Back to Journals » Journal of Pain Research » Volume 19
Diurnal Variation in Intraoperative Opioid Requirements: A Prospective Cohort Study
Authors Li Z, Gu X, Cai H ![]() , Gang T, Yan Y, Zhao J, Liu X
, Gang T, Yan Y, Zhao J, Liu X
Received 2 April 2026
Accepted for publication 4 June 2026
Published 16 June 2026 Volume 2026:19 614007
DOI https://doi.org/10.2147/JPR.S614007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Zhe Li,1 Xiaoying Gu,2 Huamei Cai,1 Tianran Gang,1 Yun Yan,3 Jing Zhao,1 Xiaowen Liu1
1Department of Anesthesiology, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Clinical Research and Data Management, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xiaowen Liu, Department of Anesthesiology, China-Japan Friendship Hospital, Beijing, People’s Republic of China, Email [email protected]
Purpose: Circadian rhythms regulate pain perception and drug metabolism, but their influence on intraoperative opioid requirements remains unclear. This study investigates how surgery timing is associated with intraoperative opioid use.
Patients and Methods: This cohort study enrolled patients undergoing laparoscopic cholecystectomy under general anesthesia at China-Japan Friendship Hospital. Patients were grouped into morning (08:00– 12:00) or afternoon (14:00– 18:00) groups according to surgery start time. Anesthesia was maintained with sevoflurane and sedation depth was monitored by bispectral index (BIS). Sufentanil was titrated by surgical pleth index (SPI) for analgesia. The primary outcome was sufentanil consumption. Secondary outcomes included plasma sufentanil, cortisol, ACTH and IL-6 concentrations, post-operative pain scores, extubation time, Aldrete scores, post-operative nausea and vomiting (PONV), length of PACU stay and rescue analgesia.
Results: 45 patients were enrolled with 24 assigned to the morning group and 21 to the afternoon group. Both groups achieved effective intraoperative sedation and analgesia with no significant differences in vital signs, BIS or SPI. However, the morning group required higher total sufentanil doses (47.50 ± 12.31 vs 36.12 ± 9.98 μg, p = 0.002), and normalized unit doses (0.52 ± 0.12 vs 0.39 ± 0.10 μg/kg/h, p < 0.001), compared to the afternoon group. Cortisol and ACTH levels in the morning group were elevated at all time points (all p < 0.001), whereas postoperative IL-6 levels only increased mildly (p = 0.008). Plasma sufentanil concentrations were higher in the morning group both 5 minutes after incision (2.75 [0.76– 4.67] vs 0.83 [0.59– 1.58] ng/mL, p = 0.027) and at the end of surgery (0.90 [0.38– 1.57] vs 0.31 [0.22– 0.54] ng/mL, p = 0.005).
Conclusion: In this selected cohort, morning surgery was associated with higher intraoperative sufentanil requirements. These findings are consistent with a possible time-of-day influence on intraoperative opioid needs and may reflect circadian neuroendocrine variation.
Keywords: diurnal variation, intraoperative opioid use, surgical pleth index, sufentanil, circadian influences
Introduction
Pain management is a crucial aspect of perioperative care, as inadequate control can adversely affect recovery and patient outcomes.1,2 While surgical trauma is a major cause of perioperative pain, individual differences in pain perception further complicate its management.3 For instance, women often report greater pain sensitivity than men, while older people may perceive pain less intensely than younger individuals.4–7 Such variations highlight the need for personalized approaches to pain management strategies to prevent opioid misuse and mitigate risks of inappropriate use.8
Opioids currently remain the cornerstone of perioperative analgesia, with anesthesiologists administering them during surgery to attenuate pain responses and reduce stress responses.9 However, opioid requirements vary widely between patients and are influenced by factors such as age, body mass index (BMI), psychological status and genetic polymorphisms, including those affecting the μ-opioid receptor gene.3,10 While these patient-specific determinants of opioid sensitivity are well documented, emerging evidence suggests that temporal factors governed by circadian rhythms may also significantly influence opioid efficacy and requirements.11–13
Circadian rhythms, regulated by the suprachiasmatic nucleus (SCN), orchestrate various physiological processes, including pain perception and drug metabolism.14,15 These rhythms affect neurotransmitter activity, pain thresholds, and hepatic enzyme function, including cytochrome P450 (CYP450), which is essential for opioid metabolism.16 Such time-dependent variations suggest that analgesic effects may fluctuate throughout the day, adding another layer of complexity to perioperative pain management.17
Recent studies have demonstrated significant diurnal variations in opioid efficacy, with different analgesic effects depending on the time of administration.13,18,19 For example, work by Gan et al identified such temporal differences in the context of post-operative pain management. Their matched observational study found that opioids such as sufentanil, dezocine and tramadol showed a better analgesic effect in the morning than in the afternoon, likely due to diurnal variations in pain sensitivity and drug metabolism.18 These findings highlight the importance of considering time of day when designing perioperative analgesic protocols. However, available evidence is derived from the postoperative setting, and whether similar time-dependent differences exist in intraoperative opioid requirements remains unclear. The intraoperative environment differs substantially from the postoperative period because anesthetic depth, unconscious nociceptive processing, surgical stimulation, drug interactions, fluid shifts, and organ perfusion may all influence opioid pharmacodynamics and analgesic requirements.20–22 Moreover, the reported analgesic levels in Gan et al were based on patients’ subjective perceptions, which may introduce bias. Under anesthesia, patients cannot actively report pain, necessitating more objective pain assessment methods. Therefore, objective nociception-guided assessment may provide a more appropriate approach for evaluating intraoperative analgesic requirements.
To address this gap, our study investigated whether the timing of surgery was associated with intraoperative opioid requirements, aiming to explore a possible role of circadian rhythm-related factors in perioperative pain management. In this study, intraoperative analgesia was guided by the surgical pleth index (SPI), an objective nociception monitoring tool that has been used to guide opioid titration during general anesthesia.23 By focusing on SPI-guided intraoperative opioid administration, this study aimed to explore a possible time-of-day influence on intraoperative opioid requirements and to provide preliminary evidence for more individualized perioperative analgesic management.
Materials and Methods
Registration and Ethical Approval
Ethical approval was obtained from the Ethics Committee of China-Japan Friendship Hospital (CJFH), Beijing, China, with reference number 2024-KY-148-1 on 20 May, 2024. The study was registered in the Chinese Clinical Trial Registry (ChiCTR2400089115). The study was conducted in accordance with the Declaration of Helsinki.
Study Population
This prospective cohort study was conducted at the CJFH between 28 August, 2024 and 6 December, 2024 to investigate the effect of diurnal variation on intraoperative opioid requirements during laparoscopic cholecystectomy. Written informed consent was obtained from all participants after the study objectives, procedures, risks and benefits were explained.
