Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Discontinuing Antipsychotic Medication After Remission from First-Episode Psychosis: A Survey of Psychiatrists’ Attitudes in Taiwan
Authors Yen K ![]() , Liu CC
, Liu CC ![]() , Lin YT, Chien YL, Hsieh MH, Liu CM, Hwang TJ, Liao WH
, Lin YT, Chien YL, Hsieh MH, Liu CM, Hwang TJ, Liao WH ![]() , Hwu HG
, Hwu HG ![]()
Received 28 September 2021
Accepted for publication 26 December 2021
Published 1 March 2022 Volume 2022:18 Pages 465—475
DOI https://doi.org/10.2147/NDT.S339866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Ko Yen,1,* Chen-Chung Liu,1– 3,* Yi-Ting Lin,1,2 Yi-Ling Chien,1,2 Ming H Hsieh,1,2 Chih-Min Liu,1,2 Tzung-Jeng Hwang,1,2 Wei-Hsiang Liao,1,2 Hai-Gwo Hwu1,2
1Department of Psychiatry, National Taiwan University Hospital, Taipei, Taiwan; 2Department of Psychiatry, College of Medicine, National Taiwan University, Taipei, Taiwan; 3Department of Psychiatry, National Taiwan University Hospital Hsin-Chu Branch, Hsin-Chu, Taiwan
*These authors contributed equally to this work
Correspondence: Chen-Chung Liu Department of Psychiatry, National Taiwan University Hospital, No. 7 Chung Shan South Road, Taipei, 10002, Taiwan Tel +886-2-23123456 ext. 66130 Email [email protected]
Background: Patients in remission after first-episode psychosis are inclined to discontinue antipsychotic treatment, which may lead to higher risk of relapse and unfavorable outcomes. Paradoxically, also there are evidences suggesting that certain patients may stay well in drug-free condition. Psychiatrists’ views towards this dilemma might affect their approaches to these patients, and discrepant attitudes are noted between Western and Asian clinicians. This study aimed to examine psychiatrists’ attitudes about discontinuing antipsychotic medications after remission from first-episode psychosis.
Methods: Psychiatrists were recruited for this study using convenience sampling. A cross-sectional survey was conducted using a set of questionnaires comprising nine items for attitudes toward medication discontinuation, six vignettes for probing psychiatrists’ practice in designated clinical scenarios, and a list of criteria that may affect their responses.
Results: Responses were provided by 118 psychiatrists, two-thirds men, mean age 39.8 ± 10.1 years and mean experience 12.7 ± 9.7 years. Half of the participants endorsed that fewer than 20% of the remitted patients should stop medication completely; the majority advised that an observation period of 1 year or longer is necessary while discontinuing medication. The majority would not initiate discussion with patients about discontinuing medication. Responding to two case vignettes, those who endorsed that more patients could stop antipsychotics were also more inclined to discuss it with patients, but not consistently in response to the other four case vignettes. Taiwan psychiatrists expressed a wide range of decision-making considerations for discontinuing antipsychotics.
Conclusion: The majority of Taiwan psychiatrists thought it was not feasible to stop medications completely but were willing to consider this option. Once being presented with actual clinical scenarios, many participants hesitated to discontinue antipsychotic medications for various reasons. The proactive attitude of psychiatrists towards conducting clinical trials to test the feasibility of medication discontinuation may help to provide better reference for this clinical dilemma.
Keywords: antipsychotics, attitude, discontinuation, first-episode psychosis, remission, questionnaire
Introduction
Schizophrenia was once known as a severe, chronic disorder with devastating effects on the affected individual, family members and society. While more attention is paid to the early stage of the illness,1 early interventions in patients with first-episode psychosis (FEP) lead to better outcomes.2–5 Meta-analysis has shown that remission rates reach 50% and higher.6 Not surprisingly, after a relatively good initial treatment response, both patients and their key caregivers are inclined to discontinue medication when symptoms improve.7–9
However, discontinuation of antipsychotic treatment is the single most significant predictor of psychosis relapse, and tends to increase the risk of relapse by 5 times.10,11 Clinical trials evaluating dose reduction or discontinuation in patients remitted from FEP revealed 3 to 6 times higher risk of relapse in intermittent or placebo treatment groups compared to continuous treatment counterparts.12–16 Yet once relapse occurs, compared to the treatment for first-episode psychosis, it usually takes longer treatment duration to achieve remission, leaves more residual symptoms and has an increased proportion of patients classified as poor responders.11,17–19 Accordingly, continuous treatment remains the “gold standard” for good clinical practice for patients with schizophrenia.20 Consequently, previous clinical guidelines for treatment in the maintenance phase of schizophrenia have recommended that antipsychotics should be maintained for 1 to 2 years or even longer after a first psychotic episode,21 and an indefinite period of time has been strongly advocated once relapse occurs.22,23
Even so, recent guidelines and algorithms seemed to have shifted toward a more positive attitude regarding antipsychotic discontinuation and dose reduction or lower dose strategies, especially for patients who have only experienced a single psychotic episode.24 This may reflect concerns about the negative impact of exposure to long‐term use of antipsychotics. Patients have tended to discontinue treatment for disliking the adverse effects of antipsychotics on physical health and cognitive functioning, as well as the inconvenience or stigma-related issues.25 Also, evidence suggests a negative impact of antipsychotics on brain structure.26 Several neuroimaging studies have revealed a subtle but measurable loss on brain biology over time27–30 and a link to cognitive decline,31,32 even though not all evidence supports such a correlation.33 Currently, the risk-to-benefit ratio of long-term antipsychotic treatment is still debatable.
