Back to Journals » International Journal of Women's Health » Volume 15
Do Case Reports and Case Series Generate Clinical Discoveries About Preeclampsia? A Systematic Review
Authors Janoudi G ![]() , Uzun (Rada) M, Boyd ST
, Uzun (Rada) M, Boyd ST ![]() , Fell DB, Ray JG, Foster AM
, Fell DB, Ray JG, Foster AM ![]() , Giffen R, Clifford TJ, Walker MC
, Giffen R, Clifford TJ, Walker MC
Received 26 November 2022
Accepted for publication 13 March 2023
Published 21 March 2023 Volume 2023:15 Pages 411—425
DOI https://doi.org/10.2147/IJWH.S397680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ghayath Janoudi,1,2 Mara Uzun (Rada),3 Stephanie T Boyd,1 Deshayne B Fell,2,4 Joel G Ray,5 Angel M Foster,6 Randy Giffen,7 Tammy J Clifford,2,8 Mark C Walker1,2,9– 12
1Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada; 2School of Epidemiology and Public Health, University of Ottawa, Ottawa, ON, Canada; 3Independent Researcher, Ottawa, ON, Canada; 4Children’s Hospital of Eastern Ontario (CHEO) Research Institute, Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada; 5Departments of Medicine, Health Policy Management and Evaluation, and Obstetrics and Gynecology, St Michael’s Hospital, University of Toronto, Toronto, ON, Canada; 6Faculty of Health Sciences, University of Ottawa, Ottawa, ON, Canada; 7IBM Canada, IBM, Toronto, ON, Canada; 8Canadian Institute of Health Research, Government of Canada, Ottawa, ON, Canada; 9International and Global Health Office, University of Ottawa, Ottawa, ON, Canada; 10Department of Obstetrics and Gynecology, University of Ottawa, Ottawa, ON, Canada; 11Department of Obstetrics, Gynecology & Newborn Care, The Ottawa Hospital, Ottawa, ON, Canada; 12BORN Ontario, Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada
Correspondence: Mark C Walker, Clinical Epidemiology Program, Ottawa Hospital Research Institute, Centre for Practice Changing Research, Box 241, 501 Smyth Road, Ottawa, ON, K1H 8L6, Canada, Tel +1 613-798-5555 x76655, Email [email protected]
Background: Preeclampsia is a leading cause of maternal and perinatal mortality and morbidity. The management of preeclampsia has not changed much in more than two decades, and its aetiology is still not fully understood. Case reports and case series have traditionally been used to communicate new knowledge about existing conditions. Whether this is true for preeclampsia is not known.
Objective: To determine whether recent case reports or case series have generated new knowledge and clinical discoveries about preeclampsia.
Methods: A detailed search strategy was developed in consultation with a medical librarian. Two bibliographic databases were searched through Ovid: Embase and MEDLINE. We selected case reports or case series published between 2015 and 2020, comprising pregnant persons diagnosed with hypertensive disorders of pregnancy, including preeclampsia. Two reviewers independently screened all publications. One reviewer extracted data from included studies, while another conducted a quality check of extracted data. We developed a codebook to guide our data extraction and outcomes assessment. The quality of each report was determined based on Joanna Briggs Institute (JBI) critical appraisal checklist for case reports and case series.
Results: We included 104 case reports and three case series, together comprising 118 pregnancies. A severe presentation or complication of preeclampsia was reported in 81% of pregnancies, and 84% had a positive maternal outcome, free of death or persistent complications. Only 8% of the case reports were deemed to be of high quality, and 53.8% of moderate quality; none of the case series were of high quality. A total of 26 of the 107 publications (24.3%) included a novel clinical discovery as a central theme.
Conclusion: Over two-thirds of recent case reports and case series about preeclampsia do not appear to present new knowledge or discoveries about preeclampsia, and most are of low quality.
Keywords: hypertensive disorders of pregnancy, eclampsia, HELLP syndrome, study design
Introduction
Knowledge of diseases, therapeutics, and the human body has been largely gained through the accumulation of clinical observations.1–3 Meticulous observation is the cornerstone of clinical research, and scientific research in general.2–5 Traditionally, case reports and case series have been utilized as a medium to communicate these preliminary clinical observations and discoveries.6–8 These descriptive observational studies serve to generate scientific hypotheses that can then be tested further in comparative study designs.9 Many medical discoveries have first been reported in the literature as case reports or case series. Several examples include lithium’s and chlorpromazine’s psychopharmacological properties,10–12 malignant hyperthermia with dantrolene as its treatment,13,14 toxic shock syndrome and its association with tampon use,15,16 and the description of rare forms of infections and malignancies leading to the discovery of HIV infection.17,18 Most recently, we have witnessed the use of individual clinical observations, communicated in various formats, in the detection and management of COVID-19.19–23
In antiquity, case reports were the main vehicles that physicians used to convey disease descriptions, treatments, and pass teachings.24 The 20th century heralded large advancements in clinical study design and generated a strong debate on the role of case reports and case series. This culminated in the adoption of the evidence-based medicine hierarchy in the 90s that relegated case reports and case series to the bottom of the clinical evidence pyramid.7 Many peer review journals no longer publish case reports. On the other hand, several journals have emerged that are specialized in publishing case reports and case series.7,25 Despite being considered at the bottom of the clinical evidence hierarchy, case reports and case series are an integral part of evidence-based medicine practices.26 This is why in 2014, a working group of researchers and methodologist was formed within The Joanna Briggs Institute (JBI), an international not-for-profit organization that aims to improve the quality of health care through evidence-based practices, to establish critical appraisal tools for case reports and case series.27
The hypertensive disorders of pregnancy are a leading cause of maternal mortality and morbidity worldwide,28 and are responsible for approximately 18% of all maternal deaths globally and affect an estimated 5% to 10% of all pregnancies.29–33 Preeclampsia is one such hypertensive disorder of pregnancy — a pregnancy complication characterized by resistant hypertension with proteinuria or with other adverse conditions or complications.34 Severe forms of preeclampsia can manifest as hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome and untreated preeclampsia can lead to eclampsia.35 Both HELLP and eclampsia are associated with a high degree of morbidity and mortality.36–38 Hypertensive disorders of pregnancy and their associated complications are some of the oldest-ever recorded medical conditions; one of the first descriptions of eclampsia was recorded by Hippocrates in the 5th century BCE.39 Understanding of the pathophysiology of hypertensive disorders of pregnancy has grown since and has advanced considerably in the past two decades, yet the clinical management of preeclampsia has not changed much.40–46 Similarly, preventive approaches to preeclampsia have mostly fallen short, with the exception of the use of aspirin for the prevention of early severe preeclampsia.47–49
Considering the traditional role of case reports and case studies in medicine as a vehicle to communicate new clinical discoveries, we aimed to assess the extent to which recent case reports and case series have communicated clinical discoveries that have advanced our knowledge of preeclampsia through a systematic review. Systematic reviews in case reports and case series are common in the literature and traditionally aim to synthesize and assess rare clinical presentations or serious adverse events.50–52
Methods
We registered this study as a systematic review protocol on the international prospective register of systematic reviews (PROSPERO) under ID number CRD42020209953, with the outlined methods that follow. We added one amendment to the protocol to further clarify exclusion criteria and to define additional terms.
Search Strategy
We developed a detailed search strategy to identify case reports and case series on hypertensive disorders of pregnancy. The search strategy was developed in consultation with a medical information specialist (see Appendix S1) and consisted of controlled vocabulary, as well as keywords. The main search concepts were hypertensive disorders of pregnancy and case reports/case series. We searched two main bibliographic databases: Ovid Embase and Ovid MEDLINE. The search strategy filtered the results for human studies and the English language. Subsequently, we retrieved studies published between 2015 and 2020 for screening. We conducted the search strategy on August 3, 2020, and did not conduct any additional searches or establish alerts.
Study Selection
This systematic review includes case reports or case series in pregnant persons diagnosed with hypertensive disorders of pregnancy. We outline the specific eligibility criteria in Table 1.
