Back to Journals » Patient Preference and Adherence » Volume 15
Do Women Enrolled in PMTCT Understand the Recommendations: A Case Study from Kilimanjaro
Authors Philemon RN ![]() , Mmbaga BT
, Mmbaga BT ![]() , Bartlett J, Renju J, Mtuy T, Mboya IB
, Bartlett J, Renju J, Mtuy T, Mboya IB ![]() , Msuya SE
, Msuya SE ![]()
Received 23 February 2021
Accepted for publication 21 April 2021
Published 16 June 2021 Volume 2021:15 Pages 1301—1309
DOI https://doi.org/10.2147/PPA.S307847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Rune N Philemon,1 Blandina T Mmbaga,1,2 John Bartlett,3 Jenny Renju,4,5 Tara Mtuy,4,6 Innocent B Mboya,4,7,8 Sia E Msuya4,7,9
1Department of Pediatrics and Child Health, Kilimanjaro Christian Medical University College (KCMUCo) & Kilimanjaro Christian Medical Centre (KCMC), Moshi, Tanzania; 2Department of Research, Kilimanjaro Clinical Research Institute (KCRI), Moshi, Tanzania; 3Duke Global Health Institute, Duke University, Durham, NC, USA; 4Institute of Public Health, Department of Epidemiology & Biostatistics, Kilimanjaro Christian Medical University College (KCMUCo), Moshi, Tanzania; 5Faculty of Population Health, London School of Hygiene and Tropical Medicine (LSHTM), London, UK; 6Faculty of Public Health and Policy and the Department of Global Health and Development, London School of Hygiene & Tropical Medicine (LSHTM), London, UK; 7Institute of Public Health, Department of Community Health, Kilimanjaro Christian Medical University College (KCMUCo), Moshi, Tanzania; 8School of Mathematics, Statistics & Computer Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa; 9Department of Community Health, Kilimanjaro Christian Medical Centre (KCMC), Moshi, Tanzania
Correspondence: Rune N Philemon
KCMUCo, P.O Box 2240, Moshi, Tanzania
Tel +255 754 389 049
Email [email protected]
Introduction: Prevention of mother-to-child transmission (PMTCT) remains a cornerstone of HIV prevention and control efforts. It is vital that the beneficiaries of PMTCT programs understand PMTCT recommendations, especially since their adherence to recommendations is key to successful PMTCT. There have been several major changes in PMTCT recommendations, and many women have encountered different recommendations. It is plausible that confusion has arisen as to what is currently recommended for successful PMTCT. This confusion can affect adherence to recommendations and hinder PMTCT efforts. However, little is known about how women enrolled in PMTCT understand the recommendations in the context of these frequent changes.
Aim: In this paper, we present our findings regarding how HIV-positive women enrolled in PMTCT in Kilimanjaro understand PMTCT recommendations pertinent to them.
Methods: From August 2019 to April 2020, we surveyed 521 mothers enrolled in PMTCT in seven districts in the Kilimanjaro region, Northern Tanzania. A pretested questionnaire was administered to consenting mothers. The questionnaire collected information on mothers’ demographic characteristics, previous encounters with PMTCT, and knowledge of various PMTCT program elements, including medication duration, breastfeeding recommendations and infant HIV testing schedule. A logistic regression model was used to determine factors associated with good PMTCT knowledge among mothers.
Results: A total of 521 women were enrolled, the median score for the 19 items used to assess knowledge was 57.9%, and 64.9% scored above the median. Counselling on ART (OR=2.17, 95% CI 1.08– 4.36) and counselling on breastfeeding during the ANC visits (OR=2.38, 95% CI 1.38– 4.11) were the only factors that we found to be significantly associated with higher odds of good knowledge of PMTCT.
Conclusion: Even amongst mothers enrolled in PMTCT, poor understanding regarding key PMTCT recommendations prevails. There is a need to reassess the training modalities and look at ways to reinforce PMTCT messages to mothers.
Keywords: PMTCT knowledge, PMTCT recommendations, mother’s knowledge, understanding PMTCT
Introduction
The World Health Organization launched option B+ in 2012 as a new approach in the prevention of mother-to-child transmission (PMTCT) of Human Immunodeficiency Virus (HIV). The main aim of this new approach was simplification and harmonization of treatment.1,2 Prior to Option B+, there have been a number of PMTCT guidelines from WHO, and these have included wildly varying information. This can be exemplified by the initial recommendations emphasizing breastfeeding avoidance, where option B+ emphasizes breastfeeding support for at least one year.
