Back to Journals » International Journal of Women's Health » Volume 15
Do Attitude, Awareness and Intention to Perform Female Genital Mutilation or Cutting for Their Daughters of Women Healthcare Providers Differ from Mothers in Somalia?
Authors Suluhan D, Keles E ![]() , Mohamud RYH
, Mohamud RYH ![]() , Eker HH, Cimen S, Yakşi N, Yildiz D
, Eker HH, Cimen S, Yakşi N, Yildiz D
Received 22 March 2023
Accepted for publication 29 July 2023
Published 11 August 2023 Volume 2023:15 Pages 1333—1343
DOI https://doi.org/10.2147/IJWH.S411217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Derya Suluhan,1 Esra Keles,2 Rahma Yusuf Haji Mohamud,3 Hasan Hüseyin Eker,4 Sertac Cimen,5 Neşe Yakşi,6 Dilek Yildiz7
1Department of Nursing, Somalia Mogadishu Recep Tayyip Erdoğan Faculty of Health Sciences, Mogadishu, Somalia; 2Department of Gynecologic Oncology, University of Health Sciences Turkey, Kartal Lütfi Kırdar City Hospital, Istanbul, Türkiye; 3Department of Education, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 4Department of Public Health, Somalia Mogadishu Recep Tayyip Erdoğan Faculty of Health Sciences, Mogadishu, Somalia; 5Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, Somalia; 6Department of Public Health, Amasya University School of Medicine, Amasya, Türkiye; 7Department of Pediatric Nursing, Gulhane Faculty of Nursing, University of Health Sciences Turkey, Ankara, Türkiye
Correspondence: Rahma Yusuf Haji Mohamud, Department of Education, Mogadishu Somalia-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia, Tel +252615216313, Email [email protected]
Aim: This study aimed to determine whether there were differences in attitude, awareness, and intention to perform female genital mutilation or cutting for their daughters in the future between female healthcare providers and mothers.
Methods: A comparative cross-sectional study design was used.
Results: A total of 508 women were included in the study. Of the participants, 68.7% (n = 349) were mothers (Group I) who visited the hospital and 31.3% (n = 159) were women healthcare professionals (Group II) [27% (n = 137) nurses and 4.3% (n = 22) doctors]. It was found that 8 (1.6%) of the participants did not have FGM/C and the FGM/C ratio was lower in group II (95%) than in group I (100%) (p < 0.001). In group I, 99.7% (n = 299) of the participants and 30.6% (n = 19) of those in group II reported intending to perform FGM for their daughters in the future (p < 0.001). The reasons for FGM/C most cited by participants were a traditional rite of passage into womanhood (78%), religious requirement (69.3%), and preservation of their virginity until marriage (59.3%). “Stop FGM” was given as a message on FGM/C by 60% of the participants (n = 79) who answered (n = 127, 100%) to open-ended questions.
Conclusion: The results of this study show that female health professionals with higher education and monthly income had less positive perception of their FGM/C and less intention to allow their daughters to undergo FGM/C.
Keywords: female genital mutilation, mothers, nurse, doctor, attitude, intention
Introduction
Female Genital Mutilation or cutting (FGM/C) is defined as “all procedures that involve the partial or total removal of the external genitalia or another injury to the female genital organs (such as stitching of the labia majora or pricking of the clitoris) for non-medical reasons” according to care of women and girls living with female genital mutilation: a clinical handbook based on the World Health Organization (WHO) Guidelines on the management of health complications from female genital mutilation.1 The prevalence report estimated that over 200 million girls and women are living with FGM/C.2,3 Although FGM/C was prohibited by many countries in the Middle East and Africa, this procedure is still too common in several countries such as Somalia, Guinea, Mali, Djibouti, and Sudan in Africa.1,2,4,5 Somali Health and Demographic Survey (2020) reported that almost every Somali woman aged 15–49 has undergone female circumcision.6
UNFPA and UNICEF have jointly led the largest global program to accelerate the elimination of female genital mutilation (FGM) since 2008 because FGM/C violates basic human rights.7 Legal and policy frameworks banning female genital mutilation have been implicated in 14 of the 17 countries supported by the UNFPA-UNICEF Joint Programme. However, FGM/C is practiced for a variety of sociocultural reasons, including respect for tradition, rite of passage, social convention, enhancing fertility, marriageability, ensuring virginity, chastity and faithfulness, cleanliness and beauty, femininity, religion in regions and ethnic groups in which it is practiced common.1,8 The most common reason for FGM/C was reported in a study as a religion by Kaplan et al9 and cultural reasons by Ali.10
Besides genital mutilation has no health benefits and the practice can cause physical, mental, and sexual health problems in female children’s and women’s lives, such as severe pain, bleeding, infection, urinary problems, mental distress, and gynecological and childbirth complications.2,3,6,11 In a study, 41% of health professionals reported that they had seen female children with complications of FGM/C in Gambia.9 Another study from Australia and New Zealand by Moeed et al indicated that 47% of obstetricians and gynecologists and trainees had seen at least one woman or girl with complications related to FGM/C “most commonly” urinary problems, problems in labour and dyspareunia.12
According to the WHO, “healthcare providers should provide girls and women with the best clinical care while avoiding further harm to them. Health professionals have a key role to influence and change attitudes about FGM/C and women’s bodies and rights.1 In addition, they could also consult in the decision-making process about whether a girl or a woman needs to seek further care. As a health-care provider, every contact with a girl or woman who has experienced FGM/C represents an opportunity to provide her with accurate information about her body and health. “In a community in which FGM/C is still common practice, it is important to be aware of the knowledge, attitude, and practice regarding FGM/C of health professionals. Although there are many studies on the determination of FGM/C knowledge, attitudes, and practice (KAP) of health professionals8,9 and mothers,13–15 there is a scarcity of research on KAP of comparison of the outcomes of both two groups.16 This study aimed to determine whether there were differences in terms of attitude, awareness, and intention to perform female genital mutilation or cutting for their daughters in the future between women healthcare providers and mothers. The outcomes of the present study could provide insight into the views of women with or without health education.
