Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Disinfection of dental impressions: knowledge and practice among dental technicians
Authors Al Mortadi N, Al-Khatib A ![]() , Alzoubi KH
, Alzoubi KH ![]() , Khabour OF
, Khabour OF ![]()
Received 13 February 2019
Accepted for publication 8 March 2019
Published 7 May 2019 Volume 2019:11 Pages 103—108
DOI https://doi.org/10.2147/CCIDE.S205144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Noor Al Mortadi,1 Aceil Al-Khatib,2 Karem H Alzoubi,3 Omar F Khabour4
1Department of Applied Dental Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Oral Medicine and Oral Surgery, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 4Department of Medical laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan
Background: Dental impressions are a common source for transmission of infection between dental clinics and dental labs. Dental impressions can be cross-contaminated by patient’s saliva and blood, which then cross-infect the dental casts poured from the impressions.
Objective: To evaluate the current practices of disinfection of dental impressions and their protocols and to assess the knowledge of cross-infection control among dental technicians in Jordan.
Method: Dental technicians (n=85) completed a self-administered questionnaire about their practices of disinfection for dental impressions.
Results: The distribution of dental technicians was 63.8% fixed prosthodontics, 23.5% removable prosthodontics, 7.8% orthodontics, and 4.8% maxillofacial prosthodontics. The majority of the laboratories did not have instructions related to disinfection of impressions. About 50% of technicians were vaccinated against HBV. About 44.7%, and 42.9% of labs reported that they never disinfect alginate or silicon impressions, respectively. In addition, the majority of lab owners (53%) believed that the dentist should disinfect the impressions before shipping them to dental laboratories, while (45%) believed that disinfecting the impressions is the responsibility of the dental assistant. Moreover, about 38% of this study population reported not using gloves in their labs. In those labs were disinfection was used, 51% used spray disinfection whereas 32.6% used immersion disinfection. The cost of disinfectant was ranked as the most important factor (51.3% of the cases) for the dental technician to choose the disinfectant followed by its effectiveness.
Conclusion: Dental technician practices in impression disinfection was not satisfactory, therefore, education programs about impression disinfection are needed.
Keywords: disinfection, dental impressions, knowledge, practice, dental technicians
Introduction
Disinfection of dental impressions is an essential routine that aims to protect dental personnel, who handle impressions or casts, against exposure to diseases brought about by contact with microorganisms such as viruses; hepatitis B, hepatitis C, herpes, and HIV, and Mycobacterium tuberculosis (Hemalatha & Ganapathy, 2016). Impression materials that have been exposed to infected saliva and blood provide asignificant source of such infectious agents.1 The British Dental Association in the Health Technical Memorandum 01–05 recommends disinfection and decontamination of dental impressions before dispatching them to the dental laboratories, and states that the responsibility for ensuring dental impressions are both disinfected and labelled as such before being sent to dental laboratory lies solely with the dentist who should inform the dental lab technicians about the status of impression disinfection.2 Such recommendations do not exist in Jordan. In addition, there are no explicit guidelines by the Jordanian Dental Association (JDA) on impressions disinfection. Most dentists rely on their undergraduate basic educational experience regarding the topic of infection control to minimize the potential for cross infection.
In 2017, the Jordanian Dental Association (JDA) made continuing education a mandatory requirement for all registered dentists. Rules of continuing medical education provide that dentists comply with completing continuing education courses every five years in order to meet their licensure renewal requirements. These courses are likely to update dentists’ knowledge and improve the standards of infection control for the benefit of the dental team.