In real-world practice, several longitudinal observational studies have demonstrated that the proportions of patients remaining in a remitted state during follow‐up are higher than expected,34,35 and strikingly, not all of these patients were maintained by antipsychotic treatment.36,37 Also, in the long term, functioning may be even better in those who discontinued medication.38–41 Therefore, even though a recent comprehensive review endorsed a favorable risk-to-benefit ratio of continuous antipsychotic treatment, it could not be denied that
a minority of individuals diagnosed initially with schizophrenia appear to be relapse-free for long periods, despite absence of sustained antipsychotic treatment.42
Current evidence derived from different FEP cohorts fails to provide consistent and replicable variables that can predict the odds of having a sustained remission or relapse during medication discontinuation after a single episode of psychosis.43–45 A survey on the views of clinicians regarding discontinuation of antipsychotic medication following symptom remission in FEP revealed that positive attitudes of clinicians toward medication discontinuation is high and a vast majority of their respondents supported the idea to test the feasibility of discontinuing antipsychotic maintenance in patients remitted from FEP.46 The Asian Network for Early Psychosis (ANEP) has adopted Thompson’s questionnaires46 and added a second part with probes by case vignettes and a list of criteria to survey clinicians’ attitudes towards dose discontinuation in patients with remitted FEP. Reports from ANEP presented similarities and minor differences between mental health professionals in Hong Kong, Japan, Korea, and Singapore, with more discrepancies compared to the original findings of Thompson et al.47
In the present study, we sought to compare Taiwan psychiatrists’ attitudes towards medication discontinuation with previous findings, by replicating the survey using the questionnaire shared by ANEP, and also analyzing the relationship between psychiatrists’ opinions and potential translation into action in clinical practice as shown by their responses to case vignettes.
Methods
Questionnaire and Participants
This cross‐sectional survey used a structured questionnaire developed by Hui et al,47 which incorporated the original version introduced by Thompson et al.46 Dr. Hui authorized us to translate her group’s questionnaire (English and Cantonese) into mandarin Chinese with amendments deemed helpful to be applied in Taiwan (personal communication). The language of the case vignettes was carefully modified to adopt considerations of social and cultural nuance. The questionnaire comprises three parts, including 1) nine items for attitude towards medication discontinuation; 2) six vignettes for indicating whether the psychiatrist will initiate the discontinuation suggestion and what they will do when patients ask for discontinuation; and 3) a list of criteria that might affect their thoughts regarding medication discontinuation of the index vignette; as well as the respondent’s basic information.
Using convenience sampling, we invited psychiatrists from different hospitals or clinics in Taiwan to respond to the questionnaire. In hospital settings, we contacted a coordinating physician who was interested in this survey to help disseminate the questionnaires to his or her colleagues. We also collected surveys in a continuous medical education event that was designated for psychiatrists in private practice. The minimum years of experience required for completing this survey was at least 1 year of having actively treated patients with psychosis.
Ethical Considerations
All participants were informed about the purpose of the survey and their participation was totally voluntary. The respondents mailed back their questionnaires anonymously with an envelope provided by the research team. A gift card was provided to thank them for their participation. The study protocol was approved by the hospital’s Research Ethics Committee, which permitted to confirm participant’s consents by receiving their response to this questionnaire survey.
Statistical Analysis
For questions assessing respondents’ attitudes towards medication discontinuation (ie, the first part of the questionnaire), the significance of differences in categorical variables were analyzed by Chi-square tests. Responses to individual items of questionnaires were dichotomized as positive and negative attitudes, and the frequencies of responses to the case vignettes and criteria of medication discontinuation were calculated and analyzed by multivariate logistic regression to determine whether significant differences were found in responses between psychiatrists with different gender and years of experience. We hypothesized that men and psychiatrists with longer years of experience might exhibit less willingness towards antipsychotic discontinuation.
To test if participant’s response to the first question
what percentage of people do you think can stop antipsychotics completely following absence of psychotic symptoms after their first episode of a psychotic disorder?
correlated with their response to each case vignette, the significance of correlations was analyzed using Mann–Whitney U-tests.
Results
Demographic Characteristics
A total of 118 psychiatrists from more than 15 sites around Taiwan participated in this survey. In general, they provided complete responses with minimal missing data to the first 3 parts of the questionnaire; however, 6 participants (5.1%) did not provide their basic information. Among all included participants, 68.8% (n=77) were men and 31.3 (n=35) were women, with mean age 39.8±10.1 years (range, 26–72 years), and mean years of experience 12.7±9.7 years (range, 1–44 years).
Attitudes Towards Medication Discontinuation
The first, second, and third most common responses to individual questions (comprising 75.4% to 100% of all responses) are summarized in Table 1. Half of the respondents (50.8%) endorsed that only 0–20% of the patients remitted after first-episode psychosis could discontinue antipsychotic medications, followed by 34.7% who endorsed that 20%‐40% could stop medications, while only 1.7% of the psychiatrists said that 0% of the patients could discontinue. Opinions regarding the observation period before considering medication discontinuation were diverse, with 28.8%, 26.3% and 29.7% of the participants thinking that the period should be less than 1 year, just 1 year, and between 1 and 2 years, respectively; while 15.2% thought an even longer duration was needed. Once ready for discontinuation, only 27.1% thought it could be done within 6 months, 29.7% thought it feasible to be done within 6‐12 months, and the remaining said it should be longer than 1 year. More than one-third of all psychiatrists (37.3%) thought that 40–60% of their patients would discontinue medication on their own accord. More than 75% of the respondents felt that more than 60% of their patients would consider medication discontinuation if given such an opportunity.
 |
Table 1 The Most Common, Second- and Third- Most Common Responses to Medication Discontinuation Questions |
After medication discontinuation, 43.2% thought that follow-up was needed for 2 years, 44% felt 1 year or shorter would be enough, while 9.3% felt lifetime follow‐up was required. Psychiatrists had an equivocal attitude toward patients’ quality of life; while 28.8% were in favor of those who discontinued medications, 28% were in favor of patients in maintenance therapy, and those remaining expressed uncertainty (43.2%). A majority (61.9%) expressed willingness (from quite happy to extremely happy) to participate in a randomized controlled trial for medication discontinuation on patients with remitted first-episode psychosis, and 78.8% agreed that evidence derived from such a study would have a definite impact on their clinical practice when treating patients in remitted psychosis.