Methods
Study Design
A comparative cross-sectional study design was used.
Study Setting
This comparative cross-sectional study was conducted in Mogadishu, Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital between October 2022 and January 2023. The hospital is one of the largest tertiary referral healthcare facilities in Mogadishu, East Africa. The hospital serves pediatric patients in the newborn intensive care unit with 18 beds and a pediatric intensive care unit with eight beds. The hospital also provides service with 54 beds and three pediatric outpatient clinics since 2015.
Participants
The participants in this study were women health professionals and mothers. A total of 508 women were included in the study, of which 68.7% (349) were women admitted to the hospital and 31.3% (159) were healthcare professionals. In post hoc power analysis using G-Power software, the power of the study was found to be 98.7% with 508 participants (Group I: 349 and Group II: 159), 0.05 alpha error, the 100% and 95% incidence rate of the event (having FGM/C) for Group I and Group II, respectively (Supplementary Figure 1).
Group I (Mothers)
The population of this group included 8236 mothers admitted for acute health conditions of their children to the pediatric outpatient clinics of the hospital between October 7, 2022, and January 15, 2023. Of those, 349 (%4.3) mothers agreed to take part in this study. Inclusion criteria for group I were (i) being mothers, (ii) aged over 18 years, (iii) being able to give informed consent, and (iv) applying to the pediatric outpatient clinics of the hospital. Exclusion criteria included fathers in the present study.
Group II (Female Health Professionals)
Between October 2022 and January 2023, 159 women health professionals in group II filled out the questionnaire, including 27% (n = 137) nurses and 4.3% (n = 22) doctors. Inclusion criteria for female health professionals were (i) being a women health professional and (ii) voluntary participation in the study. Inclusion criteria for mothers were (i) visiting the pediatric outpatient clinic of the hospital for acute health conditions of her child and (ii) voluntarily participating in the study. Exclusion Criteria for both women health professionals and mothers included (i) being male participants.
Data Collection Form
The form content was developed based on a handbook by the WHO (2018) entitled “Care of Girls & Women Living with Female Genital Mutilation: A Clinical Handbook”.1 This form consisted of both open-ended and closed questions addressing sociodemographic characteristics, types of FGM/C, perceptions, and attitudes towards FGM/C, complications related to FGM/C, and intention to practice FGM/C for their daughters (Supplementary Data Collection Form).
Procedure
The data of female health professionals and mothers were collected by four data collectors. Data collectors who were third-year nursing students who volunteered to be data collectors in this study were trained by the same researcher (DS) for three days on the familiarization of the questionnaire, interview techniques, and data collection procedure, and they delivered the questionnaire to female health professionals and mothers. Data were collected through face-to-face interviews using a structured questionnaire. The principal investigator checked the filled questionnaires daily for completeness, accuracy, and consistency.
Ethical Permissions
The study was approved by the Non-Interventional Clinical Research Ethics Committee of XX (Approval number: MSTH −12,097, Date: October 17, 2022). All participants were informed about the purpose of the study and were assured of anonymity and confidentiality of the data. Written and verbal informed consent was obtained from all participants.
Statistical Analysis
Collected data were analyzed using the Epi info 7.2 software. Descriptive data were expressed with numbers (n), percentages (%), median, minimum (min), and maximum (max) values. The distribution property of the continuous data was evaluated with the Kolmogorov–Smirnov test. The x2 test or Fisher’s exact test was used to compare two categorical variables, and Mann–Whitney U-tests were used for two-group comparisons. Statistical significance was accepted as p < 0.05.
Results
The sociodemographic characteristics of the participants are shown in Table 1. A total of 508 women were included in the study. Of the participants, 68.7% (n = 349) were mothers (Group I) admitted to the hospital and 31.3% (n = 159) were female healthcare professionals (Group II) [27% (n = 137) nurses and 4.3% (n = 22) doctors]. It was found that 8 (1.6%) of the participants did not have FGM/C and the FGM/C ratio was lower in group II (95%) than in group I (100%) (p < 0.001). Type 2 FGM/C was most commonly performed in both groups (p < 0.001). Although the frequency of FGM/C is high in healthcare workers, it was observed that positive perception of their FGM/C was significantly lower in healthcare workers (3.8%) than in mothers (99.7%) (p < 0.001). While pain, bleeding, infection, swelling in the genital area, and painful or difficult urination were more common in the mother group (p < 0.001), psychological conditions were more common in the healthcare worker group according to self-reported (p = 0.003).
