Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Does a diabetic retinopathy educational program raise awareness among elderly diabetic patients?
Authors Khalaf FR, Fahmy HM, Ibrahim AK ![]() , Mohamed GA, El Sayed Ez Eldeen M, Elkady A
, Mohamed GA, El Sayed Ez Eldeen M, Elkady A ![]() , Hetta HF
, Hetta HF ![]()
Received 8 March 2019
Accepted for publication 27 August 2019
Published 20 September 2019 Volume 2019:12 Pages 1867—1875
DOI https://doi.org/10.2147/DMSO.S208072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Fatma R Khalaf,1 Heba M Fahmy,2 Ahmed K Ibrahim,3 Ghada A Mohamed,4 Manal El Sayed Ez Eldeen,4 Azza Elkady,5 Helal F Hetta6,7
1Department of Community Health Nursing, Faculty of Nursing, Assiut University, Assiut, Egypt; 2Department of Gerontological Nursing, Faculty of Nursing, Assiut University, Assiut, Egypt; 3Department of Community Medicine, Faculty of Medicine, Assiut University, Assiut, Egypt; 4Department of Internal Medicine, Faculty of Medicine, Assiut University, Assiut, Egypt; 5Sohag University Medical Administration, Sohag, Egypt; 6Department of Medical Microbiology and Immunology, Faculty of Medicine, Assiut University, Assiut, Egypt; 7Department of Internal Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, USA
Correspondence: Helal F Hetta
Department of Internal Medicine, University of Cincinnati College of Medicine, Cincinnati, 231 Albert B. Sabin Way, PO Box 670595, Cincinnati, OH 45267-0595, USA
Email [email protected]
Background and aim: Diabetic retinopathy is a serious and common complication of diabetes that causes irreversible blindness. The aim of the present study was to assess the knowledge, attitudes, and practice regarding diabetic retinopathy among patients attending a diabetic clinic and identify the effect of an educational program about diabetic retinopathy.
Patients and methods: Two hundred diabetic patients were recruited from the outpatient’s diabetic clinic, Assiut University hospitals, Egypt. Quasi-experimental (pretest-posttest) research design was applied using a structured interview questionnaire; including socio-demographic data, assessment of the patients’ knowledge, attitude, and practices toward diabetic retinopathy.
Results: The mean score of knowledge and attitude showed significant improvement (5.3 and 15.1, respectively in pretest vs 16.7 and 16.8, respectively in posttest) among the diabetic patients (p<0.001). From multivariate linear regression model; the predictors for knowledge score were educational level, family history of diabetes and diabetic retinopathy and hypertension. Likewise, attitude score predictors were age, residence, and smoking. Predictors for practice score were hypertension, blood sugar level, and weight.
Conclusion: There was a statistically significant relationship between educational level and mean knowledge score. The diabetic education program significantly helped to improve awareness of patients in relation to diabetic retinopathy.
Keywords: diabetic retinopathy, knowledge, attitude, practices, educational program
Introduction
Diabetes mellitus (DM) is a progressive disease accompanied by metabolic disorders and microvascular complications such as retinopathy, neuropathy, and nephropathy.1–4 Diabetic retinopathy (DR) is considered one of the most common and severe complications of DM and a major cause of blindness worldwide. Also, it is associated with loss of productivity and quality of life, and may lead to additional socioeconomic burden.5–7 About 4.8% (1.8 million) of global blindness was due to DR.8–10 DR is a priority blinding disease and is now included in the disease control strategy of ‘vision 2020’ initiative.11 Symptoms of diabetic retinopathy include; seeing spots or floaters, blurred vision, having a dark or empty spot in the center of vision and difficulty seeing well at night.12 Often, the early stages of DR have no visual symptoms. That is why the American Optometric Association (AOA)13 recommended that everyone with diabetes have a comprehensive dilated eye examination once a year.
Treatment of diabetic retinopathy varies depending on the extent of the disease. People with diabetic retinopathy may need laser surgery to seal leaking blood vessels or to discourage other blood vessels from leaking.13 The vast majority of diabetic patients who lose vision do so, not because of an inability to treat their disease, but due to lack of awareness. Raising awareness about DR is an important element for early diagnosis and treatment of this blinding disease.14 To control or prevent vision loss, appropriate health education is necessary to encourage those at risk to seek timely and appropriate care. Also, this will require developing educational materials that are regionally and culturally appropriate with an understanding of the current knowledge, attitudes, and practices in the community.15
KAP is a method to collect specific information about what is patient-known, believed and done in relation to a particular topic. The community’s understanding of any given topic is the knowledge. Attitude refers to their feelings toward the subject as well as preconceived ideas that they may have toward it. Practice is the ways in which they demonstrate their knowledge and attitude through their actions.
A few studies have been conducted regarding the knowledge and awareness about DR among the diabetic population.16 This is the first study carried out on knowledge, attitude, and practice regarding DR in Assuit university hospital. So, the current study has been conducted to determine the level of knowledge, attitude, reported practice, and to identify the impact of an educational program on a diabetic population.
Subjects and methods
Research design
Quasi-experimental (pretest-posttest) research design. This design is often used to evaluate the benefits of specific interventions. It resembles experimental research but is not true experimental research. Although the independent variable is manipulated, participants are not randomly assigned to conditions or orders of conditions. Quasi-experiments are most likely to be conducted in field settings in which random assignment is difficult or impossible. They are often conducted to evaluate the effectiveness of a treatment or an educational intervention.
Setting
The present study was conducted at the outpatient’s diabetic clinic of Assiut University hospitals, where diabetic patients aged ≥60 years were recruited.