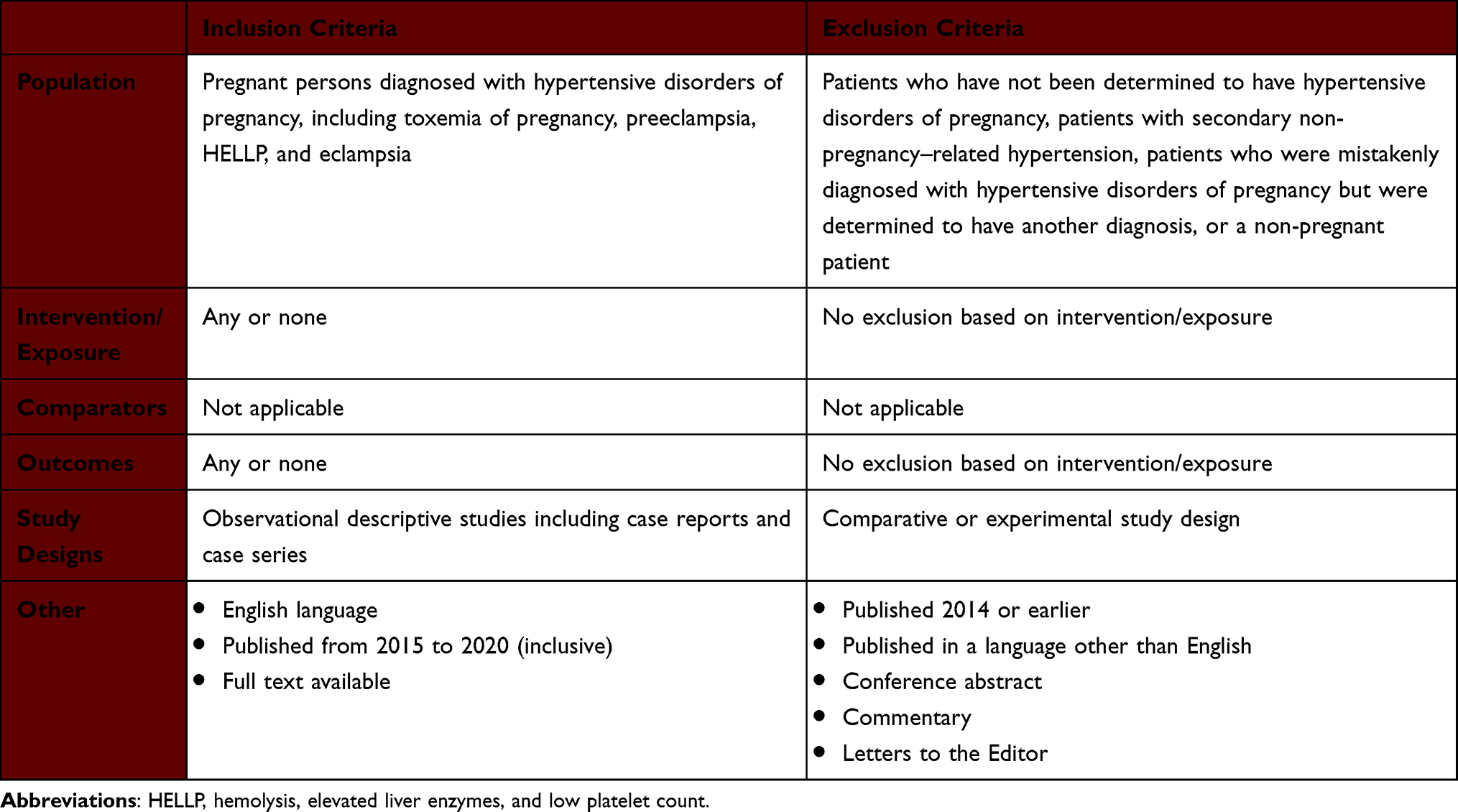 |
Table 1 Inclusion and Exclusion Criteria for the Systematic Review |
Two independent reviewers screened all retrieved records in two stages: title and abstract screening (GJ and SB) and full-text screening (GJ and MU). We resolved rare disagreements through discussion; if we were unable to reach an agreement, we engaged a third independent reviewer (MW) as arbiter.
Data Extraction and Synthesis
The overall data extraction and synthesis process followed a content analysis approach. Upon completion of article selection, we used a random sample of 10 articles to develop a codebook to establish the required data extraction fields, as well as definitions of outcome categories. We used an additional random sample of 10 articles to further refine the codebook, as well as the data extraction sheet. After finalizing the codebook and extraction sheet, GJ performed all extraction and abstraction activities. MU then conducted a data quality check on at least 20% of the extracted data.
For each included article, GJ extracted all data that were relevant to the study design characteristics, patients’ baseline and demographic characteristics, intervention/exposure characteristics, and outcome characteristics.
Based on the information presented within the full text of each included article, GJ determined the severity of each patient’s presentation or complication, the novelty of the exposure that the patient was reported to have experienced, whether the outcome was positive or negative, the reason for publishing the study, and whether a scientific hypothesis as a result of an observation was reported. We provide the definitions of these categories in Table 2.
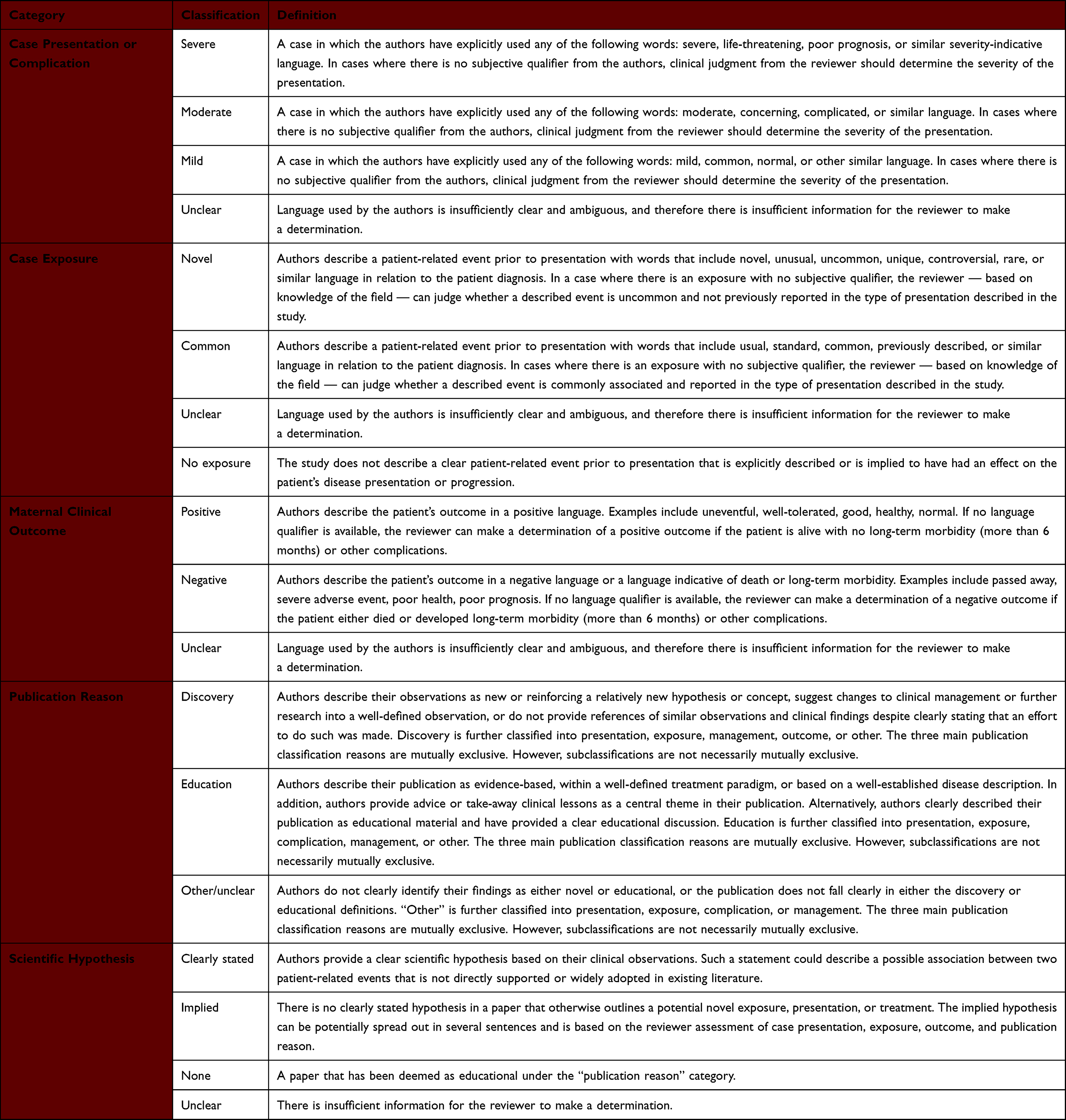 |
Table 2 Outcome Categories, Category Classification, and Associated Definitions |
We provided a descriptive summary of the number of case reports and case series within various categories and classifications. Additionally, we provided a narrative summary of case reports and case series that were determined to have a clinical discovery component. Data collected and used for this review, the codebook, and the extraction sheet are available from the corresponding author upon request.
Quality Assessment
One reviewer (GJ) assessed the quality of the included case reports and case series according to the Joanna Briggs Institute (JBI) critical appraisal Checklist for Case Reports and the JBI critical appraisal Checklist for Case Series.53 The tool consists of eight questions for case reports and 10 questions for case series that are related to the existence or absence of various reported items. We deemed articles with reported items that addressed more than two-thirds of the JBI checklist to be high quality. More than one-third was deemed moderate quality, and less than one-third was deemed to be low quality.
Results
We retrieved a total of 3415 citations from the search strategy. After level 1 title and abstract screening, we selected 303 citations for level 2 full-text screening. After level 2 screening, we included 107 articles in this systematic review.54–160 We provide a flow chart of included and excluded articles in Figure 1.
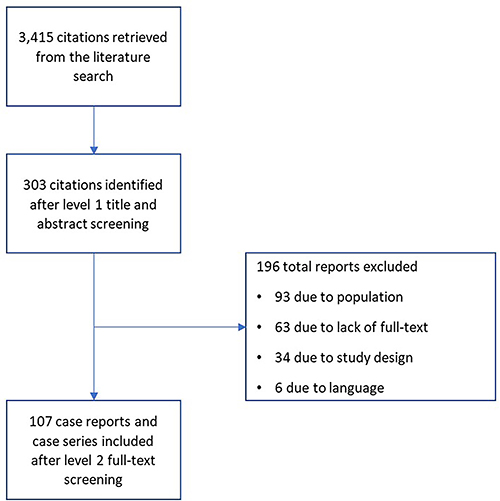 |
Figure 1 Flowchart of included and excluded studies. |
Of the 107 included publications, three were case series105,136,148 and the remainder were case reports. Authors reported on a total of 118 patients in these studies. Our quality assessment of the 104 case reports found that eight reports (8%) were high quality, 56 reports (54%) were moderate quality, and 40 reports (38%) were low quality. We found that the majority of the included case reports addressed two items on the JBI critical appraisal checklist for case reports: the description and presentation of a patient’s history as a timeline (97% addressed this item), and the availability of take-away lessons (93% addressed this item). However, we found that only 17% of the included case reports provided sufficient description of a patient’s demographic characteristics, which is the first item on the JBI checklist. Furthermore, only one-third of the included case reports provided sufficient description of the intervention (30%) and the post-intervention clinical condition (33%). A detailed description of the quality assessment of each included case report is available in Appendix S2.
