Back to Journals » Infection and Drug Resistance » Volume 16
Distribution and Antibiotic Resistance Characteristics of Bacteria Isolated from Blood Culture in a Teaching Hospital in Vietnam During 2014–2021
Authors Van An N ![]() , Hoang LH
, Hoang LH ![]() , Le HHL, Thai Son N, Hong LT, Viet TT, Le TD
, Le HHL, Thai Son N, Hong LT, Viet TT, Le TD ![]() , Thang TB, Vu LH, Nguyen VTH, Xuan Nguyen K
, Thang TB, Vu LH, Nguyen VTH, Xuan Nguyen K ![]()
Received 21 December 2022
Accepted for publication 16 March 2023
Published 23 March 2023 Volume 2023:16 Pages 1677—1692
DOI https://doi.org/10.2147/IDR.S402278
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Nguyen Van An,1,* Le Huy Hoang,2,* Hai Ha Long Le,3,4 Nguyen Thai Son,1 Le Thu Hong,1 Tien Tran Viet,5 Tuan Dinh Le,6 Ta Ba Thang,7 Luong Huy Vu,8,9 Vinh Thi Ha Nguyen,9,10 Kien Xuan Nguyen11
1Department of Microbiology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 2Department of Bacteriology, National of Hygiene and Epidemiology, Hanoi, Vietnam; 3Department of Microbiology, Mycology and Parasitology, National hospital of Dermatology and Venereology, Hanoi, Vietnam; 4Department of Clinical Microbiology and Parasitology, Ha Noi Medical University, Hanoi, Vietnam; 5Department of Infectious Diseases, Military Hospital 103, Vietnam Medical Military University, Hanoi, Vietnam; 6Department of Rheumatology and Endocrinology, Military Hospital 103, Vietnam Medical Military University, Hanoi, Vietnam; 7Respiratory Center, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 8Department of Laser and Skin Care, National hospital of Dermatology and Venereology, Hanoi, Vietnam; 9Department of Dermatology and Venereology, Ha Noi Medical University, Hanoi, Vietnam; 10Department of General Planning, National hospital of Dermatology and Venereology, Hanoi, Vietnam; 11Department of Military Medical Command and Organization, Vietnam Medical Military University, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Kien Xuan Nguyen, Department of Military Medical Command and Organization, Vietnam Medical Military University, Hanoi, Vietnam, Email [email protected]
Purpose: Studies on the epidemiology of bloodstream infection (BSI) and antimicrobial resistance (AMR) are limited in Vietnam. Thus, the present study aimed to elucidate the epidemiology of BSI and AMR of BSI-causing bacteria in Vietnam.
Methods: Data regarding blood cultures from 2014 to 2021 were collected and analyzed using the chi-square test, Cochran–Armitage test, and binomial logistic regression model.
Results: Overall, 2405 (14.15%) blood cultures were positive during the study period. In total, 55.76% of BSIs occurred in patients aged ≥ 60 years. The male-to-female ratio of patients with BSI was 1.87:1. Escherichia coli (26.11%), Staphylococcus aureus (15.79%), Klebsiella pneumoniae (10.44%), Acinetobacter baumannii (4.70%), and Pseudomonas aeruginosa (3.45%) were the leading bacterial species causing BSI. The AMR rate of these bacteria isolated in the intensive care unit (ICU) was significantly higher compared with that of those in other wards. E. coli was the least resistant to carbapenems (2.39%– 4.14%), amikacin (3.85%), and colistin (11.54%) and most resistant to penicillins (> 80.0%). S. aureus was the least resistant to glycopeptides (0%– 3.38%), quinupristin-dalfopristin (0.59%), and linezolid (1.02%) and most resistant to clindamycin (71.57%). K. pneumoniae was the least resistant to ertapenem (8.86%), amikacin (9.39%), and colistin (15.38%) and most resistant to aztreonam (83.33%). A. baumannii was the least resistant to amikacin (16.67%) and colistin (16.67%) and highly resistant to other antibiotics (≥ 50.0%). P. aeruginosa was the least resistant to colistin (16.33%) and piperacillin (28.17%) and highly resistant to other antibiotics (≥ 50.0%). Notably, the multidrug resistance rate of E. coli (76.41%) was the highest among common pathogens, followed by A. baumannii (71.57%), P. aeruginosa (64.56%), S. aureus (56.99%), and K. pneumoniae (43.72%).
Conclusion: The AMR rate of BSI-causing bacteria, particularly strains isolated from ICU, was alarmingly high. There is a need for new antibiotics, therapeutic strategies, as well as prevention and control to combat BSI and AMR.
Keywords: bloodstream infection, antimicrobial resistance, multidrug resistance, methicillin-resistantStaphylococcus aureus
Introduction
Globally, antimicrobial-resistant bacteria (ARB) are recognized as a threat to public health. In 2019, ARB infections led to 4.95 million deaths worldwide. Notably, bloodstream infection (BSI) with ARB was the second leading cause of death, accounting for approximately 1.4 million deaths in 2019.1 The distribution and resistance patterns of BSI-causing pathogens vary according to the time, geographical location, environment, population, and healthcare expenditure.2,3 Although S. aureus, E. coli, and K. pneumoniae were recognized as the leading BSI-causing bacteria in the Asian population,4,5 coagulase-negative Staphylococcus (CoNS) and Salmonella were the most common BSI-causing bacteria in European and African populations, respectively.4–7 The proportion of resistance of BSI-causing E. coli and K. pneumoniae to third-generation cephalosporins was 10.7%–43.7% and 7.4%–45.7%, respectively. In contrast, imipenem, meropenem, amikacin, colistin, and tigecycline were among the most effective antibiotics used for treating BSI caused by E. coli and K. pneumoniae.4,5 Further, A. baumannii isolated from BSI was highly resistant to most antibiotics, except for colistin and tigecycline. Similarly, these antibiotics were highly effective for the treatment of BSI caused by P. aeruginosa.4,5,8 BSI-causing S. aureus was highly resistant to erythromycin, penicillins, and clindamycin. In contrast, S. aureus was least resistant to vancomycin, linezolid, quinupristin-dalfopristin, and tigecycline.8,9 Notably, antimicrobial resistance (AMR) surveillance is important for the treatment and prevention of BSI as it provides data regarding resistance proportion, trends, and patterns, which are critical for developing treatment guidelines. Unfortunately, studies on AMR of BSI-causing pathogens in Vietnam, particularly long-term studies, are limited. Therefore, this study aimed to provide information on the epidemiology of BSI and AMR characteristics of BSI-causing bacteria in a large teaching hospital in Hanoi, Vietnam, from 2014 to 2021.
Materials and Methods
Pathogen Identification and Antimicrobial Susceptibility Test
Blood samples of patients were collected in commercial media bottles (BD, USA, and bioMérieux, France). A set of aerobic and anaerobic bottles was used for adults, whereas only aerobic bottles were used for children. Blood samples with volumes of 8–10 mL and 2–5 mL per bottle were collected from adults and children, respectively. Further, blood culture was performed using BD BACTEC FX40 (BD, USA) and BACT/ALERT 3D (bioMérieux, France). Positive blood samples were microscopically examined and subcultured on suitable media. Further, the suspected pathogens were detected using conventional biochemical tests10,11 and an automatic identification instrument (Vitek-2 Compact system, bioMérieux, France). Moreover, antimicrobial susceptibility testing (AST) was performed according to the guidelines of the Clinical & Laboratory Standards Institute (CLSI). AST was performed using disk diffusion, gradient diffusion, broth dilution, or the Vitek-2 Compact system. Antimicrobial susceptibility test disks were purchased from Oxoid, UK, and ETEST strips were purchased from bioMérieux, France. Colistin sulfate powder (Sigma-Aldrich, France) was used for broth dilution to evaluate the colistin susceptibility of bacteria. The AST results were interpreted as susceptible, intermediate, and resistant according to the latest CLSI guidelines at the time of testing.12,13 To control the quality of results, all laboratory activities were strictly conducted in accordance with ISO 15189.14 Internal quality control for blood culture media, ETEST strips, and antibiotics disks was conducted once a month or before using the new batch of these materials. Moreover, internal quality control for pathogen identification and AST on the Vitek-2 Compact system was conducted once a week. Staphylococcus aureus (ATCC 25923), Escherichia coli (ATCC 25922, NCTC 13846), and Pseudomonas aeruginosa (ATCC 27853) were used as reference bacterial strains for the internal quality control. Moreover, the laboratory participated in the external quality control programs for bacterial identification and AST of the Ministry of Health of Vietnam.
Data Collection
This was a retrospective study of blood culture conducted at Military Hospital 103 in Hanoi, Vietnam, from January 1, 2014, to December 31, 2021. Data were collected from the Microbiology Department, including the date and results of blood cultures as well as AST results, age, sex, and hospital ward. Only the first pathogen isolated from patients was analyzed in order to avoid bias due to duplicate isolates.
Definition of Multidrug-Resistant (MDR) Bacteria
MDR bacteria were defined as the bacteria that were nonsusceptible to ≥1 agent in ≥3 antimicrobial classes.15
Statistical Analysis
The chi-square test was performed to compare the differences in the proportion of positive blood cultures among the sex, age, and hospital ward groups. Moreover, this test was used to compare the differences in the rates of resistance to antibiotics among different bacterial species and hospital wards. Further, the Cochran–Armitage test for linear trends was performed to evaluate the significance of annual trends. The binomial logistic regression model was used to determine the potential predictors of bacterial infection, such as hospital ward, sex, and age. Statistical analysis was performed using SPSS Statistics 25.0 (IBM Corp, NY, USA) and R software version 4.2.1.