Sampling technique and sample size
Systematic random sampling technique was used with sampling interval of three. Sample size was calculated using Open Epi, (ver. 3) using prevalence of diabetes 15.6% according to Hegazi et al17 and 95% confidence interval. The minimum required sample was 185 subjects, 10% was added to compensate for dropout and refusals. A total number of 200 patients were recruited for the study. The field work was executed from August 2017 to January 2018.
Inclusion criteria
All diabetic patients aged 60 years and above of both sexes who were attending outpatient diabetic clinic and agreed to participate in this study were included.
Exclusion criteria
Diabetic patients aged less than 60 years, mentally challenged patients who were not able to give informed consent, and patients who were not able to understand and respond to the questions administered were excluded from the study.
Study tools
- Interview questionnaire: the details regarding socio-demographic data, knowledge, attitude, reported practices, and degree of adherence to antidiabetic medication were obtained by using structured interview questionnaire, which was designed by the researchers after reviewing the related literature.
Section I: was structured in five parts:
Part 1): socio-demographic data: age, educational status, and occupation.
Part 2): included questions regarding knowledge about diabetic retinopathy (i.e., know that diabetes can cause eye disease, any parts of the eye that can be affected by diabetes mellitus, definition, any parts of the eye that should be examined for changes due to diabetic retinopathy, signs and symptoms, risk factors, diagnosis, prevention, treatment and complications). A scoring system was designed for the assessment of patient’s knowledge containing 11 questions; a score of 1 was given for each correct answer and a score of zero was given for an incorrect answer and “don’t know”.
Part 3): included questions about eye care practices reported by the patients (i.e., how often do you go for eye examination? whom do you consult in the event of eye problems? do you take diabetic medication regularly, do you measure blood sugar regularly, and do you examine the fundus (retina) of the eye). Each correct answer of practice questions was awarded 5 marks while a wrong answer was given 0 marks.
Part 4): included questions regarding the patients’ attitudes toward DR (i.e., is regular eye checkup important even if they do not have eye problems?). It consisted of 12 statements expressing point of view about DR. The responses were based on a three-point Likert scale (agree, uncertain, and disagree) instead of five points (strongly agree, agree, uncertain, disagree, and strongly disagree). Items were scored (2, 1, and 0) respectively; the score was reversed for negative statements.
Total scores for knowledge, attitude, and practice were calculated by summing up the responses for each respondent.
Reliability of the tool
Internal consistency of the scale was estimated using Cronbach-α test; the overall Cronbach-α of the KAP questionnaire was very good (0.82) with satisfactory reliability statistics for the main domains (ranging between acceptable (>0.5) to very good (0.8–0.9) as per Bowling, 2002);18 and Cronbach-α for the total scale was not improved by removal of any of the remaining items.
Questionnaire validity
The questionnaire was evaluated by three experts from the departments of Community Health Nursing, Internal medicine, and Public Medicine at Assiut University. They assessed the instruments for clarity, relevance, comprehensiveness, and applicability.
- Assessment phase: it was based on pre-test assessment of participants’ knowledge, attitude, and practice regarding diabetic retinopathy.
- Planning phase: it included the arrangement for conduction of the program such as: teaching place: the program was conducted in diabetic clinic, teaching time: was scheduled according to availability of the participant and the coordination between the researchers and participants, teaching methods and materials: we used simple teaching methods such as: lecture, picture, video, and discussion. We prepared the media handouts regarding diabetic retinopathy and distributed it to every participant at the end of the program. The contents of the program was divided into sessions; these sessions included: introduction about diabetes, definition, signs and symptoms, risk factors, complications and prevention of diabetic retinopathy and post-test was done.
- Implementation stage: every participant goes to one session for two hours to complete the program content. Upon completion of the program, an immediate post-test was applied.
- Evaluation stage: it was performed through the post-test after implementing and completing the course to assess participants’ knowledge and attitude. After that, diabetic patients were given a brochure containing main information about diabetic retinopathy.
Procedure
- Administrative phase: official approval was obtained from the Dean of the Faculty of Nursing, Assiut University for the Director of out-patient clinics of the main Assiut hospital to start and complete the study.
- Pilot study: pilot study was carried out, before starting data collection, on 10 diabetic patients, which were excluded from the study. The aim of this study was to test the clarity of the tools and to estimate the required time to complete the questionnaire. Based on the results of pilot study, necessary modifications of the tools were made.
- Field work: the researchers met the participants and explained the aims of the study to them. Pre-test was carried out before the implementation of the program to assess the participants’ knowledge, attitude and practice. Finally, the post-test was executed to evaluate the gained knowledge and attitude regarding DR after the educational program. Responses were obtained through face-to-face interview after full explanation of the study. The program was conducted in the period from the beginning of first of August 2017, until the end of January 2018. The work was conducted three days per week with an average of 4–5 patients/day. The interview time ranged between 20–30 mins.
Ethical considerations
The protocol of this study was approved by the ethical committee of the Faculty of Nursing, Assiut University. Verbal informed consent was obtained from all participants and approved by the ethical committee of the Faculty of Nursing, Assiut University and this study was conducted in accordance with the Declaration of Helsinki. Study subjects’ privacy and confidentiality were considered during collection of the data. Participants had the right to withdraw from the study at any time and without any rationale.
Statistical analysis
Data entry and data analysis were carried out using IBM-SPSS version 21. To prepare the data for analysis, basic statistics were calculated (frequencies, cross-tabulation, and histogram). Frequency tables were examined to explore missing data, errors in the data, and data consistency. Missing data in the dependent variables (KAP scores) were treated by replacing the missing value with median values. Data were presented as mean, standard deviation frequencies and percentages. Chi-square test was used to compare the difference in distribution of frequencies among different groups. For continuous variables; independent t-test analysis was carried out to compare the means of normally distributed data. For repeated measures; paired t-test analysis was used. After adding age and sex as a priori correlates, clinical and demographic factors with proven statistical significance from the univariate analyses were further included in the multivariate linear regression models. A p-value ≤0.05 was considered statistically significant.