We considered two of the three case series to be of low quality and one of moderate quality. All of the included case series described valid methods of identifying the condition of interest and two provided sufficient description on appropriate statistical methods used in the case series. A detailed description of the quality assessment of each included case report is available in Appendix S3.
In the included studies, maternal age and gestational age at first presentation were available for 115 patients, with a mean maternal age of 30.1 years (standard deviation [SD]=6.6) and a mean gestational age of 29.7 weeks’ gestation (SD = 6.5). Authors reported information on gravidity for 90 patients: 42 (47%) were primigravida. Authors included a clear presentation complaint for 108 patients; the most common reported symptom on presentation was abdominal pain (n = 33; 31%), followed by headaches (n = 26; 24%). On presentation, the mean systolic blood pressure reported in 92 patients was 163.1 mm Hg (SD = 27.5), while the mean diastolic blood pressure reported in 91 patients was 103.2 mm Hg (SD = 20.0). Authors only sporadically reported on other baseline characteristics, including body mass index, blood laboratory results, urinary laboratory results, liver function tests, and kidney function tests.
The most commonly reported hypertensive disorders of pregnancy diagnoses were preeclampsia (n = 98; 83%), HELLP (n = 40; 34%), hepatic hematoma ― including rupture and infarction (n = 16; 14%), eclampsia (n = 10; 9%), and peripartum cardiomyopathy (n = 6; 5%). The most commonly reported interventions were magnesium sulphate (n = 46; 39%), labetalol (n = 15; 13%), hydralazine (n = 13; 11%), and nifedipine (n = 13; 11%). The authors reported that caesarean section was the method of delivery for 61 patients (52%).
Based on how the authors reported the initial patient presentation in the case report or case series, we determined that a total of 96 patients (81%) had severe clinical presentations or complications during pregnancy, 15 patients (13%) had moderate clinical presentations or complications, and four patients (3%) had mild clinical presentations or complications. We determined there was insufficient information to categorize the severity of the presentations or complications in three patients (2.5%). We were unable to identify an environmental or pharmacological exposure that may have been associated with a patient’s presentation in 105 patients (89%). Based on the description of patients’ clinical outcomes in the included articles, we determined that maternal outcomes were positive in 99 patients (84%), negative in eight patients (7%), and unclear in 11 patients (9%). These categories were defined a priori according to the Methods section and can be viewed in Table 2.
In assessing the publication reasons for the articles we studied, we determined that, of the 107 included articles, 65 (61%) were published as educational material and 26 (24%) as discovery articles; we were unable to determine a clear publication reason for 16 (15%) articles. We present a further breakdown of each classification in Table 3. Of the included studies with a clinical discovery aspect, the following interventions were considered notable ones in the assessment of the reviewers: sildenafil administration in a patient with periviable pregnancy and preeclampsia;70 selective fetal reduction in cases of discordance in dichorionic twin gestations in patients with preeclampsia or HELLP syndrome;87,92 continuous positive airway pressure in patients with obesity, obstructive sleep apnea, preeclampsia, and a high risk of developing severe preeclampsia;107,159 acupuncture therapy in a patient with preeclampsia;109 plasma exchange therapy for patients with HELLP syndrome;121,132 eculizumab in a patient with HELLP syndrome;117 eplerenone in a patient with obesity, obstructive sleep apnea, and preeclampsia;129 pravastatin in a patient with HELLP syndrome;137 and dydrogesterone to prevent preeclampsia in a patient with a history of recurrent preeclampsia.150
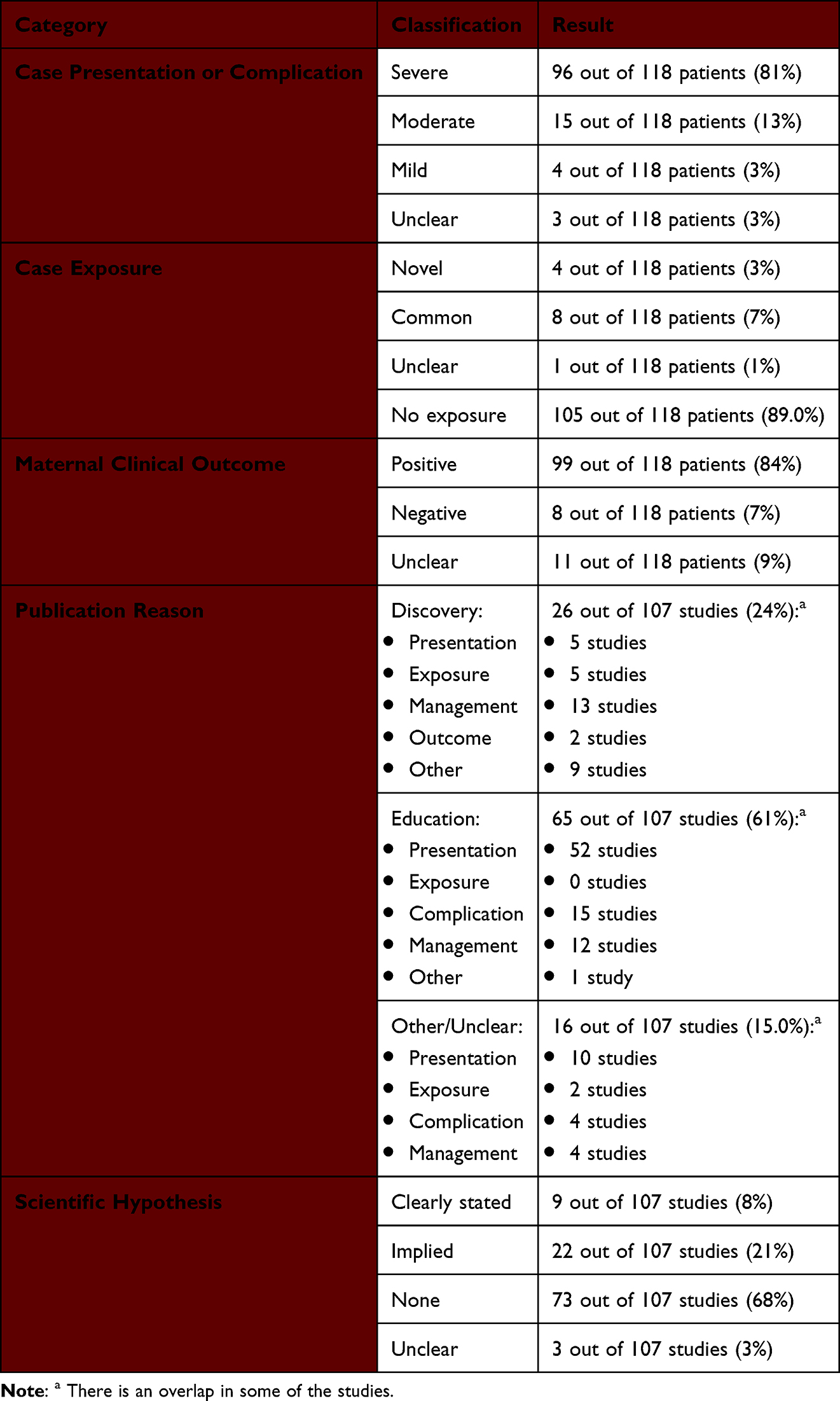 |
Table 3 Outline of the Results |
Authors of the included articles have clearly stated an observation-based scientific hypothesis in nine articles (8%), and we determined that there was an implied scientific hypothesis in 22 articles (21%). Based on our assessment criteria, we determined that the majority of articles (n = 73; 68%) did not include a clearly stated or implied scientific hypothesis. Finally, we were unable to make a determination in three cases (3%). We include a list of the studies that we determined to have reported a clear or implied hypothesis in Appendix S4.
Discussion
Main Findings
To our knowledge and best efforts, we were unable to find a previously published systematic review of case reports and case studies in patients with hypertensive disorders of pregnancy, including preeclampsia. Moreover, we were unable to find published peer-review articles that assessed the extent of clinical discovery contribution of case reports and case series in the field of preeclampsia. Over the period from 2015 to 2020, we identified a total of 104 case reports and three case series reporting on a total of 118 pregnant persons with a diagnosis related to hypertension disorders of pregnancy. Notably, we observed that there is tendency among the included articles to report on patients with severe presentation or complication (81%) and positive maternal outcomes (84%). Indeed, 96 of the 118 patients (81%) that were included in these articles had both a severe presentation or complication and a positive maternal outcome. Further, a sizable majority (61%) of identified manuscripts appeared to be published for educational purposes rather than clinical discovery. We assessed that less than one-third of the included articles were published to communicate a potential clinical discovery (24%).
