Back to Journals » Infection and Drug Resistance » Volume 16
Do Knowledge, Attitudes, and Barrier Perception Affect the Prevention and Control of Healthcare-Associated Infections? A Structural Equation Modelling Approach
Authors Wang X, Liu C, Du Y, Wang D ![]() , Zhang X
, Zhang X ![]()
Received 7 March 2023
Accepted for publication 6 May 2023
Published 17 May 2023 Volume 2023:16 Pages 3051—3063
DOI https://doi.org/10.2147/IDR.S409398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xuemei Wang,1 Chenxi Liu,2 Yaling Du,3 Dan Wang,4 Xinping Zhang2
1Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu Province, People’s Republic of China; 2School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 3First Affiliated Hospital, School of Medicine, Shihezi University, Shihezi, People’s Republic of China; 4School of Management, Hubei University of Chinese Medicine, Wuhan, Hubei Province, People’s Republic of China
Correspondence: Dan Wang, School of Management, Hubei University of Chinese Medicine, Wuhan, Hubei Province, People’s Republic of China, Email [email protected] Xinping Zhang, school of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China, Email [email protected]
Purpose: Healthcare-associated infections (HCAIs) have become a global public health problem, resulting in high mortality, serious morbidity, and heavy healthcare costs. Infection prevention and control (IPC) is a significant priority for healthcare workers (HCWs) to eliminate HCAIs. However, barriers exist in the IPC implementation in daily clinical work. This study aimed to explore the relationship between HCWs’ knowledge, attitudes, barrier perception, as well as their effects on IPC practice.
Patients and Methods: A structured questionnaire survey was conducted among HCWs who were responsible for IPC in a large tertiary hospital in China. Cronbach’s alpha, average variance extracted (AVE), composite reliability (CR), as well as confirmatory factor analyses (CFA) were performed for reliability and validity. Structural equation modelling (SEM) was applied to establish the relationship between knowledge, attitudes, barrier perception and IPC practice. A Multiple Indicators Multiple Causes (MIMIC) model was conducted to detect the effects of covariates on factor structure.
Results: In total, 232 valid questionnaires were eventually collected. The average score of knowledge, attitudes, barrier perception and IPC practice were 2.95± 0.75, 4.06± 0.70, 3.14± 0.86, and 4.38± 0.45, respectively. The instrument demonstrated good reliability and validity. The SEM results showed that knowledge was positively associated with attitudes (β=0.151, p=0.039), and attitudes had positive effects on IPC practice (β=0.204, p=0.001), whereas barrier perception was negatively associated with attitudes and IPC practice (β=− 0.234, p< 0.001; β=− 0.288, p< 0.001, respectively). Additionally, time proportion spent on IPC was significantly associated with attitudes and practice (β=0.180, p=0.015; β=0.287, p< 0.001, respectively), and training on HCAIs was a predicator for barrier perception and practice (β=0.192, p=0.039; β=− 0.169, p=0.038, respectively).
Conclusion: IPC practice was indirectly affected by knowledge through the mediation of attitudes, whereas barrier perception had a negative impact. Designing deficiency-based training programs, developing sustained IPC habits, and strengthening management support are recommended to optimize IPC practice.
Keywords: healthcare-associated infections, infection prevention and control, knowledge, attitudes, barrier perception, structural equation modelling
Introduction
Healthcare-associated infections (HCAIs) have become a major public health problem, threatening hundreds of millions of patients worldwide each year.1 It has been reported that the pooled HCAI prevalence in high-income countries was 7.6%, while it was up to 10.1% in low- and middle-income countries (LMICs).2 As the most frequent adverse event threatening patient safety, HCAIs have become one of the top 10 leading causes of deaths in the USA, resulting in high mortality, serious morbidity, and heavy healthcare costs.3,4 It was estimated that 4,131,000 patients were affected by approximately 4,544,100 episodes of HCAIs in Europe annually.5 The situation was even worse in LMICs, where the frequency of ICU-acquired infection was 2–3 times higher than in high-income countries, and the device-associated infection densities were up to 13 times higher than in America.5
Faced with such severe HCAIs situation, infection prevention and control (IPC) of healthcare workers (HCWs) is critical to ensuring patient safety and declining healthcare costs.6 It was estimated that HCWs’ compliance with disinfection and isolation may decrease the risk of HCAIs to 10.7%, and hand hygiene could contribute to a reduction of 15–30% of the HCAIs by breaking the chain of transmission of pathogens between patients and environment.7,8 However, IPC practice was suboptimal in many circumstances. A literature review concluded that most studies revealed average or poor practice with respect to preventing and controlling HCAIs.9 For instance, the overall observed compliance of hand hygiene was only 23.9%.8
Poor knowledge is one of the most important factors resulting in high prevalence of HCAIs globally, and is detrimental to achieving optimal IPC practice.9 If guidelines were strictly followed, 69% of the infections could be avoided.10 However, the knowledge level regarding IPC guidance or protocol was not always optimal. Cutinho et al11 found that only 13% of the nurses were aware of evidence-based guidelines of catheter-associated urinary tract infection. Shedu et al12 discovered that only 16% of the HCWs had good knowledge of hand hygiene. Laskar et al13 also reported that quite a few HCWs lacked basic knowledge about hand hygiene or proper use of gloves in patient care. In addition, many HCWs were not familiar with the guidelines for using alcohol hand rub, which actually had similar effect as hand washing.10
Suitable attitudes are regarded as another essential factor in IPC practice, which was necessary to promote the achievement of good IPC practice.9 The attitudes of HCWs towards IPC were not always positive. For instance, approximately 98% of HCWs believed hand hygiene could prevent the occurrence of HCAIs, of whom 56.9% believed HCAIs could be completely prevented, while 20% thought it was not their responsibility.14
In addition, many barriers exist in the IPC implementation in daily clinical work, which may impede the translation of good IPC practice. As a literature review summarized, common barriers included excess workload, understaffing, lack of knowledge, etc.10 Previous studies also reported that up to 67% of the physicians regarded hand hygiene as a difficult task, and over half of HCWs felt that excessive workload and lack of time hindered the hand hygiene adherence.13,14
In China, the prevalence of HCAIs varied between 1.73% and 5.45%, and caused a direct economic burden of $1.5 billion to $2.3 billion each year.15,16 Despite this, there are still gaps existed in current IPC practice.17 The average compliance rate of hand hygiene among HCWs in China was 54.34%, and up to 35.85% of the hospitals showed a poor IPC performance.18 However, little is known regarding the relationship between knowledge, attitudes, barrier perception and HCWs’ IPC practice in China. Although previous literature attempted to measure IPC knowledge, attitudes, and practice, few studies have considered the role of barrier perception on IPC or validated the constructed model. Therefore, there is an urgent need to assess the knowledge, attitudes, barrier perception towards IPC in China, and to explore how they affect IPC practice. This study aimed to build and validate the linkage between knowledge, attitudes, barrier perception, and IPC practice, so as to provide evidence-based instructions for optimizing IPC practice.
