Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Do Regulatory and Curriculum Requirements for Interprofessional Practice Align?
Authors Brownie S, Tokolahi E ![]() , Broman P
, Broman P ![]() , Haggie M, Andersen P
, Haggie M, Andersen P
Received 5 September 2023
Accepted for publication 8 November 2023
Published 29 November 2023 Volume 2023:16 Pages 3675—3687
DOI https://doi.org/10.2147/JMDH.S438791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sharon Brownie,1– 3 Ema Tokolahi,4 Patrick Broman,3 Marrin Haggie,3 Patrea Andersen3,5,6
1School of Health Sciences, Swinburne University of Technology, Melbourne, VIC, Australia; 2School of Health Sciences and Social Work, Griffith University, Gold Coast, QLD, Australia; 3Centre for Health and Social Practice, Wintec Te Pūkenga, Hamilton, New Zealand; 4School of Occupational Therapy, Otago Polytechnic Te Pūkenga, Dunedin, New Zealand; 5School of Health, University of the Sunshine Coast, Sippy Downs, QLD, Australia; 6School of Health, Medical and Applied Sciences, Central Queensland University, Rockhampton, QLD, Australia
Correspondence: Sharon Brownie, School of Health Sciences, Swinburne University of Technology, Hawthorn, Victoria, Australia, 3122, Email [email protected]
Background: While interprofessional (IP) competency and Interprofessional Education (IPE) has received increasing attention in health, agreement on specific competencies and teaching approaches is frequently limited by profession-specific understandings. As part of a quality improvement initiative focused on improving delivery of IPE offerings, this enquiry maps current regulatory and curricula requirements for IP practice to health professional students from 12 professions trained across Aotearoa New Zealand’s national vocational education provider.
Methods: Requirements for IP competency in national accreditation documents and in an operative teaching curricula were mapped for 12 professions, namely, clinical exercise physiology, counselling, massage, medical radiology, midwifery, nursing, occupational therapy, osteopathy, paramedicine, physiotherapy, social work, and sport and exercise science. A desk audit was conducted to identify the presence of core IP competencies for each profession. This involved a four-step process 1) Examination of regulatory standards for each profession to confirm IP requirements for each profession; 2) Examination of an operative curricula from each profession to identify the presence and translation of IP regulatory requirements to each of the profession-specific programs of study; 3) Mapping to identify within domains the core (common) IP competencies across the professions, and 4) Consideration of the similarities and differences between accreditation documents and curricula.
Results: Of 12 professions, 10 clearly identified IP competency as an expectation. Clinical Exercise Physiology and Counselling were exceptions with explicit requirement for IP competency not evident. Coordination and collaboration were the most identified competency domains in accreditation documents and curricula. In descending order of prevalence, communication, shared values, reflexivity, role-understanding, and teamwork were also identified requirements amongst the 10 professions with IP competency requirements.
Conclusion: The IP competencies identified as common across professions can be used to inform development of teaching and assessment. Greater alignment between teaching curricula and required competency standards in this area is recommended.
Keywords: interdisciplinary education, interdisciplinary communication, interprofessional relations, collaboration, competency
Introduction
In healthcare globally there is an increasing emphasis on interprofessional (IP) practice,1,2 and correspondingly, an urgent need for academic institutions to respond with opportunities for students to learn and demonstrate competency in an IP context.3 A growing body of evidence shows how interprofessional education (IPE) is an innovative pedagogical approach towards ultimately improving health outcomes.4,5 An international consensus process has identified several themes as key areas of competency to develop in IPE: role understanding; interprofessional communication; interprofessional values; coordination and collaborative decision-making; reflexivity; and teamwork.6 This list is not dissimilar to the one provided by the National Interprofessional Competency Framework in Canada, that identified six CORE competency domains: 1) interprofessional communication 2) patient-centered care 3) role clarification 4) team functioning 5) interprofessional conflict resolution, and 6) collaborative leadership.7
IPE should be supported by curricula and assessment structures, with the international consensus process having determined the purpose of IP assessment as important for, inter alia, raising the value of learning for all stakeholders; verifying capabilities for safe, effective practice; meeting the needs and expectations of those served by healthcare; measuring learning that has taken place; and offering insights into achievements.6 Further, suitable strategies for assessing IP practice were defined by the Canadian Interprofessional Health Collaborative (2010), including observation in practice, also known as fieldwork placements or practicums.7 An emerging trend is nontraditional practice education, which generates opportunities for groups of students from different professions to be supervised concurrently, by one (or more) practitioners from different professions to students.1
In the context of tertiary education, it is essential that the measurement of competency requirements is consistent with profession-specific boundaries and the learning outcomes defined in each profession’s program of study,3,8 as well as the requirements of each profession’s regulatory authority. However, there is considerable diversity in IPE approaches,1 and a subsequent need for adopting a common language across interprofessional education, as well as shared theoretical underpinnings, informed by scholarship, to guide its delivery.4 Moreover, IPE is influenced in practice by contextual factors, such as resources, facilitator experience, strategies, reflection, and feedback.2,9
A requirement for more studies investigating behavior-based or competency-based outcomes of interprofessional practice has been identified,2 as there is no current consensus about how these outcomes should look.6 More specifically, while studies have examined the IPE and IP collaborative practice requirements of accreditation standards across professions in Australia and Canada,4,10 no existing studies appear to summarize the IP practice requirements (knowledge, skills, and behaviors) required for different professions in New Zealand. There is also a need for critical analysis of how IP competencies as required by regulatory authorities are reflected in academic programs.4 While one recent study11 has explored the alignment between graduate attributes and accreditation requirements (plus industry employability criteria) in nursing, psychology and education courses at an Australian university, a comprehensive review testing alignment across a full range of health-specific professions appears lacking in Aotearoa New Zealand.