Results
The current study recruited 200 diabetic patients. Baseline demographic and clinical characteristics of study group were illustrated in Table 1. The mean age of study group was 63.2±3.9 years. Regarding sex, females represented 84.5% of the study group. Most of studied sample were from rural area 78.5%. Also, regarding the level of education, 74% of participants was illiterate. Regarding oral contraceptive use, 43.0% of the study group used them. Also, regarding family history of DM, this table revealed that 48.0% had history of DM in study group. Moreover, 39.5% had past history of chronic disease in the study group.
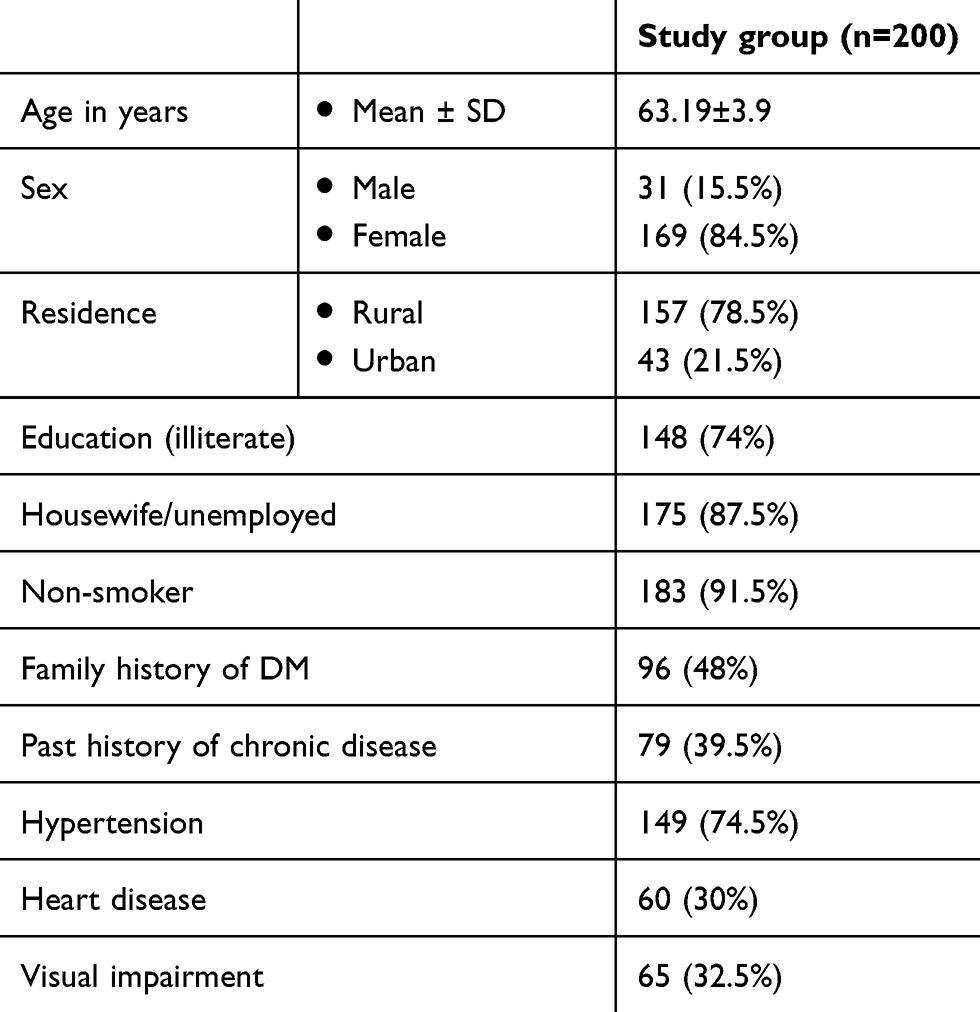 |
Table 1 Baseline demographic and clinical characteristics of study group |
About 63.0% of studied group suffered from DM type 2, as shown in Table 2. In regard to blood glucose level, it was 273.39±85.1 in study group. BMI was 31.28±11.4 in study group. Slightly half of the participated were measured blood glucose within 1 month. More than one third of study group had reported practices regarding eye exams. Within one year. Regarding consulting eye specialists, 60% of study group were going to ophthalmologists. Only 11.1% of patients said that they checked their blood glucose regularly. The majority of participants had low knowledge score and attitude score in the pre-test (5.3±1.0 and 15.08±2.1), which significantly improved in the post-test (16.7±1.8 and 16.18±1.4) respectively, with p-value <0.001, as shown in Table 3. Also, practice score in pretest was 13.83±0.7.
