")
Back to Journals » International Journal of General Medicine » Volume 16
Do We Care Enough About the Presence of Sexual Problems in Diabetic Patients?
Authors Bilen H, Dayanan R , Ciftel E, Bilen A, Ciftel S, Mercantepe F, Capoglu I
Received 30 September 2023
Accepted for publication 28 October 2023
Published 7 November 2023 Volume 2023:16 Pages 5147—5156
DOI https://doi.org/10.2147/IJGM.S441833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Satish Chandrasekhar Nair
Habib Bilen,1 Ramazan Dayanan,2 Enver Ciftel,1 Arzu Bilen,1 Serpil Ciftel,1 Filiz Mercantepe,1 Ilyas Capoglu1
1Faculty of Medicine, Internal Medicine, Endocrinology and Metabolism Department, Atatürk University, Erzurum, Turkey; 2Department of Endocrinology and Metabolism, Batman Training and Research Hospital, Batman, Turkey
Correspondence: Ramazan Dayanan, Department of Endocrinology and Metabolism, Batman Training and Research Hospital, Batman, Turkey, Email [email protected]
Purpose: Sexual health is not only the absence of sexual dysfunction or disability, but also the presence of physical, emotional, mental, and social well-being related to sexuality. The current study aims to determine whether all adult patients who have applied for their regular health check-ups due to diabetes mellitus had ever voluntarily expressed their sexual problems to a specialist and whether they were asked about the presence of sexual dysfunction. It also aims to determine how the physicians attach importance to the issue.
Patients and Methods: All patients aged 18– 65 years with type 1 and type 2 diabetes mellitus, who applied to our hospital between the years of January 2021 and 2022, were questioned by filling out a questionnaire for the presence of sexual problems in addition to screening for chronic complications of diabetes mellitus (retinopathy, nephropathy, and neuropathy) and routine history and physical examination.
Results: The association between the presence of sexual problems and whether patients were questioned about the relevant issue in their previous controls and gender and age factors, educational background, presence of comorbidities, duration of marriage, and microvascular complications of diabetes mellitus were examined. In a population of 595 patients, 53.78% of the patients stated that they had sexual problems; however, 9.91% had been questioned about this issue by the physician. It was observed that 6.3% of female and 15.3% of male patients had previously consulted a doctor voluntarily due to their sexual problems.
Conclusion: This study presents empirical findings that shed light on the inadequacies in healthcare providers’ approach to addressing sexual health concerns among individuals diagnosed with diabetes, as well as the shortcomings in patients’ effective communication of these concerns.
Keywords: sexual problem, diabetes mellitus, care
Introduction
The World Health Organization (WHO) defines health as a state of complete physical, mental, and social well-being.1 Sexual health is not only the absence of sexual dysfunction or disability, but also the presence of physical, emotional, mental, and social well-being related to sexuality.2 Sexuality is an integral part of human life and one of the essential requirements. It is not only an instinctive process, but also a learned process. For this process to be initiated and maintained healthily, it is of great importance that individuals are informed about sexuality and sexual health, as it is one of the most important components of general health.3 Problems related to sexual health threaten general health and make people unhappy. Deterioration of sexual health results in the interruption of physical health and leads to psychosocial and mental health problems as well. Therefore, this situation that impairs the health of the individual also negatively affects the health of the family and society. The difficulty in expressing sexual health problems makes treatment difficult and causes delays in the initiation of therapy.2 Sexual health requires both a positive and respectful approach to sexuality and sexual relationships, enjoyable and safe sexual experiences free from coercion, discrimination, and violence. Sexual health is a significant and positive dimension of personal health for individuals in all age groups.
The prevalence of diabetes is escalating within the realm of global health, impacting an estimated 463 million individuals globally, with projections indicating a surge to 700 million by the year 2045.4 This chronic illness is associated with numerous systemic consequences. Nevertheless, certain adverse symptoms, such as sexual dysfunction, tend to be overlooked or insufficiently addressed.5 The influence of diabetes on sexual well-being can manifest in various manners for both males and females.6 Examples of such disorders include erectile dysfunction, decreased sexual desire, challenges with achieving orgasm, and susceptibility to genital infections.7 Nevertheless, this matter is frequently disregarded or insufficiently tackled by both medical professionals and individuals seeking medical care. The maintenance of sexual health is a crucial component of an individual’s holistic state of well-being, and it holds particular significance for persons who are managing chronic diseases such as diabetes.8 Nonetheless, the present healthcare system exhibits a significant deficiency in acknowledging and addressing the sexual issues faced by individuals with diabetes.