Ethical Statement
This study was approved by the Ethics Committee of Military Hospital 103, Hanoi, Vietnam (Approval number: 35/CNChT- HĐĐĐ). Moreover, the study was conducted in accordance with the principles of the Declaration of Helsinki. All patient data were anonymized before performing the analysis.
Results
Blood Culture
The total number of blood culture tests conducted from 2014 to 2021 was 17,002, of which 2405 (14.15%) were positive. The positivity rate ranged from 10.29% to 16.70% per year. The proportion of positive blood cultures was almost the same between men and women (approximately 14.0%). The rate of positive blood cultures in the age group of ≥60 years (16.09%) was significantly higher than that in the age group of 0–17 (8.66%) and 18–59 (12.48%) years. No significant difference in the rate of positive blood cultures was observed between the age groups of 0–17 and 18–59 years. Notably, among hospital wards, the intensive care unit had the highest percentage of positive blood cultures (19.27%). The rate of positive blood cultures in ICU was remarkably higher than that in other hospital wards, including the infectious disease (14.31%), internal medicine (12.21%), and surgery (12.20%) wards (Table 1).
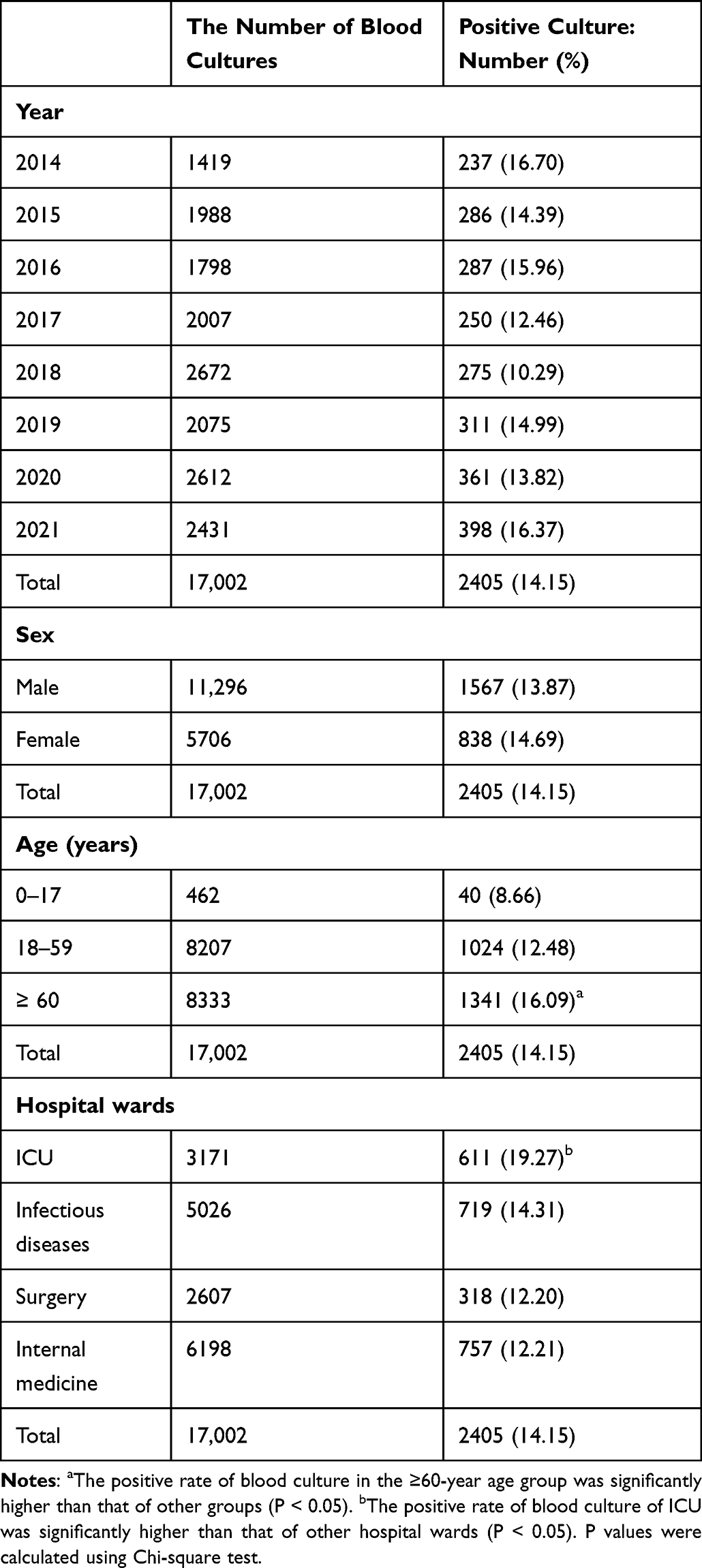 |
Table 1 Distribution of Blood Cultures |
Distribution of Bacteria
Gram-negative and gram-positive bacteria accounted for 64.12% and 28.73% of the positive blood cultures, respectively. The remaining 7.15% of the positive blood cultures were of fungus. The majority of pathogens isolated from blood cultures (accounting for 92.52% of the total pathogens) were E. coli (26.11%), S. aureus (12.56%), Klebsiella spp. (10.81%), Candida spp. (7.15%), Streptococcus spp. (7.07%), Burkholderia spp. (5.99%), Acinetobacter spp. (5.53%), CoNS (5.41%), Pseudomonas spp. (3.83%), Enterococcus spp. (3.33%), Stenotrophomonas maltophilia (2.37%), and Enterobacter spp. (2.37%) (Table 2). The remaining 7.48% of the pathogens included various types of bacteria with low frequency (Supplementary Table 1). Over the 8 years from 2014 to 2021, there was an upward trend in the rate of BSI caused by E. coli, Klebsiella spp., Pseudomonas spp., and Enterococcus spp. However, the data revealed a downward trend in the rate of BSI caused by Streptococcus spp., Acinetobacter spp., S. maltophilia, and Candida spp. (Table 2). Further, K. pneumoniae (251/261), A. baumannii (113/133), and P. aeruginosa (82/92) were the main species of Klebsiella, Acinetobacter, and Pseudomonas genera isolated in the present study.
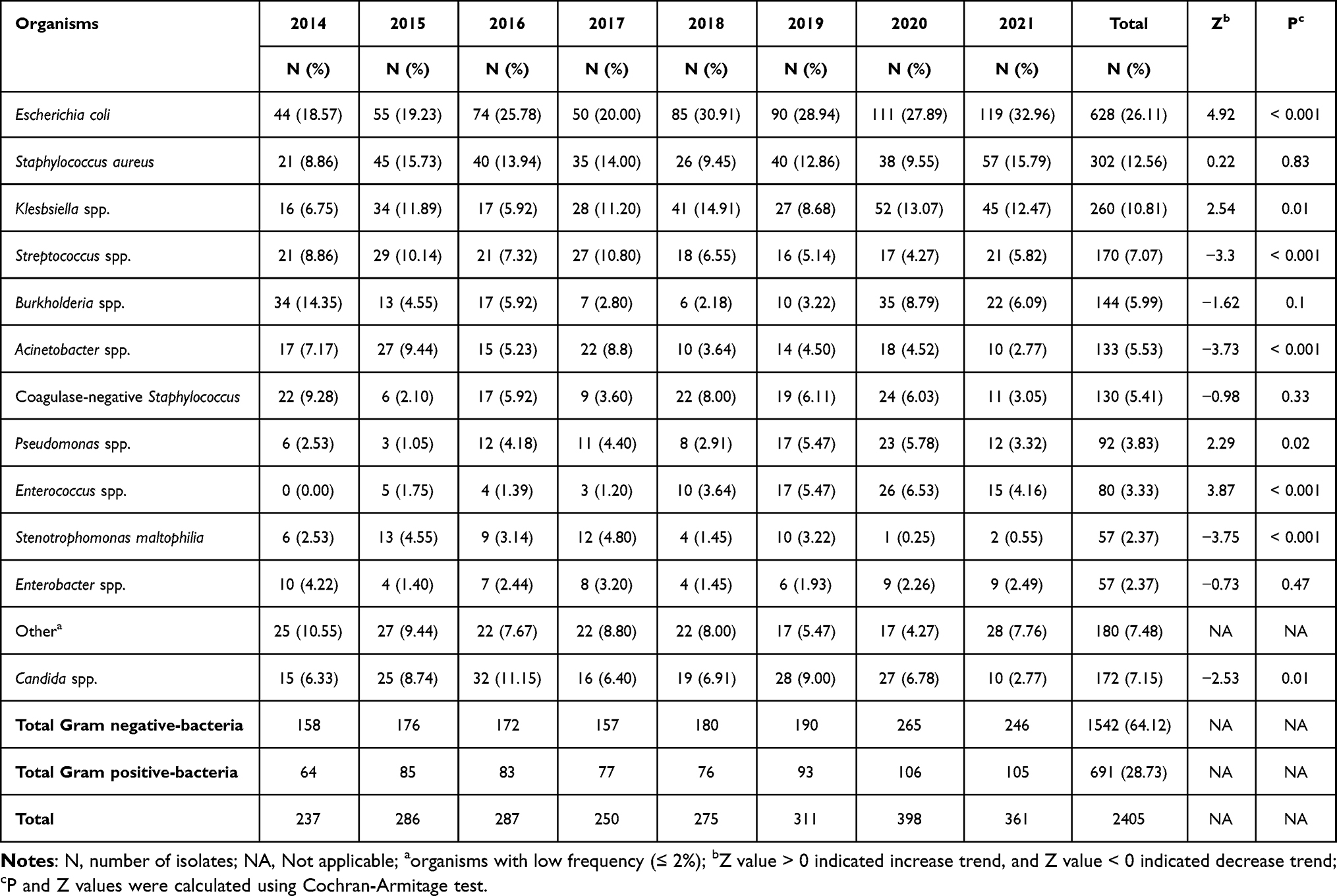 |
Table 2 The Pathogens Causing Bloodstream Infection |
Clinical Characteristics of Patients with BSI
The mean (standard deviation) age of BSI patients was 59.14 (18.86) years. Patients in the ≥60-year age group accounted for the largest proportion of BSI cases (55.76%; 1341/2405). In contrast, patients in the 0–17-year age group accounted for only 1.66% of BSI cases (40/2405). The remaining 42.58% (1024/2405) of patients with BSI were in the 18–59-year age group. The male-to-female ratio of patients with BSI was 1.87:1 (1567/838). The highest proportion of BSI cases was from the internal medicine ward (31.48%; 757/2405). The infectious disease ward and ICU had lower proportions of BSI (29.90% [719/2405] and 25.41% [611/2405], respectively). Further, surgery wards had the lowest proportion of BSI (13.22%; 318/2405) (Table 1).