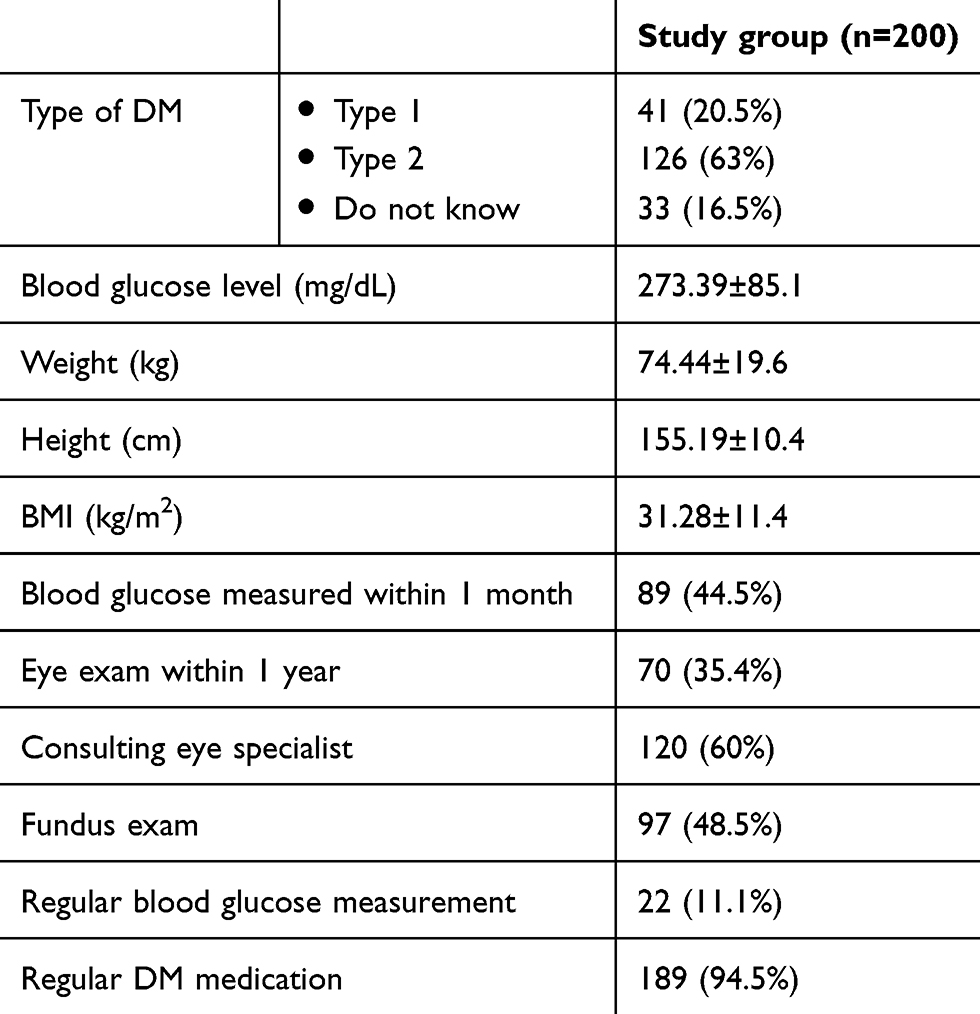 |
Table 2 Clinical characteristics of study group |
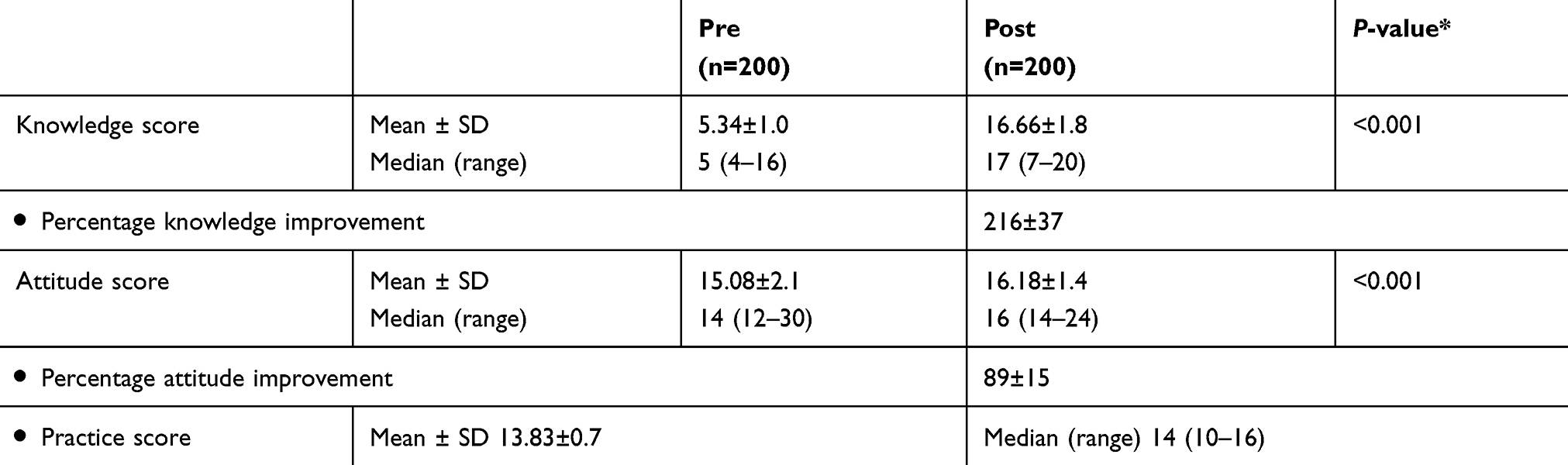 |
Table 3 Mean awareness scores among study group (pre vs post) |
Table 4 showed the multivariate linear regression analysis of the significant factors affecting DR. After adjusting for age, the final linear regression model contained seven predictors; age, sex, education, family history of DM, family history of DR, hypertension, and weight (kg). In other words, the intercept (knowledge score) was 8.41 (6.65: 10.17) after adjusting for all correlates (p<0.001). Moreover, age, education level, FH of diabetes, FH of diabetic retinopathy, hypertension, and weight (kg) were significantly associated with DR. Unadjusted analysis showed no significant association between knowledge score and gender. Regarding the intercept, attitude score was 21.17 (16.81: 25.54) after adjusting for all correlates (p<0.001). Age, residence, and smoking were significantly associated with DR. Unadjusted analysis showed no significant association between attitude score and gender. Finally, the intercept (practice score) was 13.37 (12.49: 14.26) after adjusting for all correlates (p<0.001). Also, blood glucose level, regular blood glucose measurement, and regular DM medication were significantly associated with DR.