Materials and Methods
Settings and Participants
A structured cross-sectional study was conducted in November 2018 in a large tertiary public hospital in Wuhan, China. It is a comprehensive hospital integrating medical service, teaching, scientific research, and public health, with more than 60 clinical and medical technology departments and over 6000 HCWs. The hospital has exceeding 6000 inpatient beds and provides approximately 6,317,152 outpatient and 272,002 inpatient services each year. The prevalence rate of HCAIs in the hospital was approximately 2.54%, and the overall compliance of hand hygiene among nurses was about 57.52%. The Nosocomial Infection Control Department was responsible for the hospital-wide IPC, and specific IPC work was performed by infection professionals from this department. Meanwhile, partial physicians or nurses were designated to be responsible for IPC in their own clinical departments or wards.
Respondents in this study should meet the following inclusion and exclusion criteria. Inclusion criteria included (1) physicians or nurses engaged in clinical work; (2) physicians or nurses who were responsible for IPC in their own clinical departments or wards; (3) physicians or nurses who volunteered to participate in the survey. Exclusion criteria: HCWs who did not work in clinical departments, eg, hospital administrators. Consent was obtained from respondents prior to their inclusion in the study, and a total of 232 eligible HCWs were eventually included in the study.
Data Collection
Data were collected through a structured self-administered questionnaire, involving IPC knowledge, attitudes, barrier perception and practice, as well as demographic characteristics of participants. Respondents who met the inclusion and exclusion criteria were invited to fill in the questionnaire by themselves. Before filling in the questionnaire, a brief introduction to this survey was illustrated by trained interviewers. At the end of survey, the completed questionnaires were handed in and checked for completeness, whereas the incomplete questionnaires were returned to the corresponding participants to complete.
Theoretical Framework
The measurement tool in this study was mainly developed on the basis of knowledge, attitude, and practice (KAP) theory, which emphasized that the acquisition of knowledge, generation of attitudes and formation of behavior constituted three continuous processes of human behavior.19 To achieve the expected behavior change, knowledge is the foundation, while attitudes act as the driving force. Knowledge can influence behavior either directly or indirectly through attitudes, and attitudes usually have a direct impact on behavior.
In addition, barrier perception is another important factor influencing practice, especially in heavy clinical work environment.20 Considering potential barriers (eg, time constraints) may hinder IPC practice; thus, barrier perception was incorporated into the final theoretical framework in this study (Figure 1).
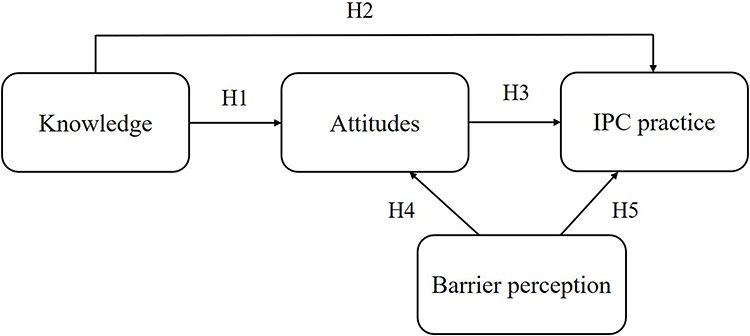 |
Figure 1 Theoretical framework of knowledge, attitudes, barrier perception and IPC practice. |
The research hypotheses in this study were proposed as follows:
Hypothesis 1: Knowledge has an impact on attitudes. Hypothesis 2: Knowledge has an impact on IPC practice. Hypothesis 3: Attitudes have an impact on IPC practice. Hypothesis 4: Barrier perception has an impact on attitudes. Hypothesis 5: Barrier perception has an impact on IPC practice.
In addition, potential risk factors (eg, demographic characteristics of participants) are likely to be associated with knowledge, attitudes, barrier perception as well as IPC practice.
Survey Instruments
A 25-item questionnaire was developed to measure IPC knowledge, attitudes, barrier perception and practice. Demographic characteristics of respondents were measured by another eight items.
Knowledge was measured using five items from previous studies, asking the respondents to make a judgment on the statement regarding IPC.11,21 The answer to each item is either “true” or “false”, and only one is correct. One point would be given on the correct answer, and the total points of correct answers per respondent were calculated. Attitudes were measured using five items, of which four items were adapted from previous studies and one item (A4) was developed in conjunction with actual situation of the surveyed hospital.21,22 Responses to each item was measured on a five-point Likert scale, ranging from “1=totally disagree” to “5=totally agree”. Barrier perception were measured using six items from previous studies, which were common problems occurring in daily IPC practice.20,23 Each item was given an option based on a five-point Likert scale, with a response from “1=almost none” to “5=very large”. Practice was measured using nine items, seven of which were adapted from previous studies, and the remaining two items (P8, P9) were developed in accordance with actual IPC requirements of the surveyed hospital.22,24,25 The answer to each item was measured on a five-point Likert scale, ranging from “1=never” to “5=always”. The specific items measuring knowledge, attitudes, barriers, IPC practice, and the sources of each item were shown in Table S1.
Statistical Analysis
Descriptive statistics were used to describe the demographic characteristics, as well as knowledge, attitudes, barrier perception, IPC practice of HCWs who participated in the survey. The difference between respondents in their knowledge, attitudes, barrier perception and IPC practice were examined using Mann–Whitney tests or Kruskal–Wallis tests, as the continuous variables were not normally distributed. The overall correct/desired responses for each item of questionnaire were summarized. Cronbach’s alpha was calculated to determine the reliability. The average variance extracted (AVE) and composite reliability (CR) were measured for convergent validity. The square roots of the AVE value and absolute values of correlation coefficients between constructs were calculated for discriminant validity. Confirmatory factor analyses (CFA) were used to validate whether the hypothetical model has a good fit. Structural equation modelling (SEM) analysis was applied to establish the linkage between knowledge, attitudes, barrier perception and IPC practice. Considering potential influencing factors may also have an impact on knowledge, attitudes, barrier perception and IPC practice, a Multiple Indicators Multiple Causes (MIMIC) model was conducted to detect the effects of covariates. Means and variance-adjusted weighted least squares (WLSMV) estimation was used for analysis as it was designed for ordinal variables, including five-point Likert scales.26
Generally, the minimum sample size for SEM research was 100 to 150, while others set this minimum to N=200.27 In our study, the number of eligible HCWs who were eventually included in this survey (N=232) met the minimum sample size requirement. To evaluate the fit of CFA, SEM and MIMIC model, goodness-of-fit indices were adopted in this study, including root mean square error of approximation (RMSEA: <0.08 is acceptable; <0.05 is excellent), comparative fit index (CFI: >0.90 is acceptable; >0.95 is excellent), Tucker–Lewis index (TLI: >0.90 is acceptable; >0.95 is excellent), standardized root mean square residual (SRMR: <0.10 is acceptable; <0.05 is excellent).28,29
All statistical analyses were performed using SPSS (version 23.0; Armonk, NY) in conjunction with MPLUS (version 8.0; Los Angeles, CA). P value less than 0.05 was considered statistically significant.