Sample Size
As a cohort study, the sample size in each group was determined based on the difference between the means of two groups. Sample size was calculated using the following formula:
As our previous preliminary experiment data suggesting, the sufentanil consumption was 0.532 ± 0.097 μg/kg/h in the morning group and 0.406 ± 0.081 μg/kg/h in the afternoon group. Given a two-sided significance level of 0.05 (α) and a power of 0.9, our calculations suggest a minimum of 21 patients should be enrolled in each group.
Data Collection
Patients scheduled to undergo laparoscopic cholecystectomy under general anesthesia were screened using predefined inclusion and exclusion criteria. After obtaining informed consent, information including demographic data, current and past medical history, relevant investigations and medication history were collected. This information was then entered and stored in the Epidata database.
Anesthetic Induction and Perioperative Management
This study followed a standardized protocol for anesthetic induction and intraoperative management to ensure consistency across patients. Patients were required to fast for 8 hours and refrain from fluids for 2 hours prior to surgery. Patients were assessed for dehydration or hypoglycemia if fasting exceeded 10 hours or abstaining from liquids for more than 4 hours, and management was adjusted as necessary. On admission to the operating theatre, peripheral intravenous access was established, and routine monitoring was initiated, including electrocardiography (ECG), non-invasive blood pressure, pulse oximetry, bispectral index (BIS), end-tidal carbon dioxide (EtCO2), body temperature, and SPI. In addition, baseline heart rate (HR) and mean arterial pressure (MAP) were measured in a static environment three consecutive times, with the results averaged to establish a benchmark for subsequent comparisons.
Anesthesia was induced with a combination of 1.5–2.0 mg/kg of propofol, 0.2 μg/kg of sufentanil, and 0.6 mg/kg of rocuronium, with all doses calculated based on actual body weight. Intubation was performed 3–5 minutes after drug administration, followed by mechanical ventilation with a tidal volume of 6 mL/kg, a respiratory rate of 12 breaths per minute, and an oxygen concentration of 40%. Ventilation parameters were adjusted as needed to maintain EtCO2 levels between 35 and 45 mmHg.
During surgery, anesthesia was maintained with 2–3% sevoflurane titrated to a minimum of 0.7 MAC to maintain a BIS between 40 and 60. Inhaled anesthetic concentration was adjusted if BIS exceeded 60 or fell below 40. Muscle relaxation was achieved with 0.1–0.2 mg/kg rocuronium, administered hourly or as required on the basis of 2–3 responses to train-of-four stimulation. Hemodynamic events were recorded and the infusion rate of lactated Ringer’s solution (baseline rate: 5–10 mL/min) was adjusted according to surgical blood loss and blood pressure. In addition, body temperature was continuously monitored during surgery, and thermal insulation measures such as warm blankets or warmed fluids were used to maintain a temperature of ≥36°C in patients at risk of hypothermia. Perioperative management of special events is detailed in the Supplementary Appendix S1.
Before the end of surgery, all patients received 5 mg of dexamethasone to minimize the risk of postoperative nausea and vomiting (PONV). Sugammadex 2–4 mg/kg was administered postoperatively to reverse neuromuscular blockade. Extubation was performed when the patient regained consciousness, demonstrated the ability to cooperate, opened their eyes and achieved sufficient muscle strength (TOFR ≥0.9).
Pain Management
Intraoperative pain was managed using the SPI as a guide. SPI values were continuously monitored and maintained between 20 and 50. If SPI exceeded 50 for 1 minute, 0.1 µg/kg of sufentanil was administered. If it remained above 50 after 5 minutes, an additional dose of 0.1 µg/kg sufentanil was administered. To simplify dosing, amounts were rounded to the nearest multiple of 0.5 μg based on patient weight (eg, 5 μg, 5.5 μg, 6 μg, 6.5 μg).
Before the end of surgery, all patients received 50 mg of flurbiprofen for postoperative pain relief. After surgery, patients were assessed in the post-anesthesia care unit (PACU) using the numeric rating scale (NRS) at 15 minutes after arrival and before discharge. Patients with an NRS score of 4 or higher received rescue analgesia with 0.1 µg/kg of sufentanil.
Outcome Measures
The primary outcome of this study was intraoperative total sufentanil consumption, also measured as dosage per unit time and weight. Secondary outcomes included postoperative pain assessed using the NRS at specific time points: upon entering the PACU, at 15 minutes and departure from the PACU, and on postoperative days (POD) 1 and 2. Other secondary outcomes were plasma measurements of sufentanil concentration, cortisol, ACTH, and IL-6; extubation time (defined as the interval from the end of anesthesia to tracheal tube removal); Aldrete scores 15 minutes after PACU entry; the use of rescue analgesics; length of PACU stay; and the incidence of PONV, recorded in the PACU and on POD1.
Patients’ vital signs were recorded at baseline, 1 minute after induction, at the end of intubation, 5 minutes post-intubation, at the start of surgery, every 10 minutes during surgery, at extubation, and upon PACU discharge. For research purposes, 5 mL venous blood samples were collected at three specific time points: before induction of anesthesia in the operating theatre, 5 minutes after skin incision, and at the end of surgery. Samples were stored in a biobank for subsequent analysis of plasma cortisol, ACTH, and IL-6 levels at these three time points, as well as blood sufentanil concentrations at 5 minutes after skin incision and at the end of surgery.
Statistical Analysis
Baseline characteristics, including demographic information, were compared between morning and afternoon groups. Continuous variables such as intraoperative sufentanil consumption, time to extubation and PACU length of stay were assessed for normality. Normally distributed data were summarized as mean ± standard deviation (SD) and compared using independent samples t-tests, while non-normally distributed data were presented as median (interquartile range) and analyzed using the Mann–Whitney U-test. Categorical variables, such as PONV, and the proportion of patients requiring postoperative analgesia, were analyzed using the chi-squared test or Fisher’s exact test, depending on sample size and expected frequency. Time-dependent variables, such as NRS scores at different time points, were analyzed using repeated measures ANOVA for normally distributed data or the Friedman test for non-parametric data. Additionally, multivariable linear regression models were used to evaluate potential factors and their interactions influencing primary outcome indicators such as age and gender. All significance tests were two-sided, and a p value less than 0.05 was considered statistically significant. Statistical analysis was performed using R software.
Results
A total of 45 patients were enrolled in this study at CJFH between August 28 2024 and December 6 2024. Based on their surgery start time, 24 patients were assigned to the morning group and 21 to the afternoon group. The screening and data collection process is illustrated in Figure 1.
