Back to Journals » Journal of Pain Research » Volume 18
Different Acupuncture Therapies Combined with Sulfasalazine for the Treatment of Ankylosing Spondylitis: Bayesian Network Meta-Analysis
Authors Han K, Yu M, Chen J ![]() , Wang S
, Wang S
Received 24 July 2025
Accepted for publication 24 October 2025
Published 8 November 2025 Volume 2025:18 Pages 5991—6006
DOI https://doi.org/10.2147/JPR.S555916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Kaili Han,1,2 Mengquan Yu,3 Jing Chen,4 Shiheng Wang1
1School of Traditional Chinese Medicine, Binzhou Medical University, Yantai, People’s Republic of China; 2The Fifth Hospital of Qinhuangdao City, Qinhuangdao, People’s Republic of China; 3Muping District Hospital of Traditional Chinese Medicine, Yantai, People’s Republic of China; 4College of Medical Imaging Laboratory and Rehabilitation, Xiangnan University, Chenzhou, People’s Republic of China
Correspondence: Jing Chen, College of Medical Imaging Laboratory and Rehabilitation, Xiangnan University, Chenzhou, Hunan, People’s Republic of China, Email [email protected] Shiheng Wang, School of Traditional Chinese Medicine, Binzhou Medical University, Yantai, Shandong, People’s Republic of China, Email [email protected]
Background: Ankylosing Spondylitis (AS) is a serious challenge to public health. Acupuncture can effectively improve pain symptoms, activity function and quality of life in patients with AS. However, there is still significant heterogeneity in the evidence of its efficacy. Therefore, by conducting a Bayesian network meta-analysis, the efficacy of different acupuncture methods can be evaluated more systematically, providing a scientific basis for the optimization of treatment strategies for AS.
Methods: Randomized controlled trials of acupuncture combined with Sulfasalazine (SASP) for AS published in commonly used databases. Time up to July 8, 2025. Analysis was conducted using R4.2.0 and Stata16.0.
Results: 31 studies included 9 acupuncture methods. Network meta-analysis results: On the BASDAI indicator: Acupuncture combined with SASP did not have a significant advantage over SASP. In terms of BASFI, SASP and Acupotomy and Tuina or Fu’s Subcutaneous needling and Traditional Chinese medicine had a significant advantage over SASP. In terms of Efficacy, compared with SASP, Acupotomy and SASP, Warm Needling and Tuina and SASP, Du Meridian Moxibustion and SASP Du Meridian Moxibustion and Traditional Chinese medicine and SASP, Du Meridian Moxibustion and Acupuncture and SASP Bowl moxibustio and SASP, Fu’s Subcutaneous needling and Traditional Chinese medicine and SASP Acupuncture and SASP, Acupuncture and Traditional Chinese medicine and SASP have significant advantages. Du Meridian Moxibustion and Acupuncture and SASP are more effective than Du Meridian Moxibustion and SASP.
Conclusion: Based on the results of this study, Acupotomy, Du Meridian Moxibustion and Cupping and SASP combined with SASP have the best effects.
Keywords: acupuncture, ankylosing spondylitis, sulfasalazine, network meta-analysis as topic
Introduction
Ankylosing Spondylitis (AS) is a chronic immune-mediated inflammatory arthritis primarily affecting the axial skeleton, peripheral joints, and entheses. The global prevalence of AS varies significantly by region, affecting approximately 1 in 200 individuals on average, with higher prevalence rates reported in Asian populations.1 AS imposes a multidimensional burden on patients, affecting physical health, mental well-being, and overall quality of life. Patients often experience substantial functional impairments, including restricted spinal mobility, joint stiffness, and chronic pain, which can significantly compromise their ability to perform daily activities.2 Furthermore, AS is frequently associated with various extra-articular manifestations, such as uveitis, psoriasis, and inflammatory bowel disease, which further contribute to the disease burden.3 Notably, mental health comorbidities in AS patients have garnered increasing attention, with recent studies indicating a potential association between AS and an elevated risk of schizophrenia and anorexia nervosa.4 From a socioeconomic perspective, AS not only incurs substantial direct medical costs but also imposes indirect economic burdens through work disability, reduced productivity, and early retirement.5 Additionally, the chronic inflammatory nature of AS is linked to multiple comorbidities, including cardiovascular diseases and certain cancers, collectively posing a significant public health challenge.6
While conventional pharmacological treatments such as non-steroidal anti-inflammatory drugs (NSAIDs) and biologic agents can alleviate symptoms, long-term use may lead to adverse effects, including gastrointestinal complications and an increased susceptibility to infections. Moreover, some patients exhibit inadequate responses to these therapies.7 Surgical interventions, such as total hip arthroplasty, can address severe joint deformities but are associated with surgical risks and potential postoperative complications.8 Importantly, current treatment modalities offer limited efficacy in managing persistent symptoms such as chronic pain and morning stiffness, and are generally unable to halt disease progression.9 In this context, acupuncture, as a traditional Chinese medicine therapy, demonstrates unique therapeutic advantages. Current evidence has confirmed that acupuncture is associated with higher safety, fewer side effects, and lower economic burden.10 Evidence suggests that acupuncture exerts its therapeutic effects through multiple mechanisms, including modulation of inflammatory cytokines and improvement of microcirculation.11 Clinical studies have shown that various acupuncture techniques, such as electroacupuncture and moxibustion, can effectively alleviate pain, improve functional mobility, and enhance quality of life in patients with AS.12 Notably, acupuncture has demonstrated particular efficacy in reducing morning stiffness and improving spinal range of motion.13 Currently, sulfasalazine (SASP) is widely used in pharmacological treatment, and numerous studies have incorporated complementary interventions such as acupuncture, moxibustion, bee venom acupuncture, or cupping therapy, achieving promising clinical outcomes.
Although acupuncture therapy demonstrates unique advantages in the treatment of autism spectrum disorder (ASD), the evidence regarding its efficacy remains incomplete across multiple dimensions, including its mechanism of action, study design, intervention protocols, operational techniques, control settings, and outcome measures. For instance, the therapeutic mechanisms of acupuncture encompass both specific and non-specific factors—such as placebo/contextual effects, which have been demonstrated to influence both acute and chronic pain.14 In particular, inconsistencies in acupuncture methodology may introduce bias into efficacy evaluations. Moreover, the invasive nature of needle insertion conveys a therapeutic significance that heightens patient awareness of the treatment process, thereby potentially influencing clinical outcomes.15 Key controversies in current research revolve around the standardization of acupuncture protocols and the methodological rigor of efficacy evaluations. On one hand, the coexistence of diverse acupuncture techniques presents a challenge in establishing standardized treatment regimens that ensure comparability across studies. On the other hand, although randomized controlled trials (RCTs) are considered the gold standard for evaluating therapeutic efficacy, the unique characteristics of acupuncture research—such as the difficulty in implementing double-blinding—have resulted in variable study quality. Moreover, the underlying mechanisms of acupuncture remain insufficiently explored, which may hinder the broader acceptance of its therapeutic benefits. These challenges underscore the need for high-quality, methodologically rigorous studies to further evaluate the efficacy of acupuncture. Therefore, conducting a Bayesian network meta-analysis would enable a more comprehensive and systematic evaluation of different acupuncture techniques, thereby providing a scientific basis for optimizing treatment strategies in AS.
Methods
Study Registration
Our study was conducted in accordance with the reporting guidelines for systematic reviews and network meta-analyses (PRISMA-NMA)16 and was prospectively registered in PROSPERO (ID: CRD420251088871).