Physicians encounter a diverse range of obstacles while engaging in discussions about sexual health with their patients.9 The problems that individuals may encounter encompass insufficient training and resources, limited time availability, and cultural or personal considerations. The aforementioned scenario presents notable challenges in the identification and management of sexual health issues, resulting in unwarranted reductions in the well-being of individuals with diabetes.
The objective of this study is to investigate the inadequacies of healthcare providers, with a particular focus on diabetes experts, in their approach to addressing the sexual health concerns of individuals with diabetes. The objective of this study is to assess the frequency and depth at which physicians engage in discussions regarding these matters with their patients, identify the obstacles they meet, and examine the incorporation of these topics in the education and training of healthcare professionals. Additionally, the objective of this study is to investigate optimal methodologies within this domain and alternative approaches that may enhance the efficacy of patient-provider communication.
Patients and Methods
The study was conducted according to the ethical standards specified in the 1964 Declaration of Helsinki. Research and publication ethical rules were followed in our study. The written consent form was obtained from all participants.
A study was conducted at Erzurum Atatürk University Endocrinology and Metabolic Diseases Polyclinic to assess the prevalence of sexual problems among patients aged 18–65 diagnosed with type 1 and type 2 diabetes for at least 1 year. The study period spanned from January 2021 to 2022. Participants who reported engaging in sexual activity within the past 6 months were included in the evaluation. A questionnaire comprising relevant inquiries was administered to gather data on sexual problems. The survey employed in the study consisted of 14 questions, which were developed by the authors of the study through modifications of the International Index of Erectile Function (IIEF-EF) and Female Sexual Function Index (FSFI) scales. These modifications were made to align the survey with the sociocultural backgrounds of the participants. The participants underwent assessment with regard to their age, marital status, level of education, occupational status, existence of any concurrent chronic illnesses, duration of marriage, sexual activity status, presence of sexual complaints, and if they sought medical consultation for treatment. Participants were queried regarding whether physicians had inquired about potential sexual issues during prior medical evaluations.7,10 Furthermore, prior to the study, all individuals involved had a thorough screening process to identify any chronic problems associated with diabetes, including retinopathy, nephropathy, and neuropathy. This screening was conducted alongside the standard assessment of medical history and physical examination.
In order to mitigate the potential confounding effects of variables unrelated to diabetes, participants with comorbid health conditions that could potentially affect sexual function, such as psychiatric disorders, were deliberately removed from the study. Simultaneously, the study excluded pregnant women, individuals utilizing medications that may potentially impact sexual function (such as antidepressants, antipsychotics, and high blood pressure medications), as well as individuals who had previously received treatment for sexual dysfunction or experienced significant sexual health issues.
Statistical Analysis
Data were analyzed using SPSS-26 for Windows (Statistical Package for Social Science, SPSS Inc. Chicago IL, USA®Z). Visual (histograms and probability plot) and analytical methods (Kolmogorov–Smirnov test) were used in order to determine whether the variables were normally distributed or not. The continuous variables were expressed as mean and standard deviation. The differences between qualitative/categorical variables such as gender distribution between groups were compared with the chi-square test since the values observed in the cells provided assumptions. The statistically significant two-tailed p-value was considered as <0.05.
Results
A total of 595 patients, 287 (48.2%) females and 308 (51.8%) males, were involved in the study, and the mean age was 51.85±8.16 and 53.43±8.66 for females and males, respectively. Of the total 595 patients, 320 (53.78%) had sexual problems, and the number of those patients was 144 (45%) and 176 (55%) for females and males.
Considering the abovementioned questionnaire, it was observed that 13 of 144 (9%) females and 33 of 176 (18.8%) males with a sexual problem were questioned about the issue. Apart from those, 4 of 143 (2.8%) females and 9 of 132 (6.8%) males without a sexual problem were also questioned. Out of a total patient population of 595, only 9.91% were questioned about sexual problems, and the figures for females and males questioned by the doctor were 28.8% and 71.1%, respectively (Table 1).