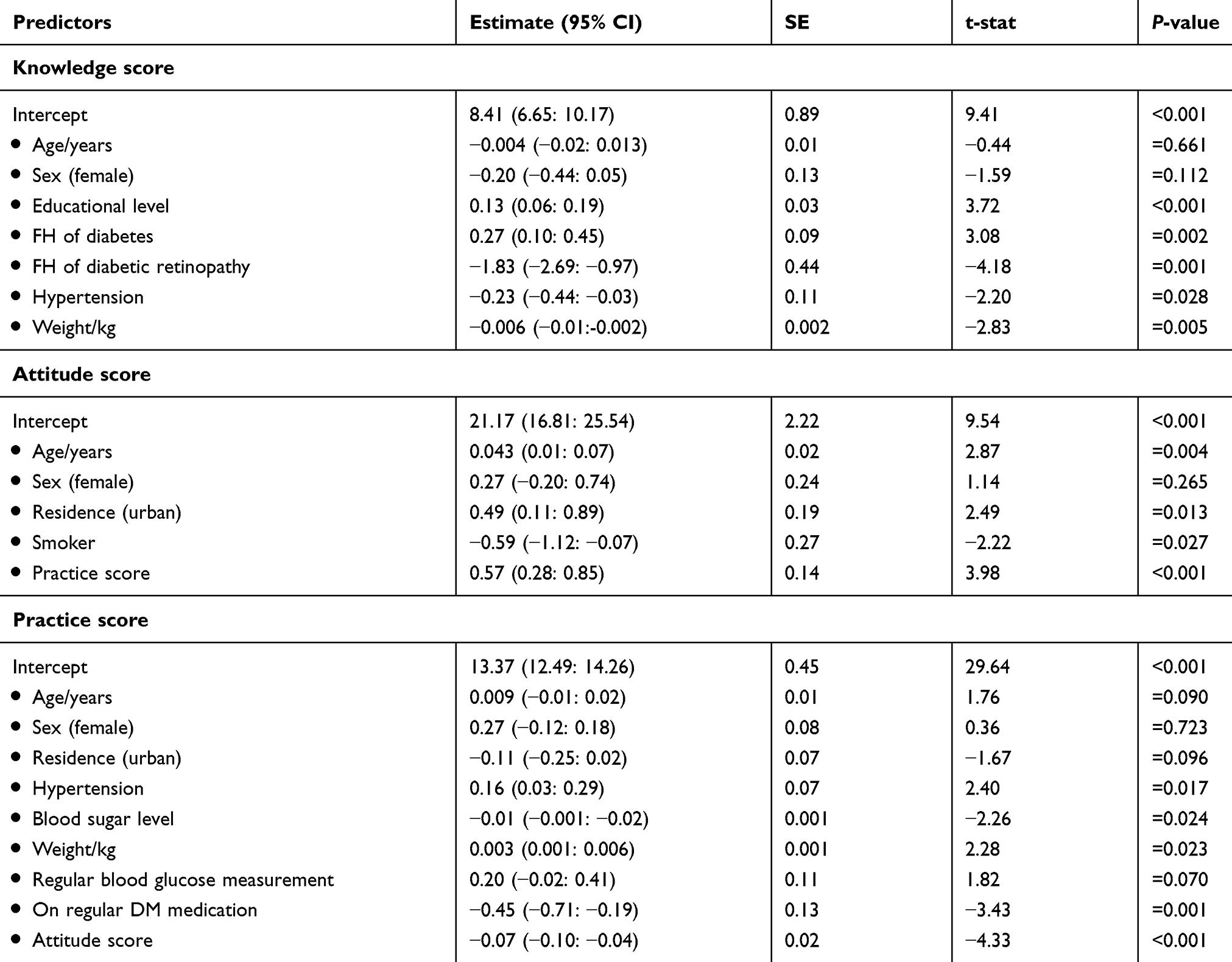 |
Table 4 Multiple linear regression analyses of KAP scores predictors |
Table 5 shows statistically significant differences between knowledge score and education, family history of DM, and hypertension for studied sample. Also, there was a statistically significant difference between attitude score and residence and smoking. Moreover, there were statistically significant differences between practice score and hypertension and regular blood sugar. It was found that there was no statistically significant difference between practice score and regular DM medication.
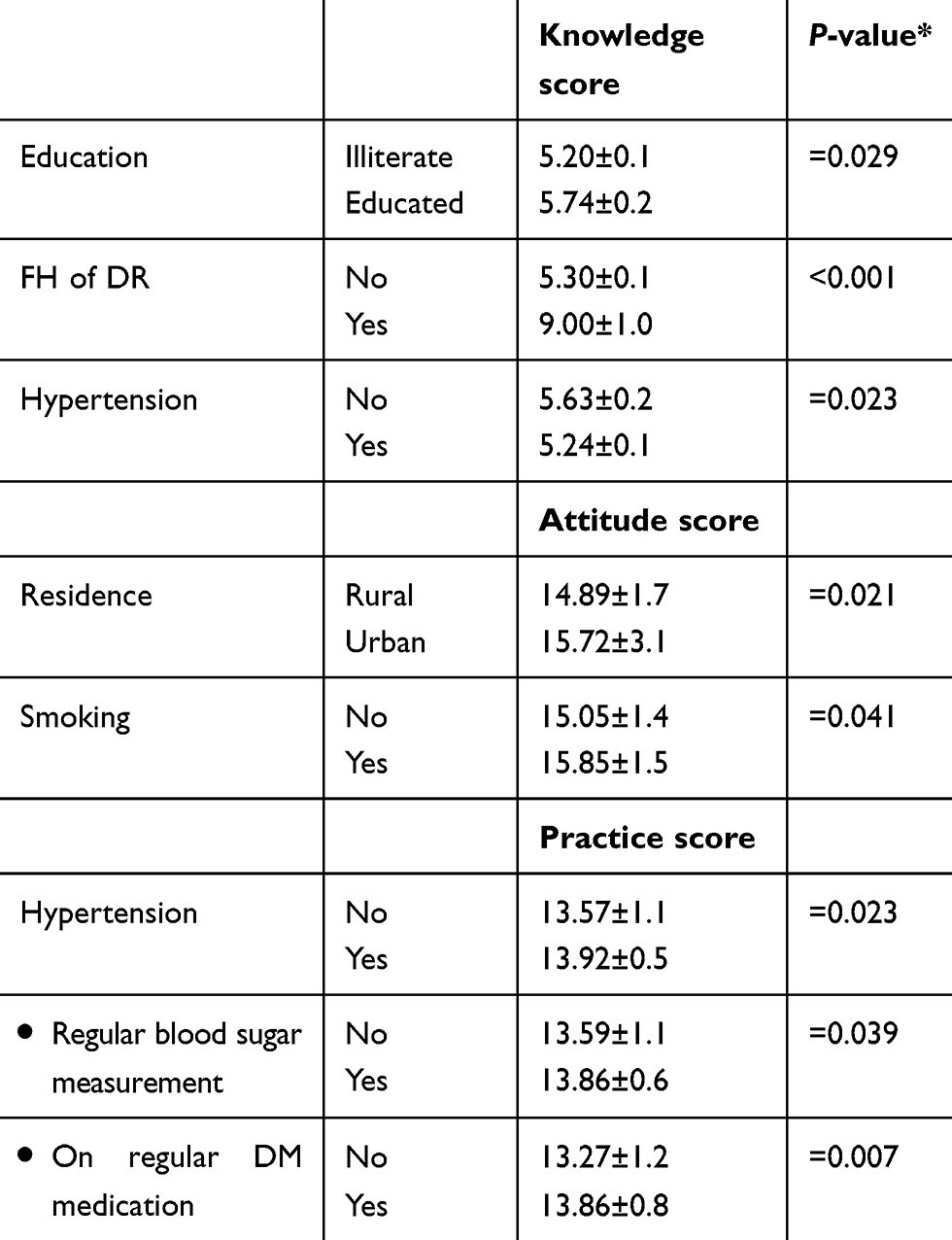 |
Table 5 Significant KAP score correlates among the study group |
Discussion
Patients with diabetes are at risk of eye complications, such as corneal abnormalities, glaucoma, iris revascularization, cataract, and DR, which affects the blood vessels of the retina and leads to blindness.19–22 The present study represented a trial to assess knowledge, attitudes, and practices regarding DR. Also, it implemented and evaluated the effect of educational program about diabetic retinopathy among diabetic patients.
The current study showed that the mean age was 63.2±3.9 years, 74% were illiterate and 84.5% were females. The higher number of female respondents is probably because the health seeking behaviors of females tend to be better than males, and this may explain the larger population of females in this study. The current study agreed with Prabhu M et al23 who found that the mean age was 57.1 years, and that 68% were literate, but most respondents (62%) were males. The study indicates that 48% of study group had family history of DM. This matched Giloyan A et alșs work24 which reported that more than half of their sample had family history of DM.
In the current results hypertension was the most prevalent chronic condition, with 74.5% of the study group suffering from it. Heart disease was reported by 30% of them. This was in agreement with Giloyan A et al24 who found that 66.3% of participants had hypertension and 43.3% of them had heart disease, which indicates that hypertension is the important risk factor for progression of DR.25
In light of results of the current study; 16.5% of the study group did not know the type of diabetes they had. Among those who knew, 20.5% had type 1, and 63% had type 2 diabetes. This finding was not in line with Giloyan A et al24 who found that about 62.9% of participants did not know the type of diabetes they were suffering from, while only 2.9% of them knew they had type 1, and 34.2% had type 2 diabetes. This is probably related to the level of education of the study population and the level of awareness about diabetes.