Results
Characteristics of Participants
A total of 232 HCWs were investigated. Respondents involved in this survey included 45 physicians and 187 nurses, most of whom were female. The average age was 37.44 years. More than half of HCWs got intermediate titles and the majority achieved associate degrees. The average length of working experience for HCWs was 14.99 years. Most of them have received training about HCAIs in the last year, whereas nearly half of them spent less than 10% of clinical working time on IPC (Table 1).
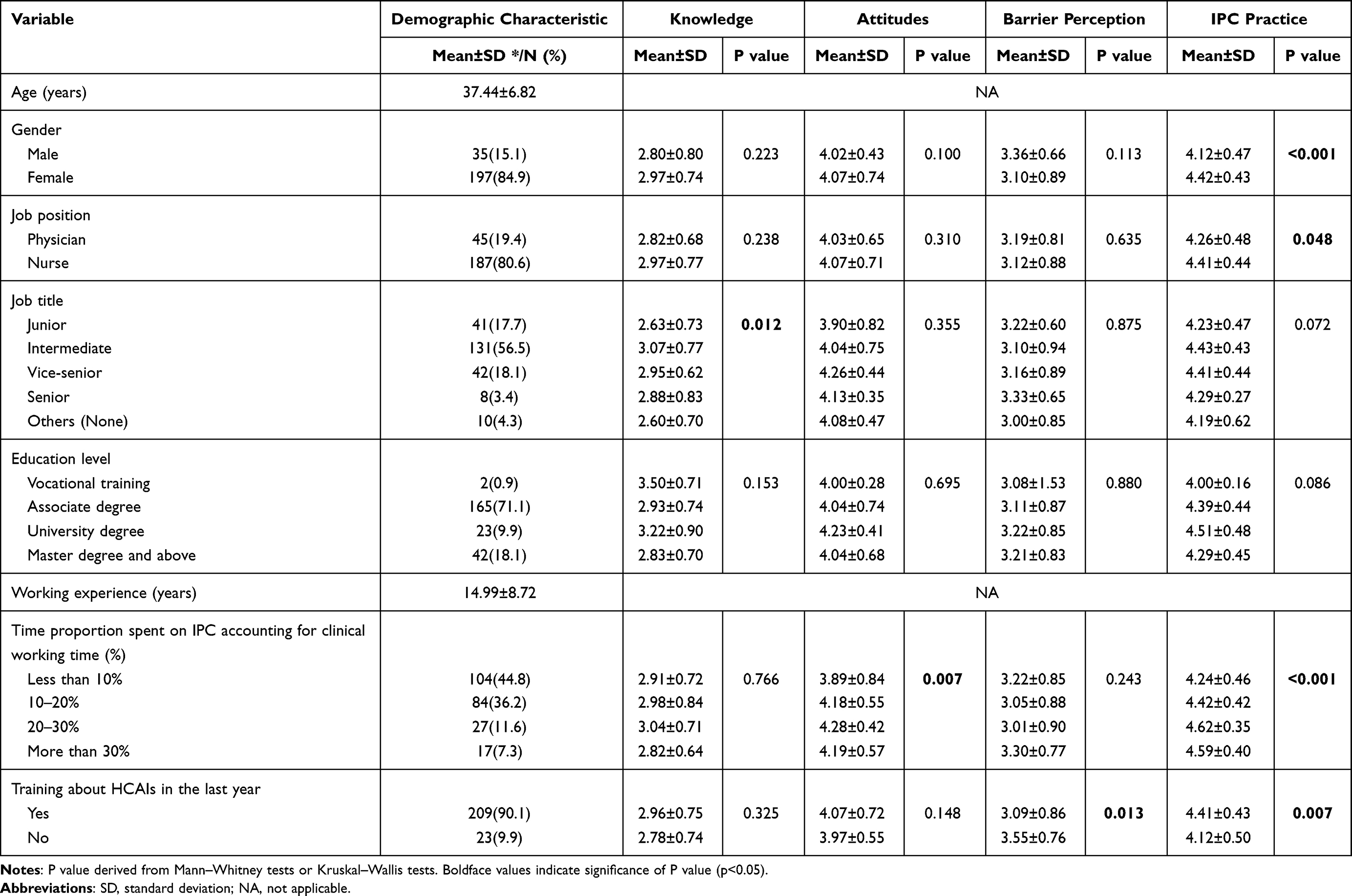 |
Table 1 Demographic Characteristics, Knowledge, Attitudes, Barrier Perception and IPC Practice of Respondents |
Overall, female HCWs had better IPC practice than male HCWs (P<0.001). Nurses had better IPC practice than physicians (P=0.048). Significant differences were found in the knowledge across job titles (P=0.012). There were also significant differences in the attitudes (P=0.007) and IPC practice (P<0.001) across HCWs who spent different proportion of time on IPC. Moreover, HCWs who received training about HCAIs in the last year had lower barrier perception and better IPC practice compared to those without training (Table 1).
Main results of Questionnaire
The average correct score of knowledge was 2.95 (SD=0.75). Of the HCWs surveyed, 66.38% knew the definition of HCAIs. A majority of HCWs knew that indwelling catheter would increase the risk of developing HCAIs, and care bundles can be used to reduce the risk of device-associated infections. However, only a few HCWs knew the major source of bacteria causing HCAIs and the function of alcohol hand rub in hand hygiene.
The average score of attitudes was 4.06 (SD=0.70). A majority of HCWs believed that IPC measures (eg, bundle care, hand hygiene) could effectively reduce risk of acquiring HCAIs. Of the HCWs surveyed, 82.33% believed that HCWs who do not perform hand hygiene or ignore IPC recommendations should be reprimanded. However, less than half of HCWs believed that they were able to implement IPC measures, even though most of them felt that they have received adequate training about HCAIs as a student.
The average score of barrier perception was 3.14 (SD=0.86). Most HCWs considered excess workload and time constraints as two major barriers. Nearly half of HCWs thought there was a lack of adequate facilities or resources. Only a minority of HCWs identified the lack of relevant knowledge, or absence of regular training as main barriers.
The average score of IPC practice was 4.38 (SD=0.45). A majority of HCWs performed hand hygiene as required, and performed disinfection after using reusable medical instruments. Besides, 61.64% of the HCWs informed the patient or family how to prevent and control HCAIs, and nearly half of them wore gloves when in direct contact with a patient (Table 2).
