Back to Journals » International Journal of General Medicine » Volume 16
Different Continuous Training Intensities Improve Echocardiographic Parameters, Quality of Life, and Functional Capacity in Heart Failure Patients with Reduced Ejection Fraction
Authors Abdeen HA, Helmy ZM, Elnaggar MI, Aldhahi MI, Taha MM ![]() , Marques-Sule E, Amin DI, Ibrahim BS, Abdel Aziz A, Castiglione V
, Marques-Sule E, Amin DI, Ibrahim BS, Abdel Aziz A, Castiglione V ![]() , Atef H
, Atef H
Received 25 May 2023
Accepted for publication 10 August 2023
Published 30 August 2023 Volume 2023:16 Pages 3933—3945
DOI https://doi.org/10.2147/IJGM.S420933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Heba A Abdeen,1 Zeinab M Helmy,1 Moustafa I Elnaggar,2 Monira I Aldhahi,3 Mona Mohamed Taha,3 Elena Marques-Sule,4 Doaa I Amin,5 Bassem S Ibrahim,6 Ahmed Abdel Aziz,6 Vincenzo Castiglione,7 Hady Atef1,8
1Department of Physical Therapy for Cardiovascular/Respiratory Disorder and Geriatrics, Faculty of Physical Therapy, Cairo University, Giza, 11432, Egypt; 2Faculty of Physical Therapy, Heliopolis University for Sustainable Development, Giza, Egypt; 3Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia; 4Physiotherapy in Motion, Multispeciality Research Group (PTinMOTION), Department of Physiotherapy, University of Valencia, Valencia, Spain; 5Basic Science Department, Faculty of Physical Therapy, Cairo University, Cairo, Egypt; 6Cardiology, National Heart Institute, Giza, Egypt; 7Fondazione Toscana Gabriele Monasterio; “Health Science” Interdisciplinary Research Center, Scuola Superiore Sant’Anna, Pisa, Italy; 8School of Allied Health Professions (SAHP), Keele University, Staffordshire, UK
Correspondence: Mona Mohamed Taha, Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, P.O. Box 84428, Riyadh, 11671, Saudi Arabia, Tel +966118240811, Email [email protected]
Background: Multiple comorbidities and physiological changes play a role in a range of heart failure conditions and influence the most effective approach to exercise-based rehabilitation. This research aimed to examine and compare the outcomes of continuous training at three different intensities, focusing on left ventricular (LV) remodeling, functional capacity, and quality of life among patients with heart failure with reduced ejection fraction (HFrEF).
Methods: In this randomized control trial, a total of 60 male patients (average age: 54.33 ± 2.35 years) with HFrEF were randomly allocated into three groups: 1) High-intensity continuous training group (HICT), 2) Moderate-intensity continuous training group (MICT), and 3) Low-intensity continuous training group (LICT). All the training was performed on a bicycle ergometer 3 times/week for 12 weeks. Echocardiographic parameters (left ventricular ejection fraction, left ventricular end-diastolic dimension, left ventricular end-systolic dimension, N-terminal pro–B-type natriuretic peptide (NT-proBNP), quality of life (Minnesota Living with Heart Failure Questionnaire), and functional capacity (6-minute walking test) were assessed before and the end of the study.
Results: The HICT group demonstrated the greatest improvements in all measured variables when compared to the other two groups (P < 0.05). These findings were consistent across all measured outcomes.
Conclusion: It was determined that HICT appears to yield the most favorable outcomes in enhancing echocardiographic measures, NT-proBNP levels, quality of life, and functional capacity among HFrEF patients.
Keywords: heart failure with reduced ejection fraction, aerobic exercises, ventricular remodeling, quality of life
Introduction
Heart failure (HF) is a global public health issue that affects over 26 million individuals.1 The prevalence of heart failure (HF) is steadily increasing worldwide and is expected to rise significantly due to the aging population.2 Despite significant advancements in treatment, HF continues to be a primary cause of hospitalizations, with a one-year mortality rate of approximately 45% among symptomatic patients.3 HF can be classified into three types: heart failure with reduced ejection fraction (HFrEF), with a mid-range reduced ejection fraction (HFmrEF), and with a preserved ejection fraction (HFpEF).1,4 HFrEF is linked to significant morbidity and poor quality of life.3 It is caused by a heart injury or any disease that affects the heart and results in reduced ventricular contractions. The left ventricular ejection fraction (LVEF) in healthy people ranges from 52% to 72% in men and 54% to 74% in women, and a value of 40% is enough to be classified as HFrEF.4
Through neurohormonal activation of the sympathetic nervous system and the renin-angiotensin-aldosterone pathway, cardiac remodeling is regarded as an initially beneficial compensatory mechanism for maintaining cardiac output. However, chronic stimulation of these mechanisms might be harmful, leading to pathological ventricular remodeling and deteriorating HF.5 Myocardial remodeling and its severity have been linked to poor patient outcomes, despite being difficult to forecast and monitor.6 Furthermore, if early ventricular remodeling can be detected and intervened in, it may present prospective therapeutic targets for mitigating disease progression.7
Identifying circulating biomarkers, specifically, natriuretic peptides, presents a viable noninvasive approach for assessing heart structure and function among individuals with heart failure with reduced ejection fraction (HFrEF). Such a strategy is highly advantageous in evaluating left ventricular (LV) remodeling.6 In HF, higher levels of brain natriuretic peptide (BNP) or N-Terminal pro-B-type natriuretic peptide (NT-proBNP) are associated with worse clinical outcomes and mortality. Further research revealed that every 100 pg/mL increase in BNP was linked to a 35% increase in mortality risk.8
Moreover, quality of life (QoL) has been established as an outcome and prognostic factor in heart failure. A significant survival outcome entails the presence of an optimal QoL for patients.9 For chronic HFrEF patients who are clinically stable, regular physical activity or exercise training is indicated to enhance the functional status, QoL, and mortality risk.10
In addition, aerobic workouts have been proven to be effective in patients with HFrEF in several studies.11 Aerobic exercise training is a well-recognized non-pharmacological tool for improving the pathophysiological, clinical, and prognostic manifestations of HF. Accurate prescribing of the appropriate exercise intensity is pivotal in achieving exercise-induced benefits while minimizing exercise-related risks. The characterization of exercise intensity domains and the lower and upper intensity limits of prescribed aerobic activity in HF patients is still unclear, and there are no cutoff data or definite exercise prescriptions (frequency, intensity, type, and time) in this era.4,9,12 Further studies are still needed to better understand the exact exercise required for heart failure cases, which can lead to significant physiological and patient-centered improvements. Therefore, the objective of this study was to compare the effects of high-intensity, moderate-intensity, and low-intensity continuous training on LV remodeling, NT-proBNP levels, and QoL in patients with HFrEF.