 |
Table 1 Frequency of Being Questioned About Sexual Problems in Male and Female Diabetic Patients |
Four of 144 (2.8%) females and 14 of 176 (8%) males answered yes to the question of whether they had received treatment for sexual problems before. On the other hand, 9 of 144 (6.3%) females and 27 of 176 (15.3%) males answered yes to the question of whether they had voluntarily consulted a doctor due to a sexual problem (Table 2). Considering the association between the presence of sexual problems and educational background, no association was found in both females and males (Table 3). Considering the association between the questioning of sexual problems in previous controls and educational background, no association was found in both females and males. The p-values for females and males were p=0.069 and p=0.148, respectively (Table 4).
 |
Table 2 Questions Asked to the Patients with Sexual Problems Based on Gender |
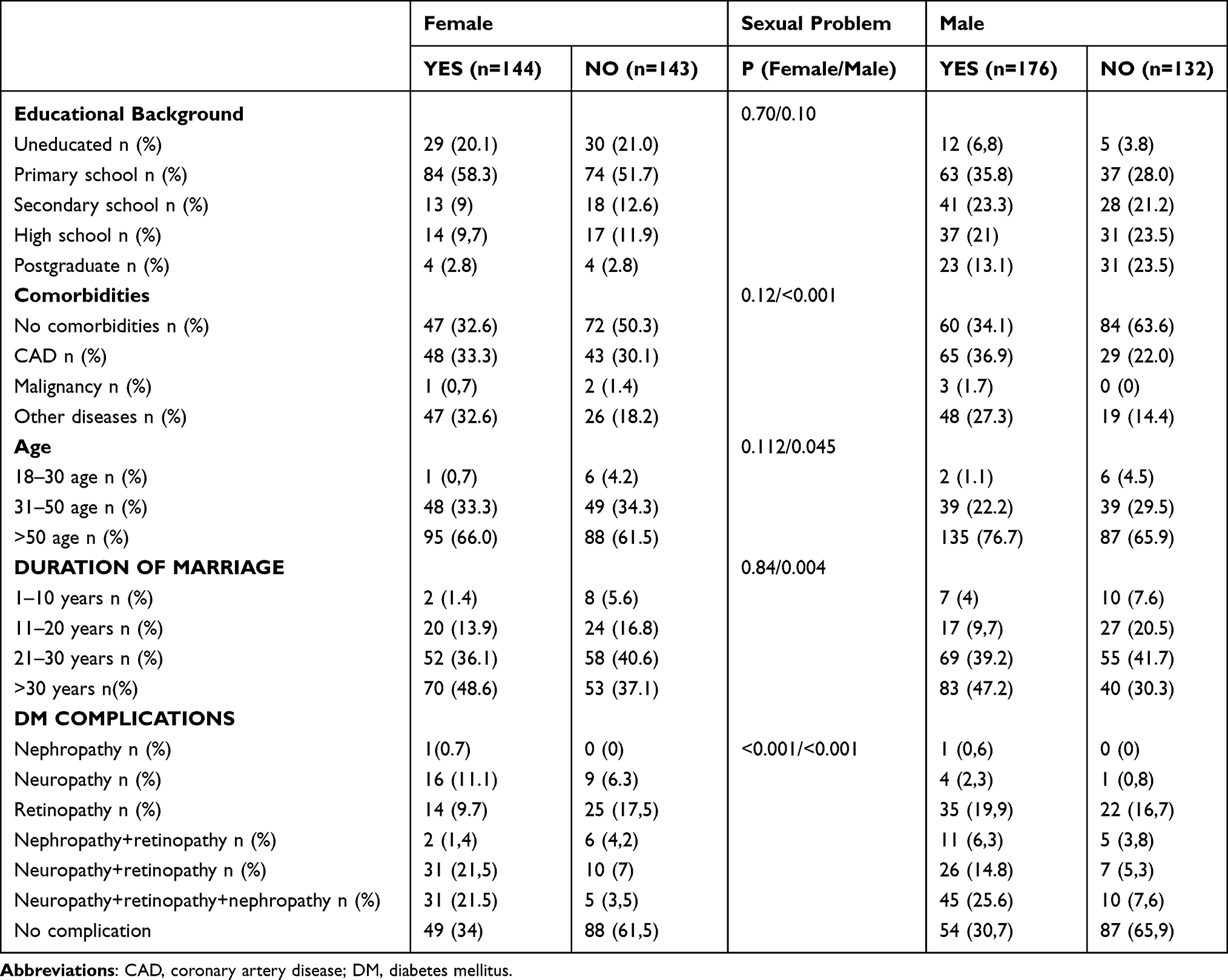 |
Table 3 The Association Between the Presence of Sexual Problems Based on Educational Background, Comorbidities, Age, Duration of Marriage, and Chronic Complications of Diabetes Mellitus Based on Gender |
 |
Table 4 The Association Between the Questioning of Sexual Problems Based on Educational Background, Comorbidities, Age, Duration of Marriage, and Chronic Complications of Diabetes Mellitus Based on Gender |
When the association between sexual problems and comorbidities was analyzed based on gender, 47 of 144 (32.6%) females with sexual problems had no comorbidities, 48 (33.3%) had cardiovascular disease, 1 (0.7%) had malignancy, and 47 (32.6%) had other chronic diseases. On the other hand, when examining the females without sexual problems, the figures were as follows in the above order: 72 of 143 (50.3%), 43 (30.1%), 2 (1.4%), and 26 (18.2%). Considering the males with sexual problems, 60 of 176 (34.1%) had no comorbidities, 65 (36.9%) had cardiovascular disease, 3 (1.7%) had malignancy, and 48 (27.3%) had other chronic diseases, whereas the figures were as follows for 132 males without sexual problems: 84 (63.6%) had no comorbidities, 29 (22%) had cardiovascular disease, 19 (14.4%) had other chronic diseases, and there were no cases with malignancy. While the presence of sexual problems was independent of chronic diseases and comorbidities in females, it was found to be associated with males (p values for females and males, p=0.12, p<0.001, respectively) (Table 3). When examining the association between the questioning of sexual problems in previous controls and comorbidities, no association was found in both females and males. The p-values for females and males were p=0.071 and p=0.694, respectively (Table 4).