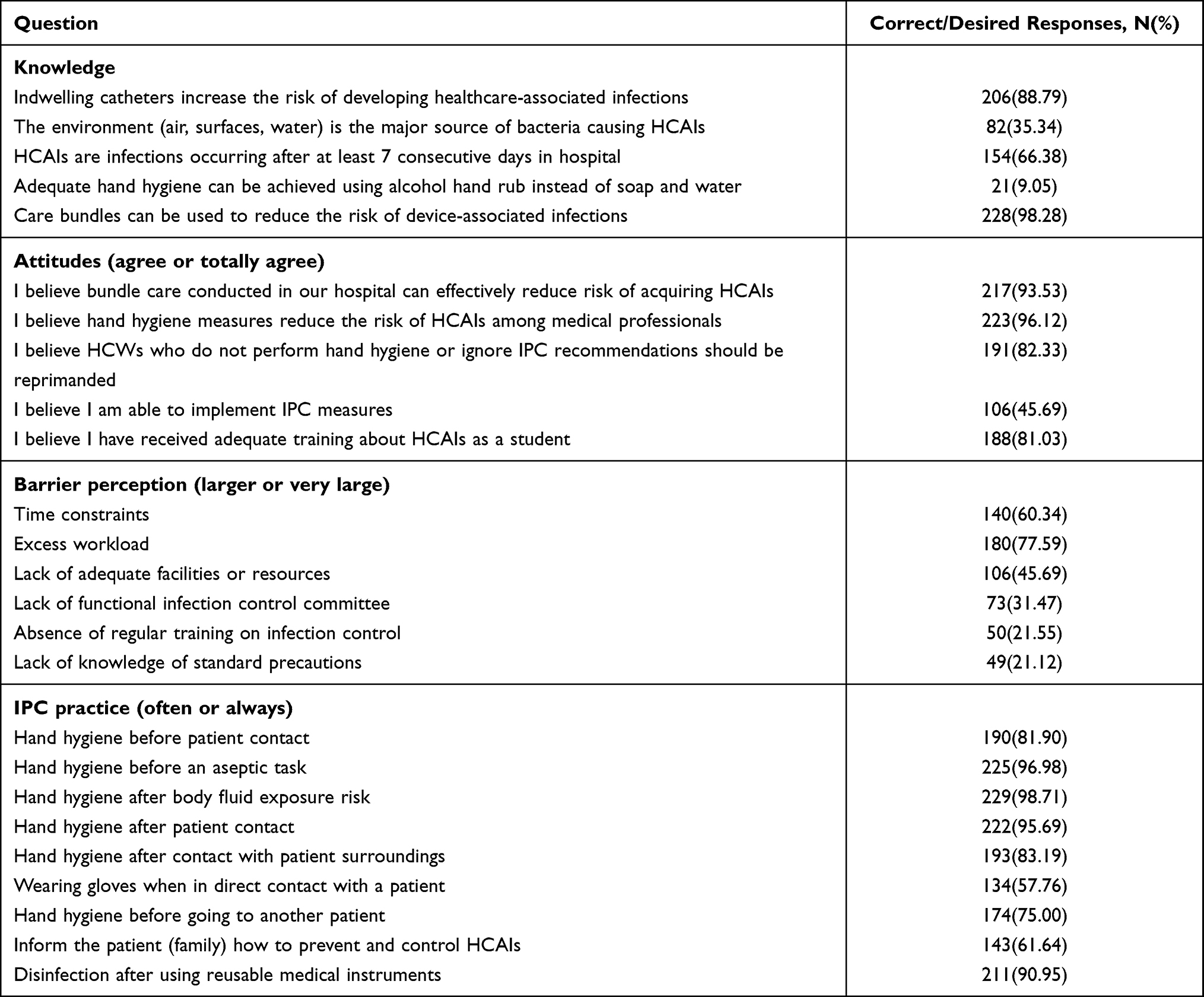 |
Table 2 Overall Knowledge, Attitudes, Barrier Perception and IPC Practice |
The Results of Reliability and Validity
This study proposed and validated the theoretical framework of knowledge, attitudes, barrier perception and IPC practice. The results demonstrated that the measurement tool had a good reliability, with Cronbach’s alpha values greater than 0.70 (the minimum acceptable value). The Cronbach’s alpha values of attitudes, barrier perception and IPC practice were 0.831, 0.862 and 0.764, respectively.
The factor loading of each item from attitudes, barrier perception and IPC practice ranged from 0.593 to 0.929, 0.391 to 0.989, 0.514 to 0.866, respectively. The AVE values of attitudes, barrier perception and IPC practice were 0.627, 0.588 and 0.478, respectively, and the CR values were all higher than 0.80. These results demonstrated a good convergent validity of the questionnaire constructs (Table 3). Additionally, the square roots of the AVE value were higher than the absolute values of correlation coefficients between attitudes, barrier perception and IPC practice, indicating that the questionnaire had a good discriminant validity (Table 4).