Tanzania adopted Option B+ in September 2013, and it has since been the main approach to PMTCT.3 It helped Tanzania be one of the 22 countries in the Global Plan, aiming to eliminate new infections in children and protect mothers.4 Although the Global Plan had great successes, Tanzania’s target of having <5% mother-to-child transmission (MTCT) by 2020 was not achieved. By 2019, MTCT of HIV in Tanzania was at 10.7%.5,6
Amongst the lessons that were hailed as essential to be carried on from the Global Plan was the participation and involvement of HIV-positive mothers in all matters pertaining to the response to the HIV epidemic. This was seen as one of the key elements behind the Global Plan’s success in lowering MTCT.5 The inadequate number of healthcare personnel in most developing countries has led to insufficient interaction of mothers and providers. This detracts from the PMTCT experiences of mothers.7
With the interaction gap between mothers and health workers in PMTCT, HIV-positive mothers, whether peers in the clinic or expert patients remain a crucial source of information and influencer of practice, particularly amongst newly diagnosed HIV positive mothers.8,9 It is important that these influencers, particularly mothers enrolled in PMTCT, have knowledge that is current as according to the health belief model, this will likely favor their adherence.10,11 The health belief model proposes that people will take action toward health goals if they are aware of the benefits, requirements and perceived control.12 Applied to PMTCT, if mothers are aware of the benefits of the various steps in PMTCT, they are more likely to take steps towards adherence to the PMTCT recommendations.
Tanzania has developed guidelines for PMTCT that outline the services and counselling steps mothers should receive from healthcare workers.13 However, the evolution of PMTCT recommendations over the years, particularly regarding breastfeeding, has led to misconceptions amongst mothers, which has bred distrust of the recommendations and non-adherence to them.14 The level of knowledge regarding various elements of PMTCT is low in many countries, including Tanzania.15–17 Some elements, such as points of transmission, appear to be well known to mothers, but others, such as prevention methods, time of child testing, and optimal infant feeding practices, had eluded mothers even before the option B+ era.18–21
We sought to assess the knowledge mothers have regarding the current PMTCT recommendations as understanding the recommendations is the first step towards adhering to them.
Methods
Study Design
This cross-sectional study targeted women enrolled in and attending PMTCT clinics with children less than two years of age. The study was conducted between August 2019 – April 2020. The aim was to gauge the understanding of these women regarding the PMTCT recommendations as they form an important source of information for each other and the community. Their understanding is also a surrogate representation of how well the PMTCT messages are communicated to the beneficiaries. By employing a cross-sectional design, we were able to capture a large number of women who are beneficiaries of the PMTCT program and capture their understanding of the program in an unrehearsed setting.
Study Site and PMTCT Program
The study was conducted in the Kilimanjaro region, Northern Tanzania. The region has seven districts: Siha, Hai, Moshi district council, Moshi municipality, Rombo, Mwanga, and Same. In collaboration with the district medical officer of each of the seven districts in the region, we identified the clinics with the highest PMTCT client load in each district. Participants were then recruited from 37 clinics during their routine clinic visits.
The PMTCT clinics handle pre-natal and post-natal clients and provide PMTCT education to the clients, counselling and testing, and medication to both mothers and children. They also collect blood samples (dry blood spots (DBS) for infant testing using DNA PCR. In the clinics, mothers are meant to be counselled on HIV transmission, prevention of transferring the infection to the child, ART use for the mother and the child, infant feeding, and infant testing schedule.13
In most of the identified clinics, PMTCT clinic operates once a week though some with lower patient load, run once a month and some with a higher patient load run daily. The districts deliberately attempt to synchronize the clinics to run on the same day to facilitate the collection of samples for early infant HIV testing, which is run by zonal laboratories. Though most conduct them on Wednesdays, there are variations due to local influences such as market days. We visited each of the clinics on all their clinic days for one month to ensure we captured as many mothers as possible as most have monthly PMTCT visits. A marker was put on all the patient’s files that had been enrolled to avoid repetition.
Study Population
The information was collected from 521 HIV positive mothers who had children aged below two years, and the children were currently enrolled in PMTCT at any of the selected clinics. We chose post-natal mothers as they would have more exposure to the program and have first-hand experience of more aspects of PMTCT than pre-natal women. Their understanding of PMTCT recommendations could thus serve as a surrogate for whether they have the correct knowledge to communicate to other mothers. All women attending the selected clinics between August 2019 and April 2020 participated in the study.
Study Tool, Users and Content
We developed a questionnaire consisting of seven sections covering socio-demographic characteristics, birth history, HIV history, previous use of antiretroviral therapy (ART) and PMTCT, antenatal care (ANC) and PMTCT attendance in relation to reference child, counselling, and teaching received in PMTCT clinics, and knowledge of key aspects of PMTCT. The resulting English version was translated into Kiswahili and back-translated into English to ensure fidelity. Testing and pretesting was conducted on a sample of 30 women from non-participating clinics until the final tool was approved.
During data collection, the questionnaire was electronically administered in Kiswahili (participant’s national/native language) by trained research assistants using Survey-CTOTM installed on password-secured tablets.