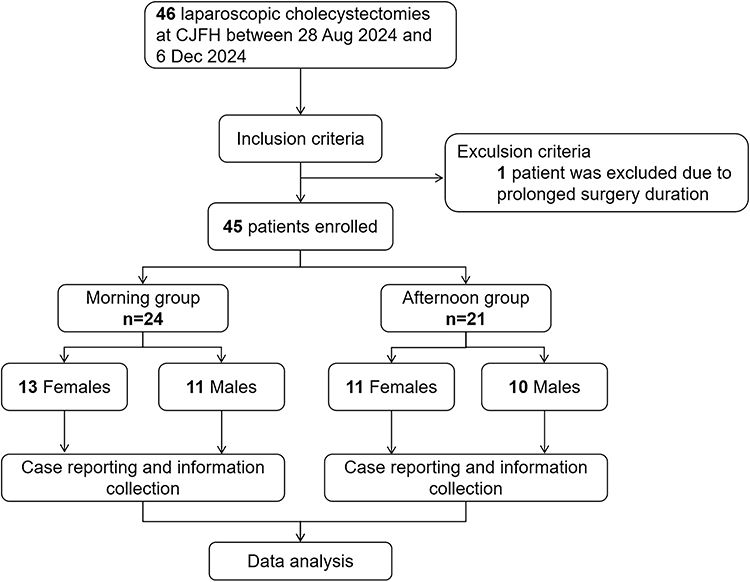 |
Figure 1 Flowchart of the study. |
Baseline Characteristics
As shown in Table 1, the baseline characteristics of the two groups were comparable. The mean age was 46.66 ± 12.46 years old for the morning group and 47.00 ± 12.49 years old for the afternoon group (p = 0.929). The mean weight was 68.92 ± 9.53 kg and 68.52 ± 11.30 kg, respectively, with corresponding BMI values of 24.59 ± 2.59 kg/m2 and 24.17 ± 2.61 kg/m2 (p = 0.779 and p = 0.591, respectively). The proportion of male patients was 45.8% in the morning group and 47.6% in the afternoon group (p = 0.905). All patients were classified as ASA I or II, with 20 (83.3%) in the morning group and 18 (85.7%) in the afternoon group being ASA II (p > 0.999).
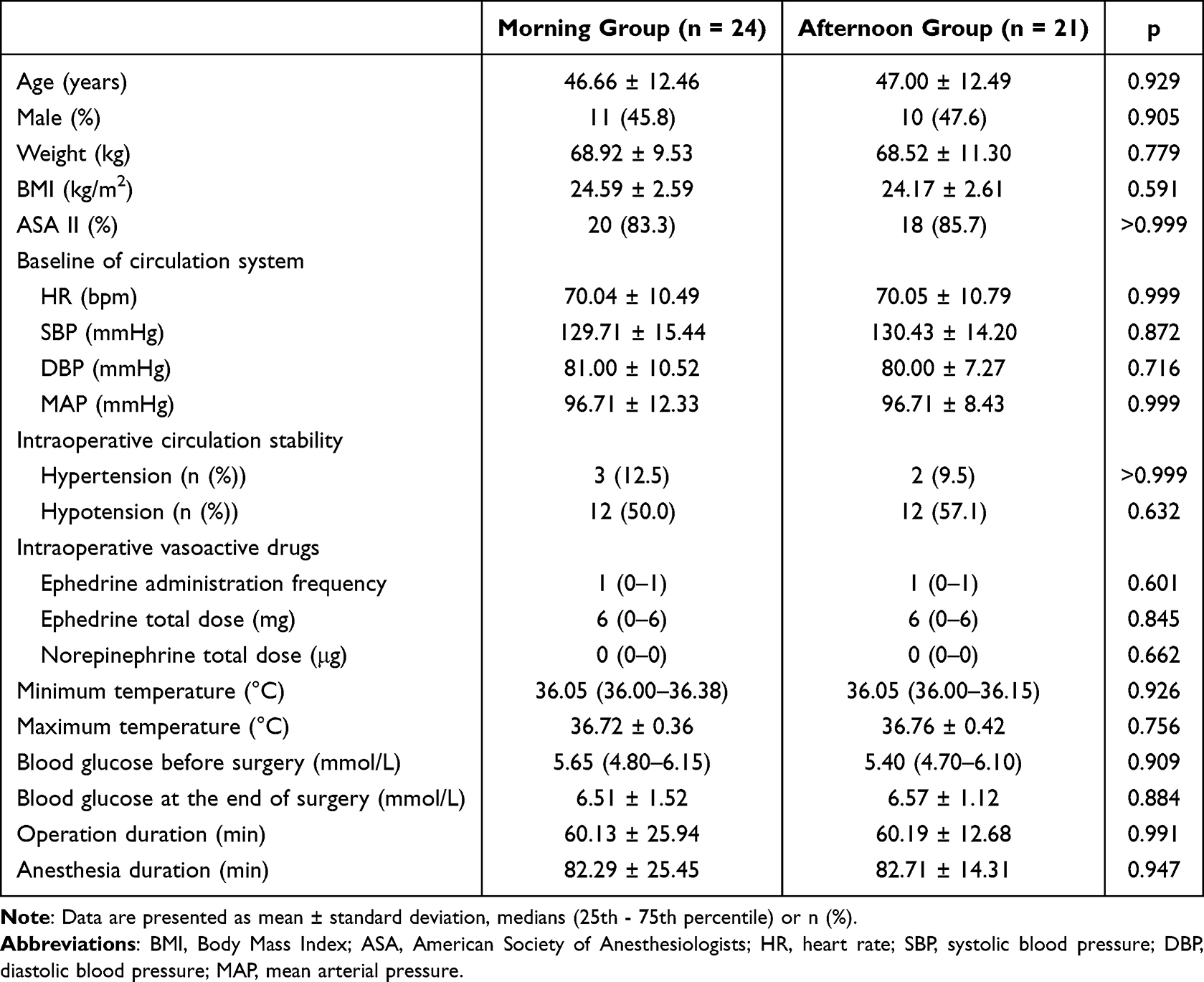 |
Table 1 Baseline Characteristics of Two Groups of Patients |
The intraoperative baseline information was basically consistent between the two groups (Also shown in Table 1). The mean anesthesia duration was 82.29 ± 25.45 minutes for the morning group and 82.71 ± 14.31 minutes for the afternoon group, with corresponding surgery durations of 60.13 ± 25.94 minutes and 60.19 ± 12.68 minutes (p = 0.947 and p = 0.991, respectively). During surgery, there were no significant differences in baseline circulatory values between the two groups, with all p-values greater than 0.05. Figure 2A presents an overview of the trends in vital signs for patients, including MAP, body temperature, and HR. Hypertension without an SPI greater than 50 occurred in 3 patients in the morning group (12.5%) and 2 patients in the afternoon group (9.5%), showing no statistical significance (p > 0.999). Hypotension was more common, affecting 12 patients in both groups (50.0% in the morning group and 57.1% in the afternoon group, p = 0.632). The mean doses and total doses of ephedrine were slightly higher in the morning group than in the afternoon group, but the differences were not statistically significant. No significant differences were observed between the groups in the mean minimum and maximum intraoperative body temperatures or in the mean pre- and postoperative blood glucose levels (shown in Table 1).