Interpretation
Case reports and case series can be an important part of the scientific discovery journey by communicating novel clinical observations in a structured and comprehensive manner. Our findings suggest that less than one-quarter of these studies in preeclampsia included a clinical discovery component. This begs the question of how today’s novel clinical observations are being communicated with the larger scientific and clinical communities. Moreover, the tendency in reporting severe presentations and complications, coupled with positive maternal outcome, suggests that these case reports and case series are unlikely to be a representative sample of the population.
An important finding is the overall low adherence of the included case reports and case series to established reporting guidelines. Most pronounced was the lack of sufficient reporting on patients’ characteristics, important measurements of the clinical condition (eg, laboratory results), type of interventions, and post-intervention status. The lack of such information drastically reduces the educational and clinical discovery value of these articles. Ideally, authors should provide sufficient information on all aspects of the clinical encounter with the patients so as to allow clinicians and researchers to understand and potentially replicate or capture the population, intervention, and outcome in future studies. Authors should note any missing information relevant to the disease of which the case report is describing (eg, blood pressure measurement in preeclampsia). Peer-review journals should ideally ensure that case reports and case series are as comprehensively reported as any other form of clinical study design, reporting on patients’ characteristics so as to allow a full understanding of risk factors, potential environmental or pharmaceutical exposures, and all the results of relevant tests or examinations. We have outlined these deficiencies and provided recommendations to address them in Table 4.
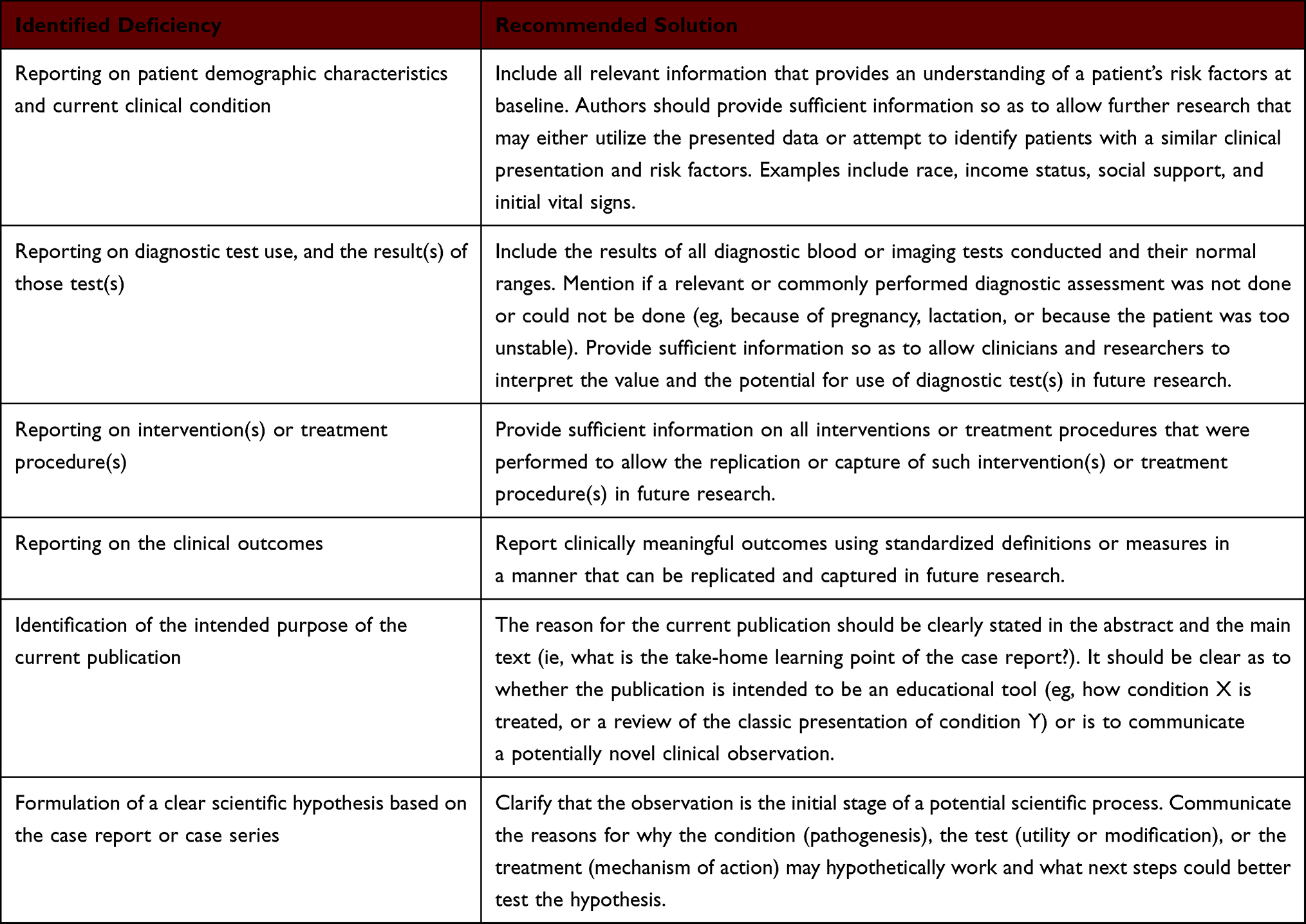 |
Table 4 Identified Deficiencies in the Quality of Reporting of Case Reports and Case Series, and Corresponding Recommended Potential Solutions |
Case reports and case series have known methodological limitations, whereby they are unable to provide any type of valid statistical inference on the population for which the cases are being described. These limitations have been amplified by misinterpreting the communicated clinical observations as a form of confirmatory evidence rather than exploratory findings that require further investigation.161 This has led to the gradual loss of favour of case reports and case series, to the extent that certain journals no longer accept case reports for consideration.162 As our findings suggest, case reports and case series are mostly used as a medium for educational purposes, with little regard to providing the same methodological rigour in comprehensive reporting that is expected from other study designs. This is further devaluing the clinical and scientific value of these important study designs.
As evident by the COVID-19 pandemic, there is an inherent need in the clinical and scientific communities to communicate unusual clinical observations or potentially beneficial forms of clinical management in a new disease area. While some communication of novel clinical observations in relation to COVID-19 have been conducted through the case reports and case series study design approaches, much has occurred in an unstructured manner through various internet-based communication platforms. This may suggest that there is room to rethink the traditional approach of identifying and communicating clinical discoveries.
Strength and Limitations
Through this systematic review, we comprehensively searched and screened all of the identified literature. In addition, we followed a content analysis approach where we developed a codebook to ensure standardization, consistency, and reliability of our data synthesis and assessment.
Limitations in this study include the restriction of the literature search to a five-year period, from 2015 to 2020. This limits the generalizability of our observation to the reviewed period. However, it is arguable that the assessment of the knowledge provided by case series and case reports over a five-year period is sufficient to demonstrate the overall value these methods of scientific communication have in the field of obstetrics. Another limitation is the restriction of our search strategy to the English language. This limits the generalizability of our findings to English-centred obstetrics clinical research. We also included three case reports that were communicated with the publishing journal in a “letter to the editor” format. This represents a minor protocol deviation, where we have excluded study types other than case reports and case series. We included these three case reports, as they were clearly describing clinical encounters with patients in an acceptable case report format.129,140,142 Finally, only a fraction of the included case reports was considered of high quality (7.7%) and none of the case series were of high quality. This reduced our ability to abstract all relevant data and to construct a meaningful picture of all the included articles, which resulted in some studies being classified as “other” or “unclear” in several categories.
Conclusion
In conclusion, our study suggests that the majority of case reports and case series related to hypertensive disorders of pregnancy do not offer new knowledge and are of poor quality. Only one-quarter of published case reports and case series published from 2015 through 2020 centred on a novel clinical observation or discovery and most of these focused on the management of preeclampsia. Lack of comprehensive reporting and an overall medium to low quality of the included studies limited the utility of these reports as viable sources of information for understanding and managing hypertensive disorders of pregnancy.
Funding
We received no funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McWhinney IR. Assessing clinical discoveries. Ann Fam Med. 2008;6(1):3–5. doi:10.1370/afm.801
2. Schulz KF, Grimes DA. The lancet handbook of essential concepts in clinical research. Lancet. 2006;2006:1.
3. Moyé LA. Statistical Reasoning in Medicine: The Intuitive p-value Primer.
4. McWhinney I. Dr Olson’s discovery and the meaning of” scientific”. Can Fam Physician. 2004;50:1192.
5. Newton I. The Principia: Mathematical Principles of Natural Philosophy. Univ of California Press; 1999.
6. Rees J. The fundamentals of clinical discovery. Perspect Biol Med. 2004;47(4):597–607. doi:10.1353/pbm.2004.0068
7. Pimlott N. Two cheers for case reports. Can Fam Physician. 2014;60(11):966–967.
8. Gittelman M. The revolution re-visited: clinical and genetics research paradigms and the productivity paradox in drug discovery. Res Policy. 2016;45(8):1570–1585. doi:10.1016/j.respol.2016.01.007
9. Grimes DA, Schulz KF. Descriptive studies: what they can and cannot do. Lancet. 2002;359(9301):145–149. doi:10.1016/s0140-6736(02)07373-7
10. Cade JF. Lithium salts in the treatment of psychotic excitement. Med J Aust. 1949;2(10):349–352. doi:10.5694/j.1326-5377.1949.tb36912.x
11. Ban TA. Fifty years chlorpromazine: a historical perspective. Neuropsychiatr Dis Treat. 2007;3(4):495–500.
12. Beveridge A. The creation of psychopharmacology by David Healy Cambridge, MA: Harvard University Press. 2002. 480 pp. £26.50 (hb). ISBN0674006194. Br J Psychiatry. 2003;182(2):177. doi:10.1192/bjp.182.2.177
13. Denborough MA, Lovell RRH. Anæsthetic deaths in a family. Lancet. 1960;276(7140):45. doi:10.1016/S0140-6736(60)92690-8
14. Harrison GG. Control of the malignant hyperpyrexic syndrome in MHS swine by dantrolene sodium. Br J Anaesth. 1975;47(1):62–65. doi:10.1093/bja/47.1.62
15. Todd J, Fishaut M, Kapral F, Welch T. Toxic-shock syndrome associated with phage-group-I Staphylococci. Lancet. 1978;2(8100):1116–1118. doi:10.1016/s0140-6736(78)92274-2
16. Todd JK. Toxic shock syndrome--scientific uncertainty and the public media. Pediatrics. 1981;67(6):921–923. doi:10.1542/peds.67.6.921
17. Gottlieb MS, Schanker HM, Fan PT, Saxon A, Weisman JD, Pozalski I. Pneumocystis pneumonia—Los Angeles. MMWR. 1981;30(21):1–3.