Data Analysis
Data analysis was performed using STATA version 15.1. Numeric variables were summarized using median and categorical variables using frequencies and percentages. Mother’s level of knowledge on PMTCT was assessed using their response to 19 questions. The questions assessed appropriate feeding duration for exclusive breastfeeding and continued breastfeeding, whether a mother can transmit to a child, when transmission occurs, methods for preventing mother-to-child transmission, duration of nevirapine prophylaxis for a new-born child, and frequency of testing for the child. To be classified as being knowledgeable on PMTCT, a mother had to have scored above the median. Comparison of the proportion of mother’s knowledge on PMTCT by participants characteristics was made using Chi-square test. Akaike information criteria (AIC) was used to select the best fitting model, where the model with the lowest AIC was considered the best. The logistic regression model was used to estimate odds ratios (OR) and the corresponding 95% confidence intervals (CI) for factors associated with knowledge on PMTCT.
All analyses were restricted to women who had ever attended ANC during their index pregnancy.
Significant association between explanatory variables and knowledge on PMTCT were evaluated at p<0.05. The variables included in the adjusted analysis were all found to be associated with PMTCT knowledge in previous literature hence were included as potential confounders.
Results
Socio-Demographic and Clinical Characteristics of Study Participants
A total of 521 mothers with children less than 24 months of age enrolled in PMTCT services were included in the study. The women came from a total of 38 clinics across the seven districts of Kilimanjaro region. The mean age of the women was 31.7 years (SD 6.6). Most of the 521 women had primary education (66.2%) and had 1–2 previous pregnancies (92%) while HIV-positive. All women had attended antenatal clinic during their pregnancy with the reference child, and 87.3% reported to have at least four visits as recommended. Of the mothers interviewed, 86.4% reported having received counselling on breastfeeding during their PMTCT visits and 92.1% reported to have been counselled on ART (Table 1).
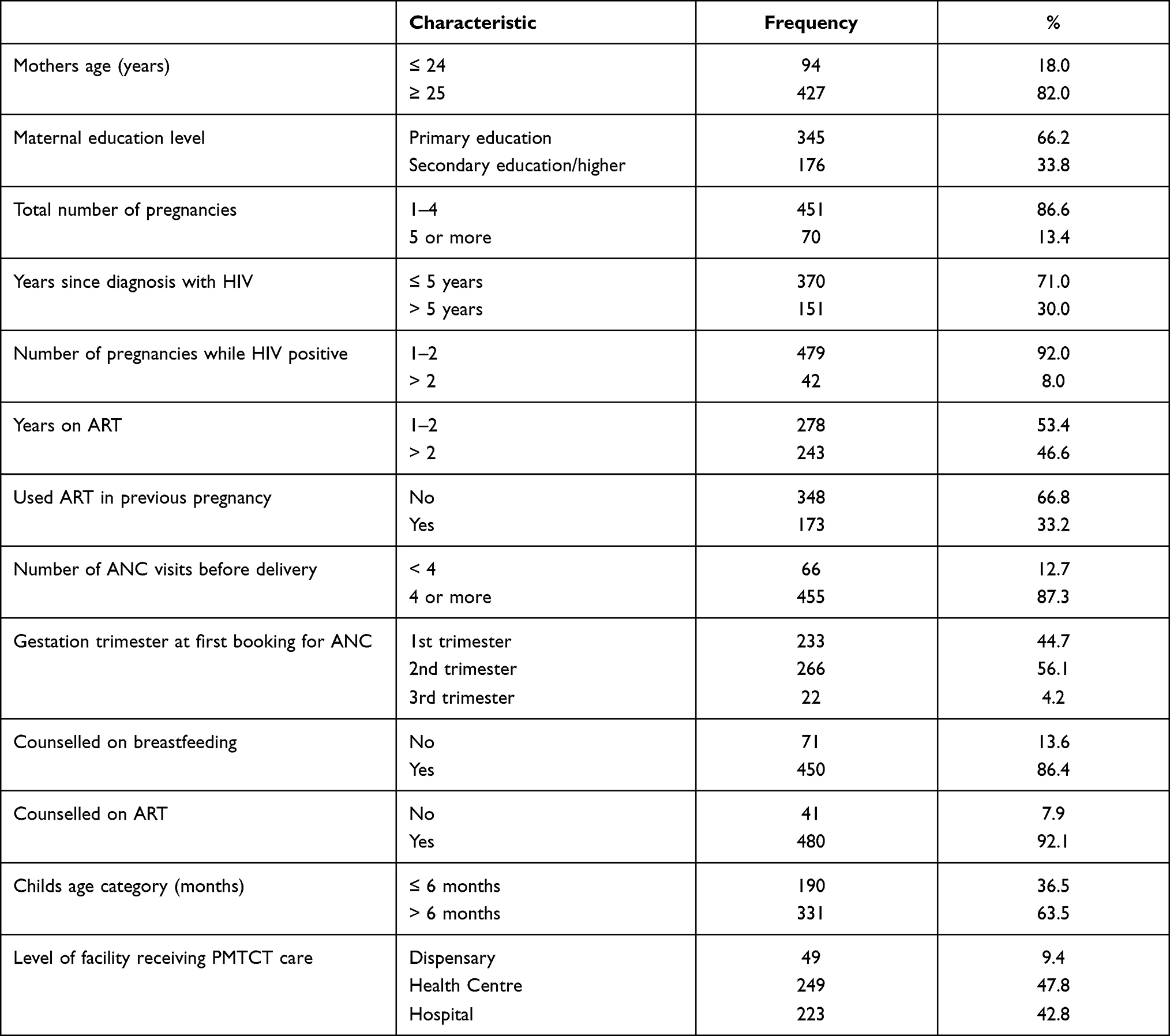 |
Table 1 Socio-Demographic and Clinical Characteristics of Study Participants (N = 521) |
Mothers Knowledge of PMTCT