Overall, gender and years of experience had no statistically significant impact on participants’ responses to attitudes towards medication discontinuation.
Response to Case Vignettes
Psychiatrists’ responses to case vignettes were quite diverse (Table 2). The majority of psychiatrists (range, 56.0% to 82.8%) responded that they would not initiate a discussion with the patient about discontinuing medication in Cases 1–5. Case 6, which depicted an apparent brief psychotic disorder, was the only exception that was endorsed by 84.6% of the respondents to discuss stopping medication. If a patient inquired whether he or she could try dose discontinuation, lower rates of positive responses were offered, and the most frequent response to patients’ inquiries (range, 37.1% to 52.6% among Cases 1 to 5) was to “observe for a longer term.” No statistically significant differences were found between the impact of psychiatrists’ gender and years of experience on their responses to individual case vignettes.
 |
Table 2 The Percentage of Responses to Each Case Vignette |
Revealed by their response to questionnaire item 1
what percentage of people do you think can stop antipsychotics completely following absence of psychotic symptoms following their first episode of a psychotic disorder?
as well as response to Case 1 and Case 4, psychiatrists who endorsed a higher percentage of patients who are able to stop antipsychotics completely following remission from FEP were also significantly more inclined to initiate discussion about medication discontinuation with their remitted patients. However, such positive correlations were not significantly present in the other four vignettes (Table 3).
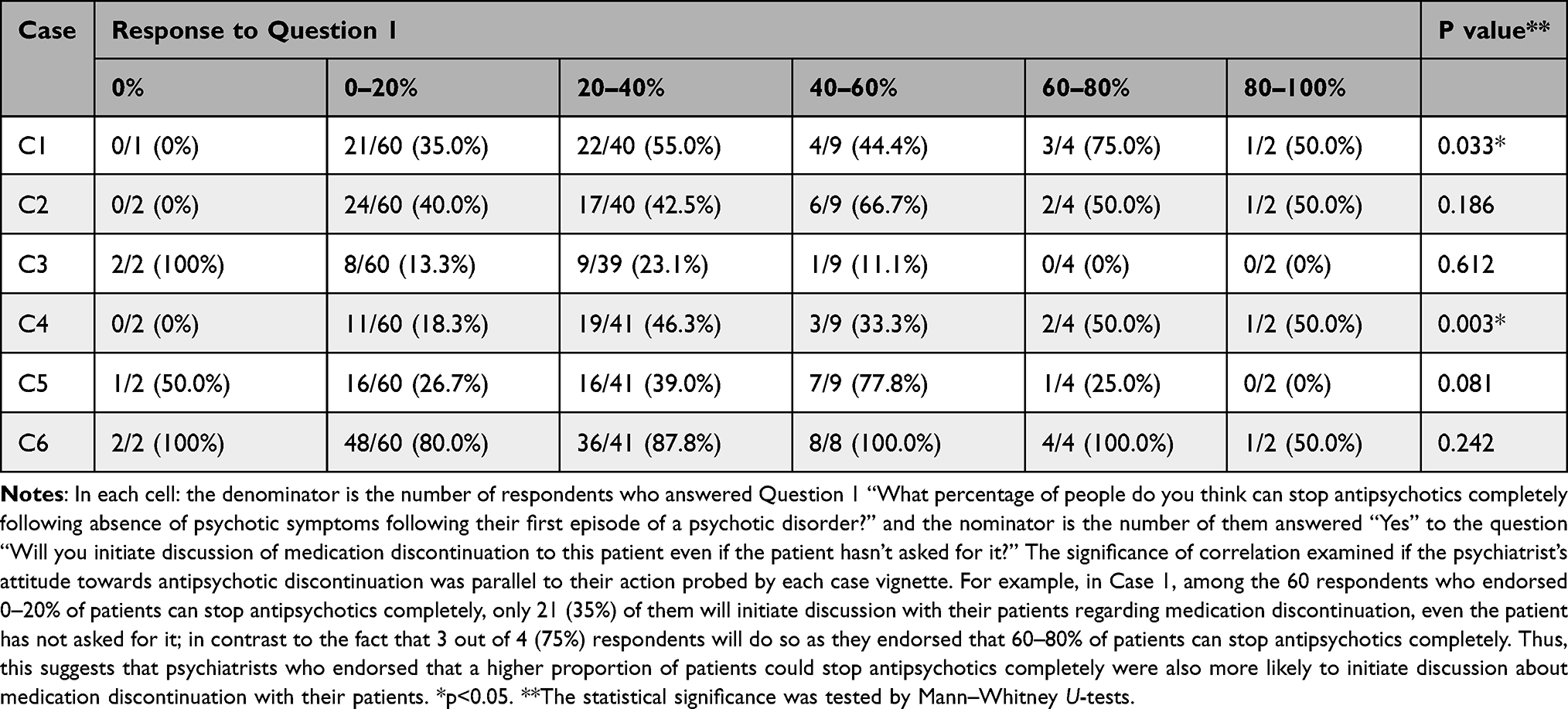 |
Table 3 Percentage of Psychiatrists Who Would Initiate Medication Discontinuation by Different Responses to Question 1 |
Criteria for Medication Discontinuation
The top five criteria for eligibility of dose discontinuation factors are no relapse since remitted from first-episode psychosis; positive view of illness; no positive symptoms; good social and family support; and willingness and readiness to taper off medication (Table 4). Psychiatrists with more years of experience had a greater tendency to think of satisfactory social functioning, absence of family history of psychotic disorder, ability to cope with stressful situations (also endorsed by more male psychiatrists), and having a sense of humor as criteria for medication discontinuation. Ranking of the frequencies of items is similar to that of the ANEP survey, though in general, psychiatrists in the present study selected higher percentages for each item (Table 5).