18. Hymes KB, Cheung T, Greene JB, et al. Kaposi’s sarcoma in homosexual men-a report of eight cases. Lancet. 1981;2(8247):598–600. doi:10.1016/s0140-6736(81)92740-9
19. Cuello-Garcia C, Pérez-Gaxiola G, van Amelsvoort L. Social media can have an impact on how we manage and investigate the COVID-19 pandemic. J Clin Epidemiol. 2020;127:198–201. doi:10.1016/j.jclinepi.2020.06.028
20. Huang C, Xu X, Cai Y, et al. Mining the characteristics of COVID-19 patients in China: analysis of social media posts. J Med Internet Res. 2020;22(5):e19087. doi:10.2196/19087
21. Pollett S, Rivers C. Social media and the new world of scientific communication during the COVID-19 pandemic. Clin Infect Dis. 2020;71(16):2184–2186. doi:10.1093/cid/ciaa553
22. Wang S, Guo L, Chen L, et al. A case report of neonatal COVID-19 infection in China. Clin Infect Dis. 2020;71(15):853–857. doi:10.1093/cid/ciaa225
23. Andrews MA, Areekal B, Rajesh KR, et al. First confirmed case of COVID-19 infection in India: a case report. Indian J Med Res. 2020;151(5):490–492. doi:10.4103/ijmr.IJMR_2131_20
24. Nissen T, Wynn R. The history of the case report: a selective review. JRSM Open. 2014;5(4):2054270414523410. doi:10.1177/2054270414523410
25. Nissen T, Wynn R. The recent history of the clinical case report: a narrative review. JRSM Short Rep. 2012;3(12):1–5. doi:10.1258/shorts.2012.012046
26. Kidd MR, Saltman DC. Case reports at the vanguard of 21st century medicine. J Med Case Rep. 2012;6(1). doi:10.1186/1752-1947-6-156
27. Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth. 2020;18(10):2127–2133. doi:10.11124/jbisrir-d-19-00099
28. Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010;376(9741):631–644. doi:10.1016/s0140-6736(10)60279-6
29. Hutcheon JA, Lisonkova S, Joseph K. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol. 2011;25(4):391–403. doi:10.1016/j.bpobgyn.2011.01.006
30. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
31. Nakimuli A, Nakubulwa S, Kakaire O, et al. The burden of maternal morbidity and mortality attributable to hypertensive disorders in pregnancy: a prospective cohort study from Uganda. BMC Pregnancy Childbirth. 2016;16(1):205. doi:10.1186/s12884-016-1001-1
32. Lindheimer MD, Taler SJ, Cunningham FG. Hypertension in pregnancy. J Am Soc Hypertens. 2008;2(6):484–494. doi:10.1016/j.jash.2008.10.001
33. Ferrazzani S, Luciano R, Garofalo S, et al. Neonatal outcome in hypertensive disorders of pregnancy. Early Hum Dev. 2011;87(6):445–449. doi:10.1016/j.earlhumdev.2011.03.005
34. Magee LA, Pels A, Helewa M, Rey E, von Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy: executive summary. J Obstet Gynaecol Can. 2014;36(5):416–438. doi:10.1016/s1701-2163(15)30588-0
35. Magee LA, Helewa M, Moutquin J-M, Von Dadelszen P, Committee HG. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can. 2008;30(3 Supplement 1):S1–S48. doi:10.1016/S1701-2163(16)32776-1
36. Ç Ç, Gezgınç K, Altintepe L, et al. Results of the pregnancies with HELLP syndrome. Ren Fail. 2003;25(4):613–618. doi:10.1081/JDI-120022553
37. Sibai BM, Ramadan MK, Usta I, Salama M, Mercer BM, Friedman SA. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). Am J Obstet Gynecol. 1993;169(4):1000–1006. doi:10.1016/0002-9378(93)90043-I
38. Ghulmiyyah L, Sibai B. Maternal Mortality from Preeclampsia/Eclampsia. Elsevier; 2012:56–59.
39. Chadwick J. The Medical Works of Hippocrates: A New Translation from the Original Greek Made Especially for English Readers. Vol. 3. Blackwell; 1950.
40. Bell MJ. A historical overview of preeclampsia-eclampsia. J Obstet Gynecol Neonatal Nurs. 2010;39(5):510–518. doi:10.1111/j.1552-6909.2010.01172.x
41. LaMarca BD, Gilbert J, Granger JP. Recent progress toward the understanding of the pathophysiology of hypertension during preeclampsia. Hypertension. 2008;51(4):982–988. doi:10.1161/hypertensionaha.107.108837
42. Phipps E, Prasanna D, Brima W, Jim B. Preeclampsia: updates in pathogenesis, definitions, and guidelines. Clin J Am Soc Nephrol. 2016;11(6):1102–1113. doi:10.2215/cjn.12081115
43. Roberts JM, Bell MJ. If we know so much about preeclampsia, why haven’t we cured the disease? J Reprod Immunol. 2013;99(1–2):1–9. doi:10.1016/j.jri.2013.05.003
44. Robillard P-Y, Dekker G, Chaouat G, Scioscia M, Iacobelli S, Hulsey TC. Historical evolution of ideas on eclampsia/preeclampsia: a proposed optimistic view of preeclampsia. J Reprod Immunol. 2017;123:72–77. doi:10.1016/j.jri.2017.09.006
45. Grimes S, Bombay K, Lanes A, Walker M, Corsi DJ. Potential biological therapies for severe preeclampsia: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19(1):163. doi:10.1186/s12884-019-2268-9
46. Magee LA, Smith GN, Bloch C, et al. Guideline No. 426: hypertensive disorders of pregnancy: diagnosis, prediction, prevention, and management. J Obstet Gynaecol Can. 2022;44(5):547–571.e1. doi:10.1016/j.jogc.2022.03.002
47. Wen SW, White RR, Rybak N, et al. Effect of high dose folic acid supplementation in pregnancy on pre-eclampsia (FACT): double blind, Phase III, randomised controlled, international, multicentre trial. BMJ. 2018;362:k3478. doi:10.1136/bmj.k3478
48. Xu H, Perez-Cuevas R, Xiong X, et al. An international trial of antioxidants in the prevention of preeclampsia (INTAPP). Am J Obstet Gynecol. 2010;202(3):239.e1–239.e10. doi:10.1016/j.ajog.2010.01.050
49. Roberge S, Bujold E, Nicolaides KH. Aspirin for the prevention of preterm and term preeclampsia: systematic review and metaanalysis. Am J Obstet Gynecol. 2018;218(3):287–293.e1. doi:10.1016/j.ajog.2017.11.561
50. Giusti A, Hamdy NAT, Papapoulos SE. Atypical fractures of the femur and bisphosphonate therapy: a systematic review of case/case series studies. Bone. 2010;47(2):169–180. doi:10.1016/j.bone.2010.05.019
51. Ferrer MF, Torres LG, Ramírez OA, Zarzuelo MR, Del Prado González N. Tuberculosis of the spine. A systematic review of case series. Int Orthop. 2012;36(2):221–231. doi:10.1007/s00264-011-1414-4
52. Posadzki P, Alotaibi A, Ernst E. Adverse effects of aromatherapy: a systematic review of case reports and case series. Int J Risk Saf Med. 2012;24:147–161. doi:10.3233/JRS-2012-0568
53. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Joanna Briggs Institute Reviewer’s Manual. The Joanna Briggs Institute; 2017:2019.
54. Abushoshah I. Spontaneous adrenal hemorrhage and preeclampsia: a case report. Saudi J Anaesth. 2020;14(1):117–119. doi:10.4103/sja.SJA_550_19
55. Al Ghamdi A. Anesthetic management of a parturient with Kearns-Sayre syndrome, dual-chamber and VVI implantable defibrillator pacemaker/defibrillator, and preeclampsia for cesarean delivery: a case report and review of the literature. Saudi J Anaesth. 2018;12(1):134–138. doi:10.4103/sja.SJA_630_17
56. Altalbishi A, Khateb S, Amer R. Elschnig’s spots in the acute and remission stages in preeclampsia: spectral-domain optical coherence tomographic features. Eur J Ophthalmol. 2015;25(5):e84–e87. doi:10.5301/ejo.5000586
57. Aoyagi R, Hayashi T, Tsuneoka H. Choroidal thickening and macular serous retinal detachment in pregnancy-induced hypertension. Int Med Case Rep J. 2015;8:291–294. doi:10.2147/IMCRJ.S95442
58. Araujo J, Penas S, Figueira L, Paiva FP, Falcao-Reis F. Malignant hypertensive retinopathy as a presenting sign of an occult dead fetus. Clin Ophthalmol. 2015;9:971. doi:10.2147/OPTH.S71246
59. Arcot R, Moorthy SN, Rajkumar TR, Ravi A. The liver and foetus at risk- antiphospholipid syndrome and HELLP syndrome. JK Sci. 2015;17(1):49–51.