Of the 19 knowledge items that were used to assess mothers’ knowledge; questions pertaining to ART use in prevention of mother-to-child transmission, testing for early infant diagnosis, alternative feeds for prevention of transmission and the lower risk of transmission in caesarean delivery seem to elude the mothers’ knowledge the most. The median score for knowledge was 57.9%. Overall, 64.9% of mothers scored above the median and were regarded as having good PMTCT knowledge. Only one mother was able to answer all 19 questions correctly (Table 2).
 |
Table 2 Mothers Responses to PMTCT Knowledge Questions (N = 521) |
Factors Associated with Mothers’ Knowledge on PMTCT
The factors associated with mother’s knowledge on PMTCT are shown in Table 3. Several factors appeared to increase mothers’ odds to have better PMTCT knowledge in the crude/unadjusted logistic regression analysis. These included being counselled on breastfeeding (OR=2.96, 95% CI 1.78–4.94) and ART (OR=2.56, 95% CI 1.34–4.87) compared to those who were not. There was also a marginal association between mothers having children aged <6 months (OR=1.45, 95% CI 1.00–2.09) with higher odds of PMTCT knowledge compared to those with children aged ≤6 months and the older (≥25 years) (OR=1.55, 95% CI 0.99–2.45) compared to the younger (<25 years) mothers.
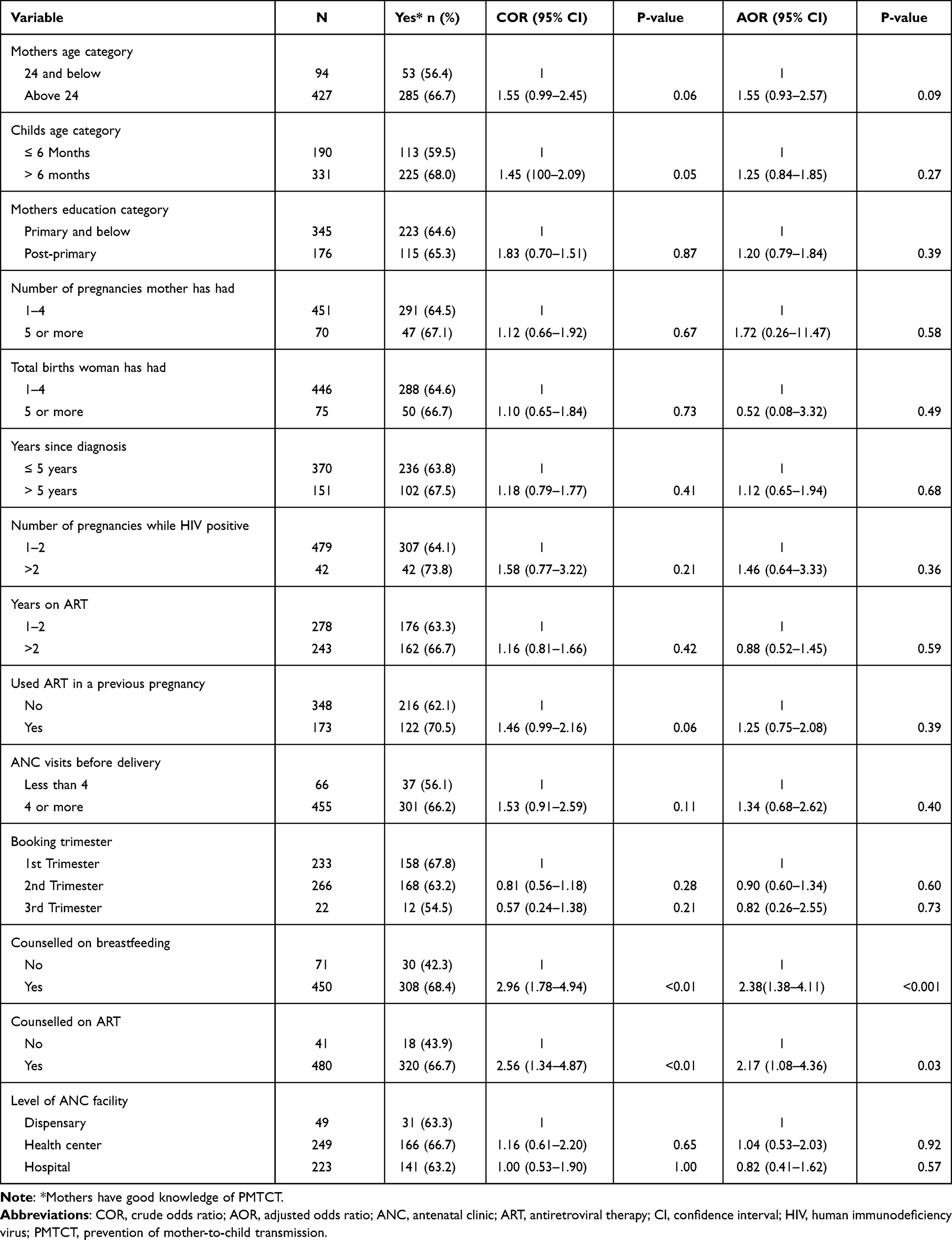 |
Table 3 Factors Associated with Mothers’ Good Knowledge of PMTCT |
After adjusting for the background and clinical characteristics of study participants, only receiving counselling on breastfeeding (OR=2.38, 95% CI 1.38–4.11) and on ART (OR=2.17, 95% CI 1.08–4.36) during PMTCT visits remained significantly associated with higher odds of better PMTCT knowledge than women who were not counselled (Table 3).
Discussion
In our study, there was a total of 521 mothers with children less than 24 months of age enrolled in PMTCT services. Of the socio-demographic and clinical characteristics of the study participants: mean age of the women was 31.7 years, 87.3% had at least four visits with the reference child, 86.4% received counselling on breastfeeding, and 92.1% were on ART during PMTCT visits. Amongst the 19 knowledge items used to assess mothers’ knowledge, 64.9% of mothers scored above the median. Despite several of the factors assessed showing to increase the odds of mothers having better PMTCT knowledge, only counselling on ART and breastfeeding during the PMTCT visits was significantly associated with good knowledge.