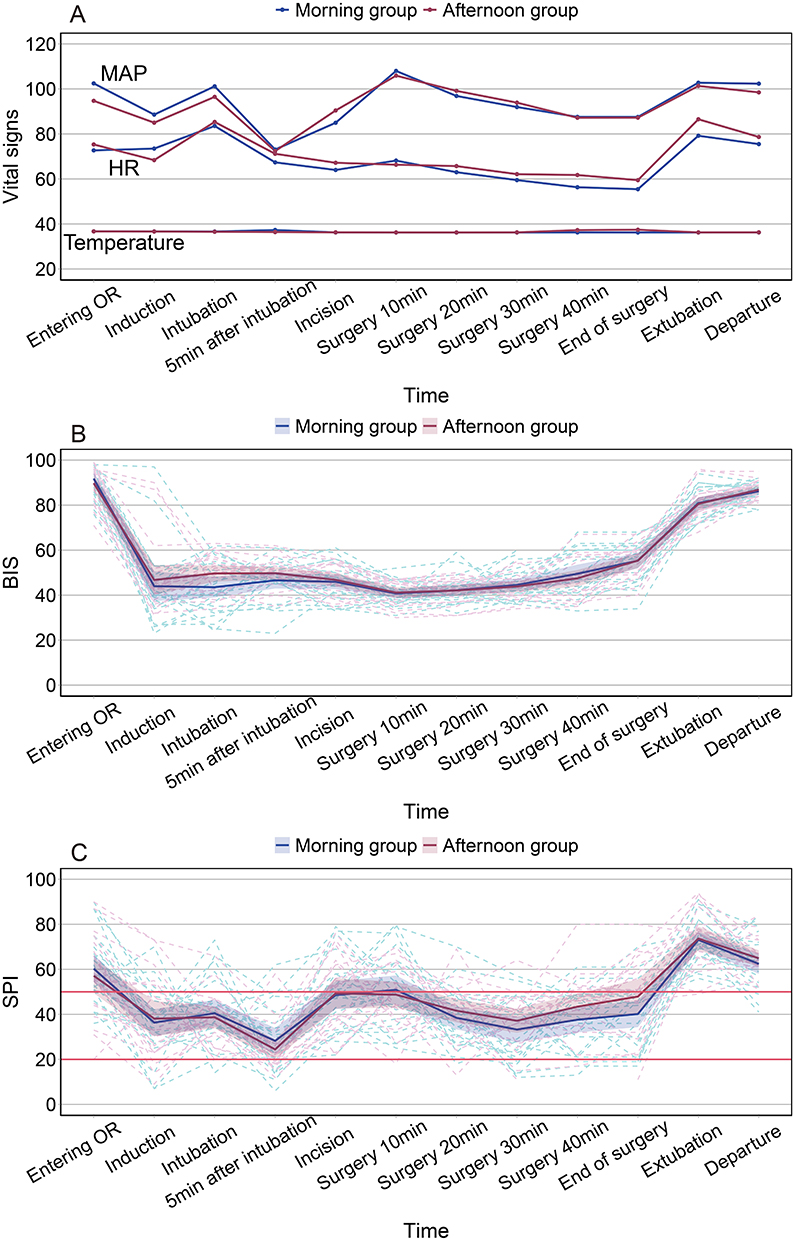 |
Figure 2 Fluctuations in vital signs of patients during surgery. This figure illustrates the intraoperative changes in vital signs and monitoring parameters for patients in the morning and afternoon groups. As approximately half of the surgeries were completed within 50 minutes, data beyond 40 minutes into surgery are incomplete. Therefore, intraoperative data are presented only up to 40 minutes. (A) The line graph shows the mean values of mean arterial pressure (MAP), heart rate (HR) and body temperature for the two groups. (B and C) show the variations in bispectral index (BIS) and surgical pleth index (SPI) during surgery for both groups. The dashed lines show the individual patient trends within each group, while the solid lines show the average trends for each group. The shaded areas around the solid lines, corresponding to the color of each group (purple for the morning group and red for the afternoon group), represent the standard deviation. No statistically significant differences in vital signs were observed between the two groups at any time point. |
The BIS and SPI values during surgery are shown in Figure 2B and C. Due to variations in the duration of surgery, approximately half of the patients remained after 50 minutes, so the figures only show data up to 40 minutes. Data from 40 minutes to extubation were collected and analyzed, but showed no significant differences between the two groups at any time.
Primary Outcome
For the primary outcome measure, intraoperative opioid consumption is detailed in Table 2. The total doses of sufentanil were significantly higher in the morning group (47.50 ± 12.31 ug) compared to the afternoon group (36.12 ± 9.98 ug, p = 0.002), indicating a potential diurnal variation in opioid requirements. When normalized by anesthesia duration and patient weight, the mean unit doses of sufentanil were also significantly higher in the morning group (0.52 ± 0.12 μg/kg/h vs 0.39 ± 0.10 μg/kg/h, p < 0.001).
 |
Table 2 Intraoperative Sufentanil Consumption |
Secondary Outcomes
The concentrations of sufentanil, cortisol, ACTH, and IL-6 at different time points during surgery are shown in Table 3. The morning group had significantly higher plasma sufentanil concentrations 5 minutes after skin incision (2.75 [0.76–4.67] ng/mL vs 0.83 [0.59–1.58] ng/mL, p = 0.027) and at the end of surgery (0.90 [0.38–1.57] ng/mL vs 0.31 [0.22–0.54] ng/mL, p = 0.005), corresponding to their higher intraoperative opioid consumption. Similarly, cortisol and ACTH levels were significantly elevated in the morning group at all three time points: before induction, 5 minutes after skin incision and at the end of surgery (all p values < 0.001). IL-6 levels did not differ significantly between groups before induction (p = 0.213) or 5 minutes after skin incision (p = 0.068). At the end of surgery, the morning group had slightly higher IL-6 levels (44.77 ± 5.59 pg/mL vs 40.32 ± 5.00 pg/mL, p = 0.008), but the difference, although statistically significant, was modest and may have limited clinical relevance.
