJ, Baune BT. Cognitive dysfunction in major depressive disorder. Curr Opin Psychiatry. 2018;31(1):26–31. doi:10.1097/yco.0000000000000378
7. Fried EI, Nesse RM. The impact of individual depressive symptoms on impairment of psychosocial functioning. PLoS One. 2014;9(2):e90311. doi:10.1371/journal.pone.0090311
8. Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychological Med. 2014;44(10):2029–2040. doi:10.1017/s0033291713002535
9. Ahern E, Semkovska M. Cognitive functioning in the first-episode of major depressive disorder: a systematic review and meta-analysis. Neuropsychology. 2017;31(1):52–72. doi:10.1037/neu0000319
10. Yen YC, Chiu NY, Hwang TJ, et al. A Multi-Center Study for the Development of the Taiwan Cognition Questionnaire (TCQ) in major depressive disorder. J Pers Med. 2022;12(3):359. doi:10.3390/jpm12030359
11. Albert KM, Potter GG, Boyd BD, Kang H, Taylor WD. Brain network functional connectivity and cognitive performance in major depressive disorder. J Psychiatr Res. 2019;110:51–56. doi:10.1016/j.jpsychires.2018.11.020
12. Hao H, Chen C, Mao W, Zhong J, Dai Z. Aberrant brain regional homogeneity in first-episode drug-naïve patients with major depressive disorder: a voxel-wise meta-analysis. J Affective Disord. 2019;245:63–71. doi:10.1016/j.jad.2018.10.113
13. Matsuo K, Glahn DC, Peluso MA, et al. Prefrontal hyperactivation during working memory task in untreated individuals with major depressive disorder. Mol Psychiatry. 2007;12(2):158–166. doi:10.1038/sj.mp.4001894
14. Bressi C, Fronza S, Minacapelli E, et al. Short-term psychodynamic psychotherapy with mentalization-based techniques in major depressive disorder patients: relationship among alexithymia, reflective functioning, and outcome variables – a Pilot study. Psychol Psychother. 2017;90(3):299–313. doi:10.1111/papt.12110
15. Carrasco JL, Kornstein SG, McIntyre RS, et al. An integrated analysis of the efficacy and safety of desvenlafaxine in the treatment of major depressive disorder. Int Clin Psychopharmacol. 2016;31(3):134–146. doi:10.1097/yic.0000000000000121
16. Dennehy EB, Marangell LB, Martinez J, Balasubramani GK, Wisniewski SR. Clinical and functional outcomes of patients who experience partial response to citalopram: secondary analysis of STAR*D. J Psychiatr Pract. 2014;20(3):178–187. doi:10.1097/01.pra.0000450317.76117.62
17. Rothschild AJ, Raskin J, Wang CN, Marangell LB, Fava M. The relationship between change in apathy and changes in cognition and functional outcomes in currently non-depressed SSRI-treated patients with major depressive disorder. Compreh Psychiatry. 2014;55(1):1–10. doi:10.1016/j.comppsych.2013.08.008
18. Athreya AP, Neavin D, Carrillo-Roa T, et al. Pharmacogenomics-driven prediction of antidepressant treatment outcomes: a machine-learning approach with multi-trial replication. Clin Pharmacol Ther 2019;106(4):855–865. doi:10.1002/cpt.1482
19. Ciudad A, Álvarez E, Roca M, et al. Early response and remission as predictors of a good outcome of a major depressive episode at 12-month follow-up: a prospective, longitudinal, observational study. J Clini Psych. 2012;73(2):185–191. doi:10.4088/JCP.10m06314
20. Novick D, Hong J, Montgomery W, Dueñas H, Gado M, Haro JM. Predictors of remission in the treatment of major depressive disorder: real-world evidence from a 6-month prospective observational study. Neuropsychiatr Dis Treat. 2015;11:197–205. doi:10.2147/ndt.S75498
21. Trivedi MH, Morris DW, Wisniewski SR, et al. Clinical and sociodemographic characteristics associated with suicidal ideation in depressed outpatients. Can J Psychiatry. 2013;58(2):113–122. doi:10.1177/070674371305800209
22. Murthy NV, Xu R, Zhong W, Harvey PD. Using self-reported vocational functioning measures to identify employed patients with impaired functional capacity in major depressive disorder. J Affective Disord. 2020;260:550–556. doi:10.1016/j.jad.2019.09.025
23. Castellano S, Torrent C, Petralia MC, et al. Clinical and neurocognitive predictors of functional outcome in depressed patients with partial response to treatment: one year follow-up study. Neuropsychiatr Dis Treat. 2020;16:589–595. doi:10.2147/ndt.S224754
24. Soares CN, Wajsbrot DB, Boucher M. Predictors of functional response and remission with desvenlafaxine 50 mg and 100 mg: a pooled analysis of randomized, placebo-controlled studies in patients with major depressive disorder. CNS Spectrums. 2020;25(3):363–371. doi:10.1017/s1092852919000828
25. Park C, Zuckerman H, Subramaniapillai M, et al. Using early changes in cold cognition to predict response to vortioxetine in major depressive disorder. Psychiatry Res. 2020;284:112767. doi:10.1016/j.psychres.2020.112767
26. Zhang Y, Long X, Ma X, et al. Psychometric properties of the Chinese version of the Functioning Assessment Short Test (FAST) in bipolar disorder. J Affective Disord. 2018;238:156–160. doi:10.1016/j.jad.2018.05.019
27. Liang S, Yu W, Ma X, et al. Psychometric properties of the MATRICS Consensus Cognitive Battery (MCCB) in Chinese patients with major depressive disorder. J Affective Disord. 2020;265:132–138. doi:10.1016/j.jad.2020.01.052