Eligibility Criteria
Inclusion criteria:
Population: Patients clearly diagnosed with Ankylosing Spondylitis. No restrictions on race, nationality, gender, age, disease duration, etc. The diagnostic criteria lack uniformity, with most studies employing the 1984 New York revised AS classification criteria:17 ① persistent low back pain for at least 3 months, with pain improving upon activity but not alleviated by rest; ② limited lumbar spinal mobility in both anterior-posterior and lateral flexion; ③ chest expansion reduced relative to normal values for age and gender; ④ bilateral sacroiliitis grade II–IV or unilateral sacroiliitis grade III–IV. A definitive diagnosis of AS can be established if criterion ④ is met along with any one of criteria ① to ③. Imaging findings suggestive of Spondyloarthritis (SpA) include: ① MRI evidence of active (acute) inflammation in the sacroiliac joints, highly indicative of SpA-associated sacroiliitis, or ② definitive radiographic changes of sacroiliitis according to the 1984 revised New York criteria.
Intervention: The use of acupuncture therapy (including acupuncture, electroacupuncture, fire acupuncture, bee acupuncture, needle knife, moxibustion, etc) in combination with sulfasalazine.
Comparison: Sulfasalazine.
Outcome: (1) Bath ankylosing spondylitis disease activity index (BASDAI) score:18 A total of 6 questions (A to F) were scored based on the patient’s review of fatigue, axial and peripheral joint pain, morning stiffness, and tendon end pain symptoms over the past week. Except for morning stiffness, which was scored at 0, 2.5, 5, 7.5 and 10 respectively for duration (none, 30, 60, 90 and more than 120 minutes), the rest were scored using the Visual Analogue Scale (VAS) method. The final score is calculated by the formula 0.2×[A+B+C + D + (E+F)/2], with a total score of 0 to 10. Generally, a score greater than 4 indicates disease activity, and the higher the score, the more obvious the disease activity. (2) Bath ankylosing spondylitis functional index (BASFI) score:19 A total of 10 questions, with daily activities such as putting on socks, bending over, and standing as the main observation, were recorded using the Visual Analog Scale (VAS) method, with a total score of 10 points, to evaluate the comprehensive function of the patients. This index can change in the short term in the clinical trial, and the higher the score, the worse the situation. (3) Efficacy (effective number/total number *100%).
Study design: A randomized controlled trial.
Exclusion criteria: Non-randomized controlled trials such as animal tests, reviews, conference papers, etc. Unclear reporting of research results, incomplete research data; The treatment plan involves other treatment measures; Small sample size; Different studies derived from the same randomized controlled trial included one with the largest sample size, the most comprehensive follow-up time, and the most outcome measures.
Data Sources and Search Strategy
We systematically searched China National Knowledge Infrastructure (CNKI), Wanfang, VIP, SinoMed, PubMed, EMbase, Cochrane Library, and Web of Science for randomized controlled trials of acupuncture combined with SASP for ankylosing spondylitis. The search was conducted up to July 8, 2025. (Search strategy see Supplementary Material 1).20
Study Selection
We imported the retrieved literature into EndNoteX9 software, which automatically marked duplicate literature by software and manually identified duplicate literature to propose duplicate published literature. For the remaining literature, we deleted the unqualified literature by reading the title and abstract, downloaded the full text of the qualified literature, and finally read the full text for further screening. To identify the original studies that fit into our systematic review. The literature screening process was conducted independently by two researchers, with cross-checks after completion and discussions with a third researcher in case of disagreement.
Data Extraction
Two researchers designed data extraction tables based on the information needed for the study and extracted independently. The content included: ① Basic information: Title, author, year, study type, diagnostic criteria, intervention measures, course of treatment, outcome measures; ② Demographic characteristics: Sample size, age, gender; ③ Methodological information: randomization methods, allocation concealment schemes, blinding, etc. When the information extracted by two people is inconsistent, discuss and resolve it first. If it still cannot be resolved, discuss and decide.
Risk of Bias in Studies
Two researchers used the Cochrane Randomized Controlled Trial bias risk assessment tool16 to assess the risk of bias. The assessment tool included seven items: generation of random sequences, allocation concealment, blinding of subjects and intervention providers, blinding of outcome evaluators, incomplete outcome data, selective outcome reporting, and other sources of bias, each of which was assessed as low bias, high bias, or unclear. Use Revman5.4 to visually present the risk of bias assessment results.
Synthesis Methods
The Bayesian random effects model was adopted to compare the effects among intervention measures in order to compare the effectiveness of various intervention methods. Modeling was done using the Markov Chain Monte Carlo method, with four Markov chains running simultaneously, with 20,000 annealing cycles set, and after 50,000 simulation iterations. And we will use the Deviation Information Standard (DIC) to compare model fit with global consistency, and if there is a closed-loop mesh, we will use node splitting to analyze local consistency. In addition, SuCRa-based ranking of the interventions and generating league tables to compare the differences in effects among the interventions. When the number of studies included in the outcome measure was ≥10, a funnel plot was used to visually show the response publication bias. Analysis at Stata 16.0 (Stata Corporation, College Station) TX) and R4.2.0 (R development Core Team, Vienna, http://www.R-project.org). P<0.05 indicates a statistically significant difference.
Quality of Evidence Assessment
Use Confidence in Network Meta-Analysis (CINeMA)21 to assess the quality of evidence. CINeMA graded the quality of evidence from six domains, namely intra-study bias, inter-study bias, indirectness, imprecision, heterogeneity, and inconsistency, and the final quality of evidence grades were high, medium, and Low and very low quality are four grades.
Results
Study Selection
A preliminary search yielded 3303 relevant studies, and 1213 duplicate studies were excluded. 40 studies were retained after reading titles and abstracts, and 9 studies were excluded through full-text screening (8 with inconsistent intervention measures and 1 with unbalanced baseline). Finally, 31 studies were included22–52 (the literature screening process is shown in Figure 1).
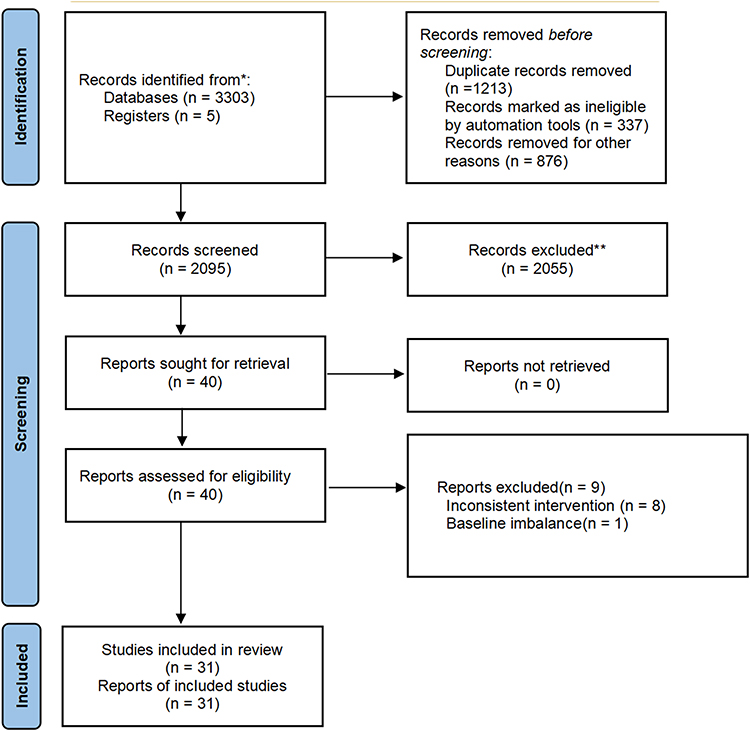 |
Figure 1 Literature screening process (*Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers. **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools). |
Study Characteristics
This study included 31 studies, involving a total of 2458 patients (1232 in the experimental group and 1226 in the control group). The year of publication in the journal was 2009–2025. Including 9 acupuncture methods: Acupotomy, warm acupuncture, Du Meridian moxibustion, thunder fire moxibustion, bowl moxibustion, wheat grain moxibustion, floating needle, acupuncture, acupoint application. The intervention for the control group was sulfasalazine (basic characteristics of the included studies are shown in Table 1).