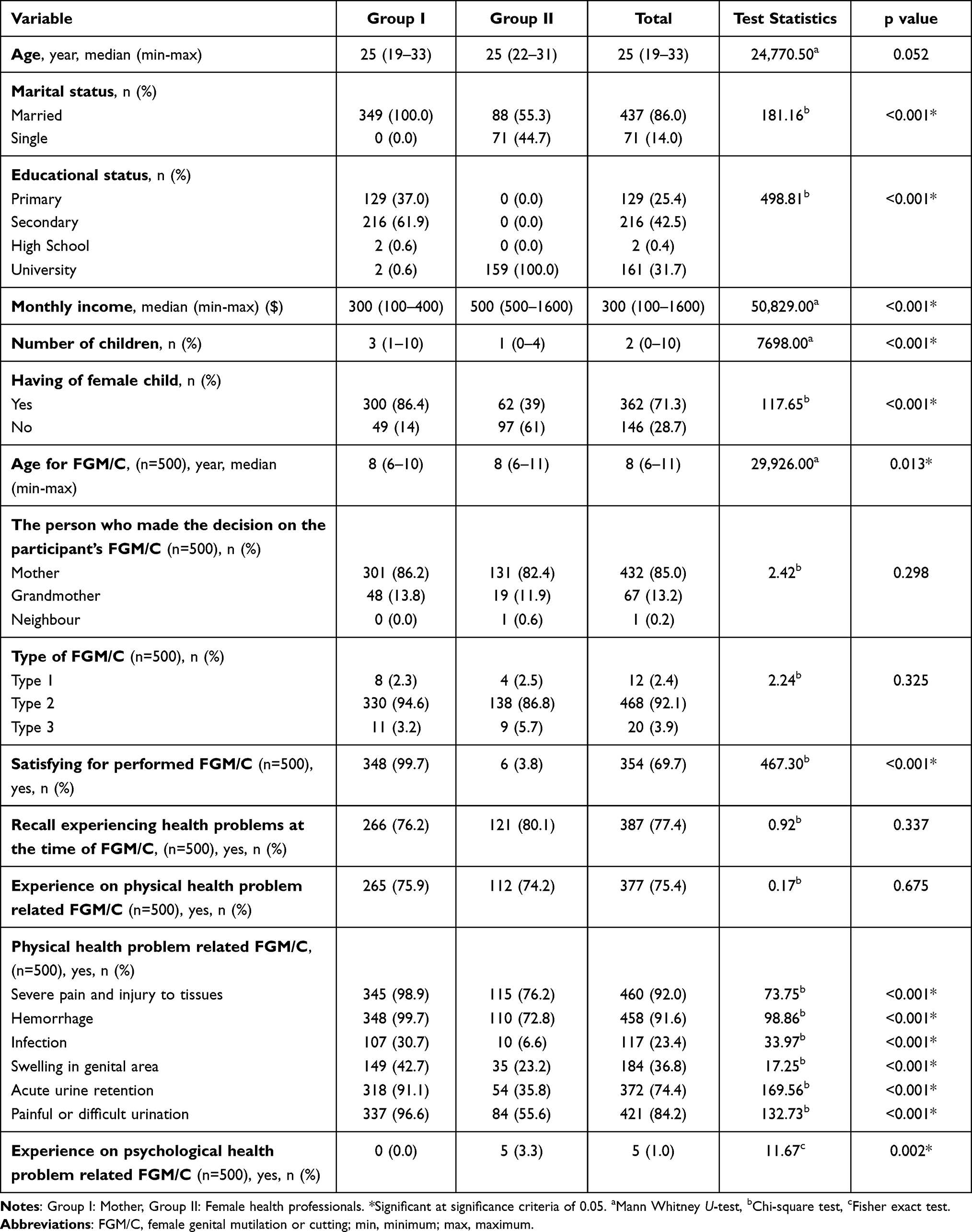 |
Table 1 Comparison Sociodemographic Characteristics, FGM/C-Related Characteristics and FGM/C Complications of Participants According to Groups (n = 508) |
Ninety-nine percent (n = 299) of the participants in group I and 30.6% (n = 19) of participants in group II group reported that they intended to perform the FGM/C for their daughters in the future in Table 2 (p < 0.001). Fifty-three percent of the participants in group I and 22.6% in group II had daughters with FGM/C (p < 0.001), with Type 2 being the most prevalent FGM/C type in both groups (p < 0.001). In terms of complications, physical problems, pain, hemorrhage, swelling in the genital area, acute urine retention, and acute urine retention were reported as more common physical health conditions in the daughters of participants in group I (p < 0.05) than in the daughters of participants in group II (p < 0.05) (Table 2).
 |
Table 2 Comparison of the Distributions of Participants’ FGM/C Intention for Their Daughters, FGM-Related Complications, and Characteristics of FGM/C Practice |
Female health professionals had less positive perception for their FGM/C and had less intention to allow their daughters to undergo FGM/C. The number of children with FGM/C of participants in Group I was more than those of Group II (Table 3).