One of 144 (0.7%) females with sexual problems was between the ages of 18–30, 48 (33.3%) were between the ages of 31–50, and 95 (66.0%) were over the age of 50, considering the association between the presence of sexual problems and age factor based on gender. However, the figures for 143 females without sexual problems, based on the age range above, were as follows: 6 (4.2%), 49 (34.3%), and 88 (61.5%), respectively. When it comes to males with sexual problems, 2 of 176 (1.1%) were between the ages of 18–30, 39 (22.2%) were between the ages of 31–50, and 135 (76.7%) were over the age of 50. However, the figures for 132 males without sexual problems, based on the age range above, were as follows: 6 (4.5%), 39 (29.5%), and 87 (65.9%), respectively. The presence of sexual problems in males was age-dependent, while it was age-independent in females. The p-values for males and females were p=0.045 and p=0.1, respectively (Table 3).
When the association between the questioning of sexual problems in previous controls and the age factor was analyzed, no association was found for males and females (Table 4). When the association between sexual problems and duration of marriage was analyzed based on gender, the duration of marriage of 144 females with sexual problems was 1–10 years for 2 (1.4%), 11–20 years for 20 (13.9%), 21–30 years for 52 (36.1%), and over 30 years for 70 (48.6%). However, the figures for 143 females without sexual problems were as follows: 8 (5.6%), 24 (16.8%), 58 (40.6%), and 53 (37.1%), respectively. For 176 males with sexual problems, the duration of marriage was 1–10 years in 7 (4%), 11–20 years in 17 (9.7%), 21–30 years in 69 (39.2%), and over 30 years in 83 (47.2%). For 132 males without sexual problems, on the other hand, the figures were 10 (7.6%), 27 (20.5%), 55 (41.7%), and 40 (30.3%), respectively. Sexual problems in males were dependent on the duration of the marriage; however, they were independent in females. The p-values for males and females were p=0.004 and p=0.84, respectively (Table 3).