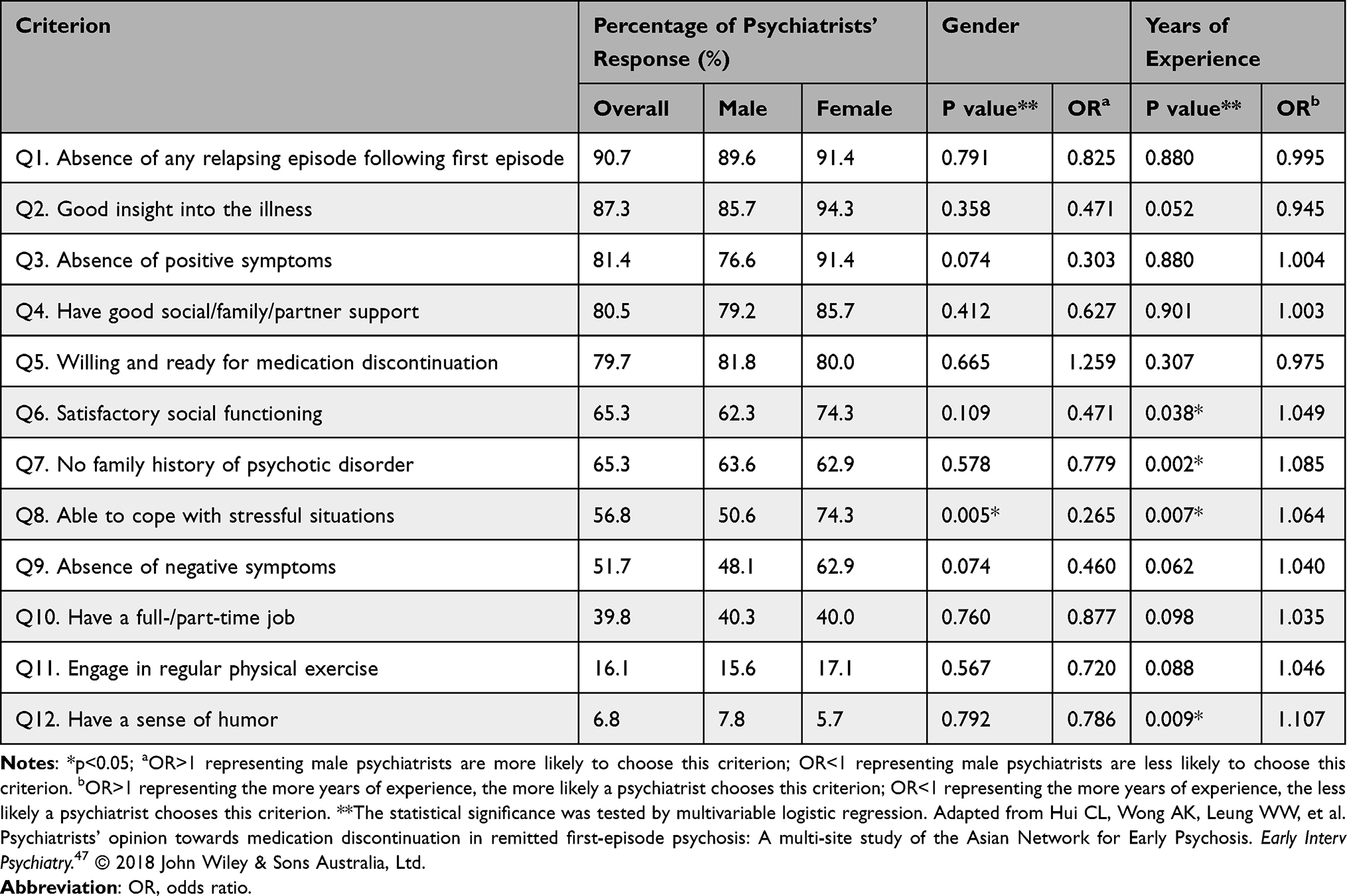 |
Table 4 Criteria for Medication Discontinuation |
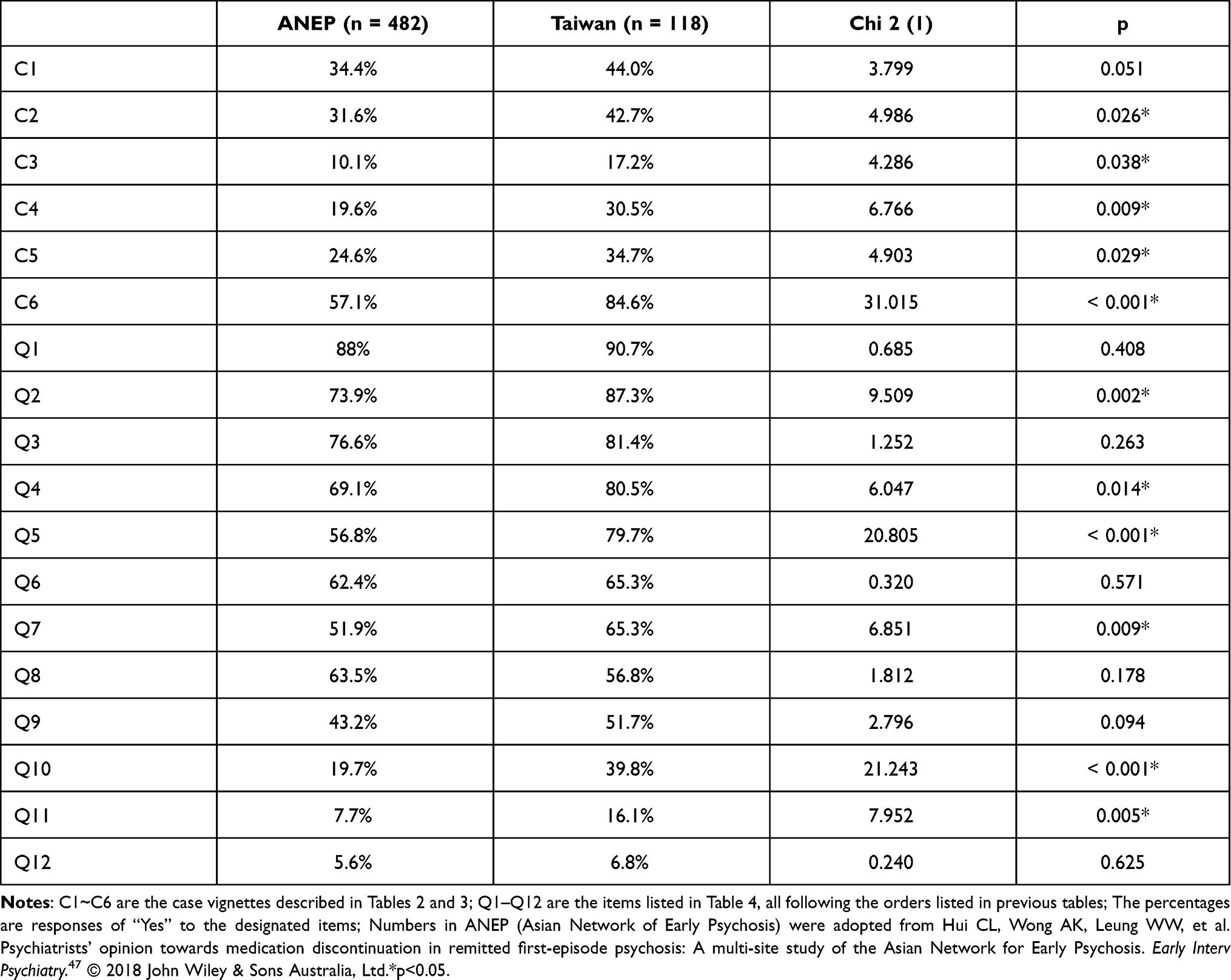 |
Table 5 Comparisons of Responses to Case Vignettes and Criteria for Medication Discontinuation Between Overall ANEP Countries and Taiwan |
Other criteria mentioned in psychiatrists’ free-text responses included a less severe diagnosis (non-schizophrenia), good therapeutic alliance, absence of history of drug or alcohol abuse, better cognitive function, pregnancy, shorter time to reach remission after first episode of psychosis, and whether discontinuation would significantly reduce side effects of the medication.
Discussion
The Chance and Pace of Medication Discontinuation
This survey has provided valuable messages from the psychiatrists’ perspective for several ongoing trials for antipsychotic dose reduction or discontinuation.48–52 Around half of the psychiatrists in this study thought that only 0–20% of the patients remitted from FEP should stop their medication, while more than half of Western psychiatrists thought that 20–40% was appropriate for stopping medication (Thompson et al).46 Such a conservative attitude regarding medication discontinuation following remission of FEP is similar to the ANEP results,47 and the attitudes of both Asian studies are closer to the guidelines that suggest maintenance therapy even after a single psychotic episode.21,22 Also, most Taiwan psychiatrists recommended stopping the medication gradually within a period of 6–12 months and even longer, and Western psychiatrists tended to do so within 3–6 months (median of Thompson et al’s survey). Indeed, a recent proposal derived from a pharmacodynamic study suggested reducing antipsychotic doses in a very slow, hyperbolic manner every 3 to 6 months,53 which implies that the seemingly slower pace of antipsychotic reduction endorsed by the psychiatrists in the present study may still be too fast to assure lower risk of relapse.
Cautious Yet Proactive Attitude of Taiwanese Psychiatrists
For most items probed by case vignettes, the ranking of positive responses to 6 cases by psychiatrists in the present study parallels the conservative approach shown in surveys conducted in the other 4 Asian countries, but generally with a higher proportion of positive responses to individual cases. Also, a greater proportion of Taiwan psychiatrists endorsed discontinuation of antipsychotic medications from 6 to 12 months after complete remission, compared to 1 to 2 years endorsed by psychiatrists in the other 4 Asian countries, as well as a larger proportion of Taiwan psychiatrists willing to support a randomized trial for medication discontinuation to provide evidence that may affect clinical practice. Such proactive attitudes are most likely related to their knowledge regarding the investigators’ ongoing project of antipsychotic dose reduction.49