Dental impressions contaminated with patient’s saliva and blood may cross infect the dental casts poured from them. Contaminated impressions and casts 3 thus become tools for the transmission of both bacteria and viruses between clinics and dental laboratories.4 In addition, casts poured from impressions can carry microorganisms and these may perhaps spread to other parts of the dental laboratory during trimming of the casts or dies.5
It is arecommended practice for dentists to send alabel indicating the status of impressions as “disinfected impressions” to the dental laboratory in order to protect the dimensional stability and the surface detail reproduction of the impressions. This practice can eliminate possible uncertainty facing dental technicians when they receive the impressions and prevent repetitive disinfection.6,7 It is known that avariety of chemical agents can be used efficiently for impression disinfection8 provided that each type is applied to the impression according to the manufacturer’s instructions. However, it has been reported that rinsing the impression with water solely does not remove contamination,9 therefore disinfecting of the impression and further rinsing the disinfectant off is required. As chemical disinfection is asurface phenomenon, it is important that prior to immersion in the disinfectant, the impressions surface is washed to remove obvious debris so that contact with the disinfectant solution is maximized.
Al-Dwairi10 investigated the awareness and practices of disinfection in Jordan in 2007 and reported that there was lack of compliance with infection control procedures of dental technicians working in commercial laboratories. In the UK, a study assessed the awareness of disinfection routine practices applied to dental impressions among both dentists and dental technicians to assess the practices, knowledge and trust between these two members of the dental team11 with regard to impression disinfection. Acommon recommendation was that professional communication and cooperation between the dental laboratories and dentists is essential to ensure that appropriate cleaning and disinfection protocols are followed for impressions.12 Distrust between dental technicians and dentists could result in repeating disinfection procedures of impressions by dental technicians even after being disinfected by dentists risking dimensional changes and alterations to the accuracy of the impression material.6 This study aimed to examine the knowledge and practice of routine disinfection for impressions among Jordanian dental technicians and the level of communication that currently exists between dentists and dental technicians.
Method
Aquestionnaire and covering letter was developed and distributed nationally to the owners of dental laboratories in Jordan (n=100). Prior to completing the questionnaire, it was piloted over asample (n=7) of the target group to ensure the clarity of the questions. Approval of the Institutional Review Board (IRB) at Jordan University of Science and Technology (1/103/2017) was sought and obtained. This was conditional upon anamed and signed consent form being completed and returned in advance of completing the questionnaire. The finalized questionnaire was randomly distributed nationally through the Jordanian Association Dental Lab Sciences Owners to sixty owners of dental technician’s laboratories during the period from February May2017-August 2017. Additionally, forty more owners were selected from the closing reception event organized by the Jordanian Association for Dental Owners on April26, 2017. Questionnaire distribution was carried out personally by the first author. To ensure confidentiality, the questionnaire and the covering letter sheets were separated.
The questionnaire consisted of anumber of closed-ended questions, one open-ended question, and two choices “yes or no”. The questionnaire was divided into four sections. Section one: consisted of demographic information such as qualification, gender, and experience of the owners of dental laboratories. Section two: included questions about disinfection practices among dental technicians upon receiving impressions. Section three included questions on the condition of received impressions; labelled as disinfected or not disinfected. Section four included questions on infection control measures; policy, and employee’s vaccinations.
Data was statistically analyzed using the software package IBM SPSS version 25 (IBM, NY, USA). Chi Square test was used to assess associations among questionnaire items. P<0.05 was considered significant.
Result
Eighty-five questionnaires were returned completed by the consenting 100 directors of dental technician laboratories with some missing answers. The response rate was therefore 85%. Table 1 shows the characteristics of dental laboratories. The number of male directors was eighty-three (97.6%). The distribution of dental technicians was 63.8% fixed prosthodontics, 23.5% removable prosthodontics, 7.8% orthodontics, and 4.8% maxillofacial prosthodontics. About half of the directors and dental technicians were reportedly vaccinated against HBV. The majority (80.5%) of the laboratories did not have instructions related to disinfection of impressions (Table 1).