When the association between the questioning of sexual problems in previous controls and the duration of marriage based on gender was analyzed, no association was found for males and females (Table 4). When the association between sexual problems and microvascular complications of diabetes mellitus was analyzed based on gender, the results were as below for 144 females with sexual problems: 1 (0.7%) had nephropathy, 16 (11.1%) had neuropathy, 14 (9.7%) had retinopathy, 2 (1.4%) had both nephropathy and retinopathy, 31 (21.5%) had both neuropathy and retinopathy, 31 (21.5%) had neuropathy, retinopathy, and nephropathy, and 49 (34%) had no microvascular complications. On the other hand, 9 of 143 (6.3%) females without sexual problems had neuropathy, 25 (17.5%) had retinopathy, 6 (4.2%) had both nephropathy and retinopathy, 10 (7%) had both neuropathy and retinopathy, 5 (3.5%) had neuropathy, retinopathy, and nephropathy, and 88 (61.5%) had no microvascular complications. For 176 males with sexual problems, the figures were as below: 1 (0.6%) had nephropathy, 4 (2.3%) had neuropathy, 35 (19.9%) had retinopathy, 11 (6.3%) had nephropathy and retinopathy, 26 (14.8%) had neuropathy and retinopathy, 45 (25.6%) had neuropathy, retinopathy, and nephropathy, and 54 (30.7%) had no microvascular complications. However, 1 of 132 (0.8%) males without sexual problems had neuropathy, 22 (16.7%) had retinopathy, 5 (3.8%) had nephropathy and retinopathy, 7 (5.3%) had neuropathy and retinopathy, 10 (7.6%) had neuropathy, retinopathy, and nephropathy, and 87 (65.9%) had no microvascular complications. The presence of sexual problems was found to be associated with microvascular complications of diabetes mellitus for both females and males. The p-values for females and males were p<0.001 and p<0.001, respectively (Table 3).
When the association between the questioning about sexual problems in previous controls and microvascular complications of diabetes mellitus based on gender was examined, the fact that there was an association between these parameters in males was found, but no such association was found in females. The p-values for males and females were p=0.009 and p=0.648, respectively (Table 4).
Discussion
This study highlights the inadequacies in the manner in which healthcare professionals inquire about sexual health issues in individuals with diabetes, as well as the challenges faced by patients in effectively communicating these concerns. The literature indicates that there is a notable deficiency in communication regarding this matter, resulting in a substantial barrier to the treatment of sexual health for both healthcare professionals and patients.9
Diabetes has been associated with several consequences, including neuropathy, vascular problems, and hormonal imbalances, all of which have been linked to the development of sexual dysfunction.5 Nevertheless, the findings from our study and the existing literature suggest that there is a lack of regular inquiry by physicians regarding sexual dysfunction in individuals with diabetes. The potential causes for this phenomenon could be attributed to a combination of insufficient training and the sense among medical professionals that this particular subject matter is unsettling.11,12
The current study focused on to what extent sexual problems were expressed by the patient and doctor, rather than investigating the causes of sexual problems in diabetic individuals. The association between the presence of sexual problems and whether patients were questioned about the relevant issue in their previous controls and gender and age factors, educational background, presence of comorbid diseases, duration of marriage, and microvascular complications of diabetes mellitus were examined. In a population of 595 patients, 53.78% of the patients stated that they had sexual problems; however, 9.91% were questioned about this issue by the physician. It was observed that 6.3% of female and 15.3% of male patients had previously consulted a doctor voluntarily due to sexual problems. These figures indicate that, when the patients are not questioned by doctors, they do not tend to mention the presence of their sexual problems.
The presence of sexual health issues among individuals with diabetes can significantly impede the effective management of diabetes and adversely affect their overall quality of life. The presence of sexual dysfunction has the potential to impact an individual’s psychological well-being and interpersonal connections, hence potentially precipitating further health complications such as depression and anxiety.2,13,14 The efficacy of patient questioning approaches is compromised by deficiencies in the sexual health training provided to medical practitioners. Insufficient knowledge among medical practitioners regarding this subject has the potential to impact not only the accuracy of diagnoses and effectiveness of treatments but also the quality of communication with patients, leading to a deficiency in comfort and empathy.9,15 According to the previous study, individuals may exhibit hesitancy in openly communicating their health concerns due to a perceived lack of safety within the healthcare system.2,16 Furthermore, it is imperative to acknowledge that cultural and societal variables play a significant role in exacerbating this phenomenon of misinterpretation.17 Sexuality remains a subject that is often seen as socially unacceptable in numerous societies, leading individuals to refrain from divulging issues related to their sexual well-being.2 Shyness in discussing sexual health issues may arise from factors such as the perception of insignificance attributed to these problems or patients’ apprehension over the willingness of healthcare professionals to address such concerns.18 Furthermore, it is worth noting that certain individuals may exhibit a lack of awareness of the symptoms associated with diabetes or fail to perceive the potential correlation between these symptoms and their condition. Consequently, this lack of recognition may serve as a deterrent, preventing patients from discussing their concerns with healthcare professionals. Furthermore, certain individuals may experience a lack of familiarity with the suitable words or terminology required to articulate their sexual concerns.