The first four most frequently chosen criteria for medication discontinuation are the same between the present study and the ANEP survey, since previous relapse is obviously a strong predictor of subsequent relapse.54 Having poor insight into the illness was also a significant risk factor for relapse after first-episode psychosis,55 and a sound supportive system of family and friends can also be a protective factor.56 However, even though the majority of psychiatrists identified that the presence of positive symptoms was not good for medication discontinuation, other studies have suggested that the severity of negative symptoms is an even stronger predictor of further relapse.43 In the present study, among the six items endorsed by significantly more Taiwan respondents (Table 5), nearly 80% selected patient’s readiness and willingness to be an important criterion for medication discontinuation, a factor taken into account by Liu’s protocol.49
Complex Relationship Between Attitude and Clinical Practice
Psychiatrists’ estimated chance of and criteria for successful discontinuation appears to affect their decisions for treating patients probed by case vignettes. Case 6 met most of the frequently chosen criteria for medication discontinuation, and therefore it was the only vignette nominated by the majority of psychiatrists as eligible for discontinuing medications. However, in the other five cases, each failed to meet certain criteria deemed to be important, thus not as many psychiatrists endorsed the patients’ eligibility for discontinuation. Exemplified by Case 1 and Case 4, individual psychiatrists’ attitudes and clinical practice were quite consistent; that is, those who expressed proactive attitudes were more likely to endorse initiation of medication discontinuation (Table 3). However, such relationships were not found in the other three cases, implying that psychiatrists’ practice is not always concordant with their attitudes, leaving some undetermined factors to be further explored.
This survey study also highlighted some subtle differences in attitudes on the criteria of medication discontinuation by psychiatrists’ years of experience. Certain indicators that could only be obtained by greater understanding of patients and family, including satisfactory social functioning, absence of family history of psychotic disorders, ability to cope with stressful situations, and a sense of humor, were more likely to be selected for discontinuation by more experienced psychiatrists. This phenomenon implies that older psychiatrists are more likely to take more heuristics into consideration when making decisions about antipsychotic dose reduction or discontinuation.