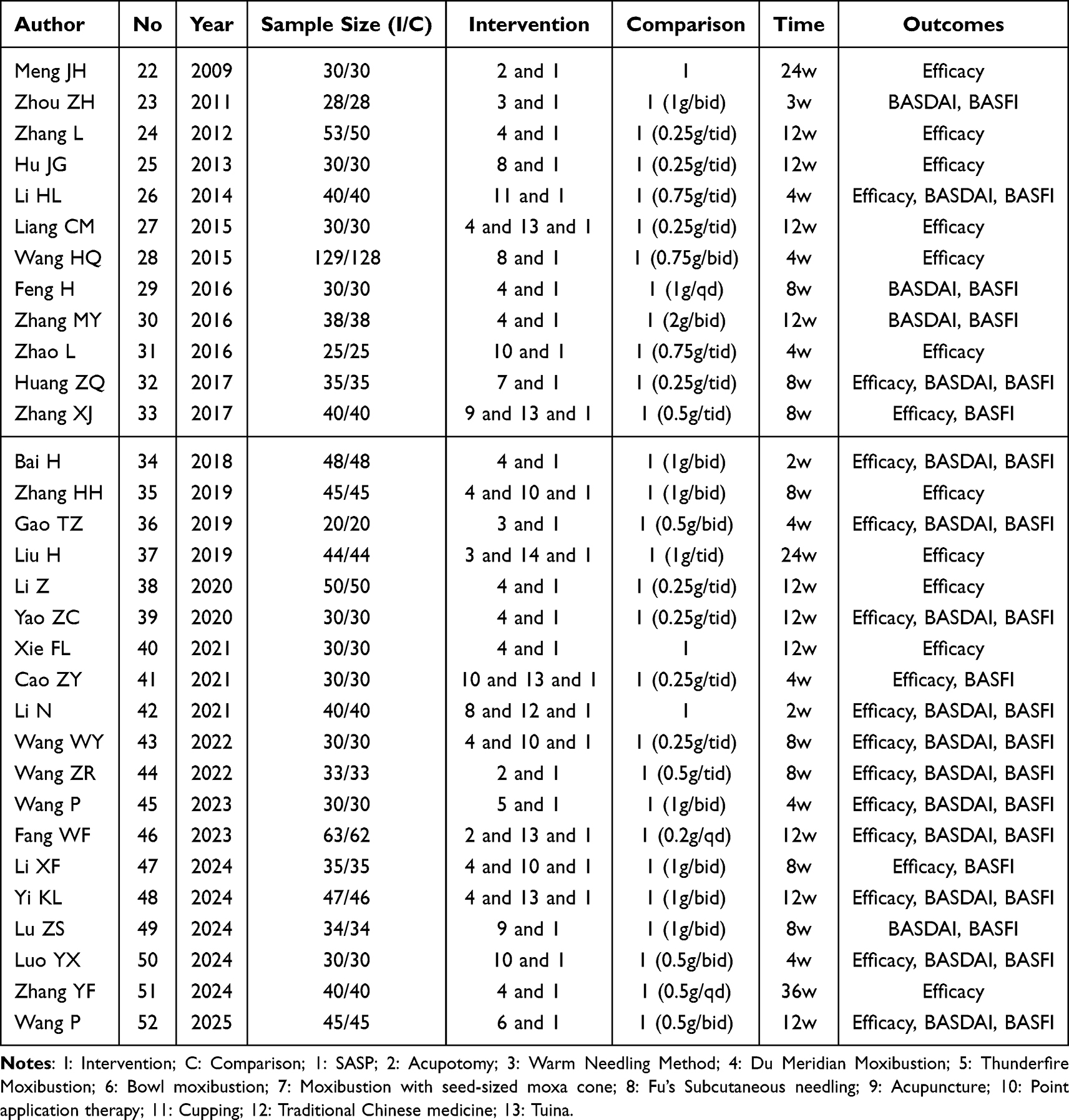 |
Table 1 Basic Characteristics of the Included Studies |
Risk of Bias in Studies
In terms of stochastic methods, 22 studies used random number table, 1 study assigned by treatment regimens. In terms of allocation concealment, 2 studies used envelopes. In terms of blinding, all studies did not specify whether blinding was used. Data from all studies were complete and no selective reporting or other publication biases were found. Figures 2 and 3 shows the risk of bias results for the included studies.
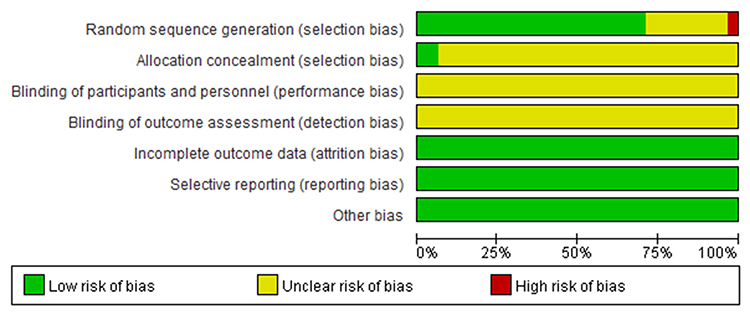 |
Figure 2 Risk of bias graph. |
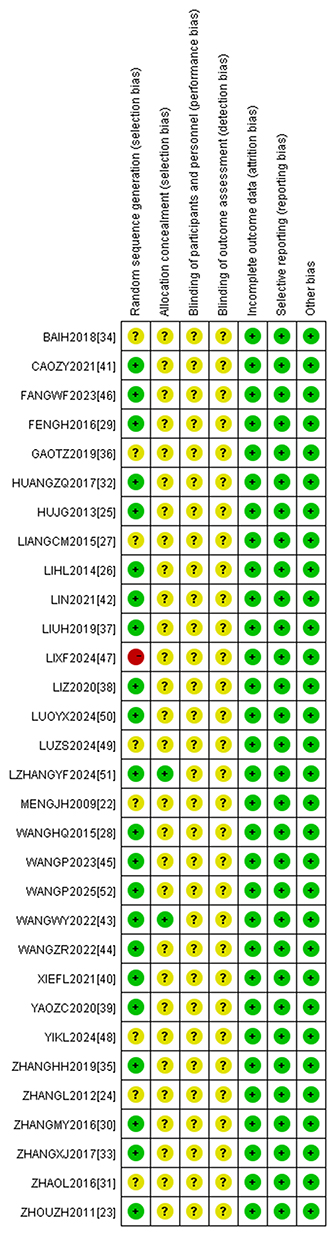 |
Figure 3 Risk of bias summary. |
Meta Analysis
BASDAI
Seventeen studies reported BASDAI, with the trial groups containing 12 interventions. Each study only reported comparisons between the experimental group and the control group. The graphs show no closed loops (see Figure 4).
 |
Figure 4 Network Diagram of acupuncture combined with SASP for AS (BASDAI). |
Heterogeneity tests showed small heterogeneity (I2=3%). The results of the network meta-analysis showed no significant advantage for each intervention compared with the control group (P > 0.05) (see Figure 5 and Supplementary Material 2). The top three SUCRas in order were: Fu’s Subcutaneous needling and SASP (0.70), Du Meridian Moxibustion and Acupuncture and SASP (0.68) Thunderfire Moxibustion and SASP (0.62) (Table 2).
 |
Table 2 SUCRA Rank |
 |
Figure 5 Forest map of acupuncture combined with SASP for AS (BASDAI). |
BASFI
Twenty studies reported BASFI, with 13 interventions included in the trial groups. The studies only reported comparisons between the groups and the controls. The graphs show no closed loops (see Figure 6).