Furthermore, about half of the studied group was obese, with BMI 31.3kg/m2. These results were in agreement with Cheung N and Wong TY26 who reported that there many eye diseases have been linked with obesity, such as cataract, glaucoma, and diabetic retinopathy. However, this observation disagreed with Shih IM et al27 who found that BMI of participants was 25.8±3.9kg/m2.
The results of the present study disclosed that only 11.1% of participants measured their blood glucose regularly. This might be attributed to the fact that participants lacked information about necessary details such as importance of measuring blood sugar persistently. This result is similar to that reported by the study conducted by Balasubramaniyan N et al,28 who studied awareness and practices of eye effects among people with diabetes in rural India, who reported that 88.6% tested their blood sugar at least once every three months.
In the present study, 60% of studied sample consulted eye specialists and 35.4% of them had eye examinations at least within one year. This could be explained by the fact that patients were aware of the effect of DM on their eyes. The study agreed with Mwangi MW et al,29 who reported that 50% of all the respondents went for eye checkups. Of the 50% who went for eye checkups, 27% of them went once a year. Also, it agrees with Al Zarea BK,12 who observed that about 95% of all the participants went for regular ocular examinations. However, the results disagreed with those of Prabhu M et al,23 who reported that only 16.5% of diabetic patients were referred for an eye examination by their physicians.
Regarding mean score of knowledge of the studied population; 5.34±1.0 in pre-test, which indicated poor knowledge, improved in post-test to 16.66±1.8, this result was similar to that of Srinivasan NK et al,16 who observed that only 4.5% of studied sample had good knowledge about retinopathy. Also, Geethadevi M et al30 found that 60.8% had no knowledge of diabetic retinopathy and Panigrahi S et al31 reported that 69.0% of the study population had poor knowledge of diabetic retinopathy. This implies that a significant proportion of diabetic patients have poor knowledge of diabetic DR and that there is a need for educational program about DR.32
Concerning the relation between participants’ knowledge in pre/post tests and socio-demographic characteristics, these results revealed the lowest mean knowledge score 5.20±0.1 was seen in illiterate respondents while in educated respondents it was 5.74±0.2 and became 16.56±1.8 and 16.69±1.8 respectively in post-test, with a statistically significant relation of p-value <0.001. This further supports the proposition that education is important in creating awareness and education has a significant role in improving patients’ information.
