Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Digitally Guided Workflow for the Esthetic and Prosthetic Oral Rehabilitation of a Patient with Excessive Gingival Display: A Case Report
Authors Alresheedi B ![]()
Received 19 July 2022
Accepted for publication 14 September 2022
Published 20 September 2022 Volume 2022:14 Pages 281—287
DOI https://doi.org/10.2147/CCIDE.S381639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Bandar Alresheedi
Department of Prosthetic Dental Sciences, College of Dentistry, Qassim University, Al-Mulaydah, Qassim, Kingdom of Saudi Arabia
Correspondence: Bandar Alresheedi, Department of Prosthetic Dental Sciences, College of Dentistry, Qassim University, P.O. Box: 6700, Al-Mulaydah, Qassim, 51452, Kingdom of Saudi Arabia, Tel +966563118990, Fax +966 0163801762, Email [email protected]
Abstract: This report describes the esthetic and prosthetic oral rehabilitation of a patient with excessive gingival display using a digital guided workflow. As per this digital workflow, the patient’s photographs, three-dimensional radiographic images, and a diagnostic digital intraoral scan were obtained. Preoperative digital case planning and designing were followed by the fabrication of surgical guides, printed casts, and matrices to accurately execute surgical esthetic crown lengthening and reproduce the digital design in the subsequent prosthetic rehabilitation.
Keywords: digital dentistry, excessive gingival display, pink esthetics, surgical guide, smile design
Introduction
A pleasing smile is composed of an esthetic, well-aligned, and proportioned dentition, in harmony with facial composition, lips, and gingiva.1 The appearance of gingival tissues plays an important role in smile esthetics; therefore, it is called pink esthetics.2 The amount of gingival tissue displayed at rest or during dynamic functional lip movements, such as speaking and smiling, and its shade, shape, and architecture, significantly influence dento-gingival esthetics.3,4 Furthermore, there is a close mutual relationship between periodontal conditions and prosthetic treatment.5,6 Healthy periodontal tissues are mandatory for the success of prosthodontic procedures and long-term success of prostheses. Similarly, good-quality prostheses with optimal placement of the margins in relation to the bone crest, respecting the supra-crestal tissue attachment, and proper marginal integrity, contours, and proximal contacts are essential for maintaining periodontal health.7
In clinical practice, excessive gingival display is a frequently encountered problem in patients undergoing esthetic and prosthetic oral rehabilitation. Excessive gingival display (>3 mm) negatively influences the appearance of the smile and is generally considered unattractive by most patients and dental practitioners.8 This condition could be caused by the following potential etiological factors (either individually or combined): short lip, hypermobile/hyperactive lip, short clinical crowns, dentoalveolar extrusion, altered passive eruption, vertical maxillary excess, and gingival hyperplasia.9
The treatment of excessive gingival display varies according to its severity and potential causes.10 Management of these cases requires a multidisciplinary treatment approach in which prosthodontists have to communicate and work with periodontists or dental surgeons to achieve the best biological, esthetic, and mechanical treatment outcomes.11 The development of computer aided design/computer aided milling and three-dimensional (3D) radiographic imaging technologies has improved and facilitated workflows in dentistry for the treatment of such multidisciplinary cases. Currently, 3D virtual analysis, design, and treatment planning are possible using these technologies. This helps in clinical decision-making and improves treatment predictability through enhanced communication among multidisciplinary treatment team members. In addition, it improves the communication with the patient, which affects treatment acceptance.12
Digitally guided workflow has been used in dental implantology and has enhanced the success and predictability of prosthetically driven implant placement.13 Recently, this approach has been implemented in guided-surgical periodontal crown lengthening procedures to achieve the best esthetic and biological outcomes in patients suffering from excessive gingival display.14,15 Previous reports have described the use of this treatment approach in patients with sound natural anterior teeth. We hypothesized that this approach can be adopted in patients with excessive gingival display and may substantially improve treatment outcomes when subsequent esthetic restorations are planned. Therefore, this report describes the esthetic and prosthetic oral rehabilitation of a patient with excessive gingival display using a digitally guided workflow. The adopted workflow was as follows: digital case planning/design followed by fabrication of surgical guides and stents/matrices to accurately execute surgical esthetic crown lengthening and reproduce the digital design in the subsequent prosthetic rehabilitation. This resulted in better esthetics and biologically integrated treatment outcomes.