The American Diabetes Association (ADA) Diabetes Care, widely used all over the world, recommends screening with serum testosterone levels in the early morning of males with diabetes mellitus who have symptoms or signs of hypogonadism, such as decreased sexual desire or activity or erectile dysfunction.6 It is emphasized that lifestyle management and psychosocial care are the cornerstones of the management of diabetes mellitus, and diabetic individuals should be referred for diabetes self-management education and support, medical nutrition therapy, and the assessment of psychosocial/emotional health problems when indicated.19 It is stated that individuals with diabetes mellitus should receive recommended preventive services (eg, vaccinations and cancer screening), smoking cessation counseling, and ophthalmologic, dental, and podiatric referrals if required. Personal history of complications and common comorbidities, such as obstructive sleep apnoea syndrome (OSAS), non-alcoholic fatty liver disease (NAFLD), obesity, hypertension, macro- and microvascular complications, the presence of anemia and hemoglobinopathy, latest dental visit, and ophthalmologic examination should be assessed at the initial admission, on patient’s follow-up, at annual health check-ups of the patients, and in the components of a comprehensive diabetes medical assessment. It is also recommended to evaluate behavioral factors like eating habits, tobacco, alcohol and substance use, sleep patterns, and physical activity.20 However, the questioning of the presence of sexual problems is not included in the initial admission and follow-up recommendations. This situation suggests that the lack of questioning of the presence of sexual problems in diabetic individuals is widespread worldwide.5,9 We consider that diabetic individuals should be evaluated by the physician in terms of sexual dysfunction at their first visit, subsequent visits, and annual controls. Moreover, the inclusion of these findings in the ADA guideline and all other diabetes guidelines will contribute to increasing the awareness of physicians. It should be emphasized during basic medical education that not only diabetic individuals but also individuals with other diseases in the etiology of sexual dysfunction need to be evaluated for sexual dysfunction at their initial admission and during their follow-ups. The questioning of sexual dysfunction should be reminded in congresses and meetings, and thus doctors will attach importance to the related issue. After this stage, more professional help can be provided to individuals with sexual dysfunction, establishing expert communities in sexual medicine.
Not so interestingly, the findings of our study revealed a notable trend wherein female patients had a decreased propensity to discuss their sexual concerns and were similarly less frequently queried about such matters by medical practitioners. Simultaneously, it is noteworthy that the occurrence of sexual problems in women does not exhibit the same correlation with age as observed in men. Moreover, women with sexual difficulties have the unfortunate circumstance of receiving comparatively less therapy for this issue. The impact of diabetes on sexual well-being can yield substantial ramifications for individuals of both genders.8,17,21 However, according to the available research, it has been observed that women tend to exhibit greater hesitancy in addressing matters related to sexual health, while healthcare providers may display a decreased inclination to engage in discussions on such concerns with their female patients.13,21,22 The potential causes of this phenomenon can be attributed to variations in gender-based communication patterns, societal expectations around gender roles, and the presence of unconscious prejudices within therapeutic settings.22,23 Research has indicated that women may encounter heightened levels of stigmatization about disclosing personal health matters, particularly those about sexual health.22,24 In certain societal contexts, there exists an expectation for women to maintain a state of silence regarding matters about sexuality. Consequently, women may exhibit a reluctance to openly communicate their experiences of sexual dysfunction. According to a study conducted by Shifren et al,25,26 there exists evidence suggesting that healthcare personnel may exhibit a reduced inclination or level of comfort when it comes to addressing women’s sexual health concerns, in comparison to their male counterparts. The potential reasons for this phenomenon include the training of clinicians, misunderstandings, or the intention to prioritize patient comfort. Moreover, it has been shown that the manifestation of sexual dysfunction symptoms may be comparatively milder in women as compared to men, as noted in previous studies.13,21 In the male population, issues such as erectile dysfunction tend to manifest more prominently with observable physical symptoms.27,28 Conversely, female sexual dysfunction often entails a blend of psychological and physiological symptoms, rendering its identification a challenging task.22 Therefore, it is imperative to acknowledge the sexual health challenges encountered by women living with diabetes, since this recognition can foster a greater willingness among healthcare professionals and patients to openly address these concerns. In order to attain a comprehensive enhancement in the treatment of diabetes and a corresponding improvement in the quality of life for patients, it is imperative to surmount the obstacles currently faced.14,29,30
The results of this study suggest that there is a need for a more comprehensive integration of sexual health issues into the training of healthcare workers. The prioritization of training programs should be centered on imparting strategies to physicians that enhance their ability to engage in discussions about these matters with greater comfort and efficacy. Furthermore, it is imperative to ensure that patients are adequately informed about matters about sexual health and are actively encouraged to engage in open discussions on these concerns with their healthcare providers.