In our study, mothers showed varying levels of knowledge regarding different components of PMTCT. In our study, 1 in 5 mothers did not recognize that transmission can occur during the breastfeeding period despite being enrolled in PMTCT. Even higher proportions did not realize that transmission can occur during pregnancy and delivery. Compared to data from the Tanzania HIV Malaria Indicator Survey, our mothers have lower knowledge of transmission during pregnancy and breastfeeding.15 Even though knowledge that transmission can occur during breastfeeding seems to have increased compared to an older study from Kilimanjaro,19 it is still much lower than in Lesotho, where 94% of the mothers recognized the transmission risk in the breastfeeding period.22 In Eswatini, levels of knowledge regarding transmission during breastfeeding were reported to be similar to ours. Still, the Eswatini study respondents seem to be more knowledgeable about the possibility of transmission during pregnancy and delivery.17 It is plausible to think that the failure to recognize the very real risk of transmission during breastfeeding might lead some mothers not to adhere to the recommendations.
Apart from lack of knowledge on time of transmission, nearly a third of HIV-positive women in this setting also had sub-optimal knowledge on the preventive role of ART during pregnancy and breastfeeding, the duration of ART prophylaxis for infants, and the testing schedule for exposed infants. This should be a cause for great concern at the program level. Low uptake of early infant diagnosis (EID) has been linked with low maternal knowledge of PMTCT and EID.23–25 Compounded with these other knowledge gaps, the effect is likely to be more defaulting from the PMTCT cascade and hindrance of the success of the PMTCT program.
There is no universal way for assessing PMTCT knowledge, and there are variations in the questionnaires used in different studies, but we found 64.9% of our mothers had good knowledge. This is similar to a study in Ethiopia which found 61% of mothers had good knowledge using a similar cut off (although with fewer questions).26 Studies from Malawi, Ghana, Uganda and elsewhere in Tanzania have reported lower levels of knowledge (25–35%). This discrepancy could likely be due to the spread of PMTCT messages with time, perhaps more than the differences in assessment methods.18,19,27,28
Compared to a previous study from Dar-es-Salaam, we found a higher proportion of mothers recognized infant prophylaxis as a means for PMTCT (90.6% vs 42.7%).20 However, fewer mothers in our study thought caesarean delivery could be a means for PMTCT (3.6% vs 12.5%). This could be a reflection of the emphasis that has been put on infant prophylaxis in the Option B+ era.