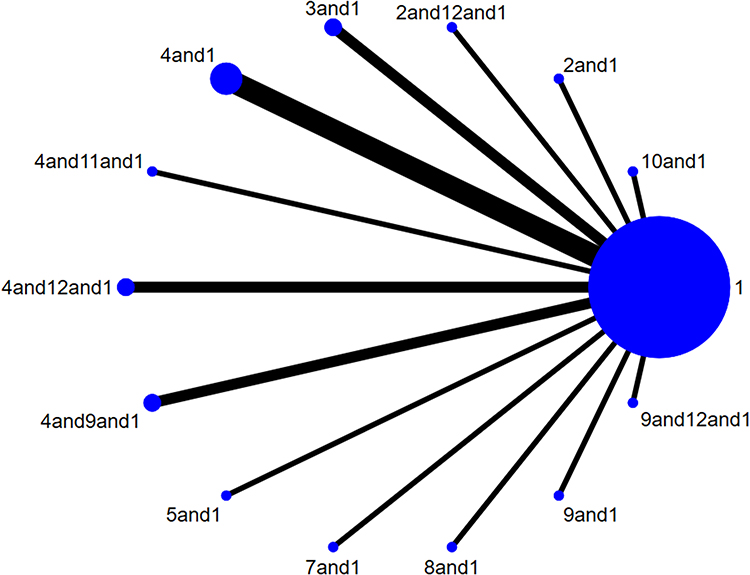 |
Figure 6 Network diagram of acupuncture combined with SASP for AS (BASFI). |
Heterogeneity tests showed small heterogeneity (I2=3%). The results of the network meta-analysis showed that compared with the control group, 2 and 12 and 1 (MD=−2.40,95% CI (−4.30, −0.43), P < 0.05) and 4 and 11 and 1 (MD=−7.20,95% CI (−14.00, −0.16), P < 0.05) had a significant advantage (see Figure 7 and Supplementary Material 2). The top three SUCRA rankings are: Du Meridian Moxibustion and 11Cupping and SASP (0.95), Acupotomy and Traditional Chinese medicine and SASP (0.81) Fu’s Subcutaneous needling and SASP (0.66) (Table 2).
 |
Figure 7 Forest map of acupuncture combined with SASP for AS (BASFI). |
Efficacy
Twenty-nine studies reported Efficacy, with the trial groups containing 15 interventions, and the graph showed no closed loop (see Figure 8).
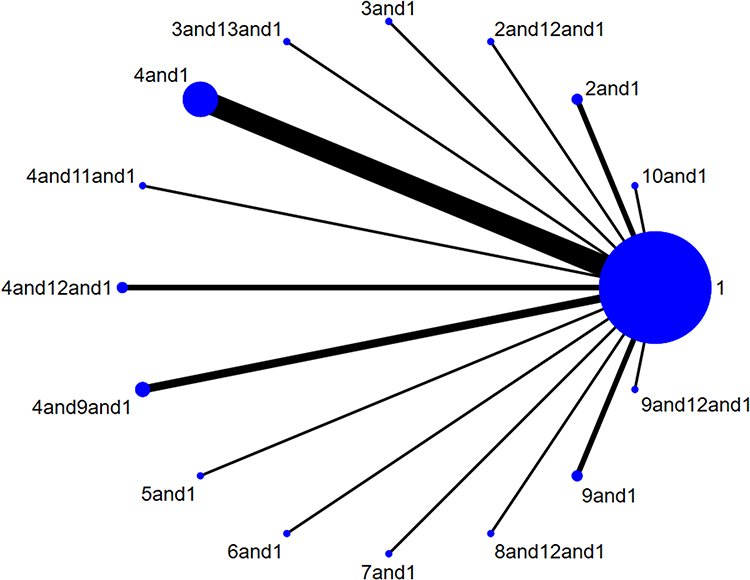 |
Figure 8 Network Diagram (Efficacy) of acupuncture combined with SASP for AS. |
Heterogeneity tests showed small heterogeneity (I2=0%). The results of the network meta-analysis showed that compared with the control group, Acupotom and 1 (RR=1.41,95% CI 1.16,1.75), P < 0.05, Warm Needling and Tuina and SASP (RR=1.23,95% CI 1.01,1.53), P < 0.05 Du Meridian Moxibustion and SASP (RR=1.13,95% CI 1.06,1.21), P < 0.05 Du Meridian Moxibustion and Traditional Chinese medicine and SASP (RR=1.24,95% CI 1.01,1.50), P < 0.05 Du Meridian Moxibustion and Acupuncture and SASP (RR=1.38,95% CI 1.18,1.66), P < 0.05 Bowl moxibustion and SASP (RR=1.31,95% CI 1.02,1.77), P < 0.05 Fu’s Subcutaneous needling and Traditional Chinese medicine and SASP (RR=1.41,95% CI 1.13,1.88), P < 0.05 Acupuncture and SASP (RR=1.29,95% CI 1.07,1.69) Acupuncture and 1Traditional Chinese medicine and SASP (RR=1.26,95% CI 1.00,1.67), P < 0.05) had significant advantages. Du Meridian Moxibustion and Acupuncture and SASP were more effective than Acupuncture and SASP (RR=1.22,95% CI 1.03,1.48), P < 0.05) (Figure 9). The results of the network meta-analysis showed no significant difference among the acupuncture methods (P > 0.05) (see Supplementary Material 2). The top three SUCRA results were: Acupuncture and Tuina and SASP (0.78), Acupotomy and SASP (0.77) Du Meridian Moxibustion and point application therapy and SASP (0.75) (Table 2).
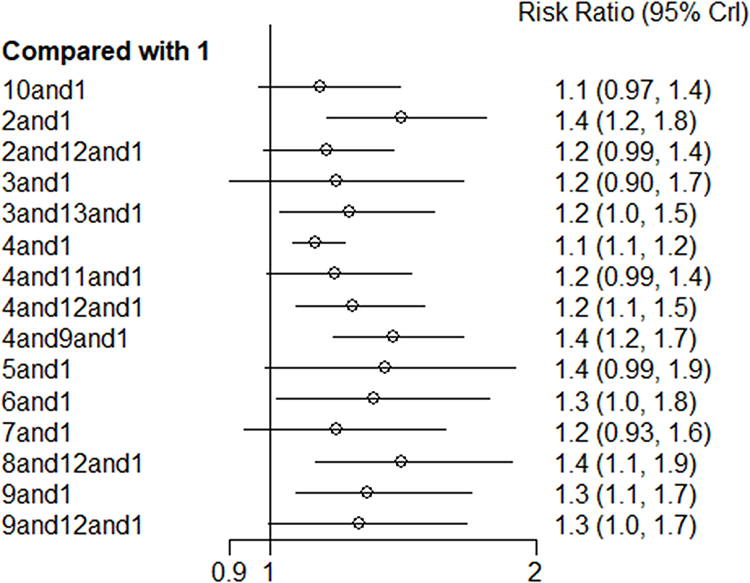 |
Figure 9 Forest map of acupuncture combined with SASP for AS (Efficacy). |
Publication Bias and Quality of Evidence Assessment
Egger’s test for the three outcome measures showed no significant differences (BASDAI: P=0.99, BASFI: P=0.99, Efficacy: P=0.78). Quality of evidence was assessed using CINeMA. The results showed that the main reasons for degradation were Imprecision and Incoherence (Supplementary Material 3).