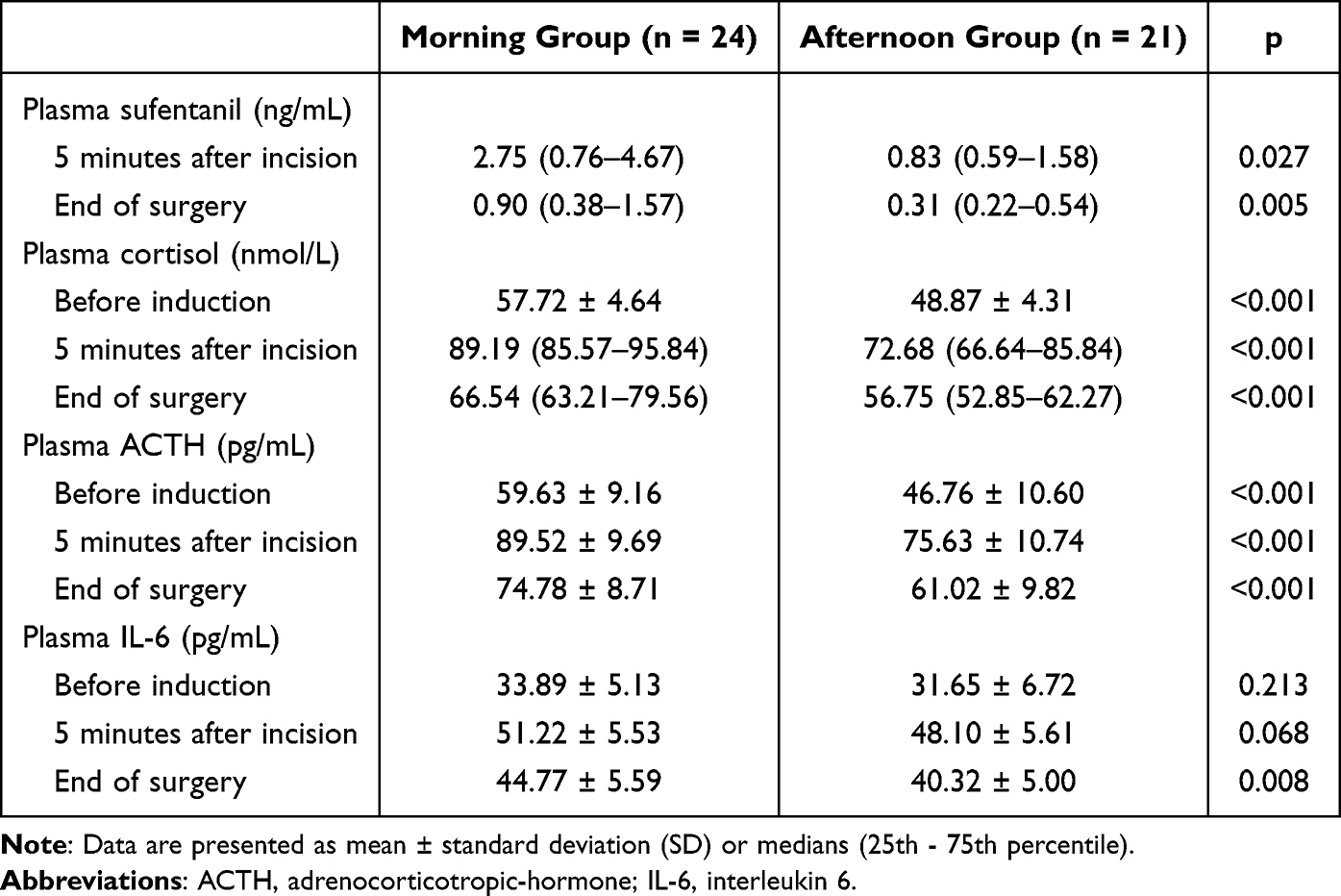 |
Table 3 Concentration of Plasma Cortisol, ACTH, IL-6 and Sufentanil at Different Time During Surgery |
Postoperative outcome measures are summarized in Table 4. Extubation time was slightly longer in the morning group (8.00 [6.00–8.75] minutes) than in the afternoon group (7.00 [6.00–8.00] minutes), but this difference was not statistically significant. NRS scores at all time points assessed showed no significant differences between groups. Postoperative pain control was effective with only one patient in the morning group requiring rescue analgesia (4.1% vs 0%, p > 0.999). All patients achieved full recovery (Aldrete score of 10) within 15 minutes of entering the PACU. The incidence of PONV was higher in the morning group both in the PACU (29.17% vs 9.52%, p = 0.143) and on postoperative day 1 (20.83% vs 9.52%, p = 0.422), but these differences were not statistically significant. Mean PACU length of stay was also similar between groups (29.58 ± 5.50 vs 27.86 ± 3.73 minutes, p = 0.232).
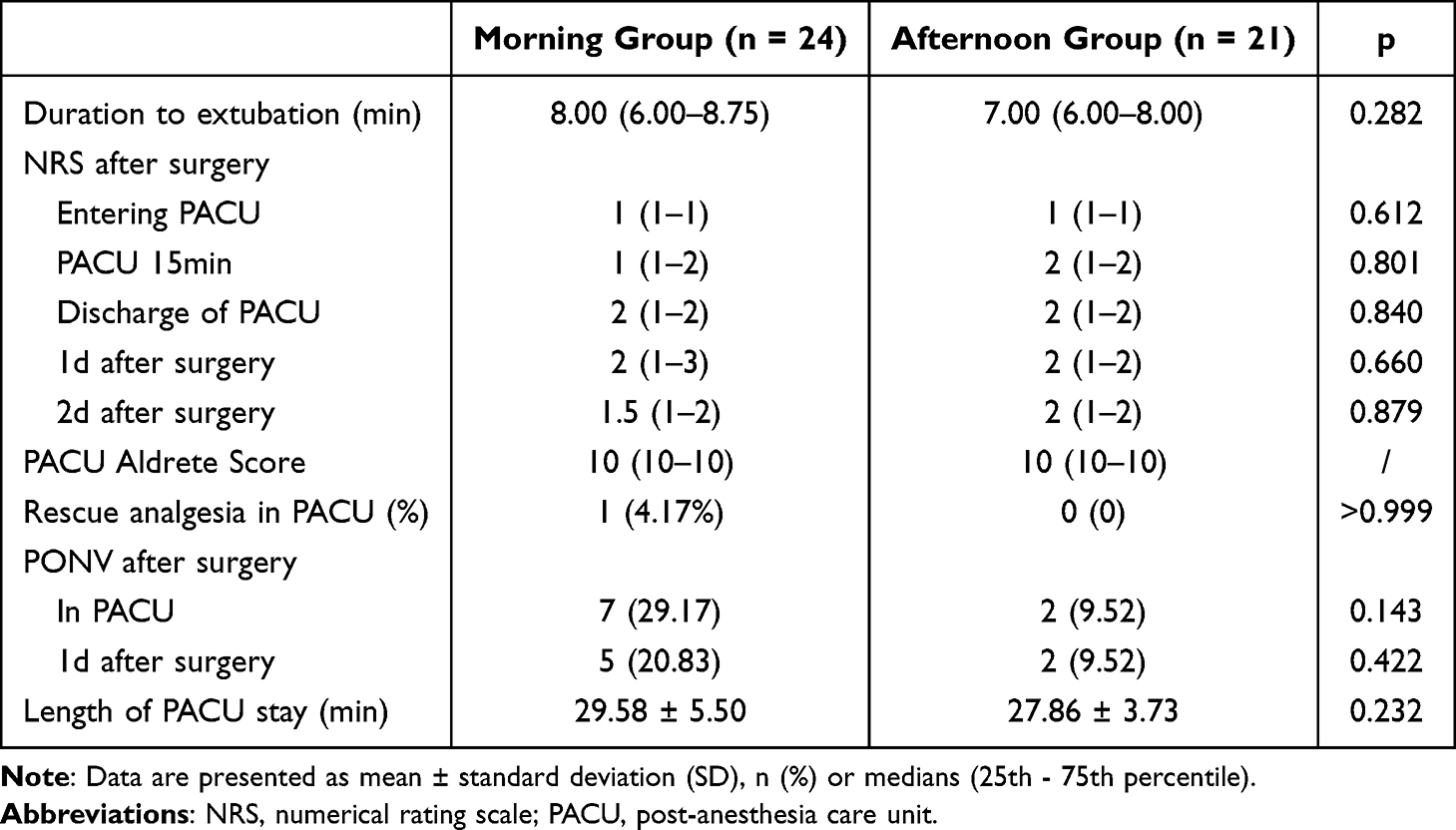 |
Table 4 Postoperative Recovery After Surgery of Two Groups |
Exploratory Subgroup Analysis
Table S1 presents an exploratory subgroup analysis comparing morning and afternoon groups stratified by sex. This analysis was not powered to detect subgroup-specific or interaction effects and should therefore be interpreted as hypothesis-generating. In terms of baseline information, we analyzed five variables: age, weight, BMI, operation duration and anesthesia duration. Within female or male no statistically significant differences were observed between the two groups, with all p-values exceeding 0.05. However, a significant difference of dose of sufentanil emerged between the morning and afternoon groups used in female patients (45.81 ± 12.00 μg vs 33.00 ± 5.72 μg, p = 0.003). Among male patients, a slight difference was also noted, although the p-value was close to our predefined statistical significance threshold (49.50 ± 12.95 μg vs 39.55 ± 12.65 μg, p = 0.091). Upon standardizing the sufentanil dosage based on operation duration and weight for both genders, significant differences were found in both female and male between the morning and afternoon groups. Specifically, female patients showed a difference of 0.51 ± 0.12 μg/kg/h vs 0.39 ± 0.07 μg/kg/h (p = 0.010), while male patients exhibited a difference of 0.55 ± 0.13 μg/kg/h vs 0.39 ± 0.12 μg/kg/h (p = 0.012).
Multivariable Analysis
Table S2 summarizes the results of our multivariable analysis with linear regression. As we have adjusted for weight and anesthesia duration when calculated unit sufentanil consumption. In this regression, we included age and gender, which have potential correlations with pain and opioid consumption, to ascertain the relevance of these variables to the outcomes. The table reveals that neither gender nor age showed a significant correlation with either the total sufentanil consumption or the unit sufentanil consumption in the multivariate analysis (p > 0.05 for all variables).
Discussion
This observational cohort study demonstrates a significant time-of-day variation in intraoperative opioid requirements, with higher sufentanil doses required for morning surgery compared with afternoon surgery. These findings highlight the influence of temporal factors on surgical analgesia and provide new insights into the interplay between circadian rhythms, nociception and drug metabolism in the intraoperative setting. This underscores the importance of objective patient monitoring and assessment in reducing opioid misuse through more precise and individualized pain management strategies.