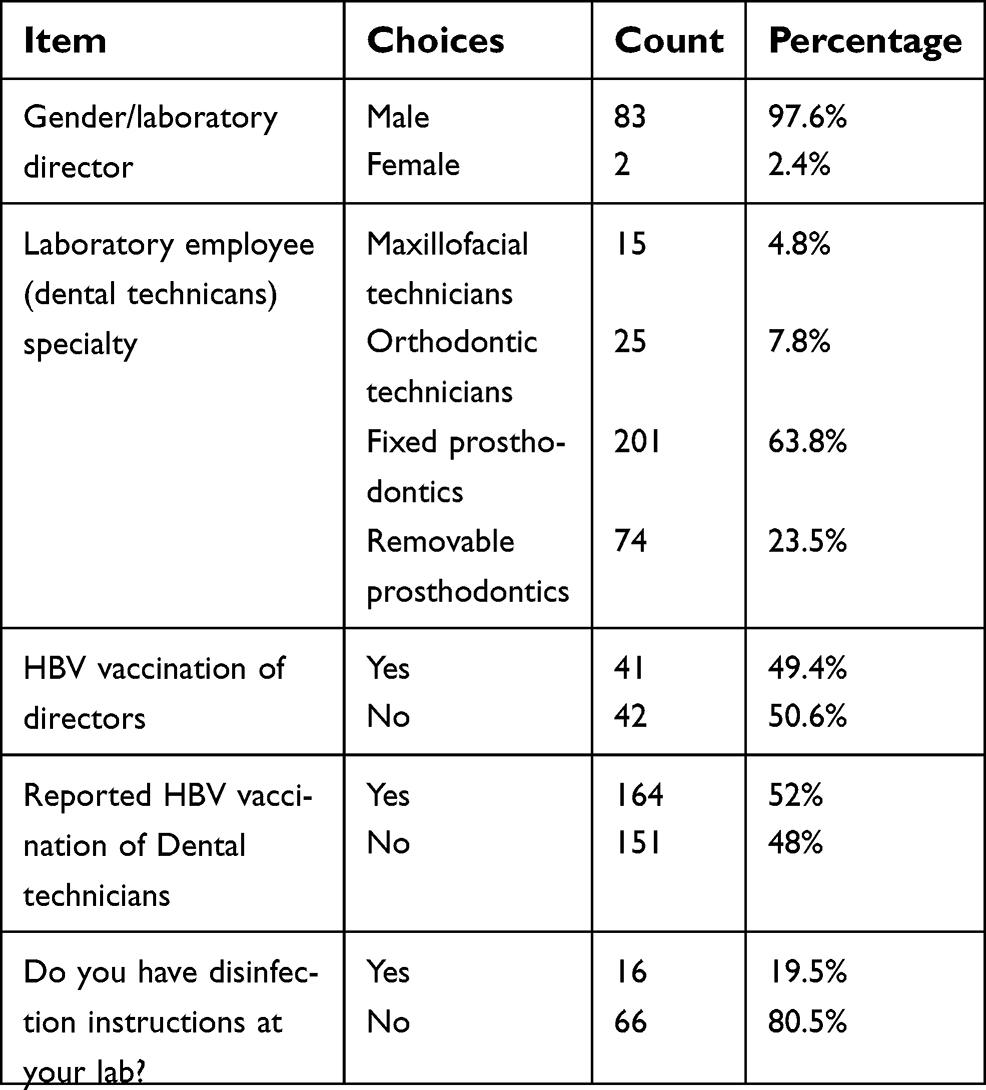 | Table 1 Characteristics of dental laboratories in Jordan |
The different practices of dental technicians upon receiving the impressions are summarized in Table 2. Upon receipt of an alginate and silicon impressions, the majority (84–89%) reported always rinsing them with water. Different practices for the disinfection of alginate and silicone impressions were apparent. About two-fifths of the labs reported never disinfecting alginate and silicon impressions and about aquarter reported that they sometimes disinfected impressions (Table 2). In the labs were disinfection was applied, 51% used spray disinfection (with or without water) whereas 32.6% used immersion disinfection (with or without water). About 38% reported not using gloves in their labs (Table 2).