Misconceptions regarding infant feeding durations have also been reported in other studies. Our study found that though most mothers understood the duration of EBF, the total duration of breastfeeding for either HIV-exposed or non-exposed infants eluded them. Chaponda et al in South Africa also found mothers to be lacking in knowledge of the appropriate duration for breastfeeding.20 Dunkley et al attributed the misunderstanding of the feeding recommendations to the changing recommendations over the years.14 Though we did not assess the effect of changing recommendations on child feeding practices, it is possible that it also has a role to play in our setting.
We found counselling on breastfeeding and ART to be significantly associated with having good PMTCT knowledge. This is also affirmed by an older study from Kilimanjaro, which had reported 2.3 higher odds for poor PMTCT knowledge amongst mothers who had not been counselled on breastfeeding.19 Unlike the study by Falnes however, our study did not find any significant association between PMTCT knowledge and maternal age or ANC booking.19
Overall, the level of knowledge regarding PMTCT was low, with most categories having less than 75% of mothers showing low knowledge regarding PMTCT. This is not a unique situation to our setting as low knowledge of PMTCT has previously been reported in mothers enrolled in PMTCT elsewhere.21,30 Liyeh et al in Ethiopia found that women who attended ANC were more likely to be more knowledgeable on PMTCT.21 Our study has gone further to show that it is the counselling that these women receive during their visits that makes the difference in knowledge. We found that though 87.3% of mothers in our study had attended ANC more than four times during their reference pregnancies. However, not all of them had received counselling on ART and breastfeeding, the two factors that showed to be significantly associated with knowledge.
The lack of information on breastfeeding during clinic visits does not seem to be a problem that is unique to our study setting. It has also been reported in Zambia and South Africa amongst other places.29,30 Where enhanced counselling and mentorship on breastfeeding has been tried, overall adherence and knowledge on PMTCT seem to benefit; hence this might be an avenue to explore for our clinics, especially since the link between knowledge and practice is well established.8,31 A study in Cameroon by Egbe et al contrasted our study in that over 98% of their participant had good knowledge on PMTCT, which they attributed to the emphasis on counselling, particularly during the first ANC visit.32
Our study was limited by not looking at how long the mothers had been in PMTCT or who provided them with the counselling during their ANC visits. However, this does not detract from the problem that our findings highlight: mothers enrolled in PMTCT still lack knowledge in key areas of PMTCT, which can lead to non-adherence to the guidelines and influence others to deviate from the guidelines. Those with children older than six months are more likely to have had more exposure to the program, but only 68% could be classified as knowledgeable on PMTCT. This leaves many questions about the mothers’ degree of exposure to health education and counselling in the program.
Conclusions
It is now 20 years since Tanzania started PMTCT services,33 and seven years since we adopted option B+ in PMTCT. Knowledge of mothers regarding PMTCT is still not universal even amongst those in the program, who serve as ambassadors of the program and a source of information for others. This knowledge deficit involves some fundamentals of the program, such as the very real possibility of mother-to-child transmission and the need for ART during pregnancy. These could pose a threat to the success of the PMTCT program. We recommend that counselling be compulsory for all mothers, and perhaps a checklist for counselling be developed to ensure that all mothers have covered pertinent topics for PMTCT during their ANC visits. The rationale of PMTCT and participation of the mothers cannot be overemphasized in this counselling.
Abbreviations
ART, antiretroviral therapy; ANC, antenatal care; DBS, dry blood spots; EID, early infant diagnosis; HIV, human immunodeficiency virus; MTCT, mother-to-child transmission; PMTCT, prevention of mother-to-child transmission.
Data Sharing Statement
Data can be obtained by request from the authors.
Ethics
The study was conducted in accordance to the Helsinki declaration. Permission to conduct this study was obtained from the Kilimanjaro Christian Medical University College Research Ethics Committee (certificate number 2434) and the regional medical officer for Kilimanjaro, and the district medical officer for each of the seven districts. The heads of all the chosen clinics also provided their approval. During their routine clinic visits, the research assistants approached the mothers and asked them to participate in the study. A written informed consent was signed by those who agreed to participate in the study. The interviews were conducted in the privacy of consultation rooms at the clinics.
Acknowledgments
This work was supported through the DELTAS Africa Initiative grant # DEL-15-011 to THRiVE-2. The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS) ’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust grant # 107742/Z/15/Z and the UK government. The views expressed in this publication are those of the author(s) and not necessarily those of AAS, NEPAD Agency, Wellcome Trust or the UK government.
This study was also supported by the United States National Institutes of Health Medical Education Partnership Initiative-Junior Faculty Award D43TW10138.
Dr Bartlett receives salary support from the Duke University Center for AIDS Research P30AI64518.