Antibiotic Resistance Characteristics of Gram-Negative Bacteria
The resistance rate of E. coli isolates to carbapenems was the lowest in the Enterobacteriaceae family, and it ranged from 2.39% (ertapenem) to 4.14% (imipenem). Meanwhile, the proportion of resistance of K. pneumoniae and Enterobacter spp. to carbapenems ranged from 8.86% (ertapenem) to 29.25% (imipenem) and from 4.0% (ertapenem) to 23.26% (imipenem), respectively. However, the resistance rate of E. coli to fluoroquinolones and third-generation cephalosporins was higher than that of K. pneumoniae and Enterobacter spp. In particular, the proportion of resistance of E. coli to fluoroquinolones ranged from 54.27% (norfloxacin) to 61.54% (levofloxacin). However, the resistance rates of K. pneumoniae and Enterobacter spp. to fluoroquinolones ranged from 38.97% (norfloxacin) to 43.48% (levofloxacin) and from 23.08% (levofloxacin) to 33.33% (norfloxacin), respectively. Furthermore, the proportion of resistance of E. coli to third-generation cephalosporins ranged from 49.38% (ceftazidime) to 61.75% (cefotaxime), whereas the proportion of resistance of K. pneumoniae ranged from 33.33% (ceftriaxone) to 45.12% (ceftazidime) and that of Enterobacter spp. ranged from 39.47% (cefotaxime) to 50.0% (ceftriaxone). The resistance rate of Enterobacteriaceae to aminoglycosides varied widely. The resistance rates of E. coli, K. pneumoniae, and Enterobacter spp. isolates to aminoglycosides ranged from 3.85% (amikacin) to 37.74% (gentamicin), from 9.39% (amikacin) to 43.48% (tobramycin), and from 10.20% (amikacin) to 35.90% (gentamicin), respectively. The resistance rates of E. coli and K. pneumoniae to colistin were 11.54% and 13.58%, respectively. Although the proportion of resistance of E. coli was the highest against ampicillin (89.47%), piperacillin (82.61%), and trimethoprim-sulfamethoxazole (70.71%), the resistance rate of K. pneumoniae to aztreonam (83.33%) and piperacillin (71.41%) was the highest among the tested antibiotics (Table 3). Over the study period, there were downward trends in amoxicillin-clavulanate- and ceftazidime-resistant E. coli. Notably, amoxicillin-clavulanate-resistant E. coli isolates significantly decreased from 39.39% in 2014 to 19.47% in 2021 (annual trend P value < 0.05), and ceftazidime-resistant E. coli isolates declined from 59.26% in 2014 to 33.04% in 2021 (annual trend P value < 0.05). In contrast, ciprofloxacin-resistant E. coli isolates increased from 42.42% in 2014 to 62.73% in 2021 (annual trend P value < 0.05). Meropenem-resistant K. pneumoniae substantially increased from 15.79% in 2018 to 37.84% in 2021 (annual trend P value < 0.05) (Figure 1). Among the nonfermentative gram-negative bacteria, the resistance rate of A. baumannii to carbapenems ranged from 57.58% (imipenem) to 60.82% (meropenem), whereas the resistance rate of P. aeruginosa ranged from 55.41% (meropenem) to 58.67% (imipenem). The proportion of resistance of A. baumannii and P. aeruginosa to fluoroquinolones (such as ciprofloxacin and levofloxacin) was >60%. The resistance rates of A. baumannii to piperacillin-tazobactam and ticarcillin-clavulanate were 71.64% and 69.23%, respectively, and those of P. aeruginosa were 66.67% and 67.57%, respectively. Further, the proportion of resistance of A. baumannii to aminoglycosides varied widely between 16.67% (amikacin) and 61.11% (gentamicin) and that of P. aeruginosa varied from 32.0% (amikacin) to 58.90% (tobramycin). The resistance rates of A. baumannii and P. aeruginosa to colistin were almost the same (approximately 16.0%) (Table 3).
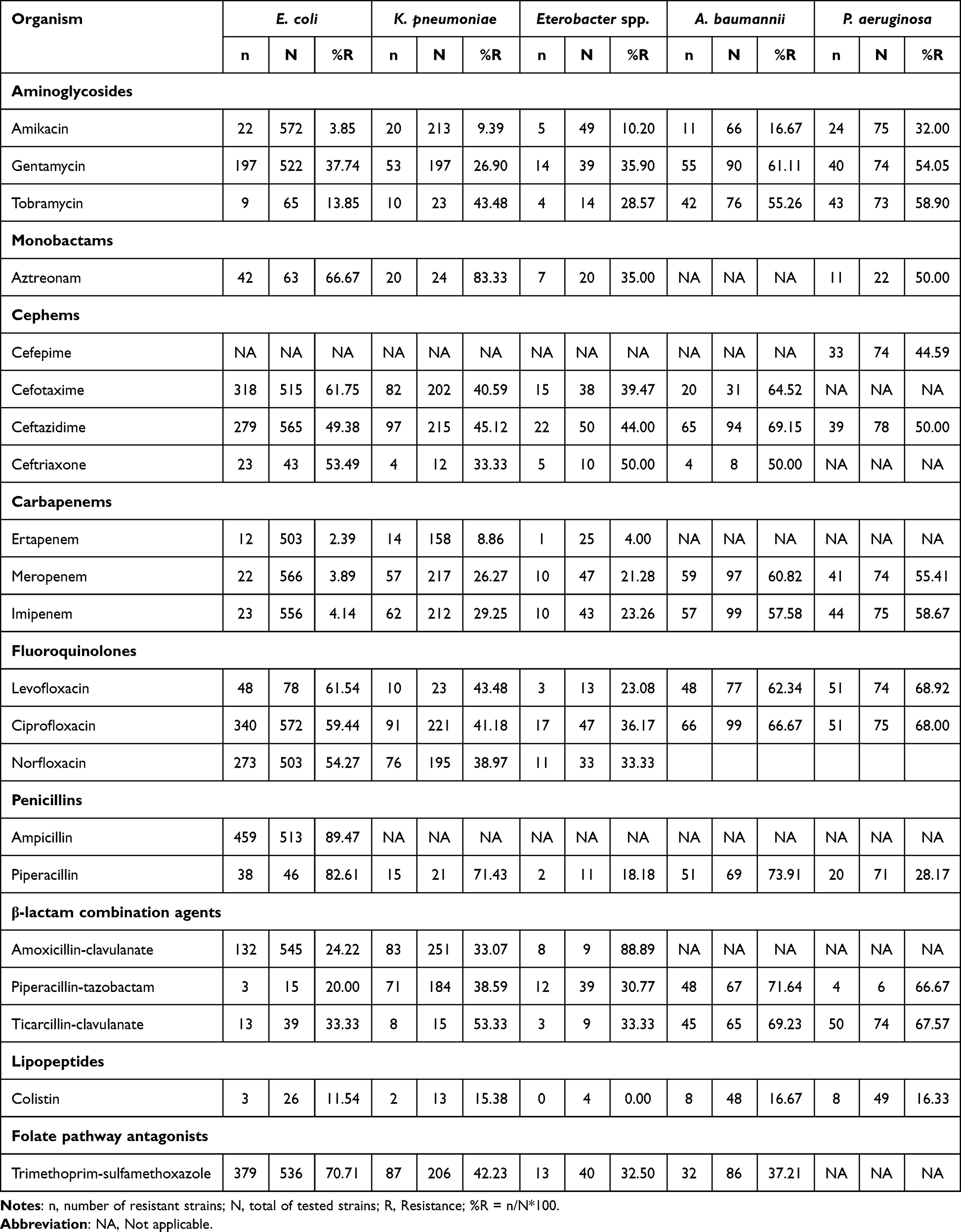 |
Table 3 Antimicrobial Resistance to Selected Antibiotics of Gram-Negative Bacteria |
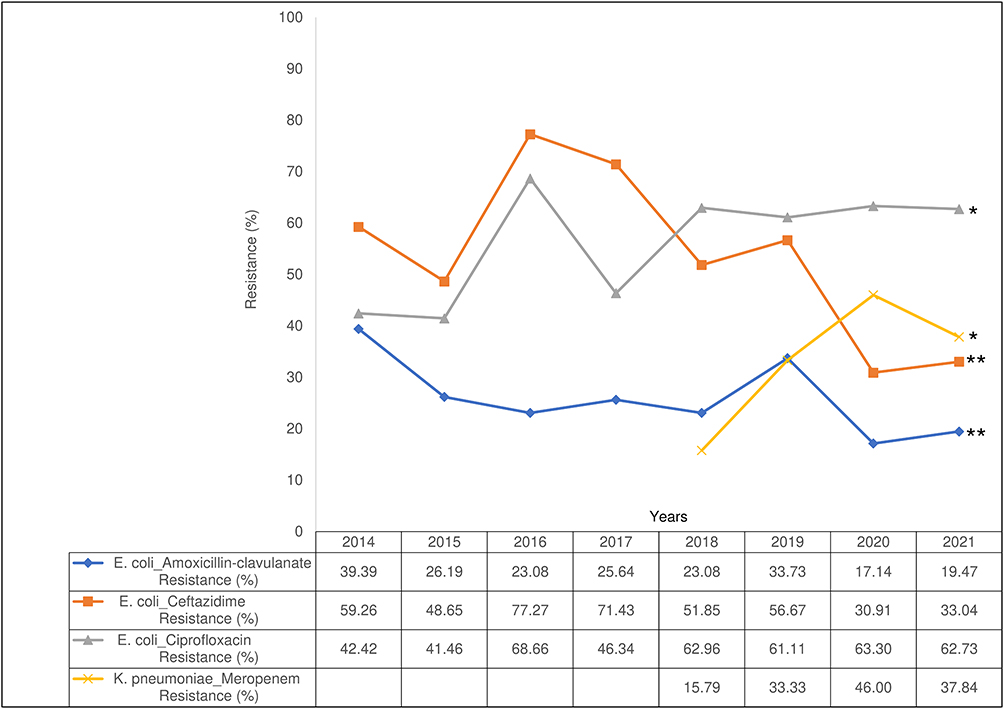 |
Figure 1 Resistance trend of Escherichia coli and Klebsiella pneumoniae. *Upward trend (Z > 0; P < 0.05); **Downward trend (Z < 0; P < 0.05). P and Z values were calculated using the Cochran–Armitage test. |
Antibiotic Resistance Characteristics of Gram-Positive Bacteria
The resistance rate of Enterococcus spp. to fluoroquinolones was the highest among gram-positive pathogens, ranging from 72.73% (levofloxacin) to 85.71% (norfloxacin). The proportion of resistance of CoNS to fluoroquinolones was considerably higher than that of S. aureus, except for norfloxacin. The resistance rates of CoNS to ciprofloxacin, levofloxacin, and moxifloxacin were 51.96%, 50.0%, and 37.21%, respectively, and those of S. aureus were 32.23%, 30.29%, and 27.78%, respectively. Meanwhile, the resistance rates of CoNS and S. aureus to norfloxacin were 43.75% and 46.43%, respectively. However, the resistance rate of Streptococcus spp. to norfloxacin was 8.87%. The proportion of resistance of S. aureus to macrolides (such as erythromycin, azithromycin, and clarithromycin) was approximately 70.0%, whereas that of CoNS ranged from 60.0% (clarithromycin) and 74.67% (erythromycin) and that of Streptococcus spp. ranged from 58.33% (azithromycin) to 80.0% (clarithromycin). The resistance rates of S. aureus and CoNS to doxycycline were <10.0%, whereas those of S. aureus and CoNS to tetracycline were >50.0%. The resistance rate of Enterococcus spp. isolates to tetracyclines ranged from 55.56% (doxycycline) to 84.72% (tetracycline). Further, the resistance rates of S. aureus and CoNS to linezolid, quinupristin-dalfopristin, and vancomycin were <9.0%; however, Streptococcus spp. were not resistant to linezolid and vancomycin but resistant to quinupristin-dalfopristin (>15.0%) (Table 4).
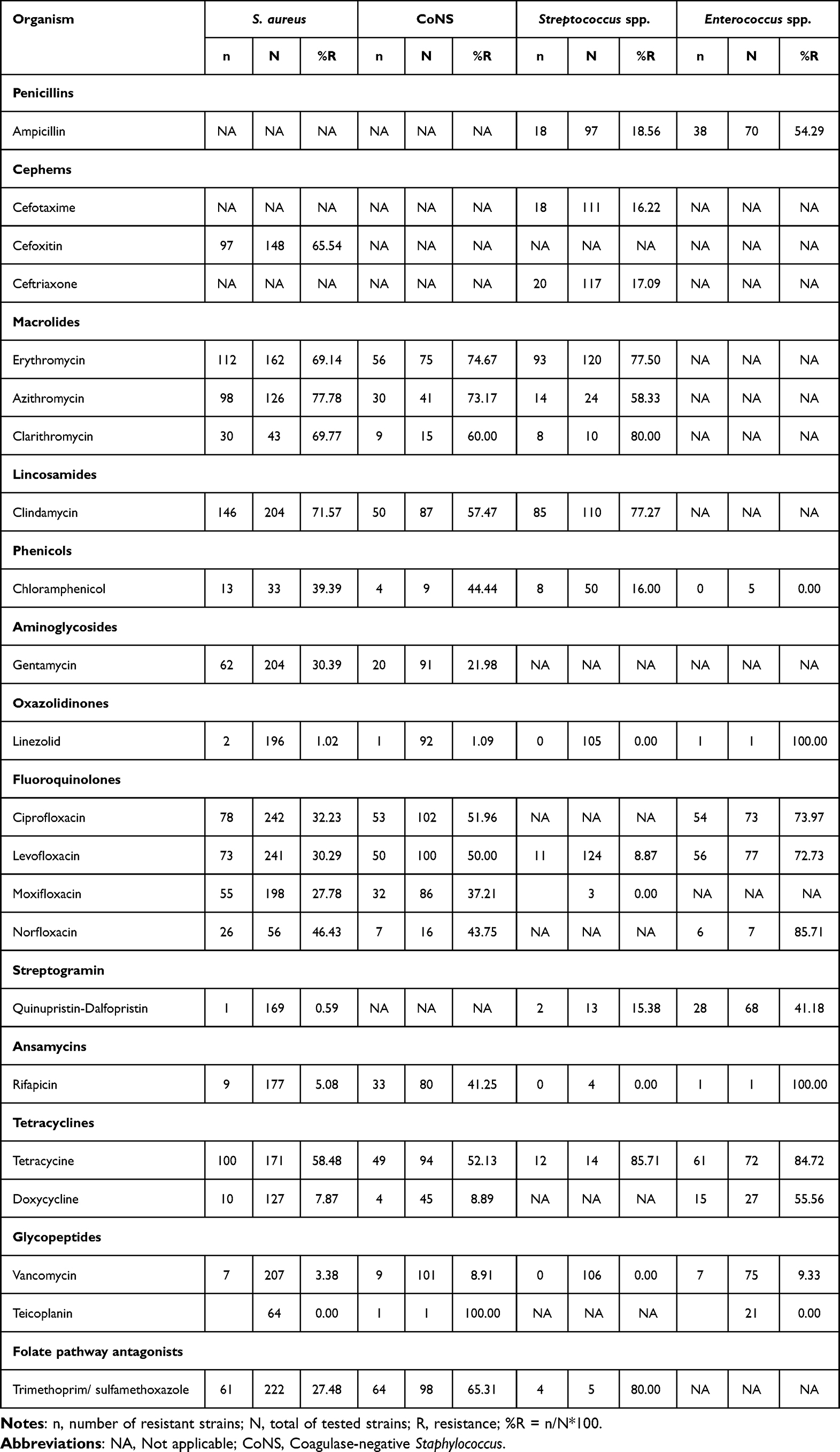 |
Table 4 Antimicrobial Resistance to Selected Antibiotics of Gram-Positive Bacteria |
AMR Characteristics of Methicillin-Resistant Staphylococcus Aureus (MRSA)
During the study period, the prevalence of MRSA was 65.54% (97/148). The resistance rate of MRSA to common antibiotics was higher than that of methicillin-susceptible Staphylococcus aureus (MSSA). Moreover, the resistance rates of MRSA and MSSA to norfloxacin, levofloxacin, ciprofloxacin, clindamycin, and erythromycin were significantly different (Figure 2).