Materials and Methods
Study Design and Setting
This study was a double-blinded randomized controlled trial with three parallel arms. Participants were recruited from the National Heart Institute’s Heart Failure Outpatient Clinic from August 2020 through September 2021. All patients signed a written consent form before their enrollment. The Declaration of Helsinki’s principles and related ethical criteria were followed in this study. Ethical approval was obtained from the Institutional Ethical Review Board of the Faculty of Physical Therapy, Cairo University (P.T.REC/012/001906) and registered on clinicaltrials.gov (clinicaltrials.gov NCT05213546).
Study Participants
A total of 60 patients with HFrEF were enrolled. Only medically stable individuals with HFrEF (one year), fractional shortening ≤25% and ejection fraction ≤40%, sinus rhythm, HF due to ischemic heart disease, NYHA class II–III, and regular medical treatment were eligible for the trial. Patients meeting any of the following criteria were excluded from the study: chronic obstructive pulmonary disease, moderate-to-severe pulmonary hypertension, recent acute coronary syndrome, revascularization during the last three months, limited exercise abilities due to angina, peripheral arterial occlusive disease, cerebrovascular diseases, exercise-induced cardiac arrhythmias, uncontrolled hypertension.
Sample Size Calculation
The sample size was calculated using the G*power program 3.1.9 (G power program version 3.1, Heinrich-Heine-University, Düsseldorf, Germany). The estimated sample size calculation is based on F-tests (MANOVA: Special effects and interactions), Type I error (α) = 0.05, power (1-β error probability) = 0.90, Pillai V = 0.2700001, and effect size f2 (V) 0.1560694 with three independent groups comparison for six major variable outcomes. The appropriate minimum sample size for this study was 60 patients, 20 patients in each group as a minimum.
Randomization and Allocation Concealment
Patients were randomly allocated into three groups: 1) High-intensity continuous training (HICT, n = 20), 2) Moderate-intensity continuous training (MICT, n = 20) and 3) Low-intensity continuous training (LICT, n = 20). The process of randomization was done using an opaque sealed envelope method with a 1:1:1 allocation ratio. Participants and outcome assessors were both blinded to group allocation. Only the investigators were oriented with the patients’ grouping. The CONSORT flow diagram is represented in Figure 1.
 |
Figure 1 Consort diagram for the study. |
Outcomes
All patients had a comprehensive consultation with the multidisciplinary team (MDT) in which sociodemographic (age, sex) and clinical characteristics (body mass index, type of revascularization [percutaneous coronary intervention, coronary artery bypass grafting], hypertension, smoking, diabetes mellitus) were assessed. During the treatment sessions, they were asked to report any side effects. Throughout the trial, all patients were on their prescribed medical therapy with no major modifications to their treatment regimen.1 All of them were monitored medically by experienced cardiologists who were unaware of the grouping. The outcomes were as follows:
Primary Outcomes
Echocardiography Parameters
Left ventricular end-diastolic dimension (LVEDD), left ventricular end-systolic dimension (LVESD), ejection fraction percent (EF %), and fraction shortening (FS percent) were measured using pulsed Doppler echocardiography (Hewlett-Packard Sonos, USA). An ultrasound system was used to perform M-mode, two-dimensional, and pulsed Doppler echocardiography exams, as well as a two-dimensional mechanical sector scanner (2.5 MHZ imaging transducer connected to Hewlett- Packard Sons Doppler flow analyzer). According to the American Cardiac Society's update on the clinical application of echocardiography,13 each patient was assessed in a supine or left lateral position. A single operator performed all echocardiographic examinations for all patients in the three groups.
Secondary Outcomes
NT-proBNP
The chemical analysis was carried out in the medical biochemistry department of the National Heart Institute. Blood samples were taken before and after the study for the detection of NT-proBNP in the three groups. Blood was collected in a plastic lavender-top (EDTA) tube and put in a fluorescence immunoassay device (Cobas e 601 analyzer, Roche Diagnostics, Germany) to determine the concentration of the NT-proBNP.