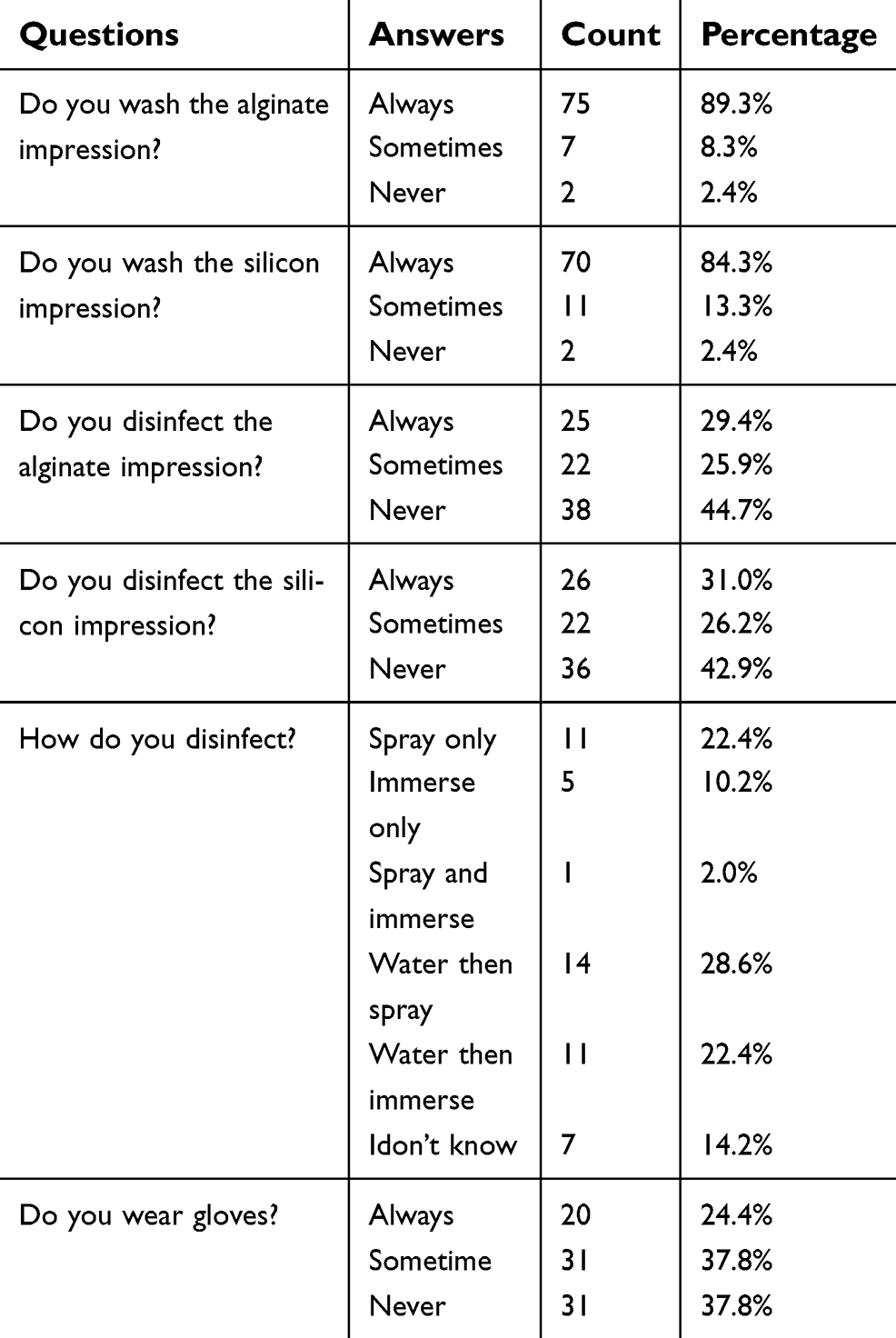 | Table 2 The practices of dental technicians upon receiving the impressions |
Table 3 shows the disinfection status in which dental technicians received the impressions from the dentists. Although there is no recommendation on how dentists should send impressions to the lab. In this investigation, the majority 65.9%) reported that they received the impressions in special sealed bags and wrapped in wet tissue. Most dental technicians (71%) had no idea how the dentists had disinfected the impressions. In contrast, about 11% reported they received such alabel most of the times from the dentists. The majority of the labs believed that the dentist (53%) or the dental assistant (45%) should disinfect the impressions before shipping them to the labs (Table 3). Variations in the time frame of disinfection of impressions received from dentist were noticed. Most of the labs (97%) reported that they did not know the type of disinfection used by the dentists.