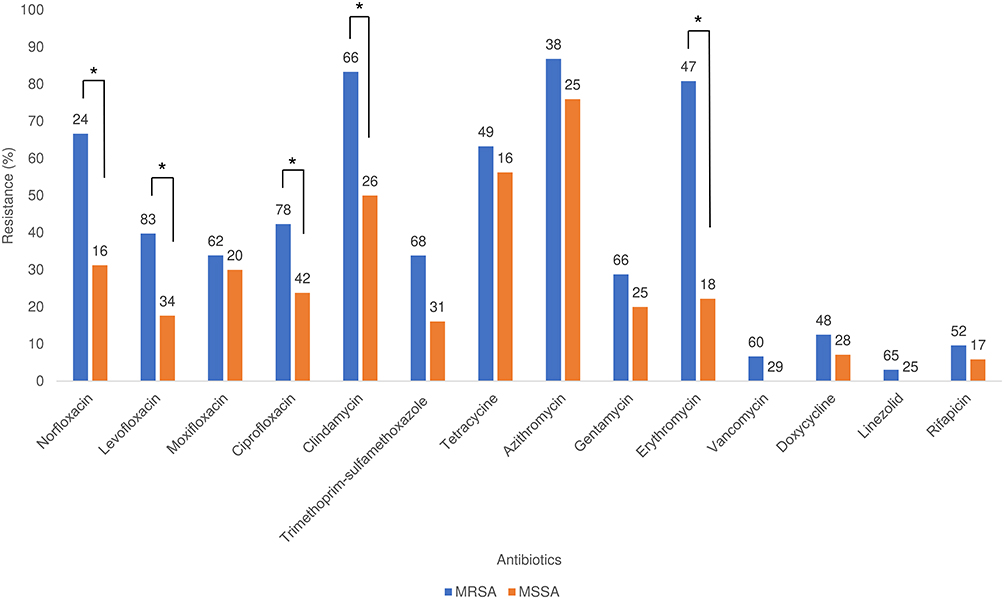 |
Figure 2 Antimicrobial resistance of methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible Staphylococcus aureus (MSSA). The number on the top of each column indicates the tested bacterial strains. *P < 0.05 according to the chi-square test. |
MDR Bacteria Causing BSI
Among the five common BSI-causing bacterial pathogens, the proportion of MDR pathogens was the highest in E. coli (76.41%). Notably, MDR strains accounted for 71.57% of the total A. baumannii. Further, the MDR rates of P. aeruginosa, S. aureus, and K. pneumoniae were 64.56%, 56.99%, and 43.72%, respectively (Table 5). The MDR rate among S. aureus substantially increased over the 8-year period, which increased from 23.53% in 2014 to 73.21% in 2021 (annual trend P value < 0.05). Finally, the MDR proportion among the other bacterial species increased over the study period (Figure 3).
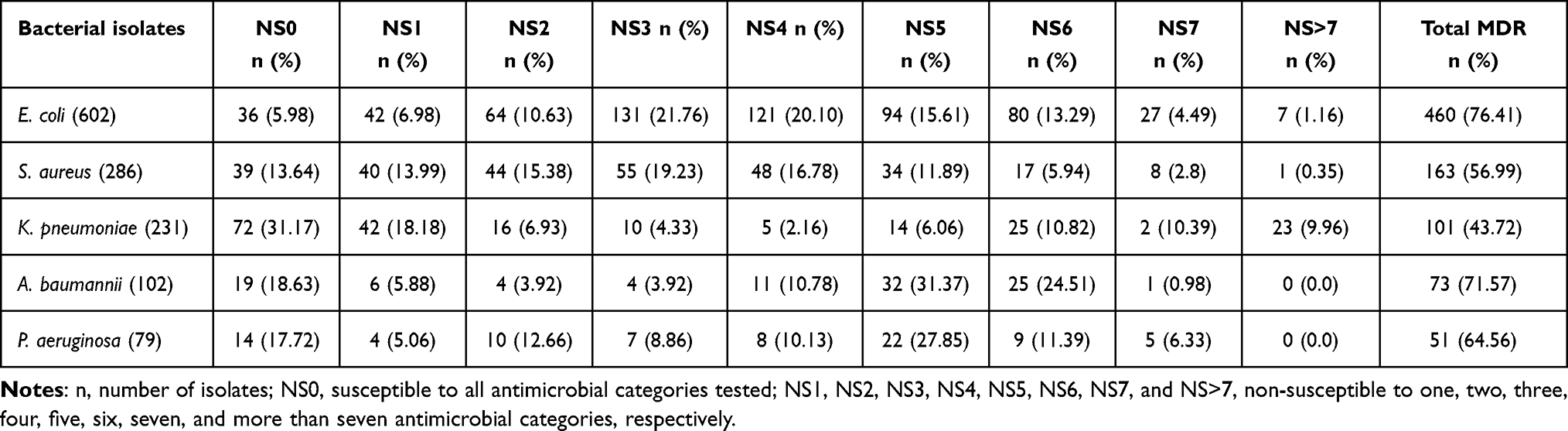 |
Table 5 Antimicrobial Resistance Pattern of Common Bacteria Causing BSI |
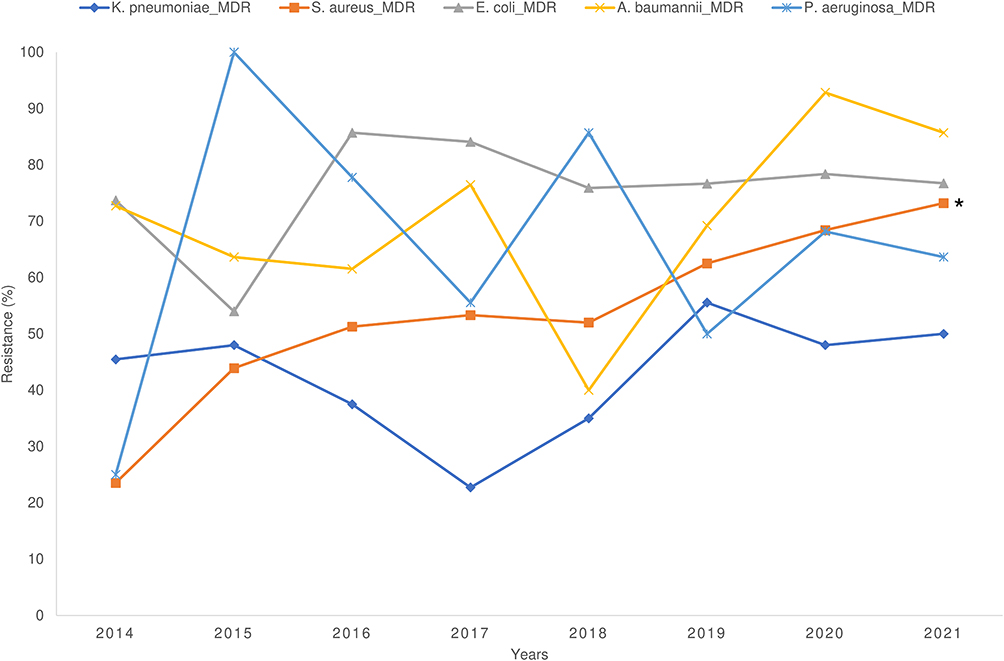 |
Figure 3 Trend of multidrug-resistance of bloodstream infection-causing common bacterial species. *Upward trend (Z > 0; P < 0.05). P and Z values were calculated using the Cochran–Armitage test. |
Analysis of AMR of Bacteria Isolated from ICU and Non-ICU Wards
Among E. coli isolates, the resistance rate of strains isolated from ICU to amoxicillin-clavulanate (AMC), cefotaxime (CTX), ceftazidime (CAZ), ciprofloxacin (CIP), norfloxacin (NOR), imipenem (IPM), meropenem (MEM), and fosfomycin (FOS) was significantly higher than that of strains isolated from non-ICU wards (P < 0.05). Moreover, the resistance rate of E. coli strains isolated from ICU to imipenem and meropenem was approximately three times higher than that of the strains isolated from non-ICU wards (ICU: 9.57% and 9.38%; non-ICU wards: 3.03% and 2.77%) (Figure 4A). The proportion of resistance of S. aureus strains isolated from ICU to fluoroquinolone agents was significantly higher than that of the strains isolated from non-ICU wards (P < 0.05) (Figure 4B). The proportion of resistance of K. pneumoniae strains isolated from ICU to all commonly tested antibiotics was significantly higher than that of the strains isolated from non-ICU wards. Furthermore, the resistance rates of K. pneumoniae strains isolated from ICU to ertapenem (ETP), imipenem (IMP), and meropenem (MEM) (21.88%, 59.09%, and 56.06%) were approximately four times higher than those of the strains isolated from non-ICU wards (5.56%, 15.75%, and 13.25%) (Figure 4C). The resistance rate of A. baumannii isolated from ICU to the most commonly detected antibiotics, except trimethoprim-sulfamethoxazole (SXT), was significantly higher than that of the strains isolated from non-ICU wards (Figure 4D). The proportion of resistance of P. aeruginosa strains isolated from ICU to all commonly tested antibiotics was higher than that of the strains isolated from non-ICU wards. However, a significant difference in the resistance rate was observed only for meropenem (MEM), imipenem (IMP), and ceftazidime (CAZ), as shown in Figure 4E.