We also wish to extend our gratitude to the regional medical office for Kilimanjaro, the district medical officers, the facilities where this study took place and all the study participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Dr Rune Philemon reports grants from THRiVe, grants from MEPI, during the conduct of the study. The author reports no other conflicts of interest in this work.
References
1. World Health Organization. Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants 2012. Geneva: World Health Organization; 2012. Available from: https://www.who.int/hiv/pub/mtct/programmatic_update2012/en/.
2. Cichowitz C, Mazuguni F, Minja L, et al. Vulnerable at each step in the PMTCT care cascade: high loss to follow up during pregnancy and the postpartum period in Tanzania. AIDS Behav. 2019;23(7):1824–1832. doi:10.1007/s10461-018-2298-8
3. Kalua T, Tippett Barr BA, Van Oosterhout JJ, et al. Lessons learned from option B+ in the evolution toward “test and start” from Malawi, Cameroon, and the United Republic of Tanzania. J Acquir Immune Defic Syndr. 2017;75(1):S43–S50. doi:10.1097/qai.0000000000001326
4. UNAIDS. Count down to zero 2011. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2011. Available from: https://www.unaids.org/sites/default/files/media_asset/20110609_JC2137_Global-Plan-Elimination-HIV-Children_en_1.pdf.
5. Haroz D, Von Zinkernagel D, Kiragu K. Development and impact of the global plan. J Acquir Immune Defic Syndr. 2017;75(1):S2–S6. doi:10.1097/qai.0000000000001318
6. UNAIDS. Country factsheets United Republic of Tanzania 2019. UNAIDS; 2021. Available from: https://www.unaids.org/en/regionscountries/countries/unitedrepublicoftanzania.
7. Williams SM, Renju J, Moshabela M, Wringe A. Understanding the influence of health systems on women’s experiences of Option B+: a meta-ethnography of qualitative research from Sub-Saharan Africa. Glob Public Health. 2021;16(2):167–185. doi:10.1080/17441692.2020.1851385
8. Hamilton ARL, le Roux KWDP, Young CW, Södergård B. Mentor mothers zithulele: exploring the role of a peer mentorship programme in rural PMTCT care in Zithulele, Eastern Cape, South Africa. Paediatr Int Child Health. 2020;40(1):58–64. doi:10.1080/20469047.2018.1474697
9. Eide KT, Fadnes LT, Engebretsen IMS, et al. Impact of a peer-counselling intervention on breastfeeding practices in different socioeconomic strata: results from the equity analysis of the PROMISE-EBF trial in Uganda. Glob Health Action. 2016;9(1):30578. doi:10.3402/gha.v9.30578
10. Ekubagewargies DT, Mekonnen HS, Siyoum TM. Assessment of knowledge, attitude, and practice of HIV positive mothers on antiretroviral treatment towards infant feeding in Gondar town health institutions, North West Ethiopia, 2017. Int J Pediatr. 2019;2019:1–9. doi:10.1155/2019/9107989
11. Karmacharya C, Cunningham K, Choufani J, Kadiyala S. Grandmothers’ knowledge positively influences maternal knowledge and infant and young child feeding practices. Public Health Nutr. 2017;20(12):2114–2123. doi:10.1017/s1368980017000969
12. Jones CL, Jensen JD, Scherr CL, Brown NR, Christy K, Weaver J. The health belief model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Commun. 2015;30(6):566–576. doi:10.1080/10410236.2013.873363
13. The United Republic of Tanzania ministry of health and social welfare, prevention of mother to child transmission of HIV pocket book; 2012. Available from: https://core.ac.uk/download/pdf/77101826.pdf.