These data are in line with Memon MS et al9 who reported that lowest mean knowledge score (5.28±6.09) was seen in illiterate respondents. Also, the current finding agrees with Seneviratne B and Prathapan S32 who found that a significant association between the level of knowledge and educational level of the spouse too was a significant factor (P<0.05). The participants who had a family history of diabetes had a mean knowledge score in pre-test of 9.00±1.0, which was better than participants without family history of diabetes (5.30±0.1) but in post-test (16.65±1.8 and 17.00±0.0 respectively) with statistically significant relation p-value <0.001.
Also, patients who had history of hypertension had a mean knowledge score in pre-test was higher (5.63±0.2) in non-hypertensive respondents as compared with hypertensive respondents (5.24±0.1) while in post-test (16.73±1.6 and 16.63±1.7 respectively) with p<0.001.
The overall mean score of attitude regarding diabetic retinopathy was 15.08±2.1 in pre-test, while it was 16.218.4 in post-test. It was higher (15.723.1) in urban participants versus rural participants (14.891.7) with p=0.021. It might be attributed to the fact that health services are more available in urban than in rural areas, and differences between rural and urban cultures also play a role.31 Panigrahi S et al reported that the mean attitude score was 15.93±0.09. No statistically significant difference was found in the attitude score among studied sample from urban and rural background.31
This was not congruent with Memon MS et al9 who observed that total mean score of attitudes toward diabetes was 5.43±2.57. It was higher (6.62±2.03) in diabetic respondents as compared with non-diabetic respondents (4.70±2.59) with p<0.000. In light of results of the current study; the mean practice score was 13.83±0.7. This was in agreement with Panigrahi S et al31 who observed that the mean practice score was 12.47±0.32 and explained this by the fact that most of the diabetic patients had the wrong concept, that they should undergo ocular examination only when their vision got affected. The bivariate logistic regression in current study showed that age, education level, family history of diabetes, family history of diabetic retinopathy, hypertension and weight/kg were significantly associated with DR. Unadjusted analysis showed no significant association between DR and gender.
Recommendations
- Application of comprehensive health education programs about DR and the importance of eye examination through different mass media, especially T.V and community leaders.
- Government, through its public insurance plan, should implement an efficient screening program among high-risk individuals, especially adults who are overweight and obese with positive family history of diabetes.
- The concept of early diagnosis and management of diabetes complications should be introduced in primary health care, especially for DR, neuropathy, and nephropathy.
Strengths and limitations
The current study had several strengths; it used random sample technique for patient recruitment, sample size based on power calculation and compensation for dropouts. However, several limitations were identified; using lengthy questionnaire and using quasi-experimental design (pretest-posttest).
Conclusion
The mean knowledge score of the studied population about diabetic retinopathy was 5.34±1.0 in pre-test, while it became 16.66±1.8 in post-test. Also, there was a statistically significant relation between educational level and mean knowledge score.
Acknowledgments
The researchers would like to acknowledge the support of Assiut University Hospital and experts who helped in reviewing the tools, and express deep thanks to all patients who participated in the study and aided in accomplishing this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bui HDT, Jing X, Lu R, et al. Prevalence of and factors related to microvascular complications in patients with type 2 diabetes mellitus in Tianjin, China: a cross-sectional study. Ann Transl Med. 2019;7(14):325. doi:10.21037/atm.2019.06.08
2. Hetta HF, Fahmy EM, Mohamed GA, et al. Does vitamin D status correlate with insulin resistance in obese prediabetic patients? An Egyptian multicenter study. Diabetes Metab Syndr. 2019;13(5):2813–2817. doi:10.1016/j.dsx.2019.07.043
3. Zahran AM, Sayed SK, El Hafeez HAA, Khalifa WA, Mohamed NA, Hetta HF. Circulating microparticle subpopulation in metabolic syndrome: relation to oxidative stress and coagulation markers. Diabetes Metab Syndr Obes. 2019;12:485. doi:10.2147/DMSO.S191750
4. Abd Ellah NH, Ahmed EA, Abd-Ellatief RB, Ali MF, Zahran AM, Hetta HF. Metoclopramide nanoparticles modulate immune response in a diabetic rat model: association with regulatory T cells and proinflammatory cytokines. Int J Nanomedicine. 2019;14:2383–2395. doi:10.2147/IJN.S196842
5. Olokoba L, Mahmud O, Adepoju F, Olokoba A. Awareness of diabetic retinopathy among patients with diabetes mellitus in Ilorin, Nigeria. Sudan J Med Sci. 2017;12(2):89–100. doi:10.18502/sjms.v12i2.919
6. Hetta HF, Mohamed GA, Gaber MA, et al. Visfatin serum levels in obese type 2 diabetic patients: relation to proinflammatory cytokines and insulin resistance. Egypt J Immunol. 2018;25(2):141–151.
7. El-Deeb T, Bakkar S, Eltoony L, et al. The adipokine chemerin and fetuin-A serum levels in type 2 diabetes mellitus: relation to obesity and inflammatory markers. Egypt J Immunol. 2018;25(1):191–202.
8. World Health Organization. Visual Impairment and Blindness Fact Sheet N°282; 2014.
9. Memon MS, Shaikh SA, Shaikh AR, Fahim MF, Mumtaz SN, Ahmed N. An assessment of knowledge, attitude and practices (KAP) towards diabetes and diabetic retinopathy in a suburban town of Karachi. Pak J Med Sci. 2015;31(1):183.