Limitations
The present cross-sectional questionnaire survey has several limitations. First, regarding the representativeness of convenience sampling, we conjectured that our respondents may be more inclined to show proactive attitude as revealed by their greater interest in antipsychotic discontinuation trials; in that respect, representativeness may be less of an issue than with purposive sampling. Second, the original questionnaire did not include certain frequently mentioned predictors, such as substance use disorders, longer duration of untreated psychosis, and a diagnosis of schizophrenia spectrum disorder; also, in the free-text responses in the last part of the questionnaire, the respondents provided additional items to be considered in future surveys. Third, the psychiatrists’ responses to case vignettes represent just a proxy of actual clinical practice. A qualitative interview would be expected to give more insightful information to this issue.
Conclusion
The psychiatrists who participated in this questionnaire survey expressed a willingness to give patients remitted from FEP a chance to try dose reduction or discontinuation. However, once patients had been presented with actual clinical scenarios, many of them hesitated to suggest discontinuation of antipsychotic medications for various reasons. In addition to clinical features, respondents also considered many aspects of patients’ lives and readiness for dose reduction to discuss with their patients. Nonetheless, clinical trials comparing the outcomes of maintenance and medication discontinuation are anticipated to provide references for psychiatrists to fine-tune their clinical practice.
Acknowledgments
The authors would like to appreciate Dr CL Hui’s permission to use their questionnaire in this survey. The authors would also like to thank all psychiatrists who provided responses to this survey, especially the coordinating doctors and their superintendents at each site.
Author Contributions
All authors have made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; reviewed and agreed on all versions of the article; gave final approval of the version submitted to the current journal and agree to be accountable for all aspects of the work.
Funding
This survey was supported by a research grant from National Taiwan University Hospital, Taipei, Taiwan (NTUH-106-003486). The preparation of this manuscript was supported by and the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-002 −222 -MY3 & 110-2314-B002-121-MY3). The funders had no role in the study design, data collection, management, analysis, interpretation of data, writing of the report, and the decision to submit the report for publication.
Disclosure
All authors declare no conflicts of interest.
References
1. McGorry PD, Hickie IB, Yung AR, Pantelis C, Jackson HJ. Clinical staging of psychiatric disorders: a heuristic framework for choosing earlier, safer and more effective interventions. Aust N Z J Psychiatry. 2006;40(8):616–622. doi:10.1080/j.1440-1614.2006.01860.x
2. Malla AK, Norman RM, Manchanda R, et al. One year outcome in first episode psychosis: influence of DUP and other predictors. Schizophr Res. 2002;54(3):231–242. doi:10.1016/S0920-9964(01)00254-7
3. Menezes NM, Malla AM, Norman RM, Archie S, Roy P, Zipursky RB. A multi-site Canadian perspective: examining the functional outcome from first-episode psychosis. Acta Psychiatr Scand. 2009;120(2):138–146. doi:10.1111/j.1600-0447.2009.01346.x
4. Gaebel W, Riesbeck M, Wolwer W, et al. Rates and predictors of remission in first-episode schizophrenia within 1 year of antipsychotic maintenance treatment. Results of a randomized controlled trial within the German Research Network on Schizophrenia. Schizophr Res. 2013;152:478–486.
5. Boter H, Peuskens J, Libiger J, et al. Effectiveness of antipsychotics in first-episode schizophrenia and schizophreniform disorder on response and remission: an open randomized clinical trial (EUFEST). Schizophr Res. 2009;115(2–3):97–103. doi:10.1016/j.schres.2009.09.019
6. Lally J, Ajnakina O, Stubbs B, et al. Remission and recovery from first-episode psychosis in adults: systematic review and meta-analysis of long-term outcome studies. Br J Psychiatry. 2017;211(6):350–358. doi:10.1192/bjp.bp.117.201475
7. Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial. Lancet. 2008;371(9618):1085–1097. doi:10.1016/S0140-6736(08)60486-9
8. McEvoy JP, Lieberman JA, Perkins DO, et al. Efficacy and tolerability of olanzapine, quetiapine, and risperidone in the treatment of early psychosis: a randomized, double-blind 52-week comparison. Am J Psychiatry. 2007;164(7):1050–1060. doi:10.1176/ajp.2007.164.7.1050
9. Cooper D, Moisan J, Gregoire JP. Adherence to atypical antipsychotic treatment among newly treated patients: a population-based study in schizophrenia. J Clin Psychiatry. 2007;68(6):818–825. doi:10.4088/JCP.v68n0601
10. Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry. 1999;56(3):241–247. doi:10.1001/archpsyc.56.3.241
11. Winton-Brown TT, Elanjithara T, Power P, Coentre R, Blanco-Polaina P, McGuire P. Five-fold increased risk of relapse following breaks in antipsychotic treatment of first episode psychosis. Schizophr Res. 2017;179:50–56. doi:10.1016/j.schres.2016.09.029
12. Chen EY, Hui CL, Lam MM, et al. Maintenance treatment with quetiapine versus discontinuation after one year of treatment in patients with remitted first episode psychosis: randomised controlled trial. BMJ. 2010;341:c4024. doi:10.1136/bmj.c4024