Discussion
This study included 31 studies encompassing nine acupuncture methods: Acupotomy, warm acupuncture, Du meridian moxibustion, thunder fire moxibustion, noodle bowl moxibustion, wheat grain moxibustion, floating needle, acupuncture, and acupoint application. A total of three outcome indicators were analyzed. Regarding BASDAI scores, acupuncture combined with sulfasalazine (SASP) did not demonstrate a significant advantage over SASP alone. In terms of BASFI scores, combinations such as acupotomy with SASP, Fu’s subcutaneous needling with Tuina, and traditional Chinese medicine (TCM) with SASP showed significant improvements compared to SASP alone. Regarding overall efficacy, several treatment regimens—including acupotomy combined with SASP, warm needling combined with Tuina and SASP, Du meridian moxibustion combined with SASP, Du meridian moxibustion combined with TCM and SASP, Du meridian moxibustion combined with acupuncture and SASP, noodle bowl moxibustion combined with SASP, Fu’s subcutaneous needling combined with TCM and SASP, acupuncture combined with SASP, and acupuncture combined with TCM and SASP—demonstrated significant advantages over SASP alone. Notably, the combination of Du meridian moxibustion and acupuncture with SASP showed greater efficacy than Du meridian moxibustion combined with SASP alone. Adverse reactions were reported in two studies. Acupuncture combined with SASP was associated with fewer adverse reactions compared to SASP alone, and severe adverse events were rare. Reported symptoms included one case of gastrointestinal discomfort (loss of appetite, abdominal distension, nausea) and two cases of minor subcutaneous bleeding that resolved spontaneously. In the control group, nine cases of gastrointestinal reactions and two cases of rash were observed. Based on the meta-analysis results and SUCRA ranking, the most effective combinations appeared to be acupotomy with SASP and Du meridian moxibustion combined with cupping and SASP. The operation steps are in Supplementary Material 4.
Published meta-analyses have confirmed the efficacy of acupuncture in treating SASP. Zhao Wenjia’s study53 included a total of 21 studies involving 1820 patients. The meta-analysis results showed that acupuncture was statistically superior to Western medicine in terms of effective rate [OR = 3.25; 95% CI (2.52; 4.20)], thoracic expansion degree [SMD = 0.32; 95% CI (0.09; 0.54)], fingertip-to-floor distance [SMD = −1.01; 95% CI (−1.27; −0.76)], occipital-to-wall distance [SMD = −0.73; 95% CI (−1.19; −0.27)], Schober test [SMD = 0.37; 95% CI (0.22; 0.53)], and erythrocyte sedimentation rate [SMD = −0.80; 95% CI (−1.21; −0.40)]. However, it did not compare the effects of different acupuncture methods. Our study controlled for variables, with SASP as the control group, to minimize heterogeneity and compare the effects of different acupuncture methods, which has clinical reference value.
Acupotomy therapy can repair tissue damage and restore mechanical balance. Acupotomy release therapy can effectively separate adhesions between muscles and ligaments, alleviate pathological traction caused by muscle contracture on the vertebral bodies, and disrupt scar tissue to promote tissue reorganization and restore normal joint biomechanics. By cutting, stripping, and releasing the affected areas, Acupotomy therapy can enhance local microcirculation, restore the elasticity of the lumbar and dorsal muscles, improve muscle contractility, reduce stiffness in small joints, and increase spinal mobility. Additionally, Acupotomy therapy can regulate immune and inflammatory factors. Studies have shown that Acupotomy therapy significantly reduces levels of inflammatory cytokines such as TNF-α, IL-6, and IL-2 in patients with axial AS.54 Clinical evidence supports the efficacy of Acupotomy therapy. Zhong55 randomly divided 80 AS patients into two groups: 40 received nimesulide treatment (control group), and 40 received Acupotomy therapy (treatment group). Post-treatment assessments showed that the treatment group exhibited significantly greater improvements in cervical range of motion, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels compared to the control group (P < 0.05). Shi56 treated 24 AS patients with Acupotomy therapy targeting the interspinous ligament, costo-transverse process joint, and facet joints. The results indicated significant improvements in spinal mobility, suggesting that Acupotomy therapy alone can effectively reduce inflammation and improve joint mobility in ASpatients. Meta-analysis results further confirmed the efficacy of Acupotomy therapy in treating AS. Compared with the control group, the Acupotomy treatment group showed statistically significant improvements in overall efficacy [OR = 6.80, 95% CI (4.29, 10.77), P < 0.00001], BASDAI score [MD = −1.06, 95% CI (−1.49, −0.63), P < 0.00001], BASFI score [MD = −0.92, 95% CI (−1.27, −0.56), P < 0.00001], Schober test [MD = 1.20, 95% CI (0.70, 1.70), P < 0.0001], morning stiffness duration [MD = −18.05, 95% CI (−20.78, −15.31), P < 0.00001], thoracic expansion [MD = 1.20, 95% CI (1.07, 1.34), P < 0.0001], and finger-to-ground distance [MD = −3.81, 95% CI (−5.39, −2.23), P < 0.00001].56
Du meridian moxibustion, through the application of thermal stimulation to the Du meridian and bladder meridian, promotes local blood circulation and enhances tissue oxygenation, thereby alleviating pain and stiffness symptoms. Research has demonstrated that the combination of moxibustion and sulfasalazine (SASP) in the treatment of cold-dampness-blocking type ankylosing spondylitis (AS) significantly reduces inflammatory markers such as CRP and ESR, while improving clinical signs without a notable increase in adverse events.57 Multiple studies have confirmed that the integration of Du meridian moxibustion into treatment regimens offers significant advantages in symptom relief and inflammatory marker reduction. Liao et al58 reported that the combination of Du meridian moxibustion and SASP significantly reduced CRP and ESR levels and improved clinical sign scores compared to conventional pharmacological treatment alone. Chen et al59 further demonstrated that the total effective rate of Du meridian moxibustion combined with acupuncture was 96.4%, significantly higher than the 88.9% observed in the acupuncture-only group. Moreover, improvements in BASFI and BASDAI scores were more pronounced in the combination therapy group. Cupping therapy, which utilizes the thermal and negative pressure effects of cupping devices, provides benign stimulation to specific acupoints, thereby accelerating metabolism and promoting the absorption of inflammatory substances.60 This therapeutic approach complements moxibustion by optimizing the internal environment in AS patients and enhancing local blood circulation. The negative pressure effect facilitates the removal of stasis and metabolic waste, effectively relieving local muscle tension, reducing joint stiffness, alleviating pain in the spinal and lumbosacral regions, improving microcirculation, promoting tissue repair and regeneration, and restoring joint structure and function. Meta-analytical evidence further supports the efficacy of Du meridian moxibustion. For instance, Li’s meta-analysis indicated that Du moxibustion significantly improved spinal mobility in AS patients. The finger-to-ground distance [SMD = 0.63, 95% CI (0.30, 0.97), P = 0.000], Distance from the pillow to the wall [MD = 0.96, 95% CI (0.19, 1.73), P = 0.01], thoracic mobility [MD = 0.41, 95% CI (0.30, 0.53), P < 0.0001], and lumbar range of motion [MD = 1.56, 95% CI (1.22, 1.90), P < 0.0001] all showed significant improvements compared to control interventions.61 He’s meta-analysis further revealed that Du moxibustion significantly increased the overall effective rate (RR = 1.19, 95% CI 1.07–1.32, P < 0.05), reduced VAS scores (MD = −1.15, 95% CI −1.95 to −0.35, P < 0.05), improved PGA scores (MD = 1.23, 95% CI 0.90–1.55, P < 0.05), and reduced morning stiffness duration (MD = −4.51, 95% CI −7.55 to −1.47, P < 0.05). However, no statistically significant differences were observed in BASFI scores (MD = 0.76, 95% CI −0.39 to 1.91, P > 0.05) or adverse reaction rates (RR = 0.62, 95% CI 0.32–1.19, P > 0.05).62
The quality of evidence and heterogeneity across outcomes represent critical challenges in existing meta-analyses of acupuncture and its combination therapies for AS. Despite accumulating evidence supporting the clinical efficacy of acupuncture, methodological inconsistencies and variations in outcome reporting across studies limit the comparability and reliability of findings. First, discrepancies in inclusion criteria—such as the inclusion of only randomized controlled trials versus mixed designs—introduce potential biases. Second, the diversity of outcome measures, including BASDAI scores, inflammatory markers (CRP, ESR), and quality of life assessments (SF-36), complicates direct comparisons. Additionally, the lack of standardized acupuncture parameters—such as acupoint selection, treatment duration, and frequency—further contributes to result variability. These factors collectively undermine the consistency and robustness of the available evidence, highlighting the need for more rigorous methodological frameworks and standardized protocols in future research.