Functional Capacity
The 6-minute walking test (6MWT) was used to evaluate the patient’s functional capacity, as it is well tolerated by patients and considered an alternative to cardiopulmonary exercise testing (CPET) for risk stratification in patients with HF.14 In this test, the patients were instructed to walk as far as they can on a flat, obstacle-free 15-m corridor and then turn 180° after they had reached the end of the corridor during the allocated time of 6 min. Patients walked unaccompanied and independently to prevent alterations to their gait velocity. At the end of the 6-min interval, the total distance walked by the patient was measured.15
Second, to establish maximum heart rate (HRmax), a symptom-limited CPET was utilized. A brief explanation of the procedures was instructed to the patients. Patients were asked to refrain from exercising for 24 hours before the test and not to eat a heavy meal, drink coffee, or smoke within two to three hours before the test. The test was carried out in a laboratory setting. Borg’s rate of perceived exertion (RPE) scale was presented to the patients. Next, the patients cycled at four submaximal rates for three minutes, each on a calibrated Electronic Bicycle Ergometer (Biodex LBC, Hewlett Packard, M2604A, New York, USA), with no breaks in between. For one minute, the patients pedaled at a work rate of 30 watts with no extra weight. The rate was then increased by 30 watts/3 min until the patients reached their symptom-limited HRmax. In the final 15 seconds of the third minute of each stage.16 The CPET ended with a cool-down stage in which the patient cycled against no resistance for a short period.17 To specify exercise intensity, Karvonen’s formula was used based on the results of the CPET:  18
18
Quality of Life
The Minnesota Living with Heart Failure Questionnaire (MLHFQ) is a questionnaire that assesses patients’ perceptions of the impact of HF on their quality of life (QoL). It is a 21-item questionnaire that considers physical, socioeconomic, and emotional limits. Each question has a scale of responses ranging from zero (none) to five (too many), with zero representing “no constraints” and five representing “maximum limitation.” The questionnaire yields an aggregate score (ranging from 0 to 105, with 0 representing optimal HFQoL and 105 the worst). The physical dimension score is calculated by adding the answers to eight questions about dyspnea and fatigue (2, 3, 4, 5, 6, 7, 12, and 13). Five questions make up the emotional dimension’s score (17, 18, 19, 20, and 21). The overall score was determined by the remaining questions (1, 8, 9, 10, 11, 14, 15, and 16) as well as the physical and emotional dimensions.19,20
Intervention
Participants were allocated into one of the three groups: 1) HICT (n = 20, 75–85% heart rate reserve: HRR, 2) MICT (n = 20, 65–75% HRR), and 3) LICT (n = 20, 55–65% HRR).21 All patients completed an individually supervised training program on an Electronic Bicycle Ergometer (Biodex LBC, Hewlett Packard, M2604A, New York, USA). An electrocardiogram (ECG) monitor and a telemetry system were utilized to monitor heart rate and rhythm.
Each session was divided in three phases: 1) Warm-up: it began with a 5 to 10-minute exercise consisting of active stretching and quiet walking; 2) Active phase: it lasted for 10 minutes which gradually increased to reach 35 minutes at the end of the study; 3) Cool down: it encompassed active recovery by pedaling slowly for 5–10 minutes with no resistance after finishing the session. Patients were closely monitored using ECG telemetry. Blood pressure was measured manually before, during, and after exercise training sessions. In addition, the Borg 6-to-20 scale was utilized to assess the rate of perceived exertion (RPE) during and after each training session.
Statistical Analysis
The statistical analysis was conducted using the SPSS Package program version 25 (SPSS, Inc., Chicago, IL). Quantitative data are expressed as mean and standard deviation for age, body mass index, duration of infarction, LVEDD, LVSED, EF, FS, NT-proBNP, MLHFQ, and 6MWT. Categorical data are expressed as frequency (percentage) for intervention, hypertension, smoking, and diabetes mellitus. Data were screened for normality assumption test and homogeneity of variance. Normality test of data used Shapiro–Wilk test, which reflected that the data were normally distributed (P > 0.05) after the removal of outliers that were detected by box and whiskers plots. Additionally, Levene’s test was used for testing the homogeneity of variance, and it revealed that there was no significant difference (P > 0.05). So, the data were normally distributed, and parametric analysis was performed. Chi-square test was used to compare HICT, MICT, and LICT groups. The one-way analysis of variance (ANOVA) test was used to compare age, body mass index, and duration of infarction between groups. Multivariate analysis of variance (MANOVA) was used to compare the tested major variables of interest in different tested groups and measuring periods. A mixed design 3 × 2 MANOVA test was used, and the first independent variable (between-subject factors) was the tested group with three levels (HICT, MICT, and LICT). The second independent variable (within-subject factor) was measuring periods with two levels (pre- and post-treatment). The Bonferroni correction test was used to compare between pairwise within and between groups of the tested variables whose P-value was significant from MANOVA test. All statistical analyses were significant at probability (P < 0.05).
Results
A total of 60 patients were included (mean age 53.51; mean BMI 27.51). For each group, baseline clinical characteristics are presented in Table 1. No significant differences (P < 0.05) in age (P = 0.893), weight (P = 0.108), height (P = 0.407), BMI (P = 0.237), duration of infarction (P = 0.691), NYHA (P = 1.000), intervention (P = 0.817), HTN (P = 0.28), smoking (P = 0.349), and DM (P = 0.189) among HIT, MIT, and LIT groups (Table 1).
 |
Table 1 Basic Characteristics of Participated Patients of HIT, MIT, and LIT Groups |
Multiple pairwise comparisons test (time effect) for outcome variables within each group revealed there were significant (P < 0.05) decrease in LVEDD and LVSED (Table 2) at post-treatment compared to pre-treatment within high-intensity group (P = 0.001 and 0.0001, respectively), moderate-intensity group (P = 0.024 and P = 0.008, respectively), and low-intensity group (P = 0.033 and P = 0.038, respectively). This significant decrease in LVEDD and LVSED at post-treatment is in favor of high-intensity group, followed by moderate-intensity group, and then low-intensity group. Moreover, high-intensity group (HIT group) significantly (P < 0.05) improved LVEDD and LVSED (10.03% and 12.92%, respectively) than moderate-intensity group (6.68% and 9.44%, respectively) and then low-intensity group (6.45% and 7.60%, respectively).