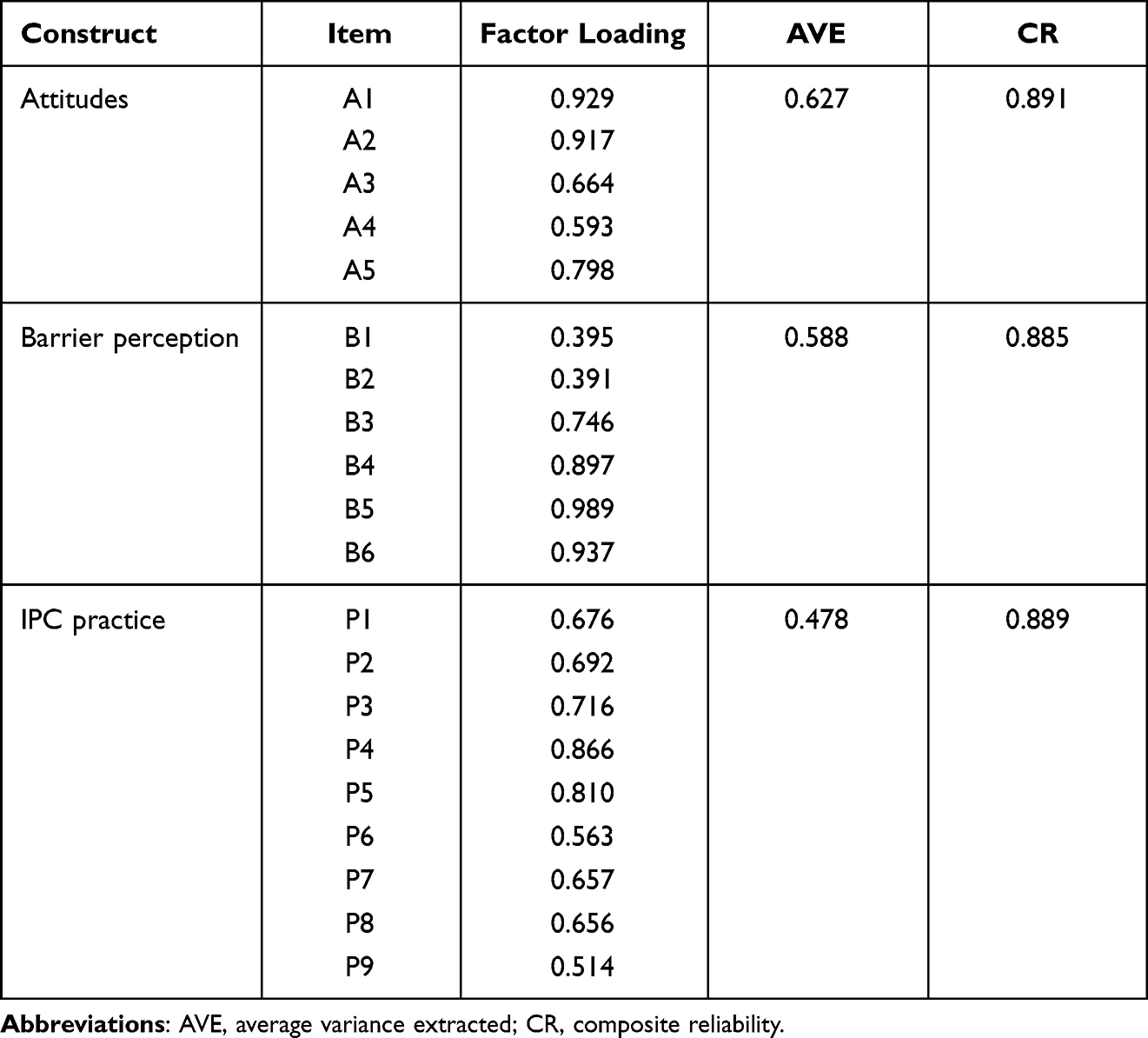 |
Table 3 Factor Loading of Each Item and the Convergent Validity, Composite Reliability Measurement |
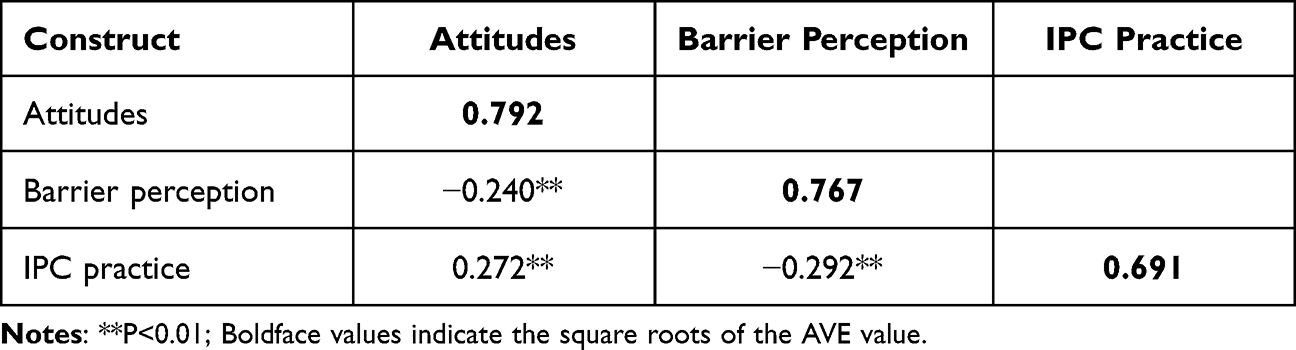 |
Table 4 Correlation Matrix of Attitudes, Barrier Perception and IPC Practice |
The initial results of CFA indicated that the three-factor model (attitudes, barrier perception and IPC practice were included as latent variables) with 20 items did not have a good fit (RMSEA=0.111, CFI=0.953, TLI=0.947, SRMR=0.107). However, the final CFA model was confirmed as providing a good fit to the data (RMSEA=0.074, CFI=0.980, TLI=0.977, SRMR=0.083), after drawing one error covariances according to the suggested modifications.
Associations Between Knowledge, Attitudes, Barrier Perception and IPC Practice
Associations between knowledge, attitudes, barrier perception and IPC practice were established using the SEM model. All the hypothesized paths were statistically significant (P <0.05), except for hypothesis 2. The final path model had a good fit (RMSEA=0.074, CFI=0.977, TLI=0.973, SRMR=0.088). Consistent with research hypotheses in this study, knowledge directly influenced attitudes (β=0.151, p=0.039), and had an indirect impact on IPC practice through attitudes (β=0.204, p=0.001). Barrier perception had negative effects on both attitudes (β=−0.234, p<0.001) and IPC practice (β=−0.288, p<0.001) (Figure 2).
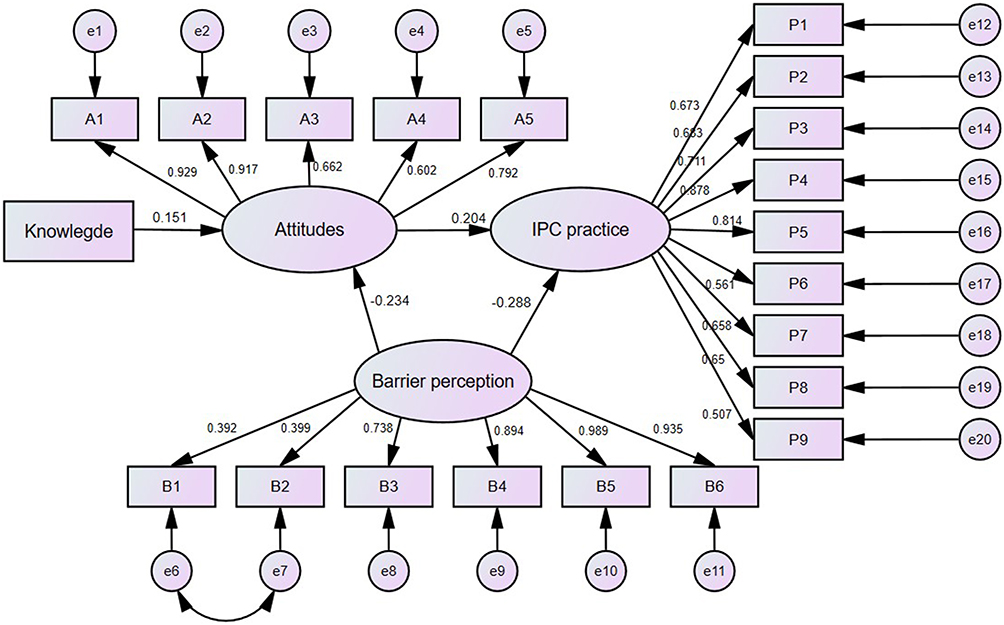 |
Figure 2 Structural equation model on knowledge, attitudes, barrier perception and IPC practice. Notes: Only significant pathways (p<0.05) were reported with standardized path coefficients. |
Effects of Covariates on Knowledge, Attitudes, Barrier Perception and IPC Practice
The MIMIC model was applied to access the effects of covariates on factor structure. Time proportion spent on IPC was significantly associated with attitudes and IPC practice (β=0.180, p=0.015; β=0.287, p<0.001, respectively), while training about HCAIs was significantly related to barrier perception and IPC practice (β=0.192, p=0.039; β=-0.169, p=0.038, respectively). The results of the MIMIC model are shown in Table 5.