This study employed a Bayesian network meta-analysis approach, offering significant methodological innovation in evaluating the comparative efficacy of acupuncture combined with SASP for AS treatment. Compared to traditional frequentist methods, the Bayesian framework allows for more flexible handling of complex intervention networks, enabling direct comparisons among multiple treatment strategies and providing intuitive efficacy rankings through posterior probability distributions. This is particularly advantageous for interventions like acupuncture, which involve diverse operational parameters and complex treatment modalities. The Bayesian approach can better accommodate heterogeneity across studies and offer more comprehensive evidence to support clinical decision-making. Nonetheless, this study has several limitations. First, the relatively small sample sizes of included studies may compromise the precision of effect estimates. Second, variations in acupuncture manipulation parameters—such as acupoint selection, stimulation intensity, and treatment duration—across studies may affect the reliability of network meta-analysis results. Third, the methodological quality of some included studies was suboptimal, with inadequate reporting of randomization and blinding procedures, which could introduce bias into the analysis. This study is the failure to quantitatively report inter-rater consistency measures (such as Kappa values) during the literature screening and data extraction phases. However, we have endeavored to minimize subjective bias and ensure process reliability through pre-reviewer training, pre-experiment calibration, and consensus discussions on all disagreements.
Evidence degradation primarily stems from imprecision and incoherence. Imprecision is often due to small sample sizes, low event rates, or wide confidence intervals, which are particularly evident in studies of acupuncture combination therapy for AS. For example, several studies reported excessively wide confidence intervals due to limited sample sizes, making definitive conclusions difficult. Furthermore, inconsistencies in acupuncture parameters exacerbate heterogeneity, leading to incoherent evidence, especially in indirect comparisons, thereby reducing the reliability of network meta-analysis findings. To enhance the quality of evidence, future research should focus on the following areas: (1) establishing standardized acupuncture protocols, including uniform acupoint selection, stimulation parameters, and treatment frequency; (2) conducting large-scale, multicenter randomized controlled trials to increase statistical power; (3) implementing long-term follow-up studies to assess the sustained efficacy and safety of combined acupuncture and moxibustion therapies; and (4) employing sensitivity and subgroup analyses to explore the impact of varying operational parameters on treatment outcomes, thereby providing more precise clinical guidance. Also, placebos actually do affect treatment outcomes. Giacomo Rossettini and others point out that designing placebos for physical therapy research is tricky, “cause manual treatments” involve tons of specific and situational factors that can sway the results. He stresses that researchers should try to pick sham treatments that are hard to tell apart from the real thing, to cut down on bias. They also need to account for all the context stuff in the treatment setting—like how the therapist and patient interact, the whole treatment ritual, and so on. The big challenge is balancing these contextual factors between the test and control groups in RCT designs. You have gotta fine-tune the sham procedures to make sure the groups are really comparable. Bottom line: we should rethink how we set up RCTs to better measure the placebo’s role and boost both the internal and external validity of the studies.63
Conclusions
Based on the findings of this study, the combination therapies of 2 and 1, 4 and 11, and 1 with sulfasalazine demonstrated the most favorable outcomes. In terms of clinical translation, this study provides valuable evidence-based support for the application of acupuncture in the treatment of ankylosing spondylitis. However, to further enhance the clinical relevance and applicability of the evidence, future research should focus on addressing several key areas: establishing standardized protocols for acupuncture manipulation, including consistent acupoint selection and stimulation parameters, to improve inter-study comparability; conducting larger-scale, high-quality randomized controlled trials to increase the precision of efficacy estimates; and strengthening the evaluation of long-term efficacy and safety profiles to provide more comprehensive data for informed clinical decision-making.