Study Objective
To map regulatory and curricula requirements for teaching IP practice to health professional students across Te Pūkenga - New Zealand’s national provider of vocational education.
Research Questions
- What IP competencies are required by the regulatory body of each profession taught within Te Pūkenga?
- What IP competencies are taught within the professional programs/curricula for each profession?
- What were the similarities and differences between the IP competencies required and taught for each profession?
New Zealand is currently progressing major reform of its vocational education sector with a view to ensuring better innovation, integration, and collaboration.12 These reforms seek to prepare graduates to better meet the needs of previously underserved populations, such as Māori and Pacific peoples and their communities.12–14 This reform involves the integration of several former providers, and unification of many teaching programs into national qualifications. In addition, the organization is undergoing educational innovation, including the development of an interprofessional student-led clinic (SLC). These developments provide impetus for developing a detailed understanding of the IP/IPE competency requirements as outlined by each of the regulatory authorities connected with the 12 health and social service professions taught within Te Pūkenga.
Methods
This quality improvement (QI) enquiry was approved by the then-Deputy Chief Executve, Delivery and Academic for Te Pūkenga who facilitated access to publicly available accreditation and curriculum documentation from across the organisation. In keeping with QI approaches where human participants are not used this enquiry did not require ethical approval.15,16 Content analysis17 was used to examine the IP competency requirements established by the regulatory authorities of health professions for which pre-registration academic programs are currently delivered by Te Pūkenga. The IPE requirements in these accreditation standards were mapped against IPE-related learning outcomes in curriculum documents for the relevant programs from Te Pūkenga.
Identifying Relevant Professions/Programs
Core IP competency requirements were sought for health professions with programs taught by Te Pūkenga which produce work-ready graduates, and which have regulatory authorities which impose competency requirements on their practitioners. Inclusions for this study involved clinical exercise physiology, counselling, massage, medical radiology, midwifery, nursing, occupational therapy, osteopathy, paramedicine, physiotherapy, social work, and sport and exercise science. Exclusions included nutrition, pharmacy, and psychology, as while qualifications were delivered in these fields within Te Pūkenga, they were not sufficient to meet professional body standards to register/practice.
Of relevance, it is important to note that many but not all professions are registered under the framework of the Health Practitioners Competence Assurance Act 200318 which requires relevant professional bodies to “to promote and facilitate inter-disciplinary collaboration and co-operation in the delivery of health services. Of the twelve professions taught pre-registration within the Te Pūkenga network, five disciplines are not covered by the Act, specifically, social work, sports and exercise science, massage, counselling, and clinical exercise physiology (CEP).
Locating Relevant Documentation
Key competency documents of each regulatory authority were retrieved in March–April 2022 through an online search of the respective regulatory organization websites for each profession. Relevant curricular document(s) for each of the 12 health professions included in this study were also sourced with the view to analyzing the translation of regulatory requirements within curricula. The profession-specific curricula were obtained primarily from one predecessor institution within Te Pūkenga. Where necessary, because the program of study was not taught in the initial institution, the search was extended to include curricula from other institutions where a pre-registration program in that profession was taught (see Table 1).