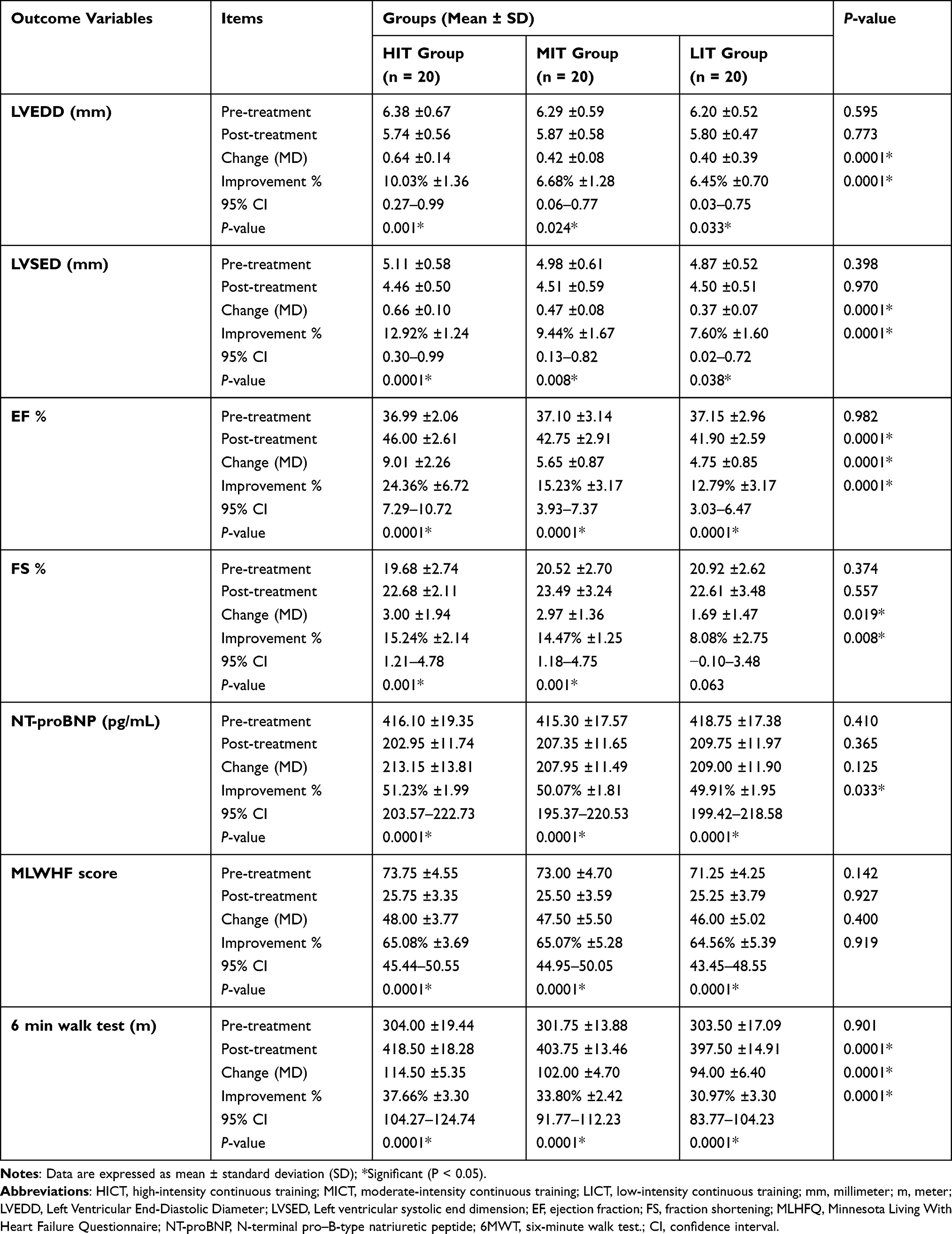 |
Table 2 Within- and Among-Group Comparisons for Outcomes Variables |
There were significant (P < 0.05) increase in EF and 6-min walk test (Table 2) at post-treatment compared to pre-treatment within high-intensity group (P = 0.0001 and P = 0.0001, respectively), moderate-intensity group (P = 0.0001 and P = 0.0001, respectively), and low-intensity group (P = 0.0001 and P = 0.0001, respectively). The FS (Table 2), also, significantly (P < 0.05) increased at post-treatment in high-intensity group (P = 0.001) and moderate-intensity group (P = 0.001), but with non-significant (P > 0.05) increase at post-treatment in low intensity (P = 0.063) compared to pre-treatment. This significant and non-significant increase in EF, 6-min walk test, and FS at post-treatment is in favor of high-intensity group, followed by moderate-intensity group, and then low-intensity group. Moreover, HIT group significantly (P < 0.05) improved higher EF, FS, and 6-min walk test (23.36%, 15.23%, and 37.66%, respectively) than moderate-intensity group (15.23%, 14.47%, and 33.80%, respectively) and then low-intensity group (12.79%, 8.08%, and 30.97%, respectively).
Both BNP and MLWHF (Table 2) significantly (P = 0.0001; P < 0.05) decreased at post-treatment compared to pre-treatment within high-intensity group, moderate-intensity group, and low-intensity group. This significant decrease in both BNP and MWHF at post-treatment is favorable for high-intensity group than for moderate- and low-intensity groups. Moreover, BNP significantly (P < 0.05) improved (51.23%) due to HIT compared with MIT group (50.07%) and then LIT group (49.91%, respectively). For MWHF, there is no significant difference (P > 0.05) in improvement percentage among HIT, MIT, and LIT groups (65.08%, 65.07%, and 64.56%, respectively).