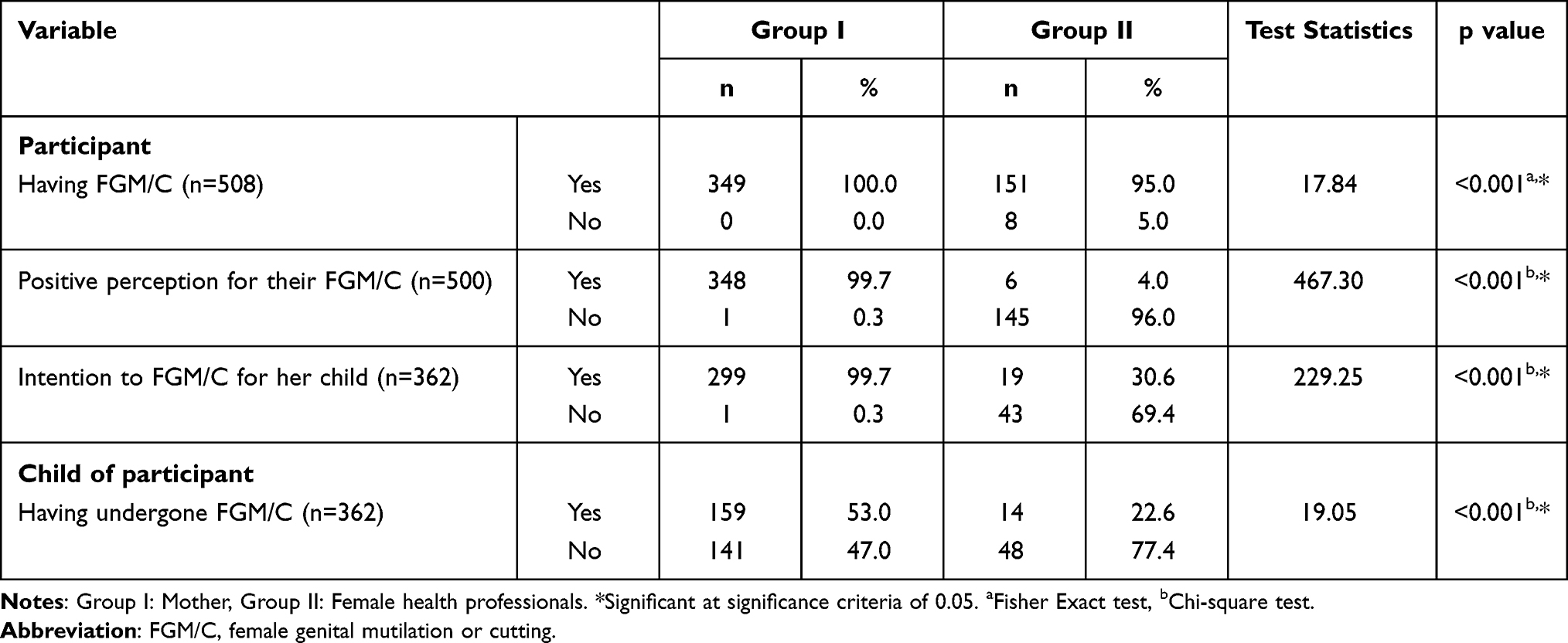 |
Table 3 Comparison of Having FGM/C, Positive Perception for Their FGM/C and Intention to FGM/C for Her Child |
In the comparison of FGM/C status and the participants’ sociodemographic characteristics, FGM/C was more common in those who were married (p = 0.016), had a low-income level (p < 0.001), and had more children (p = 0.003) (Table 4). Positive perception for their FGM/C was higher in married participants than single participants, primary school graduates compared to those with secondary school or higher education graduates (p < 0.001), those with lower income than those with higher income (p < 0.001), those with more children than those with fewer children (p < 0.001), and those with daughters than those without daughters (p < 0.001) (Table 4).
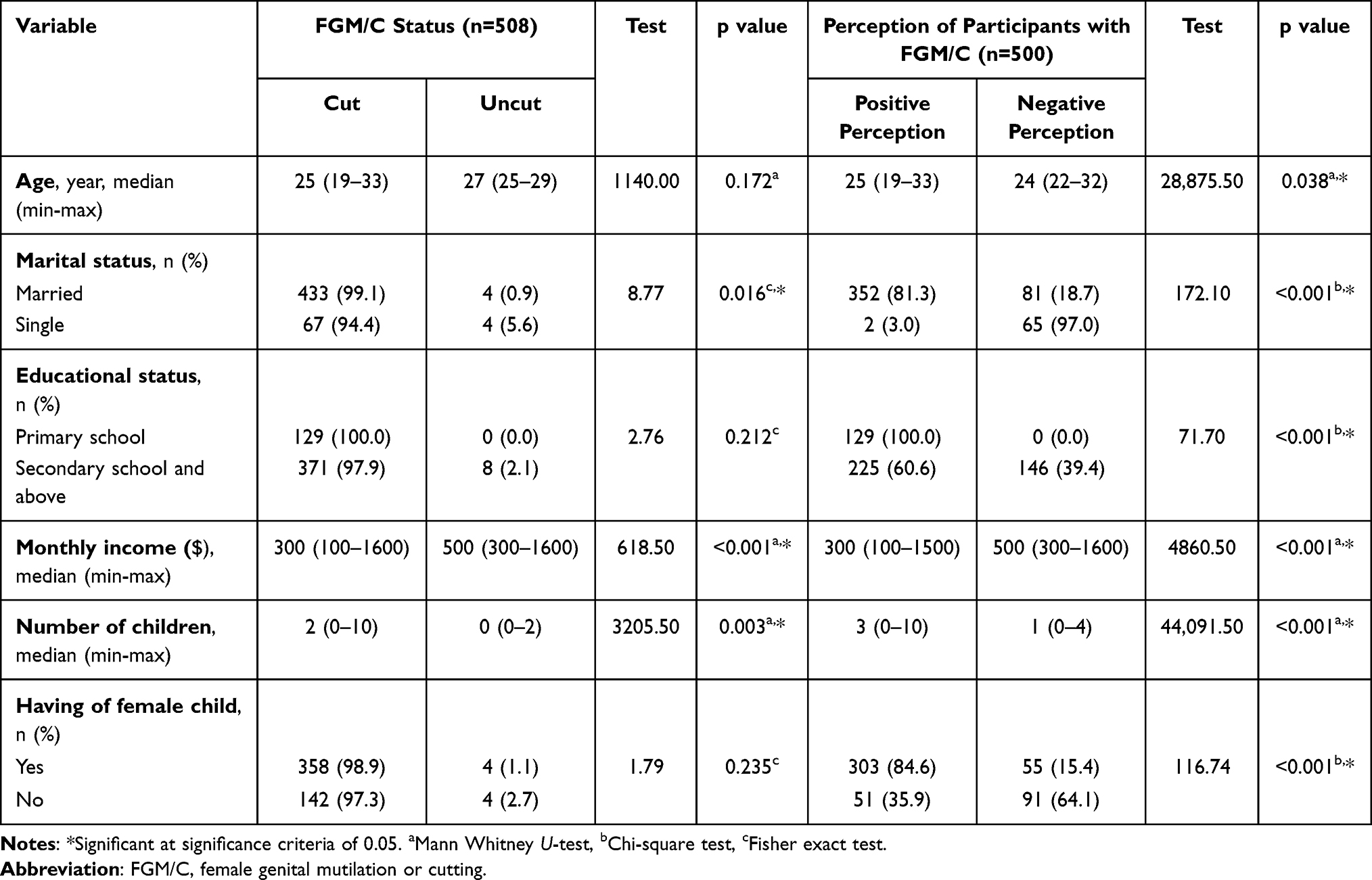 |
Table 4 Comparison of Participants’ Self-FGM/C Status and Perception with FGM/C According to Characteristics of Participants |