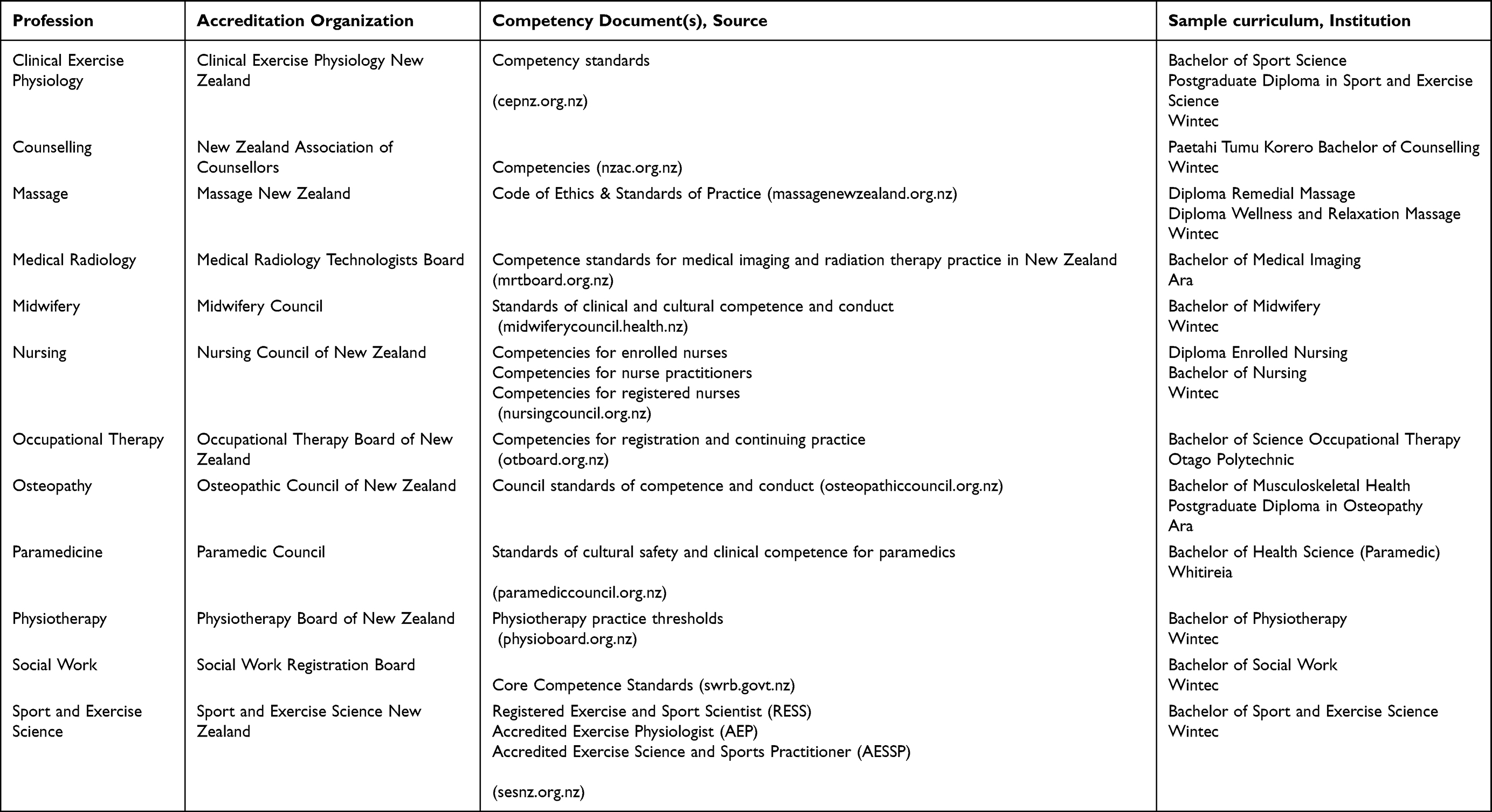 |
Table 1 Eligible Health Professions (n=12), Accrediting Organizations (n=12), Competency Documents (n=17) and Sample Curricula (n=16) |
Identification of Eligible Statements
The unit of analysis for this study comprised statements that made explicit reference to interprofessional practice. A search of the text from each regulatory board’s competency document sought to locate statements that included any of the following words: interprofessional, interdisciplinary, multidisciplinary, transdisciplinary, and collaborative/on. Statements that referred to collaborating with the client, and not specifically as part of a health team, were excluded. A close examination of the learning outcomes from the curriculum program documents, for each profession, was undertaken with the same aim of identifying eligible statements. Eligible statements from regulatory board competency requirements and the learning outcomes from curricula documentation were extracted and collated in a spreadsheet.