Multiple pairwise comparisons test (group effect) for outcomes variables among high (HIT), moderate (MIT), and low (LIT) intensity groups (Table 2) showed no significant differences (P > 0.05) at pre-treatment in LVEDD (P = 0.595), LVSED (P = 0.398), EF (P = 0.982), FS (P = 0.374), BNP (P = 0.410), MLWHF (P = 0.142), and 6-min walk test (P = 0.901) among three groups. At post-treatment, the comparisons among HIT, MIT, and LIT revealed no significant differences in LVEDD (P = 0.773), LVSED (P = 0.970), FS (P = 0.557), BNP (P = 0.365), and MLWHF (P = 0.927), while there were significant differences (P < 0.05) in EF (P = 0.0001) and 6-min walk test (P = 0.000) due to group effect. There were significant differences (P < 0.05) among HIT, MIT, and LIT groups in absolute change for LVEDD (P = 0.0001), LVSED (P = 0.0001), EF (P = 0.0001), FS (P = 0.019), and 6-min walk test (P = 0.0001), but no significant difference (P > 0.05) in BNP (P = 0.125) and MLWHF (P = 0.400). For improvement percentage significantly (P < 0.05) affected among group for LVEDD (P = 0.0001), LVSED (P = 0.0001), EF (P = 0.0001), FS (P = 0.008), BNP (P = 0.033), and 6-min walk test (P = 0.0001), but no difference (P > 0.05) in MLWHF (P = 0.919) due to group effect.
Bonferroni test and mean difference for significant variable EF and 6-min walk test at post-treatment between pairwise of the groups (Table 3). There were significant differences (P < 0.05) in EF and 6-min walk test at post-treatment between HIT group versus MIT group (P = 0.001 and P = 0.015, respectively) and HIT group versus LIT group (P = 0.0001 and P = 0.0001, respectively), but no significant difference (P > 0.05) between MIT group vs LIT group (P = 0.985 and P = 0.687, respectively).
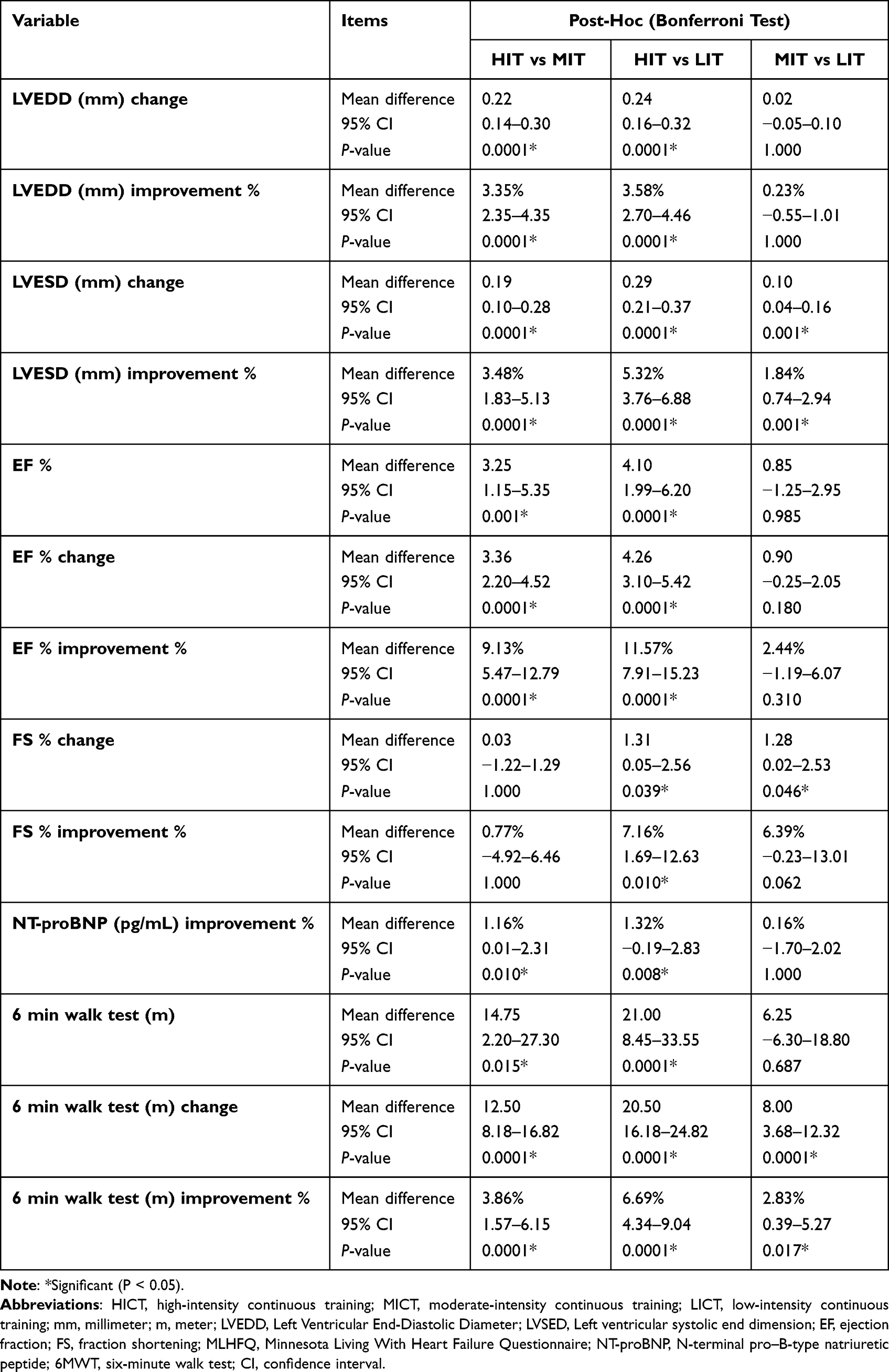 |
Table 3 Post-Hoc Test for Outcomes Variables Between Pairwise of Groups |
There were significant differences in absolute change of LVEDD and EF (Table 3) between HIT group versus MIT group (P = 0.0001 and P = 0.0001, respectively) and HIT group versus LIT group (P = 0.0001 and P = 0.0001, respectively), but no significant differences (P > 0.05) between MIT group vs LIT group (P = 1.000 and P = 0.180, respectively). Moreover, absolute change of LVESD and 6-min walk test significantly (P < 0.05) differ between HIT group versus MIT group (P = 0.0001 and P = 0.0001, respectively), HIT group versus LIT group (P = 0.0001 and P = 0.0001, respectively), and MIT group vs LIT group (P = 0.001 and P = 0.0001, respectively).