It was found that those who had their daughters undergo FGM/C were older (p < 0.001), had a lower education level (p < 0.001), had lower monthly income (p < 0.001), and had more children (p < 0.001) (Table 5). In addition, participants with low education levels (p < 0.001), low income (p < 0.001), and those with more children (p < 0.001) had a higher intention to allow their children to undergo FGM/C (Table 5).
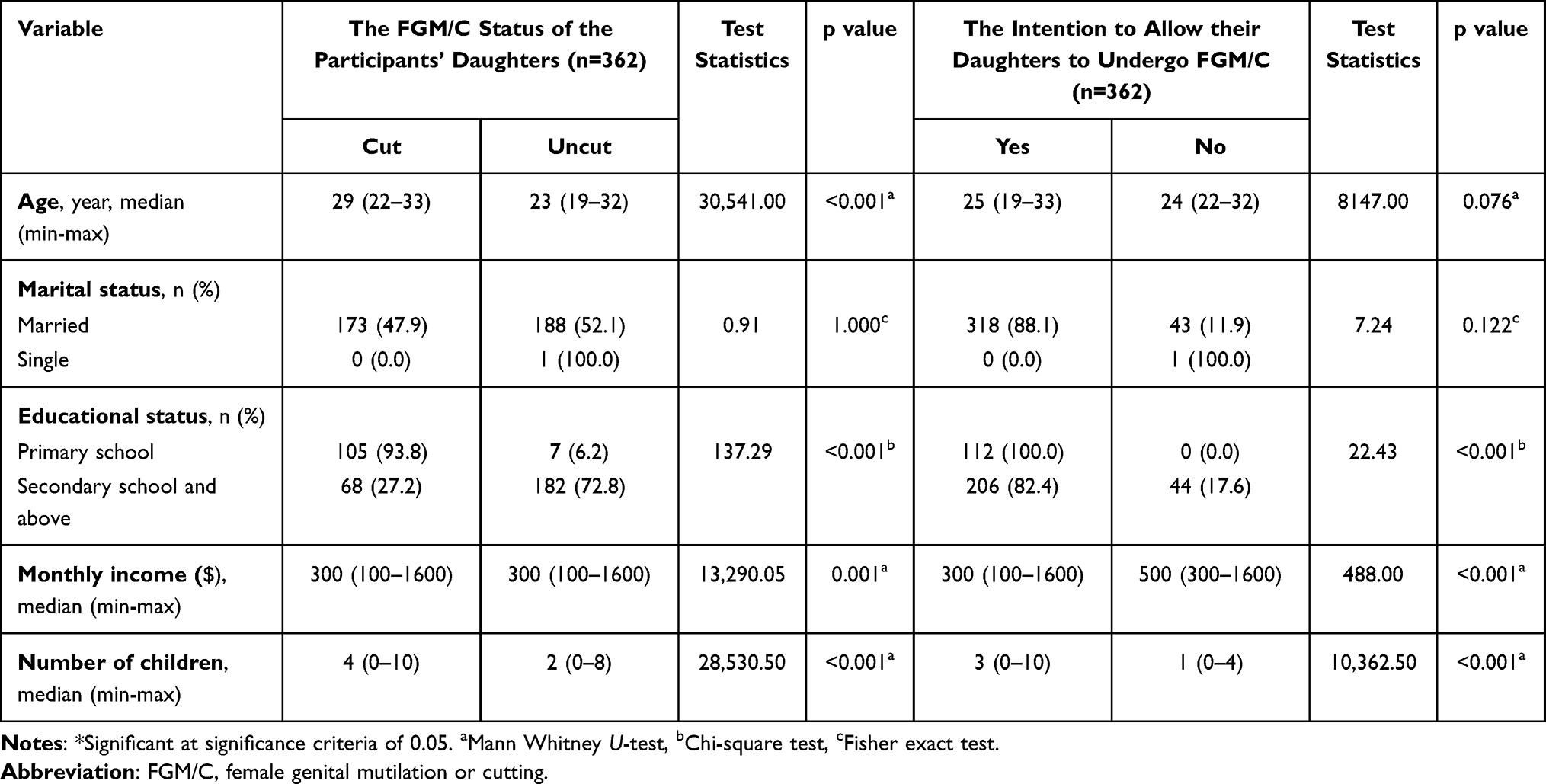 |
Table 5 Comparison of the FGM/C Status of the Participants’ Daughters and Their Intention to Allow Their Daughters to Undergo FGM/C, and Their Sociodemographic Characteristics |
Seventy-eight percent of the participants perceived FGM/C as a rite of passage, 69.3% as a religious requirement, 59.3% as preservation of their virginity until marriage, 0.4% as being more feminine and beautiful, and 1.2% as being more hygienic and more beautiful, as well as provision of spiritual purity. The opinions of the participants about FGM/C are shown in Figure 1.