Analysis Procedures
A two-stage process of analysis was undertaken: in the first stage, within-profession analysis involved conducting a comparative analysis of the eligible statements between the regulatory board competency requirements and the learning outcomes from the curricula documents, independently for each of the professions. Patterns of convergence and divergence across the two sets of expectations were considered. In the second stage, a cross-profession analysis was conducted by exploring which of the six domains from the international consensus statement on assessment of IP learning outcomes6 were addressed across both regulatory board competency requirements and learning outcomes from curricula documentation, across all the professions. Statements from each of the accreditation and curriculum documents that referred to IP competency, were mapped against the 6 domains from the international consensus statement: Co-ordination and collaboration; Communication; Values; Reflexivity; Role understanding; and Teamwork.6 Findings from the two stages were synthesized.
Results
Examples of the accreditation and curriculum documents that referred to IP competency mapped against the 6 domains from the international consensus statement: Co-ordination and collaboration; Communication; Values; Reflexivity; Role understanding; and Teamwork6 are reported in Table 2. This includes annotated examples of statements that were included.
 |
Table 2 Example Competencies (Accreditation Standards) and Learning Outcomes (Curricula) Considered as Referring to Interprofessional Competencies |
IP Competencies Required by Regulatory Body
Analysis of requirements for IP competency in 17 accreditation documents mapped from 12 professions revealed documents from 10 professions clearly identified this as an expectation (See Table 3). The two exceptions were documents from Clinical Exercise Physiology and Counselling, where the requirement for IP competency of practitioners was not evident. Analysis revealed that coordination and collaboration6, was the most common domain from the international consensus statement (6) evident, included in the accreditation standards of 9 of 10 professions that identified IP competency as an expectation (the exception being sport and exercise science. Specifically ‘collaboration’ performance indicators include a need to “work collaboratively/use collaborative skills”, though this was not typically defined further. Coordination indicators included “coordination, facilitation, development, planning and/or implementation of IP care” and “shared decision making”. The next most frequently cited domain was Teamwork (8 professions), with indicators such as “engages with others”, and “referral management”. The other IP domains, present in descending frequency, were reflexivity (5 professions), role understanding (5 professions), IP communication (5 professions) and IP values (3 professions).,
IP Competencies Taught in Curricula
Results from the assessment of the learning outcomes mentioned in all the modules or papers taught in each of the 16 sample curricula are also shown in Table 3. Of the curricula analyzed, all except three curricula, in massage (n=2), and sport and exercise science (n=1), included at least one IP competency-related learning outcome. Most commonly, indicators taught or intended as an explicit learning outcome related to Rogers et al international consensus statement6 domains of Coordination and Collaboration (present in curricula for 9 professions) and/or Communication (7 professions). Less common were outcomes related to Reflexivity (n=6) and Role Understanding (n=5). The domains of Values (present in only n=4, for nursing, osteopathy, physiotherapy, and social work) and Teamwork (in 3, clinical exercise physiology, midwifery, and nursing) were observed less often. Where curricula included IP competencies, these were mostly present across two or more IP domains. Of included curricula, however, only that for nursing included at least one indicator from each of the 6 domains, two included 5 of 6: physiotherapy (except Teamwork) and midwifery (except Values).