There were significant differences in improvement percentages of LVEDD, EF, and BNP (Table 3) between HIT group versus MIT group (P = 0.0001, P = 0.0001, and P = 0.010, respectively) and HIT group versus LIT group (P = 0.0001, P = 0.0001, and P = 0.008, respectively), but no significant difference (P > 0.05) between MIT group vs LIT group (P = 1.000, P = 0.310, and P = 1.000, respectively). Moreover, improvement percentages of LVESD and 6-min walk test significantly (P < 0.05) differ between HIT group versus MIT group (P = 0.001 and P = 0.0001), HIT group versus LIT group (P = 0.0001 and P = 0.0001), and MIT group vs LIT group (P = 0.001 and P = 0.017, respectively).
Bonferroni test and mean differences between groups (Table 3) showed that the high-intensity group (HIT group) gave the highest response LVEDD, LVSED, EF, FS, BNP, MLWHF, and 6-min walk test followed by moderate-intensity group, then low-intensity group.
Discussion
This RCT study compared the effects of high-intensity, moderate-intensity, and low-intensity continuous training on LV remodeling, NT-proBNP levels, and QoL in patients with HFrEF. Importantly, in a growing number of large-scale studies, reduced EF and elevated levels of proBNP are shown to be powerful predictors of risk for disease progression and all-cause mortality.5
Regarding echocardiographic outcomes, it was shown that both HICT and MICT showed significant differences in all echocardiographic parameters, with HICT showing superiority in all the outcomes over the rest of the groups. Although there was an improvement in LICT in EF, it did not show any significant effect on the other tested echocardiographic parameters. This is in line with the outcomes of previous studies showing that continuous training applied to HFrEF patients was associated with significant improvements in LVEF, end-diastolic volume, and end-systolic volume in exercise training groups, when compared with the control group of these studies. These central changes affect cardiac remodeling and consequently affect disease progression and mortality.22–24 In particular, HICT has been proven to reverse adverse cardiac remodeling in patients with HFrEF. In addition, it positively affects exercise capacity and QoL, and this aligns with the results of the current study.22
With regard to NT-proBNP, in the current study, all groups showed significant differences, with HICT showing superiority over the rest of the groups. Santoso et al23 found that various types of exercise training for HF patients reduced plasma levels of NT-proBNP considerably. They added that even LICT can have an impact on these biomarkers. This is consistent with the current findings of this investigation. Furthermore, a meta-analysis showed that exercise improved endothelial function, serum levels of natriuretic peptides, and proinflammatory cytokines, and these effects were constant across different exercise intensities. Additionally, the latter study stated that HICT is superior to other training intensities in terms of causing more noticeable changes in circulating biomarkers. This was in line with our findings since HICT caused the most significant alteration in NT-proBNP.25
In relation to QoL and 6MWT, in the current study, all groups showed a significant improvement in QoL scores with no significant difference between groups. The 6MWT significantly increased in the three groups, with HICT showing a superior improvement.
Regular physical activity has been shown to improve QoL in people with HF.24 Exercise training in particular has been shown to increase exercise capacity and QoL. It also reduces morbidity and mortality in patients with HFrEF.24,25 In line with the findings of this study, previous research has shown that both HICT and MICT induced a nearly identical change in the QoL in HFrEF patients, suggesting that the commitment to a regular physical training program, rather than the intensity of the training, is the most important factor in improving QoL. However, the studies did not note that these increases in QoL are more noticeable after a longer period of training (six months). As a result, a similar study in a larger context and with longer periods of exercise commitment is required.22–26
In a systematic review and meta-analysis for exercise-based rehabilitation trials in HF using MLHFQ, Ostman et al27 found that the magnitude of the effect was positively proportional to the training exercise intensity. This was the case in the current study, as higher training intensities showed slightly higher percentages of improvement in QoL.
On the other hand, Ahmeti et al28 included 118 people with HF with HFpEF and HFrEF in their study. 6MWT and QoL assessments were performed. They found that the MLHFQ is the strongest predictor of exercise capacity measured by the 6MWT, especially in HFpEF patients but not in HFrEF patients. The variability of the patient’s demographics is large to be charged for the disparity (age, NYHA classification, baseline heart rate, and smoking history), and this might affect the QoL outcomes.
In contrast to our findings, data from experimental studies suggested that HICT induces a pathological remodeling when examined on a rat model of HF. The experimental work showed that MICT is better for controlling HF, decreasing LV fibrosis, increasing angiogenesis, increasing endothelial nitric oxide synthase protein, and reducing hypoxia.29 This contrast is mostly attributed to the difference in the cardiovascular response to exercise between rodents and humans.
For human studies, HICT was proven to increase cardiorespiratory fitness (VO2max) and cardiac output.30 Also, a meta-analysis of 56 articles mentioned that there is a direct correlation between VO2max, endothelial function, and smooth muscle function, suggesting that the core effect of HICT on cardiac remodeling is derived from its effect on VO2max.31 In comparison with lower exercise intensities, HICT has been shown to induce the highest change in VO2max.32,33
Limitations and Strengths
This study had several limitations that should be mentioned. First, the sample was relatively small and the study was performed in a single center, thus any generalization of the results should be cautioned. Second, we did not perform follow-ups. Third, the medical treatment was not standardized between the groups due to the heterogeneity of the nature of the disease, in a way that might affect the optimization of the medical therapy. Fourth, this study was confined to males due to recruitment issues and compliance with treatment. Regarding the strengths, this study highlighted how exercise – in general – has positive central and peripheral effects, and how HFrEF patients might be able to safely perform HICT. It also emphasizes that this form of training is the most effective for the HFrEF patients if compared with the other less demanding forms of exercises.