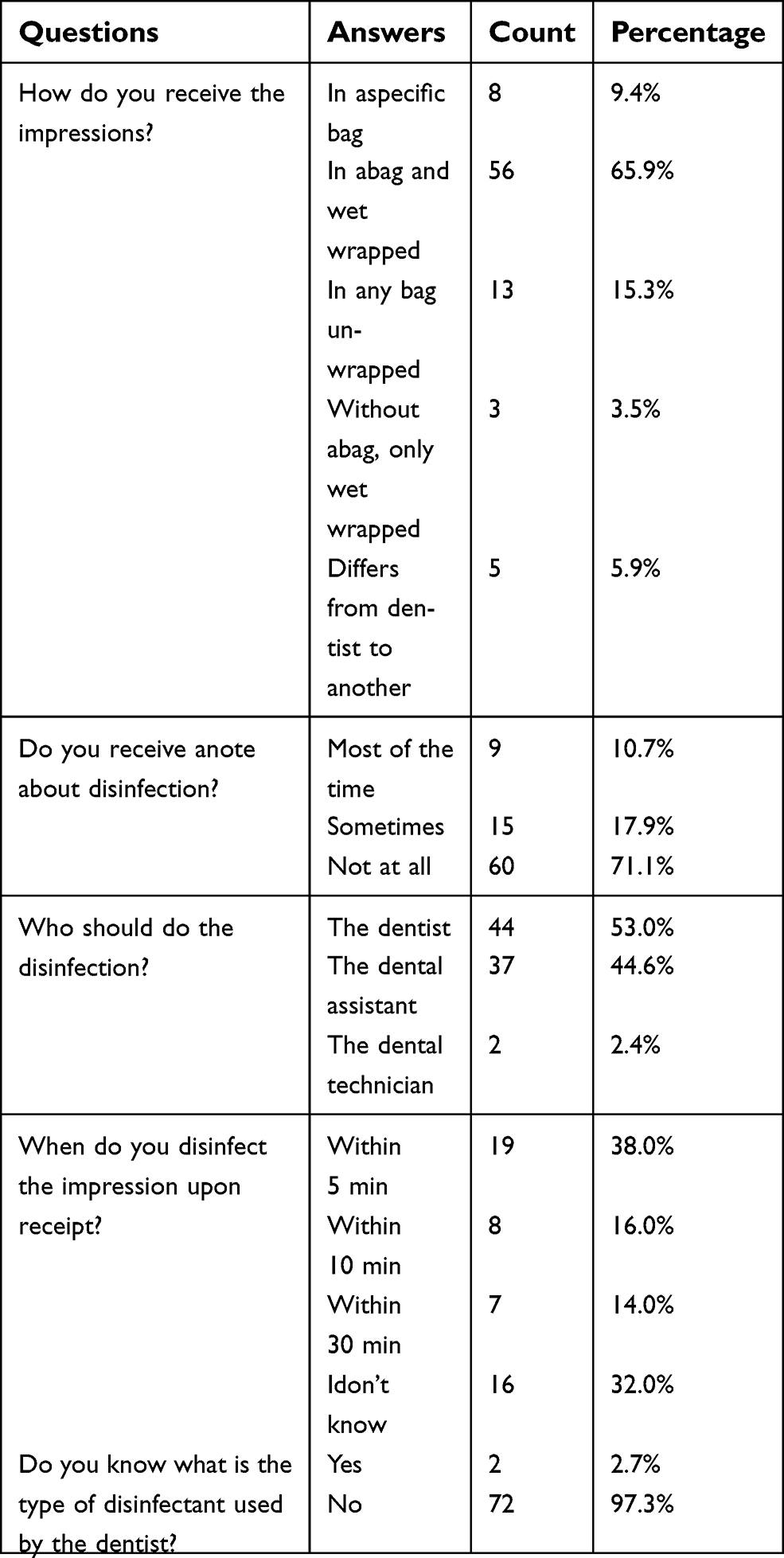 | Table 3 Conditions in which dental technicians received impressions from the dentist |
Table 4 shows that the cost and effectiveness were ranked respectively as the most andsecond most important factor for the dental technician to choose the disinfectant.