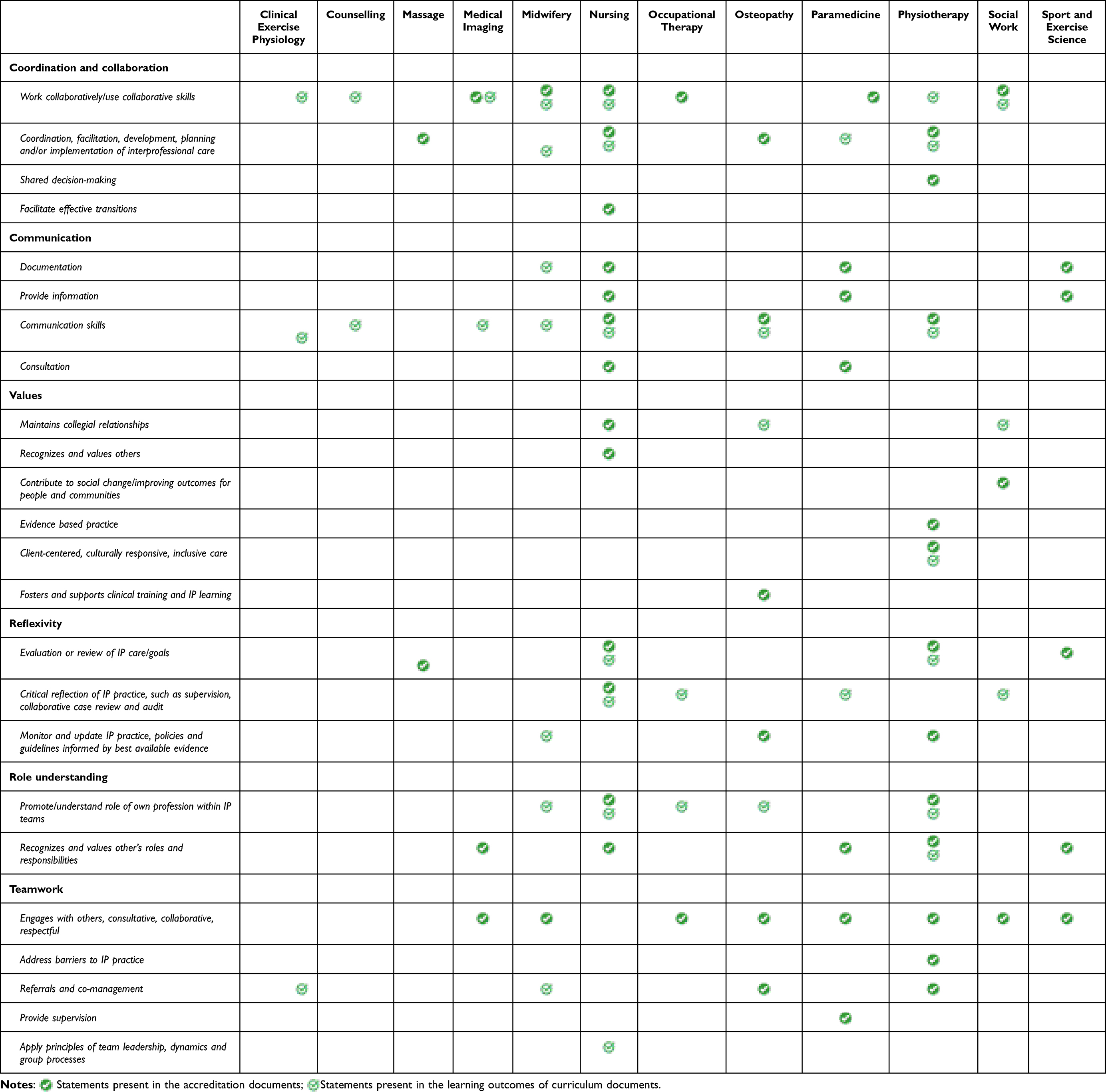 |
Table 3 Presence of Interprofessional Competency Domains and Indicators in Professional Practice Competencies/Standards and Curricula Learning Outcomes |
Similarities and Differences
The correlation between indicators required and those taught was limited for almost every profession, with the greatest overlap observed in nursing. The most reflected domain of the international consensus statement,6 in both regulatory accreditation documents and in curricula, was Coordination and Collaboration. In particular, the indicator “work collaboratively/use collaborative skills” was present in accreditation documents for six professions and curricula for seven professions. In the second most common domain overall, Communication, competency was included, across a range of indicators, in 4 professional accreditation documents (nursing, osteopathy, paramedicine and sport and exercise science), but as a learning outcome in the program curricula of 7 professions, with the indicator in all cases being communication skills. This included such outcomes as “L.O.3: Communicate and collaborate effectively with clients, whānau, and other members of the interprofessional team.” [physiotherapy clinical practice module] and L.O.4: “Demonstrate the practice of communicating professional judgements and collaborating within a professional context.” [counselling clinical practice module]. Within the Teamwork IP competency domain, the indicator “Engages with others, consultative, collaborative, respectful” was included in competency documents of 7 professions, with examples such as “You work well both alone and with others to ensure the best outcomes for your clients/tangata whaiora (Māori clients)” [occupational therapy, competency 3.1] and “effectively collaborates and engages with others and works in partnership with clients to gain access to resources” [social work, competency 8(4)]. However, this indicator was not explicitly mentioned in the learning outcomes of any sample curricula. Indeed, there is little discernible pattern of association between competencies required in practice (in accreditation documents) and those present in the learning outcomes across the Teamwork, Role Understanding, Reflexivity, or Values IP domains. Table 3
Discussion
Reflecting on results, we observed that the domain of coordination and collaborative decision making was unilaterally cited as a competency expectation across all the accreditation documents, where IP competency was identified as a requirement. Of further note, neither of the two professions where IP competency requirements were not evident, CEP or counselling, are regulated under the Health Practitioners Competency Assurance Act 2003. Without overarching legislation that mandates a requirement for IP competency, there is no legal compulsion for these professional accreditation boards to include this as a requirement of their practitioners. However, the absence of overarching legislation does not need to be prohibitive, as evidenced in the accreditation documents for massage, social work and sport and exercise science, which are also not regulated under the Act, yet do include IP competency as a requirement.