 |
Figure 1 Views of participants on FGM/C (n = 508). Abbreviation: FGM/C, female genital mutilation/cutting. |
When participants were asked to describe FGM/C, 60% (n = 76) answered “Stop FGM”, 16% (n = 21) “Biggest problem for women”, 14% (n = 18), “Trouble”, and 13% (n = 17), “No to FGM”. The distribution of participants’ perceptions of FGM/C is shown in Figure 2.
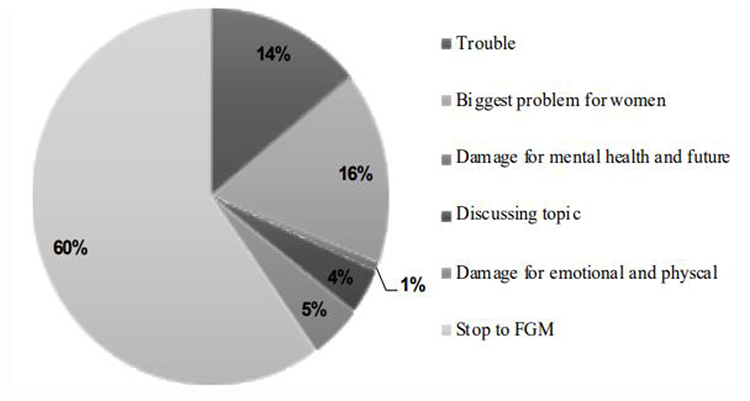 |
Figure 2 Message of participants on FGM/C (n = 127). Abbreviation: FGM/C, female genital mutilation/cutting. |
Discussion
The International Continence Society (ICS, 2018) has emphasized that FGM/C violates basic human rights. However, FGM/C is a common sociocultural practice in many countries (Payne CK). The prevalence of FGM/C varies from 0.3% to 99.2% in the African region.17 In a study, the prevalence of FGM/C among women and girls ages 15 to 49 years old in Egypt was 87%,18 FGM/C is still practiced in Somalia.19 According to the Somalia Health and Demographic Survey,6 99.2% of women have undergone FGM/C. A systematic review and meta-analysis study showed that the prevalence of FGM/C for both women and girls in 26 countries of Africa region has decreased while the prevalence for women in three countries including Somalia, Guinea-Bissau, Burkina Faso of Africa region has increased.17 Almost all mothers and female health professionals in this study have undergone FGM/C. This result presents substantial evidence for health policymakers and professionals that there is a need for interventions and policies to prevent performing FGM/C for children and women in Mogadishu.
In this study, the female health professionals stated that they were positively perception for their FGM/C, and they had experienced more physical health problems related to their self-FGM/C than mothers. A study of Keles et al found that educated women were aware of the adverse health effects of FGM/C.14 One of the associated factors of having FGM/C is socioeconomic status.20 A study conducted by Elduma showed that women from poorer households were more prone to practice FGM/C than those from wealthier households.20 This could show that female health professionals have easier access to knowledge and social media due to their educational and economical status than mothers with low education status.
This study has indicated that mothers and grandmothers were the primary decision makers for FGM/C. Regarding the key role of mothers and grandmothers in FGM/C, the results are similar to those reported by Abathun et al,21 Pashaei et al,22 Tag-Eldin et al,23 Shell-Duncan et al,24 Bjalkander et al25 and Herieka and Dhar.26 According to our findings, there is a need for educational programs for mothers and grandmothers who have a pivotal role as decision-makers on FGM/C of female children.
Beliefs about the reasons for performing FGM/C are cultural, religious requirements, social, medical, economic, and cosmetic.8 Muhula showed that girls who did not undergo FGM were considered to be children since they did not have the traditional rite of passage into womanhood. In the same study, a participant stated that
Some of us we are big girls but are going to school. We seat with circumcised girls in class. They under look at us only that they consider themselves as women and we are a girl. They will not dare even seat with you.27
Similar to the study of Muhula, three of the four participants cited as a rite of passage to womanhood for girls as the reason for FGM/C in our study. The second reason cited by 69.3% of participants was a religious requirement. According to the Somalia Health and Demographic Survey,6 72% believed that female circumcision was a religious requirement. In a study by Gele et al, almost all of the participants believed that FGM/C is a religious requirement for their culture.27
One of the reasons for FGM/C was virginity until marriage in this study. Similarly, in a study conducted in Somalia by Gele et al,27 a participant mentioned that men preferred to marry circumcised women. These reasons show that social pressure, stigmatization toward uncircumcised in society and religious beliefs contribute significantly to the practice of FGM/C.28,29 The findings of our study are in line with other studies,30 which point to daughters of participants in mothers have more undergone FGM/C than those in women health professionals and the intention to allow their daughters to undergo FGM/C has been higher in mothers than women health professionals in our study. In addition to higher education, women health professionals with higher monthly income were less likely to perform FGM/C on their daughters. This result was similar to the studies of Muhula et al28 and Setegn et al.29 These studies revealed that women who had higher education level and wealth were less supportive of the continuation of the practice of FGM. In another study conducted by Ameyaw et al,31 women with higher education levels had less intentions to perform FGM/C on their daughters. Sabahelzain et al32 indicated that education was critical in influencing mothers’ attitudes towards the practice of FGM/C.