Pain perception is a subjective and complex phenomenon influenced by various factors such as gender, age, and analgesic methods.3,24 Previous studies have shown that circadian rhythms impact hyperalgesia and postoperative opioid use.18,25–28 this study extends this understanding to the intraoperative setting. This study extends these findings to the intraoperative period, highlighting the importance of incorporating circadian biology into anesthetic protocols. For example, morning surgeries may benefit from proactive strategies to counteract heightened stress responses and hormonal fluctuations, such as optimized opioid dosing or the use of multimodal analgesia. Conversely, afternoon surgeries may require interventions to address potential hyperalgesia. Personalized analgesic strategies based on temporal factors could reduce the risk of over- or undermedication, thereby improving both safety and efficacy.
To minimize bias, this study used the SPI as an objective nociception tool,29,30 along with rigorous control of potential confounders such as blood glucose, body temperature, and fluid volume.23 Similarly, strict preoperative fasting requirements were imposed on all patients. However, due to the large patient volume and the difficulty of accurately determining surgical start times eight hours in advance, some patients inevitably experienced fasting durations longer than prescribed. This may introduce bias, as hunger has been shown to affect pain tolerance and analgesic equivalency.31–33 To ensure consistency, all patients were placed in the same Trendelenburg surgical position, a posture known to influence SPI values but applied uniformly across groups. Although the incidence of PONV was similar between groups, more patients in the morning cohort experienced PONV in the PACU, possibly due to higher doses of sufentanil, a known risk factor. In addition, exploratory subgroup and multivariable analyses were conducted to assess whether sex or age might influence sufentanil consumption. However, these analyses were not powered to detect subgroup-specific or interaction effects and should be interpreted cautiously.
The consistently elevated cortisol and ACTH levels observed in the morning group are likely to play a key role in shaping the observed diurnal variation. Cortisol, a key circadian hormone, is known to suppress descending inhibitory pain pathways and enhance nociceptive processing, potentially lowering pain thresholds during morning surgery.34,35 Additionally, elevated cortisol levels may exacerbate stress responses through increased sympathetic arousal, further contributing to higher opioid requirements.36,37 In contrast, inflammatory markers such as IL-6, although statistically higher in the morning group postoperatively, demonstrated only modest differences between groups. This disparity, alongside the more pronounced elevations in cortisol and ACTH, suggests that hormonal fluctuations, rather than inflammatory responses, are the primary drivers of the observed variations in intraoperative opioid requirements. Taken together, these findings suggest that circadian rhythm-related neuroendocrine variation may partly contribute to the observed time-of-day difference in intraoperative opioid requirements, although causality cannot be established from this observational study.
Although plasma drug concentrations do not directly reflect analgesic efficacy or patient demand, the observation that morning group patients had nearly threefold higher plasma sufentanil concentrations than afternoon group patients, despite only around 20% difference in total dose, represents a major discrepancy that warrants mechanistic consideration. The clearance of sufentanil is primarily dependent on hepatic blood flow and intrinsic metabolic capacity. Despite similar intraoperative blood pressure between the morning and afternoon groups, blood flow dynamics cannot explain the observed differences in plasma levels or opioid efficacy.38 While circadian rhythms regulate hepatic enzyme activity, such as CYP450, which may accelerate metabolism in the morning, the higher plasma concentrations observed in the morning group suggest that altered drug distribution, rather than metabolic differences, is the more likely cause. The lipophilicity of sufentanil results in significant variability in tissue distribution, which may be modulated by circadian factors and individual patient characteristics.