Five of the professions identified the IP domain of Values as a competency requirement; however, there was little consensus amongst these about which values were essential to demonstrate. In a local Delphi study by Andersen et al, understanding IP values and ethics was ranked the most important competency for IP practice in students.19 Further clarification on what IP values are, and the essential and desirable indicators for professions to demonstrate, would be useful for promoting effective IP practice and inform personal and professional development opportunities.
Definitions of IP collaboration, coordination and teamwork highlight the importance of role clarity, which overlaps with the domain Role Understanding and the indicators of “promoting one’s own profession” and “recognizing and valuing others” roles and responsibilities. Not surprisingly, the accreditation documents mapped in the current study reinforce the value of practitioners having a strong understanding of their role and how this is differentiated from, and works in collaboration with, the roles of others. This is further endorsed by a recent Delphi study,19 which highlighted these competencies under the domains Interpersonal relationships and mutual support and Leadership. Beyond the constraints of disciplinary roles to argue role dynamics, in particular leadership and followership roles, are also important skills for “an agile workforce”19 (p.09).
IP communication skills, where required by the accreditation bodies examined in this study, primarily involved effective transfer of information between professions (in writing or verbally). This was a requirement for only five of the professions examined. In other studies, communication is noted as highly important19 and it may be that, as health roles require a high degree of competency in communication generally, accreditation bodies have not considered any need to state a specific requirement that differentiates IP communication as a separate competency.
In terms of curricula, some IP competencies/indicators were very commonly reflected in learning outcomes across programs, including especially Communication (“communication skills”) and Coordination and Collaboration (“work collaboratively/use collaborative skills”). Generally speaking, IP competencies were less commonly reflected in curricula than in accreditation documents. This was consistent with a similar study, conducted in Australia, that found IP education and collaboration to be “fragmented and inconsistent” and requiring clearer definitions with evidence of accountability and relevant outcome measures to ensure authentic implementation.10 Some competencies, such as IP teamwork and IP values, were almost completely absent from learning outcomes, perhaps reflecting difficulties in formally teaching (and assessing) these skills. Teamwork, as Britton et al have argued, is difficult to empirically measure, given that it must be inferred from a range of behaviors and skills, complicating educators, and learner’s ability to track its performance in formal learning settings.20 The implication is that learning programs are relying on the informal and chance teaching of some key IP skills.
More broadly, findings suggest limited alignment between the intentions of regulators regarding IP competencies required by health professionals and the content of health professional curricula. Such misalignment between requirements of graduates and those of curricula are not unusual: a significant body of literature exists related to deviations from the “intended curricula” versus “taught curricula” and from the “taught curricula” versus “learned curricula”.21–23 Curriculum alignment includes the conceptual and operational components between what is intended, written, taught, and attained in the curriculum development and implementation process21–23 Figure 1, designed by the authors, illustrates this idealised process where regulatory and professional standards inform curriculum development and in turn the content taught. All of which should be reflected in the student outcomes.
 |
Figure 1 Components of the Curriculum Alignment Process (designed by authors). |
Ensuring effective curriculum alignment that converts what is intended to be taught into written curricula with translation to detailed lesson plans does not happen by chance, it requires deliberate and detailed action.22,24 Findings in this study highlight an opportunity for New Zealand accreditation bodies to work together in an IP collaborative forum to first align IPE and IPC expectations within their standards and secondly, to take an interprofessional approach in the approval and formal accreditation processes of written curriculum.
Ultimately, despite several decades of recognition that managing the growing burden of chronic conditions requires effective IP practice25 this has been slow to translate into policy and practice.26 The 2020 New Zealand Health and Disability System Review,27 which is noted as possibly the most comprehensive integrated look at the New Zealand Health and Disability System in a generation, found that there has been a longstanding focus on training for particular professions, rather than on competencies required.27,28 The review argued that future service models will rely more on teamwork and a range of roles, and that there is a need for learning that “allows students to gain a broader understanding and trust of other professions and reduce professional silos” (page 187).27 The review also found that regulatory authorities tend to focus on their own profession without consideration of other professions or system needs, and that this focus can hamper teamwork and innovation across the system. The differences shown here between accreditation documents and curricula, both within and between professions, would seem to support these findings. While outside the scope of this enquiry, the results may give raise questions about public safety and highlight the need for regulators and training providers to work more collaboratively to ensure that the health workforce is competent, capable, and fit-for-purpose.