The integration of sexual health evaluations within conventional diabetes management protocols is imperative for healthcare systems, necessitating a multidisciplinary approach. The proposed approach entails the establishment of a collaborative framework including experts from several disciplines, including endocrinology, cardiology, psychology, and sexual therapy. The inadequacies in addressing sexual health issues among individuals with diabetes necessitate attention and intervention at both the individual and systemic levels. The integration of education, communication, and multidisciplinary teamwork is vital in addressing this crucial matter. The prioritization of future research should be on the assessment of the efficacy of therapies in this domain and its potential ramifications on the quality of life experienced by patients.
Limitations
One of the limitations of the study pertains to the absence of a specific scale employed to operationalize sexual dysfunction. Additionally, another problem is the study’s single-center and cross-sectional design.
Conclusion
Sexual dysfunction in diabetic patients is an often-overlooked complication despite the high impact on life quality. In the present study, it was observed that diabetic individuals had voluntarily expressed their sexual problems at a very low rate and had been questioned by very few physicians about the presence of sexual problems in their previous controls. We consider that more comprehensive multicenter studies conducted throughout the world are required on this issue. Moreover, further regulations should be made in the guidelines regarding the questioning of patients in terms of sexual dysfunction at the time of initial admission and in subsequent controls.
Ethical Approval
This study was approved by the Research Ethics Committee of Medical Faculty, Erzurum Atatürk University (Number: B.30.2.ATA.0.01.00 Decision: 11/ March 25, 2021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Menatti L, Bich L, Saborido C. Health and environment from adaptation to adaptivity: a situated relational account. Hist Philos Life Sci. 2022;44(3):1–28. doi:10.1007/s40656-022-00515-w
2. Asefa A, Nigussie T, Henok A, Mamo Y. Prevalence of sexual dysfunction and related factors among diabetes mellitus patients in Southwest Ethiopia. BMC Endocr Disord. 2019;19(1):1–8. doi:10.1186/s12902-019-0473-1
3. Shiferaw WS, Akalu TY, Petrucka PM, Areri HA, Aynalem YA. Risk factors of erectile dysfunction among diabetes patients in Africa: a systematic review and meta-analysis. J Clin Transl Endocrinol. 2020;21(June):100232. doi:10.1016/j.jcte.2020.100232
4. International Diabetes Federation. IDF Diabetes Atlas.
5. Faselis C, Katsimardou A, Imprialos K, Deligkaris P, Kallistratos M, Dimitriadis K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr Vasc Pharmacol. 2019;18(2):117–124. doi:10.2174/1570161117666190502103733
6. Jayasena CN, Anderson RA, Llahana S, et al. Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clin Endocrinol (Oxf). 2022;96(2):200–219. doi:10.1111/cen.14633
7. Andlib N, Sajad M, Kumar R, Thakur SC. Abnormalities in sex hormones and sexual dysfunction in males with diabetes mellitus: a mechanistic insight. Acta Histochem. 2023;125(1):151974. doi:10.1016/j.acthis.2022.151974
8. Corona G, Isidori AM, Aversa A, et al. Male and female sexual dysfunction in diabetic subjects: focus on new antihyperglycemic drugs. Rev Endocr Metab Disord. 2020;21(1):57–65. doi:10.1007/s11154-019-09535-7
9. Pretorius D, Couper ID, Mlambo MG. Sexual history taking by doctors in primary care in North West province, South Africa: patients at risk of sexual dysfunction overlooked. African J Prim Heal Care Fam Med. 2022;14(1):1–9. doi:10.4102/phcfm.v14i1.3238
10. Martín JC, Acuña MJ, Labrador J, Blanco M, Casas C. Sexual dysfunction factors in patients with schizophrenia treated with second generation antipsychotics: not only prolactin. Actas Esp Psiquiatr. 2018;46(6):217–225.