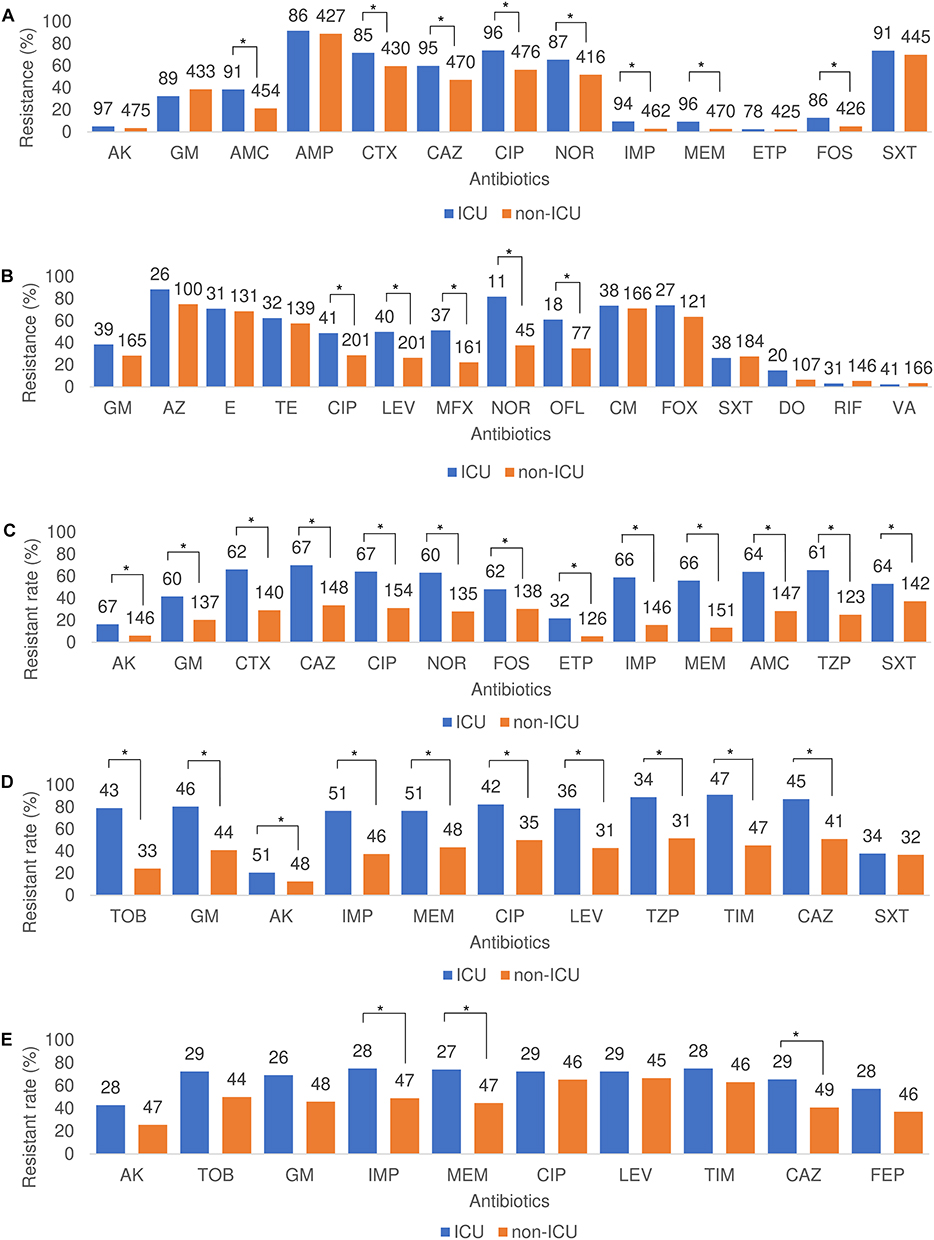 |
Figure 4 Resistance rate of bacteria to selected antibiotics in terms of hospital wards. (A) Antimicrobial resistance rate of E. coli. (B) Antimicrobial resistance rate of S. aureus. (C) Antimicrobial resistance rate of K. pneumoniae. (D) Antimicrobial resistance rate of A. baumannii. (E) Antimicrobial resistance rate of P. aeruginosa; the number on top of each column indicated the tested bacterial strains; *P < 0.05 according to the chi-square test. |
Binomial Logistic Regression Analysis
Age, sex, and hospital wards were significant predictors of bacterial pathogens (Table 6). Notably, men were more likely to be infected with K. pneumoniae (odds ratio [OR] = 1.38, 95% confidence interval [CI] = 1.03–1.85) and P. aeruginosa (OR = 1.96, 95% CI = 1.14–3.39) than women. In contrast, men were less likely to be infected with E. coli (OR = 0.48, 95% CI = 0.39–0.58) than women. The risks of infection with E. coli in the 18–59-year (OR = 3.87, 95% CI = 1.17–12.79) and ≥60-year (OR = 6.58, 95% CI = 2.00–21.64) age groups were significantly higher than those in the 0–17-year age group. In contrast, the risks of infection with S. aureus in the 18–59-year (OR = 0.19, 95% CI = 0.10–0.37) and ≥60-year (OR = 0.13, 95% CI = 0.07–0.24) age groups were lower than those in the 0–17-year age group. The risk of infection with E. coli (OR = 1.88, 95% CI = 1.49–2.39) and S. aureus (OR = 1.37, 95% CI = 1.02–1.86) among patients in non-ICU wards was significantly higher than that among patients in ICU. However, the risk of infection with A. baumannii (OR = 0.27, 95% CI = 0.19–0.40) and P. aeruginosa (OR = 0.57, 95% CI = 0.36–0.90) among patients in non-ICU wards was significantly lower than that of patients in ICU.
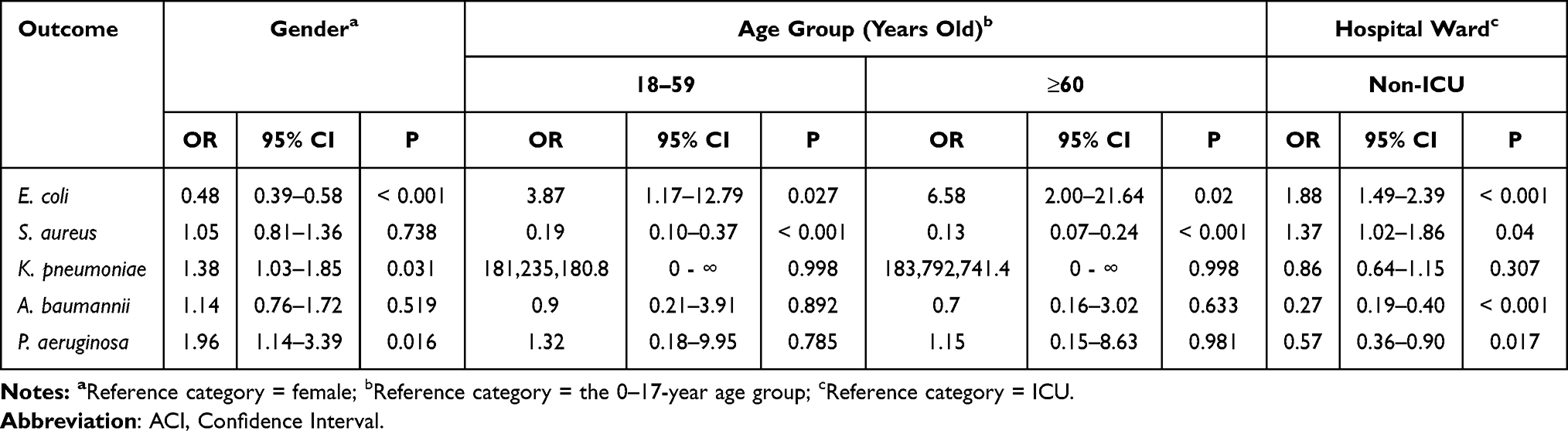 |
Table 6 Result of Binomial Logistic Regression Analysis |
Discussion
In the present study, the total number of positive blood cultures was 2405 (14.15%). Patients aged ≥60 years accounted for >50% of the total positive cases, and the rate of positive culture in this group was significantly higher than that in the younger age groups (Table 1). These findings were consistent with those of previous studies.16,17 Gram-negative bacteria (64.12%) were the dominant isolated pathogen group compared to gram-positive bacteria (28.73%) and fungi (7.15%). This finding was consistent with that of the Viet Nam Resistance network (VINARES),18,19 China Antimicrobial Surveillance Network (CHINET),20 and Korea Global AMR Surveillance System (Kor-GLASS).5 However, this finding was different from that of several studies in Europe and Africa, which reported that gram-positive bacteria were the most common BSI-causing pathogen group.2,8 The present study reported that E. coli (26.11%) was the most common BSI-causing pathogen, followed by S. aureus (15.79%) and K. pneumoniae (10.44%, 251/2405). This finding was similar to that of the VINARES report in 2016–2017 among 13 hospitals for BSI and other bacterial infections, the CHINET report in 2018 among 44 hospitals for BSI, and the Kor-GLASS report in 2017–2019 among 8 hospitals for BSI alone.4,5,19 However, this finding was different from that of the studies in European and African hospitals, indicating that CoNS and Salmonella were the most common BSI-causing pathogens in Italy and the Democratic Republic of the Congo, respectively.8,9 The variations in geographical and environmental characteristics and expenditure on healthcare may contribute to the differences in the distribution of BSI-causing bacterial pathogens between the present and other studies.3 Infection with MDR E. coli significantly increased the mortality rate among infected patients.21,22 The present study found that MDR strains accounted for >75% of the total BSI-causing E. coli isolates, and this proportion was higher than that in the data on MDR E. coli reported by VINARES (29%) (Table 5).19 Additionally, E. coli was the leading cause of BSI for all 8 years. Moreover, the present study found that the proportion of E. coli significantly increased over the 8-year period (Table 2). These results revealed that there might be an increase in the number of MDR E. coli isolates at our hospital, and the treatment of BSI caused by E. coli might be more challenging in the future. Furthermore, the present study found that the proportion of resistance of K. pneumoniae to carbapenem (22.66%, 133/587) was higher than that of other bacteria in the Enterobacteriaceae family (Enterobacter spp. [18.26%, 21/115] and E. coli [3.51%, 57/1625]) (Table 3). The VINARES report for 2016–2017 indicated that the resistance rates to carbapenems of K. pneumoniae, Enterobacter spp., and E. coli isolated in blood and cerebrospinal fluid samples were 23%, 26%, and 8%, respectively, which were slightly higher than those reported in our study.19 In contrast, the data of Kor-GLASS on BSI from 2017 to 2019 indicated that the resistance rates of K. pneumoniae and E. coli to carbapenems were 1.0%–1.4% and 0.1%–0.2%, respectively, which were much lower than those in our study.5 A previous study on BSI in Beijing, China, from 2010 to 2018 reported that the resistance rate of K. pneumoniae to carbapenems (26.58%) was moderately higher than that in our study, but the resistance rate of E. coli to carbapenems (2.58%) was substantially lower than that in our study.23 Notably, there was an upward trend in meropenem-resistant K. pneumoniae isolates from 2018 to 2021 (15.79%–37.84%, P < 0.05) (Figure 1). A previous study indicated that the spread of KPC-producing Enterobacteriaceae contributed to the increase in the isolates of carbapenem-resistant bacteria in Vietnam.24 Moreover, we observed very high resistance rates of A. baumannii (59.18%, 116/196) and P. aeruginosa to carbapenems (57.05%, 85/149) (Table 3). The resistance rate of BSI-causing A. baumannii to carbapenems in our study was lower than that in VINARES, Kor-GLASS, and a study on BSI conducted in Beijing, China, from 2010–2018. However, the resistance rate of P. aeruginosa to carbapenems in our study was significantly higher than that in these studies.5,19,23 The data of our study indicated that the majority of the carbapenem-resistant strains of E. coli, K. pneumoniae, A. baumannii, and P. aeruginosa were MDR. Furthermore, the proportion of MDR strains of these four gram-negative bacteria and S. aureus was tremendously high (Table 5). Infection with carbapenem-resistant and MDR bacteria causes prolonged hospital stays as well as increases the treatment costs and mortality rate.25,26 Carbapenems are considered the last-choice antibiotics for infections caused by MDR bacteria owing to their wide-spectrum antimicrobial activity and great potential against bacteria.27 However, with the increase in MDR and carbapenemase-producing bacteria, the treatment of patients infected with these bacteria poses a huge challenge.36 The proportion of colistin resistance of E. coli (11.54%), A. baumannii (16.67%), and P. aeruginosa (16.33%) in the present study was substantially higher than that in previous studies conducted in China, Korea, and Thailand. Moreover, the resistance rate of K. pneumoniae to colistin in the present study (15.38%) was higher than that in studies from China and Korea but slightly lower than that in a study from Thailand.4,5,28 Colistin—an old bactericidal antibiotic—is one of the last-choice of therapeutics used for the treatment of infection by carbapenem-resistant bacteria.29 Therefore, the high proportion of carbapenem-resistant bacteria in our study might lead to an increased colistin use and subsequently colistin resistance. It has been reported that genes encoding colistin resistance (mcr-1 to mcr-10), especially mcr-1, have been reported to be distributed worldwide in animals, environment, food, and travel.30–32 Additionally, bacterial strains