Abbreviations
AS, Ankylosing Spondylitis; NSAIDs, non-steroidal anti-inflammatory drugs; SASP, sulfasalazine; RCTs, randomized controlled trials; BASDAI, Bath ankylosing spondylitis disease activity index; BASFI, Bath ankylosing spondylitis functional index; VAS, Visual Analog Scale; CNKI, China National Knowledge Infrastructure; DIC, Deviation Information Standard; CINeMA, Confidence in Network Meta-Analysis; TCM, traditional Chinese medicine; ESR, Erythrocyte sedimentation rate; CRP, C-reactive protein.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hwang MC, Ridley L, Reveille JD. Ankylosing spondylitis risk factors: a systematic literature review. Clin Rheumatol. 2021;40(8):3079–3093. doi:10.1007/s10067-021-05679-7
2. Sari İ, Ozturk MA, Akkoc N. Treatment of ankylosing spondylitis. Turk J Med Sci. 2015;45(2):416–430. doi:10.3906/sag-1401-79
3. Stolwijk C, van Tubergen A, Castillo-Ortiz JD, Boonen A. Prevalence of extra-articular manifestations in patients with ankylosing spondylitis: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(1):65–73. doi:10.1136/annrheumdis-2013-203582
4. Zuo H, Li MM. Ankylosing spondylitis and psychiatric disorders in European population: a Mendelian randomization study. Front Immunol. 2023;14:1277959. doi:10.3389/fimmu.2023.1277959
5. Kwon SR, Kim TH, Kim TJ, Park W, Shim SC. The epidemiology and treatment of ankylosing spondylitis in Korea. J Rheum Dis. 2022;29(4):193–199. doi:10.4078/jrd.22.0023
6. Su ST, Lee YH, Shih PC, Wei JC. Ankylosing Spondylitis and Cancer Risk. Int J Rheum Dis. 2025;28(1):e70085. doi:10.1111/1756-185X.70085
7. Liu S, Zheng J, Wen X, Fang Q, Zhang X. Effectiveness and safety of electroacupuncture for ankylosing spondylitis: a protocol for a systematic reviews and meta-analysis. Medicine. 2022;101(45):e31706. doi:10.1097/MD.0000000000031706
8. Yeo J, Seo MR, Park JW, et al. Literature review of non-pharmacological treatment for patients with axial spondyloarthritis. Korean J Intern Med. 2025;40(1):40–48. doi:10.3904/kjim.2023.485
9. Dang S, Ren Y, Zhao B, et al. Efficacy and safety of warm acupuncture in the treatment of ankylosing spondylitis: a protocol for systematic review and meta-analysis. Medicine. 2021;100(1):e24116. doi:10.1097/MD.0000000000024116
10. Cao X, Zhang Y, Xiao Z, Peng J. Efficacy and safety of acupuncture combined with Western medicine in the treatment of ankylosing spondylitis: a systematic review and meta-analysis. Medicine. 2025;104(21):e42468. doi:10.1097/MD.0000000000042468
11. Zhang Y, Wang X, Wang L, et al. Effects of Zhoutian moxibustion on pain symptoms and inflammatory factors in patients with ankylosing spondylitis of cold-damp obstruction. Zhongguo Zhen Jiu. 2024;44(7):797–802. Chinese. PMID: 38986593. doi:10.13703/j.0255-2930.20230616-K000.1
12. Ding W, Chen S, Shi X, Zhao Y. Efficacy of warming needle moxibustion in the treatment of ankylosing spondylitis: a protocol of a randomized controlled trial. Medicine. 2021;100(20):e25850. doi:10.1097/MD.0000000000025850
13. Liu G, Yang K, Geng J, et al. Staged treatment for 32 cases of ankylosing spondylitis with different acupuncture methods based on jingjin theory. Zhongguo Zhen Jiu. 2025;45(2):156–158. Chinese. PMID: 39943754. doi:10.13703/j.0255-2930.20240321-k0004
14. Rossettini G, Campaci F, Bialosky J, Huysmans E, Vase L, Carlino E. The biology of placebo and nocebo effects on experimental and chronic pain: state of the art. J Clin Med. 2023;12(12):4113. doi:10.3390/jcm12124113
15. Ezzatvar Y, Dueñas L, Balasch-Bernat M, Lluch-Girbés E, Rossettini G. Which portion of physiotherapy treatments’ effect is not attributable to the specific effects in people with musculoskeletal pain? A meta-analysis of randomized placebo-controlled trials. J Orthop Sports Phys Ther. 2024;54(6):391–399. doi:10.2519/jospt.2024.12126
16. Chinese Rheumatology Association, Chinese Medical Association. Guidelines for the diagnosis and treatment of ankylosing spondylitis. Chin J Rheumatol. 2010;14(08):557–559. doi:10.3760/cma.j.issn.1007-7480.2010.08.012
17. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
18. Zochling J. Measures of symptoms and disease status in ankylosing spondylitis: Ankylosing Spondylitis Disease Activity Score (ASDAS), Ankylosing Spondylitis Quality of Life Scale (ASQoL), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Global Score (BAS-G), Bath Ankylosing Spondylitis Metrology Index (BASMI), Dougados Functional Index (DFI), and Health Assessment Questionnaire for the Spondylarthropathies (HAQ-S). Arthritis Care Res. 2011;63(Suppl 11):S47–58. doi:10.1002/acr.20575 PMID: 22588768.
19. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in r and omised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. Nikolakopoulou A, Higgins JPT, Papakonstantinou T, et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17:e1003082. doi:10.1371/journal.pmed.1003082
22. Meng JH, Huang D, Sun L. Clinical study of 60 cases of ankylosing spondylitis treated with triple drug plus small needle knife. Chin Med Innov. 2009;6(26):54–55.
23. Zhou ZH, Chen Z, Xu Z. Clinical study on the treatment of ankylosing spondylitis with warm acupuncture and Jiaji acupoints. J Clin Acupunct Moxibustion. 2011;27(03):11–13.
24. Zhang L, Wang Z. Big moxibustion therapy to treat ankylosing spondylitis clinical research. J Chin Med. 2012;27(8):1065–1066. doi:10.16368/j.iSSN.1674-8999.2012.08.044
25. Hu JG, Chen X, Deng Y, et al. Drug moxibustion combined treatment of ankylosing spondylitis the clinical study. J Liaoning Tradit Chin Med. 2013;40(03):497–499. doi:10.13192/j.lJTCM.2013.03.119.Hujg.018
26. Li H-L, Yang D. Observation on the therapeutic effect of Sanfu Acupoint application on ankylosing spondylitis. Hubei J Tradit Chin Med. 2014;36(10):17–19.
27. Liang CM, Zhang J, Zhang X, et al. Strong spleen du decoction and dragon moxibustion treatment of ankylosing spondylitis the clinical research. J Chin Med. 2015;30(7):1071–1073. doi:10.16368/j.iSSN.1674-8999.2015.07.370
28. Wang HQ. Evaluation of the clinical effect of Traditional Chinese Medicine moxibustion combined with sulfasalazine in the treatment of ankylosing spondylitis. J Clin Rational Drug Use. 2015;8(5):72–73. doi:10.15887/j.carolcarrollnki.13-1389/r.2015.05.044
29. Feng H, Ma Y, Wang X. Du moxibustion treatment of kidney Yang deficiency type of ankylosing spondylitis the clinical control study. J Shanghai Acupunct Mag. 2016;35(10):1245–1247. doi:10.13460/j.iSSN.1005-0957.2016.10.1245
30. Zhang MY, Song Y, Li Y. Clinical observation on the treatment of ankylosing spondylitis with Du Meridian ginger moxibustion combined with functional exercise and Western medicine. Rheumatism Arthritis. 2016;5(01):8–10+40.
31. Zhao L, Zhao Y. Observation on the clinical efficacy of acupuncture at the eight points of the waist in the treatment of ankylosing spondylitis. China Continuing Med Edu. 2016;8(12):171–172.
32. Huang ZQ, Fu C, Su Z, et al. Clinical observation on the treatment of early ankylosing spondylitis with Dazhui wheat grain moxibustion combined with sulfasalazine and functional exercise. Rheumatism Arthritis. 2017;6(07):23–28.
33. Zhang XJ, Ye M, Li T, et al. Floating needle combined ridge bi pill treatment of ankylosing spondylitis the clinical observation. J Henan Tradit Chin Med. 2017;5(6):1091–1093. doi:10.16367/j.iSSN.1003-5028.2017.06.0386
34. Bai H. Moxibustion treatment of ankylosing spondylitis the clinical study. J Henan Tradit Chin Med. 2018;38(01):111–114. doi:10.16367/j.iSSN.1003-5028.2018.01.0029
35. Zhang HH, Wang Z, Zhang Z, et al. Clinical observation of Du Meridian moxibustion combined with acupuncture in the treatment of ankylosing spondylitis. Mod Distance Educ Tradit Chin Med. 2019;17(10):91–93.
36. Gao TZ, Huang G. Observation on the efficacy of drugs combined with warm acupuncture in the treatment of ankylosing spondylitis. Hubei J Tradit Chin Med. 2019;41(04):17–19.