11. Esposito K, Maiorino MI, Bellastella G, Giugliano F, Romano M, Giugliano D. Determinants of female sexual dysfunction in type 2 diabetes. Int J Impot Res. 2010;22(3):179–184. doi:10.1038/ijir.2010.6
12. Giugliano F, Maiorino M, Bellastella G, Gicchino M, Giugliano D, Esposito K. Determinants of erectile dysfunction in type 2 diabetes. Int J Impot Res. 2010;22(3):204–209. doi:10.1038/ijir.2010.1
13. Clayton AH, Valladares Juarez EM. Female Sexual Dysfunction. Med Clin North Am. 2019;103(4):681–698. doi:10.1016/j.mcna.2019.02.008
14. Boeri L, Capogrosso P, Ventimiglia E, et al. Sexual Dysfunction in Men with Prediabetes. Sex Med Rev. 2020;8(4):622–634. doi:10.1016/j.sxmr.2018.11.008
15. Yenice MG, Danacıoğlu YO, Mert M, et al. Evaluation of factors affecting sexual dysfunction in female patients with diabetes mellitus. Arch Endocrinol Metab. 2020;64(3):319–325. doi:10.20945/2359-3997000000238
16. Clayton AH, Valladares Juarez EM. Female Sexual Dysfunction. Psychiatr Clin North Am. 2017;40(2):267–284. doi:10.1016/j.psc.2017.01.004
17. Gebeyehu NA, Gesese MM, Tegegne KD, et al. Global prevalence of sexual dysfunction among diabetic patients from 2008 to 2022: systematic review and meta-analysis. Metab Open. 2023;18(April):100247. doi:10.1016/j.metop.2023.100247
18. Harbishettar V, Krishna KR, Srinivasa P, Gowda M. The enigma of doctor-patient relationship. Indian J Psychiatry. 2019;61(Suppl 4):S776–S781. doi:10.4103/psychiatry.IndianJPsychiatry_96_19
19. Association TAD. 4. Lifestyle management: standards of medical care in Diabetes 018. Diabetes Care. 2018;41(January):S38–S50. doi:10.2337/dc18-S004
20. Association AD. 14. Diabetes Care in the Hospital: standards of Medical Care in Diabetes 2018. Diabetes Care. 2018;41(Suppl. 1):144–151. doi:10.2337/dc18-S014
21. Rahmanian E, Salari N, Mohammadi M, Jalali R. Evaluation of sexual dysfunction and female sexual dysfunction indicators in women with type 2 diabetes: a systematic review and meta-analysis. Diabetol Metab Syndr. 2019;11(1):1–17. doi:10.1186/s13098-019-0469-z
22. Imprialos KP, Koutsampasopoulos K, Katsimardou A, et al. Female Sexual Dysfunction: a Problem Hidden in the Shadows. Curr Pharm Des. 2021;27(36):3762–3774. doi:10.2174/1381612827666210719104950
23. Reed MA. Female Sexual Dysfunction. Clin Plast Surg. 2022;49(4):495–504. doi:10.1016/j.cps.2022.06.009
24. Cichocka E, Jagusiewicz M, Gumprecht J. Sexual dysfunction in young women with type 1 diabetes. Int J Environ Res Public Health. 2020;17(12):1. doi:10.3390/ijerph17124468
25. Shifren JL. Midlife sexuality in women’s words. Menopause. 2019;26(10):1088–1089. doi:10.1097/GME.0000000000001408
26. Reed SD, Carpenter JS, Larson J, et al. Toward a better measure of midlife sexual function: pooled analyses in nearly 1000 women participating in MsFLASH randomized trials. Menopause. 2022;29(4):397–407. doi:10.1097/GME.0000000000001940
27. Rambhatla A, Rajfer J. Male sexual dysfunction. Encycl Endocr Dis. 2018;10(3):767–774. doi:10.1016/B978-0-12-801238-3.65376-X
28. Salonia A, Bettocchi C, Boeri L, et al. European Association of Urology Guidelines on Sexual and Reproductive Health—2021 Update: male Sexual Dysfunction[Formula presented]. Eur Urol. 2021;80(3):333–357. doi:10.1016/j.eururo.2021.06.007
29. Rezaee ME, Ward CE, Brandes ER, Munarriz RM, Gross MS. A Review of Economic Evaluations of Erectile Dysfunction Therapies. Sex Med Rev. 2020;8(3):497–503. doi:10.1016/j.sxmr.2019.06.001
30. Bahar A, Elyasi F, Moosazadeh M, Afradi G, Kashi Z. Sexual dysfunction in men with type II diabetes. Casp J Intern Med. 2020;11(3):295–303. doi:10.22088/cjim.11.3.295
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.