Limitations
To contain the scope of this comparative document analysis, only 12 professions taught in Te Pūkenga were included, meaning there were several local health professions for which the IP competency requirements were not explored. While the competency documents associated with each of the 12 regulatory boards were examined, in some instances additional documents were noted focusing on scopes of practice or codes of ethics/conduct. Examination of these documents may yield different insights about the expectations of each regulatory board with regard to IP practice. Learning outcomes were analyzed from curricula documentation and it is acknowledged these do not always fully reflect the content and assessments utilized within programs of study. While constructive alignment promotes consistency between these three aspects of a program (ie learning outcomes, content and assessments),8 this may not have been the case, or the language may not have been as consistent, across all the documents examined. Furthermore, the six domains from Rogers et al were used as the theoretical framework against which to examine the competency requirements of each profession’s regulatory board and the learning outcomes of curricula documentation. Utilizing a different framework or taking an inductive approach may have resulted in different insights about the pattern of required IP competency across the professions included.
Conclusions
Ten of the 12 accreditation documents mapped required IP competency to be demonstrated by practitioners, and seven of those ten professions are regulated under the Health Practitioners Competency Assurance Act 2003.18
- Of the 12 professions mapped, seven professions responsible directly to the HPCA Act 2003, and three not covered under HPCA 2003 (massage, social work and sport and exercise science), have standards in relation to IP practice.
- Clinical exercise physiology (CEP) and counselling were the two exceptions where a requirement for IP practice and competency was not evident.
- Not unexpectedly, variance is evident across the professions requiring development of IP practice and competency standards.
- Coordination and Collaboration was the most identified domain with Communication, Values, Reflexivity, RoleUnderstanding, and Teamwork identified in descending order across 10 professions with IP competency requirements.
- Examination of the accredited programs identified gaps between what regulatory bodies want (intended curriculum) and what is included in the written curriculum. Opportunities exist for areas of improvement in accreditation processes to help close these gaps.
- Opportunity also exists for health professional regulators to demonstrate IP practice by collaborating and better aligning expectations.
Recommendations
A suitably supportive environment is essential to facilitate IP practice. For IP teams, it is critical that a supportive leadership structure clarifies the essential and desirable roles of individual members, facilitates effective communication between members who should be proximally located, and determines what are the predictable tasks and client pathways where IP collaboration and coordination will occur. A coordinated, whole system approach is required to enable this to occur effectively, requiring regulatory bodies to model IP practice by collaborating to align their IP expectations.
For the graduating health workforce to demonstrate the required IP competencies, education providers have a responsibility to teach curricula that sufficiently develops IP competencies. Ensuring regulator bodies focus on IP competencies in the process of (re)accrediting curricula will facilitate more effective translation between the intended and the written curriculum across health professions.
Finally, while this study mapped the relationship between the intended and written curriculum relevant to IP practice, further investigation is warranted to explore the translation of the written curriculum into the taught and assessed curriculum. This will better position the sector to develop and sustain a health workforce able to competently deliver IP practice in healthcare, thereby lifting health outcomes for all.
Ethical Approval
As a quality improvement desk audit our study did not require ethical board approval as human or animal participants were not involved. All regulatory data used for audit were publicly available and all curricula were accessed with organizational consent, the audit of which did not involve human participation.
Acknowledgments
The authors thank Dr Angela Beaton and Lauren Bennett (Te Pūkenga) for their assistance obtaining course curricula from across the Te Pūkenga network.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This project is supported by a Trust Waikato Community Impact Grant.
Disclosure
The authors declare no conflicts of interest.
References
1. Boshoff K, Murray C, Worley A, Berndt A. Interprofessional education placements in allied health: a scoping review. Scand J Occup Therapy. 2020;27(2):80–97. doi:10.1080/11038128.2019.1642955
2. McNaughton S. The long-term impact of undergraduate interprofessional education on graduate interprofessional practice: a scoping review. J Interprof Care. 2018;32(4):426–435. doi:10.1080/13561820.2017.1417239
3. Lie D, May W, Richter-Lagha R, Forest C, Banzali Y, Lohenry K. Adapting the McMaster-Ottawa scale and developing behavioral anchors for assessing performance in an interprofessional team observed structured clinical encounter. Med Educ Online. 2015;20:26691. doi:10.3402/meo.v20.26691
4. Azzam M, Puvirajah A, Girard MA, Grymonpre RE. Interprofessional education-relevant accreditation standards in Canada: a comparative document analysis. Human Res Health. 2021;19(1):66. doi:10.1186/s12960-021-00611-1
5. Gentry C, Espiritu E, Schorn MN, et al. Engaging the community through a longitudinal, interprofessional, interinstitutional experiential learning collaboration. Curr Pharm Teach Learn. 2021;13(2):169–176. doi:10.1016/j.cptl.2020.09.012
6. Rogers GD, Thistlethwaite JE, Anderson ES, et al. International consensus statement on the assessment of interprofessional learning outcomes. Medical Teacher. 2017;39(4):347–359. doi:10.1080/0142159X.2017.1270441
7. Canadian Interprofessional Health Collaborative. A national interprofessional competency framework; 2010:1–32. Available from: https://phabc.org/wp-content/uploads/2015/07/CIHC-National-Interprofessional-Competency-Framework.pdf.