13. Wunderink L, Nienhuis FJ, Sytema S, Slooff CJ, Knegtering R, Wiersma D. Guided discontinuation versus maintenance treatment in remitted first-episode psychosis: relapse rates and functional outcome. J Clin Psychiatry. 2007;68(5):654–661. doi:10.4088/JCP.v68n0502
14. Gaebel W, Riesbeck M, Wolwer W, et al. Relapse prevention in first-episode schizophrenia–maintenance vs intermittent drug treatment with prodrome-based early intervention: results of a randomized controlled trial within the German Research Network on Schizophrenia. J Clin Psychiatry. 2011;72(2):205–218. doi:10.4088/JCP.09m05459yel
15. Caseiro O, Perez-Iglesias R, Mata I, et al. Predicting relapse after a first episode of non-affective psychosis: a three-year follow-up study. J Psychiatr Res. 2012;46(8):1099–1105. doi:10.1016/j.jpsychires.2012.05.001
16. Emsley R, Oosthuizen PP, Koen L, Niehaus DJ, Martinez G. Symptom recurrence following intermittent treatment in first-episode schizophrenia successfully treated for 2 years: a 3-year open-label clinical study. J Clin Psychiatry. 2012;73(4):e541–547. doi:10.4088/JCP.11m07138
17. Emsley R, Nuamah I, Hough D, Gopal S. Treatment response after relapse in a placebo-controlled maintenance trial in schizophrenia. Schizophr Res. 2012;138(1):29–34. doi:10.1016/j.schres.2012.02.030
18. Takeuchi H, Siu C, Remington G, et al. Does relapse contribute to treatment resistance? Antipsychotic response in first- vs. second-episode schizophrenia. Neuropsychopharmacology. 2019;44(6):1036–1042. doi:10.1038/s41386-018-0278-3
19. Lieberman JA, Alvir JM, Koreen A, et al. Psychobiologic correlates of treatment response in schizophrenia. Neuropsychopharmacology. 1996;14(3 Suppl):13S–21S. doi:10.1016/0893-133X(95)00200-W
20. De Hert M, Sermon J, Geerts P, Vansteelandt K, Peuskens J, Detraux J. The use of continuous treatment versus placebo or intermittent treatment strategies in stabilized patients with schizophrenia: a systematic review and meta-analysis of randomized controlled trials with first- and second-generation antipsychotics. CNS Drugs. 2015;29(8):637–658. doi:10.1007/s40263-015-0269-4
21. Takeuchi H, Suzuki T, Uchida H, Watanabe K, Mimura M. Antipsychotic treatment for schizophrenia in the maintenance phase: a systematic review of the guidelines and algorithms. Schizophr Res. 2012;134(2–3):219–225. doi:10.1016/j.schres.2011.11.021
22. Kane JM, Garcia-Ribera C. Clinical guideline recommendations for antipsychotic long-acting injections. Br J Psychiatry. 2009;195(52):S63–67. doi:10.1192/bjp.195.52.s63
23. Secher RG, Hjorthoj CR, Austin SF, et al. Ten-year follow-up of the OPUS specialized early intervention trial for patients with a first episode of psychosis. Schizophr Bull. 2015;41(3):617–626. doi:10.1093/schbul/sbu155
24. Shimomura Y, Kikuchi Y, Suzuki T, Uchida H, Mimura M, Takeuchi H. Antipsychotic treatment in the maintenance phase of schizophrenia: an updated systematic review of the guidelines and algorithms. Schizophr Res. 2020;215:8–16. doi:10.1016/j.schres.2019.09.013
25. Perkins DO, Gu H, Weiden PJ, McEvoy JP, Hamer RM, Lieberman JA. Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder: a randomized, double-blind, flexible-dose, multicenter study. J Clin Psychiatry. 2008;69(1):106–113. doi:10.4088/JCP.v69n0114
26. Smieskova R, Fusar-Poli P, Allen P, et al. The effects of antipsychotics on the brain: what have we learnt from structural imaging of schizophrenia?–a systematic review. Curr Pharm Des. 2009;15(22):2535–2549. doi:10.2174/138161209788957456
27. Ho BC, Andreasen NC, Ziebell S, Pierson R, Magnotta V. Long-term antipsychotic treatment and brain volumes: a longitudinal study of first-episode schizophrenia. Arch Gen Psychiatry. 2011;68(2):128–137. doi:10.1001/archgenpsychiatry.2010.199
28. Fusar-Poli P, Smieskova R, Kempton MJ, Ho BC, Andreasen NC, Borgwardt S. Progressive brain changes in schizophrenia related to antipsychotic treatment? A meta-analysis of longitudinal MRI studies. Neurosci Biobehav Rev. 2013;37(8):1680–1691. doi:10.1016/j.neubiorev.2013.06.001
29. Haijma SV, Van Haren N, Cahn W, Koolschijn PC, Hulshoff Pol HE, Kahn RS. Brain volumes in schizophrenia: a meta-analysis in over 18 000 subjects. Schizophr Bull. 2013;39(5):1129–1138. doi:10.1093/schbul/sbs118
30. Vita A, De Peri L, Deste G, Barlati S, Sacchetti E. The effect of antipsychotic treatment on cortical gray matter changes in schizophrenia: does the class matter? A meta-analysis and meta-regression of longitudinal magnetic resonance imaging studies. Biol Psychiatry. 2015;78(6):403–412. doi:10.1016/j.biopsych.2015.02.008
31. Ho BC, Andreasen NC, Nopoulos P, Arndt S, Magnotta V, Flaum M. Progressive structural brain abnormalities and their relationship to clinical outcome: a longitudinal magnetic resonance imaging study early in schizophrenia. Arch Gen Psychiatry. 2003;60(6):585–594. doi:10.1001/archpsyc.60.6.585
32. Kubota M, van Haren NE, Haijma SV, et al. Association of IQ changes and progressive brain changes in patients with schizophrenia. JAMA Psychiatry. 2015;72(8):803–812. doi:10.1001/jamapsychiatry.2015.0712
33. Lesh TA, Tanase C, Geib BR, et al. A multimodal analysis of antipsychotic effects on brain structure and function in first-episode schizophrenia. JAMA Psychiatry. 2015;72(3):226–234. doi:10.1001/jamapsychiatry.2014.2178
34. Chang WC, Tang JY, Hui CL, et al. Prediction of remission and recovery in young people presenting with first-episode psychosis in Hong Kong: a 3-year follow-up study. Aust N Z J Psychiatry. 2012;46(2):100–108. doi:10.1177/0004867411428015