60. Aronsohn J, Danzer B, Overdyk F, Roseman A. Perimortem cesarean delivery in a pregnant patient with goiter, preeclampsia, and morbid obesity. A&A Case Rep. 2015;4(4):41–43. doi:10.1213/XAA.0000000000000116
61. Artinger K, Hackl G, Schilcher G, et al. The conundrum of postpartum thrombotic microangiopathy: case report and considerations for management. BMC Nephrol. 2019;20(1):91. doi:10.1186/s12882-019-1286-1
62. Atuk FA, Basuni JBM. Molar pregnancy with normal viable fetus presenting with severe pre-eclampsia: a case report. J Med Case Rep. 2018;12(1):140. doi:10.1186/s13256-018-1689-9
63. Balachandar K, Inglis E. The management of severe pre-eclampsia and HELLP syndrome in a twin pregnancy with a known morbidly adherent placenta: a case report. Case Rep Womens Health. 2019;22:e00114. doi:10.1016/j.crwh.2019.e00114
64. Balci S, Bodur T, Tohma YA, Okyay RE, Saatli B, Altunyurt S. Do preeclampsia symptoms resolve after intrauterine death of a fetus? Preeklampsi semptomlari fetal olum sonrasi kaybolur mu? Turk Jinekoloji ve Obstetrik Dernegi Dergisi. 2016;13(2):103–105. Turkish. doi:10.4274/tjod.84770
65. Belen E, Tipi FF, Helvaci A, Bayyigit A. Concurrent early-onset peripartum cardiomyopathy in a preeclampsia patient with acute pulmonary edema. Int Med. 2015;54(8):925–927. doi:10.2169/internalmedicine.54.2714
66. Berdai MA, Labib S, Harandou M. Prolonged neuromuscular block in a preeclamptic patient induced by magnesium sulfate. Pan Afr Med J. 2016;25:5. doi:10.11604/pamj.2016.25.5.6616
67. Bijral N, Qureshi I, Hameed A. A rare cause of postpartum headache. BMJ Case Rep. 2018;2018:bcr-2017–223048. doi:10.1136/bcr-2017-223048
68. Booth S, Eskandar O. A case of partial hydatidiform molar pregnancy with a placental diploid-triploid mosaicism associated with a euploid viable foetus complicated with severe pre-eclampsia. J Obstet Gynaecol. 2018;38(4):580–582. doi:10.1080/01443615.2017.1380613
69. Bradke D, Tran A, Ambarus T, Nazir M, Markowski M, Juusela A. Grade III subcapsular liver hematoma secondary to HELLP syndrome: a case report of conservative management. Case Rep Womens Health. 2020;25:e00169. doi:10.1016/j.crwh.2019.e00169
70. Brownfoot FC, Tong S, Hannan NJ, Cannon P, Nguyen V, Kaitu’u-Lino TJ. Effect of sildenafil citrate on circulating levels of sFlt-1 in preeclampsia. Pregnancy Hypertens. 2018;13:1–6. doi:10.1016/j.preghy.2018.04.011
71. Cagan M, Fadiloglu E, Unal C, Beksac MS. Granulomatosis with polyangiitis and pregnancy: anti-neutrophil cytoplasmic antibody, placental inflammation, chorangiosis and pre-eclampsia. J Obstet Gynaecol Res. 2020. doi:10.1111/jog.14356
72. Cao W, Wang X, Chen T, et al. Successful rescue of antepartum eclampsia in a Chinese patient: case report. Medicine. 2019;98(6):e14301. doi:10.1097/MD.0000000000014301
73. Celik G, Eser A, Gunay M, Yenerel NM. Bilateral vision loss after delivery in two cases: severe preeclampsia and HELLP syndrome. Turk Oftalmoloiji Dergisi. 2015;45(6):271–273. doi:10.4274/tjo.45722
74. Chan C, Mukerji M. Non-gallstone acute pancreatitis and pre-eclampsia: a case report. Case Rep Womens Health. 2018;19:e00063. doi:10.1016/j.crwh.2018.e00063
75. Chen Q, Sousa JD, Snowise S, Chamley L, Stone P. Reduction in the severity of early onset severe preeclampsia during gestation may be associated with changes in endothelial cell activation: a pathological case report. Hypertens Pregnancy. 2016;35(1):32–41. doi:10.3109/10641955.2015.1100309
76. Chenkin J, Heslop CL, Atlin CR, Romano M, Jelic T. Bilateral retinal detachments caused by severe preeclampsia diagnosed with point-of-care ultrasound. Can J Emerg Med. 2016;18(5):395–398. doi:10.1017/cem.2015.76
77. Chou MH, Huang HH, Lai YJ, Hwang KS, Wang YC, Su HY. Cardiac arrest during emergency cesarean section for severe pre-eclampsia and peripartum cardiomyopathy. Taiwan J Obstet Gynecol. 2016;55(1):125–127. doi:10.1016/j.tjog.2015.12.010
78. Dag ZO, Isik Y, Turkel Y, Alpua M, Simsek Y. Atypical eclampsia and postpartum status epilepticus. Pan Afr Med J. 2015;20:17. doi:10.11604/pamj.2015.20.17.5831
79. Davies MJ, Fletcher TL, Cox Bauer CM. Spontaneous ovarian hyperstimulation syndrome in a partial molar pregnancy with early onset severe pre-eclampsia at 15 weeks gestation. Mil Med. 2020;18. doi:10.1093/milmed/usaa008
80. El-Agwany AS. A complicated case of antepartum eclamptic fit with HELLP syndrome, acute renal failure and multiple intracranial hemorrhages: a mortality report. Egypt J Anaesth. 2016;32(2):233–236. doi:10.1016/j.egja.2015.11.004
81. El-Agwany AS, Abdelsadek AA. A rare case of normotensive HELLP syndrome complicated with massive ascites: spontaneous resolution. Egypt J Anaesth. 2016;32(1):155–158. doi:10.1016/j.egja.2015.09.003
82. Escobar Vidarte MF, Montes D, Perez A, Loaiza-Osorio S, Jose Nieto CA. Hepatic rupture associated with preeclampsia, report of three cases and literature review. Review. J Matern Fetal Neonatal Med. 2019;32(16):2767–2773. doi:10.1080/14767058.2018.1446209
83. Essa AA, Feleke LA, Ahmed DM. Semilobar holoprosencephaly with cebocephaly associated with maternal early onset preeclampsia: a case report. J Med Case Rep. 2018;12(1):207. doi:10.1186/s13256-018-1647-6
84. Ferreira BFA, Kreuz AC, Diniz PM, Rocha JVSS, Pimentel SLG. Spontaneous outer retinal layer recovery in a case of hypertensive choroidopathy secondary to pre-eclampsia: a multimodal evaluation. Arq Bras Oftalmol. 2019;82(6):522–527. doi:10.5935/0004-2749.20190100
85. Fervienza A, Bodro M, Castro P, et al. Brain abscess due to Listeria monocytogenes after HELLP syndrome in a patient with antiphospholipid syndrome. Lupus. 2017;26(9):1002–1004. doi:10.1177/0961203316682856
86. Fotiou M, Michaelidou AM, Masoura S, et al. Second trimester amniotic fluid uric acid, potassium, and cysteine to methionine ratio levels as possible signs of early preeclampsia: a case report. Taiwan J Obstet Gynecol. 2016;55(6):874–876. doi:10.1016/j.tjog.2016.09.001
87. Fuchs F, Zaki D, Morin F, Audibert F. Resolution of HELLP syndrome after selective feticide for trisomy 21 in discordant twins - a case report. Case reports. J Obstet Gynaecol. 2016;36(5):663–664. doi:10.3109/01443615.2015.1133576
88. Gainder S, Arora P, Saha SC, Kaman L. Acute pancreatitis with eclampsia-preeclampsia syndrome and poor maternal outcome: two case reports and review of literature. Obstet Med. 2015;8(3):146–148. doi:10.1177/1753495X15585257
89. Ghazali S, Al-Domyati M. Severe hyponatremia and ascites associated with preeclampsia. Crescent J Med Biol Sci. 2019;6(1):132–135.