28. Trivedi MH, Corey-Lisle PK, Guo Z, Lennox RD, Pikalov A, Kim E. Remission, response without remission, and nonresponse in major depressive disorder: impact on functioning. Int Clin Psychopharmacol. 2009;24(3):133–138. doi:10.1097/YIC.0b013e3283277614
29. Constantino MJ, Adams ML, Pazzaglia AM, Bernecker SL, Ravitz P, McBride C. Baseline patient characteristics as predictors of remission in interpersonal psychotherapy for depression. Psychother Res. 2013;23(2):190–200. doi:10.1080/10503307.2013.765997
30. Milev RV, Giacobbe P, Kennedy SH, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 4. neurostimulation treatments. Can J Psychiatry. 2016;61(9):561–575. doi:10.1177/0706743716660033
31. Pan Z, Park C, Brietzke E, et al. Cognitive impairment in major depressive disorder. CNS Spectrums. 2019;24(1):22–29. doi:10.1017/s1092852918001207
32. Sumiyoshi T, Watanabe K, Noto S, et al. Relationship of cognitive impairment with depressive symptoms and psychosocial function in patients with major depressive disorder: cross-sectional analysis of baseline data from PERFORM-J. J Affective Disord. 2019;258:172–178. doi:10.1016/j.jad.2019.07.064
33. Ladegaard N, Videbech P, Lysaker PH, Larsen ER. The course of social cognitive and metacognitive ability in depression: deficit are only partially normalized after full remission of first episode major depression. Br J Clin Psychol. 2016;55(3):269–286. doi:10.1111/bjc.12097
34. van Wingen GA, van Eijndhoven P, Tendolkar I, et al. Neural basis of emotion recognition deficits in first-episode major depression. Psychological Med. 2011;41(7):1397–1405. doi:10.1017/s0033291710002084
35. Knight MJ, Baune BT. The direct and indirect relationship between social cognition and psychosocial dysfunction in major depressive disorder. Frontiers in Psychiatry. 2019;10:347. doi:10.3389/fpsyt.2019.00347
36. Zimmerman M, McGlinchey JB, Posternak MA, Friedman M, Boerescu D, Attiullah N. Discordance between self-reported symptom severity and psychosocial functioning ratings in depressed outpatients: implications for how remission from depression should be defined. Psychiatry Res. 2006;141(2):185–191. doi:10.1016/j.psychres.2005.05.016
37. Yen YC, Rebok GW, Gallo JJ, Jones RN, Tennstedt SL. Depressive symptoms impair everyday problem-solving ability through cognitive abilities in late life. Am J Geriatric Psychiatry. 2011;19(2):142–150. doi:10.1097/JGP.0b013e3181e89894
38. Cha DS, Carmona NE, Subramaniapillai M, et al. Cognitive impairment as measured by the THINC-integrated tool (THINC-it): association with psychosocial function in major depressive disorder. J Affective Disord. 2017;222:14–20. doi:10.1016/j.jad.2017.06.036
39. Ekeblad A, Falkenström F, Holmqvist R. Reflective functioning as predictor of working alliance and outcome in the treatment of depression. J Consult Clin Psychol. 2016;84(1):67–78. doi:10.1037/ccp0000055
40. Liu X, Ma X, Wang W, et al. The functional impairment of different subtypes and occupational states in euthymic patients with bipolar disorder. BMC Psychiatry. 2021;21(1):240. doi:10.1186/s12888-021-03242-x
41. Bonnin CM, Reinares M, Martínez-Arán A, et al. Effects of functional remediation on neurocognitively impaired bipolar patients: enhancement of verbal memory. Psychological Med. 2016;46(2):291–301. doi:10.1017/s0033291715001713
42. Wang Q, Tian S, Tang H, et al. Identification of major depressive disorder and prediction of treatment response using functional connectivity between the prefrontal cortices and subgenual anterior cingulate: a real-world study. J Affective Disord. 2019;252:365–372. doi:10.1016/j.jad.2019.04.046
43. Peng X, Wu X, Gong R, et al. Sub-regional anterior cingulate cortex functional connectivity revealed default network subsystem dysfunction in patients with major depressive disorder. Psychological Med. 2021;51(10):1687–1695. doi:10.1017/s0033291720000434
44. Braund TA, Tillman G, Palmer DM, Harris AWF. Verbal memory predicts treatment outcome in syndromal anxious depression: an iSPOT-D report. J Affective Disord. 2020;260:245–253. doi:10.1016/j.jad.2019.09.028
45. Burton CZ, Vella L, Harvey PD, Patterson TL, Heaton RK, Twamley EW. Factor structure of the MATRICS Consensus Cognitive Battery (MCCB) in schizophrenia. Schizophr Res. 2013;146(1–3):244–248. doi:10.1016/j.schres.2013.02.026
46. Morimoto SS, Gunning FM, Kanellopoulos D, et al. Semantic organizational strategy predicts verbal memory and remission rate of geriatric depression. Int J Geriatr Psychiatry. 2012;27(5):506–512. doi:10.1002/gps.2743
47. Wedig MM, Weinstock LM, Epstein-Lubow G, Miller IW. Predictors of depressive symptoms at hospital discharge in patients with major depressive disorder. Int j Psychiatry Clin Pract. 2013;17(2):144–147. doi:10.3109/13651501.2013.777746
48. Abad VC, Guilleminault C. Insomnia in elderly patients: recommendations for pharmacological management. Drugs Aging. 2018;35(9):791–817. doi:10.1007/s40266-018-0569-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.