35. Ucok A, Serbest S, Kandemir PE. Remission after first-episode schizophrenia: results of a long-term follow-up. Psychiatry Res. 2011;189(1):33–37. doi:10.1016/j.psychres.2010.11.013
36. Chang WC, Chan TC, Chen ES, et al. The concurrent and predictive validity of symptomatic remission criteria in first-episode schizophrenia. Schizophr Res. 2013;143(1):107–115. doi:10.1016/j.schres.2012.10.016
37. Austin SF, Mors O, Secher RG, et al. Predictors of recovery in first episode psychosis: the OPUS cohort at 10 year follow-up. Schizophr Res. 2013;150(1):163–168. doi:10.1016/j.schres.2013.07.031
38. Morgan C, Lappin J, Heslin M, et al. Reappraising the long-term course and outcome of psychotic disorders: the AESOP-10 study. Psychol Med. 2014;44(13):2713–2726. doi:10.1017/S0033291714000282
39. Wunderink L, Nieboer RM, Wiersma D, Sytema S, Nienhuis FJ. Recovery in remitted first-episode psychosis at 7 years of follow-up of an early dose reduction/discontinuation or maintenance treatment strategy: long-term follow-up of a 2-year randomized clinical trial. JAMA Psychiatry. 2013;70(9):913–920. doi:10.1001/jamapsychiatry.2013.19
40. Harrow M, Jobe TH, Faull RN. Do all schizophrenia patients need antipsychotic treatment continuously throughout their lifetime? A 20-year longitudinal study. Psychol Med. 2012;42(10):2145–2155. doi:10.1017/S0033291712000220
41. Harrow M, Jobe TH, Faull RN, Yang J. A 20-Year multi-followup longitudinal study assessing whether antipsychotic medications contribute to work functioning in schizophrenia. Psychiatry Res. 2017;256:267–274. doi:10.1016/j.psychres.2017.06.069
42. Correll CU, Rubio JM, Kane JM. What is the risk-benefit ratio of long-term antipsychotic treatment in people with schizophrenia? World Psychiatry. 2018;17(2):149–160. doi:10.1002/wps.20516
43. Bowtell M, Ratheesh A, McGorry P, Killackey E, O’Donoghue B. Clinical and demographic predictors of continuing remission or relapse following discontinuation of antipsychotic medication after a first episode of psychosis. A systematic review. Schizophr Res. 2018;197:9–18. doi:10.1016/j.schres.2017.11.010
44. Alvarez-Jimenez M, Gleeson JF, Henry LP, et al. Prediction of a single psychotic episode: a 7.5-year, prospective study in first-episode psychosis. Schizophr Res. 2011;125(2–3):236–246. doi:10.1016/j.schres.2010.10.020
45. Alvarez-Jimenez M, Priede A, Hetrick SE, et al. Risk factors for relapse following treatment for first episode psychosis: a systematic review and meta-analysis of longitudinal studies. Schizophr Res. 2012;139(1–3):116–128. doi:10.1016/j.schres.2012.05.007
46. Thompson A, Singh S, Birchwood M. Views of early psychosis clinicians on discontinuation of antipsychotic medication following symptom remission in first episode psychosis. Early Interv Psychiatry. 2015;10(4):355–361. doi:10.1111/eip.12244
47. Hui CL, Wong AK, Leung WW, et al. Psychiatrists’ opinion towards medication discontinuation in remitted first-episode psychosis: a multi-site study of the Asian Network for Early Psychosis. Early Interv Psychiatry. 2019;13(6):1329–1337. doi:10.1111/eip.12765
48. Begemann MJH, Thompson IA, Veling W, et al. To continue or not to continue? Antipsychotic medication maintenance versus dose-reduction/discontinuation in first episode psychosis: HAMLETT, a pragmatic multicenter single-blind randomized controlled trial. Trials. 2020;21(1):147. doi:10.1186/s13063-019-3822-5
49. Liu CC, Hsieh MH, Chien YL, et al. Protocol of guided antipsychotic reduction to reach minimum effective dose (GARMED) in patients with remitted psychosis based on pragmatic design. Early Interv Psychiatry. 2021. doi:10.1111/eip.13144
50. Moncrieff J, Lewis G, Freemantle N, et al. Randomised controlled trial of gradual antipsychotic reduction and discontinuation in people with schizophrenia and related disorders: the RADAR trial (Research into Antipsychotic Discontinuation and Reduction). BMJ Open. 2019;9(11):e030912. doi:10.1136/bmjopen-2019-030912
51. Sturup AE, Jensen HD, Dolmer S, et al. TAILOR - tapered discontinuation versus maintenance therapy of antipsychotic medication in patients with newly diagnosed schizophrenia or persistent delusional disorder in remission of psychotic symptoms: study protocol for a randomized clinical trial. Trials. 2017;18(1):445. doi:10.1186/s13063-017-2172-4
52. Weller A, Gleeson J, Alvarez-Jimenez M, et al. Can antipsychotic dose reduction lead to better functional recovery in first-episode psychosis? A randomized controlled-trial of antipsychotic dose reduction. The reduce trial: study protocol. Early Interv Psychiatry. 2018;13:1345–1356. doi:10.1111/eip.12769
53. Horowitz MA, Murray RM, Taylor D. Tapering antipsychotic treatment. JAMA Psychiatry. 2020;78:125–126.
54. Ascher-Svanum H, Zhu B, Faries DE, et al. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry. 2010;10:2. doi:10.1186/1471-244X-10-2
55. Bergé D, Mané A, Salgado P, et al. Predictors of relapse and functioning in first-episode psychosis: a two-year follow-up study. Psychiatr Serv. 2016;67(2):227–233. doi:10.1176/appi.ps.201400316
56. Isohanni M, Miettunen J, Jaaskelainen E, Moilanen J, Hulkko A, Huhtaniska S. Under-utilized opportunities to optimize medication management in long-term treatment of schizophrenia. World Psychiatry. 2018;17(2):172–173. doi:10.1002/wps.20523
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.