Over half of the participants who answered the open-ended question related to the message for readers towards FGM/C practice stated “stop to FGM/C”, while only a few participants thought FGM/C was a distinguishing issue. In a study conducted by Adigüzel et al, almost all of the participants thought that FGM/C is a harmful traditional practice that should be stopped.33 The most highly cited message from both mothers and women health professionals in our study is a clue to the need for help for female children and an increase in interventional educational programs for mothers and older women in Mogadishu.
There are two limitations of the study. First, the results showed the attitudes of only female health professionals towards FGM/C. There is need to studies including male health professionals with high educational status. Second, the outcomes of our study could show the prevalence of FGM/C. Also, the study was limited to a single health center, and a restricted group, which may have been a limitation as well. Hence, the findings of this study should be interpreted with these limitations in mind.
Conclusion
This study compared Somalian mothers and female health professionals in terms of attitude towards FGM/C and intention to allow their daughters to undergo FGM. The results of this study show that female health professionals who have high education and monthly income are aware of the psychological conditions related FGM/C, and they have less intention to allow their daughters to undergo FGM/C. Our study reveals crucial insight about a key role of female health professionals for policy implications. The female health professionals have greater responsibility for empowering women who visit hospitals through educational interventions regarding FGM/C-related complications including physical and psychological health problems of mother and their children. It is recommended that women health professionals who are aware of the complications of FGM/C and they have less intention to allow their daughters to undergo FGM/C should be engage with policymakers to accelerate the elimination of female genital mutilation (FGM) for healthy future of female children.
Data Sharing Statement
The dataset used and/or analyzed in the study is available from the corresponding author on reasonable request.
Ethical Statement
Ethical approval for this study was provided by the Somalia. Mogadishu–Turkey Recep Tayyip Erdogan Training and Research Hospital Ethics Committee (Approval number: MSTH −12097). The database management in accordance with privacy legislation and the presented study in accordance with the ethical principle of the Declaration of Helsinki.
Acknowledgments
The authors would like to thank the study participants for their contribution.
Funding
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Disclosure
The authors report no conflicts of interest.
References
1. World Health Organization. Care of Women and Girls Living with Female Genital Mutilation: A Clinical Handbook. Geneva: World Health Organization; 2018.
2. The Lancet Public Health. COVID-19 hindering progress against female genital mutilation. Lancet Public Health. 2021;6(3):e136. doi:10.1016/S2468-2667(21)00030-X
3. UNICEF. Female genital mutilation/cutting: a global concern. New York: UNICEF; 2016. Available from: https://data.unicef.org/resources/female-genital-mutilationcutting-global-concern/.
4. Khosla R, Banerjee J, Chou D, Say L, Fried ST. Gender equality and human rights approaches to female genital mutilation: a review of international human rights norms and standards. Reprod Health. 2017;14(1):59. doi:10.1186/s12978-017-0322-5
5. Waigwa S, Doos L, Bradbury-Jones C, Taylor J. Effectiveness of health education as an intervention designed to prevent female genital mutilation/ cutting (FGM/C): a systematic review. Reprod Health. 2018;15(1):62. doi:10.1186/s12978-018-0503-x
6. Somalia National Bureau of Statistics. Federal Government of Somalia. The Somali Health and Demographic Survey; 2020. Available from: https://somalia.unfpa.org/sites/default/files/pub-pdf/shds_report_2020_1.pdf.
7. OHCHR, UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCR, UNICEF, UNIFEM, WHO. Eliminating female genital mutilation: an interagency statement; 2008. Available from: https://apps.who.int/iris/handle/10665/43839.
8. Zurynski Y, Sureshkumar P, Phu A, Elliott E. Female genital mutilation and cutting: a systematic literature review of health professionals’ knowledge, attitudes and clinical practice. BMC Int Health Hum Rights. 2015;15:32. doi:10.1186/s12914-015-0070-y
9. Kaplan A, Forbes M, Bonhoure I, et al. Female genital mutilation/cutting in The Gambia: long-term health consequences and complications during delivery and for the newborn. Int J Womens Health. 2013;5(1):323–331. doi:10.2147/IJWH.S42064
10. Ali AA. Knowledge and attitudes of female genital mutilation among midwives in Eastern Sudan. Reprod Health. 2012;9:23. doi:10.1186/1742-4755-9-23
11. World Health Organization. Female genital mutilation: integrating the prevention and the management of the health complications into the curricula of nursing and midwifery: a teacher’s guide. Geneva: World Health Organization; 2001 Available from: https://apps.who.int/iris/handle/10665/66857.