8. Biggs J, Tang C. Teaching for Quality Learning at University Maidenhead, UK: Open University Press; 2011.
9. Reeves S, Fletcher S, Barr H, et al. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med Teach. 2016;38(7):656–668. doi:10.3109/0142159x.2016.1173663
10. Bogossian F, Craven D. A review of the requirements for interprofessional education and interprofessional collaboration in accreditation and practice standards for health professionals in Australia. J Interprof Care. 2021;35(5):691–700. doi:10.1080/13561820.2020.1808601
11. Oraison HM, Konjarski L, Howe ST. Does university prepare students for employment? Alignment between graduate attributes, accreditation requirements and industry employability criteria. J Teach Learn Grad. 2019;10(1):173–194. doi:10.21153/jtlge2019vol10no1art790
12. Te Pūkenga. Whakaumu i te ako : Proposed Te Pūkenga Operating Model; 2021:1-103. Available from: www.tepūkenga.ac.nz/assets/OM/Proposed-Operating-Model.pdf.
13. NZQA. Reform of vocational education. Available from: https://www.nzqa.govt.nz/providers-partners/rove/.
14. Gerritsen J. Te Pūkenga says close ties with Māori priority for new operating model. Education New Zealand: Radio New Zealand; 2021.
15. Stiegler MP, Tung A. Is it quality improvement or is it research?: Ethical and regulatory considerations. Anesth Analg. 2017;125(1):342–344. doi:10.1213/ane.0000000000001815
16. Goldstein CE, Weijer C, Brehaut JC, et al. Accommodating quality and service improvement research within existing ethical principles. Trials. 2018;19(1):334. doi:10.1186/s13063-018-2724-2
17. Mayring P. Qualitative Content Analysis: A Step-by-Step Guide. Sage; 2021.
18. New Zealand Government. Health Practitioners Competence Assurance Act 2003.
19. Andersen P, Broman P, Tokolahi E, Yap JR, Brownie S. Determining a common understanding of interprofessional competencies for pre-registration health professionals in Aotearoa New Zealand: a Delphi study. Original Research. Front Med. 2023;10. doi:10.3389/fmed.2023.1119556
20. Britton E, Simper N, Leger A, Stephenson J. Assessing teamwork in undergraduate education: a measurement tool to evaluate individual teamwork skills. Assess Eval High Educ. 2017;42(3):378–397. doi:10.1080/02602938.2015.1116497
21. Phaeton MJ, Stears M. Exploring the alignment of the intended and implemented curriculum through teachers’ interpretation: a case study of a-level biology practical work. Eurasia J Math Sci Tech Ed. 2017;13:723–740.
22. Porter AC, Smithson JL. Defining, developing and using curriculum indicators. CPRE Res Rep Seri. 2001;2001:1–40.
23. Zaman Z, Khawaja U. Deviation from recommended curriculum and efforts to bridge the gap between suggested and taught curricula. Propel Int J Acad Res. 2022;2:26–36. doi:10.55464/pjar.v2i1.28
24. Hunter J, Haywood A, Parkinson N. Ending the Lesson Lottery: How to Improve Curriculum Planning in Schools. Grattan Institute; 2023:1–82.
25. Michielsen L, Bischoff E, Schermer T, Laurant M. Primary healthcare competencies needed in the management of person-centred integrated care for chronic illness and multimorbidity: results of a scoping review. BMC Prim Care. 2023;24(1):98. doi:10.1186/s12875-023-02050-4
26. Legrand T, Stone D. Governing global policy: what IPE can learn from public policy? Policy Soc. 2021;40(4):484–501. doi:10.1080/14494035.2021.1975218
27. Health and Disability System Review. Health and Disability Systems Review: Final Report Pūrongo Whakamutunga. Manatu Hauora Ministry of Health. 2020:1–259.
28. Ministry of Health. New Zealand Health and Disability System. Manatu Hauora Ministry of Health. Available from: https://www.health.govt.nz/new-zealand-health-system/new-health-and-disability-system.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
University Staff Insights on Interprofessional Education and Student-Led Clinic Opportunities at an Australian University
Collis JM, Barradell S, Broman P, Brownie S
Journal of Multidisciplinary Healthcare 2024, 17:305-315
Published Date: 20 January 2024