In addition, central mechanisms are likely to be critical in explaining the differences in opioid requirements between the groups, although the current data do not provide direct evidence. Circadian fluctuations in cortisol may affect blood-brain barrier permeability, receptor sensitivity, and drug bioavailability within the CNS, potentially limiting μ-opioid receptor activation in the morning despite higher plasma concentrations.39,40 However, these central mechanisms remain speculative at this stage, as no direct measurements of blood-brain barrier function or receptor sensitivity were performed. These findings underscore the complex interplay between circadian rhythms, drug distribution, and receptor dynamics, and highlight the need for further research into the central and systemic mechanisms influencing opioid efficacy.41–43
This study has several limitations. First, because this was an observational study rather than a randomized trial, residual confounding could not be fully eliminated. Preoperative stress, individual chronotype, sleep-wake patterns, daily routines, and fasting-duration variation were not fully assessed and may have influenced cortisol levels and opioid requirements. Second, the single-center design and relatively small sample size may limit generalizability. This cohort included selected adult ASA I–II patients undergoing elective laparoscopic cholecystectomy; therefore, the findings should not be directly generalized to elderly patients, patients with obesity, ASA III–IV patients, emergency procedures, open-conversion cases, or major/prolonged surgical populations. Third, resource constraints prevented direct measurement of liver enzyme activity, tissue distribution, free drug concentrations, or other pharmacokinetic parameters, which limits mechanistic interpretation of the plasma sufentanil findings. The proposed explanations involving altered drug distribution or central mechanisms therefore remain speculative. Finally, the exclusion of nocturnal surgery limited the analysis to daytime rhythms, leaving the effects of night-time surgery unexplored.
Conclusion
In conclusion, this study shows that intraoperative opioid requirements varied with the time of day in selected patients undergoing laparoscopic cholecystectomy, with higher sufentanil requirements observed during morning surgery than during afternoon surgery. This variation was consistent with concurrent differences in cortisol and ACTH levels and may reflect a possible association between intraoperative opioid requirements and circadian rhythm-related neuroendocrine variation. These findings suggest that surgery timing may be considered as a potential factor in individualized perioperative analgesic management, although further studies are needed to clarify the underlying mechanisms and clinical applicability.
Abbreviations
BMI, body mass index; SCN, suprachiasmatic nucleus; CYP450, cytochrome P450; CJFH, China-Japan Friendship Hospital; SPI, Surgical Pleth Index; ECG, electrocardiography; BIS, bispectral index; EtCO2, end-tidal carbon dioxide; HR, heart rate; MAP, mean arterial pressure; PONV, postoperative nausea and vomiting; PACU, post-anesthesia care unit; NRS, numeric rating scale; POD, postoperative days; SD, standard deviation.
Data Sharing Statement
Data and materials in this study are available upon request from the corresponding author. These data cannot be made public due to the privacy of the patients.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Ethics Committee of China-Japan Friendship Hospital, Beijing, China, with reference number 2024-KY-148-1 on 20 May, 2024. The study was registered in the Chinese Clinical Trial Registry (ChiCTR2400089115). Written informed consent was obtained from all participants after the study objectives, procedures, risks and benefits were explained. The study was conducted in accordance with the Declaration of Helsinki.
Funding
This study was supported by the National High Level Hospital Clinical Research Funding, Elite Medical Professionals Project of China-Japan Friendship Hospital (NO. ZRJY2023-GG11).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guo R, Yang WW, Zhong ML, et al. The relationship between anesthesia, surgery and postoperative immune function in cancer patients: a review. Front Immunol. 2024;15:1441020. doi:10.3389/fimmu.2024.1441020
2. Santa Cruz Mercado LA, Liu R, Bharadwaj KM, et al. Association of intraoperative opioid administration with postoperative pain and opioid use. JAMA Surg. 2023;158(8):854–12. doi:10.1001/jamasurg.2023.2009
3. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158 Suppl 1(Suppl 1):S11–s18. doi:10.1097/j.pain.0000000000000775
4. Keogh E. Sex and gender differences in pain: past, present, and future. Pain. 2022;163(Suppl 1):S108–s116. doi:10.1097/j.pain.0000000000002738
5. Templeton KJ. Sex and gender issues in pain management. J Bone Joint Surg Am. 2020;102 Suppl 1(Suppl 1):32–35. doi:10.2106/jbjs.20.00237
6. Stratton H, Lee G, Dolatyari M, et al. Nociceptors are functionally male or female: from mouse to monkey to man. Brain. 2024;147(12):4280–4291. doi:10.1093/brain/awae179
7. Zhi Y, Zhang Y, Zhang Y, Zhang M, Kong Y. Age-associated changes in multimodal pain perception. Age Ageing. 2024;53(5):afae107. doi:10.1093/ageing/afae107
8. El-Boghdadly K, Levy NA, Fawcett WJ, et al. Peri-operative pain management in adults: a multidisciplinary consensus statement from the association of anaesthetists and the British pain society. Anaesthesia. 2024;79(11):1220–1236. doi:10.1111/anae.16391
9. Kianian S, Bansal J, Lee C, Zhang K, Bergese SD. Perioperative multimodal analgesia: a review of efficacy and safety of the treatment options. Anesthesiology and Perioperative Science. 2024;2(1):9. doi:10.1007/s44254-023-00043-1
10. Lendrum J, Freeman T, Dayton MR, et al. Influence of body bass index (BMI) on post-operative opioid requirements in primary total joint arthroplasty patients. J Orthop. 2021;24:121–125. doi:10.1016/j.jor.2021.02.028
11. Coppes OJM, Yong RJ, Kaye AD, Urman RD. Patient and surgery-related predictors of acute postoperative pain. Curr Pain Headache Rep. 2020;24(4):12. doi:10.1007/s11916-020-0844-3
12. Elgendy HM, Ibrahim SM, Bader L, et al. Genetic factors associated with morphine consumption in women undergoing laparoscopic cholecystectomy: a prospective cohort study. J Pain Res. 2023;16:2407–2417. doi:10.2147/jpr.S420447