90. Ghorbanpour M, Makarchian HR, Yousefi B, Taghipour M. Conservative management of postpartum HELLP syndrome and intraparenchymal liver hematoma; a case report. Bull Emerg Trauma. 2019;7(2):196–198. doi:10.29252/beat-070218
91. Grimmett W, Lee J, Doherty J, Cheung B, Chinthamuneedi M, Case A. Report of preeclampsia causing severe hyponatremia: rare or rarely reported? A a Pract. 2019;12(8):261–263. doi:10.1213/XAA.0000000000000904
92. Guerby P, Sartor A, Vidal F, Vayssiere C. Selective feticide as a treatment of severe preeclampsia in discordant twins. J Gynecol Obstet Hum Reprod. 2020;49(1):101633. doi:10.1016/j.jogoh.2019.101633
93. Guo Q, Yang Z, Guo J, et al. Hepatic infarction induced by HELLP syndrome: a case report and review of the literature. BMC Pregnancy Childbirth. 2018;1:191. doi:10.1186/s12884-018-1799-9
94. Hakata S, Umegaki T, Soeda T, et al. Bromocriptine use for sudden peripartum cardiomyopathy in a patient with preeclampsia: a case report. JA Clin Rep. 2019;5(1):38. doi:10.1186/s40981-019-0256-8
95. Halliday E, Tan N. Sensorineural hearing loss and acute vestibulopathy in HELLP syndrome: a case report. Otolaryngol Case Rep. 2017;2:7–9. doi:10.1016/j.xocr.2017.01.002
96. Hassan A. Myasthenia gravis and preeclampsia: dot all the I’s and cross all the T’s. J Taibah Univ Medical Sci. 2017;12(5):461–464. doi:10.1016/j.jtumed.2017.01.006
97. Hauksdottir D, Sigurjonsdottir HA, Arnadottir M, Geirsson RT. Severe, very early onset pre-eclampsia associated with liquorice consumption. Hypertens Pregnancy. 2015;34(2):221–226. doi:10.3109/10641955.2015.1009542
98. Hayashi S, Goto M, Kira S, et al. A patient in whom symptoms of preeclampsia improved after intrauterine fetal death of a co-twin. Int J Gynecol Obstet. 2020;24(2):1–4. doi:10.5580/IJGO.55002
99. Hinkson L, Armbrust R, Moller A, Henrich W. Case report of severe maternal hyponatremia complicating preeclampsia. Case reports. J Matern Fetal Neonatal Med. 2018;31(14):1948–1949. doi:10.1080/14767058.2017.1332032
100. Horazeck C, Crockett CJ. Saved by the massive transfusion protocol: a case report of an obstetric patient with Hemolysis, Elevated Liver Enzymes, and Low Platelet Count (HELLP) syndrome and Glisson capsule rupture. A&A Pract. 2019;12(11):409–411. doi:10.1213/XAA.0000000000000949
101. Horie K, Takahashi H, Fujimoto Y, Kaneko D, Yada Y, Matsubara S. Takotsubo syndrome occurring concomitantly with pre-eclampsia: a case report. J Obstet Gynaecol Res. 2019;45(5):1071–1075. doi:10.1111/jog.13904
102. Hussain SA, O’Shea BJ, Thagard AS. Preeclamptic serous retinal detachment without hypertension: a case report. Case Rep Womens Health. 2019;21:e00098. doi:10.1016/j.crwh.2019.e00098
103. Jugnanden P, Naidoo M, Ngene NC, Moodley J. Primary care providers and hypertension in pregnancy: reflections on a patient encounter. S Afr Fam Pract. 2020;62(1):1–3. doi:10.4102/safp.v62i1.5086
104. Kaltofen T, Grabmeier J, Weissenbacher T, Hallfeldt K, Mahner S, Hutter S. Liver rupture in a 28-year-old primigravida with superimposed pre-eclampsia and hemolysis, elevated liver enzyme levels, and low platelet count syndrome. J Obstet Gynaecol Res. 2019;45(5):1066–1070. doi:10.1111/jog.13941
105. Kanonge TI, Chamunyonga F, Zakazaka N, Chidakwa C, Madziyire MG. Hepatic rupture from haematomas in patients with pre-eclampsia/eclampsia: a case series. Pan Afr Med J. 2018;31:86. doi:10.11604/pamj.2018.31.86.15975
106. Kasai A, Sugano Y, Maruko I, Sekiryu T. Choroidal morphology in a patient with hellp syndrome. Retin Cases Brief Rep. 2016;10(3):273–277. doi:10.1097/ICB.0000000000000249
107. Kim MS, Moon MJ, Lee YH, Chae KY, Ahn EH. Treatment of superimposed preeclampsia on chronic hypertension in a twin pregnancy with automatic continuous positive airway pressure: a case report. BMC Pulm Med. 2020;20(1):157. doi:10.1186/s12890-020-01196-6
108. Kinay T, Fadiloglu E, Akpinar F, Yalvac S, Tapisiz OL. An unusual case of eclampsia at 21 weeks of gestation with multiple risk factors except molar pregnancy. Gazi Med J. 2018;29(2):136–137. doi:10.12996/gmj.2018.37
109. Kocher Z, Hobbs V. Integrating acupuncture for preeclampsia with severe features and HELLP syndrome in a high-risk antepartum care setting. Med Acupunct. 2019;31(6):407–415. doi:10.1089/acu.2019.1399
110. Koseoglu SB, Deveer R, Camuzcuoglu A, Kasap B, Camuzcuoglu H. Massive ascites and pleural effusion in preeclampsia. J Clin Diagn Res. 2017;11(2):QD08–QD09. doi:10.7860/JCDR/2017/22849.9416
111. Kubota-Sjogren Y, Nelson-Piercy C. Fulminant antenatal pulmonary oedema in a woman with hypertension and superimposed preeclampsia. BMJ Case Rep. 2015;2015:A1706. doi:10.1136/bcr-2015-212751
112. Kumarasinghe D, Ratnayake A, Desilva PD, Pinto V. Superior sagittal sinus thrombosis in a patient presenting with pregnancy induced hypertension and eclampsia. Sri Lankan J Anaesthesiol. 2017;25(1):50–52. doi:10.4038/slja.v25i1.8193
113. Kuwabara Y, Yonezawa M, Kubota Y, Ichikawa T, Ohashi R, Takeshita T. Unique clinical and histological features of placental mesenchymal dysplasia complicated by severe preeclampsia in the midtrimester. AJP Rep. 2020;10(1):E113–E117. doi:10.1055/s-0040-1709186
114. Lee M, Kim DI, Lee KH, et al. HELLP syndrome in a pregnant patient with Gitelman syndrome. Kidney Res Clin Pract. 2017;36(1):95–99. doi:10.23876/j.krcp.2017.36.1.95
115. Lee YS, Peng MY, Ker CR, Chan TF. Management of pregnancy in pancreas alone transplant recipient complicated with stage-4 chronic renal insufficiency and superimposed pre-eclampsia: case report and literature review. Taiwan J Obstet Gynecol. 2017;56(5):700–702. doi:10.1016/j.tjog.2017.08.023
116. Loh M, Kathirvel R. An unusual case of severe preeclampsia in the postpartum period with hemoperitoneum. J SAFOG. 2017;9(4):363–366. doi:10.5005/jp-journals-10006-1530
117. Lokki AI, Haapio M, Heikkinen-Eloranta J. Eculizumab treatment for postpartum HELLP syndrome and aHUS-case report. Front Immunol. 2020;11:548. doi:10.3389/fimmu.2020.00548
118. Luna Russo MA, Multani SS, Ridgway M, Martin JN. Second trimester presentation of preeclampsia and choriocarcinoma in a primigravida with live birth. J Matern Fetal Neonatal Med. 2015;28(8):889–891. doi:10.3109/14767058.2014.939623
119. Manning Meurer M, Chakrala K, Gowda D, Burns C, Kelly R, Schlabritz-Loutsevitch N. A case of cannabinoid hyperemesis syndrome with Helicobacter pylori and preeclampsia during pregnancy. Subst Abus. 2018;39(1):9–13. doi:10.1080/08897077.2017.1356790
120. Martingano D, Guan X, Martingano FX. Management of pregnancy and emergency caesarean delivery in a patient with type IIB von Willebrand disease and severe preeclampsia: a case report and literature review. Obstet Med. 2018;11(2):92–94. doi:10.1177/1753495X17720626
121. Martins I, Conceicao MG, Gomes PP, Clode N. Sindrome HELLP sobreposta a sindrome hemolitica-uremica, hemolysis, elevated liver enzymes, low platelets syndrome superimposed on hemolytic uremic syndrome. Rev Bras Ginecol Obstet. 2017;39(4):195–198. doi:10.1055/s-0037-1600124
122. Mathias CR, Rizvi C. The diagnostic conundrum of maternal mirror syndrome progressing to pre-eclampsia - a case report. Case Rep Womens Health. 2019;23:e00122. doi:10.1016/j.crwh.2019.e00122
123. Mikolajczyk AE, Renz J, Diaz G, Alpert L, Hart J, Te HS. Massive hepatic infarction caused by HELLP syndrome. ACG Case Rep J. 2017;4(13):1–2. doi:10.14309/crj.2017.81
124. Millan CA, Forero JC. Right hepatectomy after spontaneous hepatic rupture in a patient with preeclampsia: a case report. Int J Surg Case Rep. 2017;39:250–252. doi:10.1016/j.ijscr.2017.07.057
125. Mor A, Fuchs Y, Zafra K, Haberman S, Tal R. Acute presentation of gestational diabetes insipidus with pre-eclampsia complicated by cerebral vasoconstriction: a case report and review of the published work. Review. J Obstet Gynaecol Res. 2015;41(8):1269–1272. doi:10.1111/jog.12694
126. Morgan J, Della Torre M, Whelan AR, Rodriguez SM, Digiovanni LM. A case of massive hepatic infarction in a patient with HELLP syndrome. AJP Rep. 2019;9(1):E84–E87. doi:10.1055/s-0039-1681028