Clinical Report
This report was approved by the Dental Research Ethics Committee at Riyadh Al-Elm University, and the patient agreed and signed a consent form to publish her case details and accompanying clinical photographs. A 46-year-old woman with a noncontributory medical history presented to the Department of Prosthodontics with the chief complaint of unsatisfactory esthetics of the maxillary anterior teeth (ie, “short teeth”, defective restorations and excessive non-ideal gingival display at rest position/in an exaggerated smile) (Figure 1). The patient had high esthetic expectations. The patient reported nocturnal bruxism (parafunctional habits), and there was evidence of incisal wear and fractured composite facings in the mandibular anterior teeth. Occlusal analysis revealed Angle Class I, overjet of 1 mm, overbite of 3 mm, and mutually protected occlusion during mandibular movements (Figure 2). Clinical and radiographic examinations revealed multiple extractions, root canal treatments (RCTs), composite veneers, metal-ceramic crowns and fixed dental prostheses (FDPs). In the anterior region, the problems identified during intraoral examination were marginal gingival inflammation with a probing depth of 4 mm due to inadequate direct and indirect restorations of the anterior maxillary teeth. Smile analysis revealed short anterior maxillary teeth with a 90% width to length ratio (for central incisors) and a high lip line/gingival display of 2 mm at rest and 4 mm in an exaggerated smile, with improper gingival architecture and thick gingival/periodontal biotype (Figure 3).
 |
Figure 1 Pretreatment, exaggerated smile view. Note non-ideal gingival display. |
 |
Figure 2 Pretreatment, retracted intraoral frontal view. |
 |
Figure 3 2D proposed smile design. |
A combination of both digital and conventional workflows was followed to address the patient’s esthetic and functional problems. In the planning phase, a two-dimensional 2D digital smile analysis and design software program was used to examine extraoral and intraoral digital photographs acquired from the patient using a DSLR camera. Once the patient accepted the proposed 2D smile design, an intraoral scanner (Omnicam; Dentsply Sirona Inc.) was used to obtain an intraoral digital scan of both arches. Cone beam computed tomography (CBCT) images were also obtained for both arches. Digital smile design, stereolithographic casts, and CBCT images were used to plan the correct relationship between the proposed tooth/restoration margin, future free gingival margin position, and bone level after surgical resection. The digital workflow described by Passos et al16 was followed to 3D-design and fabricate a crown lengthening surgical guide (Figure 4A–C). Subsequently, this surgical guide allowed for accurate execution of surgical esthetic crown lengthening according to the 3D digital planned design (Figure 5). Furthermore, a stereolithographic prototype of smile wax-up of the upper and lower teeth was then 3D printed using a light-polymerizing 3D resin (Jamghe Pro Model Resin, Jamghe) (Figure 6). Silicone putty matrices Panasil® Putty; Kettenbach GmbH & Co. KG) were then fabricated on the printed casts and used as an external surface form to fabricate the interim/provisional restorations.
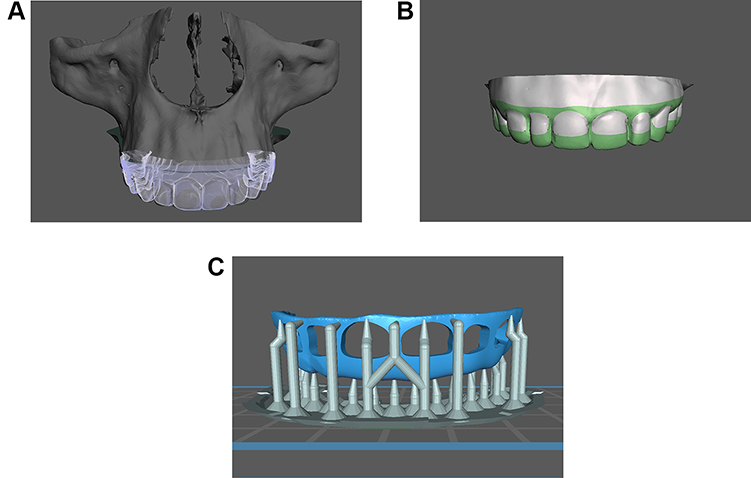 |
Figure 4 (A) Software view of superimposition of the virtual diagnostic cast, wax-up cast design, and CBCT image. CBCT, cone beam computed tomography. (B) Software view of the initial design of the surgical guide. (C) Software view of the definitive design of the surgical guide. |
 |
Figure 5 Surgical guide in place. |
 |
Figure 6 Standard tessellation language (STL) file of diagnostic wax-up. |
Surgical crown lengthening was performed using the fabricated surgical guide (Figure 7). Postsurgical instructions were provided to the patient after surgery. At the 1-week follow-up evaluation, the sutures were removed, the old restorations were removed, the teeth were properly prepared, and interim restoration was fabricated using previously fabricated silicone putty matrices using provisional Bis-Acryl resin (Pro-Temp 4; 3M ESPE). Recall visits were scheduled for 2, 4, and 12 weeks to evaluate esthetics, function, oral hygiene, and soft tissue healing; no unfavorable events or soft tissue recession were observed during this monitoring period, and the patient was satisfied with esthetics and function.