13. Bienert A, Bartkowska-śniatkowska A. Selected aspects of chronobiological studies in anaesthesia. 2014.
14. Patke A, Young MW, Axelrod S. Molecular mechanisms and physiological importance of circadian rhythms. Nat Rev Mol Cell Biol. 2020;21(2):67–84. doi:10.1038/s41580-019-0179-2
15. Zhang R, Lahens NF, Ballance HI, Hughes ME, Hogenesch JB. A circadian gene expression atlas in mammals: implications for biology and medicine. Proc Natl Acad Sci U S A. 2014;111(45):16219–16224. doi:10.1073/pnas.1408886111
16. Holmquist GL. Opioid metabolism and effects of cytochrome P450. Pain Medicine. 2009;10(s1):S20–S29. doi:10.1111/j.1526-4637.2009.00596.x
17. Bum Garner JR, Walker WH, Nelson RJ. Circadian rhythms and pain. Neurosci Biobehav Rev. 2021;129:296–306. doi:10.1016/j.neubiorev.2021.08.004
18. Gan W, Yang X, Chen J, et al. Role of daytime variation in pharmaceutical effects of sufentanil, dezocine, and tramadol: a matched observational study. Front Pharmacol. 2022;13:993506. doi:10.3389/fphar.2022.993506
19. Boom M, Grefkens J, van Dorp E, et al. Opioid chronopharmacology: influence of timing of infusion on fentanyl’s analgesic efficacy in healthy human volunteers. J Pain Res. 2010;3:183–190. doi:10.2147/jpr.S13616
20. Uhing MR, Beno DW, Jiyamapa-Serna VA, et al. The effect of anesthesia and surgery on CYP3A activity in rats. Drug Metab Dispos. 2004;32(11):1325–1330. doi:10.1124/dmd.104.000927
21. Wood M. Pharmacokinetic drug interactions in anaesthetic practice. Clin Pharmacokinet. 1991;21(4):285–307. doi:10.2165/00003088-199121040-00005
22. Hahn RG. Understanding volume kinetics. Acta Anaesthesiol Scand. 2020;64(5):570–578. doi:10.1111/aas.13533
23. Oh SK, Won YJ, Lim BG. Surgical pleth index monitoring in perioperative pain management: usefulness and limitations. Korean J Anesthesiol. 2024;77(1):31–45. doi:10.4097/kja.23158
24. Mestdagh FP, Lavand’homme PM, Pirard G, Joshi GP, Sauter AR, Van de Velde M. Pain management after elective craniotomy: a systematic review with procedure-specific postoperative pain management (PROSPECT) recommendations. Eur J Anaesthesiol. 2023;40(10):747–757. doi:10.1097/eja.0000000000001877
25. Burns JW, Hodsman NB, McLintock TT, Gillies GW, Kenny GN, McArdle CS. The influence of patient characteristics on the requirements for postoperative analgesia. A reassessment using patient-controlled analgesia. Anaesthesia. 1989;44(1):2–6. doi:10.1111/j.1365-2044.1989.tb11086.x
26. Graves DA, Batenhorst RL, Bennett RL, et al. Morphine requirements using patient-controlled analgesia: influence of diurnal variation and morbid obesity. Clin Pharm. 1983;2(1):49–53.
27. Shu B, Liu H, Zheng X, et al. Opioid infusions at different times of the day produce varying degrees of opioid-induced hyperalgesia. Br J Anaesth. 2023;131(6):1072–1081. doi:10.1016/j.bja.2023.08.039
28. Lemmens HJ. Pharmacokinetic-pharmacodynamic relationships for opioids in balanced anaesthesia. Clin Pharmacokinet. 1995;29(4):231–242. doi:10.2165/00003088-199529040-00003
29. Hung SC, Hsu WT, Fu CL, Lai YW, Shen ML, Chen KB. Does surgical plethysmographic index-guided analgesia affect opioid requirement and extubation time? A systematic review and meta-analysis. J Anesth. 2022;36(5):612–622. doi:10.1007/s00540-022-03094-z
30. Funcke S, Pinnschmidt HO, Wesseler S, et al. Guiding opioid administration by 3 different analgesia nociception monitoring indices during general anesthesia alters intraoperative sufentanil consumption and stress hormone release: a randomized controlled pilot study. Anesth Analg. 2020;130(5):1264–1273. doi:10.1213/ane.0000000000004388
31. Edwards SA, Martin SL, Rainey T, et al. Influence of acute fasting on pain tolerance in healthy subjects: a randomised crossover study. Front Pain Res (Lausanne). 2023;4:1153107. doi:10.3389/fpain.2023.1153107
32. Li T, Yue Y, Ma Y, et al. Fasting-mimicking diet alleviates inflammatory pain by inhibiting neutrophil extracellular traps formation and neuroinflammation in the spinal cord. Cell Commun Signal. 2023;21(1):250. doi:10.1186/s12964-023-01258-2
33. Xu H, Wang Y, Niu D, Xu M, Yao L. Effect of preoperative fasting on acute postoperative pain following cesarean section: a retrospective cohort study. Ann Med Surg (Lond). 2026;88(5):2743–2750. doi:10.1097/ms9.0000000000004865
34. Goto T, Nakagami G, Minematsu T, et al. Topically injected adrenocorticotropic hormone induces mechanical hypersensitivity on a full-thickness cutaneous wound model in rats. Exp Dermatol. 2019;28(9):1010–1016. doi:10.1111/exd.13994
35. Choi JC, Chung MI, Lee YD. Modulation of pain sensation by stress-related testosterone and cortisol. Anaesthesia. 2012;67(10):1146–1151. doi:10.1111/j.1365-2044.2012.07267.x
36. Jovanovic F, Jovanovic V, Knezevic NN. Glucocorticoid hormones as modulators of the kynurenine pathway in chronic pain conditions. Cells. 2023;12(8):1178. doi:10.3390/cells12081178
37. Godoy LD, Rossignoli MT, Delfino-Pereira P, Garcia-Cairasco N, de Lima Umeoka EH. A comprehensive overview on stress neurobiology: basic concepts and clinical implications. Front Behav Neurosci. 2018;12:127. doi:10.3389/fnbeh.2018.00127
38. Ayyar VS, Sukumaran S. Circadian rhythms: influence on physiology, pharmacology, and therapeutic interventions. J Pharmacokinet Pharmacodyn. 2021;48(3):321–338. doi:10.1007/s10928-021-09751-2
39. Dong D, Yang D, Lin L, Wang S, Wu B. Circadian rhythm in pharmacokinetics and its relevance to chronotherapy. Biochem Pharmacol. 2020;178:114045. doi:10.1016/j.bcp.2020.114045
40. Okyar A, Ozturk Civelek D, Akyel YK, Surme S, Pala Kara Z, Kavakli IH. The role of the circadian timing system on drug metabolism and detoxification: an update. Expert Opin Drug Metab Toxicol. 2024;20(6):503–517. doi:10.1080/17425255.2024.2356167
41. Schurhoff N, Toborek M. Circadian rhythms in the blood-brain barrier: impact on neurological disorders and stress responses. Mol Brain. 2023;16(1):5. doi:10.1186/s13041-023-00997-0
42. Bumgarner JR, McCray EW, Nelson RJ. The disruptive relationship among circadian rhythms, pain, and opioids. Front Neurosci. 2023;17:1109480. doi:10.3389/fnins.2023.1109480
43. Liu X, Zhao J. Circadian rhythms in opioid-induced hyperalgesia: call for comprehensive research. Comment on Br J Anaesth 2023; 131: 1072-81. Br J Anaesth. 2024;132(2):440–441. doi:10.1016/j.bja.2023.11.027
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.