37. Liu H, Wang X, Li J. Clinical study on the treatment of ankylosing spondylitis with acupuncture and Massage combined with sulfasalazine enteric-coated tablets. Int J Tradit Chin Med. 2019;9(9):936–940. doi:10.3760/cma.J.iSSN.1673-4246.2019.09.006
38. Li Z, Wang J, Wen X, et al. Du Meridian moxibustion box moxibustion treatment of kidney Yang deficiency type of ankylosing spondylitis the clinical study. J Henan Tradit Chin Med. 2020;40(6):909–912. doi:10.16367/j.iSSN.1003-5028.2020.06.0230
39. Yao ZC, Huang X, Zhuo S. Clinical observation on the treatment of early and middle stage ankylosing spondylitis with Du Meridian moxibustion combined with sulfasalazine. New Tradit Chin Med. 2020;52(6):114–117. doi:10.13457/j.carolcarrollnkiJNCM.2020.06.036
40. Xie FL, Zhang X, Zeng T. Observation on the therapeutic effect and nursing experience of Fire Dragon Moxibustion Combined with comprehensive Nursing in the treatment of ankylosing spondylitis. Massage Rehabil Med. 2021;12(3):13,16. doi:10.19787/j.iSSN.1008-1879.2021.03.005
41. Cao ZY, Yang L. Observation on the efficacy of Qiangjiyan formula combined with acupuncture in the treatment of liver and kidney insufficiency syndrome in early ankylosing spondylitis based on the theory of “Liver and Kidney Homology”. Hebei J Chin Med. 2021;43(09):1435–1439.
42. Li N, Yuan Q, Zhang J. Clinical observation on the treatment of kidney deficiency and cold Du type ankylosing spondylitis with bladder Meridian moxibustion by Wandering cupping. J Liaoning Univ Tradit Chin Med. 2021;23(12):130–133. doi:10.13194/j.iSSN.1673-842-x.2021.12.027
43. Wang WY, Zhao C, Zhang M, et al. Clinical observation on the treatment of ankylosing spondylitis of kidney deficiency and cold Du type with Liji Acupuncture combined with Du Moxibustion. Clin Res Tradit Chin Med. 2022;14(04):45–48.
44. Wang ZR, Li Y, Zhang J. Observation on the efficacy of Acupotomy combined with sulfasalazine in the treatment of ankylosing spondylitis. China J. 2022;49(7):120–123. doi:10.3760/cma.J.c.n115689-20220112-00157
45. Wang P, Liu Y, An Y, et al. Clinical study on the treatment of kidney deficiency and cold du type ankylosing spondylitis with leihuo moxibustion combined with Western medicine. Shaanxi J Tradit Chin Med. 2023;44(06):789–793.
46. Fang WF. Clinical Observation of Small needle knife closure release Combined with Chinese herbal fumigation as an adjunctive treatment for ankylosing spondylitis. J Pract Chin Med. 2023;39(01):119–121.
47. Li XF, Liao F, Huang Z, et al. Du Meridian acupuncture combined with clip ridge point acupuncture method for curative effect observation of ankylosing spondylitis. J Pract Comb Tradit Chin West Med Clin. 2024;24(23):1–3+11. doi:10.13638/j.iSSN.1671-4040.2024.23.001
48. Yi KL, Feng S, Liu D, et al. Observation on the therapeutic effect of Du Meridian Moxibustion combined with Zhuangdu Quhan mixture in the treatment of kidney deficiency and Du cold type ankylosing spondylitis. J Mod Integr Chin West Med. 2024;33(12):1691–1695.
49. Lu ZS, Cheng X, Gelima, et al. The effect of floating needle combined with reperfusion activity on ankylosing spondylitis. Guangming Chin Med. 2024;39(04):726–729.
50. Luo YX, Zhong D, Huang Y, et al. Acupuncture clinical observation of treatment of ankylosing spondylitis patients with sleep disorders. J Guangzhou Univ Tradit Chin Med. 2024;9(12):3210–3215. doi:10.13359/j.carolcarrollnkiGZXBTCM.2024.12.019
51. Zhang YF, Wang X, Wang L, et al. The effect of Zhoutian moxibustion on pain symptoms and inflammatory factors of cold-dampness obstruction type ankylosing spondylitis. Chin Acupunct Moxibustion. 2024;44(07):797–802. doi:10.13703/j.0255-2930.20230616-k0001
52. Wang P, Wang L, Kang J. Improvement of bone marrow edema and effects of anti-inflammatory factors, joint state and serum HLA-B27, Cbfa1 in kidney deficience-cold type ankylosing spondylitis. J Liaoning Univ Tradit Chin Med. 2025:1–12.
53. Zhao W, Liu W, Wu Y. Meta-analysis of randomized controlled clinical trials on acupuncture treatment for ankylosing spondylitis. Chin J Basic Med Tradit Chin Med. 2018;24(12):1743–1749+1766. doi:10.19945/j.cnki.issn.1006-3250.2018.12.027
54. Dong P, Yuan P, Marshal B, Wang Z, Zhang C, Gao Y. Research progress on Acupotomy therapy for ankylosing spondylitis. Hebei J Chin Med. 2024;46(11):1918–1921.
55. Zhong Y. Research on the effect of acupuncture therapy in the treatment of ankylosing spondylitis. Contemp Med Rev. 2015;13(24):282–283.
56. Shi C. Clinical observation on the treatment of ankylosing spondylitis with small needle knife. Gansu Med. 2013;32(8):617–618.
57. Xi Y, Xu L, Zhao T, et al. A systematic review and meta-analysis of Acupotomy therapy for limited movement in ankylosing spondylitis. J Yunnan Coll Tradit Chin Med. 2021;44(3):56–64. doi:10.19288/j.carolcarrollnki.Issn1000-2723.2021.03.011
58. Liao WJ. Effects of sulfasalazine combined with moxibustion methods on patients with cold-dampness obstruction type ankylosing spondylitis. Pak J Pharm Sci. 2020.
59. Chen Z. [Acupuncture assisted by dynamic moxibustion for adult ankylosing spondylitis at early-to-mid stage]. Zhongguo Zhen Jiu. 2016. Dutch
60. Wang Z, Xi Y. Quantitative research progress of cupping technique. Nurs Res. 2018;32(20):3166–3168.
61. Li L, Wang Y. Meta-analysis of the improvement of spinal range of motion in patients with ankylosing spondylitis by Du Moxibustion. Gen Nurs. 2023;21(05):581–586.
62. He J, Li M, Li C, et al. Du moxibustion treatment of ankylosing spondylitis Meta analysis. Chin J Trad Chin Med. 2020;38(02):102–107. doi:10.13193/j.iSSN.1673-7717.2020.02.027
63. Rossettini G, Testa M. Manual therapy RCTs: should we control placebo in placebo control? Eur J Phys Rehabil Med. 2018;54(3):500–501. doi:10.23736/S1973-9087.17.05024-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024
Acupuncture and Related Therapies for Endometriosis: A Network Meta-Analysis of Randomized Controlled Trials
Li H, Wang X, Wang Y, Gao Y, Zheng X, Zhang X, Li X, Zheng X, Fan X, Zuo G, She Y
Journal of Pain Research 2024, 17:3197-3216
Published Date: 2 October 2024
Efficacy of Different Acupuncture Therapies for Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Network Meta-Analysis

Qin P, Cao X, Ni H, Yang L, Tong Y, Dang M, Xu J
Journal of Pain Research 2025, 18:3653-3673
Published Date: 17 July 2025
Different Acupuncture Treatments for Myofascial Pain Syndrome in Neck or Shoulder: A Network Meta-Analysis Based on Randomized Controlled Trials
Wang T, Gu Y, Li Y, Chen J, Zeng L
Journal of Pain Research 2025, 18:4289-4305
Published Date: 24 August 2025
Efficacy and Safety of Acupuncture and Acupuncture-Combined Therapies in the Treatment of Sciatica Caused by Lumbar Disc Herniation: A Network Meta-Analysis
Ni D, Tong H, Wei S, Zheng Y, Wu W, Li M, Dong Y
Journal of Pain Research 2025, 18:4809-4832
Published Date: 16 September 2025