10. Li X, Wang Z. Prevalence and incidence of retinopathy in elderly diabetic patients receiving early diagnosis and treatment. Exp Ther Med. 2013;5(5):1393–1396. doi:10.3892/etm.2013.1021
11. World Health Organization. Prevention of Blindness from Diabetes Mellitus: Report of a WHO Consultation in Geneva, Switzerland.
12. Al Zarea BK. Knowledge, attitude and practice of diabetic retinopathy amongst the diabetic patients of AlJouf and Hail Province of Saudi Arabia. J Clin Diagn Res. 2016;10(5):NC05.
13. American Optometric Association. Diabetic Retinopathy, St. Louis, MO: American Optometric Association; 2017. Available from: https://www.aoa.org/patients-and-public/eye-and-vision-problems/glossary-of-eye-and-vision-conditions/diabetic-retinopathy. Accessed April 15, 2019.
14. Katulanda P, Ranasinghe P, Jayawardena R. Prevalence of retinopathy among adults with self-reported diabetes mellitus: the Sri Lanka diabetes and Cardiovascular Study. BMC Ophthalmol. 2014;14(1):100. doi:10.1186/1471-2415-14-100
15. Mathew R, Soman M, Nair U. Impact of Single Point Health Education on Improving Awareness of Diabetes Related Eye Diseases; 2009. Available from: https://www.worlddiabetesfoundation.org/files/impact-health-education-awareness-diabetes-related-eye-diseases. Accessed April 15, 2019.
16. Srinivasan NK, John D, Rebekah G, Kujur ES, Paul P, John SS. Diabetes and diabetic retinopathy: Knowledge, Attitude, Practice (KAP) among diabetic patients in a tertiary eye care centre. J Clin Diagn Res. 2017;11(7):Nc01–nc07.
17. Hegazi R, El-Gamal M, Abdel-Hady N, Hamdy O. Epidemiology of and risk factors for type 2 diabetes in Egypt. Ann Glob Health. 2015;81(6):814–820. doi:10.1016/j.aogh.2015.12.011
18. Bowling A. Research Methods in Health. Maidenhead: Open University Press; 2002.
19. AlKot MM, Fahim MM. Early detection of diabetic retinopathy among type 2 diabetic patients in Qaluobia Governorate, Egypt. Menoufia Med J. 2015;28(2):547. doi:10.4103/1110-2098.163916
20. Hetta HF, Elkady A, Morsy KH, Mohamed IS, Ibrahim MA. Serum level of IL17a among cirrhotic hepatitis C virus infected patients with incidence of diabetes mellitus. Egypt J Immunol. 2017;24(1):79–88.
21. Hetta HF, Elkady A, Meshaal AK. TH17/TH1 role in endocrine disorders among chronic HCV infected patients. Int J Curr Microbiol App Sci. 2017;6(8):2542–2551. doi:10.20546/ijcmas
22. Hetta HF, Khairy H, Ismail S. Circulating IL17A and IFN-gamma serum levels in cirrhotic hepatitis C virus infected patients with autoimmune thyroiditis. Int J Curr Microbiol Appl Sci. 2017;6(3):1972–1983. doi:10.20546/ijcmas.2017.603.225
23. Prabhu M, Kakhandaki A, Chandra K. A hospital based study on awareness of diabetic retinopathy in diabetic individuals based on knowledge, attitude and practices in a tier-2 city in South India. Indian J Clin Exp Opthamol. 2015;1(3):159–163. doi:10.5958/2395-1451.2015.00007.4
24. Giloyan A, Harutyunyan T, Petrosyan V. The prevalence of and major risk factors associated with diabetic retinopathy in Gegharkunik province of Armenia: cross-sectional study. BMC Ophthalmol. 2015;15(1):46. doi:10.1186/s12886-015-0032-0
25. El Haddad OA, Saad MK. Prevalence and risk factors for diabetic retinopathy among Omani diabetics. Br J Opthalmol. 1998;82(8):901–906. doi:10.1136/bjo.82.8.901
26. Cheung N, Wong TY. Obesity and eye diseases. Surv Ophthalmol. 2007;52(2):180–195. doi:10.1016/j.survophthal.2006.12.003
27. Shih IM, Mazur MT, Kurman RJ. Gestational Trophoblastic Disease. Sternberg’s Diagnostic Surgical Pathology: Sixth Edition. Wolters Kluwer Health Adis (ESP); 2015.
28. Balasubramaniyan N, Kumar SG, Babu KR, Subitha L. Awareness and practices on eye effects among people with diabetes in rural Tamil Nadu, India. Afr Health Sci. 2016;16(1):210–217. doi:10.4314/ahs.v16i1.28
29. Mwangi MW, Githinji GG, Githinji FW. Knowledge and awareness of diabetic retinopathy amongst diabetic patients in kenyatta national hospital, kenya. Int J Humanit Soc Sci. 2011;1(21):140–146.
30. Geethadevi M, Thampi B, Antony J, Raghavan RR, Sasidharan R, Mohan A. A study of knowledge, attitude and practice in diabetic retinopathy among patients attending a primary health care centre. Int J Res Med Sci. 2018;6:3020. doi:10.18203/2320-6012.ijrms20183637
31. Panigrahi S, Sahu RK, Jali S, Rath B, Pati S, Kerketta M. Knowledge, attitude and practice regarding diabetic retinopathy among medical and nursing students of a tertiary care teaching hospital of Odisha: a cross sectional study. IOSR J Dent Med Sci. 2017;16:1–7. doi:10.9790/0853-1607010106
32. Seneviratne B, Prathapan S. Knowledge on Diabetic Retinopathy among Diabetes Mellitus Patients Attending the Colombo South Teaching Hospital, Sri Lanka. Journal of US-China Medical Science. 2016;13:35–46. doi:10.17265/1548-6648/2016.01.005
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.