12. Moeed SM, Grover SR. Female genital mutilation/cutting (FGM/C): survey of RANZCOG fellows, diplomates & trainees and FGM/C prevention and education program workers in Australia and New Zealand. Aust N Z J Obstet Gynaecol. 2012;52(6):523–527. doi:10.1111/j.1479-828X.2012.01476.x
13. Van Eekert N, Van de Velde S, Anthierens S, et al. Mothers’ perceptions of the medicalisation of female genital cutting among the Kisii population in Kenya. Cult Health Sex. 2022;24(7):983–997. doi:10.1080/13691058.2021.1906952
14. Keles E, Eker HH, Bektemur G, et al. Determinants of disagreement with female genital mutilation among mothers. Int J Womens Health. 2022;14:1863–1870. doi:10.2147/IJWH.S391043
15. Melese G, Tesfa M, Sharew Y, Mehare T. Knowledge, attitude, practice, and predictors of female genital mutilation in Degadamot district, Amhara regional state, Northwest Ethiopia, 2018. BMC Women's Health. 2020;20(1):178. doi:10.1186/s12905-020-01041-2
16. El-Gibaly O, Aziz M, Abou Hussein S. Health care providers’ and mothers’ perceptions about the medicalization of female genital mutilation or cutting in Egypt: a cross-sectional qualitative study. BMC Int Health Hum Rights. 2019;19(1):26. doi:10.1186/s12914-019-0202-x
17. Farouki L, El-Dirani Z, Abdulrahim S, Akl C, Akik C, McCall SJ. The global prevalence of female genital mutilation/cutting: a systematic review and meta-analysis of national, regional, facility, and school-based studies. PLoS Med. 2022;19(9):e1004061. doi:10.1371/journal.pmed.1004061
18. Ministry of Health and Population [Egypt]. El-Zanaty and Associates [Egypt], and ICF International. Egypt Health Issues Survey. Cairo and Rockville: Ministry of Health and Population and ICF International; 2015.
19. Payne CK, Abdulcadir J, Ouedraogo C, et al. International continence society white paper regarding female genital mutilation/cutting. Neurourol Urodyn. 2019;38(2):857–867. doi:10.1002/nau.23923
20. Elduma AH. Female genital mutilation in Sudan. Open Access Maced J Med Sci. 2018;6:4304. doi:10.3889/oamjms.2018.099
21. Abathun AD, Sundby J, Gele AA. Attitude toward female genital mutilation among Somali and Harari people, Eastern Ethiopia. Int J Womens Health. 2016;8:557–569. doi:10.2147/IJWH.S112226
22. Pashaei T, Rahimi A, Ardalan A, et al. Related factors of female genital mutilation (FGM) in Ravansar (Iran). J Women’s Health Care. 2012;1(2):1000108. doi:10.4172/2167-0420.1000108
23. Tag-Eldin MA, Gadallah MA, Al-Tayeb MN, Abdel-Aty M, Mansour E, Sallem M. Prevalence of female genital cutting among Egyptian girls. Bull. World Health Organ. 2008;86(4):269–274. doi:10.2471/blt.07.042093
24. Shell-Duncan B, Moreau A, Wander K, Smith S. The role of older women in contesting norms associated with female genital mutilation/cutting in Senegambia: a factorial focus group analysis. PLoS One. 2018;13:e0199217. doi:10.1371/journal.pone.0199217
25. Bjalkander O, Leigh B, Harman G, Bergstrom S, Almroth L. Female genital mutilation in Sierra Leone: who are the decision makers? Afr J Reprod Health. 2012;16:119–131.
26. Herieka E, Dhar J. Female genital mutilation in the Sudan: survey of the attitude of Khartoum university students towards this practice. Sex Transm Infect. 2003;79(3):220–223. doi:10.1136/sti.79.3.220
27. Gele AA, Bø BP, Sundby J. Have we made progress in Somalia after 30 years of interventions? Attitudes toward female circumcision among people in the Hargeisa district. BMC Res Notes. 2013;6:122. doi:10.1186/1756-0500-6-122
28. Muhula S, Mveyange A, Oti SO, et al. The impact of community led alternative rite of passage on eradication of female genital mutilation/cutting in Kajiado County, Kenya: a quasi-experimental study. PLoS One. 2021;16(4):e0249662. doi:10.1371/journal.pone.0249662
29. Setegn T, Lakew Y, Deribe K. Geographic variation and factors associated with female genital mutilation among reproductive age women in Ethiopia: a national population based survey. PLoS One. 2016;11(1):e0145329. doi:10.1371/journal.pone.0145329
30. Gupta GR. Female genital mutilation/cutting: a statistical overview and exploration of the dynamics of change. Reprod Health Matters. 2013;21(42):184–191.
31. Ameyaw EK, Tetteh JK, Armah-Ansah EK, Aduo-Adjei K, Sena-Iddrisu A. Female genital mutilation/cutting in Sierra Leone: are educated women intending to circumcise their daughters? BMC Int Health Hum Rights. 2020;20(1):19. doi:10.1186/s12914-020-00240-0
32. Sabahelzain MM, Gamal Eldin A, Babiker S, Kabiru CW, Eltayeb M. Decision-making in the practice of female genital mutilation or cutting in Sudan: a cross-sectional study. Glob Health Res Policy. 2019;4:5. doi:10.1186/s41256-019-0096-0
33. Adigüzel C, Baş Y, Erhan MD, Gelle MA. The Female Genital Mutilation/Cutting Experience in Somali Women: their Wishes, Knowledge and Attitude. Gynecol Obstet Invest. 2019;84(2):118–127. doi:10.1159/000493130
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitude, and Practice of Insulin Pump Among Non-Endocrinology Nurses in South China

Mo C, Huang X, Lu X, Zhou Y, Su Y, Zhang H
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3417-3423
Published Date: 30 October 2023