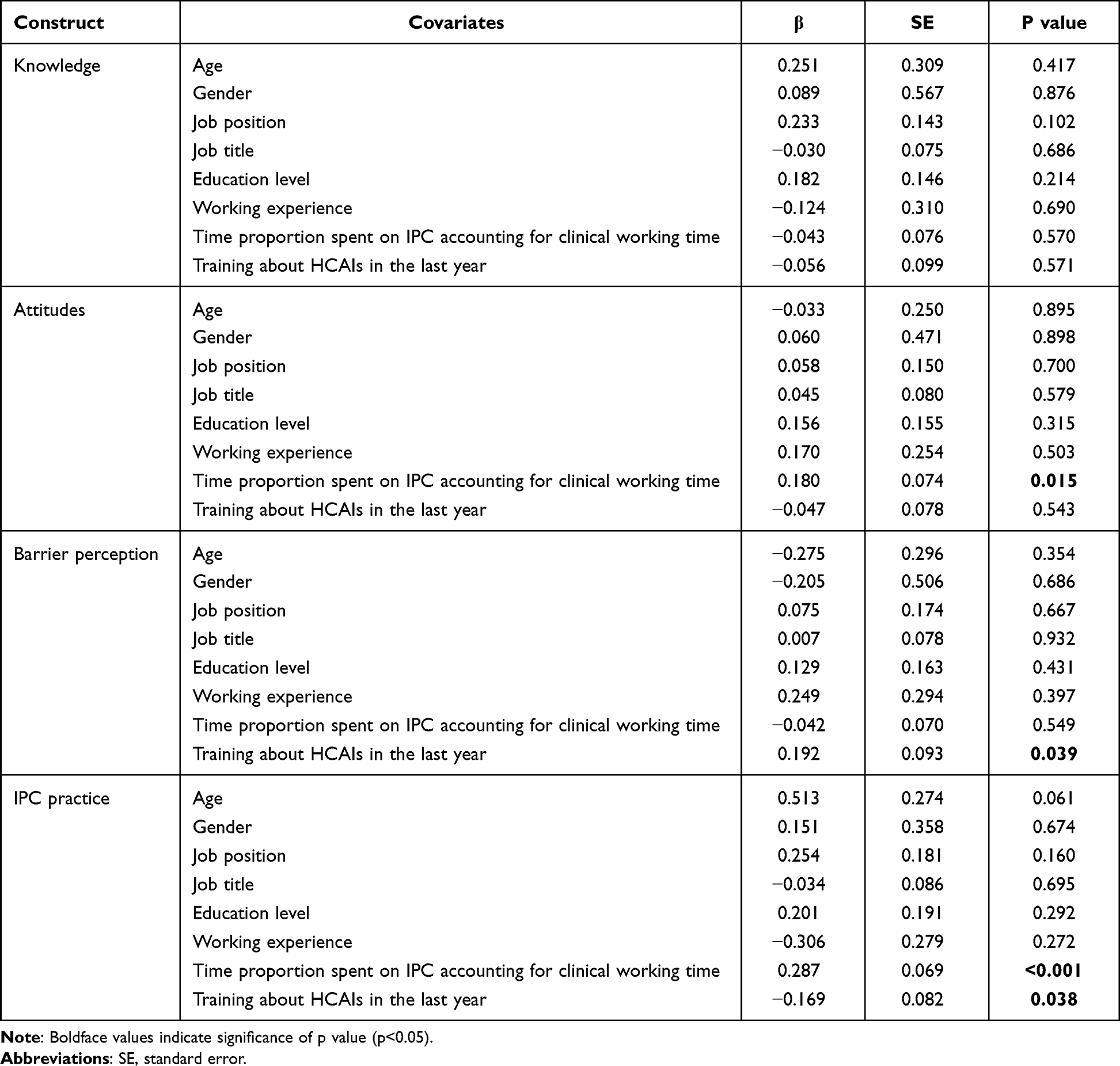 |
Table 5 MIMIC Results of Covariates on Knowledge, Attitudes, Barrier Perception and IPC Practice |
Discussion
Comparison with Other Studies
This study found that knowledge, attitudes, barrier perception, and IPC practice varied between different characteristics of HCWs, such as gender, job position, job title, etc. Consistent with our findings, Laskar et al13 reported that female HCWs usually had better IPC practice than male. In addition, it was found that nurses usually had better IPC practice than physicians.10,30 As regards training, Wu et al31 found a similar situation to ours, and suggested that training programs concerning IPC should be designed for HCWs. Besides, HCWs with intermediate title had a better knowledge than those with junior title, which may attribute to the accumulation of IPC expertise with the increasing working experience in the early stage of career.14,32 HCWs who spent more time on IPC indicated a greater emphasis on HCAIs, and as a result both their attitudes and IPC practice were more likely to perform better.
IPC practice is not totally guided by perfect logic but is instead led by potential factors that might cause inconsistencies.30 The overall IPC practice in this study was suboptimal, of which wearing gloves when in direct contact with a patient, and informing the patient or family how to prevent and control HCAIs were two poorer performances. Moreover, hand hygiene was less adhered before patient contact and before going to another patient, which was familiar to the findings by Laskar et al.13 The reason for the poor practice above was possibly that HCWs tend to have better IPC practice when they were at risk of acquiring HCAIs from patients, rather than from the perceptive of protecting patients.13
This study revealed that knowledge had positive effects on attitudes directly, whereas had no direct impact on IPC practice, proving that knowledge does not always directly translate into good practice.33 Previous studies also reported a know-do gap in IPC, where there was a contradiction between what physicians knew and what they actually did.33,34 Consistent with our findings, Russel et al35 discovered that there was no significant relationship between knowledge and self-reported IPC compliance, indicating that knowledge alone was not sufficient to account for variations in practice and emphasizing the importance of attitudes as a mediator between them. A systemic literature review showed that compliance of hand hygiene remains poor despite sound knowledge, suggesting that hand hygiene was an acquired habit.30 Nwaokenye et al36 also reported that good hand hygiene was not necessarily due to sufficient knowledge, but more out of habit and self-protection.