harboring mcr-1 have been isolated from clinical specimens, animals, communities, and food in Vietnam.33,34 Notably, we recently detected mcr-9-carrying IncHI2 plasmids in BSI-causing Enterobacteriaceae at our hospital.35 Thus, the spread of mobile colistin resistance genes may contribute to the high rate of resistance to colistin. The results of our study suggest that developing new antibiotics and suitable therapeutic strategies, including a combination of antibiotics, is necessary for treating MDR and carbapenem-resistant bacteria. Our data revealed that the frequency of MRSA was 65.54%, which was significantly higher than that of the data from CHINET in 2014–2017 (35.3%–44.6%) and Kor-GLASS in 2017–2019 (49.6%) but lower than that of data from VINARES in 2016–2017 (73%).4,5,19 Furthermore, the resistance rate of MRSA to most tested antibiotics was higher than that of MSSA (Figure 2). However, MRSA remains a serious health concern. Patients infected with MRSA have a longer hospitalization and higher mortality rate than those infected with MSSA. Vancomycin and linezolid are preferred options for treating patients with some antimicrobial gram-positive bacteria, such as MRSA, because of their effectiveness against these bacteria.37,38 Unfortunately, our data revealed that the resistance rates of MRSA to vancomycin and linezolid were 6.67% and 3.08%, respectively; in contrast, no MSSA strain was found to be resistant to vancomycin or linezolid (Figure 2). MRSA, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant A. baumannii, and carbapenem-resistant P. aeruginosa are included in the list of bacteria that pose the greatest threat to global health based on the first report by the World Health Organization in 2017; thus, there is an urgent need for new antibiotics to treat these pathogens.39 We observed that the proportion of resistance of E. coli, S. aureus, K. pneumoniae, A. baumannii, and P. aeruginosa isolated from ICU to the most tested antibiotics was substantially higher than that of strains isolated from non-ICU wards (Figure 4). Our finding was similar to that of the VINARES study conducted in 13 hospitals in Vietnam between 2016 and 2017 and a previous study conducted in Greece between 2018 and 2019.19,40 Furthermore, the present study found a very high resistance rate of A. baumannii and P. aeruginosa isolated from ICU. A. baumannii isolated from ICU were resistant to 8 out of 10 commonly tested antibiotics (76.47%–91.18%), excluding trimethoprim-sulfamethoxazole (SXT) (37.78%) and amikacin (AK) (20.59%). Meanwhile, P. aeruginosa isolated from ICU were resistant to 8 out of 10 commonly tested antibiotics (65.52%–75.0%), excluding cefepime (FEP) (57.14%) and amikacin (AK) (42.86%) (Figure 4D and E). In addition, the results of the binomial logistic regression analysis revealed that A. baumannii and P. aeruginosa were more likely to cause infections in ICU patients than in non-ICU patients (Table 6). In ICUs, patients usually have a serious condition and underlying diseases. Additionally, in the course of treating such patients, invasive devices and medical equipment, such as mechanical ventilators, are often required. These factors may contribute to the spread of bacterial pathogens, particularly MDR strains.41,42 The results of our study indicated that the rate of positive blood cultures was significantly higher in patients in ICU than in those in other hospital wards (Table 1).
Conclusions
The present study revealed that E. coli, S. aureus, K. pneumoniae, A. baumannii, and P. aeruginosa were the leading BSI-causing bacterial species, and there was a significant upward trend for E. coli, Klebsiella spp., and Pseudomonas spp isolated from BSI. Overall, the AMR rate of BSI-causing bacteria, especially bacterial strains isolated from ICU, was alarmingly high. Although the resistance rates to amikacin and colistin were relatively high among the most common BSI-causing gram-negative bacteria, these agents are still considered the best choice for the treatment of BSI caused by gram-negative bacteria. Similarly, Enterobacteriaceae were relatively highly carbapenem-resistant. Nevertheless, carbapenems remain an effective therapeutic option for the treatment of BSI caused by Enterobacteriaceae. Glycopeptides, quinupristin-dalfopristin, and linezolid are the most effective antibiotics used to treat BSI caused by S. aureus. Our results indicate the need for new antibiotics, therapeutic strategies, as well as prevention and control measures to combat BSI and AMR.
Abbreviations
AK, Amikacin; GM, Gentamicin; AMC, Amoxicillin-clavulanate; AMP, Ampicillin; CTX, Cefotaxime; CAZ, Ceftazidime; CIP, Ciprofloxacin; NOR, Norfloxacin; IMP, Imipenem; MEM, Meropenem; ETP, Ertapenem; FOS, Fosfomycin; SXT, Trimethoprim-sulfamethoxazole; AZ, Azithromycin; E, Erythromycin; TE, Tetracycline; LEV, Levofloxacin; MFX, Moxifloxacin; OFL, Ofloxacin; CM, Clindamycin; FOX, Cefoxitin; DO, Doxycycline; RIF, Rifampicin; VA, Vancomycin; TZP, Piperacillin-tazobactam; TOB, Tobramycin; TIM, Ticarcillin-clavulanate; FEP, Cefepime.
Data Sharing Statement
All data used for analyzing and generating the results of this study are included in this article.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Military Hospital 103, Hanoi, Vietnam (Approval No. 35/CNChT- HĐĐĐ). All patient data were anonymized before performing the analysis.
Acknowledgments
We would like to thank the staff of the Microbiology Department, Military Hospital 103, for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
2. Deku JG, Dakorah MP, Lokpo SY, et al. The epidemiology of bloodstream infections and antimicrobial susceptibility patterns: a nine-year retrospective study at St. Dominic hospital, Akwatia, Ghana. J Trop Med. 2019;2019:6750864. doi:10.1155/2019/6750864
3. Fisman D, Patrozou E, Carmeli Y, et al. Geographical variability in the likelihood of bloodstream infections due to gram-negative bacteria: correlation with proximity to the equator and health care expenditure. PLoS One. 2014;9(12):e114548. doi:10.1371/journal.pone.0114548
4. Hu F, Guo Y, Yang Y, et al. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur J Clin Microbiol Infect Dis. 2019;38(12):2275–2281. doi:10.1007/s10096-019-03673-1
5. Kim D, Yoon EJ, Hong JS, et al. Major bloodstream infection-causing bacterial pathogens and their antimicrobial resistance in South Korea, 2017-2019: Phase I report from kor-GLASS. Front Microbiol. 2021;12:799084. doi:10.3389/fmicb.2021.799084
6. Schöneweck F, Schmitz RPH, Rissner F, et al. The epidemiology of bloodstream infections and antimicrobial susceptibility patterns in Thuringia, Germany: a five-year prospective, state-wide surveillance study (AlertsNet). Antimicrob Resist Infect Control. 2021;10(1):132. doi:10.1186/s13756-021-00997-6
7. Robledo J, Maldonado N, Robledo C, et al. Changes in antimicrobial resistance and etiology of blood culture isolates: results of a decade (2010-2019) of surveillance in a northern region of Colombia. Infect Drug Resist. 2022;15:6067–6079. doi:10.2147/IDR.S375206
8. Licata F, Quirino A, Pepe D, Matera G, Bianco A. Antimicrobial resistance in pathogens isolated from blood cultures: a two-year multicenter hospital surveillance study in Italy. Antibiotics. 2020;10(1). doi:10.3390/antibiotics10010010
9. Tack B, Phoba MF, Van Puyvelde S, et al. Salmonella typhi from blood cultures in the Democratic Republic of the Congo: a 10-year surveillance. Clin Infect Dis. 2019;68(Suppl 2):S130–7. doi:10.1093/cid/ciy1116
10. Leber AL. Clinical Microbiology Procedures Handbook.
11. Garcia LS. Clinical Microbiology Procedures Handbook.
12. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
13. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
14. International Organization for Standardization. ISO 15189-Medical Laboratories - Requirements for Quality and Competence.
15. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
16. Skogberg K, Lyytikäinen O, Ollgren J, Nuorti JP, Ruutu P. Population-based burden of bloodstream infections in Finland. Clin Microbiol Infect. 2012;18(6):E170–6. doi:10.1111/j.1469-0691.2012.03845.x
17. Mehl A, Åsvold BO, Lydersen S, et al. Burden of bloodstream infection in an area of Mid-Norway 2002-2013: a prospective population-based observational study. BMC Infect Dis. 2017;17(1):205. doi:10.1186/s12879-017-2291-2
18. Vu TVD, Do TTN, Rydell U, et al. Antimicrobial susceptibility testing and antibiotic consumption results from 16 hospitals in Viet Nam: the VINARES project 2012-2013. J Glob Antimicrob Resist. 2019;18:269–278. doi:10.1016/j.jgar.2019.06.002
19. Vu TVD, Choisy M, Do TTN, et al. Antimicrobial susceptibility testing results from 13 hospitals in Viet Nam: VINARES 2016-2017. Antimicrob Resist Infect Control. 2021;10(1):78. doi:10.1186/s13756-021-00937-4
20. Hu F, Zhu D, Wang F, Wang M. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(Suppl 2):S128-S34:S128–34. doi:10.1093/cid/ciy657
21. Lim C, Takahashi E, Hongsuwan M, et al. Epidemiology and burden of multidrug-resistant bacterial infection in a developing country. eLife. 2016;5. doi:10.7554/eLife.18082
22. MacKinnon MC, Sargeant JM, Pearl DL, et al. Evaluation of the health and healthcare system burden due to antimicrobial-resistant Escherichia coli infections in humans: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2020;9(1):200. doi:10.1186/s13756-020-00863-x
23. Zhu Q, Zhu M, Li C, et al. Epidemiology and microbiology of Gram-negative bloodstream infections in a tertiary-care hospital in Beijing, China: a 9-year retrospective study. Expert Rev Anti-Infect Ther. 2021;19(6):769–776. doi:10.1080/14787210.2021.1848544
24. Linh TD, Thu NH, Shibayama K, et al. Expansion of KPC-producing Enterobacterales in four large hospitals in Hanoi, Vietnam. J Glob Antimicrob Resist. 2021;27:200–211. doi:10.1016/j.jgar.2021.09.007
25. Stewardson AJ, Marimuthu K, SenGupta S, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study. Lancet Infect Dis. 2019;19(6):601–610. doi:10.1016/S1473-3099(18)30792-8
26. Zhu Y, Xiao T, Wang Y, et al. Socioeconomic burden of bloodstream infections caused by carbapenem-resistant Enterobacteriaceae. Infect Drug Resist. 2021;14:5385–5393. doi:10.2147/IDR.S341664
27. Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA. Carbapenems: past, present, and future. Antimicrob Agents Chemother. 2011;55(11):4943–4960. doi:10.1128/AAC.00296-11
28. Santimaleeworagun WTS, Juntanawiwat P, Thongnoy N, Harindhanavudhi S, Nakeesathit S, Teschumroon S. The prevalence of colistin-resistant Gram-negative bacteria isolated from hospitalized patients with bacteremia. J Appl Pharm Sci. 2020;10(2):056–59.
29. Yamamoto M, Pop-Vicas AE. Treatment for infections with carbapenem-resistant Enterobacteriaceae: what options do we still have? Crit Care. 2014;18(3):229. doi:10.1186/cc13949
30. Fernandes MR, Moura Q, Sartori L, et al. Silent dissemination of colistin-resistant Escherichia coli in South America could contribute to the global spread of the mcr-1 gene. Euro Surveill. 2016;21(17):8798. doi:10.2807/1560-7917.ES.2016.21.17.30214
31. Ovejero CM, Delgado-Blas JF, Calero-Caceres W, Muniesa M, Gonzalez-Zorn B. Spread of mcr-1-carrying Enterobacteriaceae in sewage water from Spain. J Antimicrob Chemother. 2017;72(4):1050–1053. doi:10.1093/jac/dkw533
32. Caselli E, D’Accolti M, Soffritti I, Piffanelli M, Mazzacane S. Spread of mcr-1-Driven colistin resistance on hospital surfaces, Italy. Emerg Infect Dis. 2018;24(9):1752–1753. doi:10.3201/eid2409.171386
33. Nguyen PTL, Tran HTM, Tran HA, et al. Carriage of plasmid-mediated colistin Resistance-1-Positive Escherichia coli in humans, animals, and environment on farms in Vietnam. Am J Trop Med Hyg. 2022;107(1):65–71. doi:10.4269/ajtmh.21-1203
34. Ngoc VTB, Le Viet T, Nguyen Thi Tuyet M, et al. Characterization of Genetic Elements Carrying mcr-1 Gene in Escherichia coli from the Community and Hospital Settings in Vietnam. Microbiol Spectr. 2022;10(1):e0135621. doi:10.1128/spectrum.01356-21
35. Ha VTT, Tran LD, Mai NTT, et al. Potential spread of mcr-9-carrying IncHI2 plasmids in Enterobacter hormaechei in Vietnam. J Glob Antimicrob Resist. 2021;27:332–334. doi:10.1016/j.jgar.2021.09.012
36. Jean SS, Harnod D, Hsueh PR. Global threat of carbapenem-resistant Gram-negative bacteria. Front Cell Infect Microbiol. 2022;12:823684. doi:10.3389/fcimb.2022.823684
37. Birmingham MC, Rayner CR, Meagher AK, Flavin SM, Batts DH, Schentag JJ. Linezolid for the treatment of multidrug-resistant, gram-positive infections: experience from a compassionate-use program. Clin Infect Dis. 2003;36(2):159–168. doi:10.1086/345744
38. Kohno S, Yamaguchi K, Aikawa N, et al. Linezolid versus vancomycin for the treatment of infections caused by methicillin-resistant Staphylococcus aureus in Japan. J Antimicrob Chemother. 2007;60(6):1361–1369. doi:10.1093/jac/dkm369
39. WHO. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. Secondary Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics; 2017. Available from: https://www.who.int/news/item/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed.
40. Feretzakis G, Loupelis E, Sakagianni A, et al. A 2-year single-centre audit on antibiotic resistance of Pseudomonas aeruginosa, Acinetobacter baumannii and Klebsiella pneumoniae Strains from an Intensive Care Unit and other wards in a General Public Hospital in Greece. Antibiotics. 2019;8(2):90. doi:10.3390/antibiotics8020062
41. Despotovic A, Milosevic B, Milosevic I, et al. Hospital-acquired infections in the adult intensive care unit-Epidemiology, antimicrobial resistance patterns, and risk factors for acquisition and mortality. Am J Infect Control. 2020;48(10):1211–1215. doi:10.1016/j.ajic.2020.01.009
42. El Mekes A, Zahlane K, Ait Said L, Tadlaoui Ouafi A, Barakate M. The clinical and epidemiological risk factors of infections due to multi-drug resistant bacteria in an adult intensive care unit of University Hospital Center in Marrakesh-Morocco. J Infect Public Health. 2020;13(4):637–643. doi:10.1016/j.jiph.2019.08.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bacterial Etiology and Antimicrobial Resistance Pattern of Pediatric Bloodstream Infections in Beijing, 2015–2019
Lyu ZY, Zhen JH, Meng QY, Zhou W, An JY, Dong F
Infection and Drug Resistance 2023, 16:6297-6308
Published Date: 25 September 2023
Cross-sectional Hospital-based Investigation on Clinical Characteristics of Pediatric Staphylococcus aureus Isolates in a Beijing Hospital from 2013 to 2022
Wang L, Zhen JH, Dong F, Lyu ZY
Infection and Drug Resistance 2024, 17:4899-4912
Published Date: 6 November 2024
Antimicrobial Resistance and Genomic Characterization of Salmonella Serovars Typhimurium and 4,[5],12:i:- in Huzhou, China
Yan W, Ji L, Zha Y, Dong F, Xu D
Infection and Drug Resistance 2025, 18:2765-2777
Published Date: 31 May 2025
Epidemiology and Characteristics of Antibiotic Resistance of ESKAPE and E. coli Bloodstream Infections in Patients with Hematological Malignancies: High ESBL and Carbapenem Resistance in a 5-Year Single-Center Retrospective Study
Gao C, Gao G, Kong F, Hou P
Infection and Drug Resistance 2026, 19:610301
Published Date: 9 July 2026