14. Dunkley E, Ashaba S, Burns B, et al. “I beg you … breastfeed the baby, things changed”: infant feeding experiences among Ugandan mothers living with HIV in the context of evolving guidelines to prevent post-natal transmission. BMC Public Health. 2018;18(1). doi:10.1186/s12889-018-5081-x
15. Haile ZT, Teweldeberhan AK, Chertok IRA. Correlates of women’s knowledge of mother-to-child transmission of HIV and its prevention in Tanzania: a Population-Based Study. AIDS Care. 2016;28(1):70–78. doi:10.1080/09540121.2015.1062465
16. Luba TR, Feng Z, Gebremedhin SA, et al. Knowledge about mother–to–child transmission of HIV, its prevention and associated factors among Ethiopian women. J Glob Health. 2017;7(2). doi:10.7189/jogh.07.020414
17. Dlamini P, Mokoboto-Zwane TS. Knowledge, attitudes and practices associated with post-natal PMTCT in breastfeeding mothers living with HIV. Int J Africa Nurs Sci. 2019;11:100150. doi:10.1016/j.ijans.2019.100150
18. Byamugisha R, Tumwine JK, Ndeezi G, Karamagi CA, Tylleskär T. Attitudes to routine HIV counselling and testing, and knowledge about prevention of mother to child transmission of HIV in eastern Uganda: a cross-sectional survey among antenatal attendees. J Int AIDS Soc. 2010;13(1):52. doi:10.1186/1758-2652-13-52
19. Falnes EF, Tylleskär T, Paoli MM, Manongi R, Engebretsen IM. Mothers’ knowledge and utilization of prevention of mother to child transmission services in northern Tanzania. J Int AIDS Soc. 2010;13(1):36. doi:10.1186/1758-2652-13-36
20. Chaponda A, Goon DT, Hoque ME. Infant feeding practices among HIV-positive mothers at Tembisa Hospital, South Africa. Afr J Prim Health Care Fam Med. 2017;9(1). doi:10.4102/phcfm.v9i1.1278
21. Liyeh TM, Cherkose EA, Limenih MA, Yimer TS, Tebeje HD. Knowledge of prevention of mother to child transmission of HIV among women of reproductive age group and associated factors at Mecha district, Northwest Ethiopia. BMC Res Notes. 2020;13(1). doi:10.1186/s13104-020-05005-5
22. Olorunfemi SO, Dudley L. Knowledge, attitude and practice of infant feeding in the first 6 months among HIV-positive mothers at the Queen Mamohato Memorial hospital clinics, Maseru, Lesotho. Afr J Prim Health Care Fam Med. 2018;10(1). doi:10.4102/phcfm.v10i1.1438
23. Bwana VM, Mfinanga SG, Simulundu E, Mboera LEG, Michelo C. Accessibility of early infant diagnostic services by under-5 years and HIV exposed children in Muheza District, North-East Tanzania. Front Public Health. 2018;6:139. doi:10.3389/fpubh.2018.00139
24. Samson S, Mpembeni RN, Njau PF, Kishimba RS. Uptake of early infant diagnosis (EID) at six weeks after cessation of breastfeeding among HIV exposed children: a cross sectional survey at six high volume health facilities in Iringa, Tanzania. J Interv Epidemiol Public Health. 2018;110.
25. Etoori D, Renju J, Reniers G, et al. If the results are negative, they motivate us. Experiences of early infant diagnosis of HIV and engagement in option B+. Glob Public Health. 2021;16(2):186–200. doi:10.1080/17441692.2020.1795220
26. Abebe AM, Kassaw MW, Shewangashaw NE. Level of knowledge about prevention of mother-to-child transmission of HIV option B+ and associated factors among ANC clients in Kombolcha Town, South Wollo Amhara Regional State, Ethiopia, 2017. HIV AIDS. 2020;12:79–86. doi:10.2147/hiv.s242166
27. Boateng D, Kwapong GD, Agyei-Baffour P. Knowledge, perception about antiretroviral therapy (ART) and prevention of mother-to-child-transmission (PMTCT) and adherence to ART among HIV positive women in the Ashanti Region, Ghana: a Cross-Sectional Study. BMC Womens Health. 2013;13(1):2. doi:10.1186/1472-6874-13-2
28. Yeatman S, Trinitapoli J. Awareness and perceived fairness of option B+ in Malawi: a population-level perspective. J Int AIDS Soc. 2017;20(1):21467. doi:10.7448/IAS.20.1.21467
29. Wangwe P, Nyasinde M, Charles D. Effectiveness of counselling at primary health facilities: level of knowledge of antenatal attendee and their attitude on prevention of mother to child transmission of HIV in primary health facilities in Dar es salaam, Tanzania. Afr Health Sci. 2014;14(1):150. doi:10.4314/ahs.v14i1.23
30. Petrovic K, Maimbolwa M, Johansson E. Primiparous mothers’ knowledge about mother-to-child transmission of HIV in Lusaka, Zambia. Midwifery. 2009;25(6):e1–e10. doi:10.1016/j.midw.2007.08.005
31. Rutto NK, Onyango RO, Andang OP, Kishoyian GM. Predictors of exclusive breast feeding among HIV positive mothers in North Rift Region of Western Kenya. Ann Med Health Sci Res. 2019;9.
32. Egbe TO, Tazinya R-MA, Halle-Ekane GE, Egbe E-N, Achidi EA. Estimating HIV incidence during pregnancy and knowledge of prevention of mother-to-child transmission with an Ad Hoc analysis of potential cofactors. J Pregnancy. 2016;2016:1–9. doi:10.1155/2016/7397695
33. Ministry of Health and Social Welfare Tanzania Mainland. Tanzania elimination of mother to child transmission of HIV plan, 2012–2015 (Ministry of Health and Social Welfare Tanzania Mainland); 2012. Available from: https://www.healthpromotiontanzania.org/index.php/en/library122/doc_view/152-costed-emtct-plan-final-16-may-2.html.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.