A mediating role of attitudes was found between knowledge and IPC practice in this study. Consistent with our findings, Nasiri et al9 concluded that positive attitudes could help facilitate the translation of professional knowledge into good IPC practice. Huang et al10 also pointed out that only when subliming knowledge into belief, can one take a positive attitude to change the behavior. As for the direct positive link between attitudes and IPC practice, this may lie in the fact that IPC practice was more likely to be driven by subjectively held information.35 Similarly, Sunkwa-Mills et al37 demonstrated that positive attitudes of some HCWs promoted standard IPC practice. Previous studies also indicated that believing one’s own behavior can change HCAIs outcomes is essential to achieving sustained behavior change.30,38
In addition, it was necessary to eliminate barriers as they were detrimental to implementing IPC measures. More than half of HCWs perceived time constraints and excess workload as two major barriers in our study. Similarly, previous studies demonstrated that lack of time and excess workload were main barriers hindering adherence to IPC precautions, particularly in busy clinical work environment.14,33 Sunkwa-Mills et al37 also reported that HCWs sometimes regarded HCAIs concerns as secondary when faced with heavy clinical workload. Lien et al34 also found that physicians complained that patient overload was a dominant barrier for their IPC compliance. The surveyed hospital in our study was crowded with patients most of time, as it was well known in central China. HCWs working there were usually in the face of heavily workload and often had to deal with emergencies within limited time, which may fail to ensure a good IPC practice all the time.
Policy Implications
Policy interventions targeting major IPC-related factors are critical. To reduce the barriers revealed in this study, three key intervention strategies have been proposed to improve current situation.
Firstly, deficiency-based training programs concerning standard IPC knowledge should be designed according to local clinical circumstance.39 As HCWs in the surveyed hospital are generally faced with excess workload and time constraints, short-term online training programs targeting specific HCWs groups with poor IPC practice may be more effective. Moreover, providing local data on HCAIs to HCWs in the training programs are advocated. This can help awaken them to be aware of the need for IPC, thereby motivating them to put the knowledge into IPC practice.34
Secondly, policy interventions targeting experiential thinking of HCWs are recommended, as some IPC measures are acquired habits.30 Great efforts need to be made to motivate HCWs to have positive beliefs towards changing HCAIs situation and to develop sustained IPC habits in daily clinical work. Also, it is necessary to promote patient safety culture in the hospital, so as to help HCWs transform self-protective attitudes into patient-safety attitudes when faced with HCAIs risk.36
Thirdly, management support for IPC should be further strengthened, as it has been found to be pivotal in combating HCAIs.40 In the overcrowded hospital, enhanced management support is recommended to ensure adequate supply of resources, especially human resources, to alleviate time constraints and heavy workload.
Strengths and Limitations
This study explored the associations between knowledge, attitudes, barrier perception and IPC practice among HCWs based on a validated model. The findings of this study enriched the evidence to combat HCAIs and filled some gaps in literature in China.
There are some limitations in this study. Firstly, the respondents in this study were all recruited from a large tertiary hospital, thus sampling bias may exist to some extent. Future research could validate the generalization of these findings using a wider survey. Secondly, although the current study has met the minimum sample size requirements of CFA and SEM, a larger study population could also be applied to confirm the results in the future.27 Thirdly, self-assessment questionnaires may lead to overestimation when measuring IPC, though they have been a common measurement. Future studies could try to apply more objective measures, for instance, direct observation.
Conclusion
A well-fitting path model of knowledge, attitudes, barrier perception and IPC practice was established. Improving knowledge may contribute to positive attitudes, and thereby promote better IPC practice. However, heavy workload, and time constraints can be major barriers in IPC implementation. It is recommended to design deficiency-based training programs, develop sustained IPC habits, and strengthen management support to optimize IPC practice.
Ethics Statement
The study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (NO: IORG003571). As the study used anonymous and retrospective data, the Ethics Committee waived the need for participants to provide written informed consent. Verbal consent was obtained from each respondent before completing the questionnaire. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors would like to sincerely appreciate all investigators for their hard work on data collection, especially the help and support from Professor Lai Xiaoquan.
Funding
This study was supported by National Natural Science Foundation of China (grant number 72004066), Jiangsu Provincial Double-Innovation Doctor Program (grant number JSSCBS20221873).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allegranzi B, Gayet-Ageron A, Damani N, et al. Global implementation of WHO’s multimodal strategy for improvement of hand hygiene: a quasi-experimental study. Lancet Infect Dis. 2013;13(10):843–851. doi:10.1016/S1473-3099(13)70163-4
2. World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. Geneva: World Health Organization. 2011.
3. Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–241. doi:10.1016/S0140-6736(10)61458-4
4. Haque M, Sartelli M, McKimm J, Abu Bakar M. Health care-associated infections - an overview. Infect Drug Resist. 2018;11:2321–2333. doi:10.2147/IDR.S177247
5. World Health Organization. Fact sheet on HCAI endemic burden worldwide; 2010. Available from: https://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf?ua=1.