Mechanisms
Considering that heart failure with reduced ejection fraction (HFrEF) is a progressive condition accompanied by significant breathlessness, interval exercise has traditionally been the preferred choice.34 Existing literature has repeatedly suggested that continuous training may yield limited benefits for this patient population (preferring the interval approach), and if implemented, it should be at a low or moderate intensity.35 However, our findings clearly indicate that patients tolerated higher intensities of continuous training well and experienced greater cardiovascular improvements compared to lower intensities. Relatively recent evidence acknowledged that moderate continuous training is more beneficial than high-intensity interval training.36 This could be attributed to evidence suggesting that the breathlessness component and low exercise capacity in HFrEF patients contribute to a vicious cycle. In other words, improving the breathlessness component necessitates more training.37 Similarly, lower intensities may yield fewer improvements in HFrEF, while higher intensities hold more promising prospects.
Clinical Implications
All the studied types of continuous training can improve echocardiographic outcomes and functional capacity (expressed as 6MWD). In addition, the significant increase in EF and 6MWD after HICT compared to MICT and LICT, together with the benefits found in remodeling of the cardiac structures, suggest that the HICT protocol we proposed could constitute an effective tool in the functional recovery processes of patients with HFrEF. The findings suggest that in patients with HFrEF, the HICT program could be used in clinical practice, since these patients may benefit from that program. In addition, the proposed HICT program could be easily provided since the findings offer an alternative rehabilitation strategy for clinical and community care of these individuals.
Future research is suggested in order to investigate HICT programs including the assessment of outcomes such as respiratory outcomes (shortness of breath is common in HF patients) or other perceptual outcomes (patients’ adherence, acceptability, and enjoyability of the program) over longer periods in adequately sized populations, and follow-ups are advised.
Conclusion
In conclusion, the results obtained in the present study suggested that all types of continuous exercise can improve echocardiography parameters, NT-proBNP, and QoL in HFrEF patients. Among the various treatment groups, the HICT group was the most effective in improving all of the outcomes. These results suggested that HICT is an effective strategy to reverse cardiac dysfunction as a part of cardiac rehabilitation programs done for patients with HFrEF.
Abbreviations
HF, heart failure; CPET, Cardiopulmonary exercise testing; EF, Ejection fraction; FS, Fractional shortening; HFmrEF, Heart failure with mid-range Ejection Fraction; HFpEF, Heart failure with a preserved ejection fraction; HFrEF, Heart failure with a reduced ejection fraction; HICT, High-intensity continuous training; HRrest, Resting Heart rate; HRR, Heart rate reserve; LICT, Low-intensity continuous training; LV, Left ventricular; LVEDD, Left ventricular end-diastolic dimension; LVESD, Left ventricular end-systolic dimension; HRmax, Maximal heart rate; MIT, Moderate-intensity continuous training; MLWFQ, Minnesota Living with Heart Failure Questionnaire; NT-proBNP, N-Terminal Pro–B-Type Natriuretic Peptide; NYHA, New York Heart Association; QoL, Quality of life; RPE, Rate of perceived exertion; SD, Standard deviation; THR, Training heart rate; VO2 max, Maximal oxygen capacity.
Data Sharing Statement
The corresponding author [Mona Mohamed Taha] will disclose data for the current study upon reasonable request for three years post-publication.
Acknowledgments
We would like to thank Princess Nourah bint Abdulrahman University for supporting this project through Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R 286), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The authors thank residents and cardiology specialists, National Heart Institute, Egypt. Special thanks to all patients who participated in this study.
Funding
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R 286), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonagh TA, Metra M, Adamo M. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
2. Adamo MA-O, Gardner RS, McDonagh TA, Metra MA-O. The ‘Ten Commandments’ of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2022;43(6):440–441. doi:10.1093/eurheartj/ehab853
3. Hassanein M, Abdelhamid M, Ibrahim B, et al. Clinical characteristics and management of hospitalized and ambulatory patients with heart failure-results from ESC heart failure long-term registry-Egyptian cohort. ESC Heart Fail. 2015;2(3):159–167. doi:10.1002/ehf2.12046
4. Thompson PD, Arena R, Riebe D, Pescatello LS; American College of Sports M. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr Sports Med Rep. 2013;12(4):215–217. doi:10.1249/JSR.0b013e31829a68cf
5. McMurray JJV, Adamopoulos S, Anker SD. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803–869. doi:10.1093/eurjhf/hfs105
6. Gaggin HK, Dec GW. Pathophysiologyof heart failure. In: Fuster V, Harrington RA, Narula J, Eapen ZJ, editors. Hurst’s the Heart, 14e. McGraw-Hill Education; 2017.
7. Januzzi JL Jr, Chen-Tournoux AA, Christenson RH, et al. N-terminal pro-B-type natriuretic peptide in the emergency department: the ICON-RELOADED Study. J Am Coll Cardiol. 2018;71(11):1191–1200. doi:10.1016/j.jacc.2018.01.021
8. Sekaran NK, Crowley AL, de Souza FR, Resende ES, Rao SV. The role for cardiovascular remodeling in cardiovascular outcomes. Curr Atheroscler Rep. 2017;19(5). doi:10.1007/s11883-017-0656-z
9. Adebayo SO, Olunuga TO, Durodola A, Ogah OS. Quality of life in heart failure: a review. Niger J Cardiol. 2017;14(1):1. doi:10.4103/0189-7969.201914
10. Yancy CW, Jessup M, Bozkurt B. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):e240–e327. doi:10.1161/CIR.0b013e31829e8776
11. Bozkurt B, Hershberger RE, Butler J, et al. 2021 ACC/AHA key data elements and definitions for heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (writing committee to develop clinical data standards for heart failure). Circ Cardiovasc Qual. 2021;14(4):2053–2150. doi:10.1161/HCQ.0000000000000102
12. Carvalho VO, Mezzani A. Aerobic exercise training intensity in patients with chronic heart failure: principles of assessment and prescription. Eur J Cardiovasc Prev Rehabil. 2011;18(1):5–14. doi:10.1097/HJR.0b013e32833a9c63
13. Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE committee to update the 1997 guidelines for the clinical application of echocardiography). Circulation. 2003;108(9):1146–1162.