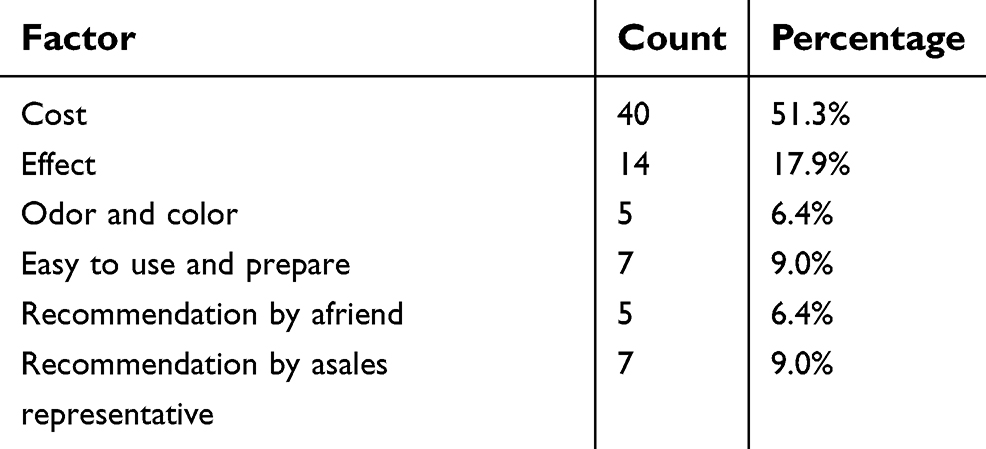 | Table 4 Factors that determine the type of disinfectant used in dental laboratories |
Discussion
Continuing Education Regulations for licensed dentists in Jordan, clearly states that every registered dentist should attend aworkshop on infection control once every five years. Dentists who fail to comply with this requirement may be subject to disciplinary action by JDA including non-renewal of their registration.
It is recommended that dentists attach labels to impressions sent to dental labs indicating the disinfection status of the impressions. Since repetitive disinfection of impressions poses risk of changes in dimensional stability and surface detail reproduction, communication between dentists and dental technicians in this regards is essential.2
This study shows that aconsiderable number of dental technicians always disinfect the alginate impressions (29.4%) and silicone (31%) upon receipt regardless of whether they have been disinfected by the dentists. This approach follows the recommendations by Lepe and co-workers12 who investigated the practices of workers in commercial dental laboratories in the UK. It is surprising that while some dental technicians reported washing the received impressions, others did not with some even thinking that washing the impression -with or without soap- is an acceptable disinfection practice. It is also clear that there was awide variation in the chemical disinfectant solutions used by the dental technicians in this study. For example, some of the chemicals used were recommended for dental uses but others were not. This indicates confusion among dental technicians regarding disinfection and suggests that education in this area is required. Selection of the correct type of disinfectant for impressions is also very important as inappropriately selected disinfectants can induce changes in both the accuracy and details of impression13
The findings of this study highlight an uncertainty among dental technicians concerning the responsible party for impression disinfection, and in relation to whether disinfection has taken place. Poor communication between dentists and technicians has been noted by other investigators previously.6,7 In the UK, asurvey reported that the majority (94.9%) of dentists always disinfected the impressions, 3.8% sometimes, and 1.3% never disinfected impressions.11
An obvious additional approach to protect the dental technician from infection is the use of protective equipment such as wearing gloves. There was poor compliance with this requirement, with 31 respondents (37.8%) stating that they had never used gloves. This finding, however, demonstrates aprogress in this area when compared to the findings of aprevious survey of dental technicians in Jordan,10 where only 12% of respondents reported wearing gloves when receiving dental impressions from various dental clinics. That study highlighted the absence of firm national rules by the Jordanian Association of Dental Owners regarding the management of impressions in dental laboratories and dental clinics.10 In contrast, astudy conducted in Saudi Arabia revealed that 60.87% of dental technicians knew that the impressions received from dental clinics were disinfected, and 56.25% of the dentists informed their laboratory technicians about the disinfection status. Therefore, dentists from the former study, followed the principles of impressions disinfection, and had abetter compliance with safety procedures than reported by Jordanian technicians. Moreover, most dental technicians (64.29%) stated that there is an agreed disinfection protocol between the laboratories and the dental clinics in Saudi Arabia.