6. Koo E, McNamara S, Lansing B, et al. Making infection prevention education interactive can enhance knowledge and improve outcomes: results from the Targeted Infection Prevention (TIP) Study. Am J Infect Control. 2016;44(11):1241–1246. doi:10.1016/j.ajic.2016.03.016
7. Olu O, Kargbo B, Kamara S, et al. Epidemiology of Ebola virus disease transmission among health care workers in Sierra Leone, May to December 2014: a retrospective descriptive study. BMC Infect Dis. 2015;15:416. doi:10.1186/s12879-015-1166-7
8. Kiprotich K, Wang H, Kaminga AC, Kessi M. Observed and Self-reported Hand Hygiene Compliances and Associated Factors among Healthcare Workers at a County Referral Hospital in Kenya. Sci Afr. 2021;14:e00984. doi:10.1016/j.sciaf.2021.e00984
9. Nasiri A, Balouchi A, Rezaie-Keikhaie K, Bouya S, Sheyback M, Rawajfah OA. Knowledge, attitude, practice, and clinical recommendation toward infection control and prevention standards among nurses: a systematic review. Am J Infect Control. 2019;47(7):827–833. doi:10.1016/j.ajic.2018.11.022
10. Huang A, Hong W, Zhao B, Lin J, Xi R, Wang Y. Knowledge, attitudes and practices concerning catheter-associated urinary tract infection amongst healthcare workers: a mixed methods systematic review. Nurs Open. 2023;10(3):1281–1304. doi:10.1002/nop2.1384
11. Cutinho MC, Sheilini M, Harish B. Knowledge on practice of urinary catheter care and compliance to urinary catheter care guidelines—A hospital based study. Indian J Public Health. 2018;9(11):218–224. doi:10.5958/0976-5506.2018.01455.9
12. Shehu NY, Onyedibe KI, Igbanugo JS, et al. Hand hygiene knowledge, training and practice: a cross-sectional study in a tertiary health institution, North-central Nigeria. Niger J Clin Pract. 2019;22(7):1008–1013. doi:10.4103/njcp.njcp_204_18
13. Laskar AM, Bhat RD. A multimodal intervention to improve hand hygiene compliance in a tertiary care center. Am J Infect Control. 2018;46(7):775–780. doi:10.1016/j.ajic.2017.12.017
14. Angelozzi A, Caminada S, Dorelli B, et al. Knowledge, attitude, barriers, professional behaviour and possible interventions: a survey on healthcare-associated infections among the healthcare workers of an intensive care unit in a large teaching hospital in Rome. Ann Ig. 2021;33(6):628–643. doi:10.7416/ai.2021.2461
15. Wang J, Liu F, Tartari E, et al. The prevalence of healthcare-associated infections in Mainland China: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2018;39(6):701–709. doi:10.1017/ice.2018.60
16. Sun B. Nosocomial infection in China: management status and solutions. Am J Infect Control. 2016;44(7):851–852. doi:10.1016/j.ajic.2016.01.039
17. Wang J, Liu F, Tan JBX, Harbarth S, Pittet D, Zingg W. Implementation of infection prevention and control in acute care hospitals in Mainland China - a systematic review. Antimicrob Resist Infect Control. 2019;8:32. doi:10.1186/s13756-019-0481-y
18. Liu W, Guo T, Li H, et al. Healthcare-associated infection prevention and control management in a tertiary hospital and an overall evaluation. Ann Palliat Med. 2020;9(4):1536–1544. doi:10.21037/apm-20-65
19. Kim TR, Ross JA, Smith DP. Korea: trends in four national KAP surveys 1964-67. Stud Family Plann. 1969;1(43):6–11. doi:10.2307/1965090
20. Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–1465. doi:10.1001/jama.282.15.1458
21. Dramowski A, Whitelaw A, Cotton MF. Healthcare-associated infections in children: knowledge, attitudes and practice of paediatric healthcare providers at Tygerberg Hospital, Cape Town. Paediatr Int Child Health. 2016;36(3):225–231. doi:10.1179/2046905515Y.0000000032
22. Parmeggiani C, Abbate R, Marinelli P, Angelillo IF. Healthcare workers and health care-associated infections: knowledge, attitudes, and behavior in emergency departments in Italy. BMC Infect Dis. 2010;10:35. doi:10.1186/1471-2334-10-35
23. Ogoina D, Pondei K, Adetunji B, Chima G, Isichei C, Gidado S. Knowledge, attitude and practice of standard precautions of infection control by hospital workers in two tertiary hospitals in Nigeria. J Infect Prev. 2015;16(1):16–22. doi:10.1177/1757177414558957
24. WHO. Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care is Safer Care. Geneva: World Health Organization; 2009.
25. Wałaszek M, Kołpa M, Wolak Z, Różańska A, Wójkowska-Mach J. Poor hand hygiene procedure compliance among Polish medical students and physicians – the result of an ineffective education basis or the impact of organizational culture? Int J Environ Res Public Health. 2017;14(9):1026. doi:10.3390/ijerph14091026
26. Beauducel A, Herzberg PY. On the performance of maximum likelihood versus means and variance adjusted weighted least squares estimation in CFA. Struct Equ Modeling. 2006;13(2):186–203. doi:10.1207/s15328007sem1302_2
27. Kyriazos TA. Applied psychometrics: sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychol. 2018;9(8):2207–2230. doi:10.4236/psych.2018.98126
28. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
29. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
30. Edwards R, Charani E, Sevdalis N, et al. Optimisation of infection prevention and control in acute health care by use of behaviour change: a systematic review. Lancet Infect Dis. 2012;12(4):318–329. doi:10.1016/S1473-3099(11)70283-3
31. Wu W, Wang W, Yuan Y, et al. Knowledge, attitude and practice concerning healthcare-associated infections among healthcare workers in Wuhan, China: cross-sectional study. BMJ Open. 2021;11(1):e042333. doi:10.1136/bmjopen-2020-042333
32. Travers J, Herzig CT, Pogorzelska-Maziarz M, et al. Perceived barriers to infection prevention and control for nursing home certified nursing assistants: a qualitative study. Geriatr Nurs. 2015;36(5):355–360. doi:10.1016/j.gerinurse.2015.05.001
33. Iliyasu G, Dayyab FM, Habib ZG, et al. Knowledge and practices of infection control among healthcare workers in a Tertiary Referral Center in North-Western Nigeria. Ann Afr Med. 2016;15(1):34–40. doi:10.4103/1596-3519.161724
34. Lien TQ, Johansson E, Lan PT, et al. A potential way to decrease the know-do gap in hospital infection control in Vietnam: “Providing specific figures on healthcare-associated infections to the hospital staff can ‘wake them up’ to change their behaviour”. Int J Environ Res Public Health. 2018;15(7):1549. doi:10.3390/ijerph15071549
35. Russell D, Dowding DW, McDonald MV, et al. Factors for compliance with infection control practices in home healthcare: findings from a survey of nurses’ knowledge and attitudes toward infection control. Am J Infect Control. 2018;46(11):1211–1217. doi:10.1016/j.ajic.2018.05.005
36. Nwaokenye J, Lakoh S, Morgan J. Perceptions of Nigerian healthcare workers towards hand hygiene: a qualitative study. Pan Afr Med J. 2020;36:204. doi:10.11604/pamj.2020.36.204.19869
37. Sunkwa-Mills G, Rawal L, Enweronu-Laryea C, Aberese-Ako M, Senah K, Tersbøl BP. Perspectives and practices of healthcare providers and caregivers on healthcare-associated infections in the neonatal intensive care units of two hospitals in Ghana. Health Policy Plan. 2020;35(Supplement_1):i38–i50. doi:10.1093/heapol/czaa102
38. Kretzer EK, Larson EL. Behavioral interventions to improve infection control practices. Am J Infect Control. 1998;26(3):245–253. doi:10.1016/s0196-6553(98)80008-4
39. Zhou Y, Zhang D, Chen Y, et al. Healthcare-associated infections and Shanghai clinicians: a multicenter cross-sectional study. PLoS One. 2014;9(8):e105838. doi:10.1371/journal.pone.0105838
40. Peter D, Meng M, Kugler C, Mattner F. Strategies to promote infection prevention and control in acute care hospitals with the help of infection control link nurses: a systematic literature review. Am J Infect Control. 2018;46(2):207–216. doi:10.1016/j.ajic.2017.07.031
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.