 |
Figure 7 Primary flap design after initial incision using the surgical guide. |
After the 3 months monitoring period, the patient was scheduled for a definitive restorative procedure. All anterior teeth received lithium disilicate pressable ceramic (IPS e.max Press; Ivoclar Vivadent AG) crowns, which were cemented using adhesive resin cement (Multilink N; Ivoclar Vivadent AG). Maxillary and mandibular posterior teeth received monolithic zirconia crowns which were cemented with resin-modified glass ionomer cement (Ketac™ Cem Plus Luting Cement; 3M ESPE) and screw retained crowns for implants.
At the end of the treatment, the smile that had been proposed and designed digitally was achieved, and the patient was satisfied. At the 1-week follow-up evaluation, the patient was happy and comfortable with her new prostheses, and a maxillary occlusal device (night guard) (Figure 8) was delivered at that time; the patient was instructed to wear it at night to protect the prostheses. The patient was scheduled for a 6-month follow-up program recall interval. After 1.5 years, she was still pleased and comfortable with her smile (Figure 9).
 |
Figure 8 Inserted definitive prostheses with occlusal appliance in place. |
 |
Figure 9 Smile after treatment. |
Discussion
This treatment approach permitted digital/virtual preoperative case planning, which helped the clinician to evaluate the treatment feasibility, the best treatment approach, and prosthetic restoration design to achieve the desired outcomes in terms of the patient’s treatment needs and expectations. Moreover, it allowed for proper communication between the prosthodontist, surgeon, patient, and dental laboratory. The collaborative virtual treatment plan was used to guide the treatment steps including periodontal surgery, tooth preparation, and the fabrication of both the provisional and final restorations.
Currently, digital smile design and strategies to reproduce the digitally designed prosthetic restoration in the patient’s mouth are popular procedures in dentistry and have been described in many previous reports.17,18 However, digitally guided esthetics periodontal surgery is still in the early stages of its development, and conclusive evidence is largely lacking. However, data from commonly performed guided implant-placement procedures, which also use software to merge files and design and print custom guides, indicate a very high accuracy of the guided surgery approach that allows implant placement with an average precision of ≤1 mm and ≤5° of deviation in inclination from the planned position.19 In the present case, the surgical guides allowed the precise placement of the surgical incision and an accurate flap design. They also helped the surgeon to control the amount and shape (scalloping) of the ostectomy considering critical esthetic and functional parameters and future restoration margins. Therefore, optimal postoperative location and architecture of the marginal gingiva and interdental gingival papillae could be achieved. This satisfied the esthetic treatment goals and also prevented morbidities due to violation of the biologic width (supra-crestal tissue attachments). These morbidities may vary according to patient’s gingival/periodontal biotype. In thick biotypes, the gingival inflammatory response results in swelling, edema, redness, and bleeding, whereas in thin biotypes, there is a higher risk for gingival recession and bone loss and a new biologic width is established at a more apical level.20,21 The surgeon did not have to estimate the placement of the final restorative margin. Direct visualization of future restoration margins through the custom surgical guide also reduced the operating time and invasiveness and preserved bone, which may have contributed to less severe postoperative complications and unfavorable events.
The digital guided-treatment approach has some limitations. Compared to the conventional approach digitally guided treatment has a higher cost; increased radiation exposure related to CBCT; an initial learning curve; and requires more time for preoperative case planning and preparation, the capability to operate the software, and equipment to fabricate casts, stents, and guides. Further studies are needed to verify the improvement in outcomes compared to the conventional approach.
Conclusion
This clinical report described the diagnosis and treatment sequence in a patient with excessive gingival display who required full-mouth rehabilitation. The use of a digital guided-treatment approach allowed precise execution of periodontal surgery according to the patient’s esthetic needs, which improved patient acceptance. Moreover, it reduced soft-tissue recession or rebound during the healing period and prevented the violation of the supracrestal tissue attachment during subsequent prosthetic treatment. Furthermore, this treatment approach improved the predictability by facilitating the reproduction of the digitally designed smile in the definitive restoration, which resulted in an esthetically and biologically integrated treatment outcome.