14. Alahdab MT, Mansour In Fau - Napan IN, Napan S, Fau - Stamos TD. Six minute walk test predicts long-term all-cause mortality and heart failure rehospitalization in African-American patients hospitalized with acute decompensated heart failure. J Card Fail. 2009;15(2):130–135. doi:10.1016/j.cardfail.2008.10.006
15. Guyatt GH, Sullivan MJ, Thompson PJ. The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J. 1985;132(8):919–923.
16. Ekblom-Bak E, Bjorkman F, Hellenius M-L, Ekblom B. A new submaximal cycle ergometer test for prediction of VO 2max. Scand J Med Sci Sports. 2014;24(2):319–326. doi:10.1111/sms.12014
17. Chatterjee S, Biondi-Zoccai G, Abbate A, et al. Benefits of blockers in patients with heart failure and reduced ejection fraction: network meta-analysis. BMJ. 2013;346(jan16 1):f55. doi:10.1136/bmj.f55
18. Karvonen MJ, Fau - Kentala E, Kentala E, Fau - Mustala O. The effects of training on heart rate; a longitudinal study. Ann Med Exp Biol Fenn. 1957;35(3):307–315.
19. Taylor RS, Walker S, Smart NA, et al. Impact of exercise rehabilitation on exercise capacity and quality-of-life in heart failure: individual participant meta-analysis. J Am Coll Cardiol. 2019;73(12):1430–1443. doi:10.1016/j.jacc.2018.12.072
20. Saccomann ICR, Cintra FA, Gallani MCBJ. Quality of life in older adults with heart failure: assessment with a specific instrument. Acta Paul Enferm. 2011;24:179–184. doi:10.1590/S0103-21002011000200004
21. Pina IL, Apstein CS, Balady GJ, et al. Exercise and heart failure: a statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. 2003;107(8):1210–1225.
22. Ismail H, McFarlane JR, Nojoumian AH, Dieberg G, Smart NA. Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure: a systematic review and meta-analysis. JACC Heart Fail. 2013;1(6):514–522. doi:10.1016/j.jchf.2013.08.006
23. Santoso A, Maulana R, Alzahra F, et al. The effects of aerobic exercise on N-terminal Pro-B-type natriuretic peptide and cardiopulmonary function in patients with heart failure: a meta-analysis of randomised clinical trials. Heart Lung Circ. 2020;29(12):1790–1798. doi:10.1016/j.hlc.2020.05.098
24. Taylor RS, Sagar VA, Davies EJ. Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev. 2014;2014(4):CD003331. doi:10.1002/14651858.CD003331.pub4
25. Haykowsky MJ, Liang Y, Pechter D, Jones LW, McAlister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll Cardiol. 2007;49(24):2329–2336. doi:10.1016/j.jacc.2007.02.055
26. Tucker WJ, Lijauco CC, Hearon CM
27. Ostman C, Jewiss D, Smart NA. The effect of exercise training intensity on quality of life in heart failure patients: a systematic review and meta-analysis. Cardiology. 2017;136(2):79–89. doi:10.1159/000448088
28. Ahmeti A, Henein MY, Ibrahimi P, et al. Quality of life questionnaire predicts poor exercise capacity only in HFpEF and not in HFrEF. BMC Cardiovasc Disord. 2017;17(1). doi:10.1186/s12872-017-0705-0
29. Holloway TM, Bloemberg D, da Silva ML, Simpson JA, Quadrilatero J, Spriet LL. High intensity interval and endurance training have opposing effects on markers of heart failure and cardiac remodeling in hypertensive rats. PLoS One. 2015;10(3):e0121138. doi:10.1371/journal.pone.0121138
30. Astorino TA, Edmunds Rm Fau - Clark RM, Clark A, et al. High-intensity interval training increases cardiac output and V˙O2max. Med Sci Sports Exerc. 2017;49(2):265–273. doi:10.1249/MSS.0000000000001099
31. Montero D. The association of cardiorespiratory fitness with endothelial or smooth muscle vasodilator function. Eur J Prev Cardiol. 2015;22(9):1200–1211. doi:10.1177/2047487314553780
32. Ruffino JS, Songsorn P, Haggett M, et al. A comparison of the health benefits of reduced-exertion high-intensity interval training (REHIT) and moderate-intensity walking in type 2 diabetes patients. Appl Physiol Nutr Metab. 2017;42(2):202–208. doi:10.1139/apnm-2016-0497
33. Wewege M, van den Berg R, Ward RE, Keech A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: a systematic review and meta-analysis. Obes Rev. 2017;18(6):635–646. doi:10.1111/obr.12532
34. DA-O L, Chen P, Zhu J. The effects of interval training and continuous training on cardiopulmonary fitness and exercise tolerance of patients with heart failure-a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(13):1660–4601. doi:10.3390/ijerph18041660
35. Edwards J, Shanmugam N, Ray R, et al. Exercise mode in heart failure: a systematic review and meta-analysis. Sports Med Open. 2023;9(1):3. doi:10.1186/s40798-022-00549-1
36. Tucker WJ, Beaudry RI, Liang Y, et al. Meta-analysis of exercise training on left ventricular ejection fraction in heart failure with reduced ejection fraction: a 10-year update. Prog Cardiovasc Dis. 2019;62(2):163–171. doi:10.1016/j.pcad.2018.08.006
37. Farghaly A, Fitzsimons D, Bradley J, Sedhom M, Atef H. The need for breathing training techniques: the elephant in the heart failure cardiac rehabilitation room: a randomized controlled trial. Int J Environ Res Public Health. 2022;19(22):14694. doi:10.3390/ijerph192214694
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.