Afurther area for improvement suggested by this study is in the selection and application of disinfectant. Some dental technicians did not recognize that washing/rinsing impression with water is not asterilization procedure. Although many dental lab directors mentioned commercial names of disinfectants bought out off the shelf for surface disinfection, these disinfectants were not suitable for use with impression materials, and in all cases, they could influence the accuracy of impressions. This study finding that asignificant percentage of directors and dental technicians have not been reportedly vaccinated, suggests that vaccination against HB virus should also be reinforced.
Conclusion
This study shows that practices and awareness of dental technicians regarding cross-infection control are less than ideal, and this might increase the risk of transmission of diseases. The findings of this study show that there is lack of communication between dentists and dental technicians, and that there is aneed for increasing awareness and establishing educational programs for both groups to decrease the risk of transmission of diseases in dental laboratories.
Acknowledgment
The authors would like to thank Prof. Graham Chadwick, Professor of Operative Dentistry and Dental Materials Science at Dundee School for his effort on this paper and Dr. Mutamed Ayyash for his assistance in statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Melilli D, Rallo A, Cassaro A, Pizzo G. The effect of immersion disinfection procedures on dimensional stability of two elastomeric impression materials. JOral Sci. 2008;50(4):441–446.
2.
3. Lewis DL, Arens M, Harllee R, Michaels GE. Risks of infection with blood- and saliva-borne pathogens from internally contaminated impressions and models. Trends Tech Contemp Dent Lab. 1995;12(5):30–34; discussion 29.
4. Garn RJ, Sellen PN. Health and safety in the laboratory. Dent Tech. 1992;45(1):103–120.
5. Leung RL, Schonfeld SE. Gypsum casts as apotential source of microbial cross-contamination. JProsthet Dent. 1983;49(2):210–211. doi:10.1016/0022-3913(83)90503-6
6. Kugel G, Perry RD, Ferrari M, Lalicata P. Disinfection and communication practices: asurvey of U.S.dental laboratories. JAm Dent Assoc. 2000;131:786–792. doi:10.14219/jada.archive.2000.0278
7. Sofou A, Lasren T, Fiehn N, et al. Contamination level of alginate impressions arriving at adental laboratory. Clin Oral Invest. 2002;6:161–165.
8. Blair FM, Wassell RW. Asurvey of the methods of disinfection of dental impressions used in dental hospitals in the United Kingdom. Br Dent J. 1996;180:369–375. doi:10.1038/sj.bdj.4809092
9. Demajo JK, Cassar V, Farrugia C, et al. Effectiveness of disinfectants on antimicrobial and physical properties of dental impression materials. IntJProsthodont. 2016;29(1):63–67. doi:10.11607/ijp.4358
10. Al Dwairi ZN. Infection control procedures in commercial dental laboratories in Jordan 2007. JDent Educ. 2007;71(9):1223–1227.
11. Almortadi A, Chadwick RG. Disinfection of dental impressions– compliance to accepted standards. Br Dent J. 2010;209:607–611. doi:10.1038/sj.bdj.2010.1134
12. Lepe X, Johnson GH, BergJC. Surface characteristics of polyether and addition silicone impression materials after long-term disinfection. JProsthet Dent. 1995;74(2):181–186. doi:10.1016/S0022-3913(05)80184-2
13. Hemalatha R, Ganapathy D. Disinfection of dental impression- Acurrent overview. JPharm Sci Res Cuddalore. 2016;8(7):661–664.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.