Acknowledgment
The researcher would like to thank the Deanship of Scientific Research, Qassim University for funding the publication of this project.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Horn S, Matuszewska N, Gkantidis N, Verna C, Kanavakis G. Smile dimensions affect self-perceived smile attractiveness. Sci Rep. 2021;11:2779. doi:10.1038/s41598-021-82478-9
2. Patil AS, Ranganath V, Yerawadekar SA, Kumar CN, Sarode GS. Pink esthetics: a study on significant gingival parameters. J Contemp Dent Pract. 2020;21:207–210. doi:10.5005/jp-journals-10024-2739
3. Fradeani M. Evaluation of dentolabial parameters as part of a comprehensive esthetic analysis. Eur J Esthet Dent. 2006;1:62–69.
4. Chen J, Chiang C, Zhang Y. Esthetic evaluation of natural teeth in anterior maxilla using the pink and white esthetic scores. Clin Implant Dent Relat Res. 2018;20:770–777. doi:10.1111/cid.12631
5. Bennani V, Ibrahim H, Al-Harthi L, Lyons KM. The periodontal restorative interface: esthetic considerations. Periodontol 2000. 2017;74:74–101. doi:10.1111/prd.12191
6. Srimaneepong V, Heboyan A, Zafar MS, et al. Fixed prosthetic restorations and periodontal health: a narrative review. J Funct Biomater. 2022;13(1):15. doi:10.3390/jfb13010015
7. Ercoli C, Tarnow D, Poggio CE, et al. The relationships between tooth-supported fixed dental prostheses and restorations and the periodontium. J Prosthodont. 2021;30:305–317. doi:10.1111/jopr.13292
8. Geevarghese A, Baskaradoss JK, Alsalem M, et al. Perception of general dentists and laypersons towards altered smile aesthetics. J Orthod Sci. 2019;8:14. doi:10.4103/jos.JOS_103_18
9. Dym H, Pierre R. Diagnosis and treatment approaches to a “gummy smile”. Dent Clin North Am. 2020;64:341–349. doi:10.1016/j.cden.2019.12.003
10. Bynum J. Treatment of a “gummy smile”: understanding etiology is key to success. Compend Contin Educ Dent. 2016;37:114–122.
11. Gibson MP, Tatakis DN. Treatment of gummy smile of multifactorial etiology: a case report. Clin Adv Periodontics. 2017;7:167–173. doi:10.1902/cap.2017.160074
12. Perakis N, Cocconi R. The decision-making process in interdisciplinary treatment: digital versus conventional approach. A case presentation. Int J Esthet Dent. 2019;14:212–224.
13. Bruno V, Badino M, Riccitiello F, Spagnuolo G, Amato M. Computer guided implantology accuracy and complications. Case Rep Dent. 2013;2013:701421. doi:10.1155/2013/701421
14. Deliberador TM, Weiss SG, Neto ATD, et al. Guided periodontal surgery: association of digital workflow and piezosurgery for the correction of a gummy smile. Case Rep Dent. 2020;2020:7923842. doi:10.1155/2020/7923842
15. Longo E, Frosecchi M, Marradi L, Signore A, de Angelis N. Guided periodontal surgery: a novel approach for the treatment of gummy smile. A case report. Int J Esthet Dent. 2019;14:384–392.
16. Passos L, Soares FP, Choi IGG, Cortes ARG. Full digital workflow for crown lengthening by using a single surgical guide. J Prosthet Dent. 2020;124:257–261. doi:10.1016/j.prosdent.2019.06.027
17. Revilla-León M, Besné-Torre A, Sánchez-Rubio JL, Fábrega JJ, Özcan M. Digital tools and 3D printing technologies integrated into the workflow of restorative treatment: a clinical report. J Prosthet Dent. 2019;121:3–8. doi:10.1016/j.prosdent.2018.02.020
18. Lin WS, Harris BT, Phasuk K, Llop DR, Morton D. Integrating a facial scan, virtual smile design, and 3D virtual patient for treatment with CAD-CAM ceramic veneers: a clinical report. J Prosthet Dent. 2018;119:200–205. doi:10.1016/j.prosdent.2017.03.007
19. Nickenig HJ, Eitner S, Rothamel D, Wichmann M, Zöller JE. Possibilities and limitations of implant placement by virtual planning data and surgical guide templates. Int J Comput Dent. 2012;15:9–21.
20. Carvalho BAS, Duarte CAB, Silva JF, et al. Clinical and radiographic evaluation of the Periodontium with biologic width invasion. BMC Oral Health. 2020;20:116. doi:10.1186/s12903-020-01101-x
21. Avetisyan A, Markaryan M, Rokaya D, et al. Characteristics of periodontal tissues in prosthetic treatment with fixed dental prostheses. Molecules. 2021;26:1331. doi:10.3390/molecules26051331
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.