127. Morisawa H, Hirashima C, Sano M, et al. Difficulty of predicting early-onset super-imposed preeclampsia in pregnant women with hemodialysis due to diabetic nephropathy by serum levels of sFlt-1, PlGF, and sEng. CEN Case Rep. 2020;9(2):101–105. doi:10.1007/s13730-019-00435-y
128. Morisawa H, Makino S, Takahashi H, Sorita M, Matsubara S. Retinal detachment in hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome: color vision abnormality as the first and predominant manifestation. J Obstet Gynaecol Res. 2015;41(11):1835–1838. doi:10.1111/jog.12781
129. Morton A, Laurie J. Eplerenone in the management of resistant hypertension with obstructive sleep apnoea in pregnancy. Letter. Pregnancy Hypertens. 2017;7:54–55. doi:10.1016/j.preghy.2016.12.001
130. Mould A, Abbott S, Welman CJ. HELLP syndrome: an ultrasound case of geographically altered liver parenchymal echogenicity with shear wave elastography, shear wave dispersion and attenuation imaging correlation. Australas J Ultrasound Med. 2020;23(2):149–155. doi:10.1002/ajum.12185
131. Moura C, Amaral L, Mendes J, et al. Hepatic rupture in HELLP syndrome. J Surg Case Rep. 2019;2019(10):rjz277. doi:10.1093/jscr/rjz277
132. Mousseaux C, Joly BS, Mohamadou I, Arrestier R, Hertig A, Severe RC. HELLP syndrome masquerading as thrombocytopenic thrombotic purpura: a case report. BMC Nephrol. 2020;21(1):204. doi:10.1186/s12882-020-01865-y
133. Nakakita B, Mogami H, Kondoh E, Tsukamoto T, Yanagita M, Konishi I. Case of soluble fms-like tyrosine kinase 1 apheresis in severe pre-eclampsia developed at 15 weeks’ gestation. J Obstet Gynaecol Res. 2015;41(10):1661–1663. doi:10.1111/jog.12760
134. Narasimhulu DM, Karakash S, Rankin L, Minkoff H. Resolution of superimposed pre-eclampsia, and improvement in umbilical artery flow in a surviving twin after intrauterine demise of its co-twin. J Obstet Gynaecol Res. 2015;41(9):1473–1477. doi:10.1111/jog.12725
135. Okumura M, Fushida K, Francisco RPV, Schultz R, Zugaib M. Triploid twin gestation with single fetal demise associated with partial mole and pre-eclampsia. Australas J Ultrasound Med. 2017;20(4):174–177. doi:10.1002/ajum.12064
136. Oliveira CA, Moreira de Sa RA, Zamprogno KV, Gutierrez da Matta F, Do Vale Araujo F. Magnesium sulfate and ophthalmic artery Doppler velocimetry in patients with severe preeclampsia: a case series. Case reports. J Med Case Rep. 2017;11(1):326. doi:10.1186/s13256-017-1490-1
137. Otten LA, Van Der Ven K, Kuhr M, Gembruch U, Merz WM. Pravastatin for prevention of HELLP syndrome. Medicine. 2017;96(42):e8229. doi:10.1097/MD.0000000000008229
138. Pacarada M, Gashi AM, Beha A, Obertinca B. One case of severe preeclampsia who died from postpartum complications ten days after caesarian delivery. Ital J Gynaecol Obstet. 2016;28(4):31–33. doi:10.14660/2385-0868-51
139. Pritchard NL, Keane JL. Wound haematoma: the first sign in a case of late postpartum HELLP syndrome. Case Rep Womens Health. 2015;8:1–3. doi:10.1016/j.crwh.2015.08.001
140. Quiros C, Suarez F, Prieto B, Rodriguez V, Vaquerizo O, Alvarez Menendez FV. The importance of angiogenic markers in the differential diagnosis of HELLP syndrome vs. non-HELLP thrombocytopenia. Letter. Clin Chem Lab Med. 2016;54(7):e187–e189. doi:10.1515/cclm-2015-0890
141. Sarkissian S, Khan Y, Farrell D, Constable D, Brem E. Hemophagocytic lymphohistiocytosis in the setting of HELLP syndrome. Clin Case Rep. 2018;6(12):2466–2470. doi:10.1002/ccr3.1828
142. Senthilnathan M, Velayudhan S, Cherian A, Kundra P. Anaesthetic management of a pregnant woman with preeclampsia and Eisenmenger’s syndrome: role of advanced haemodynamic monitoring. Letter. Indian J Anaesth. 2017;61(4):359–360. doi:10.4103/0019-5049.204244
143. Shah JS, Viteri OA, Longo M, Abdallah M, Sibai B. Twin gestation in a Swyer syndrome patient with superimposed pre-eclampsia. J Obstet Gynaecol. 2018;38(5):719–720. doi:10.1080/01443615.2017.1380615
144. Sharma N, Jethani R, Sharma S, Jante V, Agarwal M. Late onset atypical eclampsia: a case report. J Clin Diagn Res. 2019;13(1):QD07–QD08. doi:10.7860/JCDR/2019/39750.12507
145. Shirozu K, Kuramoto S, Kido S, Hayamizu K, Karashima Y, Hoka S. Hematoma after transversus abdominis plane block in a patient with HELLP syndrome: a case report. Case reports. A&A Pract. 2017;8(10):257–260. doi:10.1213/XAA.0000000000000487
146. Si C, Xiuli Z, Li X, Yong J, Ying Z, Kaiguang Z. Life-threatening bleeding from gastric dieulafoy’s lesion in a pregnant woman with hellp syndrome: a case report and literature review. BMC Gastroenterol. 2017;17(1):89. doi:10.1186/s12876-017-0646-1
147. Sienas L, Miller T, Melo J, Hedriana H. Hyperreactio luteinalis in a monochorionic twin pregnancy complicated by preeclampsia: a case report. Case Rep Womens Health. 2018;19:e00073. doi:10.1016/j.crwh.2018.e00073
148. Suryawan A, Handono B, Suryawan AZ, Rahardjo TM. Peripartum cardiomyopathy after cesarean section in women with preeclampsia related to more severe outcome: a case series. Int J Gynecol Obstet. 2020;24(1). doi:10.5580/IJGO.54805
149. Suzuki T, Ichikawa D, Nakata M, et al. Nephrotic syndrome due to preeclampsia before 20 weeks of gestation: a case report. BMC Nephrol. 2020;21(1):240. doi:10.1186/s12882-020-01876-9
150. Takahashi Y, Yamashita T, Morihara R, et al. Emergency caesarean section saved both an anti-musk antibody-positive myasthenia gravis mother with pregnancy-induced hypertension and her premature baby. Int Med. 2017;56(24):3361–3364. doi:10.2169/internalmedicine.8636-16
151. Tanaka M, Tsujimoto Y, Goto K, et al. Preeclampsia before 20 weeks of gestation: a case report and review of the literature. CEN Case Rep. 2015;4(1):55–60. doi:10.1007/s13730-014-0140-3
152. Tolefac PN, Awungafac NS, Minkande JZ. Spontaneous haemorrhagic stroke complicating severe pre-eclampsia in pregnancy: a case report in a resource-limited setting in Cameroon. BMC Pregnancy Childbirth. 2018;18(1):506. doi:10.1186/s12884-018-2157-7
153. Tolera M, Teklu AM, Ahmed A, et al. Use of a qualitative case study to learn lessons from severe preeclampsia causing a maternal near-miss: a case report. J Med Case Rep. 2018;12(1):277. doi:10.1186/s13256-018-1821-x
154. Tran T, Farasat M, Krantz MJ. Subendocardial stress in pre-eclampsia. Ann Noninvasive Electrocardiol. 2020. doi:10.1111/anec.12769
155. Tripathy K, Chawla R, Mutha V, Selvan H. Spontaneous suprachoroidal haemorrhage with exudative retinal detachment in pregnancy-induced hypertension. BMJ Case Rep. 2018;2018:223907. doi:10.1136/bcr-2017-223907
156. Troja A, Abdou A, Rapp C, Wienand S, Malik E, Raab HR. Management of spontaneous hepatic rupture on top of HELLP syndrome: case report and review of the literature. Review. Viszeralmedizin. 2015;31(3):205–208. doi:10.1159/000376601
157. Tskhay VB, Kovtun NM, Schindler AE. Successful prevention of preeclampsia in a high-risk pregnancy using progestogen dydrogesterone: a clinical case. Horm Mol Biol Clin Investig. 2016;27(3):85–88. doi:10.1515/hmbci-2016-0019
158. Vanden Eede M, Schroyens M. Severe tricuspid regurgitation and seizure on postpartum day 10: case report of late postpartum eclampsia. Acta Clin Belg. 2018;73(6):423–426. doi:10.1080/17843286.2018.1431014
159. Whitehead C, Tong S, Wilson D, Howard M, Walker SP. Treatment of early-onset preeclampsia with continuous positive airway pressure. Obstet Gynecol. 2015;125(5):1106–1109. doi:10.1097/AOG.0000000000000508
160. Zhang Z, Lu J, Qin X. Case report: optical coherence tomography can find typical features in pregnancy-induced hypertension with retinopathy. Case reports research support, Non-U.S. Gov’t. Optom Vis Sci. 2019;96(5):372–375. doi:10.1097/OPX.0000000000001369
161. Zeiler FA, Jackson AC. Critical appraisal of the Milwaukee Protocol for rabies: this failed approach should be abandoned. Can J Neurol Sci. 2016;43(1):44–51. doi:10.1017/cjn.2015.331
162. Khan KS, Thompson PJ. A proposal for writing and appraising case reports. BJOG. 2002;109(8):849–851. doi:10.1111/j.1471-0528.2002.01017.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.